Embed Size (px)
Citation preview

REVIEW
Rituximab in B-Cell Hematologic Malignancies:A Review of 20 Years of Clinical Experience
Gilles Salles . Martin Barrett . Robin Foa . Joerg Maurer .
Susan O’Brien . Nancy Valente . Michael Wenger . David G. Maloney
Received: July 14, 2017 / Published online: October 5, 2017� The Author(s) 2017. This article is an open access publication
Abstract: Rituximab is a human/murine, chi-meric anti-CD20 monoclonal antibody withestablished efficacy, and a favorable andwell-defined safety profile in patients with var-ious CD20-expressing lymphoid malignancies,including indolent and aggressive forms ofB-cell non-Hodgkin lymphoma. Since its firstapproval 20 years ago, intravenously adminis-tered rituximab has revolutionized the
treatment of B-cell malignancies and hasbecome a standard component of care for fol-licular lymphoma, diffuse large B-cell lym-phoma, chronic lymphocytic leukemia, andmantle cell lymphoma. For all of these diseases,clinical trials have demonstrated that rituximabnot only prolongs the time to disease progres-sion but also extends overall survival. Efficacybenefits have also been shown in patients withmarginal zone lymphoma and in more aggres-sive diseases such as Burkitt lymphoma.Although the proven clinical efficacy and suc-cess of rituximab has led to the development ofother anti-CD20 monoclonal antibodies inrecent years (e.g., obinutuzumab, ofatumumab,veltuzumab, and ocrelizumab), rituximab islikely to maintain a position within the thera-peutic armamentarium because it is well estab-lished with a long history of successful clinicaluse. Furthermore, a subcutaneous formulationof the drug has been approved both in the EUand in the USA for the treatment of B-cellmalignancies. Using the wealth of data pub-lished on rituximab during the last two decades,we review the preclinical development ofrituximab and the clinical experience gained inthe treatment of hematologic B-cell malignan-cies, with a focus on the well-established intra-venous route of administration. This article is acompanion paper to A. Davies, et al., which isalso published in this issue.Funding: F. Hoffmann-La Roche Ltd., Basel,Switzerland.
Enhanced content To view enhanced content for thisarticle go to http://www.medengine.com/Redeem/C80CF0607015D872.
G. Salles (&)Hematologie, Hospices Civils de Lyon andUniversite de Lyon, Pierre-Benite, Lyon, Francee-mail: [email protected]
M. BarrettRoche Products Ltd., Welwyn Garden City, UK
R. FoaDepartment of Cellular Biotechnologies andHematology, Sapienza University, Rome, Italy
J. Maurer � M. WengerF. Hoffmann-La Roche Ltd., Basel, Switzerland
S. O’BrienChao Family Comprehensive Cancer Center,University of California, Irvine, Orange, CA, USA
N. ValenteGenentech Inc., South San Francisco, CA, USA
D. G. MaloneyFred Hutchinson Cancer Research Center,Seattle, WA, USA
Adv Ther (2017) 34:2232–2273
DOI 10.1007/s12325-017-0612-x

Keywords: B-cell lymphoma; CD20; Chroniclymphocytic leukemia; Diffuse large B-celllymphoma; Follicular lymphoma; Monoclonalantibody; Non-Hodgkin lymphoma; Rituximab;Safety; Treatment outcome
INTRODUCTION
Hematologic B-cell malignancies comprise alarge, heterogeneous group of lymphoprolifer-ative disorders that range from slow-growing,indolent non-Hodgkin lymphomas (NHLs),such as follicular lymphoma (FL) and chroniclymphocytic leukemia (CLL), to more aggressiveforms of NHL, such as diffuse large B-cell lym-phoma (DLBCL) [1, 2]. B-cell disorders representmore than 85% of all NHL cases [3]. In 2012,there were an estimated 385,700 new cases ofNHL worldwide, with an estimated 199,700patients dying from the disease [4], and evi-dence from US and UK statistics suggests thatthe annual incidence has been rising steadilysince the 1970s [5, 6]. NHL incidence rates arehigher among the elderly population than inthe younger population, with diagnoses of NHLmost common among patients aged 65–74 years[7], and a projection of population dynamics forCLL patients in the USA predicts that 199,000patients will have the disease in 2025, partlydriven by improved survival [8]. In view of theaging population worldwide, the diagnosis andtreatment of B-cell hematologic malignanciesare likely to remain an important focus forhealthcare providers for the foreseeable future.
The treatment strategy for NHL is largelydetermined by histologic features, disease stage,patient age, prognosis, and the presence ofcomorbid disease. Staging is established usingvalidated systems, which include the Ann Arborstaging classification for DLBCL [9] and FL [10],and the Binet and Rai staging systems for CLL[11]. Prognostic assessments at initial diagnosisare based on the International Prognostic Index(IPI) and age-adjusted IPI for DLBCL [9], theFollicular Lymphoma International PrognosticIndex for FL [10], and the Mantle Cell Lym-phoma International Prognostic Index formantle cell lymphoma (MCL) [12]. In CLL, theBinet and Rai staging systems are both used to
categorize patients into three groups accordingto their prognosis [11], and the InternationalPrognostic Index for patients with CLL may alsobe applied [13]. In DLBCL, gene expressionprofiling can now be used to determine prog-nosis by identifying distinct disease subtypesaccording to their cell of origin [14, 15].
The development of monoclonal antibodies(mAbs) as a therapeutic treatment began in1975 by researchers funded by the NationalCancer Institute, Cesar Milstein and GeorgesKohler [16], who described the formation ofhybridomas to rescue and produce a limitlesssupply of mAbs from a single B cell. For thiswork, Milstein and Kohler received the NobelPrize for Physiology or Medicine in 1984 jointlywith Niels Jerne [17]. Treatment with the firstmAb occurred in 1980 [18], and this was fol-lowed by pioneering studies by Ron Levy’sgroup at Stanford University, which producedpatient-specific monoclonal anti-idiotype anti-bodies for treating lymphoma patients [19].These studies proved the concept that mAbscould have a dramatic antitumor effect and thatthey were safe, but commercialization was lim-ited by the fact they were patient specific. At thesame time, antibodies were being used toinvestigate cell-surface proteins, resulting in theidentification of B-cell-restricted antigens suchas CD19 and CD20. This discovery paved theway for the production of therapeutic mAbsthat could be used in patients whose tumorsexpressed those antigens. Given the widespreadexpression of CD20 on malignant B cells,treatment with a murine mAb against CD20 wasundertaken [20], and demonstrated safety,albeit with limited clinical activity. This ulti-mately led to the development of a chimericanti-CD20 mAb with increased antitumoractivity; namely, rituximab.
Rituximab (MabThera�/Rituxan�/RituxanHYCELATM, F. Hoffmann-La Roche Ltd.) is ahuman/murine chimeric, glycosylatedimmunoglobulin (Ig) G1-j mAb containingmurine light- and heavy-chain variable regionsequences, and human kappa and human IgG1constant region sequences. Rituximab hasspecific affinity for the B-lymphocyte trans-membrane protein, CD20, which is expressedon normal B cells (excluding stem cells, pro-B
Adv Ther (2017) 34:2232–2273 2233

cells, and plasma B cells) and on most malig-nant B cells [21].
Intravenously administered rituximab wasgranted regulatory approval in 1997 by the USFood and Drug Administration and in 1998 bythe European Medicines Agency for use inrelapsed/refractory indolent NHL. Approvals foruse in CLL followed in 2009 and 2010, respec-tively. Intravenously administered rituximabwas the first therapeutic mAb to be used in thefield of oncology, establishing a new class ofanticancer drugs. Since its approval, rituximabhas revolutionized the treatment of B-cellmalignancies, becoming a standard componentof care for FL [10, 22], DLBCL [9, 22], and CLL[11, 23]. Rituximab has also been included inthe WHO Model List of Essential Medicinessince 2015 [24]. A new formulation of rituximabfor subcutaneous administration has also beenapproved in the EU and USA for the treatmentof patients with NHL and CLL, based primarilyon the results of the SABRINA and SAWYERclinical trials [25, 26]. Subcutaneously admin-istered rituximab was developed primarily tosimplify administration and shorten theadministration time, and thus improve thepatient experience by decreasing the burden oftreatment. In addition, this may facilitate accessto this important drug in resource-poor settingswhere intravenous administration may pose aparticular challenge.
Clinical experience with intravenouslyadministered rituximab in B-cell hematologicmalignancies is extensive, currently extendingto 20 years and to more than four millionpatient exposures worldwide, including datafrom an estimated 18,000 patients treated withrituximab in corporate-sponsored or supportedclinical trials (Roche, data on file not publicallyavailable). Clinical experience with rituximabalso extends to off-label use in MCL, for whichrituximab is a standard component of care [27],and in other hematologic malignancies,including marginal zone lymphoma, Hodgkinlymphoma, Burkitt lymphoma, and B-lineageacute lymphoblastic leukemia (see ‘‘ClinicalEfficacy of Rituximab’’), as well as to non-hematologic licensed indications, includingrheumatoid arthritis, and granulomatosis withpolyangiitis and microscopic polyangiitis
[28–30], which are outside the scope of thisreview.
This article reviews the preclinical devel-opment of rituximab and clinical experiencewith the intravenous formulation in B-cellhematologic malignancies. Discussion of thepreclinical and clinical experience with sub-cutaneously administered rituximab is outsidethe scope of this review, but is coveredextensively in a recent publication by Davieset al. [31].The information reported in thisarticle is derived from previously conductedstudies, and does not include any new studiesof human or animal subjects performed byany of the authors.
MECHANISM OF ACTIONOF RITUXIMAB
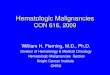
Rituximab binds with high affinity and speci-ficity to the CD20 antigen, which is expressedon the vast majority of malignant B cells. Theapparent affinity constant of rituximab forhuman CD20, as determined by Scatchardanalysis using a human lymphoblastoid cell line(SB), is approximately 5.2 nmol/L [32]. Thecharacteristics of rituximab binding to theCD20 molecule led to the definition of the‘‘type I’’ anti-CD20 mAbs, which share severalproperties and are distinct from type II mAbssuch as obinutuzumab. At least four mechanis-tic pathways are thought to be responsible forthe elimination of CD20? cells by rituximab(Fig. 1): antibody-dependent cellular cytotoxic-ity (ADCC), antibody-dependent cellularphagocytosis, complement-dependent cytotox-icity (CDC), and direct antitumor effects viaeither apoptosis or other cell death pathways[33–36]. Binding of the fragment crystallizable(Fc) portion of the rituximab mAb to tumorcells results in the reorganization of CD20molecules into lipid rafts and subsequent acti-vation of the classical pathway of the comple-ment cascade. This leads to CDC, includingtumor cell lysis and augmentation of phagocy-tosis. ADCC occurs as a result of an interactionbetween the Fc portion of rituximab in anti-body-coated tumor cells and membrane-boundFcc receptors expressed on the surface of
2234 Adv Ther (2017) 34:2232–2273

effector cells (natural killer cells, granulocytes,and macrophages) [37]. This interaction triggersthe onset of cellular immune responses centralto ADCC, including the release of cytokines,chemokines, and mediators that kill target cells.
In addition, rituximab binding to CD20 on Blymphocytes is thought to induce cell death vianonclassical apoptosis by triggering thecrosslinking of multiple CD20 molecules[34–36].
Fig. 1 Mechanisms of rituximab-mediated cell death.Rituximab-coated B cells are killed by at least fourdifferent mechanisms: (1) binding of rituximab to CD20on the B-cell surface causes activation of the complementcascade, which generates the membrane attack complex(MAC), which can directly induce B-cell lysis by comple-ment-dependent cytotoxicity (CDC). (2) Binding ofrituximab allows interaction with natural killer (NK) cellsvia Fc receptors (FcRs) III, which leads to antibody-de-pendent cellular cytotoxicity (ADCC). (3) The Fc portionof rituximab and the deposited complement fragments
allow recognition by both FcRs and complement receptorson macrophages, which leads to phagocytosis and ADCC.(4) The crosslinking of several molecules of rituximab andCD20 in the lipid raft determines the interaction of thesecomplexes with elements of a signaling pathway involvingSrc kinases that mediate direct apoptosis. FCR Fc receptor,FCcR Fcc receptor. (Republished with permission of theAmerican Society of Hematology from Jaglowski et al.[166]; permission conveyed through the Copyright Clear-ance Center)
Adv Ther (2017) 34:2232–2273 2235

PHARMACODYNAMICSOF RITUXIMAB
Potent B-cell-depleting activity in peripheralblood and lymphoid tissues was reported withrituximab in phase I and phase II studies[38, 39]. Circulating CD20? B cells underwentrapid depletion in the peripheral blood ofpatients with recurrent B-cell lymphoma treatedwith a single dose of rituximab. This effect wasdose dependent and persisted for at least 2–3 months in most patients. In addition, therewas evidence of a fall in the number of B cells inlymph node biopsy samples 2 weeks afteradministration of rituximab compared withpretreatment [38]. In a second group of patientswith relapsed low-grade NHL treated with mul-tiple doses of rituximab, B-cell depletion wasmaintained until nearly 6 months after treat-ment, followed by a slow recovery [39].
PHARMACOKINETIC PROFILEOF RITUXIMAB
The pharmacokinetic (PK) profile of rituximabin a variety of B-cell malignancies has beencharacterized throughout the product’s lifecycle, with use of original data from clinicalstudies as described herein, and by integrationof these data into population PK analyses.
Among patients with low-grade or follicularNHL treated with intravenously administeredrituximab, serum concentrations of rituximabwere detectable after the first infusion andincreased with subsequent administrations[38–40]. In 203 patients with relapsed low-gradelymphoma who received four weekly intra-venous infusions of rituximab (375 mg/m2) intwo clinical studies [39, 40], the mean maxi-mum plasma concentration (Cmax) of rituximabwas 486 lg/mL (range 77.5–996.6 lg/mL) afterthe fourth dose, and the drug was detectable inserum for up to 6 months after completion ofdosing [29, 30]. In another study, the medianserum rituximab concentration after the last offour weekly infusions in a group of 22 FLpatients with low tumor burden was approxi-mately 380 lg/mL, and the study authors
predicted a steady-state plasma concentrationin this group of 438 lg/mL if the drug had beenadministered once weekly for 8 weeks [41].
Elimination of rituximab in patients withB-cell malignancies is target mediated (i.e.,binding of the drug to CD20 on B cells clears theantibody from the serum during the initialinfusions, leading to a reduction in or satura-tion of accessible CD20-binding sites at lymphnodes). This was seen in the phase III study byBerinstein et al. [40], which found a markedincrease in mean elimination half-life (t1/2)from 76.3 to 205.8 h from the first to the fourthrituximab infusion, which corresponded to anearly fourfold decrease in clearance (from 38.2to 9.2 mL/h) and an increase in rituximab Cmax
from 205.6 to 464.7 lg/mL. Later studiesreported even slower clearance (i.e., t1/2 forrituximab of approximately 3 weeks), althoughwith large intersubject variability [41, 42]; totalsystemic clearance was estimated at3.1–11.9 mL/h/m2 in the earlier study [41].
No notable differences were observedbetween the PK profiles of rituximab when itwas administered as monotherapy and whenrituximab therapy was combined withcyclophosphamide, doxorubicin, vincristine,and prednisone (CHOP) chemotherapy [43]. Apopulation PK analysis in 298 patients withNHL from six clinical studies who were treatedwith rituximab alone or rituximab combinedwith CHOP (R-CHOP) showed that age, sex,race, and WHO performance status had noeffect on rituximab pharmacokinetics [44].Higher B-cell counts and greater baseline tumorburden were associated with increased clearancerates, and the volume of distribution varieddepending on body surface area and CHOPchemotherapy. Rituximab elimination wasreduced following multiple infusions. Thisanalysis found that the PK profile of rituximabin NHL patients is best described by atwo-compartment model with a nonspecifictime-independent clearance component and atime-dependent clearance component exhibit-ing first-order kinetics [44].
In a population PK analysis in previouslytreated patients with relapsed or refractory CLLtreated with rituximab (375 mg/m2 in cycle 1then 500 mg/m2 in cycles 2–6) and
2236 Adv Ther (2017) 34:2232–2273

standard-dose fludarabine and cyclophos-phamide (FC), PK data for rituximab in 21patients showed a time-dependent PK profilewith wide interpatient variability [45]. Thestudy authors noted differences in PK parame-ters in these CLL patients compared withpatients with NHL from a previous populationanalysis [44]: CLL patients had faster clearance(1260 mL/day vs 585 mL/day), a larger volumeof distribution (central 4150 mL vs 2700 mL,peripheral 2320 mL vs 1500 mL), and a lowerrate of change from the target-mediated clear-ance pathway (via CD20) to catabolic elimina-tion (via IgG1) compared with NHL patients[45].
Rituximab serum concentrations have beenreported to correlate with clinical response. In adetailed analysis of 166 patients with low-gradeor follicular NHL, median serum concentrationsof rituximab were higher in responders than innonresponders after each of the four weeklyinfusions and up to 3 months after treatment(e.g., 502.8 and 412.4 lg/mL, respectively, afterthe fourth infusion; P = 0.01) [40]. There was aninverse relationship between serum rituximabconcentrations and baseline tumor burdenindicators. Linear regression showed the inversecorrelation between absolute levels of circulat-ing peripheral B cells at the baseline and ritux-imab concentration to be statisticallysignificant from the second infusion until1 month after treatment. Inverse correlationsbetween rituximab concentrations in serum and(1) the maximum diameter of the largest lesionand (2) the sum of the product of the perpen-dicular diameters of the six largest lesions werestatistically significant at all time points mea-sured with the exception of the period follow-ing the first infusion.
A similar relationship between exposure andresponse was seen in a phase II study of 68Japanese patients with aggressive B-cell lym-phoma [46]. Serum rituximab concentrationswere evaluated in seven responders and fivenonresponders. The mean (± standard devia-tion) trough levels and areas under curves ofserum antibody concentration versus time(AUC) for responders and nonresponders were59.7 ± 11.4 and 43.0 ± 6.4 lg/mL, respec-tively, and 608,585 ± 147,373 and 383,053 ±
176,903 lg h/mL, respectively, with significantdifferences between groups (P = 0.021 andP = 0.037). Pretreatment tumor size (sum of theproduct of the perpendicular diameters) wasinversely correlated with AUC (P\0.05 bySpearman’s rank correlation coefficient).
Other studies have shown that rituximabexposure falls as tumor volume increases, andthat higher exposure correlated with betterresponse and/or outcome [47–50]. A recentreport from Tout et al. [50] in 108 previouslyuntreated DLBCL patients demonstrated thatrituximab exposure decreased as baseline totalmetabolic tumor volume increased, with a highAUC in cycle 1 being associated with better PETresponse after cycle 4 (odds ratio 5.56,P = 0.0006) and longer progression-free-survival(PFS; hazard ratio, HR, 0.38, P = 0.011) andoverall survival (OS; HR 0.17, P = 0.001). Sexand body weight may also influence rituximabpharmacokinetics [51, 52]. In a study of 20elderly patients (aged 61–79 years) with DLBCL,Muller et al. [51] found that rituximab clearancewas reduced and t1/2 increased in women com-pared with men. In addition, the volume ofdistribution increased by 0.1 L/kg for bodyweights greater than 75 kg. Although the ben-efit from addition of rituximab to chemother-apy is similar in younger male and femalepatients, this does not seem to hold true forolder patients, with elderly female patientsbenefitting more than elderly male patients[52]. Swedish registry data have shown similarpatterns, with possibly inadequate dosing inyounger female patients, and male patients ofall ages [53].
MANUFACTURE OF RITUXIMAB
Rituximab is produced in suspension culture bya Chinese hamster ovary transfectoma con-taining the TCAE 8 expression vector in anutrient medium. Process and product impuri-ties such as high molecular weight aggregatesare then removed by protein A affinity chro-matography and anion exchange chromatogra-phy. The purified rituximab is then formulatedas an aqueous concentrate for intravenousadministration under sterile conditions, in a
Adv Ther (2017) 34:2232–2273 2237

mixture of sodium chloride (9.0 mg/mL),polysorbate 80 (0.7 mg/mL), sodium citratedihydrate (7.35 mg/mL), and water (solution pH6.5, rituximab concentration 10 mg/mL), andpackaged in 10- or 50-mL borosilicate glassvials. As the vials are designed for single use, nopreservatives are added to the formulation. Anunopened vial has a shelf life of 30 monthswhen stored at the recommended temperatureof 2–8�C.
CLINICAL EFFICACY OF RITUXIMAB
Rituximab in Follicular Lymphoma
The initial regulatory approval of rituximab in1997 in FL was based on data from a pivotalphase II trial of rituximab monotherapy in 166patients with relapsed or refractory low-gradeNHL. The overall response rate (ORR) in thistrial was 48% [complete response (CR) rate 6%],and the median time to progression for theintent-to-treat population was 13.0 months[54]. Several other trials published between1997 and 2000 showed similar results inrelapsed/refractory low-grade NHL, with overalltumor response rates ranging from 38% to 47%after 4 weeks’ treatment with rituximab [55–57],and 57% after 8 weeks’ treatment [58]. Each ofthese studies involved between 30 and 70patients.
More recently, a 74% ORR and a 28% CRrate, with median PFS of 23.5 months and91.7% OS rate after 7 years of follow-up, werereported in 46 patients with low tumor burdendisease after first-line induction therapy withfour weekly doses of rituximab at 375 mg/m2
[59]. Two phase III studies in larger numbers ofpatients have also shown activity of rituximabmonotherapy. Taverna et al. [60] reported a16.9% CR/unconfirmed CR rate in 261 patientsundergoing induction therapy with four dosesof rituximab (this study included patients withpreviously untreated and relapsed/refractorydisease). Subsequent short-term (four doses;n = 82) or long-term (5 years or less; n = 83)rituximab maintenance therapy yielded medianevent-free survival (EFS) of 3.4 and 5.3 years,respectively (P = 0.14). In a trial in patients with
advanced disease receiving four doses of ritux-imab alone (n = 156) or in conjunction withinterferon alfa (n = 157) [61], there was a 78%ORR to an initial cycle of treatment. Responderswho received a second cycle showed CR/un-confirmed CR rates of 21% and 41%, respec-tively (P = 0.005). The median times totreatment failure were 28 and 21.5 months,respectively (P = 0.302).
Since then, substantial clinical benefit hasbeen reported in FL patients from the incorpo-ration of rituximab into induction chemother-apy regimens in both the first-line setting[62–70] and in previously treated patients[62, 71].
Induction treatment with rituximab andchemotherapy has been shown to be superior tochemotherapy alone in several large-scale trials(typical treatment duration of 6 months),mainly conducted in previously untreatedpatients with stage III/IV FL, consistentlyachieving better results in terms of ORR, CR,time to treatment failure, PFS, and OS (Table 1).A variety of chemotherapy regimens werecombined with rituximab therapy in thesestudies, including CHOP, cyclophosphamide,vincristine, and prednisolone (CVP), andmitoxantrone, chlorambucil, and prednisone(MCP) regimens. On the basis of the body ofevidence provided by these studies, rituximabtherapy plus chemotherapy has been adoptedworldwide as the standard of care for the first-line treatment of patients with FL [10, 22], andthe worldwide indications for rituximab arereflective of this.
The use of rituximab maintenance therapyto preserve responses to induction therapy inresponding patients, and to further enhanceclinical outcomes, has also been demonstratedin previously untreated patients with advancedFL, as demonstrated in the Eastern CooperativeOncology Group (ECOG) 1496 and PRIMA trials[72–74]. In these two studies, previouslyuntreated patients with advanced FL who hadresponded to either CVP (ECOG 1496) or one ofthree rituximab–chemotherapy inductiontreatment regimens [rituximab plus CVP, R-CHOP, or rituximab plus fludarabine,cyclophosphamide, and mitoxantrone (R-FCM);PRIMA] were randomized to receive rituximab
2238 Adv Ther (2017) 34:2232–2273

Table 1 Summary of key studies evaluating rituximab-based immunochemotherapy in patients with previously untreated orrelapsed/refractory follicular lymphoma
Study reference Line of therapyand no. ofpatients
Treatmentregimen
ORR CR PFS, EFS, or otherparameter asindicateda
OS
GLLSG
Hiddemann et al.
[63]
1L (428) R-CHOP vs
CHOP
96% vs
90%b
20% vs
17%
TF (median
observation time
18 months):
12.6% vs 29.8%b
Deaths:
2.7% vs
8.3%b
East German Study
Group
Herold et al. [64]
1L (201) R-MCP vs MCP 92% vs
75%b
50% vs
25%b
EFS: NR vs
26 monthsb
PFS: NR vs
28.8 monthsb
mFU: 47 months
4-year: 87%
vs 74%b
Marcus et al. [65]
Marcus et al. [66]
1L (321) R-CVP vs CVP 81% vs
57%b
41% vs
10%b
TTF: 27 months vs
7 monthsb
DFS: NR vs
21 monthsb
mFU: 30 months
4-year: 83%
vs 77%b
GELA-GOELAMS
FL2000
Salles et al. [67]
Bachy et al. [68]
1L (358) R-CHVP ? INF
vs
CHVP ? INF
81% vs
72%b
51% vs
39%b
EFS: 5.5 years vs
2.8 yearsb
5-year EFS: 53% vs
37%b
8-year EFS: 44% vs
28%b
mFU: 5 and 8.3 years
5-year: 84%
vs 79%
8-year: 79%
vs 70%
FOLL05
Federico et al. [69]
1L (504) R-CVP vs
R-CHOP
vs R-FM
88% vs
93% vs
91%
67% vs
73% vs
72%
3-year TF: 46% vs
62% vs 59%
HR 0.62, R-CHOP
vs R-CVPb,c, HR
0.63, R-FM vs
R-CVPb
3-year PFS: 52% vs
68% vs 63%
HR 0.64, R-CHOP
vs R-CVPb,c, HR
0.66, R-FM vs
R-CVPb,c
mFU: 34 months
3-year: 95%
(all
patients)
Adv Ther (2017) 34:2232–2273 2239

maintenance therapy for 2 years or observation.In the ECOG 1496 study, rituximab mainte-nance therapy achieved a significantly higher3-year PFS rate than observation (64% vs 33%;HR 0.4, P\0.001) [72]. OS at 3 years was,however, comparable between the two arms(91% vs 86%; HR 0.6, P = 0.08). In the PRIMAtrial, the 3-year PFS rate was 74.9% in therituximab maintenance therapy arm comparedwith 57.6% for patients randomized to undergoobservation (HR 0.55, P\0.001) [73], andlong-term follow-up (median of 73 months)
showed that the PFS benefit achieved withrituximab maintenance therapy was main-tained after 6 years (59.2% vs 42.7%; HR 0.58,P\0.0001) [74]. Six-year OS in the PRIMA trialwas favorable with both rituximab maintenancetherapy and observation, and did not differsignificantly between the two arms. Neithermedian PFS nor median OS had been reached inthe rituximab maintenance therapy arm at the6-year follow-up.
The RESORT trial compared the efficacy ofrituximab maintenance therapy with rituximab
Table 1 continued
Study reference Line of therapyand no. ofpatients
Treatmentregimen
ORR CR PFS, EFS, or otherparameter asindicateda
OS
Rummel et al. [70] 1L (514: 420
NHL,
including 279
FL; 94 MCL)
R ? benda vs
R-CHOP
93% vs
91%
40% vs
30%b
PFS: 69.5 months vs
31.2 months
(HR 0.58)
mFU: 45 months
Deaths:
16.5% vs
17.8%
Czuczman et al.
[62]
1L and 2L (38) R-CHOP 100% (1L
100%,
R/R
100%)d
87% (1L
90%,
R/R
78%)d
TTP: 82.3 months
mFU: NA
EORTC 20981
van Oers et al. [71]
R/R (465) R-CHOP vs
CHOP
85.1% vs
72.3%b
29.5% vs
15.6%b
PFS: 33.1 months vs
20.2 months
(HR 0.65b)
mFU: 39.4 months
3-year:
82.5% vs
71.9%
(HR
0.74)
All studies were phase III randomized trials except for the study of Czuczman et al. [62], which was a single-arm phase IIstudybenda bendamustine, CHOP cyclophosphamide, doxorubicin, vincristine, and prednisone, CHVP cyclophosphamide,doxorubicin, etoposide, and prednisone, CR complete response, CVP cyclophosphamide, vincristine, and prednisone, DFSdisease-free survival, EFS event-free survival, EORTC European Organisation for Research and Treatment of Cancer, FLfollicular lymphoma, FM fludarabine and mitoxantrone, GELA Groupe d’Etude des Lymphomes de l’Adulte, GLLSGGerman Low-Grade Lymphoma Study Group, GOELAMS Groupe Ouest Est des Leucemies et Autres Maladies du Sang,HR hazard ratio, INF interferon, 1L first line, 2L second line MCL mantle cell lymphoma, MCP mitoxantrone, chlo-rambucil, and prednisone, mFU median follow-up, NA not available, NHL non-Hodgkin lymphoma, NR not reached, ORRoverall response rate, OS overall survival, PFS progression-free survival, R rituximab, R/R relapsed/refractory, TF treatmentfailure, TTF time to treatment failure, TTP time to progressiona Median valuesb Statistically significant differencec HR adjusted by Follicular Lymphoma International Prognostic Index 0–2 vs 3–5d Updated values assessed according to International Workshop response criteria
2240 Adv Ther (2017) 34:2232–2273

retreatment in 545 patients with previouslyuntreated FL and a low tumor burden [75]. Thestudy found no difference between groups interms of the primary end point, time to treat-ment failure (this outcome measure was definedas a lack of response to rituximab retreatment),time to progression of less than 26 weeks,commencement of alternative treatment, or aninability to complete planned treatment [75].The lack of a significant benefit of rituximabmaintenance therapy over rituximab retreat-ment may have been because the primary endpoint favored the retreatment arm or becausethe study was conducted in patients with lowtumor burden, in contrast to the PRIMA study[73, 74], which was conducted in patientsrequiring treatment.
Similarly, in the relapsed/refractory FL set-ting, significant improvements in efficacy havebeen reported with rituximab induction ther-apy plus chemotherapy and rituximab mainte-nance therapy compared with standardchemotherapy (Table 2) [71, 76–79]. For exam-ple, superior outcomes were reported withR-FCM compared with fludarabine, cyclophos-phamide, and mitoxantrone (FCM) in patientswith relapsed/refractory FL or MCL enrolled in aphase III study conducted by the GermanLow-Grade Lymphoma Study Group [76]. In allstudy patients, the addition of rituximab toFCM induction therapy significantly increasedORR (79% vs 58%; P = 0.01), median PFS(16 months vs 10 months; P = 0.04), and med-ian OS (not reached vs 24 months; P\0.01)compared with FCM alone [76]. A second ran-domization, to rituximab maintenance therapyor observation in patients who had respondedto induction therapy, showed a significantprolongation of response duration with main-tenance treatment (median, not reached vs17 months; P\0.001) [77]. The phase III Euro-pean Organisation for Research and Treatmentof Cancer 20981 trial included an inductionphase during which patients with relapsed/re-fractory FL were randomized to receive R-CHOPor CHOP, followed by randomization to ritux-imab maintenance therapy or observation forthose patients who responded to inductiontherapy [71, 78]. The study investigators repor-ted a significant increase in ORR (85% vs 72%;
P\0.001) and PFS (33.1 months vs20.2 months; HR 0.65, P\0.001), and a trendtoward an increase in 3-year OS rate (83% vs72%; HR 0.74, P = 0.096) with R-CHOP com-pared with CHOP induction therapy. Rituximabmaintenance therapy subsequently achieved asignificant improvement in median PFS com-pared with observation (51.5 months vs14.9 months; HR 0.40, P\0.001); the 5-year OSrate was also greater with rituximab mainte-nance therapy (74% vs 65%; HR 0.70, P = 0.07),but the difference between the two arms did notachieve statistical significance. The investiga-tors cited the unbalanced use of rituximab inpostprotocol salvage treatment as a possiblereason for this finding [78]. A similar pattern ofresults was reported in the phase III SAKK 35/98trial evaluating induction therapy with sin-gle-agent rituximab followed by rituximabmaintenance therapy or observation (Table 2)[79], further confirming the benefit of ritux-imab maintenance therapy in patients withrelapsed/refractory FL. In a meta-analysis ofdata from 2315 patients in seven randomizedtrials, survival was significantly improved withrituximab maintenance therapy compared withobservation only (HR 0.79, 95% confidenceinterval 0.66–0.96) for all categories of patientsexcept those receiving first-line therapy thatincluded rituximab induction therapy [80].
Watchful waiting until disease progressionoccurs has conventionally been used in FLpatients with advanced disease with low tumorburden [81]. The use of rituximab in this settingto delay the need for chemotherapy or radio-therapy was explored in a multinational phaseIII study in 463 patients who underwentwatchful waiting, rituximab induction therapy(375 mg/m2 weekly for 4 weeks), or rituximabinduction therapy followed by 2 years’ mainte-nance therapy [82]. Of the patients in thewatchful waiting group, 46% had not needednew treatment at 3 years, compared with 88%in the rituximab maintenance therapy group(HR 0.21, P\0.0001). Significantly morepatients in the induction therapy group than inthe watchful waiting group (78%) had notneeded new treatment at 3 years (HR 0.35,P\0.0001), whereas the proportion not need-ing new treatment was similar in the
Adv Ther (2017) 34:2232–2273 2241

Table2
Summaryof
keyphaseIIIrand
omized
studiescomparing
rituximab
maintenance
therapywithobservationafterinductiontherapyin
patients
with
follicularlymphom
a
Stud
yreference
Lineof
therapy
andno
.of
patients
Indu
ction
regimen
RMT
regimen
and
duration
ORR
CR
PFS
,EFS
,or
other
parameter
asindicateda
OS
GLLSG
Forstpointner
etal.[77]
R/R
(176,
including105FL
)
R-FCM
vsFC
Mb
Ronce
weeklyfor4weeks
at
3and6months
Inductionb:
95%
vs
71%c
Inductionb:
41%
vs
23%
RMT
vsOBSin
FL
patientswithR-FCM
inductiontherapy
DOR:NRvs
26monthsc
mOBS:
26months
–
EORTC
20981
vanOerset
al.
[71]
vanOerset
al.
[78]
R/R
(334)
R-CHOPvs
CHOP
Revery3months
(max.2
years)
Induction
(n=
465):
85%
vs
72%c
Induction
(n=
465):
30%
vs
16%c
RMT
vsOBS
PFS:
51.5
monthsvs
14.9
months
(HR0.40)c
mFU
:39.4
monthsand
6years
RMT
vsOBS
3-year:85.1%
vs77.1%
(HR0.52)c
5-year:74%
vs
65%
(HR0.70)
SAKK
35/98
Martinelli
etal.
[79]
R/R
(151
rand
omized)
RRat
0,2,
4,and
6monthsafterend
ofinductiontherapy
––
RMT
vsOBS
EFS:24
monthsvs
13monthsc
mFU
:9.5years
RMT
vsOBS
Patientsdied:
32%
vs46%
(HR0.63)
ECOG1496
Hochsteret
al.
[72]
1L(228)
CVP
Ronce
weeklyfor4weeks
every6months
(2years)
–Induction:
12%
Maintenance:
37%
RMT
vs
21%
OBS
RMT
vsOBS
3-year
PFS:
64%
vs
33%c
PFS:
4.3yearsvs
1.3
years(H
R0.4)
c
mFU
:3.7years
RMT
vsOBS
3-year:92%
vs
86%
(HR0.6)
2242 Adv Ther (2017) 34:2232–2273

Table2
continued
Stud
yreference
Lineof
therapy
andno
.of
patients
Indu
ction
regimen
RMT
regimen
and
duration
ORR
CR
PFS
,EFS
,or
other
parameter
asindicateda
OS
PRIM
A
Salleset
al.[73]
Salleset
al.
[74]
1L(1018,
including858
confi
rmed
FL)
R? chem
otherapy
(CVP,
CHOP,
orFC
M)d
Ronce
weeklyevery8
weeks
(2years)
–RMT
vsOBS
inall
patients
71.5%
vs
52.2%c
RMT
vsOBS,
all
patients
3-year
PFS:
74.9%
vs
57.6%
(HR0.55)c
6-year
PFS:
59.2%
vs
42.7%
(HR0.58)c
mFU
:36
and73
months
RMT
vsOBS
6-year:87.4%
vs88.7%
CHOPcyclophosphamide,vincristine,doxorubicin,
andprednisone,C
Rcompleteresponse,C
VPcyclophosphamide,vincristine,andprednisone,D
ORduration
ofresponse,ECOG
Eastern
Cooperative
OncologyGroup,EFS
event-free
survival,EORTC
EuropeanOrganisationforResearchandTreatmentof
Cancer,FC
Mfludarabine,cyclophospham
ide,andmitoxantrone,FL
follicularlymphom
a,GLLSG
German
Low
-Grade
Lym
phom
aStudyGroup,H
Rhazard
ratio,1L
firstlin
e,mFU
medianfollow-up,mOBSmedianobservation,NRnotreached,OBSobservation,ORRoverallresponserate,O
Soverallsurvival,PF
Sprogression-free
survival,
Rrituximab,R
MTrituximab
maintenance
therapy,R/R
relapsed/refractory
aMedianvalues
bResultof
initialrand
omized
comparison
ofR-FCM
versus
FCM
in68
FLpatients;allsubsequent
patients
received
R-FCM
induction
therapybefore
rand
omizationto
RMTor
OBS
cStatistically
significant
difference
dOnlypatientswitharesponse
toinductiontherapyandhaving
received
sixor
morecycles
ofR-CVPtherapy,or
four
ormorecycles
ofR-CHOPor
R-FCM
therapy(including
sixinfusionsof
R)wereeligibleforrand
omization
Adv Ther (2017) 34:2232–2273 2243

maintenance therapy and induction therapygroups (HR 0.75, P = 0.33). The place of ritux-imab therapy relative to watchful waiting in FLremains under discussion in the literature [83].
Rituximab in Diffuse Large B-CellLymphoma
Rituximab is currently approved in Europe andthe USA for previously untreated CD20? DLBCLin combination with CHOP or other anthracy-cline-based chemotherapy and is also includedin current treatment guidelines in combinationwith salvage chemotherapy for relapsed/refrac-tory disease [9, 22]. A phase II trial of R-CHOP asfirst-line treatment in patients with aggressiveNHL (67% with DLBCL) was the first study todemonstrate the feasibility and safety of R-CHOP in this population, with an ORR of 94%and 20 of 33 patients (61%) having a CR [84].
Two pivotal phase III randomized trialsestablished R-CHOP therapy as the standard ofcare for elderly patients with DLBCL [85, 86](Table 3). In a study conducted by the Grouped’Etude des Lymphomes de l’Adulte (GELA;LNH98-5), previously untreated elderly patients(aged 60–80 years) with DLBCL were randomizedto receive eight cycles of R-CHOP or CHOPtherapy [85]. Sixty percent of patients weredeemed to be poor risk, with age-adjusted IPIscores of 2 or 3. The CR rate was significantlyhigher in favor of R-CHOP (76% vs 63%;P = 0.005). The proportions of patients with EFS(disease progression or relapse, institution of newtreatment, or any-cause death) at 2 years (57% vs38%; HR 0.58, P\0.001) and OS at 2 years (70%vs 57%; HR 0.64, P = 0.007) also favored R-CHOP. In a second phase III study (ECOG 4494/US Intergroup study), DLBCL patients aged60 years or older were randomized to receive R-CHOP or CHOP, followed by a second random-ization for responding patients to rituximabmaintenance therapy or observation [86]. Theproportion of patients with failure-free survival(FFS; time from randomization to relapse, non-protocol treatment, or death) at 3 years was sig-nificantly higher with R-CHOP than with CHOP(53% vs 46%; HR 0.78, P = 0.04). In addition, the2-year FFS rate from the second randomization
was 76% for rituximab maintenance therapycompared with 61% for observation (P = 0.009).Subanalyses showed that rituximab maintenancetherapy significantly prolonged FFS after CHOPtherapy (HR 0.45, P = 0.0004) but not after R-CHOP therapy, thus implying that rituximabmaintenance therapy after rituximab-basedimmunochemotherapy does not provide addi-tional clinical benefit in patients aged 60 years orolder with DLBCL. No significant differences inOS were reported.
In terms of younger patients, the MabTheraInternational Trial (MInT) Group confirmed thebenefit of adding rituximab therapy to CHOPchemotherapy compared with CHOPchemotherapy alone (given for a total of sixcycles) in patients aged 18–60 years with previ-ously untreated, good-prognosis DLBCL[87, 88]. R-CHOP therapy was associated with asignificant increase in 3-year EFS rate (79% vs59%; P\0.0001), 3-year PFS rate (85% vs 68%;P\0.0001), and 3-year OS rate (93% vs 84%;P = 0.0001) compared with CHOP chemother-apy alone [87] (Table 3). In the R-CHOP andCHOP groups, patients considered to be at lowrisk (IPI score of 0 and no bulky disease) hadsignificantly longer EFS than those at higher risk(IPI score of 1, bulky disease, or both). Impor-tantly, subsequent follow-up reports from theGELA trial and MInT indicated that the benefi-cial effect of R-CHOP therapy over CHOPchemotherapy alone was sustained over thelonger term in both older patients (GELA trial,5-year OS rate 58% vs 45%, P = 0.007; 10-yearOS rate 44% vs 28%, P\0.0001) [89, 90] andyounger patients (MInT, 6-year OS rate 90% vs80%, P = 0.0004) [88]. Comparison of rituximabmaintenance therapy and observation only inthe randomized NHL-13 trial, which enrolled683 patients with DLBCL who had responded tofirst-line rituximab therapy plus CHOP-likechemotherapy, showed no difference in theprimary end point of EFS after a median fol-low-up of 45 months [91]; however, PFS wassignificantly improved in the maintenancetherapy arm relative to the observation arm.
Salvage chemotherapy may be an option forpatients with DLBCL that is refractory toinduction therapy or who subsequently relapseafter achieving a CR. As monotherapy,
2244 Adv Ther (2017) 34:2232–2273

Table3
Summaryof
keystudiesevaluating
rituximab-based
immun
ochemotherapy
inpatientswithpreviouslyun
treatedor
relapsed/refractorydiffuselargeB-cell
lymphom
a
Stud
yreference
Lineof
therapyand
no.of
patients
Treatmentregimen
ORR
CR
PFS
,EFS
,or
other
parameter
asindicateda
OS
1L:elderlypatients
GELA,
LNH98-5
study,phaseIII
Coiffier
etal.
[85]
1L(399),medianage
69years
R-CHOPvs
CHOP,8cycles
83%
vs
69%
76%
vs
63%b
2-year
EFS:57%
vs38%
(HR0.58)b
5-year
PFS:
54%
vs30%b
10-yearPF
S:37%
vs20%b
mFU
:24months,5years,NA
2-year:70%
vs
57%
(HR0.64)b
5-year:58%
vs
45%b
10-year:44%
vs
28%b
Feugieret
al.
[89]
Coiffier
etal.
[90]
ECOG
4494/C
ALGB
9793,p
hase
III
1L(546),medianage
69years(R-CHOP),
70years(C
HOP)
R-CHOPvs
CHOP,6–
8cyclesc
77%
vs
76%
–3-year
FFS:
53%
vs46%
(HR0.78)b
mFU
:NA
HR0.83,
95%
CI0.63–1
.09
Habermann
etal.[86]
1L:youn
gerpatients
MInT,phaseIII
1L(823),medianage
47years
R-CHOP(orR?
CHOP-like
chem
otherapy)vs
CHOP(or
CHOP-likechem
otherapy),6
cycles
–86%
vs
68%b
AtmFU
of34
months:
3-year
EFS:79%
vs59%b
3-year
PFS:
85%
vs68%b
AtmFU
of72
months:
6-year
EFS:74.3%
vs55.8%b
6-year
PFS:
80.2%
vs63.9%b
3-year:93%
vs
84%(atmFU
of
34months)b
6-year:90.1%
vs
80.0%
(atmFU
of72
months)b
Pfreun
dschuh
etal.[87]
Pfreun
dschuh
etal.[88]
Adv Ther (2017) 34:2232–2273 2245

Table3
continued
Stud
yreference
Lineof
therapyand
no.of
patients
Treatmentregimen
ORR
CR
PFS
,EFS
,or
other
parameter
asindicateda
OS
R/R PhaseIIIstudies
Gisselbrecht
etal.[94]
R/R
(396)
R-ICEvs
R-D
HAP
63.5%
vs
62.8%
36.5%
vs
39.3%
(including
CRu)
3-year
EFS:26%
vs35%
3-year
PFS:
31%
vs42%
mFU
:27
months
3-year:47%
vs
51%
Vellengaet
al.
[93]
R/R
(225,including
21
otheraN
HL)
R-(DHAP-VIM
-DHAP)
vs
DHAP-VIM
-DHAP;
ASC
T
75%
vs
54%b
2-year
PFS:
52%
vs31%b
mFU
:31
months
2-year:59%
vs
52%
PhaseII
studies
Jerm
annet
al.
[95]
R/R
(50,
including25
DLBCL,1
8TBCL,
7MCL)
R-EPO
CH
68%
28%
EFS:11.8
months(M
CL15
months,TBCL12.4
months,DLBCL9.7
months)
mFU
:33
months
17.9
months
Kew
alramani
etal.[96]
R/R
(36)
R-ICEvs
ICE(147
historical
controls)
?ASC
Tforresponders
78%
vs
71%
53%
vs
27%b
2-year
PFS:
54%
vs43%
(after
ASC
T)
mFU
:NA
2-year:67%
vs
56%
(after
ASC
T)
Mey
etal.[97]
R/R
(46)
R-D
HAP(23)
vsDHAP(23);
matched-pairanalysisof
datafrom
2phaseII
trials
74%
vs
74%
44%
vs
35%
PFS:
NRvs
13.0
months
2-year
PFS:
52%
vs50%
mFU
:NA
NRvs
31.3
months
2-year:57%
vs
52%
2246 Adv Ther (2017) 34:2232–2273

rituximab achieved promising response rates in54 patients, mostly with relapsed/refractoryDLBCL, in a phase II study [92]. Subsequently,rituximab was evaluated in combination with avariety of salvage chemotherapy regimens inphase II and phase III studies in this setting,including ifosfamide, carboplatin, and etopo-side (ICE), dexamethasone, cytosine arabi-noside, and cisplatin (DHAP), and etoposide,ifosfamide, and methotrexate (VIM) regimens(Table 3). In a randomized phase III study, theaddition of rituximab therapy to DHAP–VIM–DHAP therapy followed by autologousstem cell transplantation in 225 patients withrelapsed or refractory aggressive NHL resulted ina significant improvement in FFS and PFScompared with chemotherapy alone [93]. Thesecond randomized phase III trial, in 396patients, demonstrated similar efficacy resultsfor rituximab plus ICE and rituximab plusDHAP but did not include a chemotherapy-onlyarm; the study authors considered that neitherregimen offered any benefit over other ritux-imab-based regimens given before or afterautologous stem cell transplantation in previ-ous studies [94]. Other studies in this settingwere smaller in scale (50 or fewer patients) anddid not include control arms [95–98]; however,the findings from two of these studies suggestedpotential benefits from the addition of ritux-imab therapy to chemotherapy when comparedwith historical data [95, 96] (Table 3).
Rituximab in Chronic LymphocyticLeukemia
In Europe and the USA, intravenously adminis-tered rituximab is approved in combination withchemotherapy for the treatment of patients withpreviously untreated and relapsed/refractory CLL[11, 23, 29, 30]. Two large phase III randomizedstudies investigating the concurrent administra-tion of rituximab plus FC (R-FC) compared withFC alone were conducted in patients with CLL[99, 100] (Table 4). Both studies were initiated onthe basis of the findings of earlier phase I/IImonotherapy and combination chemotherapystudies [101–106]. In the CLL8 trial, R-FC wascompared with FC alone in patients with CLL
Table3
continued
Stud
yreference
Lineof
therapyand
no.of
patients
Treatmentregimen
ORR
CR
PFS
,EFS
,or
other
parameter
asindicateda
OS
Elstrom
etal.
[98]
R/R
(15,
including6
TBCL,9
DLBCL)
R-D
ICE?
BOR
60%
20%
PFS:
3months
mFU
:26
months
10months
aNHL
aggressive
non-Hodgkin
lymphom
a,ASC
Tautologous
stem
celltransplantation,
BOR
bortezom
ib,CALGB
CancerandLeukemia
Group
BCHOP
cyclophosphamide,
doxorubicin,
vincristine,
prednisone,CIconfi
denceinterval,CR
completeresponse,CRuun
confi
rmed
completeresponse,DHAP
dexam-
ethasone,cytarabine,andcisplatin,
DICEdexamethasone,ifosfam
ide,cisplatin,
andetoposide,DLBCLdiffuselargeB-celllym
phom
a,ECOGEastern
Cooperative
OncologyGroup,E
FSevent-free
survival,E
POCH
etoposide,prednisone,vincristine,cyclophospham
ide,anddoxorubicin,
FFSfailure-freesurvival,G
ELAGroupe
d’Etude
desLym
phom
esde
l’Adulte,HR
hazard
ratio,
ICE
ifosfam
ide,
carboplatin,
andetoposide,
1Lfirst-line,MCL
mantle
celllymphom
a,mFU
median
follow-up,
MInTMabThera
InternationalTrial,N
Anotavailable,NRnotreached,
ORRoverallresponse
rate,O
Soverallsurvival,P
FSprogression-free
survival,
Rrituximab,R
/Rrelapsed/refractory,TBCLtransformed
B-celllymphom
a,VIM
etoposide,ifo
sfam
ide,andmethotrexate
aMedianvalues
bStatistically
significant
difference
cPatientsun
derwentasecond
rand
omizationto
Rmaintenance
therapyor
observationifthey
achieved
aCRor
partialresponse
afterthefirstrand
omization
Adv Ther (2017) 34:2232–2273 2247

Table4
Summaryof
keystudiesevaluating
rituximab
combination
therapyin
patients
withpreviously
untreatedor
relapsed/refractorychroniclymphocytic
leukem
ia
Stud
yreference
Lineof
therapyandno
.of
patients
Treatmentregimen
ORR
CR
PFS
,EFS
,or
other
parameter
asindicateda
OS
PhaseIIIstudies
CLL8
1L(817),medianage
61/61years(R-FC/
FC)
R-FC
vsFC
,6cycles
90%
vs
80%b
44%
vs
22%b
mFU
:3.1years
PFS:
51.8
monthsvs
32.8
months(H
R0.56)b
3-year
PFS:
65%
vs45%b
mFU
:5.9years
PFS:
56.8
monthsvs
32.9
months(H
R0.59)b
5-year
PFS:
47%
vs26%b
3-year:87%
vs83%
(HR0.67)b
mFU
:5.9years
NRvs
86.0months
(HR0.68)b
Halleket
al.[99]
Fischeret
al.[107]
CLL10
1Lfit
(561),medianage
62/61years(R-FC/
BR)
R-FC
vsBR,6
cycles
95%
vs
96%
40%
vs
31%b
mFU
:37.1
months
PFS:
55.2
monthsvs
41.7
months(H
R1.643)
b
DOR:52.7
monthsvs
38.9
months(H
R1.657)
b
EFS:55.2
monthsvs
38.5
months(H
R1.626)
b
3-year:91%
vs92%
(HR1.034)
Eichh
orstet
al.[116]
REACH
Previouslytreated(552),
medianage63/62
years(R-FC/FC)
R-FC
vsFC
,6cycles
69.9%
vs
58.0%b
24.3%
vs
13.0%b
mFU
:25
months
PFS:
30.6
monthsvs
20.6
months(H
R0.65)b
NRvs
52months
(HR0.83)b
Robak
etal.[100]
PhaseII
studies
Keating
etal.[105]
1L(224),medianage58
years
R-FC,6
cycles
95%
70%
4-year
FFS:
69%
mFU
:2years.
Deathsin
8.9%
2248 Adv Ther (2017) 34:2232–2273

Table4
continued
Stud
yreference
Lineof
therapyandno
.of
patients
Treatmentregimen
ORR
CR
PFS
,EFS
,or
other
parameter
asindicateda
OS
Tam
etal.[110]
c1L
(300),medianage
57years
R-FC,6
cycles
95%
72%
mFU
:6years
TTP:
80months
6-year
FFS:
51%
6-year:77%
Wierdaet
al.[106]
R/R
(177),medianage
59years
R-FC,6
cycles
73%
25%
mFU
:28
months
TTP:
28months
mFU
:28
months
42months
Foon
etal.[111]
Foon
etal.[112]
1L(63),m
edianage
58years
R-FC
lite
94%
73%
PFS:
5.8years
5-year
PFS:
66.9%
NR
5-year:85.5%
GCLLSG
1L(117),medianage
64years
BR,6
cycles
88%
23%
mFU
:27
months
EFS:33.9
months
PFS:
33.8
months
mFU
:27
months.
90.5%
alive
Fischeret
al.[115]
CALGB9712
1L(104),medianage
63years
FRsequentiallyvs
FR
concurrently
84%
(allFR
patients)
–mFU
:117months
PFS:
42months
5-year
PFS:
28%
10-yearPF
S:13%
mFU
:117months
85months
5-year:71%
Woyachet
al.[113]
GCLLSG
R/R
(78),m
edianage
67year
BR,6
cycles
59%
9%mFU
:24
months
EFS:14.7
months
PFS:
15.2
months
mFU
:24
months
33.9
months
Fischeret
al.[114]
Adv Ther (2017) 34:2232–2273 2249

Table4
continued
Stud
yreference
Lineof
therapyandno
.of
patients
Treatmentregimen
ORR
CR
PFS
,EFS
,or
other
parameter
asindicateda
OS
Foaet
al.[117]
1L(97),m
edianage
70years
R-Clb
vsClb,6
cycles
(ind
uction);
responders
rand
omized
toR
orOBS
82.4%
(ind
uction)
55.9%
R
34.4%
OBS
16.5%
(ind
uction)
29.4
R
18.7%
OBS
3-year
PFS:
42.7%
3-year
EFS:38.2%
ForR:over
3-year
PFS48.6%
ForOBS:
over
3-year
PFS
31.8%
mFU
:34.2
months
(34.9monthsin
rand
omized
population)
NA
Hillmen
etal.[118]
1L(100),medianage
70years
R-Clb,6
cycles
(6
additionalcycles
in
nonrespond
ers)
84%
10%
MedianPF
S:23.5
months
mFU
:30
months
NR
BRbend
amustine
andrituximab,C
ALGBCancerandLeukemiaGroup
B,C
lbchlorambucil,CRcompleteresponse,D
ORduration
ofresponse,E
FSevent-free
survival,F
Cfludarabine
andcyclophosphamide,FF
Sfailure-freesurvival,F
Rfludarabine
andrituximab,G
CLLSG
German
ChronicLym
phocyticLeukemiaStudy
Group,H
Rhazard
ratio,1L
firstlin
e,mFU
medianfollow-up,NAnotavailable,NRnotreached,OBSobservation,
ORRoverallresponserate,O
Soverallsurvival,
PFSprogression-free
survival,R
rituximab,R
/Rrelapsed/refractory,TTPtimeto
progression
aMedianvalues
bStatistically
significant
difference
cSix-year
update
ofKeating
etal.[105]
withfin
alresults
forallstudypatients(n
=300)
2250 Adv Ther (2017) 34:2232–2273

who had not received any prior chemotherapy[99]. Median PFS was significantly prolonged (by19 months) with R-FC compared with FC (HR0.56, P\0.0001), with results favoring R-FC forall three Binet stage subgroups. A significantbenefit in favor of R-FC over FC was alsoobserved in terms of OS (HR 0.67, P = 0.012),and ORR and CR rate (P\0.0001) [99]. In anupdated analysis of the CLL8 trial, median PFSwith R-FC was almost twice as long as with FC(56.8 months vs 32.9 months; HR 0.59,P\0.001) and median OS was also significantlyprolonged (R-FC, not reached; FC, 86.0 months;HR 0.68, P = 0.001) [107]. In previously treatedpatients with CLL in the REACH study, R-FCtreatment was associated with a 10-monthimprovement in median PFS compared with FC(30.6 months vs 20.6 months; HR 0.65,P\0.001) [100]. Consistent with the CLL8study, improvements in PFS in the R-FC armwere also associated with significant increases inboth the ORR and the CR rate. On the basis ofthe findings from these studies, R-FC became afirst-choice treatment for patients with newlydiagnosed or relapsed CD20? CLL. Indeed, R-FCmay be able to affect a cure in a subset of CLLpatients with favorable genetic profiles: long-term follow-up of patients treated with R-FC inclinical trials has shown that those with mutatedIg heavy chain variable region gene status andwithout the 17p and 11q deletions achieve verylong remissions [107–109].
Data from other, mostly phase II studiesevaluating rituximab combination therapy inpatients with previously untreated andrelapsed/refractory CLL have also been pub-lished, and are summarized in Table 4. Thesedata are consistent with the results of the CLL8and REACH studies, and provide further con-firmation of the clinical efficacy of R-FC in CLL[105, 106, 110–113]. Promising results have alsobeen reported with the combination of ritux-imab and bendamustine in a phase II studyinvolving patients with both previouslyuntreated and relapsed/refractory CLL[114, 115]. However, recently published datafrom the phase III CLL10 trial in 564 previouslyuntreated, fit CLL patients showed that ritux-imab plus bendamustine was associated withsignificantly shorter PFS than R-FC (median
41.7 months vs 55.2 months; HR 1.64,P = 0.0003) [116]. Although there was a cleardifference in PFS between the two study treat-ments in the overall patient population, sub-group analyses showed that the PFS benefit inthe R-FC arm was significant only in youngerpatients (65 years or younger). Additionally, thetolerability (notably the incidence of severeinfections) was better with rituximab plus ben-damustine, particularly among patients olderthan 65 years. Taken together, these findingssuggest that although R-FC may be the moreeffective regimen overall, rituximab plus ben-damustine may have a role in the treatment offit, older patients with CLL.
Another widely used treatment option forless fit patients with CLL is rituximab pluschlorambucil. In two phase II studies in previ-ously untreated patients who received thecombination (n = 85 and 100), adverse event(AE) profiles were favorable, and ORRs of up to84% were achieved, with CR rates of 17% and10% [117, 118].
The potential benefit of rituximab mainte-nance therapy in CLL has also been explored ina small number of studies, with some encour-aging results [119–121]. In a phase II study inpreviously untreated CLL patients, for example,4-year PFS and OS rates were 74.8% and 93.7%,respectively, in 67 patients who received ritux-imab maintenance therapy after responding toR-FCM induction therapy, compared with69.1% and 90.5%, respectively, for the patientpopulation overall (n = 81; treated with R-FCMas induction therapy with or without rituximabmaintenance therapy) [120]. Results from therandomized CLL 2007 SA trial of 2 years ofrituximab maintenance therapy versus obser-vation following induction therapy with fourcycles of R-FC therapy in patients aged 65 yearsor older included a significant improvement inmedian PFS (59.3 months vs 49.0 months; HR0.60, P = 0.001). Rituximab maintenance ther-apy also improved PFS in patients with geneticmarkers indicative of poorer prognosis,although no difference in 3-year OS was seen,and maintenance treatment was associated witha greater incidence of AEs [121]. In addition,studies are ongoing to determine the efficacyand safety of rituximab in combination with
Adv Ther (2017) 34:2232–2273 2251

newer agents such as inhibitors of Bruton’styrosine kinase and phosphoinositide 3-kinase,as well as inhibitors of the mechanistic target ofrapamycin, and BCL2 inhibitors [122–125].However, approval of these new drugs could bemany years away in many countries, and inthose with more limited healthcare budgets, thecost of these agents is likely to be prohibitive;for this reason, immunochemotherapy withrituximab combined with FC, bendamustine, orchlorambucil will continue to be a mainstay ofpatient treatment.
Other B-Cell Malignancies
Encouraging results have also been reported infour studies of rituximab in other B-cell malig-nancies for which use of the drug is not yetlicensed.
In the final report of the randomizedIELSG-19 study in 454 patients with extranodalmarginal-zone B-cell lymphoma, a combinationof rituximab and chlorambucil was associatedwith significantly longer EFS and PFS thanchlorambucil or rituximab alone after a medianfollow-up of 7.4 years [126]. In a randomizedphase III trial of 52 nonfollicular indolent NHLpatients with low tumor burden who respondedto rituximab induction therapy, those whoreceived 3-monthly rituximab maintenancetherapy had a 3.5-fold longer time to treatmentfailure than those who received retreatment atthe time of progression [127]. In two other trialsthat assessed the addition of rituximab therapyto chemotherapy in highly aggressive lymphoidmalignancies, significant increases in EFS rela-tive to chemotherapy alone were seen in 209patients with CD20?, Philadelphia chromo-some-negative acute lymphoblastic leukemiaafter a median follow-up of 30 months [128],and in 260 patients with previously untreatedBurkitt lymphoma after a median follow-up of38 months [129].
Rituximab has also been shown to improveOS in older patients with MCL, both in thefirst-line setting when added to inductionchemotherapy and when used as maintenancetherapy after rituximab therapy pluschemotherapy as induction therapy [130, 131].
Additional B-cell malignancies in which ritux-imab treatment has been associated with posi-tive outcomes in phase II and phase III clinicaltrials include Waldenstrom macroglobulinemia,posttransplant lymphoproliferative disorders,and Hodgkin lymphoma [132–134]. Rituximabis not yet licensed for use in any of thesediseases.
Development of Resistance to Rituximab
Although the efficacy of rituximab for thetreatment of B-cell hematologic malignancies iswell established, some patients do not respondto first-line treatment, and others experiencerelapse after initial response to therapy[54, 135].
Despite many years of study, the exactmechanisms underlying the development ofresistance to rituximab remain unclear. How-ever, given the reliance of rituximab onimmune-effector mechanisms for its antitumorefficacy, it has been hypothesized that intrinsictumor cell alterations and the host immuno-logic environment may both play a role. Thereare many postulated in vivo mechanisms ofresistance, and these are described in detailelsewhere [136, 137]. In brief, they includeinhibition of three of the pathways that areinvolved in the mechanism of action of ritux-imab; namely, CDC, ADCC, and apoptosis.Complement depletion, through exhaustion ofthe store of complement proteins, has beenimplicated in the development of resistance torituximab-mediated CDC. Furthermore, hostimmunologic factors, such as polymorphism ofFcc receptor IIIa on cytotoxic cells, may affectthe sensitivity of tumor cells to ADCC, whereasalterations in apoptotic pathway signaling,through overexpression of antiapoptotic geneproducts, may facilitate the development ofapoptosis resistance in the presence of ritux-imab [136, 137]. Another possible mechanismof rituximab resistance is loss of the CD20 targetantigen, which has been demonstrated in lym-phoma cell lines and in biopsy samples fromrelapsed patients [138, 139]. This phenomenonmay occur in several ways, including decreasedexpression at both the pretranslational level
2252 Adv Ther (2017) 34:2232–2273

and the posttranslational level, antigenic mod-ulation (whereby CD20 antibody–antigencomplexes are internalized following rituximabbinding), or the acquisition of CD20 mutations.Removal of rituximab/CD20 complexes fromthe B-cell surface by monocytes in a processcalled ‘‘trogocytosis’’ or ‘‘CD20 shaving’’ has alsobeen reported [140]. In addition, generation ofrituximab-resistant clones, the tumor microen-vironment, and the PK profile of rituximab mayalso have a role in the development of ritux-imab resistance [136, 137].
Patients treated with rituximab may developan antibody against rituximab, termed ‘‘humanantichimeric antibody.’’ These patients have thepotential to mount allergic reactions whensubsequently treated with other antibodies. Todate, immune responses against rituximab havebeen much more common in patients treatedfor rheumatoid arthritis than in those withother diseases. During clinical trials in patientswith B-cell malignancies, up to 2% of patientsdeveloped human antichimeric antibody, butno effect of this antibody on the efficacy orsafety of rituximab has been demonstrated[29, 30].
Various strategies are being investigated toovercome rituximab resistance. One suchapproach is the use of adjuncts to inhibithyperactivated survival/antiapoptotic path-ways, which regulate downstream antiapoptoticgene products. Possible candidates include his-tone deacetylase inhibitors, targeted chemicalinhibitors, proteasome inhibitors, selectiveinhibitors for antiapoptotic gene products, andmicroRNAs [137]. The combination of ritux-imab and lenalidomide, an immunomodulatorydrug that has been shown to enhance ADCC inin vitro and in vivo leukemia models, hasdemonstrated efficacy in patients with indolentB-cell lymphomas, DLBCL, and CLL who wererituximab resistant or had previously relapsedfollowing rituximab therapy [141–144].Another important avenue of research tocounter rituximab resistance is the develop-ment of novel, next-generation anti-CD20mAbs with different mechanisms of action. Thisapproach is exemplified by obinutuzumab, asecond-generation type II anti-CD20 mAb,which has recently been approved in
combination with bendamustine followed bysingle-agent maintenance therapy for thetreatment of patients with FL who do notrespond to or whose disease progresses aftertreatment with rituximab or a rituximab-con-taining regimen [145].
SAFETY AND TOLERABILITYOF RITUXIMAB IN PATIENTSWITH HEMATOLOGICMALIGNANCIES
Overview of the Safety Profile
With 20 years of postmarketing surveillanceexperience and more than four million patientexposures, the safety profile of rituximab, bothas monotherapy (induction and/or mainte-nance) and in combination with chemother-apy, in the treatment of patients with B-cellhematologic malignancies is very well defined.Furthermore, in the two decades since the reg-ulatory approval of rituximab, no new orunexpected safety signals have been identified,thus confirming a favorable therapeuticwindow.
From clinical trial and postmarketingsurveillance data from patients with NHL andCLL, infusion-related reactions (IRRs) wereidentified as the most common adverse drugreactions (ADRs) in patients treated with ritux-imab as monotherapy or combination therapy[29, 30]. In those studies, IRRs of any grade andtype, including cytokine-release syndrome,were observed in 77% of patients. Severe IRRs(grade 3 or 4), including bronchospasm andhypotension, were reported in 12% of patients[29]. Although rare, fatal reactions have occur-red within 24 h of drug infusion (most com-monly with the first infusion), and it istherefore recommended that patients be closelymonitored, and treatment be stopped if there isa severe reaction [30]. Most IRRs occurred dur-ing the first rituximab infusion (in the first1–2 h), and the frequency of reactions typicallydecreased with subsequent infusions, to lessthan 1% after eight doses of rituximab [29, 30].Now that physicians have more experience of
Adv Ther (2017) 34:2232–2273 2253

rituximab administration, the management ofIRRs has improved, for example, by use ofslower infusion rates and by premedication(described later), and IRRs now occur less fre-quently than during the registration trials.
In addition to IRRs, other common AEsreported in patients treated with rituximabinclude infections, hematologic AEs, and car-diovascular events. Infections (bacterial andviral) were reported in approximately 30–55%of patients with NHL and in about 30–50% ofpatients with CLL in clinical trials. Grade 3/4infections occurred in approximately 4% ofpatients treated with rituximab as monotherapyin randomized studies, and were more commonwith rituximab maintenance therapy than withobservation [29, 30]. Documented infections inrituximab-treated patients included localizedCandida infections, herpes zoster, and cytome-galovirus infections. Rarely, cases of fatal pro-gressive multifocal leukoencephalopathy andsevere mucocutaneous reactions, some of whichwere fatal, have occurred [30]. Hepatitis B reac-tivation has also been reported, mainly inpatients receiving rituximab plus chemother-apy, with outcomes of fulminant hepatitis,hepatic failure, and death in some cases [30].Among patients with relapsed/refractory CLL,grade 3/4 hepatitis B (reactivation and primaryinfection) was reported in 2% of patients treatedwith R-FC compared with 0% of patients treatedwith FC [29].
Generally mild and reversible cytopenias,including neutropenia, leukopenia, andthrombocytopenia, were reported during treat-ment with rituximab as monotherapy for4 weeks in clinical trials, and grade 3/4 eventswere relatively uncommon, occurring in 4.2%(neutropenia), 1.1% (anemia), and 1.7%(thrombocytopenia) of patients [29]. Comparedwith observation, patients treated with ritux-imab as maintenance therapy for up to 2 yearsexperienced a higher incidence of grade 3/4leukopenia (5% vs 2%) and neutropenia (10% vs4%) but a similar low incidence of thrombocy-topenia (both less than 1%). In clinical studiesin NHL and CLL, rituximab therapy pluschemotherapy (CHOP, FC, or CVP) was gener-ally associated with a higher incidence of grade3/4 leukopenia, neutropenia, and pancytopenia
compared with chemotherapy alone [29, 30];however, despite the increased incidence ofneutropenia, patients treated with rituximabplus chemotherapy were not at higher risk ofdeveloping infections compared with patientstreated with chemotherapy alone [29]. In stud-ies in previously untreated and relapsed/refrac-tory CLL, prolonged neutropenia (resolvingbetween 24 and 42 days after the last dose) orlate-onset neutropenia (resolving later than42 days after the last dose) was reported morefrequently in those receiving R-FC than in thosereceiving FC alone (up to 25% of R-FC patients)[29, 30].
Cardiovascular events were reported in up to25% of patients receiving rituximabmonotherapy in clinical trials, most commonlyhypotension and hypertension [29, 30]. Somecases of grade 3/4 arrhythmias and angina pec-toris were also reported during infusion ofrituximab. In the maintenance setting, cardiacdisorders were reported as serious AEs in 3% ofrituximab-treated patients and in less than 1%of untreated patients [29]. In studies evaluatingrituximab in combination with chemotherapy,R-CHOP was associated with a higher incidenceof grade 3/4 cardiac arrhythmias (mainlytachycardia and atrial flutter/fibrillation) com-pared with CHOP [29, 30]; however, there wasno difference between R-CHOP and CHOP interms of the incidence of other grade 3/4 cardiacevents, including heart failure, myocardial dis-ease, and manifestations of coronary arterydisease [29].
Other common AEs reported with rituximabtherapy include respiratory system disorders(e.g., dyspnea, cough, and chest pain), gas-trointestinal disorders (e.g., nausea, vomiting,and diarrhea), skin and suncutaneous tissuedisorders (e.g., pruritus, rash, and urticaria),metabolic disorders (e.g., angioedema andhyperglycemia), and nervous system disorders(e.g., paresthesia, hypoesthesia, and agitation)[29, 30]. In addition, IgG levels are frequentlyreduced among rituximab-treated patients, withlevels below the lower limit of normal reportedin approximately 60% of patients with FLreceiving rituximab maintenance therapy for2 years (vs 36% in the observation group) [29].
2254 Adv Ther (2017) 34:2232–2273

Safety in Patient Subpopulations
In the current summary of product characteris-tics for rituximab, brief reference is made to thetolerability profile of rituximab monotherapy inspecific patient subpopulations with NHL,including older patients (65 years or older),patients with bulky disease, and patientsundergoing retreatment [29]. In older patients,the incidence of ADRs (all grades) and grade 3/4ADRs is generally similar to that seen inyounger patients (younger than 65 years).However, in patients with previously untreatedor relapsed/refractory CLL treated with ritux-imab plus chemotherapy, the incidence andseverity of grade 3/4 hematologic AEs and bac-terial infections was found to be higher inpatients aged 70 years or older than in youngerpatients [30]. In the monotherapy setting,patients with bulky B-cell lymphomas experi-enced a higher incidence of grade 3/4 ADRsthan those with nonbulky disease (25.6% vs15.4%), although the incidence of ADRs of anygrade was generally similar in the two groups[29]. Retreating patients with further courses ofrituximab monotherapy does not appear toaffect the drug’s tolerability profile, with theproportion of patients experiencing ADRs dur-ing later treatment courses being similar to thatduring initial exposure (both for grade 3/4 ADRsand for ADRs of any grade) [29]. Information onthe safety profile of rituximab in children andadolescents is currently scarce, but a random-ized phase III trial that is assessing the additionof rituximab therapy to chemotherapy in thissubpopulation [146] will help to address thisissue.
Management and Prevention Strategiesfor Rituximab-Associated Adverse Events
Current rituximab patient information providesdetails of management and prevention strate-gies for rituximab-associated AEs [29, 30]. Beforeinfusion of rituximab, all patients shouldreceive premedication, comprising an antihis-tamine and acetaminophen (paracetamol), tominimize the occurrence of cytokine-mediatedreactions (flushing, low blood pressure, etc.). In
patients with CLL, adequate hydration andadministration of uricostatics starting 48 hbefore infusion of rituximab is recommended toreduce the risk of tumor lysis syndrome. Pred-nisone (100 mg intravenously) should also beadministered shortly before rituximab infusionto decrease the rate and severity of acute infu-sion reactions and/or cytokine-release syn-drome; European prescribing informationrecommends this for CLL patients with lym-phocyte counts greater than 25 9 109/L [29].
In the event of mild-to-moderate IRRs, theinfusion rate should be decreased and thenincreased on symptom abatement. Somephysicians use a more rapid infusion (90-minduration) for all infusions after the first dose,and this dosing option is approved in the USA.All patients should undergo screening for hep-atitis B, including assessment of hepatitis Bsurface antigen and hepatitis B core antibodystatus, before treatment with rituximab becauseof the possible risk of reactivation of the disease.Consideration should also be given to with-holding antihypertensive medicines 12 h beforerituximab infusion because of the risk ofhypotension.
PHARMACOECONOMICCONSIDERATIONS
Numerous pharmacoeconomic analyses ofrituximab have been conducted in the last20 years that show rituximab is a cost-effectiveoption compared with reference interventionsfor the treatment of B-cell hematologic malig-nancies, with the incremental cost-effectivenessratios consistently at or below national will-ingness-to-pay thresholds. Table 5 presents asummary of the key findings from analysespublished between 2010 and 2016, specificallyevaluating the cost-effectiveness of intra-venously administered rituximab for the treat-ment of FL [147–154], DLBCL [155–157], andCLL [158–161]. These studies were performed ina variety of countries (including several Euro-pean countries, the USA, Canada, and Australia)from either a payer perspective or a societalperspective. Most of the analyses used Markovmodels that incorporated outcomes data from
Adv Ther (2017) 34:2232–2273 2255

Table5
Summaryof
results
from
pharmacoeconomicanalyses
publishedbetween2010
and2016
evaluating
thecost-effectivenessof
intravenously
administered
rituximab
forthetreatm
entof
B-cellhematologicmalignancies
Stud
yreference
Setting
Cou
ntry,
year
ofcosting,
and
perspective
Metho
dology/datasources
Costs
includ
edCost-effectiveness
Follicularlymphom
a
Deconinck
etal.[147]
R/R
,RMT,o
rOBSafter
inductiontherapy
(R-CHOPor
CHOP)
France
(2006,
national
healthcare
system
perspective)
Markovmodel
PFSandOSdata
from
EORTC
20981,
French
officialcost
data,literature,expertopinion
Direct:drug
acquisition,
drug
administration,
treatm
ent
ofAEs,FU
visits(clin
ical
exam
ination,
diagnostics),
investigations,radiotherapy,
routinepatientmanagem
ent
RMT
vsOBS
€71,314vs
€62,251
(lifetimecosts)
ICER/LYG:€7612
ICER/Q
ALYgained:
€8729
Ray
etal.
[148]
1L,R
?chem
otherapy
(MCP,
CVP,
CHOP,
orCHVP)
vs
chem
otherapy
UK
(2008,
national
healthcare
system
perspective)
Markovmodel
Event
rate
data
from
four
phase
IIIclinicaltrials,
lifetabledata,
NationalHealth
Service
references
andpublished
literature
Direct:drug
acquisition,
drug
administration,
routine
patientmanagem
entand
surveillance
R?
chem
otherapy
vs
chem
otherapy
£28,582to
£33,513vs
£20,708to
£29,621
(lifetimecosts)
ICER/LYG:£6503
(R-M
CP),£
7473
(R-CVP),£
9294
(R-CHOP),£
7370
(R-CHVP)
ICER/Q
ALYgained:
£7455(R-M
CP),£
8613
(R-CVP),£
10,676
(R-CHOP),£
8498
(R-CHVP)
2256 Adv Ther (2017) 34:2232–2273

Table5
continued
Stud
yreference
Setting
Cou
ntry,
year
ofcosting,
and
perspective
Metho
dology/datasources
Costs
includ
edCost-effectiveness
Soiniet
al.
[149]
R/R
,R-CHOP(ind
uction),
R-CHOP-R
(ind
uction
?maintenance),
orCHOP
Finland
(2008,
national
healthcare
system
perspective)
Markovmodel
PFSandOSdata
from
EORTC
20981,
officialdrug
cost
listings,Finn
ish
case-m
ix-adjustednationalun
it
costsforhealthcare
resources
Direct:drug
acquisition,
drug
administration(including
traveling),relapse
managem
ent,routine
treatm
ent,treatm
entof
AEs
R-CHOPvs
R-CHOP-R
vsCHOP
€59,521vs
€68,331vs
€49,562(lifetimecosts)
ICER/LYG:R-CHOP-R
vsR-CHOP€16,380;
R-CHOP-Rvs
CHOP
€13,041;
R-CHOPvs
CHOP€11,049
ICER/Q
ALYgained:
R-CHOP-R
vsR-CHOP
€18,147;
R-CHOP-Rvs
CHOP€14,360;
RCHOPvs
CHOP
€12,123
Griffithsetal.
[150]
1L(elderly)
R?
chem
otherapy
(CVP,
CHOP)
vschem
otherapy
(CVP,
CHOP)
USA
(2009,
Medicare
perspective)
Observationalcohort
SEERregistry
data,M
edicare
claimsdata
Direct:drug
acquisition,cancer
care,noncancercare(alltotal
direct
coststo
Medicare)
R?
chem
otherapy
vs
chem
otherapy
Increm
entaltotalcost:
$18,695(costsover
4
years)
ICER/LYG:€102,142
Adv Ther (2017) 34:2232–2273 2257

Table5
continued
Stud
yreference
Setting
Cou
ntry,
year
ofcosting,
and
perspective
Metho
dology/datasources
Costs
includ
edCost-effectiveness
Hornberger
etal.[151]
RMT
orOBS(after
1LR?
chem
otherapy)
USA
(NA,
payer
perspective)
Markovmodel
Event
rate
data
from
PRIM
A
andEORTC
20981,
Centers
forDisease
Control
and
Prevention
data,C
entersfor
MedicareandMedicaid
Services
data,p
ublished
literature
Direct:drug
acquisition,
drug
administration,
managem
ent
ofAEs,outpatient
monitoring,postprogression
care
RMT
vsOBS
$183,963
vs$145,418
(lifetimecosts)
ICER/LYG:$31,934
ICER/Q
ALYgained:
$34,842
Blommestein
etal.[152]
R/R
,RMT
vsOBS(3
scenarios:trial
efficacy?
costs,trial
efficacy?
matched
real-world
costs,real-world
efficacy?
costs)
Netherlands
(2012,
healthcare
system
perspective)
Markovmodel
PFSandOSdata
from
EORTC
20981,
population-based
registries,N
etherlands
Cancer
Registry,literature,national
referencelistfordrug
prices
Direct:drug
acquisition,
hospitalinpatientdays,d
ay
treatm
ent,outpatient
days,
AEs,postprogressioncare
RMT
vsOBS
Trialefficacy?
costs
€17,425,
trial
efficacy?
real-world
costs€32,668,
real-world
efficacy?
costs€23,736
(lifetimeincrem
ental
costs)
ICER/LYG:trial
efficacy?
costs€11,259,
trialefficacy?
real-world
costs€21,202,
real-world
efficacy?
costs€10,591
ICER/Q
ALYgained:trial
efficacy?
costs€12,655,
trialefficacy?
real-world
costs€23,821,
real-world
efficacy?
costs€11,245
2258 Adv Ther (2017) 34:2232–2273

Table5
continued
Stud
yreference
Setting
Cou
ntry,
year
ofcosting,
and
perspective
Metho
dology/datasources
Costs
includ
edCost-effectiveness
Chenet
al.
[153]
1L,R
MT
vsOBS
USA
(2013,
payer
perspective)
Markovmodels
PFSandOSdata
from
PRIM
A
andECOG
1496,literature,
Medicarephysicianfee
schedule,C
entersforMedicare
andMedicaidServices
database,life
tabledata,expert
opinion
Direct:drug
acquisition,
drug
administration,
monitoring,
bloodtests,CTscans,AEs,
hospitalization
RMT
vsOBSlifetim
e
costs:PR
IMA
$112,781
vs$68,856;
ECOG
1496
$124,406
vs$72,066
ICER/LYG:PR
IMA
$39,968;
ECOG
1496
$37,627
ICER/Q
ALYgained:
PRIM
A$40,335;
ECOG
1496
$37,412
Pricaet
al.
[154]
1L,R
IT?
RMT
vsRIT
(only)
vsWW
Canada
(2012,
payer
perspective)
Markovmodel
Survival,responseandQOL
data
from
clinicaltrials,
cost
data
from
publishedliterature
anddatabases,Statistics
Canadalifetables
Direct:drug
acquisition,
cost
ofpatientFU
,physician,
nursing,pharmacy
laboratory,and
radiology
services,A
Es,salvage
chem
otherapy,p
alliative
care
RIT
?RMT
vsRIT
vs
WW
$67,489vs
$59,953vs
$75,895(costsover
30
years)
ICER/Q
ALYgained:
$62,360(RMT
vsRIT)
Adv Ther (2017) 34:2232–2273 2259

Table5
continued
Stud
yreference
Setting
Cou
ntry,
year
ofcosting,
and
perspective
Metho
dology/datasources
Costs
includ
edCost-effectiveness
DiffuselargeB-celllymphom
a
John
ston
etal.[155]
1L,R
-CHOPvs
CHOP
Canada
(2006,NA)
Observationalcohort
BCCA
Lym
phoidCancer
Database,BCCA
Provincial
System
icTherapy
Drug
Database,literature
Direct:drug
acquisition,
radiotherapy,p
alliative
care,
assessment,hospitalization,
outpatient
care,stem
cell
transplantation
R-CHOPvs
CHOP
$46,337vs
$36,765(age
\60
years);$42,892vs
$34,968(age
C60
years)
(costsover
15years)
ICER/D
F-LYG:$11,965
(age\60
years),$
4313
(age
C60
years)
ICER/Q
ALYgained:
$19,144(age\60
years),
$5853(age
C60
years)
Griffithsetal.
[156]
1L,R
?chem
otherapy
vs
chem
otherapy
(elderly)
USA
(2009,
payer
perspective)
Observationalcohort
SEERregistry,M
edicareclaims
Direct:im
mun
ochemotherapy,
othercancer
andnoncancer
costs(not
specified)
R-CHOPvs
CHOP
Meancostdifference
over4
years$23,097
ICER/LYG:$62,424
2260 Adv Ther (2017) 34:2232–2273

Table5
continued
Stud
yreference
Setting
Cou
ntry,
year
ofcosting,
and
perspective
Metho
dology/datasources
Costs
includ
edCost-effectiveness
Khoret
al.
[157]
1L,R
-CHOPvs
CHOP
Canada
(2009,
healthcare
system
perspective)
Observationalcohort
Population-based
administrative
healthcare
databases,
cancer-specific
databases,
health
insuranceplan
databases
forcosts
Direct:drug
acquisition,
hospitalization,
laboratory
tests,im
agingservices,
emergencydepartmentvisits,
homecareservices,
rehabilitation,
palliativecare
R-CHOPvs
CHOP
$85,293vs
$68,995(costs
over
5years)
ICER/LYG:$61,984(all
patients),$31,789(age
\60
years),$
80,601
(age
60–7
9years),$
110,071
(age
C80
years)
Chroniclymphocyticleukem
ia
Hornberger
etal.[158]
1L,R
-FC
vsFC
USA
(NA,
payerand
societal
perspective)
Markovmodel
Event
rate
data
from
CLL8,
generalUSpopulation
data,
CentersforMedicareand
MedicaidServices
reim
bursem
entdata,literature
Direct:drug
acquisition,
drug
administration,
AEs,salvage
therapy
Indirect:caregivercosts,lost
workproductivity
R-FC
vsFC
Payerperspective
$110,267
vs$83,240
(lifetimecosts)
ICER/LYG:$12,558
ICER/Q
ALY:$23,530
Societalperspective
$205,147
vs$172,565
(lifetimecosts)
ICER/LYG:$15,140
ICER/Q
ALY:$31,513
Adv Ther (2017) 34:2232–2273 2261

Table5
continued
Stud
yreference
Setting
Cou
ntry,
year
ofcosting,
and
perspective
Metho
dology/datasources
Costs
includ
edCost-effectiveness
Adena
etal.
[159]
1LandR/R
,R-FC
vsFC
Australia
(2009,
healthcare
perspective)
Markovmodel
Event
rate
data
from
CLL8and
REACH,treatmentguidelines,
expertopinion,
literature,
Australianprescription
data
Direct:drug
acquisition,
administration,
AEs,routine
monitoring
R-FC
vsFC
$62,365vs
$22,097(costs
over
15years)
ICER/LYG:$36,387
ICER/Q
ALYgained:
$42,906
Mandrik
etal.[160]
1LandR/R
,R-FC
vsFC
Ukraine
(2014,
healthcare
system
perspective)
Markovmodel
Event
rate
data
from
CLL8and
REACH,literature,clinical
guidelines,u
tilitydata
(UK),
resource
utilization/costs
(Ukraine)
Impact
oflower
lifeexpectancy
inUkraine
(1Lonly)also
assessed
Direct:drug
costs,
hospitalization,
AEs,salvage
therapycosts
R-FC
vsFC
ICER/Q
ALYgained:
US$8704
(1L),
US$11,056
(R/R
),
US$13,000
(based
on
higher
mortalityof
Ukrainian
population)
2262 Adv Ther (2017) 34:2232–2273

Table5
continued
Stud
yreference
Setting
Cou
ntry,
year
ofcosting,
and
perspective
Metho
dology/datasources
Costs
includ
edCost-effectiveness
Mulleret
al.
[161]
1L,R
-FC
vsFC
Germany
(2014,
payer
perspective)
Markovmodel
Event
rate
data
from
CLL8,
treatm
entguidelines,h
ospital/
hematologicpractice
patterns,
physicians,fee
scalewithin
statutoryhealth
insurance
scheme,German
pharmacy
referencesources
Direct:drug
acquisition,
drug
administration,
AEs(FU
visits,tum
orassessments,
routinemanagem
ent
excluded)
R-FC
vsFC
€28,384vs
€8118(costs
over
5.9years)
ICER/LYG:€15,773
ICER/Q
ALYgained:
€17,979
AE
adverseevent,BCCA
British
Colum
biaCancerAgency,
CHOPcyclophosphamide,
doxorubicin,
vincristine,
andprednisolone,CHVPcyclophosphamide,
doxorubicin,
etoposide,andprednisone,C
Tcomputedtomography,CVPcyclophosphamide,vincristine,andprednisolone,D
F-LYG
disease-free
lifeyear
gained,
EORTCEuropeanOrganisationforResearchandTreatmentof
Cancer,FC
fludarabine
andcyclophosphamide,FU
follow-up,ICERincrem
entalcost-effectiveness
ratio,
1Lfirst
line,
LYG
lifeyear
gained,MCPmitoxantrone,
chlorambucil,andprednisolone,NA
notavailable,
OBSobservation,
OSoverallsurvival,PF
Sprogression-free
survival,Q
ALYquality-adjusted
lifeyear,Q
OLqualityof
life,Rrituximab,R
ITrituximab
inductiontherapy,RMTrituximab
maintenance
therapy,
R/R
relapsed/refractory,SE
ERSurveillance,Epidemiology,and
End
ResultsWW
watchfulwaiting
Adv Ther (2017) 34:2232–2273 2263

clinical trials, and a small number were basedon real-life data from large observationalcohorts.
In FL, rituximab was shown to be cost-ef-fective both as maintenance therapy comparedwith observation in the first-line [151, 153] andrelapsed/refractory [147, 149, 152] settings andas induction therapy combined withchemotherapy compared with chemotherapyalone in previously untreated patients[148, 150]. In DLBCL, rituximab therapy pluschemotherapy was generally found to becost-effective compared with chemotherapyalone when administered as first-line treatment[155, 157], although results were conflicting asto whether cost-effectiveness increased ordecreased with increasing age [155, 157]. In oneanalysis based on data from a large observa-tional cohort of DLBCL patients in the USA,previously reported cost savings associated withrituximab-related survival benefits in clinicaltrials were not realized; according to the studyauthors, this finding was consistent with anongoing accrual of medical costs associatedwith multiple comorbidities among elderlycancer survivors treated with rituximab [156].Cost-effectiveness analyses of rituximab in CLLevaluated rituximab therapy plus chemother-apy versus chemotherapy alone in patients withpreviously untreated and relapsed/refractorydisease [158–161]. In both settings, rituximabtherapy plus chemotherapy was consideredcost-effective, although in the Ukraine this wasconsidered applicable only under conditions ofeconomic stability, cost-effectiveness thresholdgrowth, or with rituximab price negotiations[160]. In an analysis that evaluated the eco-nomic benefit of adding rituximab therapy toFC chemotherapy in CLL in the USA, R-FC wasfound to be cost-effective from both a payer anda societal perspective [158].
A population analysis of the benefits andcosts of rituximab in patients with FL, DLBCL,and CLL in the USA over a 15-year period basedon cancer registry data found that almost280,000 cumulative life years were saved bycombining rituximab therapy with chemother-apy, corresponding to a net economic gain of$16.5 billion, when treatment costs were takeninto account [162].
CONCLUSION
Since its first approval 20 years ago, theanti-CD20 mAb rituximab has changed thetreatment landscape for patients with B-cellhematologic malignancies and established anew standard of care. By prolonging survival ina range of these diseases, rituximab has reducedmortality and improved the clinical prognosisfor many patients with B-cell malignancies.Extensive clinical data from the last two decadeshave confirmed the efficacy of rituximab andallowed its tolerability profile to be clearlydefined. On the basis of this evidence, ritux-imab is now incorporated routinely into treat-ment regimens for FL, DLBCL, CLL, and MCL: itis designated as a recommended treatment incurrent clinical practice guidelines for B-cellhematologic malignancies developed by theEuropean Society of Medical Oncology and theUS National Comprehensive Cancer Network[9–11, 22, 23], and is included in the WHOModel List of Essential Medicines [24]. Theexperience with rituximab has confirmed thevalue of the CD20 protein as an importantmechanistic target in the search for new lym-phoma treatments. Advances in the design ofanti-CD20 antibodies have resulted in thedevelopment of new therapies for the treatmentof B-cell hematologic malignancies, such asobinutuzumab, which has shown benefit for thetreatment of FL, both as first-line treatment andin patients with rituximab-refractory disease,and CLL (see the reviews by Tobinai et al. [163]and Goede et al. [164] for detailed assessmentsof this agent). Other examples of newer agentsinclude ofatumumab, veltuzumab, and ocre-lizumab [165]. Both obinutuzumab and ritux-imab are important backbones of therapy in thissetting for the foreseeable future. Anotherexample of development of a drug that exploitsthe CD20 pathway is CD20/CD3 antibodies.Furthermore, the introduction of subcuta-neously administered rituximab (extensivelyreviewed by Davies et al. [31]), with its simpli-fied administration schedule, reduced treat-ment burden for patients, and the potentialresource savings for healthcare systems, is likelyto further strengthen the position of rituximab
2264 Adv Ther (2017) 34:2232–2273

as an essential treatment for symptomatic,advanced B-cell malignancies.
ACKNOWLEDGEMENTS
The study and article processing charges,including the open access fee, were funded by F.Hoffmann-La Roche Ltd., Basel, Switzerland.Support for third-party writing assistance forthe manuscript, provided by Cheryl Wright ofGardiner-Caldwell Communications, was fun-ded by F. Hoffmann-La Roche Ltd., Basel,Switzerland. All authors had full access to theinformation included in this review and takecomplete responsibility for the integrity of thedata discussions. All named authors meet theInternational Committee of Medical JournalEditors criteria for authorship for this article,take responsibility for the integrity of the workas a whole, and have given final approval for theversion to be published. We thank all currentand former researchers and investigators as wellas patients and their families who participatedin clinical trials establishing MabThera/Rituxanas an essential drug to treat patients with B-cellmalignancies. We also thank Peter Morcos ofRoche for his careful review and contributionsto the pharmacokinetics section.
Compliance with Ethics Guidelines Theinformation reported in this review is derivedfrom previously conducted studies: this doesnot include any new studies of human or ani-mal subjects performed by any of the authors.All authors had full access to the informationincluded in this review and take completeresponsibility for the integrity of the datadiscussions.
Disclosures Martin Barrett is an employee ofRoche Products Ltd. and holds share options.Robin Foa has received honoraria from F. Hoff-mann-La Roche Ltd. Joerg Maurer is anemployee of F. Hoffmann-La Roche Ltd. andholds share options. Michael Wenger is anemployee of F. Hoffmann-La Roche Ltd. andholds share options. David G. Maloney hasnothing to disclose. Nancy Valente is anemployee of Genentech Inc. and holds share
options. Gilles Salles has received research andtravel grant support and honoraria from F.Hoffmann-la Roche Ltd., and honoraria fromAmgen, BMS, Celgene, Gilead, Janssen, Kite,Merck, Morphosys, Novartis, and Servier. SusanO’Brien has received research grant supportfrom ProNAI, Regeneron, and Acerta, and con-sultant/research support from Gilead, Pharma-cyclics, TG Therapeutics, and Pfizer, and hasacted as a consultant for Amgen, Astellas, Cel-gene, GlaxoSmithKline, Janssen Oncology,Aptose Biosciences Inc., Vaniam Group LLC,Abbvie, Sunesis, and Alexion.
Data availability Data sharing is not applica-ble to this article as no datasets were generatedor analyzed during the current study.
Open Access. This article is distributed underthe terms of the Creative Commons Attribu-tion-NonCommercial 4.0 International License(http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use,distribution, and reproduction in any medium,provided you give appropriate credit to theoriginal author(s) and the source, provide a linkto the Creative Commons license, and indicateif changes were made.
REFERENCES
1. Boffetta P. Epidemiology of adult non-Hodgkinlymphoma. Ann Oncol. 2011;22(Suppl 4):iv27–31.
2. Hallek M. Chronic lymphocytic leukemia: 2015Update on diagnosis, risk stratification, and treat-ment. Am J Hematol. 2015;90:447–60.
3. National Cancer Institute. SEER cancer statisticsreview 1975–2013. Non-Hodgkin lymphoma. 2016.https://seer.cancer.gov/csr/1975_2013/results_merged/sect_19_nhl.pdf. Accessed 21 Jun 2017.
4. Torre LA, Bray F, Siegel RL, et al. Global cancerstatistics, 2012. CA Cancer J Clin. 2015;65:87–108.
5. Fisher SG, Fisher RI. The epidemiology of non-Hodgkin’s lymphoma. Oncogene. 2004;23:6524–34.
6. Cancer Research UK. Non-Hodgkin lymphoma(C82-C86): 1979-2013 European age-standardisedincidence rates per 100,000 population, by sex,Great Britain. 2013. http://www.cancerresearchuk.
Adv Ther (2017) 34:2232–2273 2265

org/sites/default/files/cstream-node/inc_asr_gb_nhl_1.pdf. Accessed 21 Jun 2017.
7. National Cancer Institute. Surveillance, Epidemiol-ogy, and End Results Program. Cancer Stat Facts:Non-Hodgkin Lymphoma. 2017. http://seer.cancer.gov/statfacts/html/nhl.html. Accessed 21 Jun 2017.
8. Chen Q, Jain N, Ayer T, et al. Economic burden ofchronic lymphocytic leukemia in the era of oraltargeted therapies in the United States. J ClinOncol. 2017;35:166–74.
9. Tilly H, Gomes da Silva M, Vitolo U, et al. Diffuselarge B-cell lymphoma (DLBCL): ESMO clinicalpractice guidelines for diagnosis, treatment andfollow-up. Ann Oncol. 2015;26(Suppl 5):v116–25.
10. Dreyling M, Ghielmini M, Rule S, et al. Newlydiagnosed and relapsed follicular lymphoma: ESMOclinical practice guidelines for diagnosis, treatmentand follow-up. Ann Oncol. 2016;27(Suppl5):v83–90.
11. Eichhorst B, Robak T, Montserrat E, et al. Chroniclymphocytic leukaemia: ESMO clinical practiceguidelines for diagnosis, treatment and follow-up.Ann Oncol. 2015;26(Suppl 5):v78–84.
12. Hoster E, Dreyling M, Klapper W, et al. A newprognostic index (MIPI) for patients with advan-ced-stage mantle cell lymphoma. Blood.2008;111:558–65.
13. International CLL-IPI Working Group. An interna-tional prognostic index for patients with chroniclymphocytic leukaemia (CLL-IPI): a meta-analysis ofindividual patient data. Lancet Oncol.2016;17:779–90.
14. Lenz G, Wright GW, Emre NC, et al. Molecularsubtypes of diffuse large B-cell lymphoma arise bydistinct genetic pathways. Proc Natl Acad Sci U S A.2008;105:13520–5.
15. Scott DW, Mottok A, Ennishi D, et al. Prognosticsignificance of diffuse large B-cell lymphoma cell oforigin determined by digital gene expression informalin-fixed paraffin-embedded tissue biopsies.J Clin Oncol. 2015;33:2848–56.
16. Kohler G, Milstein C. Continuous cultures of fusedcells secreting antibody of predefined specificity.Nature. 1975;256:495–7.
17. National Cancer Institute. Using the immune systemin the fight against cancer: discovery of rituximab.2014. http://www.cancer.gov/research/progress/discovery/blood-cancer. Accessed 21 Jun 2017.
18. Nadler LM, Stashenko P, Hardy R, et al. Serotherapyof a patient with a monoclonal antibody directed
against a human lymphoma-associated antigen.Cancer Res. 1980;40:3147–54.
19. Miller RA, Maloney DG, Warnke R, Levy R. Treat-ment of B-cell lymphoma with monoclonalanti-idiotype antibody. N Engl J Med.1982;306:517–22.
20. Press OW, Appelbaum F, Ledbetter JA, et al. Mon-oclonal antibody 1F5 (anti-CD20) serotherapy ofhuman B cell lymphomas. Blood. 1987;69:584–91.
21. Banchereau J, Rousset F. Human B lymphocytes:phenotype, proliferation, and differentiation. AdvImmunol. 1992;52:125–262.
22. National Comprehensive Cancer Network. NCCNclinical practice guidelines in oncology. B-celllymphomas. Version 3.2016. 2016. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#site. Accessed 21 Jun 2017.
23. National Comprehensive Cancer Network. NCCNclinical practice guidelines in oncology. Chroniclymphocytic leukemia/small lymphocytic lym-phoma. Version 1.2017. 2017. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp#site.Accessed 21 Jun 2017.
24. World Health Organization. WHO Model Lists ofEssential Medicines, adults. 20th edn. 2017.http://www.who.int/medicines/publications/esse-ntialmedicines/en/. Accessed 21 Jun 2017.
25. Davies A, Merli F, Mihaljevic B, et al. Pharmacoki-netics and safety of subcutaneous rituximab in fol-licular lymphoma (SABRINA): stage 1 analysis of arandomised phase 3 study. Lancet Oncol.2014;15:343–52.
26. Assouline S, Buccheri V, Delmer A, et al. Pharma-cokinetics, safety, and efficacy of subcutaneousversus intravenous rituximab plus chemotherapy astreatment for chronic lymphocytic leukaemia(SAWYER): a phase 1b, open-label, randomisedcontrolled non-inferiority trial. Lancet Haematol.2016;3:e128–38.
27. Dreyling M, Geisler C, Hermine O, et al. Newlydiagnosed and relapsed mantle cell lymphoma:ESMO clinical practice guidelines for diagnosis,treatment and follow-up. Ann Oncol.2014;25(Suppl 3):iii83–92.
28. Lopez-Olivo MA, Amezaga Urruela M, McGahan L,Pollono EN, Suarez-Almazor ME. Rituximab forrheumatoid arthritis. Cochrane Database Syst Rev.2015;1:CD007356.
29. Mabthera 100 mg concentrate for solution forinfusion [summary of product characteristics].Roche Products, Welwyn Garden City. 2017.
2266 Adv Ther (2017) 34:2232–2273

https://www.medicines.org.uk/emc/medicine/2570.Accessed 18 Sept 2017.
30. Rituxan� (rituximab) injection, for intravenous use.Genentech, South San Francisco. 2016. https://www.gene.com/download/pdf/rituxan_prescribing.pdf. Accessed 21 Jun 2017.
31. Davies A, Berge C, Boehnke A, et al. Subcutaneousrituximab for the treatment of B-cell hematologicalmalignancies: scientific rationale and clinicaldevelopment. Adv Ther. 2017.
32. Reff ME, Carner K, Chambers KS, et al. Depletion ofB cells in vivo by a chimeric mouse human mono-clonal antibody to CD20. Blood. 1994;83:435–45.
33. Maloney DG, Smith B, Rose A. Rituximab: mecha-nism of action and resistance. Semin Oncol.2002;29(1 Suppl 2):2–9.
34. Weiner GJ. Rituximab: mechanism of action. SeminHematol. 2010;47:115–23.
35. Boross P, Leusen JH. Mechanisms of action of CD20antibodies. Am J Clin Res. 2012;2:676–90.
36. Abulayha A, Bredan A, El Enshasy H, Daniels I.Rituximab: modes of action, remaining dispute andfuture perspective. Future Oncol. 2014;10:2481–92.
37. Weiner GJ, Bowles JA, Link BK, et al. Anti-CD20monoclonal antibody (mAb) with enhanced affinityfor CD16 activates NK cells at lower concentrationsand more effectively than rituximab. Blood.2005;106:348.
38. Maloney DG, Liles TM, Czerwinski DK, et al. Phase Iclinical trial using escalating single-dose infusion ofchimeric anti-CD20 monoclonal antibody(IDEC-C2B8) in patients with recurrent B-cell lym-phoma. Blood. 1994;84:2457–66.
39. Maloney DG, Grillo-Lopez AJ, White CA, et al.IDEC-C2B8 (rituximab) anti-CD20 monoclonal anti-body therapy in patients with relapsed low-gradenon-Hodgkin’s lymphoma. Blood. 1997;90:2188–95.
40. Berinstein NL, Grillo-Lopez AJ, White CA, et al.Association of serum rituximab (IDEC-C2B8) con-centration and anti-tumor response in the treat-ment of recurrent low-grade or follicularnon-Hodgkin’s lymphoma. Ann Oncol.1998;9:995–1001.
41. Regazzi MB, Iacona I, Avanzini MA, et al. Pharma-cokinetic behaviour of rituximab. A study of dif-ferent schedules of administration for heterogenousclinical settings. Ther Drug Monit. 2005;27:785–92.
42. Tran L, Baars JW, Aarden L, Beijnen JH, HuitemaAD. Pharmacokinetics of rituximab in patients with
CD20 positive B-cell malignancies. Hum Antib.2010;19:7–13.
43. Blasco H, Chatelut E, Benz de Bretagne I,Congy-Jolivet N, Le Guellec C. Pharmacokinetics ofrituximab associated with CHOP chemotherapy inB-cell non-Hodgkin lymphoma. Fundam ClinPharmacol. 2009;23:601–8.
44. Li L, Levi M, Charoin J-E, et al. Rituximab exhibits along half-life based on a population pharmacoki-netic analysis in non-Hodgkin’s lymphoma (NHL)patients. Blood. 2007;110:2371.
45. Li J, Zhi J, Wenger M, et al. Population pharma-cokinetics of rituximab in patients with chroniclymphocytic leukemia. J Clin Pharmacol.2012;52:1918–26.
46. Tobinai K, Igarashi T, Itoh K, et al. Japanese multi-center phase II and pharmacokinetic study ofrituximab in relapsed or refractory patients withaggressive B-cell lymphoma. Ann Oncol.2004;15:821–30.
47. Dayde D, Ternant D, Ohresser M, et al. Tumorburden influences exposure and response to ritux-imab: pharmacokinetic-pharmacodynamic model-ing using a syngeneic bioluminescent murinemodel expressing human CD20. Blood.2009;113:3765–72.
48. Igarashi T, Kobayashi Y, Ogura M, et al. Factorsaffecting toxicity, response and progression-freesurvival in relapsed patients with indolent B-celllymphoma and mantle cell lymphoma treated withrituximab: a Japanese phase II study. Ann Oncol.2002;13:928–43.
49. Jager U, Fridrik M, Zeitlinger M, et al. Rituximabserum concentrations during immuno-chemother-apy of follicular lymphoma correlate with patientgender, bone marrow infiltration and clinicalresponse. Haematologica. 2012;97:1431–8.
50. Tout M, Casasnovas O, Meignan M, et al. Rituximabexposure is influenced by baseline metabolic tumorvolume and predicts outcome of DLBCL patients: aLymphoma Study Association report. Blood.2017;129:2616–23.
51. Muller C, Murawski N, Wiesen MH, et al. The role ofsex and weight on rituximab clearance and serumelimination half-life in elderly patients withDLBCL. Blood. 2012;119:3276–84.
52. Pfreundschuh M, Muller C, Zeynalova S, et al.Suboptimal dosing of rituximab in male and femalepatients with DLBCL. Blood. 2014;123:640–6.
53. Junlen HR, Peterson S, Kimby E, et al. Follicularlymphoma in Sweden: nationwide improved
Adv Ther (2017) 34:2232–2273 2267

survival in the rituximab era, particularly in elderlywomen: a Swedish Lymphoma Registry study. Leu-kemia. 2015;29:668–76.
54. McLaughlin P, Grillo-Lopez AJ, Link BK, et al.Rituximab chimeric anti-CD20 monoclonal anti-body therapy for relapsed indolent lymphoma: halfof patients respond to a four-dose treatment pro-gram. J Clin Oncol. 1998;16:2825–33.
55. Davis TA, White CA, Grillo-Lopez AJ, et al. Sin-gle-agent monoclonal antibody efficacy in bulkynon-Hodgkin’s lymphoma: results of a phase II trialof rituximab. J Clin Oncol. 1999;17:1851–7.
56. Feuring-Buske M, Kneba M, Unterhalt M, et al.IDECC2B8 (rituximab) anti-CD20 antibody treat-ment in relapsed relapsed advanced-stage follicularlymphomas: results of a phase-II study of the Ger-man Low-Grade Lymphoma Study Group. AnnHematol. 2000;79:493–500.
57. Foran JM, Gupta RK, Cunningham D, et al. A UKmulticentre phase II study of rituximab (chimaericanti-CD20 monoclonal antibody) in patients withfollicular lymphoma, with PCR monitoring ofmolecular response. Br J Haematol. 2000;109:81–8.
58. Piro LD, White CA, Grillo-Lopez AJ, et al. Extendedrituximab (anti-CD20 monoclonal antibody) ther-apy for relapsed or refractory low-grade or follicularnon-Hodgkin’s lymphoma. Ann Oncol.1999;10:655–61.
59. Colombat P, Brousse N, Salles G, et al. Rituximabinduction immunotherapy for first-line low-tu-mor-burden follicular lymphoma: survival analyseswith 7-year follow-up. Ann Oncol. 2012;23:2380–5.
60. Taverna C, Martinelli G, Hitz F, et al. Rituximabmaintenance for a maximum of 5 years after sin-gle-agent rituximab induction in follicular lym-phoma: results of the randomized controlled phaseIII trial SAKK 35/03. J Clin Oncol. 2016;34:495–500.
61. Kimby E, Ostenstad B, Brown P, et al. Two courses offour weekly infusions of rituximab with or withoutinterferon-a2a: final results from a randomizedphase III study in symptomatic indolent B-celllymphomas. Leuk Lymphoma. 2015;56:2598–607.
62. Czuczman MS, Weaver R, Alkuzweny B, et al. Pro-longed clinical and molecular remission in patientswith low-grade or follicular non-Hodgkin’s lym-phoma treated with rituximab plus CHOPchemotherapy: 9-year follow-up. J Clin Oncol.2004;22:4711–6.
63. Hiddemann W, Kneba M, Dreyling M, et al. Front-line therapy with rituximab added to the combi-nation of cyclophosphamide, doxorubicin,vincristine, and prednisone (CHOP) significantly
improves the outcome for patients with advan-ced-stage follicular lymphoma compared withtherapy with CHOP alone: results of a prospectiverandomized study of the German Low-Grade Lym-phoma Study Group. Blood. 2005;106:3725–32.
64. Herold M, Haas A, Srock S, et al. Rituximab added tofirst-line mitoxantrone, chlorambucil, and pred-nisolone chemotherapy followed by interferonmaintenance prolongs survival in patients withadvanced follicular lymphoma: an East GermanStudy Group hematology and oncology study.J Clin Oncol. 2007;25:1986–92.
65. Marcus R, Imrie K, Belch A, et al. CVP chemother-apy plus rituximab compared with CVP as first-linetreatment for advanced follicular lymphoma.Blood. 2005;105:1417–23.
66. Marcus R, Imrie K, Solal-Celigny P, et al. Phase IIIstudy of R-CVP compared with cyclophosphamide,vincristine, and prednisone alone in patients withpreviously untreated advanced follicular lym-phoma. J Clin Oncol. 2008;26:4579–86.
67. Salles G, Mounier N, de Guibert S, et al. Rituximabcombined with chemotherapy and interferon infollicular lymphoma patients: results of theGELA-GOELAMS FL2000 study. Blood.2008;112:4824–31.
68. Bachy E, Houot R, Morschhauser F, et al. Long-termfollow-up of the FL2000 study comparingCHVP-interferon to CHVP-interferon plus ritux-imab in follicular lymphoma. Haematologica.2013;98:1107–14.
69. Federico M, Luminari S, Dondi A, et al. R-CVP ver-sus R-CHOP versus R-FM for the initial treatment ofpatients with advanced-stage follicular lymphoma:results of the FOLL05 trial conducted by the Fon-dazione Italiana Linfomi. J Clin Oncol.2013;31:1506–13.
70. Rummel MJ, Niederle N, Maschmeyer G, et al.Bendamustine plus rituximab versus CHOP plusrituximab as first-line treatment for patients withindolent and mantle-cell lymphomas: an open-la-bel, multicentre, randomised, phase 3 non-inferi-ority trial. Lancet. 2013;381:1203–10.
71. van Oers MH, Klasa R, Marcus RE, et al. Rituximabmaintenance improves clinical outcome ofrelapsed/resistant follicular non-Hodgkin lym-phoma in patients both with and without ritux-imab during induction: results of a prospectiverandomized phase 3 intergroup trial. Blood.2006;108:3295–301.
72. Hochster H, Weller E, Gascoyne RD, et al. Mainte-nance rituximab after cyclophosphamide, vin-cristine, and prednisone prolongs progression-free
2268 Adv Ther (2017) 34:2232–2273

survival in advanced indolent lymphoma: results ofthe randomized phase III ECOG1496 study. J ClinOncol. 2009;27:1607–14.
73. Salles G, Seymour JF, Offner F, et al. Rituximabmaintenance for 2 years in patients with hightumour burden follicular lymphoma responding torituximab plus chemotherapy (PRIMA): a phase 3,randomised controlled trial. Lancet.2011;377:42–51.
74. Salles GA, Seymour JF, Feugier P, et al. Updated6-year follow-up of the PRIMA study confirms thebenefit of 2-year rituximab maintenance in follicu-lar lymphoma patients responding to frontlineimmunochemotherapy. Blood. 2013;122:509.
75. Kahl BS, Hong F, Williams ME, et al. Rituximabextended schedule or re-treatment trial for low-tu-mor burden follicular lymphoma: Eastern Cooper-ative Oncology Group protocol E4402. J Clin Oncol.2014;32:3096–102.
76. Forstpointner R, Dreyling M, Repp R, et al. Theaddition of rituximab to a combination of flu-darabine, cyclophosphamide, mitoxantrone (FCM)significantly increases the response rate and pro-longs survival as compared with FCM alone inpatients with relapsed and refractory follicular andmantle cell lymphomas: results of a prospectiverandomized study of the German Low-GradeLymphoma Study Group. Blood. 2004;104:3064–71.
77. Forstpointner R, Unterhalt M, Dreyling M, et al.Maintenance therapy with rituximab leads to asignificant prolongation of response duration aftersalvage therapy with a combination of rituximab,fludarabine, cyclophosphamide, and mitoxantrone(R-FCM) in patients with recurring and refractoryfollicular and mantle cell lymphomas: results of aprospective randomized study of the German LowGrade Lymphoma Study Group (GLSG). Blood.2006;108:4003–8.
78. van Oers MH, Van Glabbeke M, Giurgea L, et al.Rituximab maintenance treatment of relapsed/resistant follicular non-Hodgkin’s lymphoma: long-term outcome of the EORTC 20981 phase IIIrandomized intergroup study. J Clin Oncol.2010;28:2853–8.
79. Martinelli G, Schmitz SF, Utiger U, et al. Long-termfollow-up of patients with follicular lymphomareceiving single-agent rituximab at two differentschedules in trial SAKK 35/98. J Clin Oncol.2010;28:4480–4.
80. Vidal L, Gafter-Gvili A, Salles G, et al. Rituximabmaintenance improves overall survival of patientswith follicular lymphoma–Individual patient datameta-analysis. Eur J Cancer. 2017;76:216–25.
81. Hagemeister FB. ‘Watch and wait’ as initial man-agement for patients with follicular lymphomas:still a viable strategy? BioDrugs. 2012;26:363–76.
82. Ardeshna KM, Qian W, Smith P, et al. Rituximabversus a watch-and-wait approach in patients withadvanced-stage, asymptomatic, non-bulky follicularlymphoma: an open-label randomised phase 3 trial.Lancet Oncol. 2014;15:424–35.
83. Armitage JO, Longo DL. Is watch and wait stillacceptable for patients with low-grade follicularlymphoma? Blood. 2016;127:2804–8.
84. Vose JM, Link BK, Grossbard ML, et al. Phase IIstudy of rituximab in combination with CHOPchemotherapy in patients with previouslyuntreated, aggressive non-Hodgkin’s lymphoma.J Clin Oncol. 2001;19:389–97.
85. Coiffier B, Lepage E, Briere J, et al. CHOPchemotherapy plus rituximab compared with CHOPalone in elderly patients with diffuse large-B-celllymphoma. N Engl J Med. 2002;346:235–42.
86. Habermann TM, Weller EA, Morrison VA, et al.Rituximab-CHOP versus CHOP alone or withmaintenance rituximab in older patients with dif-fuse large B-cell lymphoma. J Clin Oncol.2006;24:3121–7.
87. Pfreundschuh M, Trumper L, Osterborg A, et al.CHOP-like chemotherapy plus rituximab versusCHOP-like chemotherapy alone in young patientswith good-prognosis diffuse large-B-cell lymphoma:a randomised controlled trial by the MabTheraInternational Trial (MInT) Group. Lancet Oncol.2006;7:379–91.
88. Pfreundschuh M, Kuhnt E, Trumper L, et al.CHOP-like chemotherapy with or without ritux-imab in young patients with good-prognosis diffuselarge-B-cell lymphoma: 6-year results of anopen-label randomised study of the MabTheraInternational Trial (MInT) Group. Lancet Oncol.2011;12:1013–22.
89. Feugier P, Van Hoof A, Sebban C, et al. Long-termresults of the R-CHOP study in the treatment ofelderly patients with diffuse large B-cell lymphoma:a study by the Groupe d’Etude des Lymphomes del’Adulte. J Clin Oncol. 2005;23:4117–26.
90. Coiffier B, Thieblemont C, Van Den Neste E, et al.Long-term outcome of patients in the LNH-98.5trial, the first randomized study comparing ritux-imab-CHOP to standard CHOP chemotherapy inDLBCL patients: a study by the Groupe d’Etudes desLymphomes de l’Adulte. Blood. 2010;116:2040–5.
91. Jaeger U, Trneny M, Melzer H, et al. Rituximabmaintenance for patients with aggressive B-cell
Adv Ther (2017) 34:2232–2273 2269

lymphoma in first remission: results of the ran-domized NHL13 trial. Haematologica.2015;100:955–63.
92. Coiffier B, Haioun C, Ketterer N, et al. Rituximab(anti-CD20 monoclonal antibody) for the treatmentof patients with relapsing or refractory aggressivelymphoma: a multicenter phase II study. Blood.1998;92:1927–32.
93. Vellenga E, van Putten WLJ, van ‘t Veer MB, et al.Rituximab improves the treatment results ofDHAP-VIM-DHAP and ASCT in relapsed/progressiveaggressive CD20? NHL: a prospective randomizedHOVON trial. Blood. 2008;111:537–43.
94. Gisselbrecht C, Glass B, Mounier N, et al. Salvageregimens with autologous transplantation forrelapsed large B-cell lymphoma in the rituximabera. J Clin Oncol. 2010;28:4184–90.
95. Jermann M, Jost LM, Taverna C, et al. Ritux-imab-EPOCH, an effective salvage therapy forrelapsed, refractory or transformed B-cell lym-phomas: results of a phase II study. Ann Oncol.2004;15:511–6.
96. Kewalramani T, Zelenetz AD, Nimer SD, et al.Rituximab and ICE as second-line therapy beforeautologous stem cell transplantation for relapsed orprimary refractory diffuse large B-cell lymphoma.Blood. 2004;103:3684–8.
97. Mey UJ, Olivieri A, Orlopp KS, et al. DHAP incombination with rituximab vs DHAP alone as sal-vage treatment for patients with relapsed or refrac-tory diffuse large B-cell lymphoma: a matched-pairanalysis. Leuk Lymphoma. 2006;47:2558–66.
98. Elstrom RL, Andemariam B, Martin P, et al. Borte-zomib in combination with rituximab, dexam-ethasone, ifosfamide, cisplatin and etoposidechemo- immunotherapy in patients with relapsedand primary refractory diffuse large B-cell lym-phoma. Leuk Lymphoma. 2012;53:1469–73.
99. Hallek M, Fischer K, Fingerle-Rowson G, et al.Addition of rituximab to fludarabine andcyclophosphamide in patients with chronic lym-phocytic leukaemia: a randomised, open-label,phase 3 trial. Lancet. 2010;376:1164–74.
100. Robak T, Dmoszynska A, Solal-Celigny P, et al.Rituximab plus fludarabine and cyclophosphamideprolongs progression-free survival compared withfludarabine and cyclophosphamide alone in previ-ously treated chronic lymphocytic leukemia. J ClinOncol. 2010;28:1756–65.
101. Byrd JC, Murphy T, Howard RS, et al. Rituximabusing a thrice weekly dosing schedule in B-cellchronic lymphocytic leukemia and small
lymphocytic lymphoma demonstrates clinicalactivity and acceptable toxicity. J Clin Oncol.2001;19:2153–64.
102. O’Brien SM, Kantarjian H, Thomas DA, et al.Rituximab dose-escalation trial in chronic lympho-cytic leukemia. J Clin Oncol. 2001;19:2165–70.
103. Schulz H, Klein SK, Rehwald U, et al. Phase 2 studyof a combined immunochemotherapy using ritux-imab and fludarabine in patients with chroniclymphocytic leukemia. Blood. 2002;100:3115–20.
104. Byrd JC, Peterson BL, Morrison VA, et al. Random-ized phase 2 study of fludarabine with concurrentversus sequential treatment with rituximab insymptomatic, untreated patients with B-cellchronic lymphocytic leukemia: results from Cancerand Leukemia Group B 9712 (CALGB 9712). Blood.2003;101:6–14.
105. Keating MJ, O’Brien S, Albitar M, et al. Early resultsof a chemoimmunotherapy regimen of fludarabine,cyclophosphamide, and rituximab as initial therapyfor chronic lymphocytic leukemia. J Clin Oncol.2005;23:4079–88.
106. Wierda W, O’Brien S, Wen S, et al. Chemoim-munotherapy with fludarabine, cyclophosphamide,and rituximab for relapsed and refractory chroniclymphocytic leukemia. J Clin Oncol. 2005;23:4070–8.
107. Fischer K, Bahlo J, Fink AM, et al. Long-termremissions after FCR chemoimmunotherapy inpreviously untreated patients with CLL: updatedresults of the CLL8 trial. Blood. 2016;127:208–15.
108. Rossi D, Terzi-di-Bergamo L, De Paoli L, et al.Molecular prediction of durable remission afterfirst-line fludarabine-cyclophosphamide-rituximabin chronic lymphocytic leukemia. Blood.2015;126:1921–4.
109. Thompson P, Tam CS, O’Brien SM, et al. Fludara-bine, cyclophosphamide, and rituximab treatmentachieves long-term disease-free survival inIGHV-mutated chronic lymphocytic leukemia.Blood. 2016;127:303–9.
110. Tam CS, O’Brien S, Wierda W, et al. Long-termresults of the fludarabine, cyclophosphamide, andrituximab regimen as initial therapy of chroniclymphocytic leukemia. Blood. 2008;112:975–80.
111. Foon KA, Boyiadzis M, Land SR, et al. Chemoim-munotherapy with low-dose fludarabine andcyclophosphamide and high-dose rituximab inpreviously untreated patients with chronic lym-phocytic leukemia. J Clin Oncol. 2009;27:498–503.
112. Foon KA, Mehta D, Lentzsch S, et al. Long-termresults of chemoimmunotherapy with low-dose
2270 Adv Ther (2017) 34:2232–2273

fludarabine, cyclophosphamide and high-doserituximab as initial treatment for patients withchronic lymphocytic leukemia. Blood.2012;119:3184–5.
113. Woyach JA, Ruppert AS, Heerema NA, et al. Che-moimmunotherapy with fludarabine and rituximabproduces extended overall survival and progres-sion-free survival in chronic lymphocytic leukemia:long-term follow-up of CALGB study 9712. J ClinOncol. 2011;29:1349–55.
114. Fischer K, Cramer P, Busch R, et al. Bendamustinecombined with rituximab in patients with relapsedand/or refractory chronic lymphocytic leukemia: amulticenter phase II trial of the German ChronicLymphocytic Leukemia Study Group. J Clin Oncol.2011;29:3559–66.
115. Fischer K, Cramer P, Busch R, et al. Bendamustine incombination with rituximab for previouslyuntreated patients with chronic lymphocytic leu-kemia: a multicenter phase II trial of the GermanChronic Lymphocytic Leukemia Study Group.J Clin Oncol. 2012;30:3209–16.
116. Eichhorst B, Fink AM, Bahlo J, et al. First-linechemoimmunotherapy with bendamustine andrituximab versus fludarabine, cyclophosphamide,and rituximab in patients with advanced chroniclymphocytic leukaemia (CLL10): an international,open-label, randomised, phase 3, non-inferioritytrial. Lancet Oncol. 2016;17:928–42.
117. Foa R, Del Giudice I, Cuneo A, et al. Chlorambucilplus rituximab with or without maintenance ritux-imab as first-line treatment for elderly chroniclymphocytic leukemia patients. Am J Hematol.2014;89:480–6.
118. Hillmen P, Gribben JG, Follows GA, et al. Rituximabplus chlorambucil as first-line treatment for chroniclymphocytic leukemia: final analysis of anopen-label phase II study. J Clin Oncol.2014;32:1236–41.
119. Del Poeta G, Del Principe MI, Buccisano F, et al.Consolidation and maintenance immunotherapywith rituximab improve clinical outcome inpatients with B-cell chronic lymphocytic leukemia.Cancer. 2008;112:119–28.
120. Abrisqueta P, Villamor N, Terol MJ, et al. Rituximabmaintenance after first-line therapy with rituximab,fludarabine, cyclophosphamide, and mitoxantrone(R-FCM) for chronic lymphocytic leukemia. Blood.2013;122:3951–9.
121. Dartigeas C, van den Neste E, Maisonneuve H, et al.Rituximab maintenance after induction with abbre-viated FCR in previously untreated elderly (C65 years)CLL patients: results of the randomized CLL 2007 SA
trial from the French FILO Group (NCT00645606).J Clin Oncol. 2016;34(15 Suppl):7505.
122. Awan FT, Gore L, Gao L, Sharma J, Lager J, Costa LJ.Phase Ib trial of the PI3K/mTOR inhibitor voxtalisib(SAR245409) in combination with chemoim-munotherapy in patients with relapsed or refractoryB-cell malignancies. Br J Haematol. 2016;175:55–65.
123. Chanan-Khan A, Cramer P, Demirkan F, et al.Ibrutinib combined with bendamustine and ritux-imab compared with placebo, bendamustine, andrituximab for previously treated chronic lympho-cytic leukaemia or small lymphocytic lymphoma(HELIOS): a randomised, double-blind, phase 3study. Lancet Oncol. 2016;17:200–11.
124. Kipps TJ, Eradat H, Grosicki S, et al. A phase 2 studyof the BH3 mimetic BCL2 inhibitor navitoclax(ABT-263) with or without rituximab, in previouslyuntreated B-cell chronic lymphocytic leukemia.Leuk Lymphoma. 2015;56:2826–33.
125. Del Poeta G, Postorino M, Pupo L, et al. Venetoclax:Bcl-2 inhibition for the treatment of chronic lym-phocytic leukemia. Drugs Today. 2016;52:249–60.
126. Zucca E, Conconi A, Martinelli G, et al. Final results ofthe IELSG-19 randomized trial of mucosa-associatedlymphoid tissue lymphoma: improved event-free andprogression-free survival with rituximab plus chlo-rambucil versus either chlorambucil or rituximabmonotherapy. J Clin Oncol. 2017;35:1905–12.
127. Williams ME, Hong F, Gascoyne RD, et al. Ritux-imab extended schedule or retreatment trial for lowtumour burden non-follicular indolent B-cellnon-Hodgkin lymphomas: Eastern CooperativeOncology Group protocol E4402. Br J Haematol.2016;173:867–75.
128. Maury S, Chevret S, Thomas X, et al. Rituximab inB-lineage adult acute lymphoblastic leukemia.N Engl J Med. 2016;375:1044–53.
129. Ribrag V, Koscielny S, Bosq J, et al. Rituximab anddose-dense chemotherapy for adults with Burkitt’slymphoma: a randomised, controlled, open-label,phase 3 trial. Lancet. 2016;387:2402–11.
130. Griffiths R, Mikhael J, Gleeson M, et al. Addition ofrituximab to chemotherapy alone as first-line ther-apy improves overall survival in elderly patientswith mantle cell lymphoma. Blood.2011;118:4808–16.
131. Kluin-Nelemans HC, Hoster E, Hermine O, et al.Treatment of older patients with mantle-cell lym-phoma. N Engl J Med. 2012;367:520–31.
132. Dimopoulos MA, Anagnostopoulos A, KyrtsonisMC, et al. Primary treatment of Waldenstrom
Adv Ther (2017) 34:2232–2273 2271

macroglobulinemia with dexamethasone, ritux-imab, and cyclophosphamide. J Clin Oncol.2007;25:3344–9.
133. Oki Y, Pro B, Fayad LE, et al. Phase 2 study ofgemcitabine in combination with rituximab inpatients with recurrent or refractory Hodgkin lym-phoma. Cancer. 2008;112:831–6.
134. Trappe RU, Dierickx D, Zimmermann H, et al.Response to rituximab induction is a predictivemarker in B-cell post-transplant lymphoprolifera-tive disorder and allows successful stratification intorituximab or R-CHOP consolidation in an interna-tional, prospective, multicenter phase II trial. J ClinOncol. 2016. doi:10.1200/JCO.2016.69.3564.
135. Davis TA, Grillo-Lopez AJ, White CA, et al. Ritux-imab anti-CD20 monoclonal antibody therapy innon-Hodgkin’s lymphoma: safety and efficacy ofre-treatment. J Clin Oncol. 2000;18:3135–43.
136. Rezvani AR, Maloney DG. Rituximab resistance.Best Pract Res Clin Haematol. 2011;24:203–16.
137. Bonavida B. Postulated mechanisms of resistance ofB-cell non-Hodgkin lymphoma to rituximab treat-ment regimens: strategies to overcome resistance.Semin Oncol. 2014;41:667–77.
138. Czuczman MS, Olejniczak S, Gowda A, et al.Acquirement of rituximab resistance in lymphomacell lines is associated with both global CD20 geneand protein down-regulation regulated at the pre-transcriptional and posttranscriptional levels. ClinCancer Res. 2008;14:1561–70.
139. Hiraga J, Tomita A, Sugimoto T, et al. Down-regu-lation of CD20 expression in B-cell lymphoma cellsafter treatment with rituximab-containing combi-nation chemotherapies: its prevalence and clinicalsignificance. Blood. 2009;113:4885–93.
140. Beum PV, Peek EM, Lindorfer MA, et al. Loss ofCD20 and bound CD20 antibody from opsonized Bcells occurs more rapidly because of trogocytosismediated by Fc receptor-expressing effector cellsthan direct internalization by the B cells. J Im-munol. 2011;187:3438–47.
141. Badoux XC, Keating MJ, Wen S, et al. Phase II studyof lenalidomide and rituximab as salvage therapy forpatients with relapsed or refractory chronic lym-phocytic leukemia. J Clin Oncol. 2013;31:584–91.
142. Ivanov V, Coso D, Chetaille B, et al. Efficacy andsafety of lenalidomide combined with rituximab inpatients with relapsed/refractory diffuse large B-celllymphoma. Leuk Lymphoma. 2014;55:2508–13.
143. Chong EA, Ahmadi T, Aqui NA, et al. Combination oflenalidomide and rituximab overcomes rituximab
resistance in patients with indolent B-cell and mantlecell lymphomas. Clin Cancer Res. 2015;21:1835–42.
144. Leonard JP, Jung SH, Johnson J, et al. Randomizedtrial of lenalidomide alone versus lenalidomide plusrituximab in patients with recurrent follicular lym-phoma: CALGB 50401 (Alliance). J Clin Oncol.2015;33:3635–40.
145. Gazyvaro� 1000 mg concentrate for solution forinfusion [summary of product characteristics]. RocheProducts, Welwyn Garden City. 2016. http://www.medicines.org.uk/emc/medicine/29057. Accessed 1Jun 2017.
146. Minard-Colin V, Auperin A, Pillon M, et al. Resultsof the randomized Intergroup trial Inter-B-NHLRitux 2010 for children and adolescents withhigh-risk B-cell non-Hodgkin lymphoma (B-NHL)and mature acute leukemia (B-AL): evaluation ofrituximab (R) efficacy in addition to standard LMBchemotherapy (CT) regimen. J Clin Oncol.2016;34(15 Suppl):10507.
147. Deconinck E, Miadi-Fargier H, Pen CL, Brice P. Costeffectiveness of rituximab maintenance therapy infollicular lymphoma: long-term economic evalua-tion. Pharmacoeconomics. 2010;28:35–46.
148. Ray JA, Carr E, Lewis G, Marcus R. An evaluation ofthe cost-effectiveness of rituximab in combinationwith chemotherapy for the first-line treatment offollicular non-Hodgkin’s lymphoma in the UK.Value Health. 2010;13:346–57.
149. Soini EJ, Martikainen JA, Nousiainen T. Treatmentof follicular non-Hodgkin’s lymphoma with orwithout rituximab: cost-effectiveness and value ofinformation based on a 5-year follow-up. AnnOncol. 2011;22:1189–97.
150. Griffiths RI, Gleeson ML, Mikhael J, Danese MD.Impact on medical cost, cumulative survival, andcost-effectiveness of adding rituximab to first-linechemotherapy for follicular lymphoma in elderlypatients: an observational cohort study based onSEER-Medicare. J Cancer Epidemiol.2012;2012:978391.
151. Hornberger J, Chien R, Friedmann M, et al.Cost-effectiveness of rituximab as maintenancetherapy in patients with follicular non-Hodgkinlymphoma after responding to first-line rituximabplus chemotherapy. Leuk Lymphoma.2012;53:2371–7.
152. Blommestein HM, Issa DE, Pompen M, et al.Cost-effectiveness of rituximab as maintenancetreatment for relapsed follicular lymphoma: resultsof a population-based study. Eur J Haematol.2014;92:398–406.
2272 Adv Ther (2017) 34:2232–2273

153. Chen Q, Ayer T, Nastoupil LJ, Rose AC, Flowers CR.Comparing the cost-effectiveness of rituximabmaintenance and radioimmunotherapy consolida-tion versus observation following first-line therapyin patients with follicular lymphoma. Value Health.2015;18:189–97.
154. Prica A, Chan K, Cheung M. Frontline rituximabmonotherapy induction versus a watch and waitapproach for asymptomatic advanced-stage follicu-lar lymphoma: a cost-effectiveness analysis. Cancer.2015;121:2637–45.
155. Johnston KM, Marra CA, Connors JM, NajafzadehM, Sehn L, Peacock SJ. Cost-effectiveness of theaddition of rituximab to CHOP chemotherapy infirst-line treatment for diffuse large B-cell lym-phoma in a population-based observational cohortin British Columbia, Canada. Value Health.2010;13:703–11.
156. Griffiths RI, Gleeson ML, Mikhael J, Dreyling MH,Danese MD. Comparative effectiveness and cost ofadding rituximab to first-line chemotherapy forelderly patients diagnosed with diffuse large B-celllymphoma. Cancer. 2012;118:6079–88.
157. Khor S, Beca J, Krahn M, et al. Real world costs andcost-effectiveness of rituximab for diffuse largeB-cell lymphoma patients: a population-basedanalysis. BMC Cancer. 2014;14:586.
158. Hornberger J, Reyes C, Shewade A, et al. Cost-ef-fectiveness of adding rituximab to fludarabine andcyclophosphamide for the treatment of previouslyuntreated chronic lymphocytic leukemia. LeukLymphoma. 2012;53:225–34.
159. Adena M, Houltram J, Mulligan SP, Todd C, Mala-nos G. Modelling the cost effectiveness of rituximabin chronic lymphocytic leukaemia in first-line
therapy and following relapse. Pharmacoeco-nomics. 2014;32:193–207.
160. Mandrik O, Corro Ramos I, Knies S, Al M, SeverensJL. Cost-effectiveness of adding rituximab to flu-darabine and cyclophosphamide for treatment ofchronic lymphocytic leukemia in Ukraine. CancerManag Res. 2015;7:279–89.
161. Muller D, Fischer K, Kaiser P, et al. Cost-effective-ness of rituximab in addition to fludarabine andcyclophosphamide (R-FC) for the first-line treat-ment of chronic lymphocytic leukemia. Leuk Lym-phoma. 2016;57:1130–9.
162. Danese MD, Reyes CM, Gleeson ML, Halperin M,Skettino SL, Mikhael J. Estimating the populationbenefits and costs of rituximab therapy in the Uni-ted States from 1998 to 2013 using real-world data.Med Care. 2016;54:343–9.
163. Tobinai K, Klein C, Oya N, Fingerle-Rowson G. Areview of obinutuzumab (GA101), a novel type IIanti-CD20 monoclonal antibody, for the treatmentof patients with B-cell malignancies. Adv Ther.2017;34:324–56.
164. Goede V, Klein C, Stilgenbauer S. Obinutuzumab(GA101) for the treatment of chronic lymphocyticleukemia and other B-cell non-Hodgkin’s lym-phomas: a glycoengineered type II CD20 antibody.Oncol Res Treat. 2015;38:185–92.
165. Cang S, Mukhi N, Wang K, Liu D. Novel CD20monoclonal antibodies for lymphoma therapy.J Hematol Oncol. 2012;5:64.
166. Jaglowski SM, Alinari L, Lapalombella R, et al. Theclinical application of monoclonal antibodies inchronic lymphocytic leukemia. Blood.2010;116:3705–14.
Adv Ther (2017) 34:2232–2273 2273