Embed Size (px)
Citation preview

AKIHIRO SHIMOSAKA, MD
Houston, USA• Chairperson, Asian Cellular Therapy Organization,
Tokyo, Japan
• Director, R & D, Research Foundation for Community
Medicine, Utsunomiya, Japan Secretary, ISCT Asian
Region
• Honorary Professor, Hematology Institute, Peking
Union Medical College
• Chinese Academy of Medical Sciences, Tianjin, China
• Honorary Professor, School of Oncology, Peking
University, Beijing, China
• Visiting Professor, the Fourth Military Medical
University, Xi-an, China

2
Akihiro Shimosaka, Ph.D.
Asian Cellular Therapy Organization
Research Foundation for Community Medicine
Human NK cell expansion
for cancer therapy

•3
Study Start
material
Stimulation Feeder
cells
NK cell
isolatio
n
Serum Medium NK fold
expansion/timeReferences
Alici PBMC Anti-CD3 No No Human AB
serum
CellGro
SCGM
x190/3w Hum Immunol
62:1092, 2001
Campana PBMC 4-1BB&IL-15
gene-
transfected K562
K562 No Fetal
bovine
serum
CellGro
SCGM
x152/2w Cancer Res
69:4010, 2009
Childs PBMC No EBV-TM
B-cell line
Yes Human AB
serum
X-VIVO 20 x300-900/19d Cytotherapy
11:341, 2009
Multhoff PBMC Hsp-70-peptide No No No CellGro
SCGM
0.9-1.9x109 J Transl Med
7:50, 2009
Dolstra Umbical
Cord
CD34+
SCF,IL7,Flt3L,
TPO,
G-CSF,GM-CSF,
IL-6, MIP-1a, LIF
No No No GBGM x1500-6500/5w
(4.6±2.4x109)PlosONE
5:e9221, 2010
Masuyama PBMC Ab-immobilized
culture bag
No No Self-
plasma
NKGM x859/2w
(6.4±2.3x109/20ml
peripheral blood)
Culture methods for expansion of human NK cells

Protocol for human NK cell expansion
PBMCs + autologous plasma
+
Large bags containing
NKGM (1Lx2~3,) + IL-2
A small bag immobilized with two different
GMP level antibodies
•2 w
eeks
Suspended in 100ml
physiological saline
Stimulation
Expansion
NKGM
Cel
lGro
SCGM
X-V
IVO 1
0
AIM
-V
0
200
400
600
800
Fo
ld e
xpansio
n o
f N
K c
ells
NK cell expansion by various media
4

•5
Large-scale expansion of NK cells
with JM NK cell culture kits
(20 ml peripheral blood from healthy donors, n = 25)
Yield of cells (x109)
NK cell yield (x109)
Fold expansion of NK cells
: 11.4 ± 1.6 (mean ± SD)
: 6.4± 2.3
: 1101 ± 670

•6
Large-scale expansion of NK cells
with JM NK cell culture kits
Subsets of bulk NK cells(%)
NK cell
CD8 T cell
CD4 T cell
: 56.9 ± 18.6 (mean ± SD)
: 26.3 ± 15.9
: 15.9 ± 10.9

•7
0 5 10 15 20 25
0
2
4
6
8
10
12
(x 2100)
CD4+T cell
CD8+
T cell
CD3 CD56 + NK cell
addition of culture medium
Days of culture
Cell n
um
ber(x109)
-Peripheral
blood 30ml
Selective proliferation of NK cells derived
from peripheral blood lymphocytes

•8
Selective proliferation of NK cells derived
from peripheral blood lymphocytes
- FACS analysis -
CD
56
CD3
Initial PBL
4.0x107
Proliferative
lymphocytes
1x1010
culture
for 2 w
NKNK
CD3 CD56+ NK cells 25.1% (1.0x106) 74.4% (7.4x109)-

•9
Cytotoxicity of expanded and resting NK cells
Target : K562
4h exposure
0
20
40
60
80
100
0.3:1 1:1 3:1 10:1
E:T ratio
% c
yto
toxi
city
resting
expanded

•10
Activating receptors Inhibitory receptors
Enhanced expression of activating receptors on expanded NK cells
Control IgG
Resting NK
Expanded NK

•11
CXCR3 expression of NK cells
Peripheral
resting NK
LAK (stimulation
by IL-2 alone)
Expanded NK(Our method)
CX
CR
3
CD16
5% 15% 98%
NK

•12
CXCR3+ NK cells
1. Type1-immune response
Induction of Th1 and CTL
via NK-stimulated DC(DC1)
High level secretion of IFN-gMigration to inflamed tissues
1. Infiltration to tumor sites
augmented by chemokines
2. Recruitment to lymph nodes
Two different functions of CXCR3-expressing NK cells

•13
IFN-g production of NK cells purified from expanded NK cells
compared to CD3-stimulated T lymphocytes
Stimulation of 2 x 104 cells
for 36 h with IL-12 (10 ng/ml)
+ IL-18 (10 ng/ml)
nil IL-12 nil IL-120
1000
2000
3000NK cellCD3-stimulated T cell
+IL-18 +IL-18
IFN
-g (
pg/m
l)

•14
NKG2D and MICA/B
NKG2D+ lymphocytes
NK cell
CD8 T cell
gd T cell
stimulation
Killing
Normal cell
NK
MICA/B (or ULBP)
Malignant cell
NK
NKG2D
binding
Perforin
NKG2D, an activating receptor of NK cells,
binds to MICA/B expressed on malignant cells,
resulting in NK cell activation and killing.

•15
Enhanced expression of NKG2D on expanded NK
CD16
NK
G2D
30 15847 98
Resting PBL Expanded NK
Stimulation
NK NK
& Culture
MFI
CD8 T CD8 T

•16
Re-expression of CD3 z chains of expanded NK cells
PBMCPBMC Expanded NK cells
CD16
CD
3 z
chain
Patient with cancerHealthy subject
NK NKNK
Although expression of CD3 zeta chains which is necessary to induce
ADCC activity is often low in NK cells of cancer patients, expanded NK
cells re-express CD3 zeta chains.

Large-scale expansion of NK cells(20 ml peripheral blood from healthy donors, n = 25)
8
10
12
14
16
Yie
ld o
f cells (
x 10
9)
NK CD8 CD40
20
40
60
80
100
Pro
po
rtio
n o
f e
xpa
nd
ed
ce
lls (
%)
0
5
10
15N
K c
ell
yie
ld (x
10
9)
0
1000
2000
3000
Fo
ld e
xpansio
n o
f N
K c
ells
: Cryopreserved

18
JM NK Cell Expansion Kit
to culture large number of NK cells from peripheral blood

19
Characteristics of JM human NK cell culture method
1. Simple and safe: only use patient PBMC, autologous plasma
without fetal bovine serum or accessory cells
2. High Expansion : 860-fold (n = 25, normal subjects)
One of other methods : 150-fold (Cancer Res 69:4010, 2009)
3. Highly Active NK cell :
Enhanced expression of activating molecules, such as
NKG2D with high level cytotoxicity and IFN-g production

20
Experiences of JM method cultured NK cell
therapy for cancer patients
All patients were at stage III/IV and failed to
conventional therapy

21
Cancer patients treated in New City Osaki ClinicTotal 541 cases (2004.7~2012.11)

•22
Increase of NK cell activity in patients with cancer
after NK cell therapy
NK cell activity
The increase rate 127% 50% 5%
Normal range
“Low” (<25%) “Normal” (25~40%) “High” (40%<)
NK
cell
activity (%)
before after before after before after0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
0
10
20
30
40
50
60
70
Patients were divided in 3 groups based on the ranges of NK cell
cytotoxicity before NK cell therapy.

23
Case 3 55 y.o., FemaleDiagnosis: Breast cancer local recurrence and multiple liver metastases
Chemotherapy: S-1NK cell therapy: x 10
Before NK cell therapy After NK cell therapy
(5 mo. later)

24
Before NK cell therapy After NK cell therapy
(5 mo. later)
Case 3 55 y.o., FemaleDiagnosis: Breast cancer local recurrence and multiple liver metastases
Chemotherapy: S-1NK cell therapy: x 10 。

May, 2011 August, 2011
Case 2 Lung cancer 84 y.o. Male
Diagnosis: Lung cancer
Chemotherapy: none
NK cell therapy: x 6, at a 2-week interval

Case 3 56 y.o. male
Pancreatic tail cancer with multiple liver
metastases and peritoneal dissemination
10 infusions
Lymphocytes : 156.1x109
NK cells : 89.6x109
from a total of 280 ml peripheral blood
0 10 20 30 400
5000
10000
15000
20000
25000
0
50
100
150
200
250CA19-9
CEA
S-1 (day 1-14/3 weeks)GEM (day 1, 8 and 15/4 weeks)
NK cell therapy
GEM (day 1 and 8/3 weeks)
(weeks)
CA
19-9
(U
/ml) C
EA
(ng
/ml)
0 10 20 30 400
20
40
60
80
NK
acti
vit
y (
%)
0 10 20 30 400
200
400
600
800
1000 NKG2D+ NKNKG2D+ T
Nu
mb
er
of
cells
in p
eri
ph
era
l b
loo
d (
/
l)
CT scanNK cell therapy
(w)
(w)
NK and CD8 T cells having NKG2D are activated through specific recognition with MICA/B molecules
widely expressed on malignant cells, and eventually exert cytotoxicity.
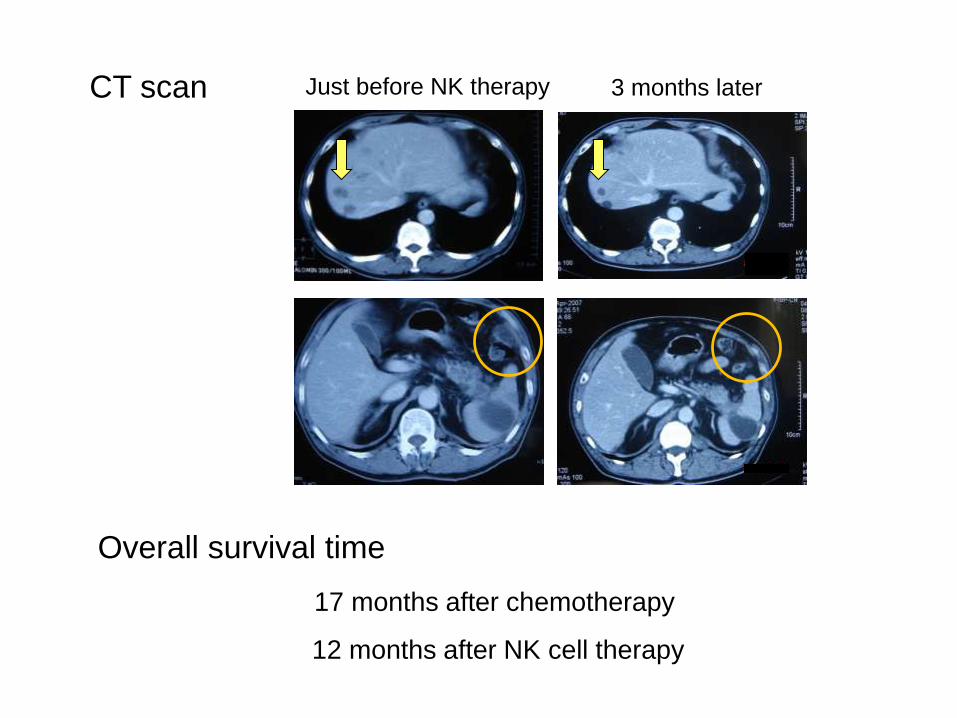
Just before NK therapy 3 months later
17 months after chemotherapy
12 months after NK cell therapy
Overall survival time
CT scan

Profile of patients with pancreatic cancer
NK cell therapy
(infusions*)
0~3 4~
Number of patients 20 33
Mean age (y), M/F 65, 12/8 64, 20/13
PS 0-2
3-4
8
1230
3
Stage IVa / IVb 3/17 12/19
+ Resection 3 8
+ Chemotherapy 12 29
* usually performed at a 2-week interval

29
Ref.1.Jpn J Clin Oncol 38:755, 20082.Cancer Chemother Pharmacol 61:615, 2008 3.ASCO, Abstract #4550、2007 4.Jpn J Clin Oncol 39:49, 2009
1-year survival rate of patients with pancreatic cancer
(%, median)
Gemcitabine+S-1
33
Gemcitabine 264 1)
S-1 40 2)
54 3)
22 4)Gemcitabine+S-1
CasesChemotherapy
25
19
12
NK therapy
NK therapy
NK therapy
NK therapyPS 2-3
IVb
without resection/PS 0-1
+GEM/S- 1(88%)

30
Overall survival time of patients with pancreatic cancer
(month, median)
Gemcitabine+S-1
33
Gemcitabine 264 1)
S-1 40 2)
54 3)
22 4)Gemcitabine+S-1
CasesChemotherapy
25
19
12
NK therapy
NK therapy
NK therapy
NK therapyPS 2-3
Stage IVb
without resection/PS 0-1
+GEM/S- 1(88%)(range:4~52)
(range:4~25)
(range:4~52)
(range:5~37)
Ref.1.Jpn J Clin Oncol 38:755, 20082.Cancer Chemother Pharmacol 61:615, 2008 3.ASCO, Abstract #4550、2007 4.Jpn J Clin Oncol 39:49, 2009

31
Short-term survivors ( n = 8)
died within 5 months after NK cell therapy
not effective
Long-term survivors (n = 13)
survived over 10 months after NK cell therapy
effective
Comparison of immunological changes
between short and long term survivors
in pancreas cancer patients

32
Changes of number of NK cells in peripheral blood
after NK cell therapy
0
200
400
600
800
1000
Healthysubjects(n=25)
Short termsurvivors
(n=8)
Long termsurvivors(n=13)
pre post pre post
Num
ber
of N
K c
ells
in p
erip
hera
l bl
ood
(/l)ns p<0.005

33
Changes of number of NKG2D+ cells in peripheral blood
after NK cell therapy
0
400
800
1200
1600
Healthysubjects(n=25)
Short termsurvivors
(n=8)
pre post
Long termsurvivors(n=13)
pre post
Num
ber
of N
KG
2D+
cells
(/
l)
p<0.005ns

Adverse effects
Adverse effect Notes % of
patients
Relation to NK
cell therapy
Fever (37.5oC~) transient 17 yes
Liver dysfunction increase in LDH,
ALP, etc.
18 no
Anemia decrease in Hb 8 no
Renal dysfunction slight increase
in Cr level
3 no
Dyspnea exacerbation of
COPD
1 possible
Vomiting 1 no
All adverse effects observed in 100 patients (ID:1 ~100) received NK cell therapy.

•35
Application of NK cell therapy
- ADCC –Antibody Dependent Cellular Cytotoxicity
Cancer cell specific attack by NK cells through ADCC pathway
CD16 : FcgRIII
Activating receptor
dependent on CD3 z expression
NK cell
CD16
Cancer cell
antibody
Tumor
antigen
killing
Antibody therapy
Breast cancer : trastuzumab
Malignant lymphoma: rituximab

•36
ADCC activity of expanded NK cells
Ab alone
Target
Daudi 1x105/well
Effector
CD4 12 %
CD8 44 %
NK 43 %
Antibody
Rituximab 5 g/ml
16 h culture
0.8 4 200
20
40
60
80
100w/o Ritux.
w/ Ritux.
E/T ratio
% C
ell
lysis

NK Cell Therapy of CancerDr. Dario Campana, Singapore
Allogeneic hematopoietic
stem cells transplant
Infusion of NK cells
Donor KIR profiles predictive of
alloreactivity are associated
with lower relapse rates
Selection of donor with
alloreactive KIR profile
Immunosuppressive but non-
myeloablative conditioning
5/19 patients with high-risk
AML achieved complete
remission (Miller et al. Blood 2005)
Infused NK cells persist for at
least 1 week (Miller et al. Blood
2005; Rubnitz et al. J Clin Oncol 2010)
No GvHD

NK Cell Expansion from:
Peripheral blood of healthy donors, children with acute lymphoblastic leukemia in remission, patients with multiple myeloma, patients with gastric cancer
Cord blood
Liver lymphocytes

Clinical Use of Expanded NK Cells
Acute Myeloid Leukemia
Solid tumors
Acute Lymphoblastic Leukemia

Conclusion
1. This novel method is feasible for expansion of
human NK cells.
2. NK cell therapy presented here is safe for
cancer patients.
3. Further study is necessary to confirm the clinical
effects of NK cell therapy on cancer.
•40

41
Enhancement of NK cell killing
• Through ADCC activity in combination with antibody-based therapy
for cancer.
• In the allogeneic setting to avoid the negative signals.
Enhancement of CTL induction
• With cancer vaccine therapy (peptide, DC, DNA) through dendritic
cell-NK cell cross-talk.
Replace T-cell donor lymphocyte infusion
To manage MRD, relapse and uncontrollable infection
Future challenges of NK-cell based immunotherapy

AcknowledgmentDr. Junichi Masuyama
New Osaki Clinic, Tokyo
Dr. Dario Campana
Department of Pediatrics, Yong Loo Lin School of
Medicine, National University of Singapore