Embed Size (px)
Citation preview

ARDS
ITACCS Key West 2006
Ruben J Azocar, M.D.Assistant Professor of AnesthesiologyBoston University School of Medicine

ARDS: DefinitionsARDS: Definitions First described in 1967 as Adult Respiratory
Distress Syndrome American-European Consensus Conference
Committee (1994) criteria– Acute onset– Bilateral infiltrates in chest radiography– Pulmonary-artery wedge pressure<18 mmHg– Acute lung injury PaO2/FiO2<300– Acute respiratory distress syndrome PaO2/FiO2<200

ARDS: CausesARDS: Causes

ARDS:EpidemiologyARDS:Epidemiology
Incidence: 80 per 100,000 Outcomes:
– Traditionally 40-60% mortality– Majority of deaths due to MSOF– Low tidal volume ventilation decreases mortality – Other critical care improvements may be involved– Predictive factors for death: CLD, non pulmonary
organ dysfunction, sepsis and advance age– Survivors: Most of them will have normal
pulmonary function within a year

ARDS:PathogenesisARDS:Pathogenesis
ARDS is the manifestation of SIRS in the lungs– Influx of protein rich edema into the air spaces due
to increased permeability of the alveolar-capillary barrier
Endothelial damage pathophysiology is similar to that of SIRS/SEPSIS

ARDS:PathogenesisARDS:Pathogenesis
– Epithelial damage Loss of epithelial integrity which in normal
conditions less permeable than endothelium Type II cells injury
– disrupts normal epithelial fluid transport– reduces production of surfactant
May lead to septic shock in patients with pneumonia
Severely injured epithelium lead to disorganized repair and fibrosis

ARDS:PathogenesisARDS:Pathogenesis
Neutrophils Cytokines
– Unbalanced production of pro-inflammatory and anti-inflammatory cytokines
Ventilator induced injury– High FiO2– Overdistention– Recruitment/De-recruitment– May exacerbate and perpetuate ARDS/ALI as well
as SIRS/Sepsis/MSOF

ARDS: Exudative PhaseARDS: Exudative Phase
The definition applies for the acute “exudative” phase Rapid onset Hypoxemia refractory to supplemental oxygen CXR similar to pulmonary edema CT Scan: Alveolar filling, consolidation and
atelectasis in the dependent lung zones Pathologic findings:
– diffuse alveolar damage with capillary injury and disruption of the alveolar epithelium
– hyaline membranes – protein rich fluid edema with neutrophils and
macrophages

ARDS:PathogenesisARDS:Pathogenesis

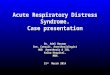
ARDS: Exudative PhaseARDS: Exudative Phase CT Scan During Acute Phase

ARDS: Fibroproliferative phaseARDS: Fibroproliferative phase
Some patients progress to fibrosing alveolitis with persistent hypoxemia, increase alveolar dead space and further decrease in pulmonary compliance
The process may start as early as 5-7 days The alveolar space becomes filled with
mesenchymal cells and their products as well as new blood vessels

ARDS: Fibroproliferative phaseARDS: Fibroproliferative phase
Pulmonary HTN due to obliteration of pulmonary bed may lead or worsen RV dysfunction
CXR shows linear opacities. PTX and bullae are common Histologically, there is fibrosis and partial
resolution of the pulmonary edema Mortality is 80% if this phase persists

ARDS: Fibroproliferative phaseARDS: Fibroproliferative phaseCT Scan during fibroproliferative phase.
– Diffuse interstitial opacities and bullae

ARDS:PathogenesisARDS:Pathogenesis

ARDS:TreatmentARDS:Treatment
Recent decrease of mortality – Treatment of underlying cause– Better supportive ICU Care
Prevention of infections Appropriate nutrition GI prophylaxis Thromboembolism prophylaxis

ARDS TreatmentARDS Treatment
Mechanical ventilation– Buys time for the lungs to heal and solve the
inciting cause – “New” ventilator strategies
Recognition of ventilator induced injury (VILI)– Overdistention – Recruitment/de-recruitment
Mechanical ventilation induces cytokine response which is worse with alveoli overdistention and recruitment/ de-recruitment of the lung (Ranieri et al JAMA 1999;282: 54-61)

ARDS: TreatmentARDS: Treatment

ARDS: TreatmentARDS: Treatment
Protective ventilation– Smaller tidal volumes
• Avoid overdistention• Tolerate “permissive hypercarbia”
– “Open lung” ventilation• Avoid alveolar collapse and reopening

Ventilation with Lower Tidal Volumes Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal as Compared with Traditional Tidal
Volumes for Acute Lung Injury and the Volumes for Acute Lung Injury and the Acute Respiratory Distress SyndromeAcute Respiratory Distress Syndrome
The Acute Respiratory Distress Syndrome Network The Acute Respiratory Distress Syndrome Network N Engl J Med 2000;342:1301-8N Engl J Med 2000;342:1301-8
Study stopped after 2nd interim analysis
Reduction of mortality by 22%

NIH/ARDS NetworkNIH/ARDS Network VARIABLES
– Ventilator mode– Tidal Volume– Plateau Pressure– Ventilation rate/pH
goal– Inspiration flow, I:E– Oxygenation goal
– FIO2/PEEP– Weaning
PROTOCOL– Volume assist control– < 6mL/Kg body weight– <30 cm H2O– 6-35/min adjusted for pH of
7.30 if possible– Adjust to 1:1-1:3– PaO2>55 and or
SpO2>88%– Combinations– PS wean when
FiO2/PEEP<.40/8

Ventilation with Lower Tidal VolumesVentilation with Lower Tidal Volumes
The goal of providing small tidal volumes is to maintain the patient on the steep, more compliant portion of the curve without exceeding the upper inflection point

ARDS:Permissive HypercapniaARDS:Permissive Hypercapnia
Hypercarbic acidosis– Hypoxemia– Respiratory failure and
arrest– Decrease myocardial
contractility– Cerebral vasodilatation– Decrease seizure
threshold– Hyperkalemia
Permissive hypercapnia– Supplemental oxygen
overcomes CO2 induced hypoxia
– No evolution to respiratory arrest
– Lack of significant deleterious effects
– Is hypercarbia beneficial?

Kregenov et al: Hypercapnic acidosis and Kregenov et al: Hypercapnic acidosis and mortality in ALI mortality in ALI CCM 2006;34:1-7CCM 2006;34:1-7
Patients from the low tidal volume trial
Hypercapnic acidosis was associated with reduced 28-day mortality in the 12 mL/kg VT group after controlling for comorbidities and severity of lung injury.
These results are consistent with a protective effect of hypercapnic acidosis against ventilator-associated lung injury that was not found when the further ongoing injury was reduced by 6 mL/kg predicted body weight tidal volumes.

Effect of a protective ventilation strategy Effect of a protective ventilation strategy on mortality in ARDSon mortality in ARDS
Amato M et al NEJM 1998;338:347-354Amato M et al NEJM 1998;338:347-354 End-expiratory pressure above the lower inflection
point VT less 6ml/kg Driving pressures less than 20 cm H2O above PEEP Permissive hypercarbia 38% Mortality in protective group vs. 71% in control
group 66% of patient in “protective” group wean off
ventilation vs. 29% control group No difference in survival at 28 days

Optimal “PEEP”Optimal “PEEP”
Positive end-expiratory pressure should be high enough to shift the end-expiratory pressure above the lower inflection point by 2-3 cm H2O (usually 12-15 cm H2O)
– Allows maximal alveolar recruitment
– Decreases injury by repeated opening and closing of small airways

Slutsky, A. S. et al. N Engl J Med 2006;354:1839-1841
Ventilation of an ex Vivo Rat Lung

Higher Vs. Lower PEEP in Higher Vs. Lower PEEP in Patients With ARDS, Patients With ARDS, NEJM 2004NEJM 2004
NIH/ARDS Trail Network549 patientsLower PEEP 8.3+/- 3.2Higher PEEP 13.2+/-3.5All on low tidal volume ventilationNo differences on clinical outcomeTrial stop due to rule of futility

BUT…..BUT….. In the first 171 patients: “the difference in
mean PEEP levels between study groups on days 1 to 7 was less that the difference in the previous study that tested the effects of higher PEEP levels and smaller tidal volumes”
Should have these patients not been included, would have the trial been stopped early?

ARDS: TreatmentARDS: Treatment
Recruiting maneuvers Prone positioning Steroids APRV
Volume cycle vs. pressure cycle Inverse-Ratio Ventilation Non invasive Positive Pressure Ventilation High-Frequency Ventilation Tracheal Gas Insufflation Extracorporeal gas exchange Fluorocarbon Liquid Gas Exchange

Recruitment maneuversRecruitment maneuvers
Lung recruitment in patients with ARDS Gattinoni NEJM 2006;354:1175-86
– Sixty eigt patients with ALI/ARDS underwent whole lung CT Scan during breath holding session at airway pressures of 5, 15 and 45 cm of water
– The percentage of potentially recruitable lung was defined as the proportion of lung tissue in which aeration was restored (Recruited)

RecruitmentRecruitment The potentially recruitable lung was significantly
variable but highly correlated with the percentage of lung tissue in which aeration was maintained with PEEP
Patients with more recruitable lung were sicker– Greater lung weight– Poorer oxygenation– Poorer compliance– Higher levels of death space– Higher mortality

RecruitmentRecruitment
Knowing the % of recruitable lung might be the key to the effects of PEEP
PEEP in patients with limited recruitable areas might be of little benefit or harmful– Overdistention– Worsening of Shunt– Authors suggest PEEP of 15 for those
recruitables and 10 for those who are not

ARDS TreatmentARDS Treatment
Prone positioning– In about 70% of ARDS patients, prone positioning
improves the PaO2 by > 20%
– Consider a lung recruitment strategy, since allows a decrease in FiO2 and PEEP
– A more uniform distribution of pleural pressure gradients, result in greater ventilation of dependent lung than in supine positioning

ARDS TreatmentARDS Treatment
Gattinoni et al, NEJM 2001;345:568-573– 304 patients with ARDS– Prone group: at least six hours/day for ten days– Better oxygenation in the prone patients– Similar incidence of complications– No improvement in survival– However patient only prone for 7 hours a day and
up to 10 days

ARDS TreatmentARDS Treatment
Fluid and hemodynamic management– Optimal fluid management is controversial
There is data supporting fluid restriction as a mean to minimize lung edema
However maintenance and preservation of oxygen delivery may require fluid administration
– Euvolemia, judicious use of vasopressors– Effects of ventilation in circulation– To Swan or not to Swan

Swan and ARDSSwan and ARDS
PAC versus CVP to guide treatment of ALI NEJM 2006; 354: 2213-2224
– 1000 patients– Mortality at 60 days was similar between
groups, as well as the ventilator free days and days not spent in the ICU
– Fluid balances were similar among the groups
– PAC had double complications mainly arrhythmias

APRVAPRV
It uses a release of airway pressure from an elevated baseline to simulate expiration.
The elevated baseline facilitates oxygenation avoids collapsing of alveoli and the timed releases aid in carbon dioxide removal.
Potential advantages of APRV include lower airway pressures, lower minute ventilation, minimal adverse effects on cardio-circulatory function.
Airway pressure release ventilation is consistent with lung protection strategies that strive to limit lung injury associated with mechanical ventilation, particularly recruitment/derecruitment
More (larger) studies are needed to define its role in ALI/ARDS

ARDS:TreatmentARDS:Treatment Inhaled nitric oxide and other vasodilators
– Most ARDS/ALI patient may have mild to moderate pulmonary HTN
– Improvement in oxygenation was small and not sustained
– No change on mortality or duration of mechanical ventilation
– May be used as “rescue” therapy
Surfactant– Successful in neonatal respiratory distress
syndrome

ARDS: TreatmentARDS: Treatment Glucocorticoids
– No benefits in acute phase– Some evidence of improvement during
proliferative phase (Meduri et al JAMA 1998;280:159-165)
Methylprednisolone 2mg/kg initially for 32 days Improvement in Lung injury scores, MOSD scores and
mortality Benefits may be noticed by day 3
– High risk of infection– ? May consider a short course of high dose as
rescue therapy

ARDS: SteroidsARDS: Steroids Efficacy and safety of corticosteroids for persistent
acute respiratory distress syndrome NEJM 2006.354: 1671-84
– 180 patients – Mortality at 60 days
28.9% mortality in the placebo group and 29.2% in the methylprednisolone group
Methylprednisolone increased the number of ventilator free and shock free days during the first 28 days in association with an improvement in oxygenation, respiratory system compliance and blood pressure with fewer vasopressor days
But methylprednisolone was associated with a significant increase 60-180 days mortality in patients enrolled at least 14 days after the onset of ARDS

ARDS: TreatmentARDS: Treatment
Anti-inflammatory Strategies– Prostaglandin agonist/inhibitors– Lisofylline and pentoxifylline– Anti IL-8
Antioxidant therapyEnhanced resolution of pulmonary
edemaEnhanced repair of alveolar epithelial
barrier

ARDS: QuestionsARDS: Questions



Azocar - El Cuerpo de Los Complejos(Esp)](https://img.dokumen.tips/doc/110x75/5695cf0e1a28ab9b028c648b/matematicaedmirazocar-el-cuerpo-de-los-complejosesp.jpg)