Embed Size (px)
Citation preview
University of Groningen
The significance of preoperative vascular mapping of donor- and acceptor vessels in free flapsurgeryKlein, Steven
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2013
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Klein, S. (2013). The significance of preoperative vascular mapping of donor- and acceptor vessels in freeflap surgery Groningen: s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 25-08-2018
21
Chapter 3
Donor site necrosis following fibula free flap transplantation
Klein S
Hage JJ
Woerdeman LAE
Microsurgery 2005; 25: 538-542

22

23
Summary
The free fibula flap is the microsurgeon’s workhorse for the reconstruction of osseous or
osteocutaneous defects. Donor-site morbidity of this flap is reported to occur infrequently, and is
generally considered minor and transient. We present the case histories of three patients with necrosis
at the fibula flap donor site to stress the risks and explain the possible mechanisms of such severe
complications. The small risk of debilitating donor-site necrosis should be considered and discussed
preoperatively with the patient.
Introduction
The fibula free flap has become the microsurgeon’s workhorse for the reconstruction of osseus or
osteocutaneous defects of the head and neck region,(1-3) the extremities,(3-5) and the trunk.(3,6) Flap
survival and receptor site function after fibula flap transplantation have been evaluated extensively, but
donor-site morbidity has been assessed less often. Donor-site morbidity includes wound healing
disturbance and cellulitis,(1-3) transient peroneal sensory loss or cold intolerance,(1-4,7,8) motor
weakness of lower leg muscles,(1,4-9) pain or occasional cramp,(1-4,7-9) impingement of the peroneal
muscle,(10) edema after prolonged standing,(2-4,8) and ugly scarring.(4) Even though valgus deformity,
instability, or stiffness of the ankle,(1,2,4,7-9,11) and walking restriction or gait disturbances,(2,3,5,6)
can be considered more serious donor-site complications, most of the complications mentioned above
are generally rated as acceptable by patients.(1,2,4,6,8,9)
Major donor-site complications with extensive wound breakdown or necrosis are generally considered to
occur infrequently after fibula free-flap transfer. To date, only five cases of such debilitating
complications due to necrosis have been reported to lead to deep necrotectomy. Among these five were
two cases of acute compartment syndrome,(3,12) two cases of late necrosis,(13) and one case of
necrotizing infection.(4) To stress that such donor-site necrosis can lead to severe postoperative
disability, we present three more patients who suffered from extensive necrosis of the lower leg, and we
discuss how to prevent these complications.

24
Case reports
Patient 1
A 36-year-old woman underwent commando resection and supraomohyoidal lymphadenectomy for
T4N0M0 squamous-cell carcinoma of the floor of the mouth and left hemimandible. Her medical history
included systemic lupus erythematosis, tobacco abuse, and a mild myocardial infarct sustained 2
months prior to surgery. Because preoperative angiography showed no acquired or congenital
anomalies of the crural arteries, the defect was reconstructed using a fibula free flap, including a
significant part of the lateral hemisoleus muscle and a skin segment of 6 x 14 cm (Fig.1). Per our
routine, no tourniquet was used during surgery. The donor defect was closed primarily over a suction
drain after loose approximation of the muscles of the lateral compartment. No attempt was made to
approximate the lateral fascia. The lower leg and foot were splinted on a dorsal cast to prevent pes
equinus, and the patient was kept on subcutaneous heparin prophylaxis. No pressure or tensor
bandage was applied to the leg, but the patient was required to keep the leg elevated until mobilization,
one week postoperatively.
On the first postoperative day, however, the patient complained of pain in the donor leg and sensory
loss of the dorsum of the foot. On physical examination, there was functional loss of the extensor
digitorum muscle, decreased capillary refill of the foot, and lack of a Dopptone signal over the dorsal
tibial artery. These symptoms being indicative of compartment syndrome, the cast and skin sutures
were removed to reduce tension in the calf.(14,15) Angiography subsequently showed arterial filling of
both tibial arteries (Fig.2). Still, necrosis of the extensor digitorum muscle and parts of both peroneal
and long flexor hallucis muscles occurred, and repeated necrotectomy had to be performed surgically,
on postoperative days 11 and 22. After this, the crural wound healed except for its most distal part
(Fig.3). Six months after surgery, part of the distal fibula remnant still protruded from the wound, and X-
ray examination could not exclude osteomyelitis. Consequently, this part was resected, and the
remaining bone was covered during a fourth and final surgical procedure. When last seen at 44 months
of follow-up, the patient was free of recurrence, and the neomandible was functional. However, her gait
and walking distance were severely impaired.
Figure 1. Design of fibula free flap used on patient 1. Flap included significant part of lateral hemisoleus
muscle, and skin segment measuring 6 x 14 cm.

25
Figure 2. Postoperative angiography of patient 1 showed arterial filling of both tibial arteries.

26
Figure 3. Six months after fibula free-flap transplantation in patient 1, distal part of crural wound had not
closed, and protruding part of distal fibula remnant was resected.
Patient 2
A 74-year-old woman with a history of alcohol and tobacco abuse underwent commando resection and
modified radical lymphadenectomy for a T3N0M0 squamous-cell carcinoma of the floor of the mouth
extending to the left hemimandible. As the preoperative angiography showed no vascular anomalies,
the defect was reconstructed using an osteocutaneous free fibula flap with a skin paddle of 5 x 12 cm.
As no tourniquet was used intraoperatively, it could be confirmed that the manipulated muscles
remained well-vascularized throughout the entire procedure. Following approximation of the donor-site
muscles, the lower leg skin defect was covered with a split-thickness skin graft to avoid undue pressure,
and the lower leg and foot were splinted to prevent pes equinus. Again, no tensor bandage was applied,
and the patient was required to keep the leg elevated until mobilization, 1 week postoperatively.
The postoperative course was uneventful up to day 15, when edema occurred in the donor leg. Even
though wound cultures remained negative for necrotizing species, subsequent necrosis of the skin graft
and surrounding skin and subcutaneous tissue necessitated necrotectomies on postoperative days 23
and 37 (Fig.4). The resulting skin defect measured 10 x 25 cm, and skin grafts were applied
secondarily. Using a vacuum-assisted closure system, the wound completely healed by 10 weeks after
primary surgery. At 24 months of follow-up, the patient was free of recurrence, and her neomandible
functioned adequately. No remaining functional loss of the donor leg was observed.

27
Figure 4. In patient 2, skin defect resulting from initial surgery, postoperative ‘‘pseudo’’-compartment
syndrome, and subsequent necrotectomy measured 10 x 25 cm.
Patient 3
A 56-year-old diabetic man underwent segmental mandibulectomy for residual ameloblastoma, after
local resections had twice been attempted elsewhere. Because the preoperative angiography showed
no atherosclerosis or vascular anomalies, the left hemimandible and gingiva defect was reconstructed
with a fibula osteocutaneous free flap. The skin paddle measured 6 x 11 cm, and was raised on one
mid-lower leg muscular perforator, as no adequate septocutanous vessels were found. This perforator
had a long intramuscular course and a peroneal origin near the crural trifurcation, and several muscular
branches originating from the peroneal artery had to be clipped to allow for its dissection. Again, no
tourniquet was used, allowing for proper hemostasis and assessment of the muscles that were
manipulated during flap dissection. Following microsurgical flap transfer, the lateral lower leg muscles
were loosely approximated, and no attempt was made to close the fascia. The skin was partly closed
primarily, and partly by use of a skin graft. A splint was applied to prevent pes equinus, and the patient
was kept in bed and on heparin prophylaxis for 1 week. No tensor bandage was applied.
The postoperative course was uneventful until the patient became febrile and complained of pain in the
donor leg on postoperative day 11. Wound culture was positive for beta-hemolytic Streptococcus, and
antibiotic therapy was initiated. At surgical exploration, the long peroneal muscle was found to have
necrosed. Following necrotectomy, it took 10 weeks of extensive conservative treatment, including
application of a vacuum-assisted closure system, for the wound to heal. When last seen at 24 months of
follow-up, the patient was free of recurrence of osteoblastoma, and his neomandible was functional, but
exorotation and plantar flexion of the foot were compromised.

28
Discussion
Fibula flap donor-site morbidity and its consequences for daily life function are generally considered to
be rare and minor. Still, we observed severe donor-site necrosis in 3 of 74 patients in whom a fibula flap
transplantation was performed in the Netherlands Cancer Institute from January 1985 until December
2003. The mechanism of necrosis may differ. Our first patient represented an obvious case of acute
compartment syndrome, whereas a delayed ‘‘pseudo’’-compartment syndrome and a necrotizing
infection were the probable causes in our second and third patient, respectively.
Compartment syndrome is allegedly a rare consequence of free fibula flaps, and has been reported only
twice to date.(3,12) This syndrome occurs when intra-compartment pressure builds up in cases where
the fascia surrounding the compartment is intact. Obviously, this is no longer true in cases where the
lateral fascia is not closed after fibula flap transplantation. In these cases, closure of the skin under
excessive tension may be a cause of compartment syndrome, and there- fore it has been advised to
restrict primary closure of the donor site to skin paddles of maximal 6-cm width.(13,16) Alternatively,
compartment pressure may build up as a result of edema, even in cases where skin closure was
performed without undue tension.(13) In both instances, the skin acts analogous to the fascia, and
complete release of the wound may be expected to alleviate the ‘‘skin compartment syndrome.’’
In our first patient, the width of the skin paddle was restricted to the 6-cm maximum. Moreover, part of
the lateral hemisoleus muscle was harvested along with the flap, and this may be expected to reduce
the circumference of the leg and hence the closure tension. Even after adequate response to symptoms
presenting on the first postoperative day,(14,15,17) necrosis of some muscles of the anterior, lateral,
and deep compartments occurred, and hence we feel that avoidance of primary skin closure might have
prevented the compartment syndrome.(12) More careful patient selection might not have prevented the
occurrence of compartment syndrome in this patient. Such occurrence has been associated with age
under 35 years, male sex, diabetes mellitus, obesity, hypertension, traumatic rather than surgical injury,
bleeding disorders or the intake of anticoagulant drugs, low preoperative ankle-arm index, extended
duration of surgery or surgery in the lithotomy position, intraoperative hypothermia or hypotension, and
the postoperative use of regional nerve blockades.(18-22) Furthermore, patients suffering from
peripheral vascular disease were reported to run a higher risk of compartment syndrome when a
tourniquet was used during surgery.(18,20) Except for the duration of surgery, none of these
predisposing factors applied to this patient.
As for our second patient, we feel that the tension that developed in the lower leg after some delay was
too high, notwithstanding the use of a skin graft. The physical mechanism underlying the development
of the delayed necrosis seems to have been a vicious cycle of excessive tension caused by edema
leading to tissue damage and increased capillary permeability.(13) The resulting intercellular pressure
and soft-tissue edema led to more tissue damage and an increase of venous, lymphatic, and arterial
vessel compression, thus perpetuating the cycle. This cycle of gradually increasing ischemia has been
termed ‘‘pseudo’’-compartment syndrome, and may explain why the symptoms in this patient only
presented after 15 days.(13)
Paradoxically, fibulectomy used to be the treatment modality for lower leg compartment
syndrome.(14,17) Still, fibulectomy may not prevent occurrence of the complication. Rather than closing
the wound primarily, we currently apply a skin graft, irrespective of the width of the skin paddle included
in the flap. Often, this graft can safely be resected after the period of edema has passed. Still, a delayed
29
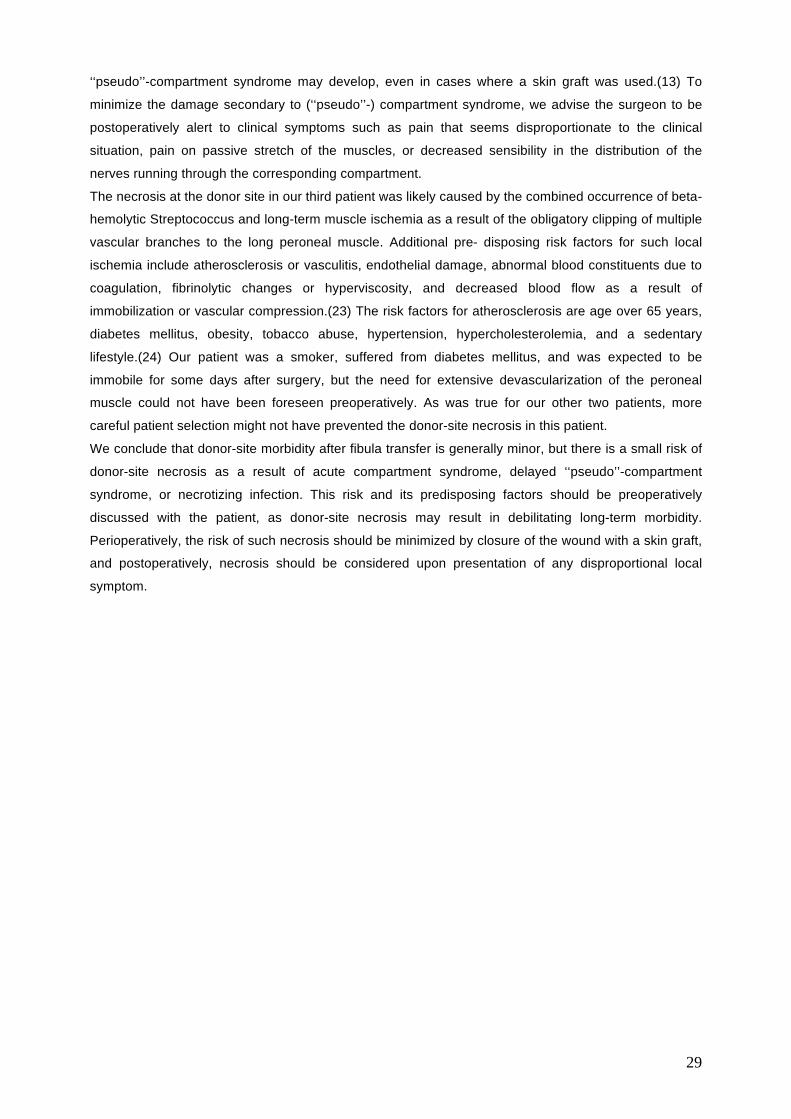
‘‘pseudo’’-compartment syndrome may develop, even in cases where a skin graft was used.(13) To
minimize the damage secondary to (‘‘pseudo’’-) compartment syndrome, we advise the surgeon to be
postoperatively alert to clinical symptoms such as pain that seems disproportionate to the clinical
situation, pain on passive stretch of the muscles, or decreased sensibility in the distribution of the
nerves running through the corresponding compartment.
The necrosis at the donor site in our third patient was likely caused by the combined occurrence of beta-
hemolytic Streptococcus and long-term muscle ischemia as a result of the obligatory clipping of multiple
vascular branches to the long peroneal muscle. Additional pre- disposing risk factors for such local
ischemia include atherosclerosis or vasculitis, endothelial damage, abnormal blood constituents due to
coagulation, fibrinolytic changes or hyperviscosity, and decreased blood flow as a result of
immobilization or vascular compression.(23) The risk factors for atherosclerosis are age over 65 years,
diabetes mellitus, obesity, tobacco abuse, hypertension, hypercholesterolemia, and a sedentary
lifestyle.(24) Our patient was a smoker, suffered from diabetes mellitus, and was expected to be
immobile for some days after surgery, but the need for extensive devascularization of the peroneal
muscle could not have been foreseen preoperatively. As was true for our other two patients, more
careful patient selection might not have prevented the donor-site necrosis in this patient.
We conclude that donor-site morbidity after fibula transfer is generally minor, but there is a small risk of
donor-site necrosis as a result of acute compartment syndrome, delayed ‘‘pseudo’’-compartment
syndrome, or necrotizing infection. This risk and its predisposing factors should be preoperatively
discussed with the patient, as donor-site necrosis may result in debilitating long-term morbidity.
Perioperatively, the risk of such necrosis should be minimized by closure of the wound with a skin graft,
and postoperatively, necrosis should be considered upon presentation of any disproportional local
symptom.

30
References
1 Anthony JP, Rawnsley JD, Benhaim P, Ritter EF, Sadowsky SH, Singer MI. Donor leg morbidity and
function after fibula free flap mandibula reconstruction. Plast Reconstr Surg 1995;96:146-152.
2 Hidalgo DA, Rekow A. A review of 60 consecutive fibula free flap mandible reconstructions. Plast
Reconstr Surg 1995;96:585-596.
3 Zimmermann CE, Börner BI, Hasse A, Sieg P. Donor site morbidity after microvascular fibula
transfer. Clin Oral Invest 2001;5:214-219.
4 Shpitzer T, Neligan P, Boyd B, Gullane P, Gur E, Freeman J. Leg morbidity and function following
fibular free flap harvest. Aesthetic Plast Surg 1997;38:460-464.
5 Babovic S, Johnson CH, Finical SJ. Free fibula donor site morbidity: the Mayo experience with 100
consecutive harvests. J Reconstr Microsurg 2000;16:107-110.
6 Youdas JW, Wood MB, Cahalan TD, Chao EYS. A quantitative analysis of donor site morbidity after
vascularized fibula transfer. J Orthop Res 1988;6:621-629.
7 Parker VT. Donor-site morbidity with use of vascularized autogenous fibular grafts. J Bone Joint
Surg [Am] 1996;78:204-211.
8 Papadopulos NA, Schaff J, Bucher H, Groener R, Geishauser M, Biemer E. Donor site morbidity
after harvest of free fibular flaps with an extended skin island. Aesthetic Plast Surg 2002;49:138-144.
9 Gore DR, Gardner GM, Sepic SB, Mollinger LA, Murray MP. Function following partial fibulectomy.
Clin Orthop 1987;220:206-210.
10 Meagher PJ, Morrison WA. Free fibula flap donor site morbidity: case report and review of the
literature. J Reconstr Microsurg 2002;18:465-467.
11 Wiltse LL. Valgus deformity of the ankle - a sequel to acquired or congenital abnormalities of the
fibula. J Bone Joint Surg [Am] 1972;54:595-606.
12 Saleem M, Hashim F, Babu Manohar M. Compartment syndrome in a free fibula osteocutaneous
flap donor site. Br J Plast Surg 1998;51:405-407.
13 Shindo M, Fong BP, Funk GF, Karnell LH. The fibula osteocutaneous flap in head and neck
reconstruction - a critical evaluation of donor site morbidity. Arch Otolaryngol Head Neck Surg
2000;126:1467-1472.
14 Rollins DL, Bernhard VM, Towne JB. Fasciotomy: an appraisal of controversial issues. Arch Surg
1981;116:1474-1481.
15 Weiner G, Styf J, Nakhostine M, Gershuni DH. Effect of ankle position and a plaster cast on
intramuscular pressure in the human leg. J Bone Joint Surg [Am] 1994;76:1476-1481.
16 Hayden RE. Harvest and clinical application of the fibula flap - editorial review. Curr Opin Otolaryngol
Head Neck Surg 1995;3:257-260.
17 Hyde GL, Peck D, Powell DC. Compartment syndromes. Early diagnosis and a bedside operation.
Am Surg 1983;49:563-568.
18 Ullrich W, Biermann E, Kienzle F, Krier C. Lagerungsschäden in Anästhesie und operativer Medizin.
Anasth Intensivmed Notfallmed Schmertzther 1997;32:4-20.
19 McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. Who is at risk? J Bone
Joint Surg [Br] 2000;82:200-203.
20 Tison C, Perigaud C, Vrignaud S, Capelli M, Lehur PA. Syndrome bilatéral des loges de jambe aprés
chirurgie colorectale en position àdouble équipe. Ann Chir 2002;127:535-538.

31
21 Thonse R, Ashford RU, Williams TI, Harrington P. Differences in attitudes to analgesia in
postoperative limb surgery put patients at risk of compartment syndrome. Injury 2004;35:290-295
22 Modrall JG, Sadjadi J, Ali AT, Anthony T, Welborn MB 3rd, Valentine RJ, Hynan LS, Clagett GP.
Deep vein harvest: Predicting need for fasciotomy. J Vasc Surg 2004;39:387-394.
23 Cotton DWK. Ischaemia, infarction and shock. In: Underwood JCE, editor. General and systematic
pathology. 2nd ed. New York: Churchill Livingstone; 1996. p 165-177.
24 Hooi JD, Kester ADM, Stoffers HEJH, Overdijk MM, van Ree JW, Knottnerus JA. Incidence of and
risk factors for asymptomatic peripheral arterial occlusive disease: a longitudinal study. Am J
Epidemiol 2001;153:666-672.

32
![HYDROXYAPATITE/POLYMER COMPOSITES FOR BONE … · and Cruess 1982]. Common donor sites include the iliac crest, tibia, fibula and greater trochanter. However, the amount of autogenous](https://img.dokumen.tips/doc/110x75/6060c7dc66668a1ee7158d9c/hydroxyapatitepolymer-composites-for-bone-and-cruess-1982-common-donor-sites.jpg)




























