Embed Size (px)
Citation preview

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 1/9
Search the site ...
Contrast Nephropathy, myth thereof
May 1, 2019 by Josh Farkas
CONTENTS
Venous injection of contrast (e.g. for CT scan)The birth of the contrast nephropathy myth (#contrast_nephropathy:_a_myth_is_born)
Current lack of evidence regarding contrast nephropathy (#current_lack_of_evidence_regarding_contrast_nephropathy)
Weighing the risks vs. bene�ts of using contrast (Renalism) (#weighing_the_risks_vs._bene�ts_of_using_contrast_(Renalism))
The attention given to contrast nephropathy is insane (#the_attention_given_to_contrast_nephropathy_is_disproportionately_insane)
Intra-arterial contrast (e.g. cardiac catheterization) (#intra-arterial contrast_(e.g._cardiac_catheterization))
Algorithm (#checklist)
Podcast (#podcast)
Questions & discussion (#questions_&_discussion)
Pitfalls (#pitfalls)
contrast nephropathy: a myth is born(back to contents) (#top)
The concept of contrast nephropathy was born in the 1950's, when it was observed that some patients developed renal failure following injectionof IV contrast dye for intravenous pyelography. This might have represented a true nephrotoxic reaction. The contrast dye used at that time
TOC ABOUT THE IBCC TWEET US IBCC PODCAST
AIRWAY ARCHIVES
1

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 2/9
probably was poisonous (50% diodone, a high-osmolar contrast dye which nobody would imagine using today). However, none of these earlystudies had adequate control groups, so it's impossible to know for sure. This was before the establishment of evidence-based medicine.
Regardless, a myth was born. Over time, fear of contrast nephropathy blossomed and took root. Any renal failure which occurred following theadministration of contrast was likely to be labeled as “contrast nephropathy.” Over the ensuing decades, well over a thousand publications werewritten about contrast nephropathy.
current lack of evidence regarding contrast nephropathy(back to contents) (#top)
Older contrast dyes probably were nephrotoxic. However, modern contrast dyes (with lower osmolarity) don't seem to cause renal failure.
Contrast DyeIncreasedCreatinine
True kidneyinjury with
elevated renalbiomarkers
Patient-centeredoutcome
(e.g. Dialysis)
(https://emcrit.org/wp-content/uploads/2019/04/conneph.svg)
“Contrast nephropathy” is usually de�ned as a small increase in creatinine within the days following contrast administration (e.g. 0.3 mg/dL). Theassumption driving this is that even small bumps in creatinine re�ect genuine renal damage, which in turn is clinically relevant. However, uponcloser examination, this chain of reasoning doesn't hold up…
(1) does contrast dye cause an increase in creatinine?
Contrast DyePatient-centered
outcome(e.g. Dialysis)
?IncreasedCreatinine
True kidneyinjury with
elevated renalbiomarkers
(https://emcrit.org/wp-content/uploads/2019/04/conneph2.svg)
Unfortunately, it would be unethical to perform a prospective RCT to evaluate this. Consequently, we are limited to retrospective, propensity-matched studies (which attempt to eliminate confounding variables). Recently, numerous studies and meta-analyses have emerged which don'tdetect any relationship between contrast dye administration and elevation of creatinine.2–12

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 3/9
One clever study examined creatinine changes in patients who had received both a contrasted CT scan and also a non-contrasted CT scan atdifferent points in time. Changes in creatinine following both scans were the same, regardless of whether the patient had received a contrastedor non-contrasted CT scan. This demonstrates that creatinine levels normally bounce a certain amount. If we examine only creatinine elevationsand assume that these represent “contrast nephropathy,” then we may manufacture a disease – when in fact we are looking at random statisticalnoise.
Indeed, several studies have found that the average creatinine of a group of patients exposed to IV contrast doesn't change at all. Somepatients experience an increase in creatinine, while an equal number experience a decrease. By focusing on the former patients and ignoring thelatter, we convert statistical noise into a clinical “disease.”
(2) do creatinine bumps re�ect genuine renal injury?
Contrast DyePatient-centered
outcome(e.g. Dialysis)
IncreasedCreatinine
True kidneyinjury with
elevated renalbiomarkers
?
(https://emcrit.org/wp-content/uploads/2019/04/conneph3.svg)
Let's imagine for a moment that contrast dye does cause a transient elevation in creatinine. Creatinine is an inert molecule, with no physiologicaleffect. The next question is whether small elevations in creatinine actually re�ect genuine kidney injury (or whether they might simply re�ecttransient reductions in creatinine secretion). It's crucial to realize that some drugs cause transient reductions in creatinine secretion withoutactually damaging the kidneys – such drugs are termed pseudo-nephrotoxins.
There is no evidence in the literature that small increases in creatinine sometimes seen following contrast dye administration re�ect actual kidneyinjury. Studies using renal biomarkers have found no signal of renal injury following contrast dye exposure – even in patients with elevatedcreatinine levels meeting the de�nition of “contrast nephropathy.” Thus, the de�nition of “contrast nephropathy” in terms of small creatininebumps is �awed, as these elevations don't seem to re�ect any genuine renal injury.
(3) what is the impact on patient-oriented clinical endpoints?
Contrast DyePatient-centered
outcome(e.g. Dialysis)
IncreasedCreatinine
True kidneyinjury with
elevated renalbiomarkers
?
(https://emcrit.org/wp-content/uploads/2019/04/conneph4.svg)
Let's be honest though – what everyone worries about most is dialysis. We're not really worried about causing a small bump in the patient'screatinine, or even causing transient renal injury. We're worried about a severe renal insult which would require dialysis. And, of course, we worryabout mortality.
4
9,13–15
16

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 4/9
Virtually every study has found no evidence that contrast increases the risk of dialysis or death. One study focusing on ICU patients did�nd that contrast correlated with an increased likelihood of requiring dialysis among patients with a GFR<45 ml/min. Bizarrely, this same studyfound no signal that contrast correlated with increased creatinine levels. How could contrast dye increase the risk of dialysis, without affectingrenal function? The answer might be an increased rate of dialysis due to the volume overload associated with contrast dye (which may largelyre�ect �uid given to prevent “contrast nephropathy”).
bottom line: no coherent evidence of harm
Contrast dyePatient-centered
outcome(e.g. Dialysis)
IncreasedCreatinine
True kidneyinjury with
elevated renalbiomarkers
? ? ?
(https://emcrit.org/wp-content/uploads/2019/04/conneph5.svg)
Despite decades of searching and literally thousands of publications, there is no coherent evidence that modern contrast dyes cause clinicallymeaningful harm. The vast majority of recent publications suggest that modern contrast dyes are safe. A few publications raise the possibility ofharm, but these studies are overall inconsistent (e.g. increased risk of dialysis without increased risk of kidney injury).
Unfortunately, we will never be able to exclude the possibility that contrast dye is nephrotoxic with 100% certainty (this is methodologicallyimpossible, because it would require a massive prospective RCT). However, the best available evidence indicates that contrast dye is safe. Ifcontrast dye were nephrotoxic, then it would have to be an extremely weak nephrotoxin of no real clinical signi�cance.
Overall, given the massive amount of study which has been spent on this issue, it's highly reassuring that no de�nitive evidence of harm has beenfound. The renal effects of contrast dye have probably been more intensely investigated than the renal effect of any other drug or substance inmedical history.
2,5,8,11,17,18
19
Lauren Westafer@LWestafer
Replying to @LadyWhoLiftsBasically 5-8% of people who have Cr measured for 24-72 h will have an AKI (bc they’re sick and/or getting nephrotox meds) and if you control for confounders, no assoc w/contrast. Whole myth came from this crazy case report onlinelibrary.wiley.com/doi/abs/10.111…
Acute Annria Following Intravenous Pyelogr…Click on the article title to read more.onlinelibrary.wiley.com

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 5/9
weighing the risks vs. bene�ts of using contrast (Renalism)(back to contents) (#top)
Clinicians are often tasked with balancing the risk-vs-bene�t of the administration of IV contrast for CT scanning. Currently, this calculation wouldseem to be as follows:
Risk of using contrast dye: There is no high-quality evidence that this risk exists.Bene�t of using contrast dye: This is often quite real (although it will certainly vary, depending on the clinical scenario).
From an evidentiary standpoint, avoidance of contrast dye is di�cult to justify. Physicians are often risk-averse, as we certainly want to avoidcausing harm. However, the best available evidence suggests that our patients will bene�t the most if we don't shy away from using contrast dyein scenarios where it is indicated.
“Renalism” refers to the avoidance of contrast dye in patients with renal dysfunction, causing a failure to perform important studies and leading toharm. In the current era of improved contrast dyes, renalism poses a greater risk to our patients than does “contrast nephropathy.”
Hinson et al. sums this up well in their conclusions following a trial involving septic patients at John Hopkins (CM=contrast medium):
32 8:40 AM - Mar 17, 2019
See Lauren Westafer's other Tweets
ATS Crit Care@ATSCritCare
Still avoiding iodinated contrast in sick patients going for CT scan? Radiology literature no longer suggests that contrast-induced nephropathy is a significant threat ow.ly/63xp30jG5aP
126 2:30 PM - Apr 27, 2018
83 people are talking about this
20
6

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 6/9
the attention given to contrast nephropathy is disproportionately insane(back to contents) (#top)
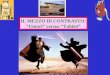
Given how much we worry about contrast nephropathy, you might think that contrast dye is the only potentially nephrotoxic substance in thehospital. In fact, contrast dye is probably among the least nephrotoxic things that we prescribe. The following list includes commonly useddrugs which are de�nitely nephrotoxic:
known nephrotoxins commonly encountered in critical care:
AntibioticsVancomycinAminoglycosidesAmphotericinAntivirals: Acyclovir, ganciclovir
ACE-inhibitors, Angiotensin receptor blockers (ARBs)NSAIDsMannitolNormal saline (in large volumes)
We worry a lot about contrast nephropathy because it has its own special name. Meanwhile, we often don't think much about other drugs, whichare proven nephrotoxins. This is entirely illogical.
Vancomycin nephrotoxicity Contrast nephropathy
Does it exist? Definitely, yes.(No debate about this)
Probably not.(Debatable)
Do alternatives exist? Yes (linezolid, ceftaroline,daptomycin)
Not really.
How much do we worry about it? Not much. A lot.
Do concerns about nephrotoxicitydelay care?
Not really. Yes (delay in imaging due toclearance for CT scans and/or labsto return)
The Internet Book of Critical Care, by @PulmCrit
(https://emcrit.org/wp-content/uploads/2019/04/vancocontr.svg)
Avoiding nephrotoxins among critically ill patients is obviously important. Our efforts along this vein should be aimed at drugs which are knownnephrotoxins. We need to stop worrying about IV contrast dye and focus more on drugs which are actually causing harm. We're wasting our timechasing a ghost, while true card-carrying nephrotoxins often pass by without much attention.
intra-arterial contrast (e.g. cardiac catheterization)(back to contents) (#top)

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 7/9
Renal injury can occur following intra-arterial procedures (e.g. cardiac catheterization). It's unclear why this occurs, with possible causesincluding the following:
1. Patients are in heart failure or cardiogenic shock with high risk of renal failure (regardless of any intervention). The occurrence of renalfailure following catheterization may merely represent association, not causation.
2. Dislodgment of cholesterol plaques with embolization to the kidneys.3. Other peri-procedural complications (e.g. arrhythmia, hemorrhage).4. Use of intra-aortic balloon pumps (which may occlude renal blood �ow when positioned incorrectly).5. Direct effect of contrast dye.
This is hard to sort out because it's impossible to perform a non-contrast cardiac catheterization. Therefore, it's even harder to investigate thistopic than it is to investigate IV contrast for CT scans.
No clear statement can be made on this topic currently. Unlike CT scans, this issue is less ubiquitous among critically ill patients. It may be bestto defer management of this issue to interventional cardiologists (who will invariably be involved in the management of any patient going to thecardiac catheterization lab).
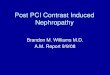
algorithm(back to contents) (#top)
Algorithm for avoiding contrast nephropathy from CT scans
Critically ill patient who needs a CT scan
What is the glomerular filtration rate (GFR)?
Could IV contrast help improve diagnostic imaging & provide better therapy?
No Yes
Actually, forget it. I don’t really care.
Don’t use contrast Use contrast
The Internet Book of Critical Care, by @PulmCrit
(https://emcrit.org/wp-content/uploads/2019/04/contrastalgo2.svg)
podcast(back to contents) (#top)
(https://i1.wp.com/emcrit.org/wp-content/uploads/2016/11/apps.40518.14127333176902609.7be7b901-15fe-4c27-863c-7c0dbfc26c5c.5c278f58-912b-4af9-
88f8-a65fff2da477.jpg)
Follow us on iTunes (https://itunes.apple.com/ca/podcast/the-internet-book-of-critical-care-podcast/id1435679111)
The Podcast Episode
Want to Download the Episode?Right Click Here and Choose Save-As (http://tra�c.libsyn.com/ibccpodcast/IBCC_EP_35_-_Contrast_Induced_Nephropathy_Final.mp3)
questions & discussion
21
00:00 00:00 (javascript:void(0);)

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 8/9
(back to contents) (#top)
To keep this page small and fast, questions & discussion about this post can be found on another page here (https://emcrit.org/pulmcrit/contrast/) .
(https://i1.wp.com/emcrit.org/wp-content/uploads/2016/11/pitfalls2.gif)
Failing to use contrast for CT scans due to fear of nephropathy, leading to suboptimal imaging studies which impair subsequentmanagement (a.k.a. Renalism).Delaying scans in critically ill patients while awaiting “clearance” to use IV contrast.Administration of additional �uid to prevent “contrast nephropathy” for CT scans in critically ill patients who have already been volumeresuscitated (if the patient is already euvolemic, additional �uid may provoke volume overload, which itself is nephrotoxic!).
Key articles to cite supporting the use of IV contrast dye
If you need some solid peer-reviewed articles to drop into the chart & protect your posterior:Aycock RD, Westafer LM, Boxen JL et al. Acute Kidney Injury after CT: A meta-analysis. Annals of Emergency Medicine 2018 PMID28811122. Exhaustive, modern literature review in the Annals showing no difference in acute kidney injury, mortality, or dialysis. PDF here(https://emcrit.org/wp-content/uploads/2019/04/aycock2017.pdf) . Hinson JS, Jalbout NA, Ehmann MR et al. Acute kidney injury following contrast media administration in the septic patient: A retrospectivepropensity-matched analysis. Journal of Critical Care 2019 PMID 28131489. Large study evaluating patients presenting to John Hopkinswith suspected sepsis. No effect was detected from contrast dye, even among patients with GFR<30 ml/min. Ehrmann S, Aronson D, Hinson JS. Contrast-associated acute kidney injury is a myth: Yes. Intensive Care Medicine 2017 PMID 29242967.
Going further:
Post Contrast AKI (https://emergencymedicinecases.com/journal-jam-post-contrast-acute-kidney-injury-pcaki/) : EM Cases with Lauren Westafer, JustinMorgenstern, Rory Spiegel and Anton Helman.Contrast Induced Nephropathy: A unicorn? (https://thesgem.com/2018/10/sgem234-contrast-induced-nephropathy-a-unicorn/) Lauren Westafer on theSkeptics Guide to EM.Does contrast cause kidney injury? (https://�rst10em.com/cin/) Justin Morgenstern First10EM.Contrast nephropathy: Confounding causation (http://www.emdocs.net/contrast-induced-nephropathy-confounding-causation/) Robert Sinert, EMDocsIs contrast induced nephropathy really not a thing? (https://rebelem.com/contrast-induced-nephropathy-cin-really-not-thing/) Salim Rezai, RebelEMDo CT scans cause contrast nephropathy? (https://emcrit.org/pulmcrit/do-ct-scans-cause-contrast-nephropathy/) PulmCrit archives from 2015.
References
1. BARTELS E, BRUN G, GAMMELTOFT A, GJØRUP P. Acute anuria following intravenous pyelography in a patient with myelomatosis. ActaMed Scand. 1954;150(4):297-302. https://www.ncbi.nlm.nih.gov/pubmed/13217726 (https://www.ncbi.nlm.nih.gov/pubmed/13217726) .
2. McDonald J, McDonald R, Comin J, et al. Frequency of acute kidney injury following intravenous contrast medium administration: asystematic review and meta-analysis. Radiology. 2013;267(1):119-128. https://www.ncbi.nlm.nih.gov/pubmed/23319662 (https://www.ncbi.nlm.nih.gov/pubmed/23319662) .
3. McDonald J, McDonald R, Carter R, Katzberg R, Kallmes D, Williamson E. Risk of intravenous contrast material-mediated acute kidney injury:a propensity score-matched study strati�ed by baseline-estimated glomerular �ltration rate. Radiology. 2014;271(1):65-73. https://www.ncbi.nlm.nih.gov/pubmed/24475854 (https://www.ncbi.nlm.nih.gov/pubmed/24475854) .
4. McDonald R, McDonald J, Bida J, et al. Intravenous contrast material-induced nephropathy: causal or coincident phenomenon? Radiology.2013;267(1):106-118. https://www.ncbi.nlm.nih.gov/pubmed/23360742 (https://www.ncbi.nlm.nih.gov/pubmed/23360742) .
5. Hinson J, Ehmann M, Fine D, et al. Risk of Acute Kidney Injury After Intravenous Contrast Media Administration. Ann Emerg Med.2017;69(5):577-586.e4. https://www.ncbi.nlm.nih.gov/pubmed/28131489 (https://www.ncbi.nlm.nih.gov/pubmed/28131489) .
6. Hinson J, Al J, Ehmann M, Klein E. Acute kidney injury following contrast media administration in the septic patient: A retrospectivepropensity-matched analysis. J Crit Care. 2019;51:111-116. https://www.ncbi.nlm.nih.gov/pubmed/30798098 (https://www.ncbi.nlm.nih.gov/pub
8
5
22

10/29/2019 Contrast Nephropathy, myth thereof - EMCrit Project
https://emcrit.org/ibcc/contrast/ 9/9
med/30798098) .
7. Ehrmann S, Quartin A, Hobbs B, et al. Contrast-associated acute kidney injury in the critically ill: systematic review and Bayesian meta-analysis. Intensive Care Med. 2017;43(6):785-794. https://www.ncbi.nlm.nih.gov/pubmed/28197679 (https://www.ncbi.nlm.nih.gov/pubmed/28197679) .
8. Aycock R, Westafer L, Boxen J, Majlesi N, Schoenfeld E, Bannuru R. Acute Kidney Injury After Computed Tomography: A Meta-analysis. AnnEmerg Med. 2018;71(1):44-53.e4. https://www.ncbi.nlm.nih.gov/pubmed/28811122 (https://www.ncbi.nlm.nih.gov/pubmed/28811122) .
9. Azzouz M, Rømsing J, Thomsen H. Fluctuations in eGFR in relation to unenhanced and enhanced MRI and CT outpatients. Eur J Radiol.2014;83(6):886-892. https://www.ncbi.nlm.nih.gov/pubmed/24656402 (https://www.ncbi.nlm.nih.gov/pubmed/24656402) .
10. Ng C, Shaw A, Bell C, Samuels J. Effect of IV contrast medium on renal function in oncologic patients undergoing CT in ICU. AJR Am JRoentgenol. 2010;195(2):414-422. https://www.ncbi.nlm.nih.gov/pubmed/20651198 (https://www.ncbi.nlm.nih.gov/pubmed/20651198) .
11. McDonald R, McDonald J, Carter R, et al. Intravenous contrast material exposure is not an independent risk factor for dialysis or mortality.Radiology. 2014;273(3):714-725. https://www.ncbi.nlm.nih.gov/pubmed/25203000 (https://www.ncbi.nlm.nih.gov/pubmed/25203000) .
12. Gorelik Y, Yaseen H, Heyman S, Khamaisi M. Negligible Risk of Acute Renal Failure Among Hospitalized Patients After Contrast-EnhancedImaging With Iodinated Versus Gadolinium-Based Agents. Invest Radiol. 2019;54(5):312-318. https://www.ncbi.nlm.nih.gov/pubmed/30480553 (https://www.ncbi.nlm.nih.gov/pubmed/30480553) .
13. Lencioni R, Fattori R, Morana G, Stacul F. Contrast-induced nephropathy in patients undergoing computed tomography (CONNECT) – aclinical problem in daily practice? A multicenter observational study. Acta Radiol. 2010;51(7):741-750. https://www.ncbi.nlm.nih.gov/pubmed/20707658 (https://www.ncbi.nlm.nih.gov/pubmed/20707658) .
14. Sandstede J, Roth A, Machann W, Kaupert C, Hahn D. Evaluation of the nephrotoxicity of iodixanol in patients with predisposing factors tocontrast medium induced nephropathy referred for contrast enhanced computed tomography. Eur J Radiol. 2007;63(1):120-123. https://www.ncbi.nlm.nih.gov/pubmed/17317065 (https://www.ncbi.nlm.nih.gov/pubmed/17317065) .
15. Schmalfuss C, Woodard P, Gitter M, et al. Incidence of acute kidney injury after intravenous administration of iodixanol for computedtomographic angiography. Int J Cardiol. 2014;177(3):1129-1130. https://www.ncbi.nlm.nih.gov/pubmed/25183538 (https://www.ncbi.nlm.nih.gov/pubmed/25183538) .
16. Kooiman J, van de, Sijpkens Y, et al. No increase in Kidney Injury Molecule-1 and Neutrophil Gelatinase-Associated Lipocalin excretionfollowing intravenous contrast enhanced-CT. Eur Radiol. 2015;25(7):1926-1934. https://www.ncbi.nlm.nih.gov/pubmed/25773936 (https://www.ncbi.nlm.nih.gov/pubmed/25773936) .
17. McDonald J, McDonald R, Lieske J, et al. Risk of Acute Kidney Injury, Dialysis, and Mortality in Patients With Chronic Kidney Disease AfterIntravenous Contrast Material Exposure. Mayo Clin Proc. 2015;90(8):1046-1053. https://www.ncbi.nlm.nih.gov/pubmed/26250726 (https://www.ncbi.nlm.nih.gov/pubmed/26250726) .
18. Gar�nkle M, Stewart S, Basi R. Incidence of CT Contrast Agent-Induced Nephropathy: Toward a More Accurate Estimation. AJR Am JRoentgenol. 2015;204(6):1146-1151. https://www.ncbi.nlm.nih.gov/pubmed/26001222 (https://www.ncbi.nlm.nih.gov/pubmed/26001222) .
19. McDonald J, McDonald R, Williamson E, Kallmes D, Kashani K. Post-contrast acute kidney injury in intensive care unit patients: a propensityscore-adjusted study. Intensive Care Med. 2017;43(6):774-784. https://www.ncbi.nlm.nih.gov/pubmed/28213620 (https://www.ncbi.nlm.nih.gov/pubmed/28213620) .
20. Weisbord S. AKI and medical care after coronary angiography: renalism revisited. Clin J Am Soc Nephrol. 2014;9(11):1823-1825. https://www.ncbi.nlm.nih.gov/pubmed/25318756 (https://www.ncbi.nlm.nih.gov/pubmed/25318756) .
21. Rastan A, Tillmann E, Subramanian S, et al. Visceral arterial compromise during intra-aortic balloon counterpulsation therapy. Circulation.2010;122(11 Suppl):S92-9. https://www.ncbi.nlm.nih.gov/pubmed/20837932 (https://www.ncbi.nlm.nih.gov/pubmed/20837932) .
22. Ehrmann S, Aronson D, Hinson J. Contrast-associated acute kidney injury is a myth: Yes. Intensive Care Med. 2018;44(1):104-106. https://www.ncbi.nlm.nih.gov/pubmed/29242967 (https://www.ncbi.nlm.nih.gov/pubmed/29242967) .
The Internet Book of Critical Care is an online textbook written by Josh Farkas (@PulmCrit), an associate professor ofPulmonary and Critical Care Medicine at the University of Vermont.
EMCrit is a trademark of Metasin LLC. Copyright 2009-. This site represents our opinions only. See our full disclaimer, our privacy policy, commenting policy and here for credits
and attribution.