Embed Size (px)
Citation preview

Hematologic Malignancies
Kim Noonan, RN, ANP, AOCN
Hematologic Malignancies • Cancers that affect blood, bone
marrow and lymphatic system.
• Liquid tumors vs solid tumors
• Leukemia
• Lymphoma
• Multiple Myeloma
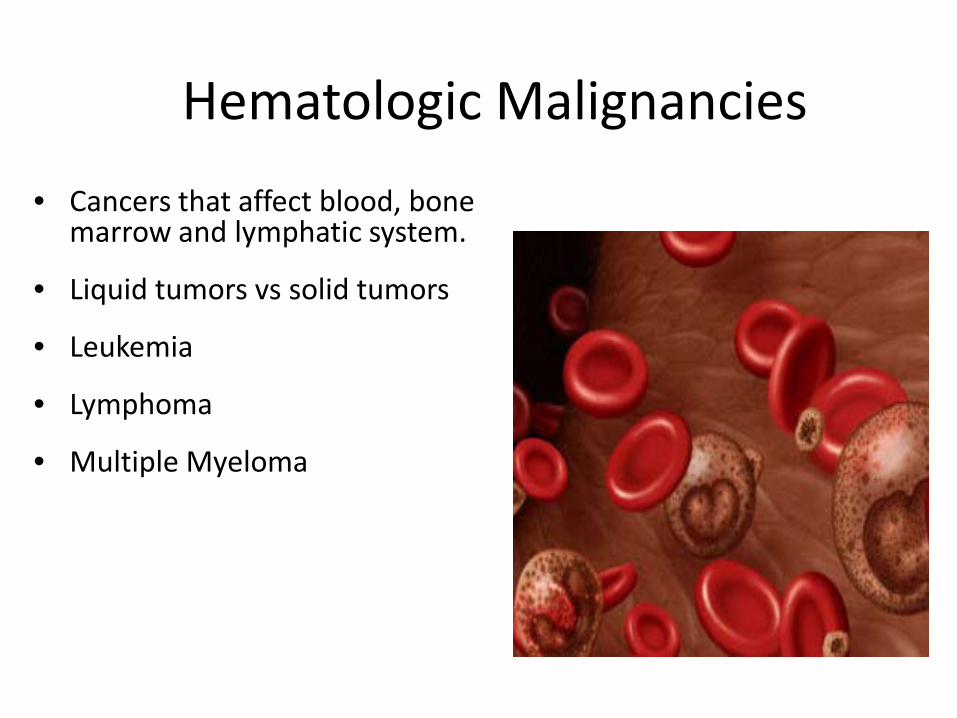
Hematopoietic tree

Leukemia

Leukemia objectives
• Identify risk factors for developing leukemia • Describe the pathophysiology of leukemia • Identify measures and tumor markers used to make a
diagnosis of leukemia • Outline how leukemia is classified • Describe the different types of treatments for leukemia
and identify nursing interventions appropriate to patient care
• Design a plan of care for individuals with leukemia, include planning related to side effects and other concerns regarding treatment

Leukemia epidemiology
• The American Cancer Society's estimates for leukemia in the United States for 2015 are: – About 54,270 new cases of leukemia (all kinds) and
24,450 deaths from leukemia (all kinds) • Leukemia occurs more often in adults than
children • Acute lymphocytic leukemia (ALL) is the most
common form in children • Acute myeloiod leukemia (AML) & Chronic
lymphocytic leukemia (CLL) are the most common forms in adults

Leukemia – risk factors
• Gender - Male > female • Age - Over 50 • Genetic predisposition
– Downs’s Syndrome – Ataxia telangiectasia – Fanconi anemia – Bloom syndrome
• Exposure to radiation
• Family history - CLL • Chemical exposure –
Benzene • Viruses – HIV, HTLV-1 &
EBV • History of cancer
therapy • Myelodysplastic/
myloproliferative disorders
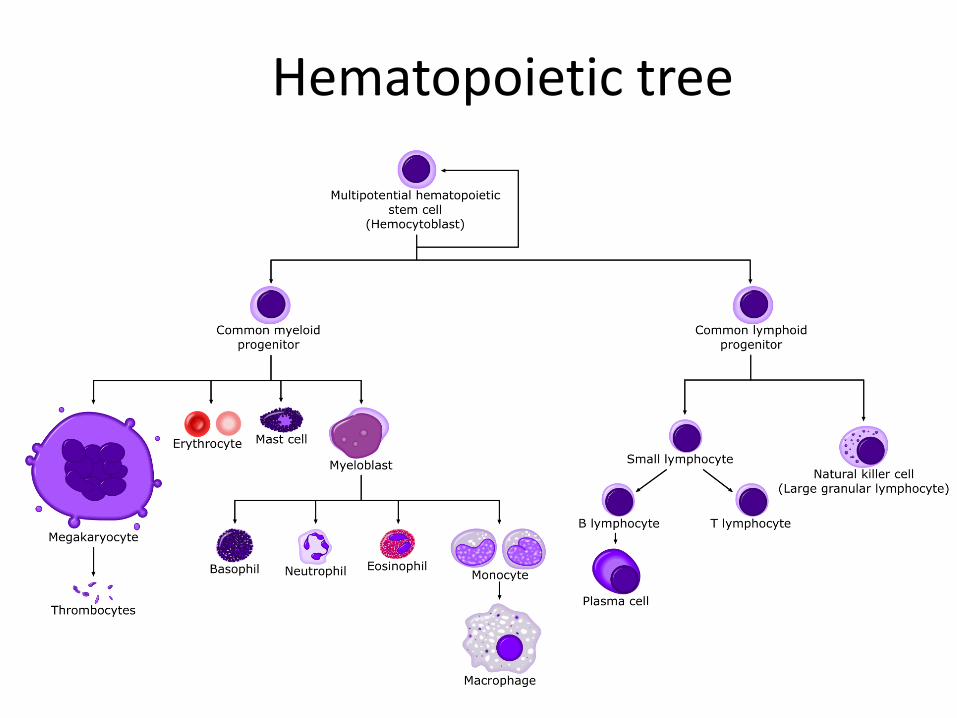
Leukemia pathophysiology
• Malignant disorders of blood forming cells – WBC
• Diffuse replacement of bone marrow
• Starts in bone marrow • Myeloid vs lymphoid • Chronic vs acute

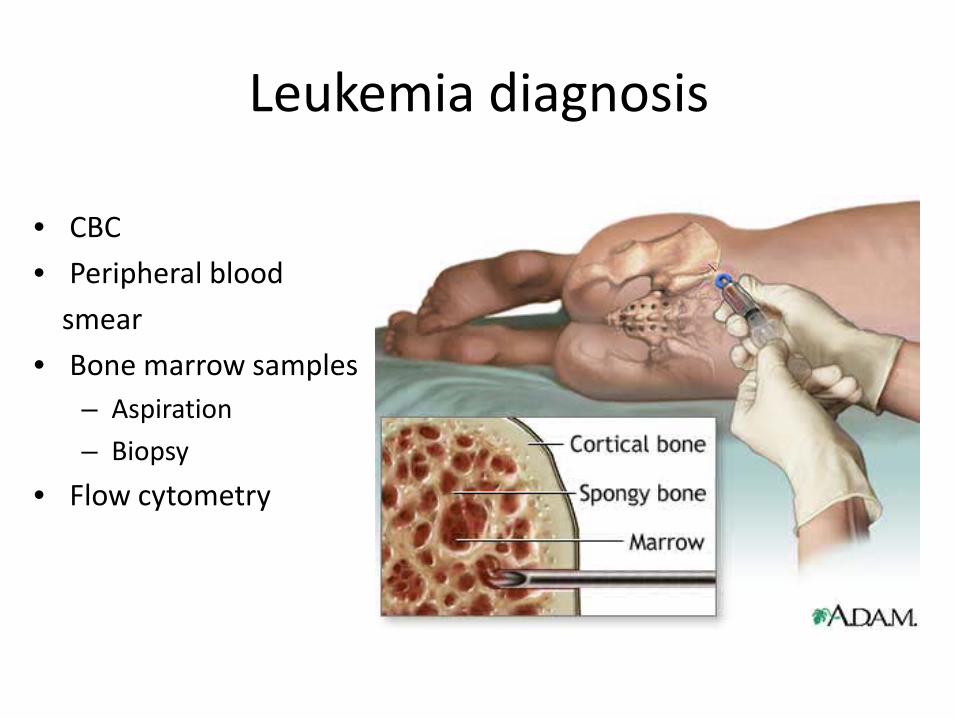
Leukemia diagnosis
• CBC • Peripheral blood smear • Bone marrow samples
– Aspiration – Biopsy
• Flow cytometry
Leukemia - types
• Rate of cell growth - Acute vs chronic • Type of cell - Myeloid vs lymphoid
– Acute myelogenous leukemia - AML – Chronic myelogenous leukemia -CML – Acute lymphocytic leukemia- ALL – Chronic lymphocytic leukemia -CLL – Hairy cell leukemia ( rare chronic leukemia)
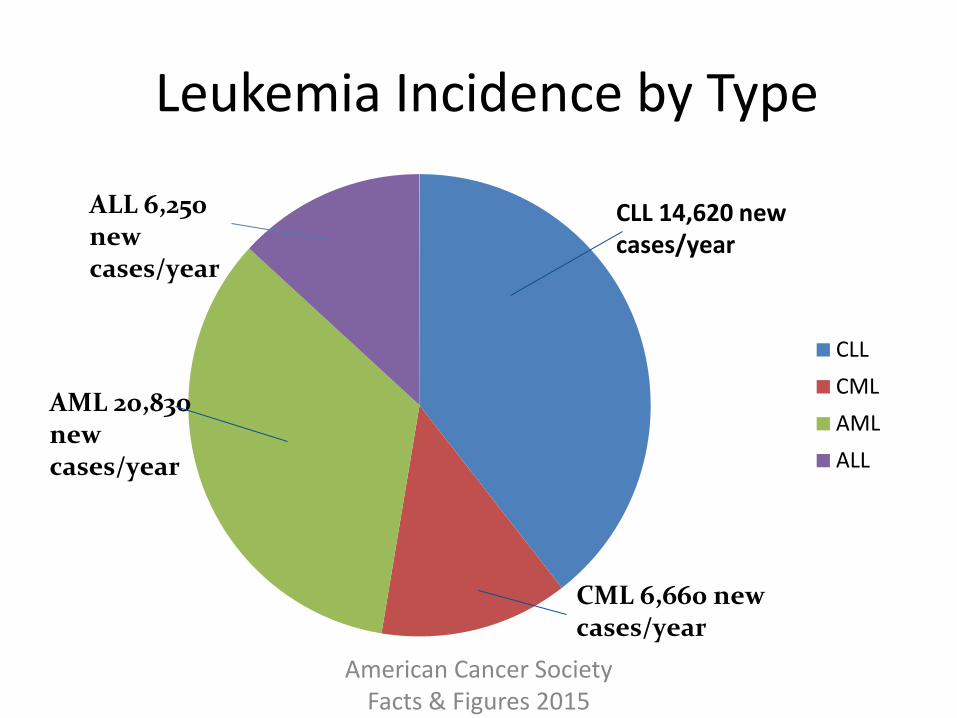
Leukemia Incidence by Type
CLL CML AML ALL
CLL 14,620 new cases/year
ALL 6,250 new cases/year
AML 20,830 new cases/year
CML 6,660 new cases/year
American Cancer Society Facts & Figures 2015
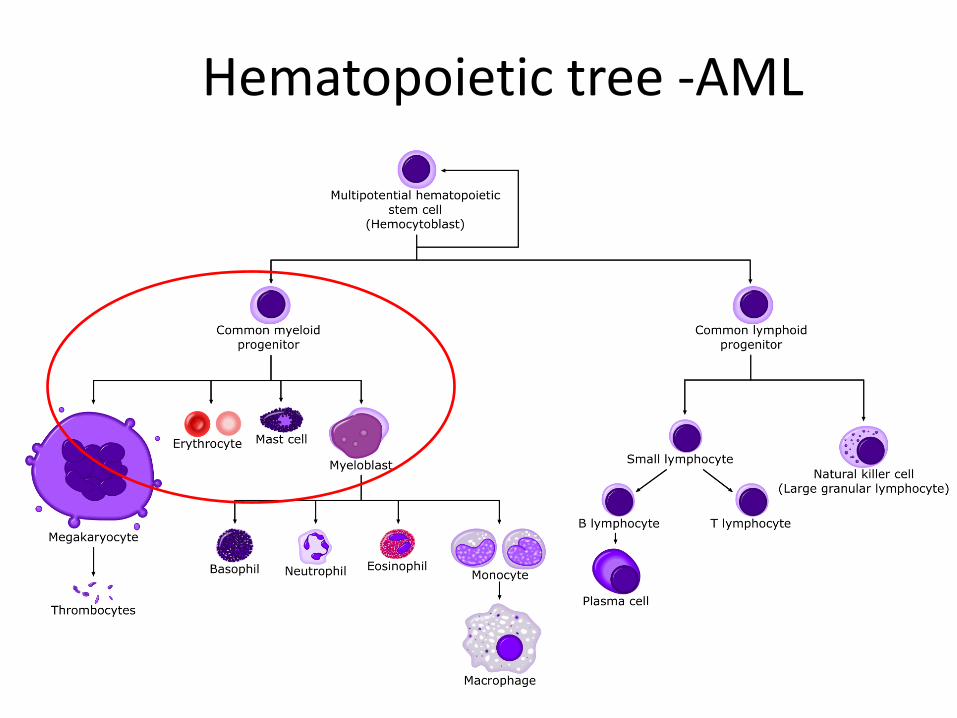
Hematopoietic tree -AML

Acute myelogenous leukemia (AML) • Most common acute leukemia in adults – 80% • In 2014 about 18,860 new cases of acute myeloid leukemia
(AML). Most will be in adults. • In 2014 about 10,460 deaths from AML. Almost all will be in
adults. • Average age = 67 • Men > women • Increased risk of AML associated with:
– Smoking – Chemical exposure – benzene – MDS – Downs syndrome – RX with chemotherapy & radiation
Acute myelogenous leukemia (AML)
• Symptoms – Fatigue – Malaise – Weight loss – Fever/night sweats – Recurrent infections – Unexplained bleeding – Anorexia – Bone pain – Neuro (h/a, vomiting,
visual changes, Sz)
• Signs – Sudden onset – Rapid down hill course – Bone marrow failure – Anemia – Thrombocytopenia – Neutropenia – Hepatomegaly – Organ/gingival
infiltration – Pale skin, skin lesions

Acute myelogenous leukemia (AML) – Clinical Abnormalities
• 95% have circulating myeloblasts in the peripheral smear
• 75% have platelet counts <100,000 • 25% have platelet counts <25,000 • 20% have a WBC of >100,000 • 25-40% have a WBC <5,000 • Auer rods are present in the peripheral smear • Normocytic anemia with a decrease or normal
reticulocyte count
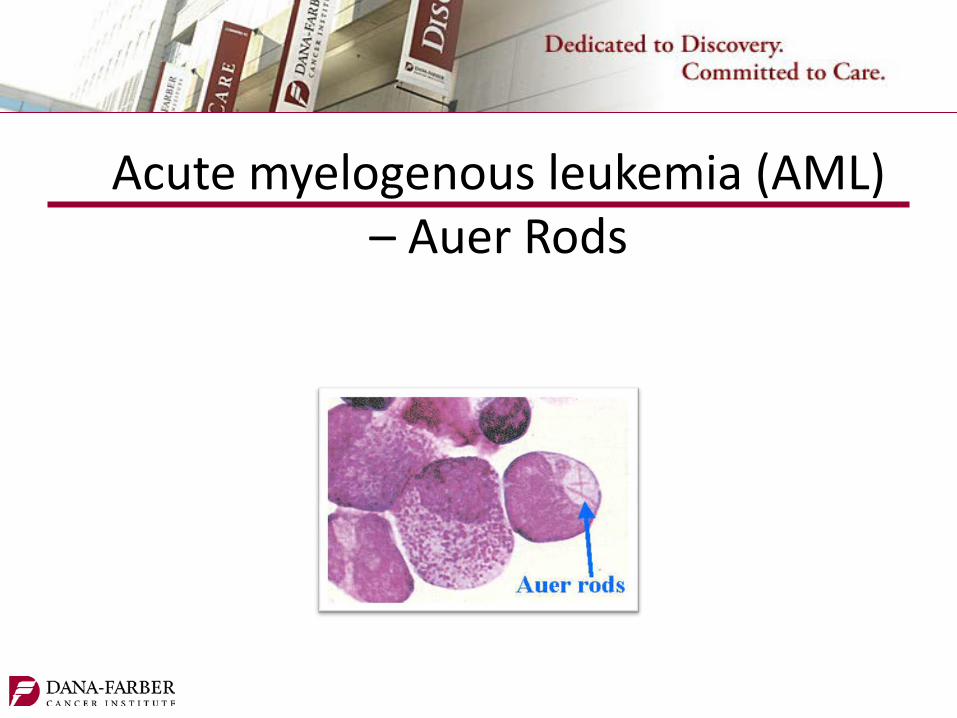
Acute myelogenous leukemia (AML) – Auer Rods

Acute myelogenous leukemia (AML) - Classification FAB – Classification
• M0 – Minimally differentiated • M1 – Undifferentiated
Myelocyte • M2 - Myelocytic • M3 - Promylecytic • M4 - Myelomonocytic • M5 - Monocytic • M6 - Erythroleukemia • M7 - Megakaraycytic
WHO - Classification • Genetic Abnormalities • Prognostic factors • Chromosome abnormalities • Gene mutations • Age • WBC count • Prior blood disorders or
cancers • Infection present • CNS involvement • Response to treatment

Acute myelogenous leukemia (AML) - Treatment
• Induction – initial high dose chemotherapy to achieve complete remission = bone marrow repopulation with normal cells (<5% blasts)
• Post-remission-given to reduce leukemic cell population – Consolidation- 1 or 2 cycles of same chemo used in
induction – Intensification – High dose chemo given shortly after
induction ( same or different drugs) – Maintenance- lower doses of same drugs as induction
given monthly for prolonged period to maintain disease free state
Acute myelogenous leukemia (AML) Treatment
• Induction high dose chemotherapy
– 7 +3 Cytarabine (Ara-c) + anthracycline (Daunorubicin) – Other Anthrcyclines – Decreased doses in patients older than 60 – Intrathecal cytarabine or methotrexate , with or without cranial
radiation, if CNS leukemia present – M4 • Consolidation
– Ara-C 3-4 cycles – Dose is age dependent
• Stem Cell Transplant – Allogeneic in 1st remission when cytogenetic suggest poor prognosis – In relapsed patients
Acute promyelogenous leukemia M3 - Treatment
• Induction – All trans retinoic acid (ATRA) + cytarabine and
daunarubicin – Arsenic trioxide (ATO)+ ATRA
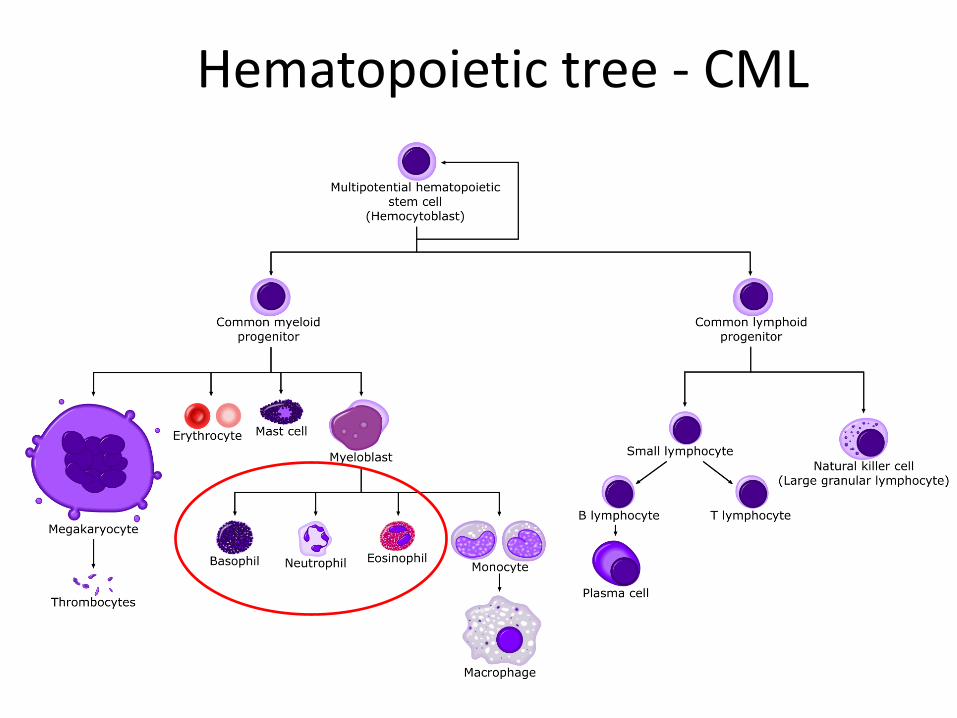
Hematopoietic tree - CML
Chronic myelogenous leukemia • CML - 10% of all new cases of leukemia. • In 2015 about 6,660 new cases of CML will be
diagnosed. • In 2015 about 1,140 people will die of CML. • Men > women • Whites > African-Americans • The average age - 65 years ( rare in children) • Philadelphia chromosome – Chromosomes 9 & 22 • Increased risk of CML associated with:
– High dose radiation – Older age & male gender
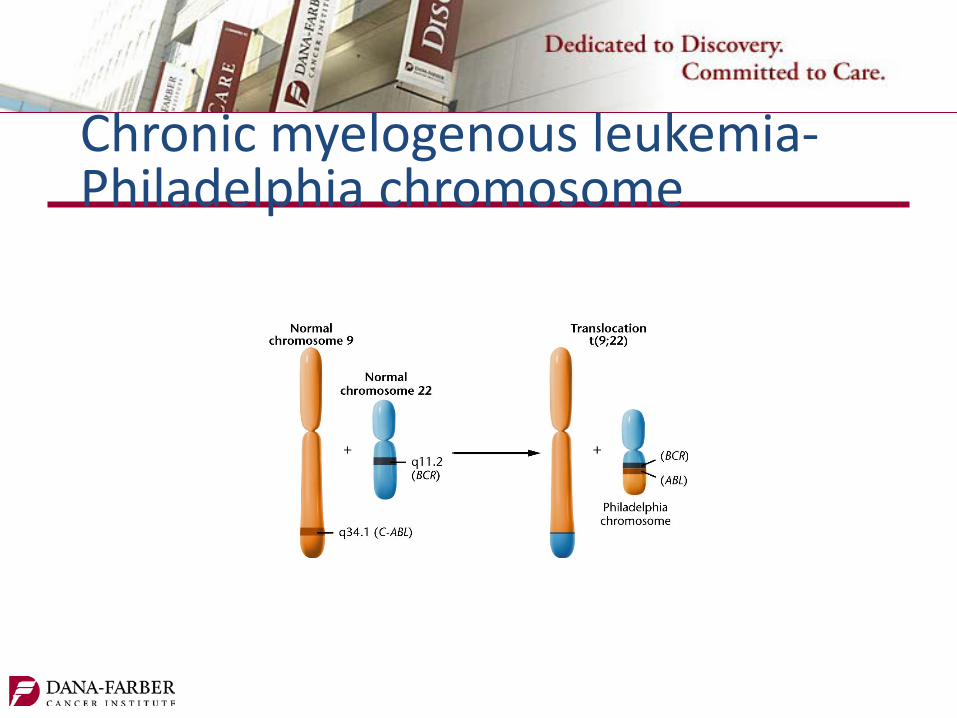
Chronic myelogenous leukemia- Philadelphia chromosome
Chronic myelogenous leukemia
• Insidious Onset • Fatigue / Weakness • Pale skin • Night sweats • Weight loss • Fever • Bone pain • Spleenomegaly • Abdominal pain or a sense of "fullness” • Feeling full after eating even a small amount of food

Chronic myelogenous leukemia - phases • Chronic phase
– Excessive mature granulocytes ( < 10% blasts) – Mild symptoms (if any) – Philadelphia chromosome in 90% – Oral therapies
• Accelerated phase – Increase in immature blast cells - > 10% but < 20% blasts – Increase in basophil count- 20% of the WBCs – High WBC that do not respond treatment – Very high or very low platelet counts – New chromosome changes in the leukemia cells – SX: fever, poor appetite, and weight loss – Does not respond as well to treatment
• Blast phase (also called acute phase or blast crisis) – Bone marrow and/or blood samples > 20% blasts – tissues and organs infiltration – Resembles AML

Prognostic factors for chronic myeloid leukemia
• Adverse prognostic factors: – Accelerated phase or blast phase – Enlarged spleen – Areas of bone damage from growth of leukemia – Increased number of basophils and eosinophils – Very high or very low platelet counts – Age 60 years or older – Multiple chromosome changes in the CML cells

Chronic myelogenous leukemia - treatment
• Targeted therapies – Imatinib (Gleevec) – Dasatinib (Sprycel) – Nilotinib (Tasigna)
• Interferon alpha
• Chemotherapy – Hydroxyurea (Hydrea®) – Cytarabine (Ara-C) – Busulfan – Cyclophosphamide
(Cytoxan®) – Vincristine (Oncovin®)
• Splenectomy
• Radiation therapy – lytic bone lesions
• Bone marrow or peripheral blood stem cell transplant – Allogeneic stem cell
transplants- only cure
• Blast phase treated like acute leukemia

Hematopoietic tree - ALL
Acute lymphocytic leukemia • In 2015, about 6,250 new cases of ALL • In 2015, about 1,450 deaths from ALL • ALL represents the most common pediatric
malignancy • 60% of cases in patients < 20 years old • Cure rate more favorable in children than adults • Males > females • Whites > African-Americans

Acute lymphocytic leukemia – risk factors
• Radiation exposure • Chemical exposure –
benzene/ chemotherapy
• Male > female • White > black • Viral infections
– HTLV-1 – EBV
• Genetic – Down syndrome – Klinefelter syndrome – Fanconi anemia – Bloom syndrome – Ataxia-telangiectasia – Neurofibromatosis
Acute lymphocytic leukemia • Symptoms
– Fatigue – Malaise – Weight loss – Fever/night sweats – Recurrent infections – Unexplained bleeding – Anorexia – Bone pain – Neuro (h/a, vomiting,
visual changes, Seizures)
• Signs – Sudden onset – Rapid down hill course – Bone marrow failure – Anemia – Thrombocytopenia – Neutropenia – Hepatomegaly – Organ infiltration – Pale skin – Enlarged thymus- SVC – Lymphadenopathy – Splenomegaly
Acute lymphocytic leukemia – clinical presentation
• Increase in WBC consisting of lymphoblasts • Granulocytopenia • Decrease in hemoglobin • Decrease in platelets • Increase in LDH
Acute lymphocytic leukemia -classification • Morphology - FAB
– L1: childhood lymphoblasts (pre B and T cell) (85-89%) – L2: adult lymphoblasts (pre B and T cell) (11-14%) – L3: Burkitts’s type (B-cell)<1% poor prognosis
• B Cell ALL – Most common – About 85% are precursor B cell ALL – Markers: CD19, CD22, CD20 and CD79; CD10 and CD45
• T Cell ALL – Uncommon – Lymphadenopathy is common – Markers: CD3, CD2,CD5,CD1a, CD4 and/or CD8

Acute lymphocytic leukemia –prognostic indicators
• Age at diagnosis > 35 years • Initial WBC count • ALL subtype • CNS disease at diagnosis • Chromosomal abnormalities
– Translocation 11 q 23 – Philadelphia chromosome
• Response to chemotherapy

ALL – Induction treatment • Induction – 8 weeks
– Goal – cure – Combination Chemotherapy – 4 drug regimen
• Steriod • VinCRIStine (Oncovin®) • Anthracycline • +/- L-asparaginase (Elspar®) • And/or Cytoxan • Imatininb (Gleevec) with + Phildelphia chromosome
– Supportive care – 5% induction mortality • Symptom Management • Routine transfusions • Empiric broad spectrum antibiotics

ALL – Consolidation treatment • Post-remission/ Consolidation
– Must be in remission • Blast <5% • No S & S of ALL • No S & S of organ involvement • No S & S of CNS involvement
– Children intensification regimens • Methotrexate • L-asparaginase
– Adults • High dose chemotherapy • Allogenic stem cell transplant
ALL- CNS Prophylaxis
• Adults – Intrathecal methotrexate – High-dose IV methotrexate or cytarabine – Radiation therapy to the brain and spinal cord
• Children – Intrathecal Methotrexate – High dose chemotherapy
ALL – Bone marrow/ stem cell Transplantation
• Autologous stem cell transplant – Patient’s own stem cells – Will not reject – Cancer may continue to grow
• Allogeneic stem cell transplant – HLA matched donor 6/6 match
preferred • Synergistic – identical twin • Myeloablative HSCT
• Non-myeloablative – “mini” HSCT – Lower doses of chemo with
whole body RT – Allogenic HSCT – Graft vs tumor – Age >60 – Comorbidities
• Stem cell sources – Bone marrow – Peripheral stem cells – Umbilical cord blood – Placenta

ALL- Maintenance
• 2-3 years • Metheltrexate • 6-mercaptopurine (6-MP)
• May include steroid and Vincristine • Imatinib (Gleevec) + Philadelphia chromosome • Adults - CNS prophylaxis
ALL- Response Rates
• Children – The 5-year survival rate for children with ALL –
85%
• Adults – 80-90% achieve complete remission – 50% or more relaspe – 30-40% of adults treated with the conventional
ALL protocol will survive
Chronic lymphocytic leukemia • Characterized by accumulation of small mature
lymphocytes • Slow growing • Predominately in B cells • CLL accounts for about one-third of all leukemias. • In 2015 about 14,620 new cases of chronic lymphocytic
leukemia (CLL) • In 2015 about 4,650 deaths from CLL • Men > women • Family history • Average age - 72 years
Chronic lymphocytic leukemia Symptoms • Asymptomatic in early
stages • Weakness • Fatigue • Weight loss • Fever • Night sweats • Enlarged lymph nodes • Abdominal pain • Early satiety • Recurrent infections
Signs • Insidious onset • Splenomegaly • Hepatomegaly • Lymphadenopathy • Anemia • Thrombocytopenia • Hypogammaglobulinemia • Rashes

Chronic lymphocytic leukemia – staging- Rai system
• Rai system: This is used more often in the United States – The Rai system divides CLL into 5 stages:
• 0 - lymphocyte count > 10,000 • 1 - Lymphocytosis plus enlarged lymph nodes • 2 - Lymphocytosis plus an enlarged spleen (and possibly an
enlarged liver), +/- enlarged lymph nodes • 3 - Lymphocytosis plus anemia , + /- enlarged lymph nodes,
spleen, or liver • 4 - Lymphocytosis plus thrombocytopenia, +/- anemia,
enlarged lymph nodes, spleen, or liver
Chronic lymphocytic leukemia – staging- Binet system
• Binet system: This is used more widely in Europe – Stage A: Fewer than 3 areas of lymphoid tissue are
enlarged, with no anemia or thrombocytopenia. – Stage B: 3 or more areas of lymphoid tissue are
enlarged, with no anemia or thrombocytopenia. – Stage C: Anemia and/or thrombocytopenia are
present.
Chronic lymphocytic leukemia – Adverse prognostic factors
• Diffuse pattern of bone marrow involvement • Advanced age • Male gender • Increased proportion of large or atypical lymphocytes in the blood • Lymphocyte doubling time of less than 12 months • Deletions of parts of chromosomes 17 or 11 • High blood levels of certain substances, such as beta-2-microglobulin • CLL cells containing ZAP-70 (more than 20%) or CD38 (more than • 30%) • CLL cells with unchanged (not mutated) gene for the immunoglobulin
heavy chain variable region (IgVH)
Chronic lymphocytic leukemia - treatment
• Watchful waiting until symptomatic – Physical exam and blood counts every 3-6 months
• Goal – Control symptoms, reduce infections, QOL • Chemotherapy
– Purine analogs – fludarabine – Alkylating agents chlorambucil (Leukeran) and
cyclophosphamide (Cytoxan), bendamustine (Treanda) – Corticosteroids – Monoclonal antibodies – Rituximab, Alemtuzumab (Campath)
• Spleenectomy • Radiation therapy – painful lymphadenopathy
/spleenomegaly
Chronic lymphocytic leukemia – complications/nursing considerations
• Tumor lysis syndrome • Transformation to high grade non- Hodgkin's
Lymphoma • Hemolytic anemia and thrombocytopenia • Recurrent Infection
– Prophylactic support – Annual attenuated vaccinations
• Emotional impact of chronic disease

Nursing Considerations • Acute leukemia are very ill at diagnosis and hospitalized for
several weeks • Profound bone marrow suppression • Infection
– Sepsis – DIC
• Transfusional support • Side effect management • Tumor lysis syndrome • Psychological support • Oral adherence • Educational support

Lymphoma
Scientific Basis for Practice

Lymphoma - objectives
Identify risk factors for developing lymphoma Describe the pathophysiology of lymphoma Identify measures and tumor markers used to make a
diagnosis of lymphoma Outline how lymphoma is classified Describe the different types of treatments for lymphoma and
identify nursing interventions appropriate to patient care Design a plan of care for individuals with lymphoma, include
planning related to side effects and other concerns regarding treatment

Lymphoma
• Most common hematologic malignancy • Account for 5% of all cancers in U.S. • Two categories:
– Hodgkin’s lymphomas (Hodgkin’s Disease) – Non-Hodgkin’s lymphomas
All Other Cancers
Lymphomas
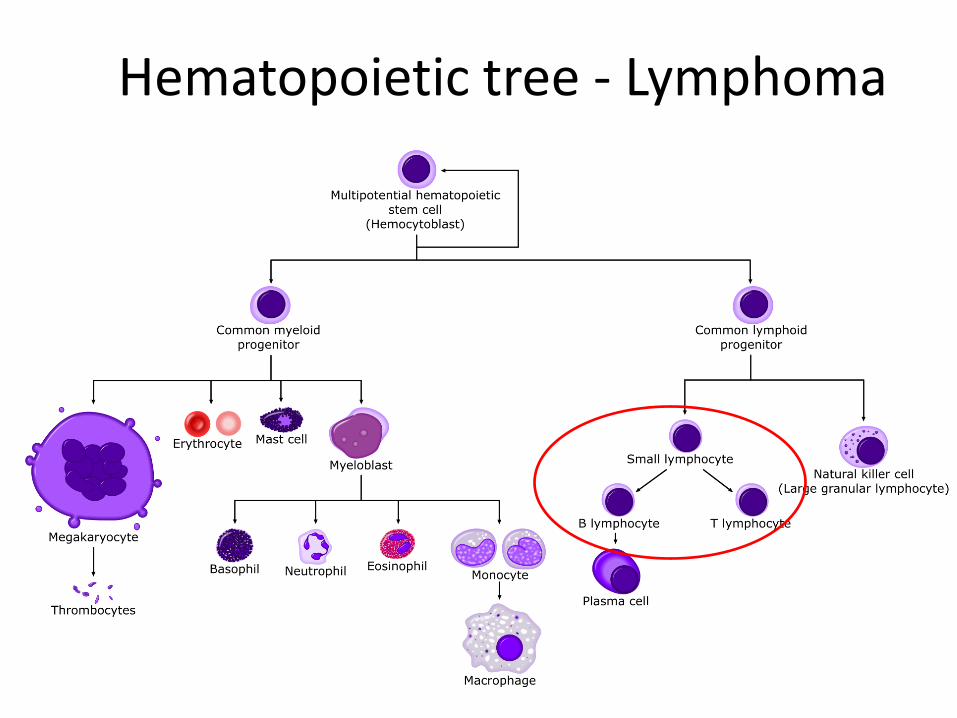
Hematopoietic tree - Lymphoma

Lymphoma
• Neoplasm of Lymphoid tissue – Lymph nodes, spleen,
thymus, adenoids, tonsils, GI tract, bone marrow
• Lymphocytes – B – cell -antibodies – T- cell- cellular
immunity • Non-Hodgkin’s
lymphoma • Hodgkin’s lymphoma
Hodgkin Lymphoma- (Hodgkin’s disease)
• Starts in lymphoid tissue, usually B cells • Spreads through lymph system in step wise orderly fashion • Reed Sternberg cell • In 2015, about 9,050 new cases will occur (3,950 in females
and 5,100 in males) • In 2015 about 1,150 people (490 females, 660 males) will
die of Hodgkin's Lymphoma • Bimodal age distribution – ages 15-34 and age >60 • 1-year relative survival rate – 92% • 5-year and 10-year survival rates are about 85% and 80%,
respectively
Hodgkin Lymphoma- risk factors • Viral
– Epstein-Barr virus infection/mononucleosis – HIV
• Age – bimodal incidence early adulthood (15-34) & late adulthood (>60)
• Gender - males > females • Geography • Family history • Socio-economic status

Hodgkin Lymphoma- signs & symptoms
• Painless enlargement of one or more lymph nodes
• B symptoms – Fever – Night sweats – Anorexia/weight loss
• Itching • Fatigue • Loss of appetite • Cough, SOB, chest pain
Hodgkin Lymphoma- diagnostics
• Biopsy – Excisional or incisional biopsy – Fine needle aspiration (FNA) or core needle biopsy
• Pathology – Reed-Sternberg cell
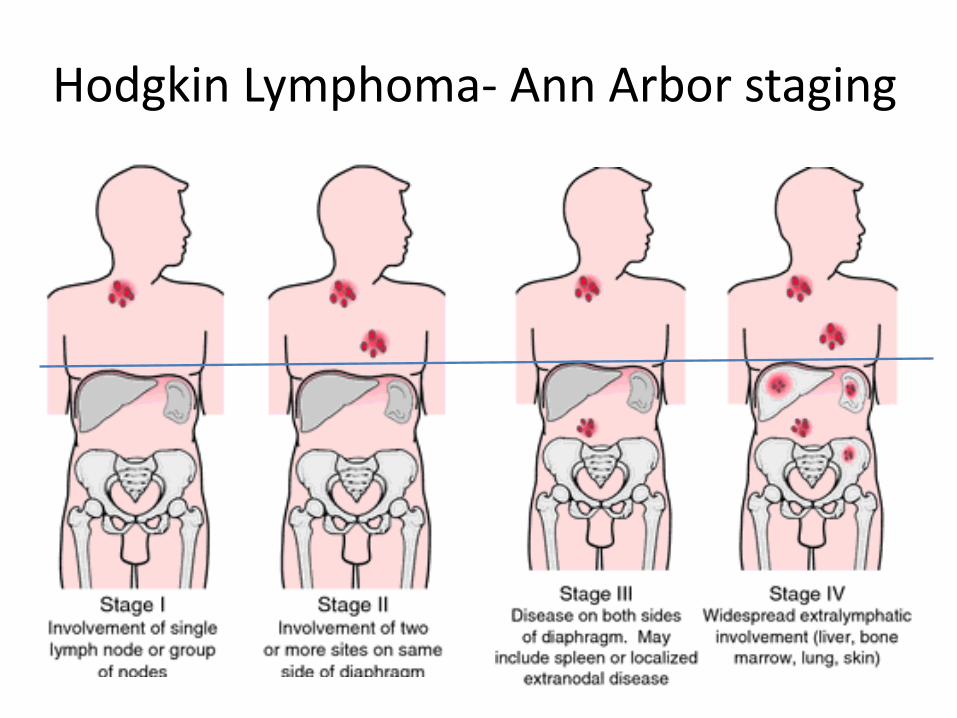
Hodgkin Lymphoma- Ann Arbor staging
Hodgkin’s Lymphoma– Adverse prognostic factors
• B symptoms or bulky disease • Age > 45 • Being male • WBC > 15,000 • Hemoglobin level < 10.5 • Lymphocyte count < 600 • Albumin level < 4
Hodgkin Lymphoma- treatment
• Goal – cure • Chemotherapy
– Adriamycin (doxorubicin) – Bleomycin – Vinblastine – Dacarbazine (DTIC)
• Radiation therapy – Involved field radiation – Extended field radiation
• Long tern side effects – Heart Disease – Stroke – Second malignancies – Hypothyroidism – Fertility issues
• Infections
Non-Hodgkin’s Lymphoma
• Most common hematologic cancer • In 2015, about 71,850 people (39,850 males
and 32,000 females) will be diagnosed with NHL.
• In 2015, about 19,790 people will die from this cancer (11,480 males and 8,310 females).
• Average risk 1 in 50 • 95% of case occur in adults

Non-Hodgkin’s Lymphoma • > 40 different types of NHL
• Malignancies of the B & T lymphocytes – B-cell lymphomas - 85% – T-cell lymphomas – 15%
• Indolent (slow growing) vs aggressive (fast –growing)
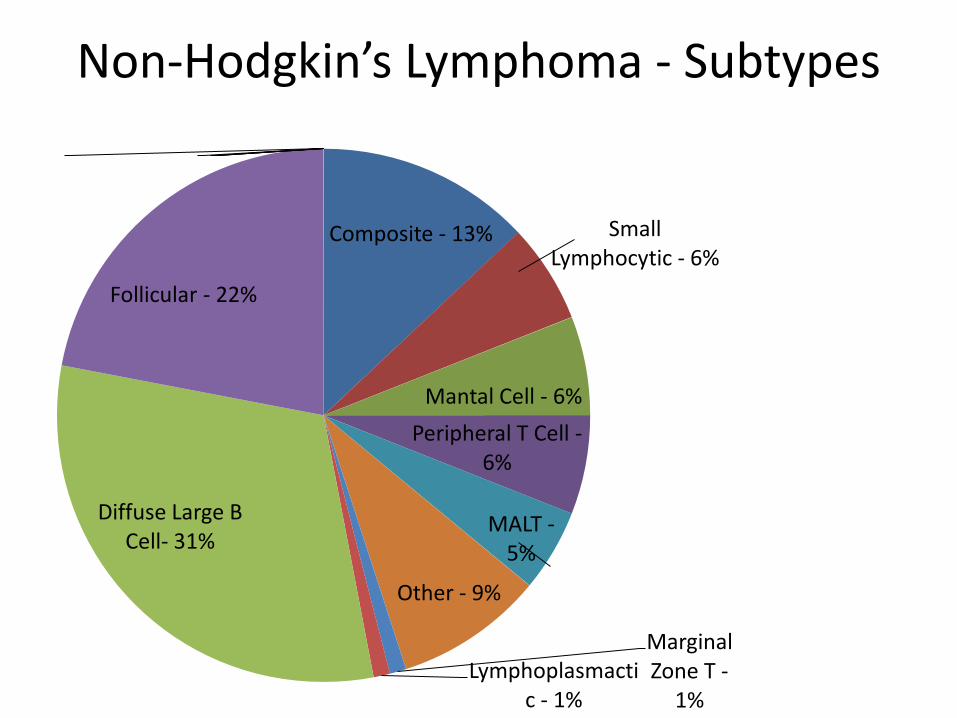
Non-Hodgkin’s Lymphoma - Subtypes
Composite - 13% Small Lymphocytic - 6%
Mantal Cell - 6% Peripheral T Cell -
6%
MALT - 5%
Other - 9%
Marginal Zone T -
1% Lymphoplasmacti
c - 1%
Diffuse Large B Cell- 31%
Follicular - 22%

Non-Hodgkin’s Lymphoma – risk factors
• Age • Gender • Race, ethnicity, and geography • Exposure to certain chemicals • Radiation exposure • Immune system deficiency • Autoimmune diseases • Certain infections
Non-Hodgkin’s Lymphoma – sign & symptoms
• Enlarged lymph nodes • Swollen abdomen • Nausea/vomiting/ abdominal pain • Feeling full after only a small amount of food • Chest pain or pressure • Shortness of breath or cough • Headache/neuro changes • B Symptoms:
– Fever – Weight loss – Night sweats
• Sx of Low blood counts
NonHodgkin Lymphoma- diagnostics • Biopsy
– Excisional or incisional biopsy – Fine needle aspiration (FNA) or core needle biopsy
• Pathology • Lab Tests
– Flow cytometry – Cytogenetic (chromosomal) analysis – Molecular studies
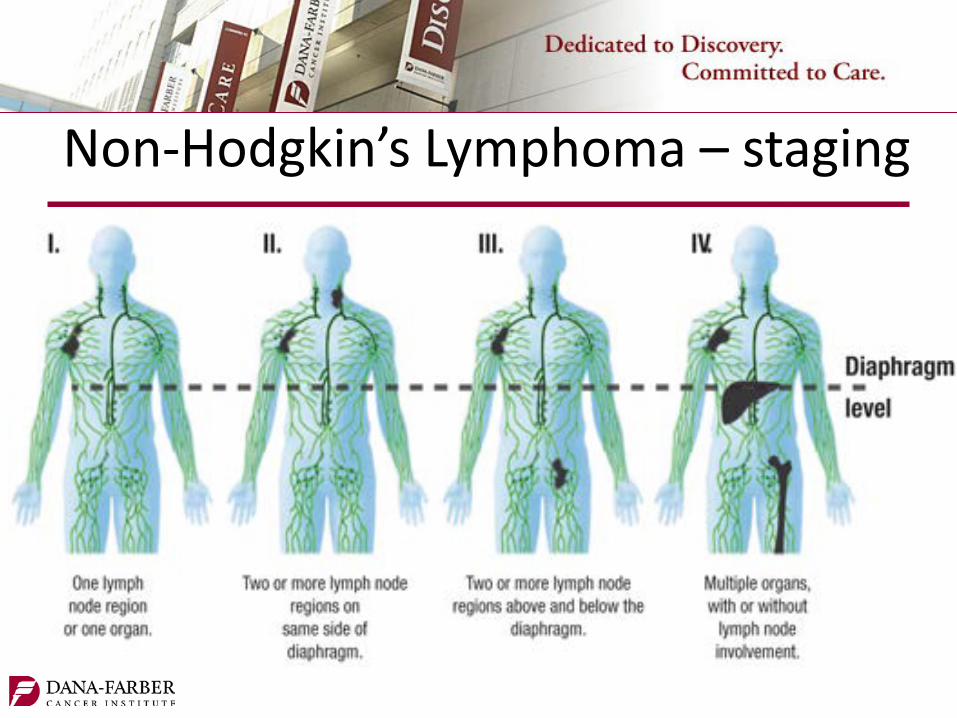
Non-Hodgkin’s Lymphoma – staging

Non-Hodgkin’s Lymphoma – International Prognostic Index
• IPI – Age > 60 – Stage III or IV – Number of extranodal sites >1 – Elevated LDH – ECOG Performance status > 2
• FLIPI – Follicular Lymphoma – Age > 60 – Stage III or IV – Elevated LDH – Hemoglubin < 12 g/dl – Number of extranodal sites >4

Non-Hodgkin’s Lymphoma- classification and grade
• REAL/WHO classification – Cell type
• B cell • T cell • Natural Killer cell
– Morphology – form & structure – Immunophenotype – type of protein expressed – Genetic
• Grade – Indolent - Survival of untreated disease = years
– Intermediate -Survival of untreated disease = months
– Aggressive - Survival of untreated disease = weeks
Non-Hodgkin’s Lymphoma – Indolent • Indolent low grade lymphoma – chronic disease
– Follicular – SLL/CLL – Marginal zone – Lymphoplasmacytic Lymphoma/Waldenstrom’s macroglobulinemia – Hairy Cell Leukemia
• Watchful waiting – Rapidly progressive disease – Organ impairment – Disease related symptoms
• Chemotherapy + Rituximab – R-CHOP – R-CVP – R-FC – Bendamustin (Treanda) + Rituximab
• Single agent Rituximab
Non-Hodgkin’s Lymphoma – Relapsed
• Retreatment with initial chemotherapy • New regimen • Stem cell transplantation • Clinical trials
– Benefit of maintenance Rituximab – Potential of cure with allogenic stem cell
transplant
Non-Hodgkin’s Lymphoma – Aggressive
• Aggressive high grade lymphomas – Diffuse Large B- Cell – Burkitt’s – highly aggressive, RX similar to ALL – Primary CNS – Mantle cell lymphoma – Peripheral T-cell lymphoma – Lymphoblastic lymphoma
• Immediate Treatment – R CHOP – ? Cycle length 21 days vs 14 days – Radiation therapy
• Respond well – can be curable • Relapsed disease
– High dose chemotherapy – Stem cell transplant
Lymphoma – Nursing Considerations
• Infusion reactions – Rituximab • Tumor lyses syndrome • Lung damage – Bleomycin
– Baseline pulmonary function tests
• Cardiac changes – Adriamycin – MUGA or ECHO
• Nausea/ vomiting • Diarrhea/constipation • Alopecia (hair loss) • Fatigue
• Bone marrow suppression – Infection prevention
• Bactrim/Acyclovir/Diflucan – Transfusions – Neulasta
• Mucositis • Peripheral Neuropathy • Sexual health & fertility • Cognitive dysfunction – “Chemo
brain” • Lymphodema

Multiple Myeloma
Scientific Basis for Practice
Multiple Myeloma - objectives • Identify risk factors for developing multiple myeloma • Describe the pathophysiology of multiple myeloma • Identify measures and tumor markers used to make a
diagnosis of multiple myeloma • Outline how multiple myeloma is classified • Describe the different types of treatments for multiple
myeloma and identify nursing interventions appropriate to patient care
• Design a plan of care for individuals with multiple myeloma, include planning related to side effects and other concerns regarding treatment
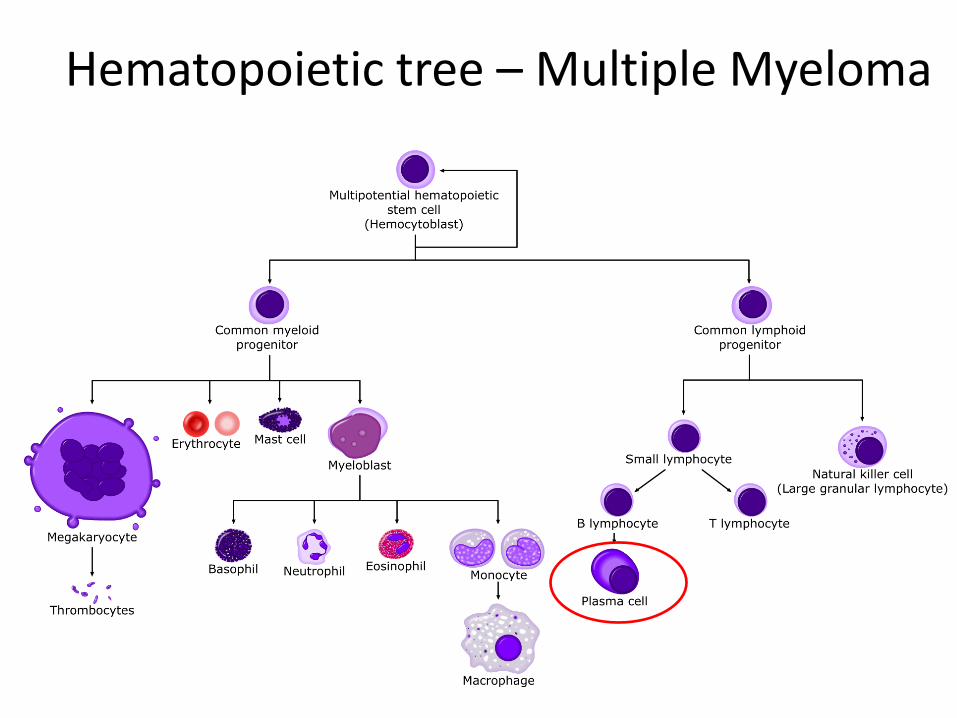
Hematopoietic tree – Multiple Myeloma

Multiple Myeloma • Incurable malignancy of plasma cells • Plasmacytoma • Myeloma cells prefer bone marrow • 1-2 % of all malignancies • 10-15% of hematologic malignancies • In 2015 about 26,850 new cases will be diagnosed
(14,090 in men and 12,760 in women). • In 2015 about 11,240 deaths are expected to occur
(6,240 in men and 5,000 in women). • The 5-year relative survival rate for multiple myeloma is
around 33%.

Multiple Myeloma – risk factors
• Age - > 65 years old. • Gender - Men >women. • Race - black Americans > white Americans • Radiation exposure • Environmental toxins • Viruses • Genetic factors

Multiple Myeloma – diagnosis • Laboratory tests • Imaging • Bone marrow biopsy • Diagnosis of Multiple Myeloma requires:
– A plasmacytoma (proven by biopsy) OR – 10% bone marrow = plasma cells. AND one of the following: – M protein present in blood and/or urine – Myeloma related organ dysfunction

Multiple Myeloma – signs & symptoms
• CRAB – C – serum Calcium elevation – R – Renal insufficiency (SCr >2 mg/dl) – A – Anemia (Hg , 10 g/dL) – B – Lytic Bone lesions
• Neuro S & S • Infections
Multiple Myeloma – staging • Durie-Salmon system • The International Staging System
– Stage I - Serum beta-2 microglobulin is less than 3.5 (mg/L) and the albumin level is above 3.5 (g/L)
– Stage II- Neither stage I or III – Stage III- Serum beta-2 microglobulin is
greater than 5.5

Multiple Myeloma – survival International Staging System Median Survival Stage I 62 months ~5yr Stage II 44 months ~ 3.5yr Stage III 29 months ~ 2.5yr
Poor Prognostic factors: – Older age – Kidney function – IgA sub type – Increased circulating peripheral plasma cells – Chromosomal abnormalities
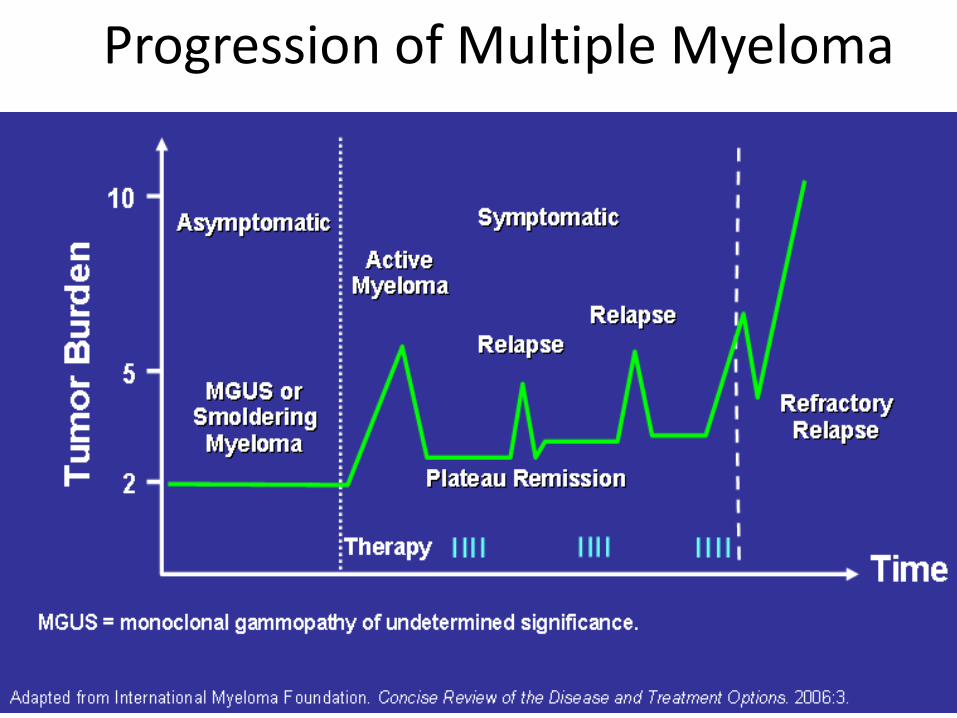
Progression of Multiple Myeloma
Multiple Myeloma – treatment
• Observation with treatment at disease progression
• Indications for treatment – Symptomatic disease – Evidence of organ impairment
• Anemia • Hypercalcemia • Lytic bone leisions • Renal failure

Multiple Myeloma – interventions • Chemotherapy • Immunomodulating agents • Steroids • Bisphosphonates • Radiation • Surgery • Plasmapheresis • Kyphoplasty or Vertebroplasty • Stem Cell Transplant
– Autologous – Allogeneic

Multiple Myeloma – Interventions • Chemotherapy
– melphalan, vincristine, cyclophosphamide, carmustine, and doxorubicin (and liposomal doxorubicin).
• Corticosteroids • Immunomodulating agents
– Thalidomide • Side effects: drowsiness, fatigue, severe constipation, and
neuropathy, blood clots, serious birth defects – Lenalidomide (Revlimid)
• Side effects: thrombocytopenia, low WBCs, painful nerve damage, blood clots, serious birth defects
Multiple Myeloma – Interventions • Proteasome inhibitors - Bortezomib (Velcade)
– Side effects : • Immunosuppression (Acyclovir) • Cytopenias especially thrombocytopenia • Peripheral neuropathy • Diarrhea • Constipation • Rash • Hypotension • Asthenias- lack of strength
Multiple Myeloma - Biophosphonates • Zometa (Zoledronic acid) and Aredia
(Pamidronate Disodium) and Denosumab – Indication
• Hypercalcemia and bone strengthening – Mechanism of action –not fully understood
• Binds to bone matrix • Inhibition of bone resorption • Inhibition osteoclastic activity
• Complications: • Osteonecrosis of the jaw • Renal impairment • Hypocalcemia