-
UvA-DARE is a service provided by the library of the University
of Amsterdam (https://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Diagnostic guidelines for chronic ankle pain. From loose bodies
to joint venture
Verhagen, R.A.W.
Publication date2004
Link to publication
Citation for published version (APA):Verhagen, R. A. W. (2004).
Diagnostic guidelines for chronic ankle pain. From loose bodies
tojoint venture.
General rightsIt is not permitted to download or to
forward/distribute the text or part of it without the consent of
the author(s)and/or copyright holder(s), other than for strictly
personal, individual use, unless the work is under an opencontent
license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital
publication of certain material infringes any of your rights or
(privacy) interests, pleaselet the Library know, stating your
reasons. In case of a legitimate complaint, the Library will make
the materialinaccessible and/or remove it from the website. Please
Ask the Library: https://uba.uva.nl/en/contact, or a letterto:
Library of the University of Amsterdam, Secretariat, Singel 425,
1012 WP Amsterdam, The Netherlands. Youwill be contacted as soon as
possible.
Download date:05 Jul 2021
https://dare.uva.nl/personal/pure/en/publications/diagnostic-guidelines-for-chronic-ankle-pain-from-loose-bodies-to-joint-venture(ded9a4f5-59da-4800-ac56-fb303e842b23).html
-
Chapter r
I n t r o d u c t i on n a nd d
A i mm of t h is thes is
-
Chapterr 1
Introductio n n Chronicc ankle pain Inversionn sprains of the
ankle and ankle fractures are common injuries. In 2002, in The
Netherlands,, 78,000 patients presented at hospital emergency
departments with ankle injuries,
59%% of which were treated for an inversion sprain.1 In more
than 40% of cases the injuries
weree sports-related. Most patients with sprains of the lateral
ligaments are young working
adults.11 These patients place a large demand on the healthcare
system and are often temporarily
disabledd due to the ankle injury. This leads to higher
healthcare costs and loss of productivity.
Althoughh most patients go on to an uncomplicated recovery,
those who continue to have
painn in the ankle and hindfoot can present a diagnostic
problem.2 This is known as chronic
anklee pain.
Causess of chronic ankle pain Thee causes of chronic ankle pain
can be divided into three main groups: intra-articular, extra-
articular,, and peri-articular (Table). Nowadays most
intra-articular conditions can be treated
byy means of an arthroscopic procedure. In the past
extra-articular and peri-articular causes
weree not an indication for arthroscopy, however currently
tendonitis, os trigonum syndrome,
andd subtalar pathology can all be treated by soft tissue
endoscopy.3"10
Tablee Causes of chronic ankle pain
Intra-articularr Bony impingement Softt tissue impingement
Osteochondrall lesion Loosee bodies Osteoarthritis s Infection n
Neoplasm m Rheumaticc diseases
rheumatoidd arthritis pigmentedd villonodular synovitis
synoviall chondromatosis hemophilia a otherr inflammatory
arthritides (gout, chondrocalcinosis, Crohn disease)
Extra-articularr Subtalar pathology Vascularr / neurological
problems Neoplasm m
Peri-articularr Chronic instability Syndesmoticc injury Oss
trigonum syndrome Tendonitiss TA/TP/FHL/Per * Recurrentt peroneal
tendon (sub-) luxation Tarsall tunnel syndrome
** TA = Tibialis Anterior tendon TPP = Tibialis Posterior tendon
FHLL = Flexor Hallucis Longus tendon Perr = Peroneal tendon
11 1
-
Introductionn and Aim of this thesis
Impingement t
Thee most important cause of residual ankle pain is impingement.
This can be divided into
bonyy or soft tissue impingement.
Bonyy impingement
Anteriorr impingement spurs in the ankle were first described by
Morris in 1943, and later by
McMurrayy and O'Donoghue.11 Anterior bony impingement is a
common cause of chronic pain
inn the ankle, especially in athletes. It is a clinical
diagnosis, caused by anteriorly located bony
impediments.12"188 It is characterized by anterior pain,
aggravated by repetitive movements, and
restrictedd dorsiflexion.19 Physical examination reveals pain on
palpation over the anterior aspect
off the ankle joint with recognition of the pain. The
differentiation between anterolateral and
anteromediall impingement is generally accepted.19-20 Standard
AP and lateral radiographs are
usedd to detect the presence or absence of osteophytes.11 In
patients with anterior talar and/or
tibiall spurs, these spurs are regarded as the cause of the
anterior bony impingement
syndrome.14"16,211 Due to their location they can lead to the
"kissing" phenomenon and
concomitantt pinching of hypertrophic synovial tissue. This
results in a limited dorsiflexion
withh associated symptoms of impingement.12
Althoughh it is a recognized clinical diagnosis, some authors
state that additional diagnostic
evaluationn is necessary to differentiate between symptomatic
and asymptomatic lesions.22
Bonee scans may show increased uptake in the area of impingement
in symptomatic lesions,
whilee computed tomography (CT) can be helpful to determine the
precise anatomical location
andd medial and lateral extent of the osteophyte
preoperatively.
Inn ankles with no severe osteoarthritic changes, arthroscopic
treatment of the anterior
impingementt syndrome has produced good
results.11"14,16,19,23"27
Softt tissue impingement
Thee clinical diagnosis of soft tissue impingement is one of
exclusion. In patients with clinical
signss of an anterior ankle impingement syndrome and no visible
osteophytes on radiography,
thee diagnosis of anterior soft tissue impingement syndrome is
made. Similar symptoms can
occurr in chronic ankle instability, peroneal tendon tears or
subluxations, sinus tarsi syndrome,
stresss fractures, loose bodies, osteochondral lesions, bony
impingement, and degenerative
jointt disease.28 Patients with the soft tissue impingement
syndrome present with anterolateral
anklee pain and tenderness after sprains, fractures, or
surgery.24,28 Other clinical signs include
exacerbationn of the pain on dorsiflexion and an effusion.24
28,29
Ann magnetic resonance imaging (MRI) finding of an abnormal soft
tissue structure within the
anterolaterall ankle gutter, as distinct from the anterior
tibiofibular ligament and chondromalacia
off the talus, suggests the diagnosis of anterolateral soft
tissue impingement.14,20,28
Thee predictive outcome in treating synovial impingement may be
compromised when
12 2
-
Chapterr 1
documentedd ankle instability is present. Therefore, it is
recommended that patients with
associatedd chronic ankle instability should have ankle ligament
reconstruction as their initial
treatment.26 6
Iff in patients with clinical signs of an anteromedial ankle
impingement syndrome, routine
radiographss show no abnormalities, a soft tissue impediment can
be expected. However, it
hass been demonstrated that in the majority of these patients an
anteromedially located
osteophytee can be present.30 The reason being that in the
standard lateral projection
anteromediall osteophytes remain undetected due to superposition
or overprojection of the
moree prominent anterolateral border of the distal tibia.19
Severall authors have stated that surgical distinction between
normal variant bony and soft
tissuee and pathological conditions is difficult, due to subtle
variations in joint anatomy.31,32
Anteromediall bony spurs are often poorly visualized at
arthroscopy and can be easily missed
particularlyy in patients with accompanying secondary synovial
reflections overlying the
concealedd osteophytes.33 As radiographic classification of the
spur formation has proven to be
correlatedd with the outcome of surgery, detection of these
osteophytes is important for a precise
diagnosis,, defining a treatment plan, the peroperative
procedure and the final outcome.1119'34,35
Osteochondrall lesion Anotherr important cause of residual pain
after an ankle sprain is osteochondral lesion of the
taluss (OLT). It is defined as the separation of a fragment of
articular cartilage, with or without
subchondrall bone.36"38 The incidence of OLT after an ankle
sprain is probably underestimated
becausee these lesions often remain undetected. The incidence
has been reported to be as high
ass 6.5% after ankle sprains.39,40 OLTs most frequently occur in
young adults with a nearly
equall distribution between the sexes. In the acute situation,
symptoms depend on the amount
off damage to the peri-articular tissues and the involvement of
afferent pain fibres in the
subchondrall bone.
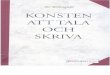
Figuree Arthroscopic view of 42-year old man with persistent
ankle pain after ankle sprain. A.. Posterolateral osteochondral
lesion of talar dome with loose fragment B.. Same lesion after
removal of loose fragment, curettage and drilling
13 3
-
Introductionn and Aim of this thesis
Usually,, the lesion is located in the anterolateral or
posteromedial aspect of the talar dome.
Histologicallyy the medial and lateral lesions are identical,
but morphologically they differ.
Thee lateral lesions are shallow and more wafer shaped,
indicating a shear mechanism of
injury.. In contrast, medial lesions are generally deep, cup
shaped, and located posteriorly,
indicatingg a mechanism of torsional impact.36,41 From the
aetiological point of view, trauma is
thee most common cause of OLT, but idiopathic osteonecrosis may
often be the underlying
pathologicall process. In the literature the latter has been
associated with alcohol abuse, use
off steroids, endocrine disorders and some hereditary
conditions.40,42"47
Althoughh initial symptoms may be absent, in chronic cases most
patients present with
intermittentt pain located deep in the ankle joint which
increases on weight bearing. On physical
examinationn signs are often lacking. A discrete limitation of
range of motion with some synovitis
mayy be present. Local tenderness on palpation with recognition
is absent in most cases.
Sincee there are no specific pathognomonic signs or symptoms, it
is of key importance that the
examiningg physician and radiologist are aware that an
osteochondral lesion could be present.
Thee frequent absence of radiographic changes on conventional
radiography has led to the
usee of more sensitive methods for detection.48,49
Radionuclidee bone scanning,50 CT,51"53 MRI,43,54^7 and
diagnostic arthroscopy58 have been used
too assess the ankle joint for osteochondral lesions.
Theree have been no reports on the accuracy of CT arthrography
for detection of osteochondral
lesionss in the ankle. However, case reports suggest that CT
arthrography may be a useful tool
forr assessing the stability of osteochondral lesion.59
Neverthelesss prospective studies that compare the efficacy of
these modalities in the evaluation
off osteochondral lesions are still absent.60
Loosee bodies
Chondrall and osteochondral loose bodies of the ankle joint are
often caused by trauma (ankle
sprainss and fractures of the ankle and talus), degenerative and
posttraumatic osteoarthritis,
osteochondrall lesion of the talus, and synovial chondromatosis.
Loose bodies are not as common
inn the ankle as in the knee and elbow.61
Loosee bodies may cause locking, catching, swelling, pain, and
decreased range of motion as
theyy float freely within the joint. These symptoms can be
intermittent because the loose
bodiess may become fixed to the synovium and are therefore
asymptomatic, only to recur
whenn the chondral or osteochondral fragments come loose.
Physical examination is usually
unremarkable.. Rarely is there any specific area of tenderness
or a palpable loose body.
Nowadays,, radiographs are still the modality of choice when a
loose body is suspected on
clinicall grounds. However, the false positive rate is quite
high. Lesions that appear to be loose
bodiess on standard radiographs may actually be intracapsular,
or extra-articular in location,
particularlyy in the posterior ankle joint compartment.32
14 4
-
Chapterr 1
Iff additional imaging is requested CT is the modality of
choice. CT arthrography can help
detectt intra-articular loose bodies.62 On MRI loose bodies are
sometimes difficult to identify,
butt in MR arthrography the detection of intra-articular loose
bodies is improved due to the
highh contrast and joint distension.63
Osteoarthr i t is s
AA noteworthy characteristic of the ankle is its resistance to
osteoarthritis. This observation is
reinforcedd when the incidence of osteoarthritis in the ankle is
compared with that of the hip
orr the knee, but ankle osteoarthritis is still a fairly common
sequela of traumatic injuries.64
Diagnosiss is by definition made by standard AP and lateral
weight-bearing radiographs. The
severityy of the osteoarthritic changes of the ankle can be
classified.16
Operativee arthroscopy for osteoarthritis of the ankle has not
been successful.1265 Arthroscopic
debridementt does not offer a cure for all forms of degenerative
joint disease of the ankle.
However,, it does alleviate symptoms in many patients and seems
to resolve symptoms
permanentlyy in some cases of degenerative arthritis.66
Diagnosticc modalities in chronic ankle pain Theree are multiple
imaging options for the assessment of chronic ankle pain, including
stress
radiography,, radionuclide bone scanning, ultrasound, CT, MRI,
and injection procedures.
Injectionn procedures for assessment include arthrography, CT
arthrography, MR arthrography,
andd diagnostic injection with anaesthetics.
Thee first and most important steps in the preoperative
diagnostic process are history taking,
physicall examination, combined with standard AP and lateral
weight bearing radiographs.67
Mostt research on additional diagnostic imaging for chronic
ankle pain has focused on the
accuracyy of one imaging method for specific conditions. Only a
few studies have compared
imagingg methods for a specific condition.68 There have been no
studies comparing imaging
methodss for the assessment of chronic ankle pain of uncertain
aetiology. For example there
havee been no studies specifically addressing the value of plain
films in the assessment of
chronicc ankle pain.68 However, plain films are routinely
obtained as the first option to exclude
arthritis,, infection, fracture, or neoplasm. Because there are
many different tests available for
usee in diagnosing ankle and foot problems, they must be used
judiciously. Therefore, a keen
understandingg of the indications and limitations of each
diagnostic test is mandatory. At
presentt no single test clearly stands out as superior for foot
and ankle problems.
Thee diagnostic modality of choice depends not only on
effectiveness, but also on availability
andd costs. Generally in medical practice there is a growing
awareness of the need for practice
guideliness for diagnosis and treatment of disease. This is also
true of orthopaedic surgery. To
addresss this need for practice guidelines a prospective study
was designed at the Academic
Medicall Center in Amsterdam, The Netherlands.
15 5
-
Introductionn and Aim of this thesis
Questionss that remain
Reviewingg the literature reveals that most studies concerning
chronic ankle pain are
retrospectivee and non-comparable. Nor have there been studies
in which different diagnostic
modalitiess are prospectively compared with particular reference
to their accuracy. Healthcare
financess play an important role and the diagnostic modality
used depends not only on
effectivenesss (accuracy), but also on costs of that modality.
This has led to evidence based
algorithmss ('evidence based medicine').68
Althoughh there are existing orthopaedic and radiological
guidelines for chronic ankle pain,68"70
improvementss in CT and MR imaging and an ever-expanding armoury
of therapeutic options
requiree that these guidelines be continuously updated.
Aimm of this thesis Thee aim of this thesis is to develop
evidence based guidelines for diagnosis of patients with
chronicc ankle pain, especially osteochondral lesions of the
talus.
Inn Chapter 2 the prevalence and incidence of ankle sprains
leading to residual complaints in
thee long term is presented and discussed. The incidence of
residual complaints after lateral
anklee ligament rupture is compared with the data from the
literature.
Inn Chapter 3 a prospective study concerning the need for a
preoperative diagnosis in the
treatmentt of chronic ankle pain is presented. Does the outcome
of an arthroscopic procedure
dependd on having a preoperative diagnosis or not? If it does
then preoperative diagnostic
modalitiess have to be evaluated for their accuracy in patients
with chronic ankle pain.
Consideringg the conclusion of chapter 3 the accuracy of
existing and new diagnostic modalities
forr patients with chronic ankle pain has to be evaluated.
Inn Chapter 4 a new type of radiograph for detecting
anteromedial bony impingement of the
anklee joint is evaluated.
Forr detection of osteochondral lesions of the talar dome and
tibia plafond, ankle distraction
cann be used. In Chapter 5 a new resterilizable non-invasive
distraction device is presented
andd discussed. By using joint distraction in ankle arthroscopy
more posterior localized
osteochondrall lesions can be detected and treated.
Variouss diagnostic modalities for identifying osteochondral
lesions in the ankle are described
inn Chapter 6. It concentrates on single diagnostic strategies
in a prospective cohort study. In
Chapterr 7 the same cohort of patients is used to find the best
combination of diagnostic strategies
forr detection or exclusion of osteochondral lesions in a study
based on decision modelling.
Inn Chapter 8 the results of a systematic review are presented
considering the treatment options
off osteochondral lesions of the talar dome.
16 6
-
Chapterr 1
Inn Chapter 9 an overview of the results of the studies
presented is given and the conclusions
aree discussed. Potential new developments and areas for future
research are described.
-
Introductionn and Aim of this thesis
References s 1.. Consumer Safety Institute. [The Dutch
Injuryy Surveillance System: Ankle injuries]. PersonalPersonal
Communication, 2004.
2.. Verhagen RA, de Keizer G, van Dijk CN: Long-termm follow-up
of inversion trauma of thee ankle. Arch Orthop Trauma Surg
1995;114:92-6. 1995;114:92-6.
3.. van Dijk CN, Kort N: Tendoscopy of the peroneall tendons.
Arthroscopy 1998;14:471-8.
4.. van Dijk CN, Scholten PE, Kort NP: Tendoscopyy (tendon
sheath endoscopy) for overusee tendon injuries. Operative
TechniquesTechniques in Sports Medicine 1997;5:170-8.
5.. van Dijk CN: Hindfoot endoscopy. Sports MedicineMedicine and
Arthroscopy Review 2000;8:365-71. .
6.. van Dijk CN, van Dyk GE, Scholten PE, Kort NP:: Endoscopic
calcaneoplasty. Am J Sports MedMed 2001;29:185-9.
7.. van Dijk CN, Kort N, Scholten PE: Tendoscopyy of the
posterior tibial tendon. ArthroscopyArthroscopy 1997;13:692-8.
8.. van Dijk CN, Scholten PE, Krip s R: A 2-portall endoscopic
approach for diagnosis and treatmentt of posterior ankle pathology.
ArthroscopyArthroscopy 2000;16:871-6.
9.. Zimmer TJ, Ferkel RD: Future developments: Endoscopicc
procedures for the retrocalcaneal bursa,, plantar fascia, and
achilles tendon. In: Whipplee TL ed. Arthroscopic surgery: The
footfoot and the ankle. Philadelphia, USA: Lippincott-Ravenn
Publishers, 1996:31-324.
10.. Frey C, Feder KS, DiGiovanni C: Arthroscopicc evaluation of
the subtalar joint: doess sinus tarsi syndrome exist? Foot Ankle
IntInt 1999;20:185-91.
11.. Scranton PE, Jr., McDermott JE: Anterior tibiotalarr spurs:
a comparison of open versus arthroscopicc debridement. Foot Ankle
1992;13:125-9. .
12.. Biedert R: Anterior ankle pain in sports medicine::
aetiology and indications for arthroscopy.. Arch Orthop Trauma Surg
1991;110:293-7. .
13.. Ferkel RD, Scranton PE, Jr.: Arthroscopy of thee ankle and
foot. J Bone Joint Surg [Am] 1993;75-A:: 1233-42.
14.. Ogilvie-Harri s DJ, Mahomed N, Demazière A:: Anterior
impingement of the ankle treated byy arthroscopic removal of bony
spurs, f Bone JointJoint Surg [BrJ 1993;75-B:437-40.
15.. Ogilvie-Harri s DJ, Gilbar t MK, Chorney K: Chronicc pain
following ankle sprains in athletes:: the role of arthroscopic
surgery. ArthroscopyArthroscopy 1997;13:564-74.
16.. van Dijk CN, Verhagen RA, Tol JL: Arthroscopyy for problems
after ankle fracture. JJ Bone Joint Surg [BrJ 1997;79-B:280-4.
17.. Bal BS, Jones L, Jr.: Arthroscopic resection of aa
chondroblastoma in the knee. Arthroscopy 1995;11:216-9. .
18.. van Dijk CN, Fiévez AW, Heijboer MP, et al.:: Arthroscopy
of the ankle. Acta Orthop 5caW1993;64:9(S253). .
19.. van Dijk CN, Tol JL, Verheyen CC: A prospectivee study of
prognostic factors concerningg the outcome of arthroscopic surgeryy
for anterior ankle impingement. Am J SportsSports Med
1997;25:737-45.
20.. Ferkel RD, Karzel RP, Del Pizzo W, Friedmann MJ, Fischer
SP: Arthroscopic treatmentt of anterolateral impingement of the
ankle.. Am J Sports Med 1991;19:440-6.
21.. van Dijk CN, Bossuyt PM, Mart i RK: Medial anklee pain
after lateral ligament rupture. / BoneBone Joint Surg [Br]
1996;78-B:562-7.
22.. Ferkel RD, Ruland CM: Operative arthroscopyy of the ankle.
In: Andrews JR, Timmermann LA eds. Diagnostic and operative
arthroscopy.arthroscopy. Philadelphia, USA: W.B. Saunderss Company,
1998:431-47.
23.. Ferkel RD, Fischer SP: Progress in ankle arthroscopy.. Clin
Orthop 1989;240:210-20.
24.. Liu SH, Raskin A, Osti L, Baker C, Jacobson K,, Finerman G:
Arthroscopic treatment of anterolaterall ankle impingement.
ArthroscopyArthroscopy 1994;10:215-8.
25.. Marti n DF, Baker CL, Curl WW, Andrews JR,, Robie DB, Haas
AF: Operative ankle arthroscopy.. Long-term follow-up. Am J
SportsSports Med 1989;17:16-23.
26.. Meislin RJ, Rose DJ, Parisien JS, Springer S: Arthroscopicc
treatment of synovial impingementt of the ankle. Am J Sports Med
1993;21:186-9. .
27.. Tol JL, Verheyen CP, van Dijk CN: Arthroscopicc treatment
of anterior impingementt in the ankle. J Bone Joint Surg
/J'r/2001;83-B:9-13. .
28.. Rubin DA, Tishkoff NW, Britto n CA, Conti SF,, Towers JD:
Anterolateral soft tissue impingementt in the ankle: diagnosis
using MR imaging.. ^/n/ieoeiif^e/7o71997;169:829-35.
18 8
-
Chapterr 1
29.. Bassett FH, Gates HS, Billys JB, Morri s HB, Nikolaouu PK:
Talar impingement by the anteroinferiorr tibiofibular ligament. A
cause of chronicc pain in the ankle after inversion sprain.. J Bone
Joint Surg [Am] 1990,72-A.55-9.
30.. Seil R, Rupp S, Pape D, Dienst M, Kohn D: [Approachh to
open treatment of osteochondral lesionss of the talm]. Orthopade
2001;30:47-52.
31.. Vogler HW, Stienstra JJ> Montgomery F, Kippp L: Anterior
ankle impingement arthropathy.. The role of anterolateral
arthrotomyy and arthroscopy. Clin Podiatr MedMed Surg 1994;
11:425-47.
32.. Ferkel RD: Articvdar surface defects, loose bodies,, and
osteophytes. In: Whipple TL ed. ArthroscopicArthroscopic surgery:
The foot and the ankle. Philadelphia,, USA: Lippincott-Raven
Publishers,, 1996:145-84.
33.. Ray RG, Gusman DN, Christensen JC: Anatomicall variation of
the tibial plafond: the anteromediall tibial notch, f Foot Ankle
Surg 1994;33:419-26. .
34.. van Dijk CN, Wessel RN, Tol JL, Maas M: Obliquee radiograph
for the detection of bone spurss in anterior ankle impingement.
Skeletal RadiolRadiol7002:31:214-21. 7002:31:214-21.
35.. Ferkel RD, Fasulo GJ: Arthroscopic treatment off ankle
injuries. Orthop Clin North Am 1994;25:17-32. .
36.. Berndt AL, Harty M: Transchondral Fracturess
(Osteochondritis Dissecans) of the talus,, f Bone Joint Surg [Am]
1959;41 -A:988-1020. .
37.. Alexander AH, Lichtman DM: Surgical treatmentt of
transchondral talar-dome fracturess (osteochondritis dissecans).
Long-termm follow-up. J Bone Joint Surg [Am] 1980;62-A:646-52.
.
38.. König F: Ueber freie Körper in den Gelenken. DeutschDeutsch
Z Chir 1888;27:90-109.
39.. Bosien WR, Staples OS, Russell SW: Residual disabilityy
following acute ankle sprains. / BoneBone Joint Surg [Am]
1955;37-A:1237-43.
40.. Flick AB, Gould N: Osteochondritis dissecans off the talus
(transchondral fractures of the talus):: review of the literature
and new surgical approachh for medial dome lesions. Foot Ankle
1985;5:165-85. .
41.. Davis AW, Alexander I J: Problematic fracturess and
dislocations in the foot and anklee of athletes. Clin Sports Med
1990;9:163-81. .
42.. Goldstone RA, Pisani AJ: Osteochondritis dissecanss of the
talus. A^ YState J Med 1965;65:2487-94. .
43.. DeSmet AA, Fisher DR, Bumstein MI , Graf BK,, Lange RH:
Value of MR imaging in stagingg osteochondral lesions of the talus
(osteochondritiss dissecans): results in 14 patients.. Am J
Roentgenol 1990;154:555-8.
44.. Rynn M, Fazekas EA, Hecker RL: Osteochondrall lesions of
the talus. J Foot Surg 1983;22:155-8. .
45.. Wells D, Oloff-Solomon J: Radiographic evaluationn of
transchondral dome fractures of thee talus. J Foot Surg
1987;26:186-93.
46.. Naumetz VA, Schweigel JF: Osteocartilagenouss lesions of
the talar dome, ƒ TraumaTrauma 1980;20:924-7.
47.. Hanley WB, McKusick VA, Barranco FT: Osteochondritiss
dissecans with associated malformationn in two brothers. J Bone
Joint SurgSurg [Am] 1967;49-A:925-37.
48.. Kabbani YM, Mayer DP: Magnetic resonance imagingg of
osteochondral lesions of the talar dome.. J Am Podiatr Med Assoc
1994;84:192-5.
49.. McCullough RW, Gandsman EJ, litchman HE,, Schatz SL:
Dynamic bone scintigraphy in osteochondritiss dissecans. Int Orthop
1988;12:317-22. .
50.. Loomer R, Fisher C, Lloyd-Smith R, Sisler J, Cooneyy T:
Osteochondral lesions of the talus. AmAm J Sports Med
1993;21:13-9.
51.. Meyer JM, Hoffmeyer P, Savoy X: High resolutionn computed
tomography in the chronicallyy painful ankle sprain. Foot Ankle
1988;8:291-6. .
52.. Zinman C, Wolfson N, Reis ND: Osteochondritiss dissecans of
the dome of the talus.. Computed tomography scanning in diagnosiss
and follow-up. J Bone Joint Surg [Am][Am] 1988;70-A:1017-9.
53.. Kelberine F, Frank A: Arthroscopic treatmentt of
osteochondral lesions of the talar dome:: a retrospective study of
48 cases. ArthroscopyArthroscopy 1999;15:77-84.
54.. Yulish BS, Mulopulos GP, Goodfellow DB, Bryann PJ, Modic
MT, Dollinger BM: MR imagingg of osteochondral lesions of talus. /
ComputComput Assist Tomogr 1987; 11:296-301.
55.. Anderson IF, Crichton KJ, Grattan-Smith T, Cooperr RA,
Brazier D: Osteochondral fracturess of the dome of the talus. J
Bone Joint SurgSurg [Am] 1989;71-A:1143-52.
56.. Bohndorf K: Osteochondritis (osteochondrosis)) dissecans -
a review and neww MRI classification. Eur Radiol 1998;8:103-12.
.
19 9
-
57.. Aerts P, Disier DG: Abnormalities of the foot andd ankle:
MR imaging findings. Am J RoentgenolRoentgenol 1995;165:119-24.
58.. Helgason JW, Chandnani VP: Magnetic resonancee imaging
arthrography of the ankle. TopTop Magn Reson Imaging
1998;9:286-94.
59.. Heare MM , Gillespy T, III , Bittar ES: Direct coronall
computed tomography arthrography off osteochondritis dissecans of
the talus. SkeletalSkeletal Radiol 1988; 17:187-9.
60.. Stroud CC, Mark s RM: Imaging of osteochondrall lesions of
the talus. Foot Ankle ClinClin 2000;5:119-33.
61.. Baker CL, Graham JM, Jr.: Current concepts inn ankle
arthroscopy. Orthopedics 1993;16:1027-35. .
62.. Tehranzadeh J, Gabriele OF: Intra-articular calcifiedd
bodies: detection by computed arthrotomography.. South Med f
1984;77:703-10. .
63.. Trattni g S, Rand T, Breitenseher M, Ba-Ssalamahh A, Schick
S, Imhof H: [MRI arthrographyy of the ankle joint]. Radiologe
1999;39:47-51. .
64.. Hansen ST, Jr.: Posttraumatic and degenerativee problems in
the joints. FunctionalFunctional reconstruction of the foot and
ankle.ankle. Philadelphia, USA: Lippincott Williams &&
Wilkins, 2000:145-86.
65.. Demazière A, Ogilvie-Harri s DJ: [Operative arthroscopyy of
the ankle. 107 cases]. Rev RhumRhum Mai Osteoartic
1991;58:93-7.
66.. Cheng JC, Ferkel RD: The role of arthroscopyy in ankle and
subtalar degenerativee joint disease. Clin Orthop 1998;349:65-72.
.
67.. van Dijk , C. N. [Beweegredenen. De patiënt alss bron van
inspiratie]. Inaugural lecture. Amsterdam,, The Netherlands,
Vossiuspers UvA,, 2002.
68.. DeSmet AA, Dalinka MK , Alazraki N, Berquistt TH, Daffher
RH, el Khoury GY, Goergenn TG, Keats TE, Manaster BJ, Newbergg A,
Pavlov H, Schweitzer ME, Haralsonn RH, III , McCabe JB: Chronic
ankle pain.. American College of Radiology. ACR Appropriatenesss
Criteria. Radiology 2OQ0;2\5 Suppl:321-32. .
69.. Ferkel RD: Soft tissue lesions of the ankle. In: Whipplee
TL ed. Arthroscopic surgery: The footfoot and ankle. Philadelphia,
USA: Lippincott-Ravenn Publishers, 1996:121-43.
70.. Traughber PD: Imaging of the foot and ankle. In:: Mann RA,
Coughlin MJ eds. Surgery of thethe foot and ankle. 6 ed. St. Louis,
USA: Mosby,, 1997:61-139.