Embed Size (px)
Citation preview

Optimizing the Treatment of
Hematologic Malignancies With HSCT
Sergio A. Giralt, MD
Melvin Berlin Family Chair in Myeloma Research
Professor of Medicine
Weill Cornell Medical College
Chief Attending, Adult BMT Service
Memorial Sloan Kettering Cancer Center

Disclosures
Dr. Giralt discloses the following commercial
relationships:
Advisory Board: Amgen, Celgene, Jazz Pharmaceuticals, Kite
Pharma, Novartis, Sanofi, Takeda
Research Support: Amgen, Celgene, Janssen Pharmaceuticals,
Miltenyi Biotec, Sanofi, Takeda

Learning Objectives
Differentiate patient selection criteria for younger
versus older HSCT candidates
Apply emerging and evolving data on HSCT in
treatment planning for patients with hematologic
malignancies
Assess strategies to manage transplant-related
complications so that patients may achieve the
optimal HSCT outcomes
HSCT = hematopoietic stem cell transplant.

Indications for HSCT
PCD = primary ciliary dyskinesia; NHL = non-Hodgkin’s lymphoma; AML = acute myeloid
leukemia; HD = hemodialysis; ALL = acute lymphocytic leukemia; MDS = myelodysplastic
syndromes; MPN = myeloproliferative neoplasms; CLL = chronic lymphocytic leukemia; CML =
chronic myelogenous leukemia.
D'Souza & Zhu, 2016.

Annual Number of Auto vs Allo
Transplant Recipients
D'Souza & Zhu, 2016.

There Is a Significant Unmet Need for
HSCT Across All Indications
Besse et al, 2015.

Autologous Hematopoietic
Progenitor Cell Transplant
AHPCT = autologous hematopoietic progenitor cell transplant.
Costa et al, 2015.
# of Newly
Diagnosed Cases # of First AHPCTs
0
5000
10000
15000
20000
25000
18-49 50-64 65+
0
0.1
0.2
0.3
0.4
0.5
0.6
40 45 50 55 60 65 70 75 80 85 90
AHPCT “Utilization Rate”
0
5000
10000
15000
20000
25000
18-49 50-64 65+
Black man
Blackwomen
White man
Whitewomen
men
men

Barriers to HSCT Access
Majhail et al, 2010.
Access to Transplant
Donor Availability
Economic
Socioeconomic status
Education
Number of wage earners
Employment status
Insurance coverage
Place of residence
Transportation
Health Care System
Limited number of HSCT centers
Workforce shortage
Capacity limitations
Infrastructure issues
Provider
Physician referral
Provider attitudes/biases
Provider expertise
Provider diversity
Social
Age
Ethnicity and race
Language
Culture
Health literacy
Patient/family attitudes
Caregiver availability

HSCT Volume by Center
Based on 2010 total HSCT volume (N=84 centers)
Majhail, Mau et al, 2015.

Donor Availability No Longer the
Greatest Barrier to HSCT
Estey et al, 2007
2001-2003
99 AML/MDS patients in CR1
53 received HSCT consulto Donor identified in 49% of
patients
o 14 underwent allo HSCT in CR1
Most common stated reason for
not proceeding to HSCT:
o No donor
CR1 = first complete remission.
Estey et al, 2007; Mawad et al, 2013.
Mawad et al, 2013
2008-2011
116 AML patients in CR1
78 (67%) underwent HSCT
Reasons for not proceeding to
HSCT: o Early relapse (32%)
o Poor performance status
(21%)
o Financial or psychosocial
issues (21%)

Trends in Allogeneic HSCT by Agea
aTransplants for AML, ALL, NHL, Hodgkin lymphoma, and multiple myeloma.
D'Souza & Zhu, 2016.
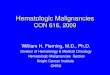
100-Day Mortality by HCT-CI After Auto
HSCT: KPS and Malignancy
KPS = Karnofsky performance score; HCT-CI = Hematopoietic Cell Transplant Comorbidity Index.
Farina et al, 2009.
10
0-D
ay M
ort
alit
y (
%)
P<0.001 P<0.001P<0.001 P<0.001
0
5
10
15
KPS <80 KPS>80 Myeloma Lymphoma
HCT CI 0
HCT CI 1-2
HCT CI >3
KPS <80 KPS >80 Myeloma Lymphoma

2-Year Mortality Rate for
Patients Aged ≥70 Years
8% if fully independent
14% if dependent in IADL
27% if dependent in ADL
40% if institutionalized
IADL = instrumental activities of daily living; ADL = activities of daily living.
Reuben et al, 1992.

Geriatric Assessment Predicts
Survival and Toxicities
HR = hazard ratio; CI = confidence interval; CCI = Charlson Comorbidity Index; ISS = International Staging System; OS
= overall survival; PFS = progression-free survival; AEs = adverse events.
Palumbo et al, 2015.

OS and PFS by Risk Group
Palumbo et al, 2015.

Who Is Transplant Ineligible?
BiologicFrail and poor PS
Active uncontrolled
comorbidities
PsychosocialPoor caregiver support
Patient refusal
PS = performance status.
Majhail, Farnia et al, 2015.
Low-risk disease with
major responseRisk/benefit ratio
Progressive disease
Patients >85 years for
auto
Patients >80 years for
allo
Absolute Relative

HLA Matters and So Does Timing
Patients transplanted earlier in their disease have superior outcomes vs those with
advanced disease, regardless of the degree of match
HLA = human leukocyte antigen.
Lee et al, 2007.
8/8 Match 7/8 Match 6/8 Match
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60
Surv
ival
Early Disease Stage Intermediate Disease Stage Advanced Disease Stage
Su
rviv
al
Su
rviv
al
Months After Transplant Months After Transplant Months After Transplant

Barriers to Referral
Late referral or lack of referralReferring physician’s unfamiliarity with the evolving indications
for HSCT
Financial disincentives
Different perspectives between oncologists and transplant
physicians regarding appropriate transplant candidates
Poor communication and coordination between referring
physician and transplant center
Costa et al, 2015.

HSCT Referral Guidelines
HSCT consultation timing for
15+ diseases
Recommended posttransplant
screening and preventive
practices
Clinical screening and diagnostic
tools for chronic GVHD
Recommended vaccination
schedule
GVHD = graft-versus-host disease.
Available via mobile app, print, and online
BeTheMatchClinical.org/guidelines

Case Study
67-year-old woman with history of NHL 5 years ago,
successfully treated with 6 cycles of CHOP-rituximab
Presents with progressive fatigue and is found to be
pancytopenic
Bone marrow aspiration reveals 28% myeloid blasts
with complex cytogenetic abnormalities
Diagnosed with AML
Has no HLA-compatible donors in the family. Two sons:
ages 30 and 32 years
Achieves a CR after induction therapy with cytarabine
and daunorubicin (“7+3” regimen)
NHL = non-Hodgkin lymphoma; CHOP = cyclophosphamide, doxorubicin, vincristine, prednisone; CR =
complete response.

Go or No Go?

Determinants of the Decision Process
Current
Expectation of cure with standard
chemo
Risk of death from transplant-
related complications
Risk of relapse post-HSCT
Future
Molecular classification that
separates standard risk groups
into subgroups with different risk
ratios
Novel treatment strategies that
may result in improved outcomes
(FLT3 inhibitors)
Improved donor selection
Better supportive care
Improved GVHD prophylaxis
Better conditioning regimens
Post-HSCT maintenance
Majhail, Farnia et al, 2015.

Allo HSCT for High-Risk AML
Stelljes et al, 2011.
Transplant patients
Non-transplant patients

AML Revised Risk Stratification
Patel et al, 2012.
Favorable
Any
Favorable
Normal
karyotype or
intermediate-
risk
cytogenetic
lesions
Intermediate
Unfavorable
Unfavorable
FLT3-ITD-negative
FLT3-ITD-negative
FLT3-ITD-positive
FLT3-ITD-negative
FLT3-ITD-positive
FLT3-ITD-negative
or positive
Mutant NPM1 and IDH1 or IDH2
Wild-type ASXL1, MLL-PTD,
PHF6, and TET2
Mutant CEBPA
Wild-type MLL-PTD, TET2, and
DNMT3A and trisomy 8-negative
Mutant TET2, MLL-PTD, ASXL1,
or PHF6
Mutant TET2, MLL-PTD,
DNMT3A, or trisomy 8, without
mutant CEBPA
Any
Cytogenetic
Classification
Mutations Overall Risk
Profile

AML Revised Risk Stratification:
Integrated Genetic Analysis
Patel et al, 2012.

Prognostic Factors for Allo
HSCT-Related Nonrelapse Mortality
Cornelissen et al, 2012.
Pretransplant Peritransplant Posttransplant
Favorable prognostic factors
Sibling donor Nonmyeloablative conditioning
Shorter time from diagnosis to transplantStem-cell source (bone marrow
or peripheral blood)
White ethnicity
Adverse prognostic factors
Increased age Myeloablative conditioning Acute GVHD - Grade III-IV
Recipient and donor sex Alternative donorsChronic GVHD - Persistent,
extensive
Comorbidities
Cytomegalovirus status
Cytokine polymorphism
Unrelated donor
HLA-mismatched
Performance score
Refractory leukemia
Therapy-related AML

Recommendation for Allogeneic HSCT
for AML in CR1
NRM = nonrelapse mortality; WBC = white blood cell count.
Cornelissen et al, 2012.
Risk Assessment
Risk of Relapse
Prognostic Scores for NRM That
Would Indicate Allogeneic
HSCT as Preferred Consolidation
Chemotherapy or
Auto HSCT (%)
Allo
HSCT (%)
Prognostic
ScoreNRM (%)
Good
t(8;21) with WBC ≤20
inv(16)/t(16;16)
Mutated CEBPA (bi-allelic)
Mutated NPM1 (no FTL3-ITD
mutation)
Early first CR and no MRD
35-40 15-20 1 > 10-15
Intermediate
t(8;21) with WBC >20
Cytogenetically normal (or with
loss of X and Y chromosomes)
WBC ≤100 and early first CR
50-55 20-25 2≥ <20-25
Poor
No CR after first cycle of
chemotherapy
Cytogenetically normal and WBC
>100
Cytogenetically abnormal
70-80 30-40 ≥3-4 <30
Very poor Monosomal karyotype
Abn3q26
Enhanced Evi-1 expression
>90 40-50 ≥5 <40

Outcomes of Allo HSCT in
Elderly Patients With AML
RFS = relapse-free survival; CIR = cumulative incidence of relapse.
Rashidi et al, 2016.

CALGB 100103/BMT CTN 0502:
Outcomes by Donor Type
BMT CTN = The Blood and Marrow Transplant Clinical Trials Network.
Devine et al, 2015.
Nonrelapse Mortality by
Donor Type
Relapse by
Donor Type

HSCT in MDS: The Problem
Getta et al, 2016.

Components of the HSCT
PatientIndication
Comorbidity
Cell sourceAutologous vs allogeneic
Related vs unrelated
Bone marrow vs peripheral blood vs cord blood
Manipulated vs unmanipulated
Conditioning regimenChemical and physical agents to eliminate malignant disorder
and “open space” for donor cells

Components of the HSCT (cont.)
Supportive careProtocols and SOPs required to maintain organ function and
prevent serious fatal complications in severely immune-
compromised patients recovering from the effects of high-dose
therapy○ Hydration and electrolytes
○ Antibiotics
○ Graft-versus-host disease prevention
○ Nutrition
○ Symptom management
Post-HSCT therapies Prevent relapse
Monitor and treat long-term complications
SOPs = standard operating procedures.
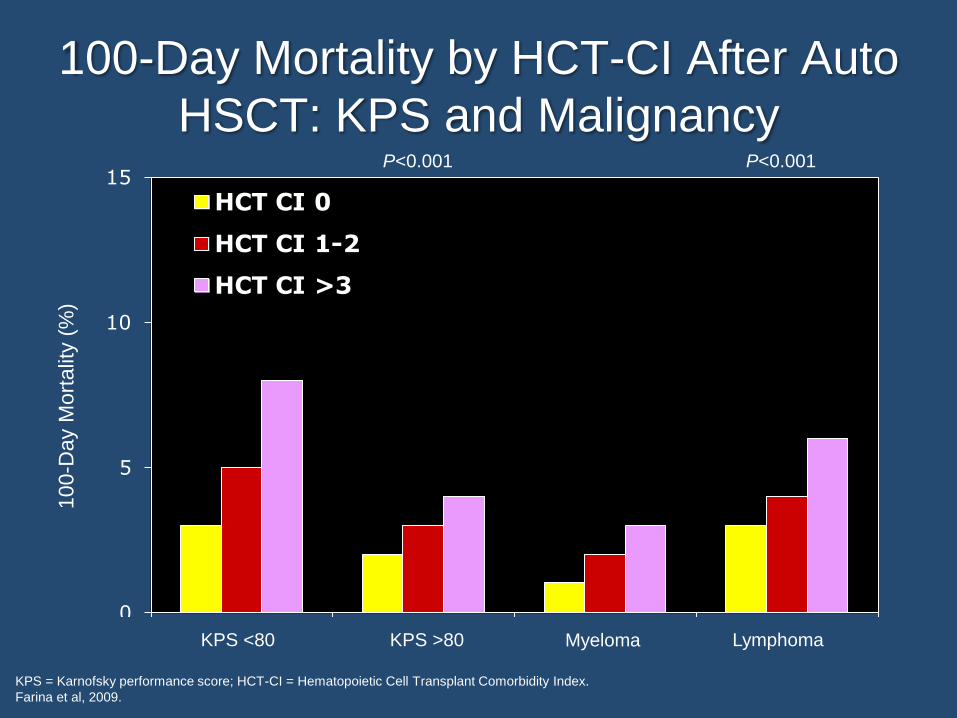
Allo-HSCT Recipients in US
by Donor Type
URD = unrelated donor; BM = bone marrow; PB = peripheral blood; UCB = umbilical cord blood.
D'Souza & Zhu, 2016.

Relative Risks and Benefits of Different
Cell Sources
Majhail, Farnia et al, 2015.
Unrelated Donor Cord Haplo
Engraftment Fast Slow Fast
Graft failure Rare More commonRare with new
techniques
GVHDHigh (esp with
mismatch)
Lower than
expected with
mismatch
Low due to
techniques
RelapsePossibly lower than
sibling
Possibly lower
than siblingHigher
Overall survival Many recent studies show equivalence

Haploidentical vs Unrelated Donor:
Overall Survival
Ciurea et al, 2015.
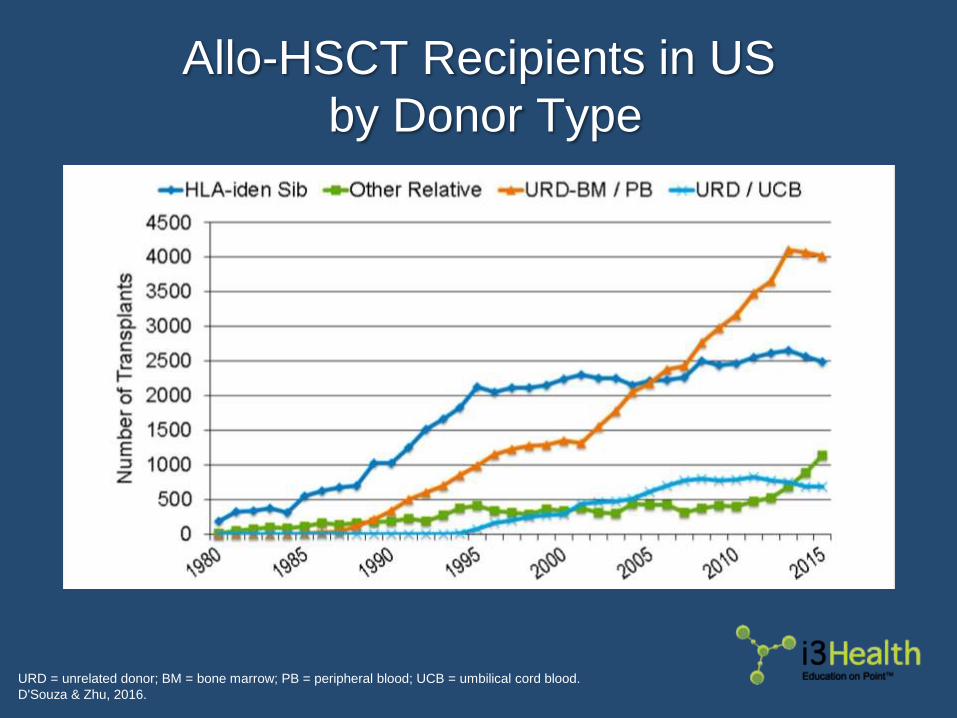
Haploidentical vs Unrelated Donor:
Nonrelapse Mortality
Ciurea et al, 2015.

Minnesota-Fred Hutchinson
Experience: Leukemia-Free Survival
MM URD = mismatched unrelated donor; DUCB = double umbilical cord blood.
Brunstein et al, 2010.
Cu
mu
lative
Pro
po
rtio
n
MRD
P = 0.19
MM URD
MUDDUCB
0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5
II I I II I I I IIIIIIIIIII
II
IIIII
I II II I
I I I I I II I I I I I I I II I I I III II I I I I IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII
III
II IIIIIIIII I
II I II IIIIIIIIIIIIIII IIIII II I I I I I I I I I I I I I IIII I I IIIIII
III
I
IIIIIIIIII II I I II I IIIII II I III III I I
IIII IIII II I I II II I III IIII I II I IIIIIIIIIIIIII
Years Posttransplant

Minnesota-Fred Hutchinson
Experience: Relapse by Donor Type
Brunstein et al, 2010.
Cu
mu
lative
In
cid
en
ce
MRD
P < 0.01
MMUD
MUD
DUCB0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5Years Posttransplant

Donor Selection: Current Status
With the increasing availability of alternative donors,
donor availability should no longer be the most common
barrier to HSCT
In 2017, the algorithm remains the same:1st choice: 10/10 sibling donor
2nd choice: 10/10 unrelated donor
3rd choice: Alternative donor of preference
This algorithm is much more flexible and should
considerNeed for rapid HSCT
Donor age and comorbidities
Donor-specific antibodies
Other HLA disparities

Autologous Stem Cell Sources by
Recipient Age
Pasquini & Wang, 2013.

Disease-Free Survival From Transplant
Anasetti et al, 2012.

Cumulative Incidence of Chronic GVHD
From Time of Transplant
Anasetti et al, 2012.
Treatment Arm
Bone Marrow Peripheral Blood
N (%) N (%)
None 160 (60.6%) 128 (48.9%)
Limited 23 (8.7%) 13 (5.0%)
Extensive 81 (30.7%) 121 (46.2%)
Total 264 (100.0%) 262 (100.0%)

TRM and LFS in Patients With Acute and Chronic
Leukemia After BM and PBSC Transplant
TRM = transplant-related mortality; LFS = leukemia-free survival; PBSC = peripheral blood stem cell.
Schmitz et al, 2006.

Conditioning Regimen Effects
Gyurkocza & Sandmaier, 2014.
Conditioning Regimen Spectrum
High
Intensity
Low
Intensity
Increase immediate antitumor effect
Increase toxicity
Rely on later graft-versus-disease effect
Decreased regimen-related toxicity
Number of
candidates for
HSCT

Common Conditioning Regimens in
AML or MDS Allo HSCT: 2000-2015
MAC = myeloablative conditioning; RIC = reduced-intensity conditioning; TBI = total body irradiation.
D'Souza & Zhu, 2016.

Nonrelapse Mortality in AML:
Myeloablative Conditioning
EBMT = European Group for Blood and Marrow Transplantation.
Cornelissen et al, 2012.
100
80
60
40
20
1 2 3 4 5
No
nre
lap
se
Mo
rtality
(%)
0
Years
EBMT Data
0 (n=598): 5% (4–8%)
1 (n=2,378): 12% (10–13%)
2 (n=3,482): 19% (18–21%)
3 (n=1,900): 27% (24–29%)
4–5 (n=300): 34% (28–40%)EBMT Factors:
Age >50
Disease not in CR1
Donor not 10/10 sib
Time to transplant >1 yr
Female donor/male patient

Nonrelapse Mortality in AML: Reduced-
Intensity Conditioning
Cornelissen et al, 2012.
100
80
60
40
20
1 2 3 4 5
No
nre
lap
se
Mo
rtality
(%)
0
Years
EBMT Risk Score
1 (n=164): 12% (7–19%)
2 (n=1,413): 14% (12–16%)
3 (n=1,410): 24% (21–26%)
4–5 (n=239): 25% (19–32%)

Causes of HSCT Morbidity and Mortality
EBV = Epstein-Barr virus; PTLD = posttransplant lymphoproliferative disorder.
ACS, 2016.
→ Mucositis
→ Infection due to neutropenia
→ Hemorrhagic cystitis
→ Cardiomyopathy
→ Sinusoidal obstruction disease
→ Graft rejection
→ Graft-versus-host disease
→ Opportunistic infection
→ EBV - PTLD
→ Disease recurrence
→ Endocrine: growth, infertility, cataracts, caries
→ Secondary malignancies
Early Late

Risk Factors for Regimen Toxicity
Patient relatedComorbiditiesPrior therapyDisease statePolymorphismsSocioeconomic status
Regimen relatedIntensityAgents used○ Gemtuzumab
ozogamicin○ Inotuzumab○ Radiation○ Busulfan○ Myeloablative
MTX = methotrexate.
Bacigalupo et al, 2009.
Transplant relatedStem cell source○ Auto
○ Allo
○ Cord
○ Matched/mismatched
GVHD prophylaxis○ MTX
○ Posttransplant
cyclophosphamide
○ CD34 selection

Prognostic Tools for HSCT
Several prognostic risk scores predict mortality risk
after HSCTHCT-CI
EBMT risk assessment score for allogeneic HSCT
Pretransplant Assessment of Mortality (PAM) score
CIBMTR 1-year survival calculator
As patient selection, conditioning regimens, and
supportive care strategies evolve, these scores will
need to be revalidated
CIBMTR = Center for International Blood and Marrow Transplant Research.
Sorror et al, 2005; Gratwohl et al, 1998; Parimon et al, 2006.

Impact of Charlson Comorbidities
Sorror et al, 2005.

Nonrelapse Mortality and
Overall Survival by HCT-CI
Sorror et al, 2005.

BMT CTN 0901:
Randomized Phase III Design
Scott et al, 2017.
MDS/AML
BM <5% Blasts
Randomization
RIC Regimens:
Flu/Bu
Flu/Mel
MAC Regimens:
Bu/Flu
Bu/Cy
Cy/TBI
18-Month Overall Survival
GVHD Prophylaxis
T-cell Replete per
Institutional
Guidelines

MAC vs RIC Regimen Choices
Regimen was prespecified by center before randomization
Scott et al, 2017.
Prespecified Regimen Pair Patients n (%)
MAC RIC Total
Flu/Bu4 vs Flu/Bu2 79 (58.5) 78 (56.9) 157 (57.7)
Flu/Bu4 vs Flu/Mel 8 (5.9) 10 (7.3) 18 (6.6)
Bu4/Cy vs Flu/Bu2 20 (14.8) 22 (16.1) 42 (15.4)
Bu4/Cy vs Flu/Mel 20 (14.8) 16 (11.7) 36 (13.2)
Cy/TBI vs Flu/Bu2 7 (5.2) 10 (7.3) 17 (6.3)
Cy/TBI vs Flu/Mel 1 (0.7) 1 (0.7) 2 (0.7)
Total 135 137 272

Overall Survival by Disease Group
Scott et al, 2017.

Relapse-Free Survival by
Treatment Arm
Scott et al, 2017.
P<0.01 (18 mo pointwise)
Difference of MAC and RIC, 20.4%
(95% CI: 8.8%, 31.9%)

Relapse/Progression by
Disease and Treatment Arm
Scott et al, 2017.

Treatment-Related Mortality
Scott et al, 2017.
P = 0.002

Selecting the Conditioning Regimen
No longer does “one size fit all”Patient and disease characteristics should guide choice of
conditioning regimen
For autografts, intensity is important but
melphalan 140 vs 200 mg/m2 preferred for older patients
In myeloid leukemias, dose intensity may be
important but TBI may not be beneficial
PK-directed busulfan should be standard of carePotential role for PK-directed therapy for other agents
PK = pharmacokinetic.
Majhail, Farnia et al, 2015.

Case Study (cont):
Planning the Transplant
Because of patient’s age and disease status she
receives fludarabine/busulfan for 3 days with PK
monitoring
Her donor is a young 30-year-old man who is
matched at 10/10 alleles
You discuss various GVHD prophylactic strategies
and because of a history of recurrent CMV infection
during her induction therapy you opt for the
standard tacrolimus and methotrexate with donor
bone marrow support
CMV = cytomegalovirus.

5 Phases of Transplant
HSV = herpes simplex virus; IP = interstitial pneumonitis; PCP = pneumocystis; QoL = quality of life; VOD = veno-occlusive disease;
VZV = varicella zoster virus.
Bredeson, 2006.

Transplant Complications
TPN = total parenteral nutrition.
Apperley et al, 2012.
Complication Comment
Marrow toxicity
Common complication
Management
o Neutropenia: Growth factor support
o Anemia and thrombocytopenia: Transfusional support
Mucositis
Common complication
Incidence and severity associated with regimen intensity and patient
characteristics
Pain and compromised nutritional intake common
Management: Palifermin, oral care, pain control, TPN
Diffuse alveolar
hemorrhage
Rare complication (incidence <1%) but with high mortality (>80%)
Associated with infection, diffuse alveolar damage
Clinical presentation: Dyspnea, tachypnea, and hypoxia;
hemoptysis rare
Management: High-dose steroids + transfusion support

Transplant Complications (cont.)
TLS = tumor lysis syndrome.
Apperley et al, 2012; Dalle & Giralt, 2016.
Complication Comment
Cardiac toxicity
Preexisting conditions (eg, coronary artery disease, prior regimen-
related toxicity, disease-related amyloidosis)
Cardiomyopathy
Arrhythmias
Hypertension
Acute renal toxicity
Most common causes: acute tubular necrosis, calcineurin inhibitors,
amphotericin B, aminoglycosides, sinusoidal obstruction syndrome
Less common cause: TLS, thrombotic microangiopathy, emolysis due
to ABO incompatibility
Often multifactorial
Sinusoidal
obstruction syndrome
(veno-occlusive
disease)
Risk factors: preexisting liver conditions (eg, hepatitis, cirrhosis) prior
therapy (eg, second transplant), conditioning regimen (eg, busulfan,
high-dose radiation)
Diagnosis based on clinical suspicion, ultrasound (ascites, abnormal
portal vein waveform, reversal of flow in the portal vein, increased
hepatic artery resistance index), and liver biopsy

Defibrotide for SOS:
Survival Up to Day +100
SOS = sinusoidal obstruction syndrome.
Richardson et al, 2016.
Su
rviv
al
(%)
No. at risk:
Defibrotide 102 101 93 86 71 65 55 50 46 42 39
Controls 32 32 27 23 17 12 11 10 9 9 8
Time Since Transplant (d)
Defibrotide (n=102)
Controls (n=32)
P = 0.0499

Graft-Versus-Host Disease
AcuteMaculopapular rash, persistent nausea/vomiting, abdominal cramps with diarrhea, rising bilirubin○ Within <100 days: Classic acute GVHD○ After 100 days: Late acute GVHD
Incidence○ Up to 40% of sibling donor recipients○ Up to 70% of unrelated donor recipients
Prophylaxis○ Cyclosporine/methotrexate
Treatment○ Grade 1: Topical steroid○ Grade ≥2: Corticosteroid○ Steroid-refractory: ATG, monoclonal antibodies, MSC, ECP, ruxolitinib
Supportive care○ Antimicrobial prophylaxis, antibody replacement, manage
hyperglycemia and cytopenia
ATG = antithrombocyte globulin; MSC = mesenchymal stromal cells; ECP = extracorporeal photochemotherapy.
Socié & Ritz, 2014.

Graft-Versus-Host Disease (cont.)
ChronicSkin involvement resembling lichen planus or scleroderma, dry
oral mucosa with ulcerations, sclerosis of GI tract, rising
bilirubin○ With signs of acute GVHD: Overlap syndrome
Occurs in 40-70% of allo HSCT patients
Prophylaxis○ ATG
○ Other preventive agents for acute GVHD have no effect on chronic
GVHD
Treatment○ Corticosteroid
○ Ibrutinib (approved 2017) after corticosteroid failure
GI = gastrointestinal.
Socié & Ritz, 2014; Palmer et al, 2012; Miklos et al, 2017.

Opportunistic Infection
HHV = human herpesvirus.
Tomblyn et al, 2009.
Patients must be carefully
monitored and receive early
intervention for signs or symptoms
of infection
Immunocompetence improves
progressively with increasing time
after transplant in most patients
Many remain
immunocompromised >2 years
posttransplant, especially those
with chronic GVHD

Causes of Death After HLA-Matched
Sibling HSCT: 2013-2014
D'Souza & Zhu, 2016.
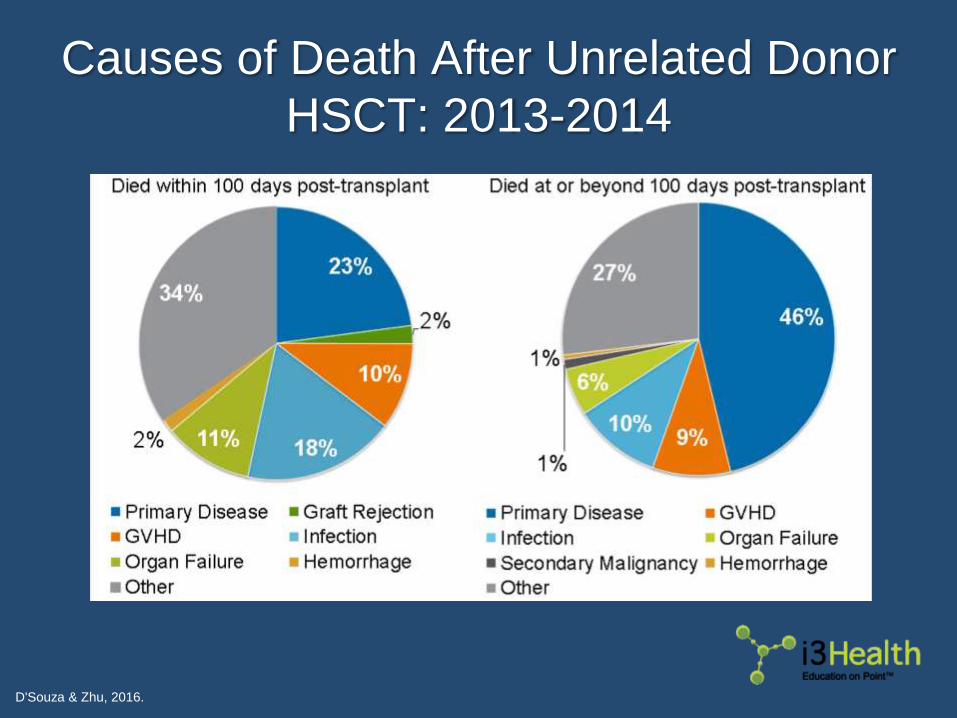
Causes of Death After Unrelated Donor
HSCT: 2013-2014
D'Souza & Zhu, 2016.

Key Takeaways
Donor availability is no longer the most common barrier
to HSCT
Patient and disease characteristics should guide choice
of conditioning regimen
Patients transplanted earlier in their disease have better
outcomes than patients with advanced disease,
regardless of the degree of match
As patient selection, conditioning regimens, and
supportive care strategies evolve, prognostic tools will
need to be revalidated

Questions?

References
American Cancer Society (2016). Stem cell transplant side effects. Available at: https://www.cancer.org
Anasetti C, Logan BR, Lee SJ, et al (2012). Peripheral-blood stem cells versus bone marrow from unrelated donors. N Engl J Med,
367(16):1487-1496. DOI:10.1056/NEJMoa1203517
Apperley J, Carreras E, Gluckman E & Masszi T, Eds. (2012). The 2012 revised edition of the EBMT-ESH Handbook on Haematopoietic Stem
Cell Transplantation. Available at: http://www.ebmt.org
Bacigalupo A, Ballen K, Rizzo D, et al (2009). Defining the intensity of conditioning regimens: working definitions. Biol Blood Marrow Transplant,
15(12):1628-1633. DOI:10.1016/j.bbmt.2009.07.004
Besse KL, Preussler JM, Murphy EA, et al (2015). Estimating demand and unmet need for allogeneic hematopoietic cell transplantation in the
United States using geographic information systems. J Oncol Pract, 11(2):e120-e130. DOI:10.1200/JOP.2014.000794
Bredeson C (2006). Hematopoietic stem cell transplantation conditioning regimens: understanding the cookbook. Presented at the CIBMTR
Clinical Research Professionals/Data Management Conference. February 15, 2006; Honolulu, HI. Available at: https://www.cibmtr.org/
Brunstein CG, Gutman JA, Weisdorf DJ, et al (2010). Allogeneic hematopoietic cell transplantation for hematologic malignancy: relative risks
and benefits of double umbilical cord blood. Blood, 116(22):4693-4699. DOI:10.1182/blood-2010-05-285304
Ciurea S, Zhang MJ, Bacigalupo AA, et al (2015). Haploidentical transplant with posttransplant cyclophosphamide vs matched unrelated donor
transplant for acute myeloid leukemia. Blood, 126(8):1033-1040.
Cornelissen JJ, Gratwohl A, Schlenk RF, et al (2012). The European LeukemiaNet AML Working Party consensus statement on allogeneic
HSCT for patients with AML in remission: an integrated-risk adapted approach. Nat Rev Clin Oncol, 9(10):579-590.
DOI:10.1038/nrclinonc.2012.150
Costa LJ, Kumar S, Stowell SA, et al (2015). Mobilization and transplantation patterns of autologous hematopoietic stem cells in multiple
myeloma and non-Hodgkin lymphoma. Cancer Control, 22(1):87-94.
D'Souza A & Zhu X (2016). Current uses and outcomes of hematopoietic cell transplantation (HCT): CIBMTR summary slides. Available
at: http://www.cibmtr.org
Dalle JH & Giralt SA (2016). Hepatic veno-occlusive disease after hematopoietic stem cell transplantation: risk factors and stratification,
prophylaxis, and treatment. Biol Blood Marrow Transplant, 22(3):400-409. DOI:10.1016/j.bbmt.2015.09.024
References
Devine SM, Owzar K, Blum W, et al (2015). Phase II study of allogeneic transplantation for older patients with acute myeloid leukemia in first
complete remission using a reduced-intensity conditioning regimen: results from cancer and leukemia group B 100103 (alliance for
clinical trials in oncology)/blood and marrow transplant clinical trial network 0502. J Clin Oncol, 33(35):4167-4175.
DOI:10.1200/JCO.2015.62.7273
Estey E, de Lima M, Tibes R, et al (2007). Prospective feasibility analysis of reduced-intensity conditioning (RIC) regimens for hematopoietic
stem cell transplantation (HSCT) in elderly patients with acute myeloid leukemia (AML) and high-risk myelodysplastic syndrome (MDS).
Blood, 109(4):1395-1400. DOI:10.1182/blood-2006-05-021907
Farina L, Bruno B, Patriarca F, et al (2009). The hematopoietic cell transplantation comorbidity index (HCT-CI) predicts clinical outcomes in
lymphoma and myeloma patients after reduced-intensity or non-myeloablative allogeneic stem cell transplantation. Leukemia, 23:1131-
1138.
Getta B, Kishtagari A, Hilden P, et al (2016). Allogeneic hematopoietic stem cell transplantation is underutilized in patients with myelodysplastic
syndromes. Blood, 128(22):3188.
Gyurkocza B & Sandmaier BM (2014). Conditioning regimens for hematopoietic cell transplantation: one size does not fit all. Blood, 124(3):344-
353. DOI:10.1182/blood-2014-02-514778
Gratwohl A, Hermans J, Goldman JM, et al (1998) Risk assessment for patients with chronic myeloid leukaemia before allogeneic blood or
marrow transplantation. Chronic leukemia working party of the European group for blood and marrow transplantation. Lancet,
352(9134):1087-1092.
Lee SJ, Klein J, Haagenson M, et al (2007). High-resolution donor-recipient HLA matching contributes to the success of unrelated donor marrow
transplantation. Blood, 110(13):4576-83.
Majhail NS, Farnia SH, Carpenter PA, et al (2015). Indications for autologous and allogeneic hematopoietic cell transplantation: guidelines from
the American Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant, 21(11):1863-1869.
DOI:10.1016/j.bbmt.2015.07.032
Majhail NS, Mau LW, Payton T & Denzen E (2015). National survey of blood and marrow transplant center personnel, infrastructure and models
of care delivery. Available at: http://www.cibmtr.org.
Majhail NS, Omondi NA, Denzen E, et al (2010). Access to hematopoietic cell transplantation in the United States. Biol Blood Marrow
Transplant, 16(8):1070-1075. DOI:10.1016/j.bbmt.2009.12.529

References
Mawad R, Gooley TA, Sandhu V, et al (2013). Frequency of allogeneic hematopoietic cell transplantation among patients with high- or
intermediate-risk acute myeloid leukemia in first complete remission. J Clin Oncol, 31(31):3883-3888. DOI:10.1200/JCO.2013.50.2567
Miklos D, Cutler CS, Arora M, et al (2017). Ibrutinib for chronic graft-versus-host disease after failure of prior therapy. Blood. [Epub ahead of
print] PII:blood-2017-07-793786 DOI:10.1182/blood-2017-07-793786
Palmer JM, Lee SJ, Chai X, et al (2012). Poor agreement between clinician response ratings and calculated response measures in patients with
chronic graft-versus-host disease. Biol Blood Marrow Transplant, 18(11):1649-1655. DOI:10.1016/j.bbmt.2012.05.005
Palumbo A, Bringhen S, Mateos MV, et al (2015). Geriatric assessment predicts survival and toxicities in elderly myeloma patients: an
International Myeloma Working Group report. Blood, 125(13):2068-2074. DOI:10.1182/blood-2014-12-615187
Parimon T, Au DH, Martin PJ, et al (2006). A risk score for mortality after allogeneic hematopoietic cell transplantation. Ann Intern Med,
144(6):407-414.
Pasquini MC & Wang Z (2013). Current use and outcome of hematopoietic stem cell transplantation: CIBMTR Summary Slides. Available at:
http://www.cibmtr.org
Patel JP, Gönen M, Figueroa ME, et al (2012). Prognostic relevance of integrated genetic profiling in acute myeloid leukemia. N Engl J Med,
366(12):1079-1089. DOI:10.1056/nejmoa1112304
Rashidi A, Ebadi M, Colditz GA & DiPersio JF (2016). Outcomes of allogeneic stem cell transplantation in elderly patients with acute myeloid
leukemia: a systematic review and meta-analysis. Bio Blood Marrow Transplant, 22(4):651-657. DOI:10.1016/j.bbmt.2015.10.019
Reuben DB, Rubenstein LV, Hirsch SH, et al (1992). Value of functional status as a predictor of mortality: results of a prospective study. Am J
Med, 93(6):663-669.
Richardson PG, Riches ML, Kernan NA, et al (2016). Phase 3 trial of defibrotide for the treatment of severe veno-occlusive disease and multi-
organ failure. Blood, 127(13):1656-1665. DOI:10.1182/blood-2015-10-676924
Schmitz N, Eapen M, Horowitz MM, et al (2006). Long-term outcome of patients given transplants of mobilized blood or bone marrow: a report
from the International Bone Marrow Transplant Registry and the European Group for Blood and Marrow Transplantation. Blood,
108(13):4288-4290.
Scott BL, Pasquini MC, Logan B, et al (2017). Myeloablative versus reduced-intensity hematopoietic cell transplantation for acute myeloid
leukemia and myelodysplastic syndromes. J Clin Oncol, 25(11):1154-1161.

References
Socié G & Ritz J (2014). Current issues in chronic graft-versus-host disease. Blood, 124(3):374-384. DOI:10.182/blood-2014-01-514752
Sorror ML, Maris MB, Storb R, et al (2005). Hematopoietic cell transplantation (HCT)-specific comorbidity index: a new tool for risk assessment
before allogeneic HCT. Blood, 106(8):2912-2919.
Stelljes M, Beelen DW, Braess J, et al (2011). Allogeneic transplantation as post-remission therapy for cytogenetically high-risk acute myeloid
leukemia: landmark analysis from a single prospective multicenter trial. Haematologica, 96(7):972-979.
DOI:10.3324/haematol.2011.041004
Tomblyn M, Chiller T, Einsele H, et al (2009). Guidelines for preventing infectious complications among hematopoietic cell transplantation
recipients: a global perspective. Biol Blood Marrow Transplant, 15(10):1143-1238. DOI:10.1016/j.bbmt.2009.06.019