Embed Size (px)
Citation preview

ARDSARDS
DR. T. MOHAN KUMAR, MD, AB, DPPR, FCCPDR. T. MOHAN KUMAR, MD, AB, DPPR, FCCP
CHIEF & SENIOR CONSULTANT,CHIEF & SENIOR CONSULTANT,
DEPARTMENT OF PULMONOLOGY & CRITICAL DEPARTMENT OF PULMONOLOGY & CRITICAL CARE,CARE,
SRI RAMAKRISHNA HOSPITAL,SRI RAMAKRISHNA HOSPITAL,
COIMBATORECOIMBATORE

30/07/2000 DR.T.M.K- ARDS 2
DIAGNOSTIC CRITERIA
ARDSAcute
PaO2/Fio2<200 mmHg
Bilateral interstitial
or alveolar infiltrates
Pcwp <15-18 mmHg
ALIAcute
<300 mm Hg
Same
same

30/07/2000 DR.T.M.K- ARDS 3
Clinical diagnosisRapidWithin 12 to 48 hr of the predisposing eventAwake patients become anxious,agitated &
dyspnoeicDyspnoea on exertion proceeding to severe when hypoxemia intervenesStiffening of lung leads to increase work of breathing,small tidal volumes,rapid respiratory rateInitially respiratory alkalosis Respiratory failure

30/07/2000 DR.T.M.K- ARDS 4
Clinical disorders associated with ARDS
Direct lung injury Aspiration of
gastric contents Pulmonary
contusion Toxic gas
inhalation Near drowning Diffuse pulmonary
infection
Indirect lung injury Severe sepsis Major trauma Hypertransfusion Acute pancreatitis Drug overdose Reperfusion injury Post cardiac
bypass/lung transplants

30/07/2000 DR.T.M.K- ARDS 5
Clinical disorders associated with ARDS
FREQUENT CAUSES
SEPSISBACTEREMIA WITHOUT SEPSIS SYNDROME 4%
SEVERE SEPSIS/SEPSIS SYNDROME 35-45%
MAJOR TRAUMA
MULTIPLE BONE FRACTURES 5-10%PULMONARY CONTUSION 17-22%
HYPERTRANSFUSION 5-36%ASPIRATION OF GASTRIC CONTENTS 22-36%

30/07/2000 DR.T.M.K- ARDS 6
CLINICAL MANIFESTATIONS
ARDS occurs in the setting of acute severe illnessClinical manifestations may varySepsis and trauma most importantMultiple organ failureAtelectasis and fluid filled lungsHypoxemia/dyspnoeaFever /leukocytosis

30/07/2000 DR.T.M.K- ARDS 7
Laboratory studiesTo date no lab findings pathognomonic of ARDS
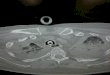
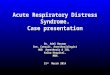
X-ray chest shows bilateral infiltrates consistent with pulmonary edema, may be mild or dense, interstitial or alveolar, patchy or confluent
ABG shows hypoxemia with respiratory alkalosis. In late stages hypoxemia, acidosis, hypercarbia may be seen.

30/07/2000 DR.T.M.K- ARDS 8
Leukocytosis/Leukopenia/anemia are common
Renal function abnormalities/or liver function
Von willebrand’s factor or complement in serum may be high
Acute phase reactants like ceruloplasmin or cytokine (TNF,IL-1,IL-6,IL-8) may be high.

30/07/2000 DR.T.M.K- ARDS 9
BRONCHOALVEOLAR LAVAGEInflammatory mediators like cytokines, reactive oxygen species, leukotrienes & activated complement fragments are found in the fluid
Cellular analysis shows more than 60% of neutrophils.
As ARDS resolves neutrophils are replaced with alveolar macrophages.
Another interesting finding is the presence of a marker of pulmonary fibrosis called procollagen peptide III (PCPIII) and this correlates with mortality.
Presence of more eosinophils suggest eosinophilic pneumonia, high lymphocyte counts may be seen in hypersensitivity pneumonitis, sarcoidosis, BOOP, or other acute forms of interstitial lung disease.

30/07/2000 DR.T.M.K- ARDS 10
Differential diagnosis
Infectious causes Bacteria - Gm neg & pos , mycobacteriae,
mycoplasma, rickettsia, chlamydia
Viruses- CMV, RSV, hanta virus, adeno virus, influenza virus
Fungi- H.capsulatum, C.immitis
parasites- pneumocytis carinii, toxoplasma gondii

30/07/2000 DR.T.M.K- ARDS 11
Differential DiagnosisNon infectious causes
CCF Drugs & toxins (paraquat, aspirin, heroin, narcotics,
toxic gas, tricyclic anti depressants, acute radiation pneumonitis)
Idiopathic (esinophilic pneumonia, Acute interstitial pneumonitis, BOOP, sarcoidosis, rapidly involving idiopathic pulmonary fibrosis)
Immunologic (acute lupus pneumonitis, Good Pastures syndrome, hypersensitivity pneumonitis)
Metabolic (alveolar proteinosis) Miscellaneous (fat embolism, neuro/high altitude
pulmonary oedema) Neoplastic (leukemic infiltration, lymphoma)

30/07/2000 DR.T.M.K- ARDS 12
Therapy -goals
Treatment of the underlying precipitating eventCardio-respiratory supportSpecific therapies targeted at the lung injurySupportive therapies

Respiratory Support

30/07/2000 DR.T.M.K- ARDS 14
Spontaneously Breathing Patient
In the early stages of ARDS the hypoxia may be corrected by 40 to 60% inspired oxygen with CPAP
Peak inspiratory flow rates of >= 70ltrs / min require a tight-fitting face mask with a large reservoir bag or a high flow generator
If the patient is well oxygenated on <= 60 % inspired oxygen and apparently stable without CO2 retention and apparently stable, then ward monitoring may be feasible but close observation( 15 to 30 Min), continuous oximetry, and regular blood gases are required
Contd..

30/07/2000 DR.T.M.K- ARDS 15
Indications for mechanical ventilation
Inadequate Oxygenation(PaO2 < 8k Pa on FiO2 >= 0.6)
Rising or elevated PaCO2(>= 6k Pa) Clinical signs of incipient
respiratory failure

30/07/2000 DR.T.M.K- ARDS 16
Mechanical Ventilation
The Aims are to increase PaO2 while
minimizing the risk of further lung injury
(Oxygen toxicity, Barotrauma). This is
the realm of the IRCU Physician: seek
specialist advice early to prevent
complications. The general principles are
the following:
Contd..

30/07/2000 DR.T.M.K- ARDS 17
Start with FiO2 = 1.0, tidal volume 6 to 10 ml per Kg, PEEP <= 5 cm H2O and inspiratory flow rates ~ 60 L / min. Subsequent adjustments are done to try to achieve arterial oxygen sats. of > 90% with FiO2 < 0.6 and peak airway pressures < 40 to 45 cm H20
Controlled Mandatory Ventilation (CMV) with sedation and neuromuscular blockade (to try to suppress the respiratory drive and reduce respiratory muscle oxygen requirement.)

30/07/2000 DR.T.M.K- ARDS 18
PEEP improves PaO2 in most patients and allows reduction of FiO2. Increase by 2 to 5 cm H2O increments every 20 min watching for hemodynamic deterioration (due to impaired venous return and decreased cardiac out put). Optimal PEEP is usually 10 to 15 cm H2OInverse Ratio Ventilation may decrease peek inflation pressures and thus Barotrauma. Inspiratory time : Expiratory time ratio (I:E ratio) of between 1:1 and 4:1 may be tried.
Contd..

30/07/2000 DR.T.M.K- ARDS 19
The ventilatory rate required to clear CO2 and normalize pH is commonly high (20 to 25 breaths / min). However this may result in unacceptable airway pressures.
Another strategy is’ permissive hypercapnoea’ which as the name suggests is controlled hypoventilation. PaCO2 up to 13 kPa is generally well tolerated; acidosis (pH < 7.25) may be treated with intravenous bicarbonate

30/07/2000 DR.T.M.K- ARDS 20
Changing the patients position (lateral decubitus or prone instead of supine) can improve oxygenation by improving perfusion of aerated portion of lung. Consider this in patients with non uniform or predominantly posterior and lower lobe infiltrates
Inhaled nitric oxide (18 ppm) reduces pulmonary artery pressures, intra pulmonary shunting and improves oxygenation while not affecting mean arterial pressure or cardiac output. However studies showing an effect on mortality are awaited.
Newer methods such as high frequency jet ventilation, extra corporeal gas exchange (CO2 removal +- Oxygenation) and intravascular oxygenation devices (IVOX) may be of use but are currently not widely available.

Cardiovascular Support

30/07/2000 DR.T.M.K- ARDS 22
Invasive monitoring is mandatory(Arterial line, PA catheter (Swan-Ganz) to measure cardiac outputs and if available, continuous mixed venous oxygen saturation)
In order to minimize pulmonary oedema, aim to keep PCWP low (8 to 10 mm Hg) and support the circulation with inotropes if necessary
The role of colloids and albumin is relatively minor: the increased capillary permeability allows these molecules to equilibrate with the alveolar fluid with little increase in net plasma oncotic pressure
Contd..

30/07/2000 DR.T.M.K- ARDS 23
Renal failure is common and may require haemofiltration to achieve a negative fluid balance and normalize blood chemistry.
Oxygen consumption (VO2) in patients with ARDS appears to be delivery dependent. The current trend is to aim for target levels of oxygen delivery (DO2 = Cardiac Index(HbXSao2X1.34)X10) as guided by tissue perfusion (clinically and serum lactate, pHi from a gastric tonometer). DO2 may be increased by blood transfusion, inotropes and vasodilators including prostacyclin).

30/07/2000 DR.T.M.K- ARDS 24
Selection of appropriate inotropes and vasodilators can only be made by repeated measurements of haemodynamic parameters and calculating DO2 and VO2 while evaluating the effects of the various agents
Nutritional support must be chosen to try to avoid fluid overload. Lipid metabolism produces marginally less CO2 than dextrose metabolism and thus favourably affects the respiratory quotient but there is controversy as to whether lipid can exacerbate lung injury

Treatment of Sepsis

30/07/2000 DR.T.M.K- ARDS 26
Fever, Neutrophil leukocytosis and raised inflammatory markers (CRP) are common in patients with ARDS and do not always imply sepsis. However sepsis is common precipitant of ARDS
A trial of empirical antibiotics guided by possible pathogens should be given early. Eg Cefotaxime. This may be modified in light of the results of appropriate cultures. Avoid nephrotoxic antibiotics.
Enteral feeding seems to carry a lower risk of sepsis than parenteral feeding and helps maintain the integrity of the gut mucosa. Ileus is common in multi-organ failure, so entral feeding may not be possible.

Minimizing lung injury and treating the cause

30/07/2000 DR.T.M.K- ARDS 28
Look for a precipitant
In general prevention (example of aspiration of gastric acid) is more effective than trying to treat ARDS. However there are no effective measures for prophylaxis in patients at risk ( Eg from Trauma)
Steroids : there is no benefit from treatment early in the disease. Treatment later (> 7 to 14 days from onset) especially in patients with peripheral blood eosinophilia or eosinophils in bronchoalveolar lavage, improves prognosis

30/07/2000 DR.T.M.K- ARDS 29
Give 2 to 4 mg / Kg prednisolone or equivalent: the duration depends on the clinical response( 1 to 3 weeks)
Other therapies such as inhaled nitric oxide , exogenous surfactant, antioxidants (acetylcysteine), ketoconazole, NSAIDs, Pentoxifylline and anticytokine antibodies are still under investigation

30/07/2000 DR.T.M.K- ARDS 30
Causes of Sudden deterioration in ARDS
Respiratory Cardiovascular
Pneumothorax Arrhythmia
Bronchial plugging Cardiac tamponade
Displaced ET tube Myocardial infarction
Pleural effusion (Haemothorax)
GI bleed(Stress Ulcer)
Aspiration(Eg NG feed)
Septicaemia

30/07/2000 DR.T.M.K- ARDS 31
Completed trialsReducing lung stretching
Lisophyllin
Corticosteroids in late ARDS
ALVEOLI study

30/07/2000 DR.T.M.K- ARDS 32
Completed trials -II Fluids and catheters treatment trial (FACTT)
Low tidal volume versus high tidal volume ventilation
Ketoconazole
Role of MODS

30/07/2000 DR.T.M.K- ARDS 33
WHAT IS NEW?ALI & Gene transfer
New approaches to enhancing lung edema clearance
Nitric oxide donors
New treatment for altered pulmonary vascular permeability
Inflammatory & cytokine networks in ARDS

30/07/2000 DR.T.M.K- ARDS 34
What is new
Use of surfactant therapy
Liquid ventilation in ALI
CPAP trial