Embed Size (px)
Citation preview

Update in nephrology Update in nephrology Contrast induced nephropathy, nephrogenic Contrast induced nephropathy, nephrogenic
systemic fibrosis and acute phosphate systemic fibrosis and acute phosphate nephropathynephropathy
Steven D. Weisbord MD, MSc, FASNRenal-Electrolyte Division
University of Pittsburgh School of Medicine

1) A 45 year old WM with a serum creatinine of 1.0 mg/dL is undergoing a procedure. He is at risk for:a) Contrast induced nephropathyb) Acute phosphate nephropathyc) Nephrogenic systemic fibrosisd) Contrast nephropathy and acute phosphate
nephropathye) Contrast nephropathy and nephrogenic systemic
fibrosisf) Acute phosphate nephropathy and nephrogenic
systemic fibrosisg) All of the above

2) A 45 year old WM with a serum creatinine of 1.8 mg/dL is undergoing a procedure. He is at risk for:
a) Contrast nephropathyb) Acute phosphate nephropathyc) Nephrogenic systemic fibrosisd) Contrast nephropathy and acute phosphate
nephropathye) Contrast nephropathy and nephrogenic systemic
fibrosisf) Acute phosphate nephropathy and nephrogenic
systemic fibrosisg) All of the above

3) A 45 year old WM on chronic hemodialysis is undergoing a procedure. He is at risk for:
a) Contrast nephropathyb) Acute phosphate nephropathyc) Nephrogenic systemic fibrosisd) Contrast nephropathy and acute phosphate
nephropathye) Contrast nephropathy and nephrogenic systemic
fibrosisf) Acute phosphate nephropathy and nephrogenic
systemic fibrosisg) All of the above

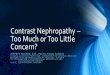
Pathophysiology of CIN
Radiocontrast Administration
CIN
Medullary Hypoxia
Generation of ROS
IntrarenalVasoconstriction
DirectCytotoxicity
RheologicEffects
OsmoticLoad

Risk factors for CIN• Patient-related
– Renal insufficiency – Diabetes mellitus*– Intravascular volume depletion– Reduced cardiac output– Concomitant nephrotoxins
• Procedure-related– ↑ volume of radiocontrast– Multiple procedures w/i 72 hours– Intra-arterial administration– Type of radiocontrast
}
* Diabetes alone not strong risk factor
additive risk

Renal Insufficiency and Diabetes Mellitus
Creatinine Clearance (mL/min)
CIN Requiring Dialysis
Non-Diabetic Diabetic
50 0.04% 0.2%
40 0.3% 2%
30 2% 10%
20 12% 43%
10 48% 84%
McCullough PA et al. Am J Med. 1997;103:368-375.

• Known renal insufficiency • Diabetes mellitus• Proteinuria• Advanced age• Hypertension• Nephrotoxic drug use• History of kidney problem after radiocontrast • Advanced liver disease
Consider screening SCr if pt has 1 or more of these:
Weisbord SD, my approach
Approach to screening with SCrApproach to screening with SCr

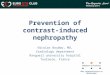
Relationship Between Serum Relationship Between Serum Creatinine and eGFRCreatinine and eGFR
0
20
40
60
80
100
120
0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0
Serum creatinine (mg/dL)
eGF
R (
mL
/min
/1.7
3 m
2)
75yo AAM 75yo WF
59 ml/min/1.73m2
36 ml/min/1.73m2

Implications of CINImplications of CIN
• CIN may result in any or all of the following:
– Delay in discharge of patient
– Permanent kidney damage
– Dialysis
– Increased patient mortality
Dangas G et al. Am J Cardiol. 2005;95:13-19.

CIN and mortalityCIN and mortality
0%
10%
20%
30%
40%
50%
Mor
talit
y
No AKI AKI
Levy et al. JAMA 1996; 275:1489-1494
Adjusted OR: 5.5; p<0.01
Mortality
Apache II No AKI AKI
0-3 4% 17%
4-7 5% 40%
8-11 28% 52%
>12 33% 62%

• CCB• Loop diuretics*• Mannitol*• Dopamine*• Fenoldopam*• ANP• Hemodialysis*
• NAC• Theophylline• Aminophylline• Ascorbic acid• Statins• Hemofiltration
• IVF• Choice of
contrast
Ineffective EffectiveUnclear benefit
* Possibly harmful
Preventive strategies for CINPreventive strategies for CIN

NAC for CIAKI (n=83)
Tepel M, et al. N Engl J Med 2000; 343:180-184
0%
5%
10%
15%
20%
25%
% C
IN (
Scr
↑
0.5
mg/
dL
@ 4
8h)
Control
2%
21%
P=0.01
NAC

Meta-Analyses of NACMeta-Analyses of NAC
Studies Subjects
RR
(95% CI) Heterogeneity
Pannu, et al 15 1776 0.65 (0.43-1.00) Yes
Kshirsagar, et al 16 1538 ** Yes
Nallamothu, et al 20 2195 0.73 (0.52-1.03) Yes
Duong, et al 14 1584 0.57 (0.37-0.88) Yes
Kelly, et al 26 3393 0.62 (0.44-0.88) Yes
Gonzalez et al 22 2746 ** Yes
Subgroup 1 18 2445 0.87 (0.68-1.12) No
Subgroup 2 4 301 0.15 (0.07-0.33) No
** Given degree of heterogeneity, calculation of summary estimate would be invalid

NAC - summaryNAC - summary
• Protective effect unclear• Many studies to date have methodological
flaws• Cheap and benign (in oral form)• Should not be used in lieu of other measures

Clinical trials of volume expansionClinical trials of volume expansion
• 1994 → present• Provide clinical basis for:
– Protective effect of IVF– Deleterious effect of furosemide– Superiority of isotonic IVF– Superiority of IVF to pt-directed oral fluids– Potential benefit of oral NaCl

Rate of CIN: 11% 28% 40%
Solomon R, Werner C, Mann D, D’Elia J, Silva P. N Engl J Med. 1994;331:1416-1420.

Isotonic v. hypotonic saline Isotonic v. hypotonic saline
Mueller C, et al. Arch Int Med. 2002; 162:329-336
P=0.04
P=0.35
P=0.93

Saline vs. Bicarbonate IV fluidSaline vs. Bicarbonate IV fluid
13.6%
1.7%
0%
2%
4%
6%
8%
10%
12%
14%
NaCl (n=59) NaHCO3(n=60)
rate of CIN
(8/59)
(1/60)
Merten et al. JAMA 2004;291:2328-2334
P = 0.02

Meta-analysis of NaCl v. NaHCOMeta-analysis of NaCl v. NaHCO33
Navaneethan SD et al. 617-627; 2009; American Journal of Kidney Diseases
OR 0.46 [0.26-0.82]

IV NaCl v. oral NaClIV NaCl v. oral NaCl
6.6%5.2%
7.5%
15.2%
0
2
4
6
8
10
12
14
16
Oral IV IV/ Theo IV/ Fur
P=NSP=NS
N=76N=76 N=77N=77 N=80N=80 N=79N=79
Dussol et al. Nephrology Dialysis Transplantation. 2006;21:2120-2126
% CIN

Meta-analysis of IOCM v. LOCM
3.5%
15.5%
2.4%
5.1%
0.6%
1.9% 1% 1.6%
0
2
4
6
8
10
12
14
16
+CKD/+DM +CKD/-DM -CKD/+DM -CKD/-DM
NS
NS NS
P=0.003
% p
ts
IOCM LOCM
McCullough et al. JACC 2006;48:692-9

Meta-analysis of IOCM v. LOCMMeta-analysis of IOCM v. LOCM
Favors IOCM Favors LOCM
Heinrich et al. Radiology 2009;250:68-86

Summary of preventionSummary of prevention
• NAC – of unclear benefit – I use 1200 mg po bid x 2 days
• IV fluids beneficial – isotonic >> hypotonic– ? Superiority of NaHCO3– Abbreviated regimen OK – 1 hr pre and 4-6 hr post
• Low or iso-osmolal contrast– Mixed data on superiority of iso-osmolal

Summary of CINSummary of CIN
• Remains common due to high use of iodinated contrast
• Risk factors well known – CKD• Adverse outcomes with CIN• Prevention:
– Isotonic IV fluids– NAC - ? benefit– Choice of contrast

26
NSF - History and NomenclatureNSF - History and Nomenclature
• Disease initially identified in late 1990s as fibrosing skin condition Named nephrogenic fibrosing dermopathy (NFD)
• Subsequently found to also have systemic manifestationsskeletal muscle, lung, liver, testes, myocardiummost prominent findings are dermatologic
• Re-named Nephrogenic Systemic Fibrosis (NSF)
Cowper SE. Available at http://www.icnfdr.org; Deo A et al. Clin J Am Soc Nephrol. 2007;2:264-267.

27Marckmann P et al. Clin Nephrol. 2008;69:161-168; Mitka M. JAMA. 2007;297:252-253; Thomsen HS. Eur Radiol. 2006:16:2619-2621; Cowper SE. http://www.icnfdr.org. Issa N et al. Cleve Clin J Med. 2008;75:95-111
• Distribution– Usually symmetrical– Extremities trunk– Face/neck typically spared
• Signs– Swelling and erythema of extremities – Induration: distal proximal– Woody papules
• Symptoms– Burning, itching, pain– Reduced flexibility immobility– Muscle weakness
NSF: Skin manifestationsNSF: Skin manifestations
} Can be very disabling

NSF: EpidemiologyNSF: Epidemiology
• No gender predilection
• Affects patients of all ages; most commonly middle age
• Affects various ethnic/racial groups
• Seen in North America, Europe, and Asia
• Only seen in pts with kidney disease
Cowper SE. Available at http://www.icnfdr.org.

NSF: Clinical appearanceNSF: Clinical appearance
Occurs days to many months after exposure to GBCA
Marckmann P et al. Clin Nephrol. 2008;69:161-168

30
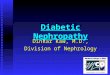
NSF: Association With Renal DiseaseNSF: Association With Renal Disease• All reported NSF in pts with renal impairment
– Reported in stages 4-5 CKD • eGFR <30 mL/min/1.73 m2
– Most commonly dialysis pts
Issa N et al. Cleve Clin J Med. 2008;75:95-111.
Stage I Stage II Stage III Stage IV Stage V
130 120 110 100 90 80 70 60 50 30 25 20 15 040 10 5
GFR
NSFNSF
Most cases

31

32
1. Markmann et al – 13 of 370 ESRD pts (3.5%) 2. Deo et al – 3 of 87 ESRD pts – (3.4%)3. Broome et al – 12 of 301 HD-pt exposures (4%)4. Prince et al – 1 of 265 ESRD pt (0.4%)
Incidence after GBCA in ESRD = 0.4-4% based on retrospective analyses
NSF: Incidence After GBCA in End-Stage NSF: Incidence After GBCA in End-Stage Renal DiseaseRenal Disease
Markmann P et al. J Am Soc Nephrol. 2006:2359-62; Deo A et al. Clin J Am Soc Nephrol. 2007:264-7; Broome DR et al. AJR 2007:586-92; Prince MR et al. Radiology. 2008;248:807-816.

33
Incidence of NSF in stages 4 and 5 Incidence of NSF in stages 4 and 5 CKD following MRACKD following MRA
• 2 retrospective analyses of:– Large tertiary referral center in UK– Database of pts screened/enrolled in ASTRAL study
• Results:– 0 of 252 pts with eGFR < 30 developed NSF– 0 of 485 pts with eGFR < 60 developed NSF– 1 of 1735 pts (0.06%) with CKD developed NSF (data
extrapoloated and pt with NSF had stage 4-5 CKD)
Chrysochou et al. Journal of Mag Reson Imag 29:887-94

34
NSF – Pathogenesis and GBCANSF – Pathogenesis and GBCA
• Gd is a lanthanide ion• Free Gd is highly toxic• Contrast agents for MR imaging – metal ion (Gd)
bound to ligand (Gd-chelate complex)• GBCA – excreted by the kidneys• With impaired kidney function, T1/2 of GBCA increases• ? displacement of Gd from chelate (transmetallation)• Tissue exposure of Gd ? Fibrosis leading to NSF
Perazella MA. Clin J Am Soc Nephrol. 2007;2:200-202; Rofsky NM et al. Radiology. 2008:608-12.

35
NSF: Speculative PathogenesisNSF: Speculative Pathogenesis
cF, circulating fibrocyte; Cyto, cytokinesPerazella MA. Clin J Am Soc Nephrol. 2007;2:200-202.
1
2
3
4 5

36
NSF and Specific GBCA NSF and Specific GBCA Volunteer case reports to MedWatch (FDA) as of 10/07
Penfield JG et al. Semin Dial. 2008;21:129-134.
Agent
FDA-reported cases, n
Published case reports, n
Gadodiamide 283 93
Gadopentetate dimeglumine 125 18
Gadoversetamide 20 0
Gadobenate dimeglumine 10* 1‡
Gadoteridol 9† 0
*Only 2 received that GBCA alone; †Only 1 received that GBCA alone;‡Patient also received Omniscan

37
Risk factors for NSF - GBCARisk factors for NSF - GBCA
Agarwal R et al. 2008 Nephrol Dial Transplant: 1-7; Wahba M. et al. Amer J. Transplant 2007;7:2425-32
- GBCA strongly associated with NSF
- Few case reports of NSF without known GBCA exposure

38
NSF and dose of GBCANSF and dose of GBCA
• 83,121 pts received GBCA• 15 cases of NSF confirmed after GBCA• 74,124 pts - low dose GBCA (0.1 mmol/kg) – NSF = 0%• 8,997 pts – high dose GBCA (0.2-0.4 mmol/kg) – NSF = 0.17%
• Retrospective review - biopsy-confirmed NSF cases from 1997–2007 in 2 large hospitals
Prince MR et al. Radiology. 2008;248:807-816.

39
NSF and pro-inflammatory stateNSF and pro-inflammatory state
Sadowski EA et al. Radiology. 2007;243:148-157.

NSF: Associated Clinical ConditionsNSF: Associated Clinical Conditions
• Hypercoagulability states• Surgical procedures
– Esp, reconstructive vascular components
• Hepatic disease– Hepatorenal syndrome– Liver transplantation– Hepatitis B and C
• Thrombotic events• Idiopathic pulmonary
fibrosis• SLE• Hypothyroidism• serum Ca or PO4
• Hyperparathyroidism• Metabolic acidosis
Issa N et al. Cleve Clin J Med. 2008;75:95-111.
- These conditions may be associated with increased use of MRI- Some conditions result from or cause renal disease

41
NSF and other forms of renal diseaseNSF and other forms of renal disease
• Acute kidney injury appears to be a risk factor for NSF– Acute kidney injury an “inpatient” disease– No need to routinely screen outpatients for
acute kidney injury before MR• Peritoneal dialysis (PD)
– Appears to be risk factor - ? > HD– Reduced clearance of Gd with PD
Joffe P et al. Acad Radiol. 1998;5:491-502; Prince MR et al. Radiology. 2008;248:807-816.

42
NSF: attempted treatment strategiesNSF: attempted treatment strategies• Oral steroids (eg,
prednisone)• Topical Dovonex (under
occlusion)• Extracorporeal
photopheresis• Plasmapheresis• Cytoxan
• Thalidomide• Ultraviolet therapy• Physical therapy• Pentoxifylline• High-dose IV Ig therapy• Renal transplantation• IV sodium thiosulfate
Cowper SE. Available at http://www.icnfdr.org; Issa N et al. Cleve Clin J Med. 2008;75:95-111.
- Most evidence anecdotal and/or unconfirmed.- Improving renal function may slow, arrest, and reverse NSF- PREVENTION IS KEY !!!!

43
Prevention: FDA recommendations on Prevention: FDA recommendations on use of GBCAuse of GBCA
• Screen all pts for renal dysfunction: history and/or lab tests
• Avoid GBCA in pts with known risks for NSF unless diagnostic information cannot be obtained with non-contrast MR or other diagnostic procedures
• When administering GBCA:
– Do not exceed recommended GBCA dose in product labeling
– Allow sufficient time for elimination of GBCA from the body prior to any re-administration
• For pts on HD, consider prompt HD following GBCA
http://www.fda.gov/cder/drug/InfoSheets/HCP/gcca_200705.htm

Summary of NSFSummary of NSF
• Debilitating fibrosing condition - 10 skin findings
• Associated with gadolinium contrast agents• Risk factors – high dose GBCA, inflammation• Incidence is 2-4% in dialysis and < 0.1% in
advanced CKD• Treatment is limited• Prevention is key in high risk pts

• 7,349 native kidney bx• 31 cases of nephrocalcinosis• 21 of 31 pts had AKI and normal [Ca] + prior
colonoscopy with oral sodium phosphate (OSP)• Mean baseline SCr 1.0 mg/dL• @ 16+ months of f/u:
– 4 developed ESRD– 17 had persistent CKD
JASN 16:3389-3396,2005

Hyperphosphatemia and AKIHyperphosphatemia and AKI
• Acute tubular nephropathy and late radiologic vascular calcifications following treatment of a hypercalcemia with intravenous administration of phosphates – - Bernheim et al 1968
• Acute hyperphosphatemia and acute persistent renal insufficiency induced by oral phosphate therapy – Ayala et al. 1975
• Acute renal insufficiency caused by major hyperphosphatemia (normal blood uric acid) following treatment of acute lymphoblastic leukemia – Boudailliez et al 1986

NephrocalcinosisNephrocalcinosis
AJR:136;April 1981;831

Acute phosphate nephropathy
• Form of acute/subacute kidney injury:– Occurs following use of oral sodium phosphate
solution for colonoscopy prep– Commonly leads to CKD– Can lead to ESRD

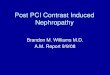
Acute phosphate nephropathy: PathogenesisAcute phosphate nephropathy: Pathogenesis

Acute Phosphate nephropathy – risk factors
• CKD – greater retention of po4• Use of ACEi/ARB, diuretics, nsaids• Older age• Female gender• Higher doses of OPS and closer dosing
interval

Acute phosphate nephropathy - prevention
• Boxed warning for OSP preparations• Oral preps no longer available OTC• Recognize risk factors• Work closely with gastroenterologists to avoid
OSP preparations in pts at risk• Some recommendations are to avoid OSP
completely

1) A 45 year old WM with a serum creatinine of 1.0 mg/dL is undergoing a procedure. He is at risk for:a) Contrast induced nephropathyb) Acute phosphate nephropathyc) Nephrogenic systemic fibrosisd) Contrast nephropathy and acute phosphate
nephropathye) Contrast nephropathy and nephrogenic systemic
fibrosisf) Acute phosphate nephropathy and nephrogenic
systemic fibrosisg) All of the above

2) A 45 year old WM with a serum creatinine of 1.8 mg/dL is undergoing a procedure. He is at risk for:
a) Contrast nephropathyb) Acute phosphate nephropathyc) Nephrogenic systemic fibrosisd) Contrast nephropathy and acute phosphate
nephropathye) Contrast nephropathy and nephrogenic systemic
fibrosisf) Acute phosphate nephropathy and nephrogenic
systemic fibrosisg) All of the above

3) A 45 year old WM on chronic hemodialysis is undergoing a procedure. He is at risk for:
a) Contrast nephropathyb) Acute phosphate nephropathyc) Nephrogenic systemic fibrosisd) Contrast nephropathy and acute phosphate
nephropathye) Contrast nephropathy and nephrogenic systemic
fibrosisf) Acute phosphate nephropathy and nephrogenic
systemic fibrosisg) All of the above

??????