HEREDITARY BREAST CANCER IN DEVELOPING
COUNTRIES
Prof. Richard Pestell
Prof. Jan Lubinski
Prof. T.Rajkumar
QUESTIONS TO BE DISCUSSED
• What is cancer genetic counseling?• Issues related to setting up a Hereditary
cancer programme in a developing country?
• Socio-economic issues in India and in the West.
• Financial implications in testing.• Guidelines in gene testing• What could be the take home message.
Assessing the Genetic Risks of Cancer
• If the family history reveals one or more of the following features, then a further assessment is warranted:
cancer in two or more close relatives multiple primary tumors in the same individual bilateral cancer in paired organs an earlier-than-usual onset of cancer a specific constellation of tumors that comprise a known
cancer syndrome
• If one of these features are found in the individual's own or family history, familial or hereditary factors should be considered and further evaluated.
Cancer Risk Counseling
• In contrast to "traditional" genetic counseling, which often focuses on reproductive risks, those seeking cancer risk counseling are usually at an increased risk of developing cancer themselves.
• Therefore, much of the discussion and focus of cancer risk counseling concerns the individual's personal risk of developing a disease.
Cancer Risk Counseling• Thus, those who provide cancer risk counseling
should: emphasize prevention of cancer, convey recommendations for surveillance, discuss life-style modifications that may
reduce the risk of developing cancer, and provide an assessment of risk to the
individual and other family members. Gene testing – implications of a positive,
negative or uninformative test result
Assessing the Genetic Risks of Cancer
• The two major decision points in the assessment of cancer risk are:
Is the risk of cancer higher or lower than in the general population?
Is the risk higher or lower than that perceived by the patient?
Assessing the Genetic Risks of Cancer
• The family history questionnaire provides the initial information to answer the first question—individuals with negative family histories and minimal family concerns should be counseled as such, putting their concerns in the context of the general population risk. Cancer screening and prevention information are probably all that is needed.
Assessing the Risks of Hereditary Cancer Syndromes
• Although the specific genes involved in several hereditary cancer syndromes have been discovered, the initial identification of families with these syndromes is based on clinical and family history criteria.
• Hereditary cancer syndromes follow Mendelian inheritance patterns...usually autosomal dominant with reduced penetrance and variable expressivity.
PENETRANCE AND EXPRESSIVITY
• The parent transmitting the gene did not show the trait, even though he or she carried the allele; this is known as incomplete penetrance, that is, the inconsistent phenotypic expression of a gene even though the gene is present.
• The parent of the affected individual expressed the gene but in ways that were not readily recognized; this is known as variable expressivity.
MATERIALS
Hereditary breast and ovarian cancer study
Total number of cases studied – 80
Hereditary Breast Cancer Families - 26
Hereditary Breast and Ovarian Cancer Families - 15
Hereditary Ovarian Cancer Families - 3
Breast and Ovarian Cancer cases - 3
Early onset Breast Cancer cases - 29
Early onset Ovarian Cancer cases - 3
Hereditary Prostate and Breast Cancer families -1
CRITERIA FOR GENETIC TESTING
HBOC STUDY
Early onset of breast cancer ( at or less than 35 years of age).
Two cases of breast cancer diagnosed under the age of 50 years.
Three cases of breast cancer diagnosed under 60 years of age.
Four or more cases of breast cancer diagnosed at any age.
Presence of breast and ovarian cancer in the family or in the same individual.
Male breast cancer with a relative (of either sex) with breast cancer.
CRITERIA FOR GENETIC TESTING
DHPLC
Reverse phase ion exchange chromatography
DHPLC analysis – All fragments analyzed at a basal temperature of 50°C plus two or more higher partial denaturing temperatures.
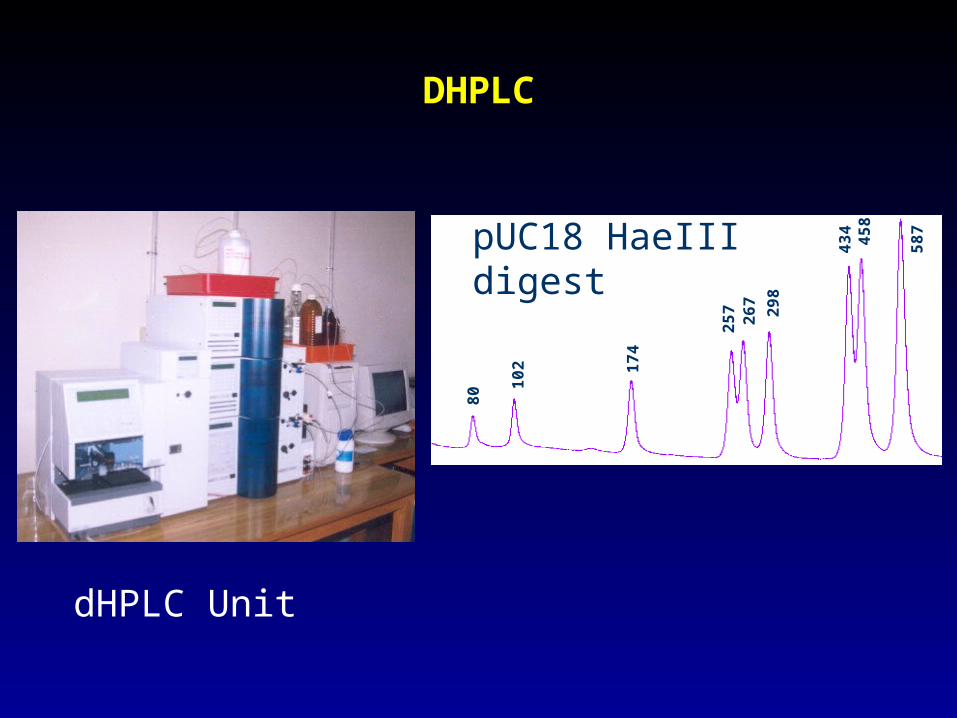
The DHPLC system’s performance was validated with pUC18 HaeIII digest once every 200 runs.
DHPLC
dHPLC Unit
pUC18 HaeIII digest
80
43
4
10
2 17
4
29
8
26
72
57
45
8
58
7
METHODS - SEQUENCING
Cycle sequencing was done with both forward and reverse primers in separate reaction and run in ABI 310 Genetic Analyzer.
The sequences were analyzed in Sequence Analysis v 3.4.1.
For the samples that showed mutation, DNA from fresh aliquot of lymphocytes was used to sequence again to confirm the results.
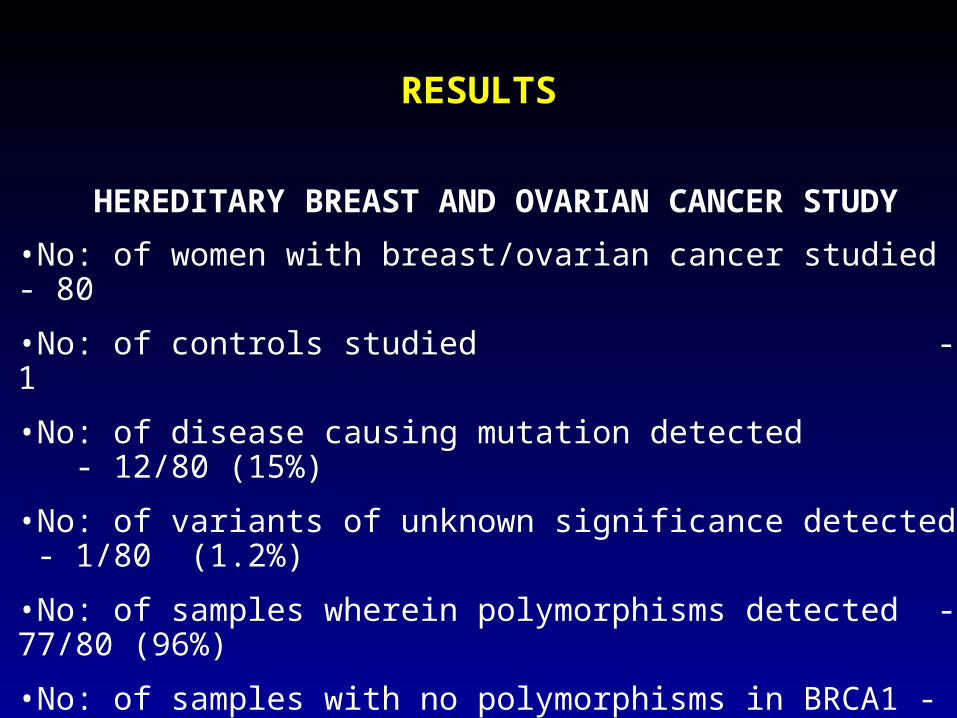
RESULTS
HEREDITARY BREAST AND OVARIAN CANCER STUDY
•No: of women with breast/ovarian cancer studied - 80
•No: of controls studied - 1
•No: of disease causing mutation detected - 12/80 (15%)
•No: of variants of unknown significance detected - 1/80 (1.2%)
•No: of samples wherein polymorphisms detected - 77/80 (96%)
•No: of samples with no polymorphisms in BRCA1 - 20/80 (25%)
•No: of samples with no polymorphisms in BRCA2 - 10/80 (12.5%)
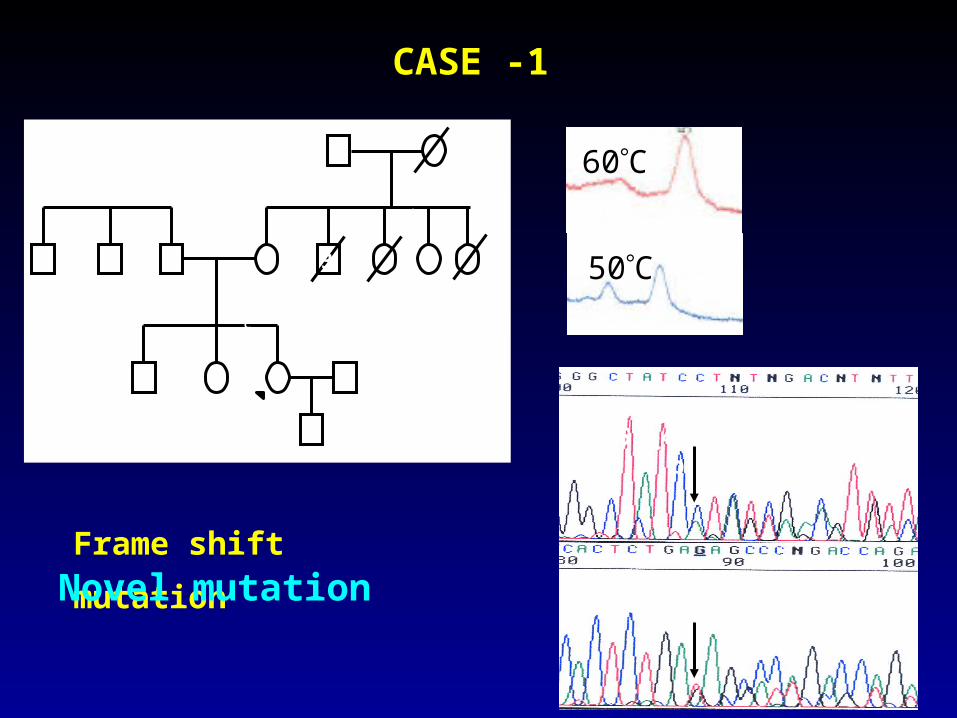
CASE -1
50C
60C
B1 E12 - c.4158_4162delCTCTC; p.Ser1369Ser fsX2
50
2 3362
28
6
50
Breast44
3
Breast
Breast50
Breast
Frame shift mutation
Novel mutation
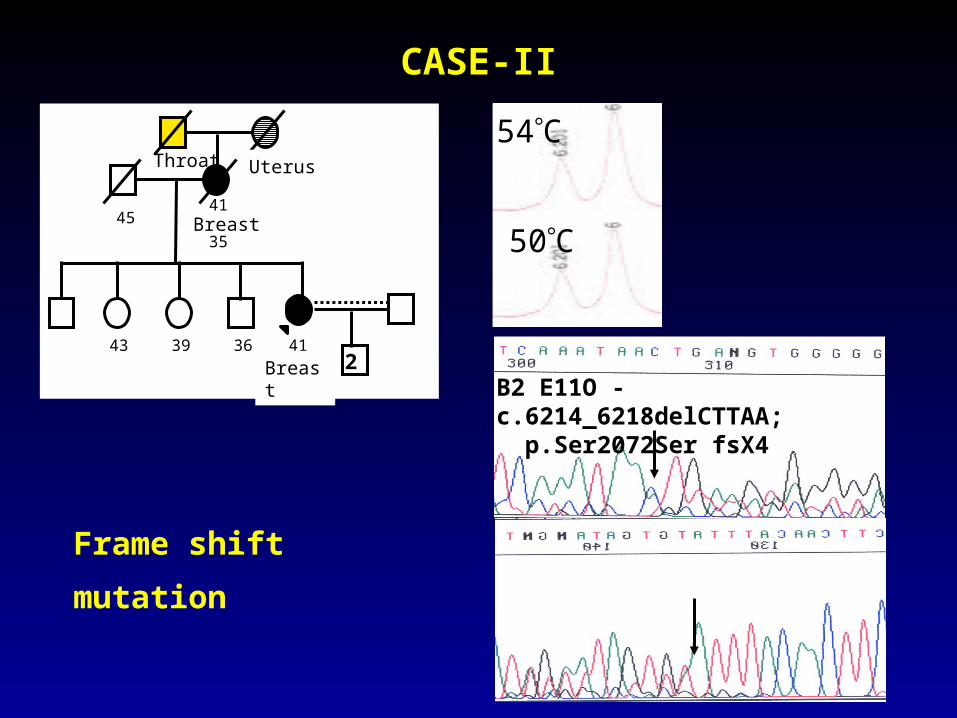
CASE-II
Throat
4541
Uterus
43 36
35
39 41
Breast
Breast
2
Throat
B2 E11O - c.6214_6218delCTTAA; p.Ser2072Ser fsX4
54C
50C
Frame shift mutation
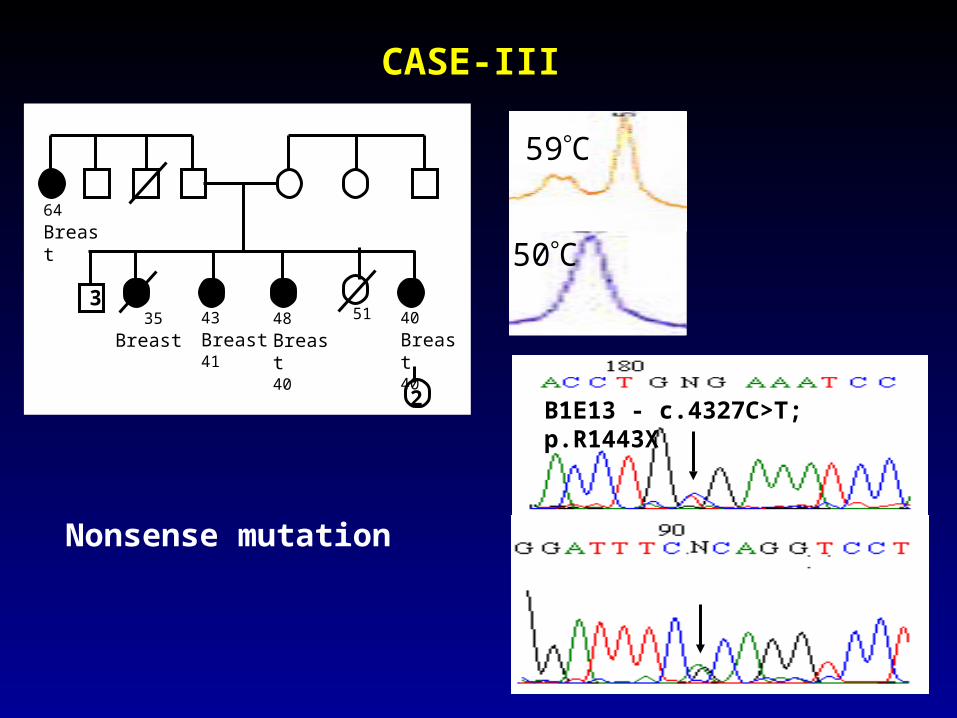
CASE-III
50C
59C
64
Breast
2
48
Breast40
43
Breast41
35
Breast
513
40
Breast40
B1E13 - c.4327C>T; p.R1443X
Nonsense mutation
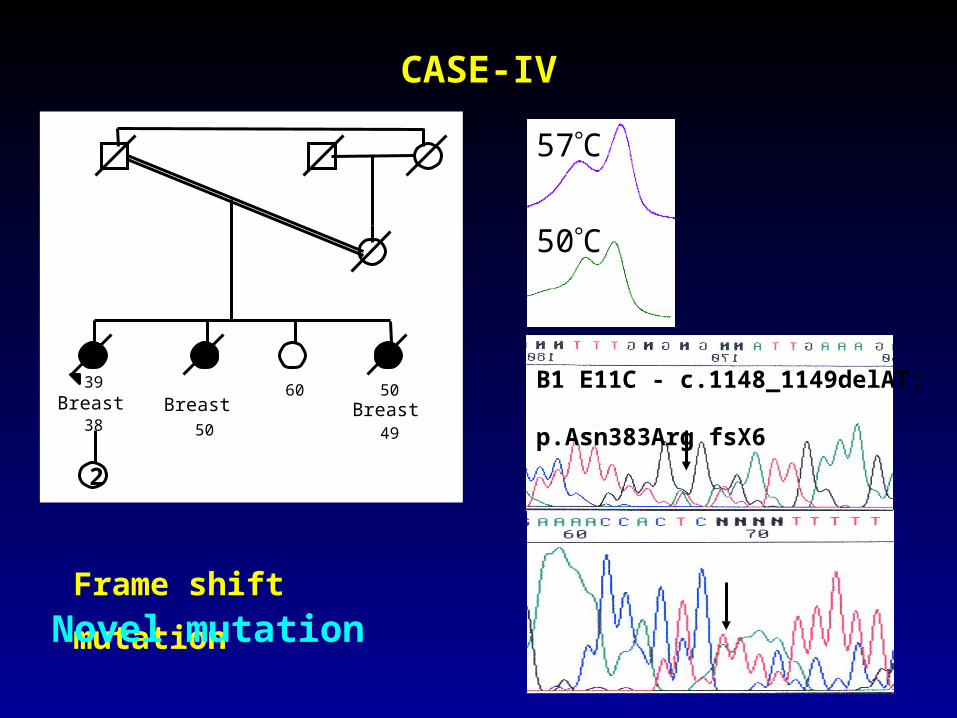
CASE-IV
B1 E11C - c.1148_1149delAT; p.Asn383Arg fsX6
50C
57C
2
39Breast
38Breast
50
60 50Breast
49
2
Frame shift mutation
Novel mutation
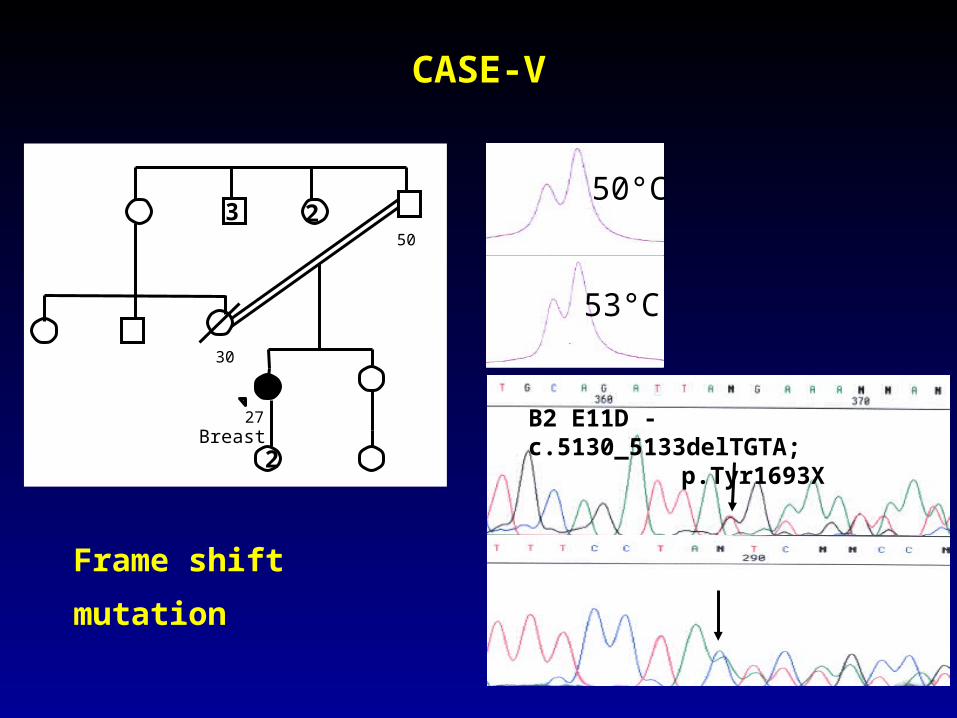
CASE-V
53°C
50°C
B2 E11D - c.5130_5133delTGTA; p.Tyr1693X
30
50
27Breast
2
3 2
Frame shift mutation
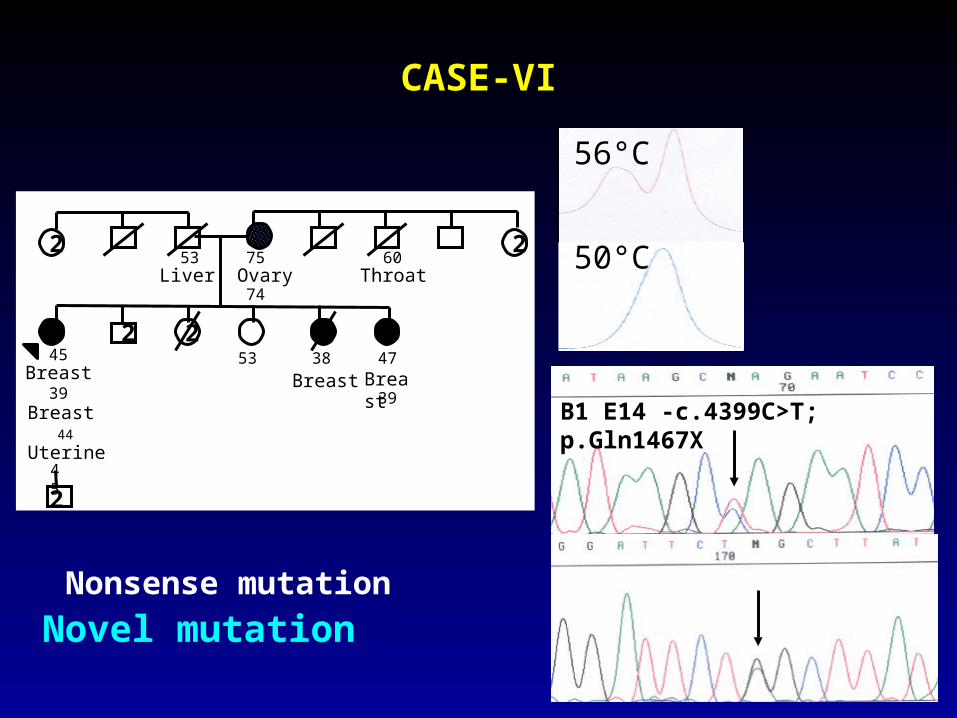
CASE-VI
56°C
50°C
B1 E14 -c.4399C>T; p.Gln1467X
75Ovary74
53Liver
60Throat
45Breast
39Breast
Uterine45
53 38
Breast 47
Breast 39
2
2
2
2
2
44
Nonsense mutation
Novel mutation
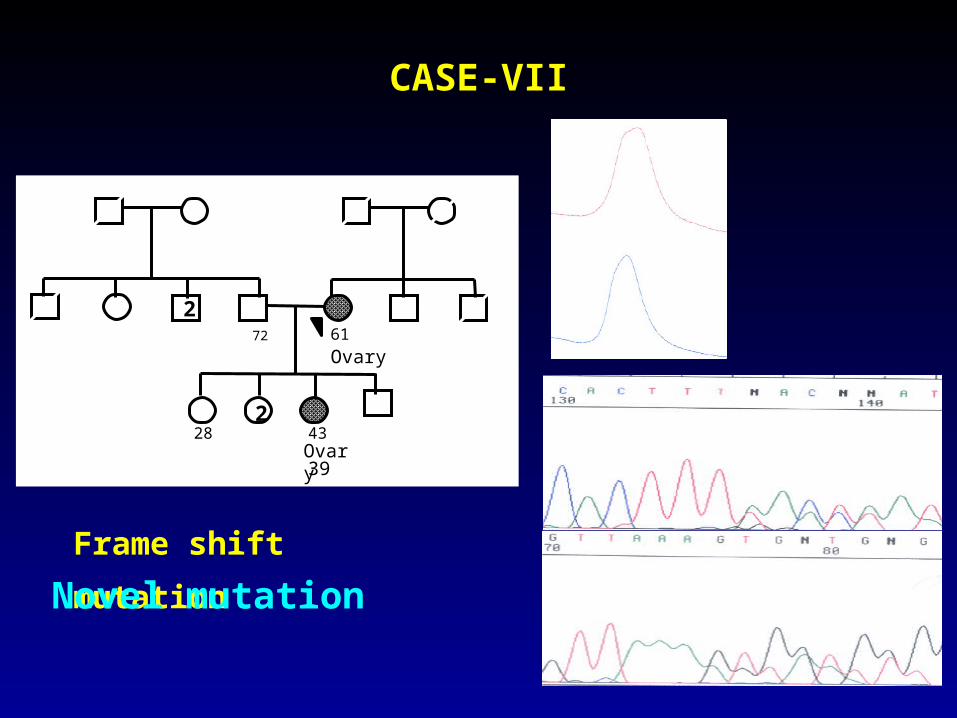
CASE-VII
50°C
56°C
61
Ovary72
2
282
43Ovary39
B1 E17 - c.5024_5025insT; p. Thr1675Thr fsX4
Frame shift mutation
Novel mutation
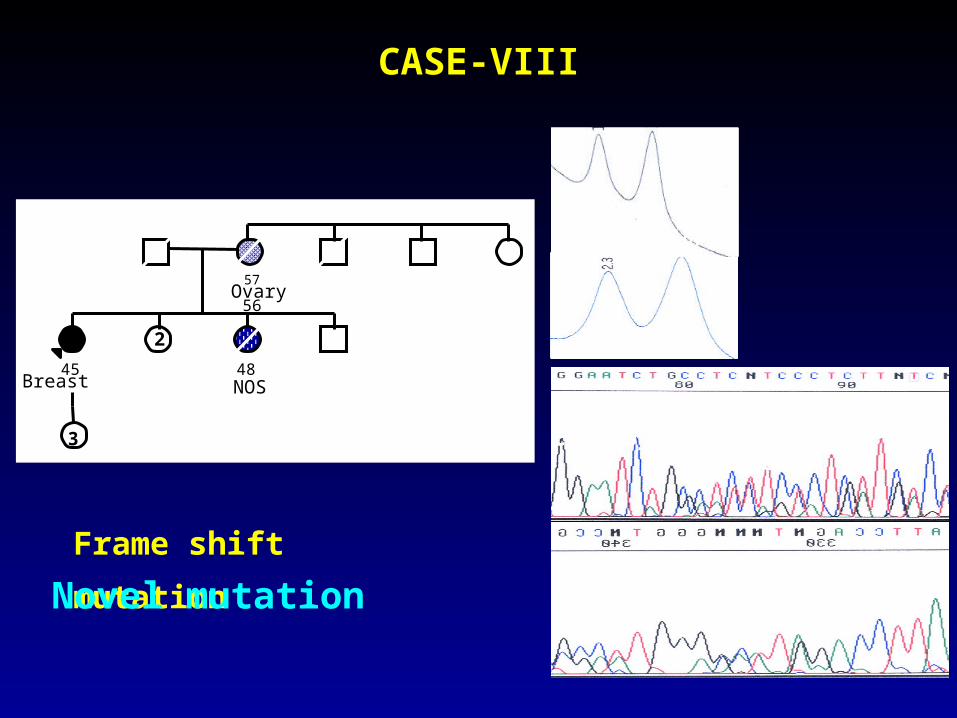
CASE-VIII
50°C
59°C
B1EX16- c.4705_4706insTGGAATC; p.Ilefsx5
57Ovary
56
Breast45
2
NOS48
3
3
Frame shift mutation
Novel mutation
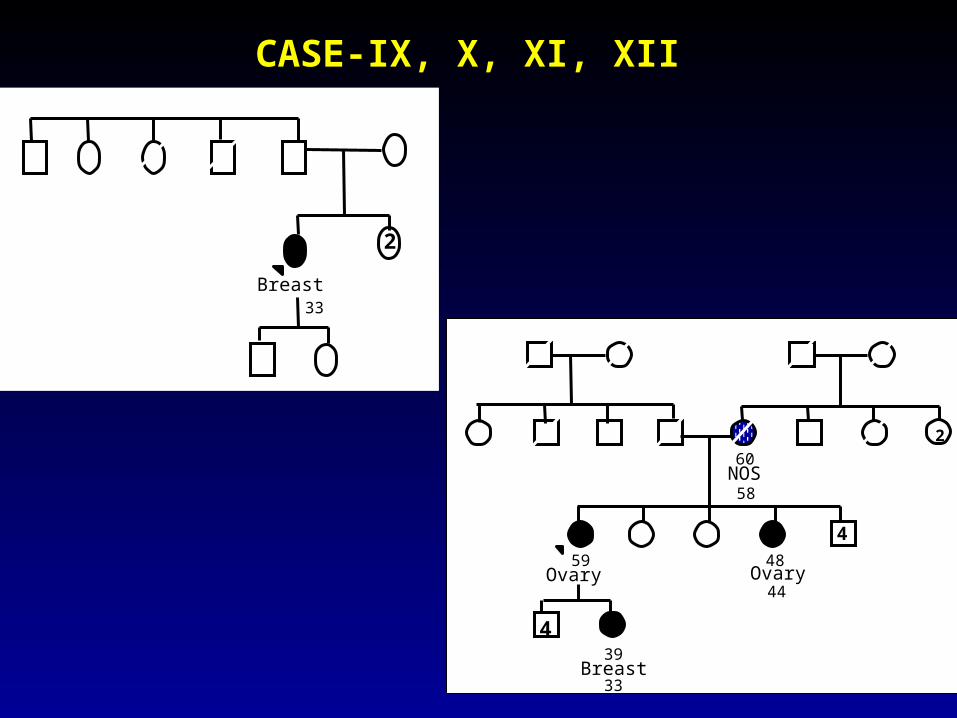
CASE-IX, X, XI, XII
33
Breast
2
60NOS
58
2
59Ovary
48Ovary
44
4
439
Breast 33
5058
Breast33
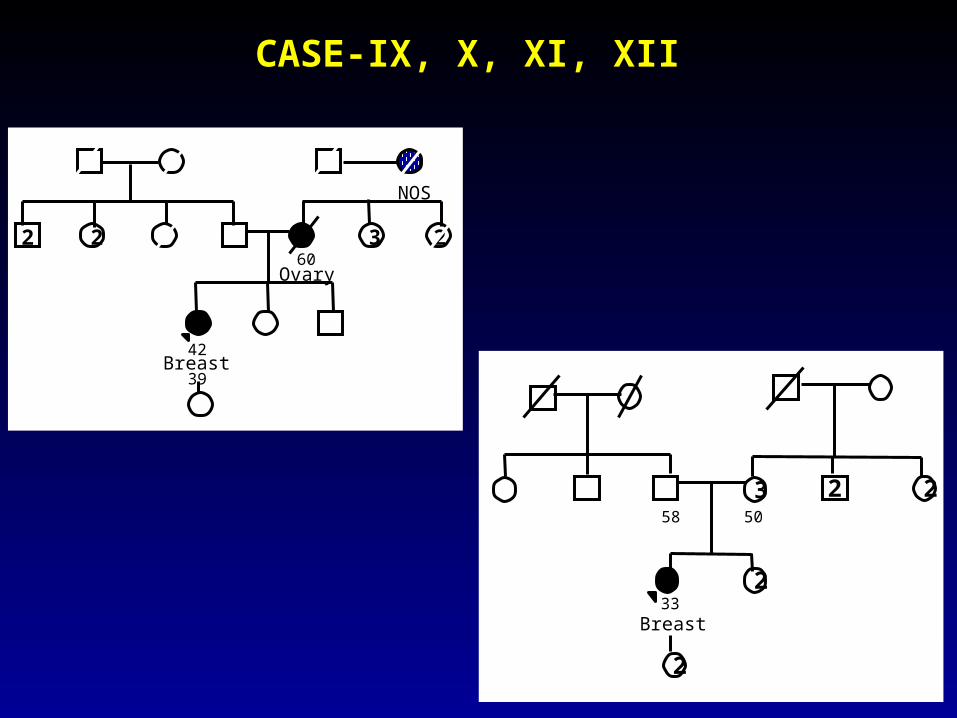
3
2
22
2
NOS
60Ovary
3 222
42Breast
39
CASE-IX, X, XI, XII
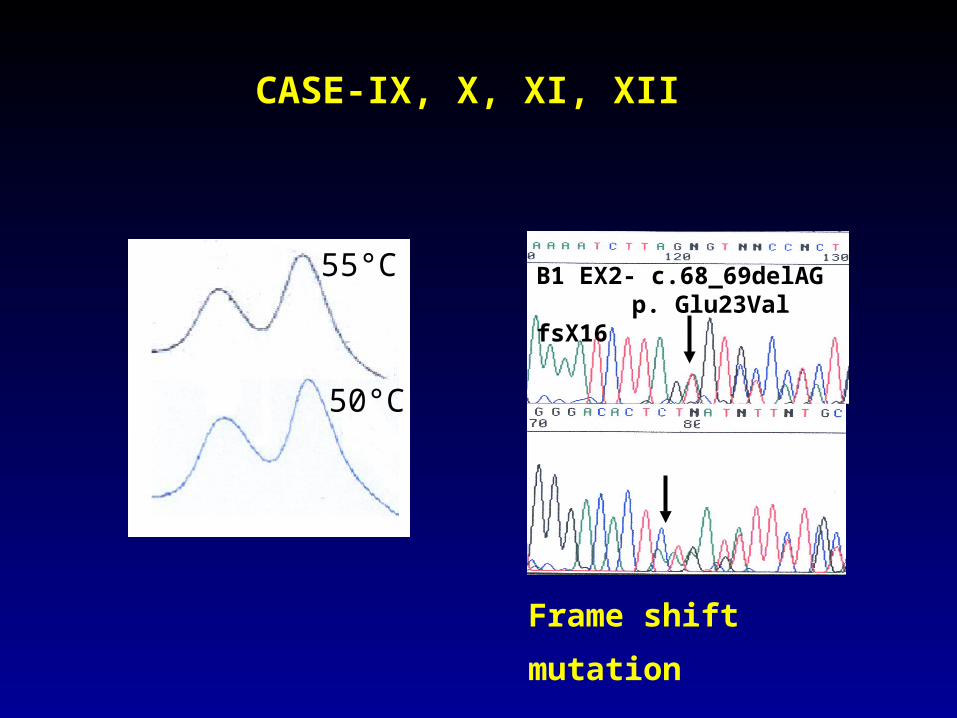
50°C
55°C B1 EX2- c.68_69delAG p. Glu23Val fsX16
CASE-IX, X, XI, XII
Frame shift mutation
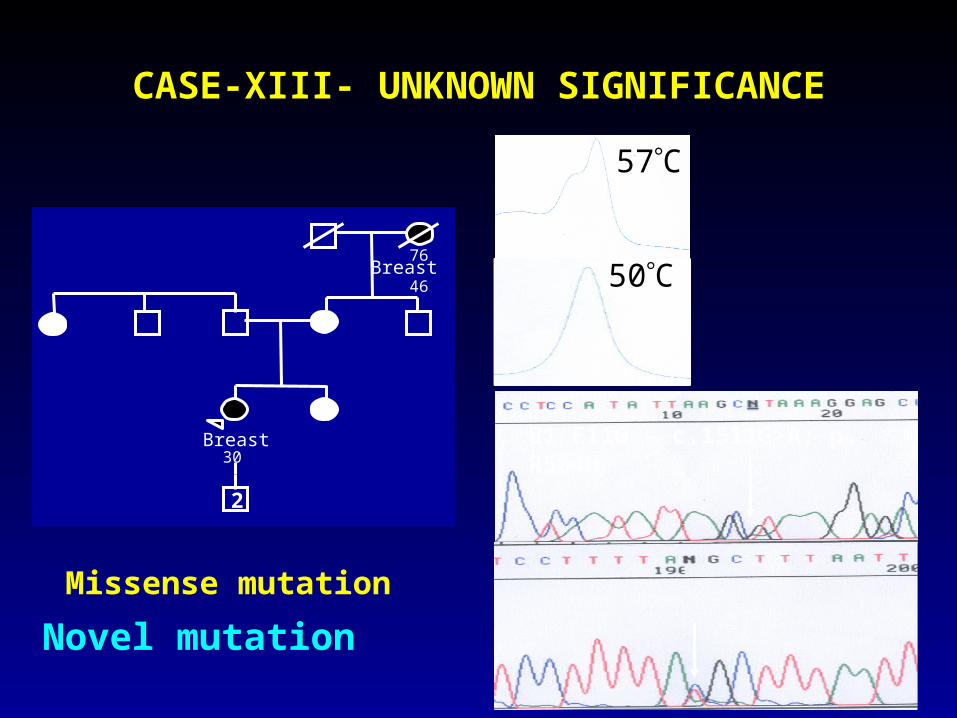
CASE-XIII- UNKNOWN SIGNIFICANCE
B1 E11G – c.1511G>A; p. R504HBreast30
76Breast
46
4
2
4
50C
57C
Missense mutation
Novel mutation
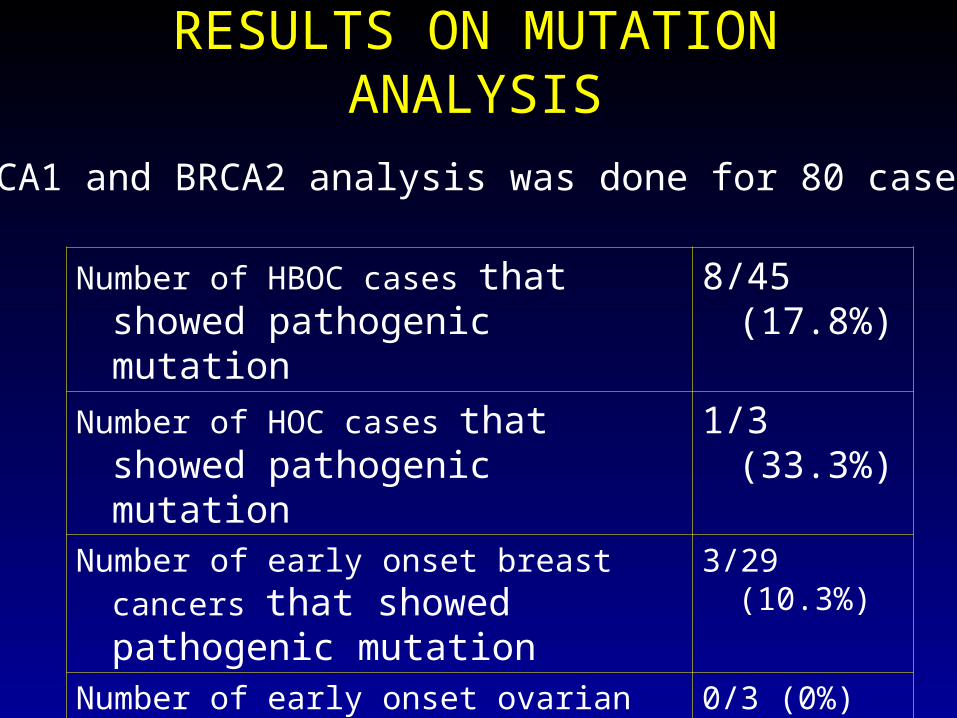
RESULTS ON MUTATION ANALYSIS
BRCA1 and BRCA2 analysis was done for 80 cases
Number of HBOC cases that showed pathogenic mutation
8/45 (17.8%)
Number of HOC cases that showed pathogenic mutation
1/3 (33.3%)
Number of early onset breast cancers that showed pathogenic mutation
3/29 (10.3%)
Number of early onset ovarian cancers that showed pathogenic mutation
0/3 (0%)
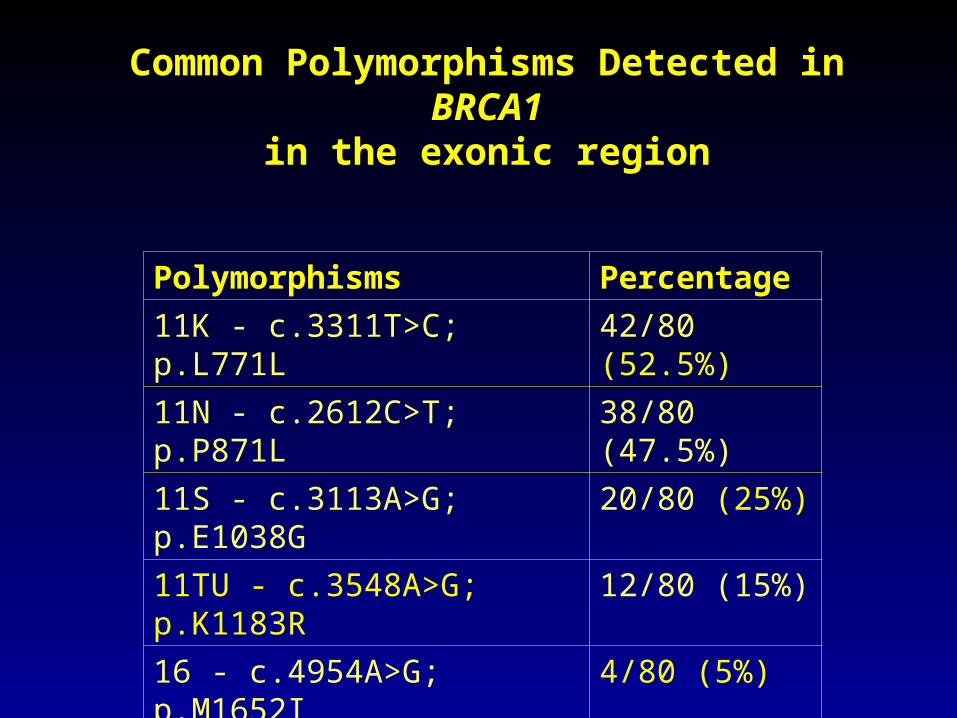
Common Polymorphisms Detected in BRCA1in the exonic region
Polymorphisms Percentage
11K - c.3311T>C; p.L771L 42/80 (52.5%)
11N - c.2612C>T; p.P871L 38/80 (47.5%)
11S - c.3113A>G; p.E1038G 20/80 (25%)
11TU - c.3548A>G; p.K1183R 12/80 (15%)
16 - c.4954A>G; p.M1652I 4/80 (5%)
16 - c.4839G>A; p.S1613G 4/80 (5%)
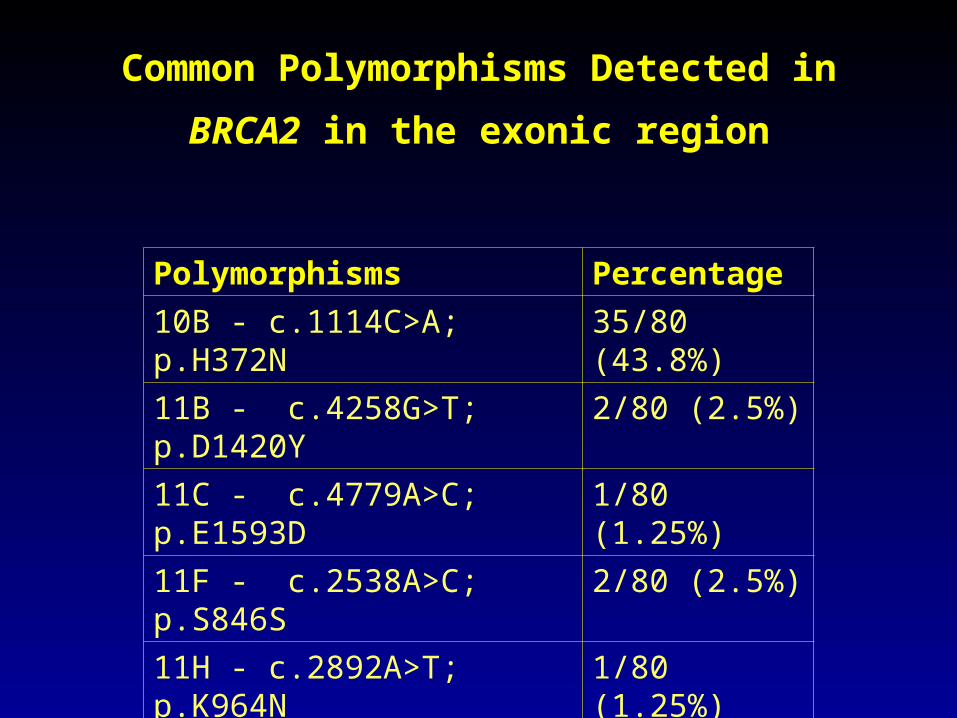
Common Polymorphisms Detected in BRCA2
in the exonic region
Polymorphisms Percentage
10B - c.1114C>A; p.H372N 35/80 (43.8%)
11B - c.4258G>T; p.D1420Y 2/80 (2.5%)
11C - c.4779A>C; p.E1593D 1/80 (1.25%)
11F - c.2538A>C; p.S846S 2/80 (2.5%)
11H - c.2892A>T; p.K964N 1/80 (1.25%)
11I - c.2971A>G; p.N991D 5/80 (6.25%)
11K - c.3807T>C; p.V1269V 4/80 (5%)
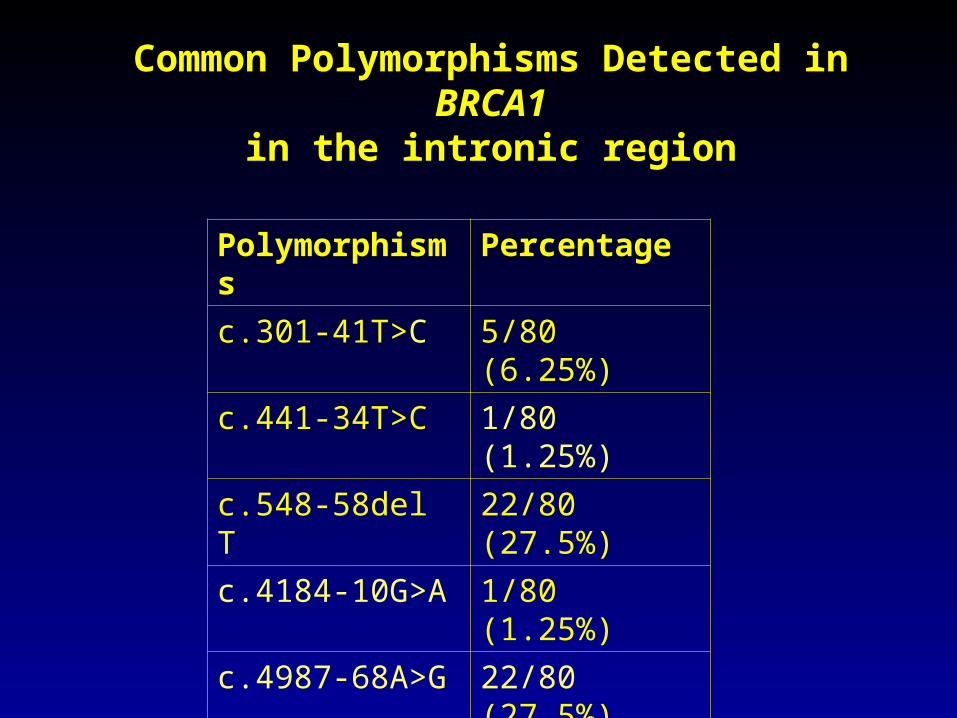
Common Polymorphisms Detected in BRCA1in the intronic region
Polymorphisms Percentage
c.301-41T>C 5/80 (6.25%)
c.441-34T>C 1/80 (1.25%)
c.548-58del T 22/80 (27.5%)
c.4184-10G>A 1/80 (1.25%)
c.4987-68A>G 22/80 (27.5%)
c.4987-92A>G 22/80 (27.5%)
c.5075+66G>A 5/80 (8.1%)
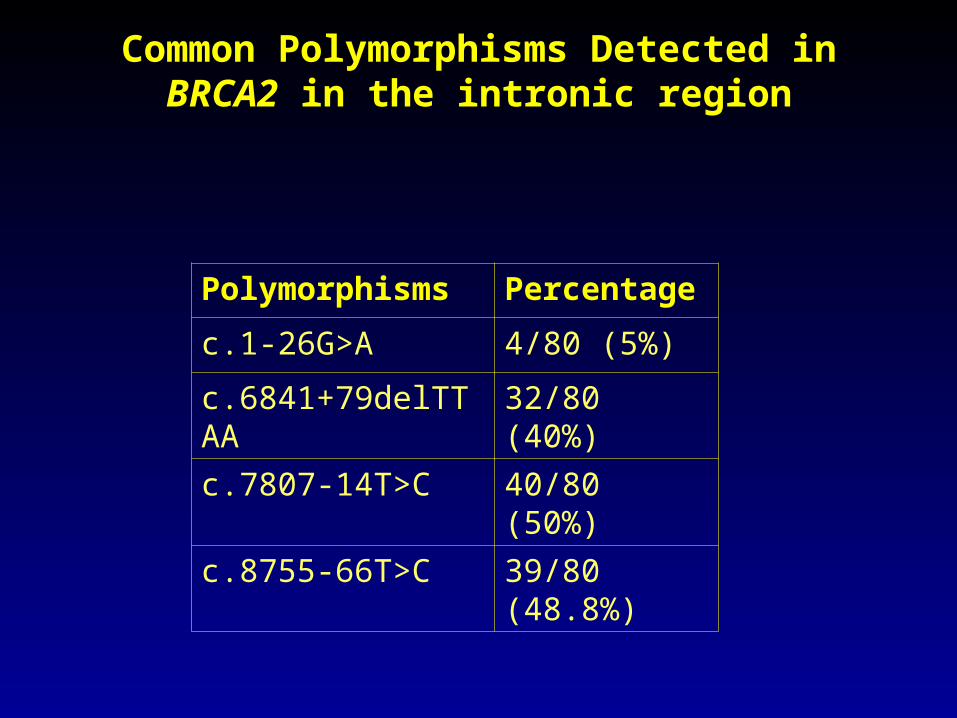
Common Polymorphisms Detected in BRCA2 in the intronic region
Polymorphisms Percentage
c.1-26G>A 4/80 (5%)
c.6841+79delTTAA 32/80 (40%)
c.7807-14T>C 40/80 (50%)
c.8755-66T>C 39/80 (48.8%)
QUESTIONS TO BE DISCUSSED
• What is cancer genetic counseling?• Issues related to setting up a Hereditary
cancer programme in a developing country?
• Socio-economic issues in India and in the West.
• Financial implications in testing.• Guidelines in gene testing• What could be the take home message.
Recommended