Embed Size (px)
Citation preview

The OAT Analysis Toolkit
A Quality and Patient Safety Roadmap
UPMC St. Margaret Hospital
August 2012

2
Table of Contents Introduction ..................................................................................................................................... 3
OAT Analysis Roadmap ................................................................................................................. 5
Executive Summary ........................................................................................................................ 7
Top 22 Questions .......................................................................................................................... 11
OAT Survey and Results .............................................................................................................. 17
Demographics ........................................................................................................................... 17
Safety Culture ........................................................................................................................... 19
Leadership ................................................................................................................................. 21
Measurement ............................................................................................................................. 22
Medication ................................................................................................................................ 26
Purchasing Practice ................................................................................................................... 28
Procedural ................................................................................................................................. 31
Risk Management ..................................................................................................................... 36
Nursing Practice ........................................................................................................................ 38
Communication ......................................................................................................................... 41
Infection Control ....................................................................................................................... 45
Resources and Toolkits ................................................................................................................. 49

3
Introduction
Efforts to transform quality and patient safety in hospitals are sweeping across the country
through the Partnership for Patients (PfP) initiative. As part of this initiative, The Hospital &
Healthsystem Association of Pennsylvania (HAP) was awarded a federal contract to create the
Pennsylvania Hospital Engagement Network (PA-HEN) to promote strategies that foster a
culture of safety and reduce adverse events. Those hospitals that joined the PA-HEN were given
the opportunity to complete the Organizational Assessment Tool (OAT), a self-assessment tool
that was developed by the National Content Developer (NCD), the PfP technical contractor. This
self-assessment tool was comprised of 138 questions that addressed ten content domains that
affect quality and patient safety. These domains include Safety Culture, Leadership,
Measurement, Medication, Purchasing Practice, Procedural, Risk Management, Nursing Practice,
Communication, and Infection Control. The OAT was meant to assist hospitals in identifying the
use of quality and patient safety evidence-based best practices within their hospitals, as well as
new areas of opportunity where suggested practices could be implemented.
Many hospitals found that simply completing the OAT helped them to discover gaps in their
organizational culture and areas of practice that needed to be re-evaluated. The OAT also can
help hospitals identify cultural and leadership factors that affect patient safety and quality
initiatives. Evaluating your facility’s culture and administrative systems will help hospital
leaders determine the facility’s readiness for change. In order to assist hospitals in this process,
the PA-HEN leadership developed the following toolkit. This toolkit includes a high level
aggregate analysis of how you and other hospitals in the PA-HEN responded to the OAT
questions, and provides other analytic tools that can be used to identify strong areas of practices
as well as opportunities for improvement.
In reviewing the average domain scores, there were three domains that represented the highest
areas of success and three that represented the greatest opportunity for improvement across the
PA-HEN. The three highest scoring domains were Measurement, Nursing Practice and
Purchasing Practice. The three lowest scoring domains were Leadership, Safety Culture, and
Communication. Not only do these lowest scoring domains represent the greatest areas of
opportunity across the PA-HEN, but they are also the keystones to many other facets of hospital
operations and patient outcomes. Many of the components within the Leadership, Safety Culture,
and Communication domains greatly affect your hospital’s patient safety culture, and we are now
discovering that patient safety culture affects more than just patient outcomes — it also affects
patient experiences. There is a growing body of research that demonstrates a link between the
AHRQ Hospital Survey on Patient Safety Culture (HSOPS) scores and Hospital Consumer
Assessment of Healthcare Providers Survey (HCAHPS) scores. Furthermore, there is a great deal
of evidence that demonstrates how important culture can be to the safety and reliability of an
organization.

4
While PA-HEN leadership recognizes the value of the OAT, the tool does have its limitations.
Although the contents of the OAT focus on evidence-based best practices, the format of the OAT
is more of a self-assessment tool rather than a validated survey. The aggregate data from the
OAT results cannot be used for statistical analyses across facilities. However, PA-HEN
leadership does believe that reviewing your results and comparing your responses with other PA-
HEN hospitals may help to facilitate discussion and identify areas of opportunity for action
regarding patient safety and quality at your hospital.
Because the OAT was self-reported, responses to OAT questions contain bias and may not
accurately depict the patient safety environment of the hospitals. In reviewing the OAT, and
when analyzing your hospital’s responses with an interdisciplinary team, it is important to ask
and discuss the following thought-provoking questions, “Does this response accurately represent
the practices or environment in our hospital?” and “If you asked five front-line staff on a unit
about ‘X’, what would be their response?” Answers to these questions will help guide your next
steps and your investigation into whether decisions and policies that have been made by
leadership have affected patient care as intended.
While there are some limitations with the OAT, these limitations do not negate the value that can
come from analyzing your OAT results. After moving through the analysis toolkit, hospitals
should be able to identify the practices within the domains that may be contributing to a lower
overall domain score. Hospitals also should have a full discussion about patient safety culture,
communication and leadership engagement within their facility with the use of the “Top 22”
questions. Not only are these domains important for performance improvement and
sustainability, these three domains represent the greatest opportunity for improvement across the
PA-HEN. After discussing these factors, hospitals can then use the toolkits that are provided in
the “Resources and Toolkits” section to determine how to proceed and to implement those
actions and changes that are necessary to support quality and patient safety transformation.
Thank you for participating in the PA-HEN and for helping to transform quality and patient
safety across Pennsylvania. All Pennsylvania hospitals and the patients they serve can benefit
from the sharing of each other’s practices, experiences, and lessons learned, no matter the size of
the facility or where they are on their quality and safety journey. Collaboration, networking and
shared learning are vital and valuable components for success in achieving the national
Partnership for Patients goals, and are fully embodied in the PA-HEN and The Hospital &
Healthsystem Association of Pennsylvania philosophy of “Achieving More Together.”

5
OAT Analysis Roadmap
Many respondents found that completing the OAT was useful in helping to reflect on quality and
patient safety within their facilities. Hospitals’ responses and domain scores, and overall PA-
HEN level scores and response frequencies also should provide a basis for greater review and
deeper analysis of quality improvement efforts within facilities. The following steps are meant to
generate discussion and give insight as to where efforts should be focused, and how to support
PA-HEN initiatives within facilities.
1. Develop and convene an interdisciplinary team to review the OAT. Quality
improvement cannot be the sole responsibility of one person or one department. Systemic
approaches that include hospital leadership, clinicians, administrators, quality
improvement directors, patient safety officers, and front-line staff are most effective in
improving and sustaining quality.
2. Review your hospital’s domain scores in the “Executive Summary” on page 7 with
your team. The domains that are shown in Exhibits 1 and 2 represent ten areas of focus
that affect overall quality and patient safety. Exhibit 1 is meant to give a quick overview
of your hospital’s highest and lowest scoring domains. To identify possible areas for
improvement, hospitals should then compare their domain scores with the average and
maximum PA-HEN scores that are provided in Exhibit 1 and Exhibit 2.
3. Closely review the OAT questions that are provided in the “Top 22 Questions”
section. These questions highlight elements of safety culture, leadership, and
communication which are vital to the success and sustainability of performance
improvement projects. Reviewing these OAT questions will help hospitals identify
cultural, structural or administrative obstacles that may affect your PA-HEN projects and
other hospital operations.
When reviewing your responses to the “Top 22 Questions”, the following questions may
be useful in generating discussions:
“Does this response accurately represent the practices or environment in our
hospital?”
“If you ask five front-line staff on a unit about “X”, what would their response
be?”
“When was the last time that you used policy “X”, and was it effective in
achieving the intent of the policy?”
Included in the “Top 22 Questions” section are examples of suggested practices to
consider for implementation. Further information about these practices can be found in
the “Resources and Toolkits” section.

6
4. Drill down into the domains where you have identified opportunities for
improvement. Questions from the OAT and the overall PA-HEN level response
frequencies are included in the “OAT Survey and Results” section. Hospital key contacts
also have been provided with a PDF copy of their OAT responses as a separate
attachment. This attachment can be used as a reference to see how your hospital
responded to OAT questions.
Responses can then be compared to the frequency of responses by other PA-HEN
hospitals. This exercise will help hospitals to determine what items, within their low-
scoring domains, that they can improve upon.
5. Discuss your above average domain scores and sustainability plans. Reviewing areas
of success are important for identifying what your facility does well and for identifying
areas where your quality improvement efforts have been sustained. Explore successful
strategies and interventions that can be used for addressing identified opportunities in the
low scoring domains.
6. Revisit those questions that ask about the perceptions or practices of front-line staff.
Asking front-line staff about culture, best-practices, and patient safety is a good way to
investigate whether leadership decisions and organizational policies have affected the
patient care that is being delivered. OAT questions that ask about the practices and
perceptions of front-line staff include numbers 17, 25, 27, 29, 103, and 116.
7. Use the resources and toolkits to develop a plan of action for identified improvement
opportunities. At the end of this toolkit is the “Resources and Toolkits” section. The
resources and toolkits provided can help determine the approaches and tools that would
best fit with your hospital in addressing opportunities for improvement.
Within this section you can find links to the “Implementation Support Packages” that
were developed by the National Content Developer (NCD). Within these support
packages there are guides, articles, and tools that you can use to implement patient safety
culture, better communication, and stronger leadership engagement within your facility.
To best execute the practices within these support packages, PA-HEN leadership
encourages senior leaders to adopt the units where these action plans are being
implemented.
There also are other resources listed from the Institute for Healthcare Improvement (IHI),
information on the Board of Trustee Quality Curriculum that is offered by HAP and
information and a link to the PA-HEN PassKey collaborative workspace being utilized to
support the PA-HEN initiatives.

7
Executive Summary
The OAT was created as a self-assessment tool for hospitals to identify areas where they have
successfully implemented best practices and to identify areas of opportunity where suggested
practices can be implemented. Reviewing and comparing your hospital’s scores and responses
with overall scores and responses from the PA-HEN is an excellent way to evaluate your
successes and areas of opportunity.
The exhibits on the following page show a comparison between your hospital’s OAT domain
scores and the average and maximum PA-HEN domain scores. Exhibit 1 shows a table that
displays your hospital’s score, and the PA-HEN average and maximum scores for each of the ten
domains. The two green domains indicate your two highest scoring domains. The two red
domains are your two lowest scoring domains, and may represent your hospital’s greatest
opportunities for improvement.
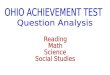
Exhibit 2 shows a comparison of your domain scores with the PA-HEN average scores using a
comparative bar graph. Hospitals are encouraged to review this graph to determine the domains
where they scored below the PA-HEN average and above the PA-HEN average. Identifying your
above average scores is important in order to identify the practices or strategies that can be used
to improve practices in your lower scoring domains.
As the PA-HEN leadership team analyzed the overall PA-HEN domain scores and responses,
one of the most interesting findings was that the three highest domains, based on average domain
scores, were Measurement, Purchasing Practice, and Nursing Practice. The three lowest PA-
HEN average domain scores were in Safety Culture, Leadership, and Communication.
In creating the “Top 22 Questions” section that is found in this toolkit, PA-HEN leadership
focused on questions from three of the lowest scoring domains, Safety Culture, Leadership and
Communication. Not only is it important to focus on these domains because they present the
greatest opportunity for improvement, these domains also include elements of culture that
contribute to a hospital’s overall patient safety culture. Moreover, there is an ever-growing body
of evidence that demonstrates a relationship between improvements in patient safety culture,
HSOPS and HCAHPS scores. For hospitals looking to improve their HCAHPS scores, in light of
pay-for-performance programs, identifying opportunities for improvement in these areas may be
one tactic for improving overall patient safety culture, patient care, and patient experiences.
Furthermore, these actions and changes also are best implemented when senior leaders play an
active role in the operations of a select unit. PA-HEN leadership recommends that senior leaders
“adopt a unit.” When senior leaders “adopt a unit,” they play a leadership role in the quality
improvement projects that are being implemented, and demonstrate to front-line staff that this
quality improvement project and these patient safety values are priorities in their facility.
If your hospital has scored above the average in any of the lower scoring aggregate PA-HEN
domains, you should still analyze areas of opportunity within these three domains in order to

8
enhance your hospital’s patient safety culture. Nevertheless, the exhibits that are included in this
section of the toolkit are meant to give hospitals an overview of where they stand in terms of
quality and patient safety practices as compared to other hospitals within the PA-HEN.
To assist hospitals in identifying and addressing opportunities for improvement within their
patient safety culture, PA-HEN, along with the Pennsylvania Patient Safety Authority, will be
offering future educational programs. There also will be education on patient safety culture
improvement included in the various PA-HEN projects as they continue over the next two years.
The PA-HEN plans on re-administering the “Top 22” questions that were identified as pertinent
cultural questions before the end of the PA-HEN contract so that hospitals can assess their
success in implementing best practices and addressing culture within their organization.

9
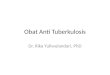
Exhibit 1. Hospital-level and PA-HEN Domain Scores
OAT Domains Hospital Score (%)
PA-HEN level Average Score
(%)
PA-HEN level Maximum Score (%)
Safety Culture 50.0 49.1 75.0
Leadership 30.0 47.8 95.0
Measurement 76.1 55.3 93.0
Medication 81.3 56.9 93.8
Purchasing Practice 82.7 68.5 98.1
Procedural 52.1 51.1 88.5
Risk Management 65.7 55.4 97.1
Nursing Practice 93.1 62.0 100.0
Communication 48.4 50.4 75.3
Infection Control 81.3 57.8 92.0
Overall OAT 67.1 55.4 79.4
Please refer to the Executive Summary for a description of Exhibits 1 and 2.
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
No
rmal
ized
OA
T Sc
ore
(%
)
OAT Domains
Exhibit 2. Hospital and PA-HEN Domain Scores Summary
Your Hospital
PA-HEN

10
Scoring Methodology
The National Content Developer, in partnership with IMPAQ, developed and completed the
following scoring methodology for the OAT. The OAT was divided into ten domains that represent
areas of importance in quality and patient safety. In order to standardize analyses, a scoring
methodology was used for each question, and a score was then assigned to each response. Below is a
brief description of how the overall domain scores were generated.
1. Each response was assigned a different weighted score, with the use of evidence-based best
practices receiving the highest weighted scores and the absence of evidence-based practices receiving
the lowest weighted scores, or a zero.
2. For questions that asked respondents to check all that apply, a score of one was assigned to each
practice that was checked, and a score of zero was assigned to those practices that respondents did
not check.
3. The individual scores for each question and within each domain were then summed. The sum of
response scores were then divided by the total possible number of points available within the domain
to create the percentages listed in the “Domain Scores” section.

11
Top 22 Questions
This section includes the top 22 questions from the OAT that the PA-HEN leadership identified
as important questions that represent an organization’s overall culture. There are many questions
that are included from the Safety Culture, Leadership, and Communication domains, as well as a
few other questions from the other domains. Hospitals should move through each of the
questions and discuss their responses, using the PDF copy of your OAT responses, and identify
possible opportunities for improvement and action.
Questions, Response Options, and Suggested Practices Frequency
of Responses
% Indicating
Use of Practice
Question 17: How strongly do you agree or disagree with the following statement? “Front line staff perceive that hospital leadership is committed to delivering necessary resources to achieve national benchmark standards on patient safety (e.g. qualified staff, appropriate medical equipment, information technology infrastructure, educational materials, laboratory)."
Strongly Agree 16 13.6%
Agree 84 71.2%
Neither 10 8.5%
Disagree 8 6.8%
Strongly Disagree 0 0.0% Suggested Practice: Implement leadership and board rounding; Assign senior leaders to units. Question 18: Which of the following is true about your hospital regarding adverse events? (Check all that apply)
There is a structure to triage and analyze adverse events 114 96.6% There is frequent (monthly or more frequent) communication of adverse events to staff (e.g., through newsletter articles, meetings, presentations) 68 57.6% Leadership routinely seeks feedback from staff on reported events and on how to reduce adverse events in the future 80 67.8% Suggested Practice: Develop a process for frequent communication of adverse events to staff. Question 19: How are results from your hospital's survey of patient safety culture used? (Check all that apply)
Develop quality improvement interventions 84 71.2%
Tied to unit score cards 13 11.0%
Tied to the hospital’s score card 17 14.4%
Compared to national standards or benchmarks 71 60.2%
To examine the effectiveness of safety programs 74 62.7%
Tracked over time to monitor hospital safety culture 81 68.6%
Not applicable 11 9.3%
Other 2 1.7%

12
Questions, Responses, and Suggested Practice Frequency % Use Suggested Practice: Develop a tracking system utilizing national standards or benchmarks; Develop quality improvement interventions and communicate these interventions throughout the facility with the possible development of scorecards or dashboards. Question 24: Which of the following is true about the engagement of patients and their families in your hospital? (Check all that apply)
They take part in multidisciplinary rounds 18 15.3%
They are partners in monitoring for compliance with safety practices 41 34.7%
They actively participate on patient safety committees 59 50.0%
They participate in root cause analysis 6 5.1%
They sit on the board 32 27.1%
Suggested Practice: Consider implementing above practices as appropriate Question 25: If five front-line staff were asked at random, how many do you think
would be able to describe a reported incident, good catch, near miss, and/or close call that led to a change (improvements in safety)?
0 1 0.8%
1 22 18.6%
2 35 29.7%
3 39 33.1%
4 16 13.6%
5 5 4.2% Suggested Practice: Develop a process for frequent communication to staff regarding adverse events and changes made due to event reporting and knowledge of near-miss events. Question 27: If five front-line staff were asked at random to describe how patient safety leadership rounds have led to changes that improved safety, how many do you think could give a description?
0 6 5.1%
1 27 22.9%
2 21 17.8%
3 22 18.6%
4 12 10.2%
5 28 23.7%
No leadership rounds 2 1.7% Suggested Practice: Implement leadership and board rounding; Assign senior leaders to units; Communicate changes that occur as a result of leadership and board rounding. Question 29: If "yes", How strongly do you think front line staff would agree with the following statement "If any leader or physician violated the policy against disruptive and inappropriate behavior, they would be removed from the hospital."
Strongly Agree 0 0.0%
Agree 25 21.2%
Neither 26 22.0%
Disagree 50 42.4%

13
Questions, Responses, and Suggested Practice Frequency % Use
Strongly Disagree 16 13.6% Suggested Practice: Implement and consistently apply principles of fair and just culture within your facility.
Question 36: Which of the following practices is part of the hospital’s quality practices around measurement? (Check all that apply) A dashboard of key results is shared at all levels of the hospital from the board to the front-line staff 92 78.0%
The data are always presented in a manner that shows the trend over time 102 86.4%
The data broadly cover all settings and include more than mandated core measures 100 84.7%
The performance of leadership is tied to key safety and quality measures 74 62.7% A significant subset of the results are shared with the public; data include both positive and negative results 51 43.2%
Other 7 5.9%
Suggested Practice: Consider implementing above practices as appropriate. Question 41: Which of the following is applicable to your hospital? (Check all that apply)
Every unscheduled return to the OR is reviewed for quality of care issues 96 81.4% Every unplanned transfer to a higher level of care (ICU, NICU, level 3 nursery, tertiary care hospital) is reviewed for quality of care issues 57 48.3% Review of unplanned transfer for quality of care issues have led to improvements in the last year 44 37.3%
Suggested Practice: Consider implementing above practices as appropriate. Question 53: What measures does your hospital include in its dashboard to track pharmacy performance? (Check all that apply)
Adverse drug reactions 97 82.2%
Adverse drug events 104 88.1%
Automated dispensing system discrepancies 84 71.2%
Bar code scanning compliance 50 42.4%
After hour medication use 34 28.8%
IV mixture competency of nursing staff 19 16.1%
Narcotic wasting compliance 71 60.2%
SCIP core measure compliance 87 73.7%
Overtime and medication error rate 22 18.6%
Other 9 7.6% Suggested Practice: Consider implementing the above pharmacy dashboard tracking areas as appropriate. Question 57: Which aspects of your hospital's evaluation of the safety of a device are you aware of? (Check all that apply) Different aspects of the evaluation process (e.g., device failure, user errors, interface design flaws, environmental factors, social factors) 94 79.7%
Staff responsible for safety evaluation 72 61.0%
Techniques used to evaluate safety 59 50.0% Channels used to communicate evaluation results to management and different units (e.g., purchasing department) 70 59.3%

14
Questions, Responses, and Suggested Practice Frequency % Use Actions taken (e.g., by purchasing department) based on results from safety evaluation of devices 77 65.3%
Other 5 4.2% Suggested Practice: Review your facility’s device evaluation process and consider implementing above practices as appropriate. Question 63: Is there a formal process for patient safety and risk involvement in equipment analysis and due diligence, selection, and purchasing?
Yes 78 66.1%
No 39 33.1%
No Response 1 0.8% Suggested Practice: Consider utilizing a patient safety checklist when performing these functions; Include patient safety and risk management staff in the process and on committees that make these types of decisions. Question 80: Which of the following is true regarding the process and effect of credentialing, privileging and peer review in your hospital? (Check all that apply) Risk management is included in the peer review process of unexpected outcomes and issues relating to deviations from accepted standards of care and other risk exposures 94 79.7% There is a process in place to support an adequate and objective medical staff and a nursing peer review process that demonstrates effectiveness for improvement 80 67.8%
Peer review has resulted in changes in protocol, purchasing, or practices 84 71.2%
Suggested Practice: Consider implementing above practices as appropriate. Question 81: What does your hospital do to prevent recurrence of serious safety events? (Check all that apply) Active involvement by the CEO in serious safety event prevention and apprised of effectiveness for prevention 72 61.0% Active involvement by senior leadership in serious safety event prevention and apprised of effectiveness for prevention 108 91.5% A measurement process that ensures RCA/FMEA actions are effective in preventing a repeat occurrence 84 71.2% A system to track implementation and effectiveness of programs to reduce serious safety events 86 72.9%
Patient safety culture matrix 42 35.6%
A user friendly and "safe" reporting tool for front line staff 101 85.6%
Other 1 0.8%
Suggested Practice: Consider implementing above practices as appropriate. Question 85: Is there a patient safety incident dashboard for communicating risk management and 'lessons learned' information to senior management, the Board of Directors, and hospital staff?
Yes 48 40.7%
Yes, but only to senior management and Board of Directors 32 27.1%
No 36 30.5%
No Response 2 1.7% Suggested Practice: Implement and/or enhance two-way communication regarding risk management activities and “lessons learned” with all levels of the organization. Question 86: In your hospital’s staff performance reviews are staff asked about awareness of hospital quality improvement and patient safety initiatives?

15
Questions, Responses, and Suggested Practice Frequency % Use
Yes 44 37.3%
No 72 61.0%
No Response 2 1.7% Suggested Practice: Increase staff awareness and knowledge of quality and patient safety initiatives and consider incorporating as part of staff performance review process. Question 89: Does the board of your hospital actively participate in risk management, quality management, and patient safety?
Yes, directly and routinely 63 53.4%
Yes, but through a board risk management subcommittee 36 30.5%
No 17 14.4%
No Response 2 1.7% Suggested Practice: Educate the board on the importance of quality and their roles and responsibility regarding quality, risk management and patient safety principles and activities. Question 101: Do staff regularly perform comfort rounds to assess and address patient needs for pain relief, toileting, and positioning?
Yes, hourly 74 62.7%
Yes, every 2 hours 32 27.1%
Yes, during shift changes 4 3.4%
Only when patients call for assistance 8 6.8%
Suggested Practice: Implement frequent and consistent rounding. Question 103: If you asked five front line providers how many do you think would
respond “I always use the repeat back technique with patients.”
0 9 7.6%
1 18 15.3%
2 31 26.3%
3 34 28.8%
4 13 11.0%
5 12 10.2%
No Response 1 0.8%
Suggested Practice: Implement teach-back techniques, and audit for compliance. Question 105: Which of the following does your hospital do to ensure smooth and safe patient transition upon admission, during shift and unit changes, and/or at discharge? (Check all that apply) Provide patients information about their medical conditions and treatment care plan in a way that is understandable to them 100 84.7%
Inform patients and family members of the next steps in their care 99 83.9% Inform patients who the responsible provider of care is during each shift and whom to contact if they have a concern about the safety or quality of care 86 72.9% Create opportunities for patients and family members to address any medical care questions or concerns with their health care providers 94 79.7% Involve patients and family members in decisions about their care at the level of involvement that they choose 98 83.1%

16
Questions, Responses, and Suggested Practice Frequency % Use Use a standard handoff communication system, such as SBAR, and a verification process to ensure that information is both received and understood 77 65.3%
Effective communication of patient care to the next provider 94 79.7%
Other 5 4.2%
Suggested Practice: Consider implementing above practices as appropriate. Question 112: Which of the following is true regarding your hospital? (Check all that apply)
There is at least one patient and family advisory council (PFAC) 18 15.3% Patients and their family members serve on key service-based and hospital-wide committees 33 28.0% The minutes of PFAC meetings and their accomplishments are provided to the hospital’s governing body and its Board of Trustees 14 11.9% Patient and family care experiences are incorporated into the hospital’s planning and day-to-day operation 77 65.3%
Suggested Practice: Consider implementing above practices as appropriate. Question 116: If you asked five front line staff on a unit about current blood stream infection rates, how many would know?
0 22 18.6%
1 19 16.1%
2 25 21.2%
3 22 18.6%
4 17 14.4%
5 11 9.3%
Not Applicable 2 1.7% Best Practice: Infection rates and other HACs should be regularly communicated on dashboards and/or via other communication mechanisms.

17
OAT Survey and Results
The “OAT Survey and Results” section provides the frequency of responses and the percentage
of respondents who indicate that they use the practice outlined in the OAT questions. This
section can be used for a drill down analysis once hospitals have identified successful domains
and domains where there are opportunities for improvement. The ten demographics are split out
into their own tables, with the domain name highlighted at the beginning of the tables.
Questions and Response Options
Frequency of
Responses
% of Indicating
Use of Practice
Baseline: Total # of Hospitals Reporting n=118
Demographics
Question 4: Region
Rural 44 37.3%
Urban 35 29.7%
Suburban 39 33.1%
Question 5: Hospital type (Check all that apply)
General 86 72.9%
Specialized 12 10.2%
Teaching 47 39.8%
Academic 12 10.2%
Non teaching 20 16.9%
For-profit 16 13.6%
Safety net 3 2.5%
Critical access 6 5.1%
Community 67 56.8%
Not-for-profit 80 67.8%
Other 3 2.5%
Question 6: What service does your hospital provide to most of its patients?
General medical and surgical 104 88.1%
Surgical 0 0.0%
Psychiatric care 0 0.0%
Tuberculosis and other respiratory diseases care 0 0.0%
Cancer care 1 0.8%
Obstetrics and gynecology 1 0.8%
Orthopedic 1 0.8%
Chronic disease care 1 0.8%
Acute long-term care 1 0.8%

18
Questions and Response Options Frequency % Use
Pediatrics 1 0.8%
Cardiac care 0 0.0%
Other 7 5.9%
Question 13: Does your hospital use an Electronic Health Records (EHR)?
Yes 84 71.2%
No 33 28.0%
No Response 1 0.8%
Question 14: If “yes”, who is your hospital’s main Electronic Health Records (EHR) Vendor?
Open Responses N/A N/A
Question 15: If "yes", Which of the following do you have in your hospital? (Check all that apply)
Computerized provider order entry (CPOE) N/A N/A
Automated checks for allergies and drug-drug interactions N/A N/A
Patient- and disease-specific reminders N/A N/A
Electronic nursing documentation N/A N/A
Question 16: If "yes", Have you evaluated whether and how an EHR is making a difference in your facility (e.g. on areas of patient care, business practices, provider productivity, risk management, medical errors, and patient education)? n=84
Yes 35 41.7%
No 20 23.8%
No, but we plan to evaluate our EHR 29 34.5%

19
Safety Culture Questions and Response Options Frequency % Use
Question 17: How strongly do you agree or disagree with the following statement? “Front line staff perceive that hospital leadership is committed to delivering necessary resources to achieve national benchmark standards on patient safety (e.g. qualified staff, appropriate medical equipment, information technology infrastructure, educational materials, laboratory)."
Strongly Agree 16 13.6%
Agree 84 71.2%
Neither 10 8.5%
Disagree 8 6.8%
Strongly Disagree 0 0.0%
Question 18: Which of the following is true about your hospital regarding adverse events? (Check all that apply)
There is a structure to triage and analyze adverse events 114 96.6%
There is frequent (monthly or more frequent) communication of adverse events to staff (e.g., through newsletter articles, meetings, presentations) 68 57.6%
Leadership routinely seeks feedback from staff on reported events and on how to reduce adverse events in the future 80 67.8%
Question 19: How are results from your hospital's survey of patient safety culture used? (Check all that apply)
Develop quality improvement interventions 84 71.2%
Tied to unit score cards 13 11.0%
Tied to the hospital’s score card 17 14.4%
Compared to national standards or benchmarks 71 60.2%
To examine the effectiveness of safety programs 74 62.7%
Tracked over time to monitor hospital safety culture 81 68.6%
Not applicable 11 9.3%
Other 2 1.7%
Question 20: What percent of hospital staff respond to the safety culture survey?
More than 90% 1 0.8%
75% - 90% 19 16.1%
Less than 75% 89 75.4%
No Response 9 7.6%
Question 21: What percent of physicians respond to the safety culture survey?
More than 90% 0 0.0%
75% - 90% 5 4.2%
Less than 75% 101 85.6%

20
Questions and Response Options Frequency % Use
No Response 12 10.2%
Question 22: Does your hospital have a system to report serious adverse events?
Yes 118 100.0%
No 0 0.0%
Question 23: If "yes", Are all serious adverse events reported in the system within 24 hours of occurrence?
Yes, every event in the past 2 years is reported 70 59.3%
No, but incident is logged and filled out later 20 16.9%
No, not always 28 23.7%
Question 24: Which of the following is true about the engagement of patients and their families in your hospital? (Check all that apply)
They take part in multidisciplinary rounds 18 15.3%
They are partners in monitoring for compliance with safety practices 41 34.7%
They actively participate on patient safety committees 59 50.0%
They participate in root cause analysis 6 5.1%
They sit on the board 32 27.1%
Question 25: If five front-line staff were asked at random, how many do you think would be able to describe a reported incident, good catch, near miss, and/or close call that led to a change (improvements in safety)?
0 1 0.8%
1 22 18.6%
2 35 29.7%
3 39 33.1%
4 16 13.6%
5 5 4.2%

21
Leadership Questions and Response Options Frequency % Use
Question 26: Does hospital leadership use a checklist to assess the priority of safety on strategic agendas of senior leadership team, high-level operational meetings, and board meetings?
Yes 23 19.5%
No 93 78.8%
No Response 2 1.7%
Question 27: If five front-line staff were asked at random to describe how patient safety leadership rounds have led to changes that improved safety, how many do you think could give a description?
0 6 5.1%
1 27 22.9%
2 21 17.8%
3 22 18.6%
4 12 10.2%
5 28 23.7%
No leadership rounds 2 1.7%
Question 28: Does your hospital have policies against disruptive and inappropriate behavior by staff?
Yes 118 100%
No 0 0%
Question 29: If "yes", How strongly do you think front line staff would agree with the following statement "If any leader or physician violated the policy against disruptive and inappropriate behavior, they would be removed from the hospital."
Strongly Agree 0 0.0%
Agree 25 21.2%
Neither 26 22.0%
Disagree 50 42.4%
Strongly Disagree 16 13.6%
No Response 1 0.8%
Measurement

22
Measurement Questions and Response Options Frequency % Use
Question 30: How does your hospital measure improvements in health-care workers' hand-hygiene adherence? (Check all that apply)
Periodically monitor and record adherence (as the number of hand-hygiene episodes performed by personnel/number of hand-hygiene opportunities) by ward or by service and provide feedback to personnel regarding their performance 111 94.1%
Monitor the volume of alcohol-based hand rub (or detergent used for hand washing or hand antisepsis) used per 1,000 patient-days 30 25.4%
Monitor adherence to policies dealing with wearing of artificial nails 62 52.5%
When outbreaks of infection occur, assess the adequacy of health care worker hand hygiene 54 45.8%
Other 6 5.1%
Question 31: Is it possible to identify patients in your hospital with each of the AHRQ Patient Safety Indicators (PSI)?
Yes, within 24 hours but with 6-week lag due to billing 36 30.5%
Yes, but it would take a couple of weeks to obtain 51 43.2%
No feasible way to find this data 23 19.5%
No Response 1 0.8%
Question 32: Would it be possible to identify patients with an International Normalized Ratio greater than 5 (INR>5)?
Yes, this can be done electronically within minutes by the lab 93 78.8%
Yes, this can be done electronically with a 1-2 week delay 9 7.6%
Yes, this can be obtained with chart review 8 6.8%
No feasible way to find this data 5 4.2%
Question 33: Would it be possible to identify patients who received the drug Argatroban from the list of patients with INR>5?
Yes, this can be done electronically within minutes 73 61.9%
Yes, this can be done electronically with a 1-2 week delay 15 12.7%
Yes, this can be done with INR>5, but would require chart review to remove Argatroban patients 21 17.8%
No feasible way to find this data 5 4.2%
No Response 4 3.4%
Question 34: Is it possible in the hospital’s current system to page or e-mail a care-giver when a patient has a lactate > 4 and is likely a septic shock patient?
Yes, this practice or something similar is used now 49 41.5%
Yes, but it is only used to identify research study patients 0 0.0%
Yes, the system allows for it but is not currently in place 31 26.3%

23
Questions and Response Options Frequency % Use
No feasible way to do this 32 27.1%
No Response 6 5.1%
Question 35: Is it possible to identify a particular group of patients (e.g. all patients with glucose below 50 ml/dL) based on lab work being done within 12 hours of admission or the location of the patient?
Yes, the hospital is able to identify patients’ location and length of time in a setting and integrate that information with other data 83 70.3%
Yes, the hospital is able to find admission time but not location information 4 3.4%
No, these data cannot be retrieved from the current system 17 14.4%
Other 9 7.6%
No Response 5 4.2%
Question 36: Which of the following practices is part of the hospital’s quality practices around measurement? (Check all that apply)
A dashboard of key results is shared at all levels of the hospital from the board to the front-line staff 92 78.0%
The data are always presented in a manner that shows the trend over time 102 86.4%
The data comprehensively cover all settings and include more than mandated core measures 100 84.7%
The performance of leadership is tied to key safety and quality measures 74 62.7%
A significant subset of the results are shared with the public; data include both positive and negative results 51 43.2%
Other 7 5.9%
Question 37: Does your hospital have a linked perinatal database (that connects preconception information, maternal medical conditions and pediatric outcomes)?
Yes 13 11.0%
No 61 51.7%
Not applicable 43 36.4%
No Response 1 0.8%
Question 38: Is it possible to electronically obtain the timeliness of administration for specific drugs?
Yes, it is possible to pull the time of any drug administration in any setting 63 53.4%
Yes, this can be pulled in some settings (e.g., ER) or for some special medications 29 24.6%
Yes, but information is used only by pharmacy and not by leadership 3 2.5%
No, can only be obtained with chart review 22 18.6%
No Response 1 0.8%

24
Questions and Response Options Frequency % Use
Question 39: Does your hospital conduct checklist-assisted data collection on pressure ulcer (PU) rates (e.g. % of at-risk patients receiving full PU preventive care) and practices (e.g. frequent monitoring of PU incidence and prevalence, comprehensive skin assessment within 24 hours of admission)?
Yes 56 47.5%
Yes, but only for PU rates 12 10.2%
Yes, but only for PU practices 16 13.6%
No 32 27.1%
Not applicable 1 0.8%
No Response 1 0.8%
Question 40: What does your hospital do to identify and minimize the risk of unexpected Emergency Department (ED) return visits? (Check all that apply)
Review/identify patients who returned unexpectedly to ED within 48 hours of discharge 69 58.5%
Immediate initiation of serious safety event investigations to prevent repeat occurrence (minimally within 24 hours of occurrence) 24 20.3%
Collect and evaluate process of care quality measures routinely 55 46.6%
Use evaluation results to introduce QI initiatives 45 38.1%
Unexpected ED return visits are reviewed by leadership outside ED 26 22.0%
Unexpected ED return visits are not monitored 11 9.3%
Other 15 12.7%
Question 41: Which of the following is applicable to your hospital? (Check all that apply)
Every unscheduled return to the OR is reviewed for quality of care issues 96 81.4%
Every unplanned transfer to a higher level of care (ICU, NICU, level 3 nursery, tertiary care hospital) is reviewed for quality of care issues 57 48.3%
Review of unplanned transfer for quality of care issues have led to improvements in the last year 44 37.3%
Question 42: Does your hospital participate in the National Database for Nursing Quality Indicators (NDNQI)?
Yes 53 44.9%
No 64 54.2%
Yes, currently a member but does not report data 1 0.8%
Question 43: If "yes", Which hospital acquired condition does your hospital report to the National Database for Nursing Quality Indicators (NDNQI)? (Check all that apply) n=53
Patient falls/Injury falls 50 94.3%
Pressure ulcers-hospital acquired 47 88.7%

25
Questions and Response Options Frequency % Use
Pressure ulcers-unit acquired 43 81.1%
CAUTI 30 56.6%
CLABSI 29 54.7%
VAP 30 56.6%
Question 44: If "yes", How does your hospital use data from NDNQI reports? (Check all that apply) n=53
For quality improvement 49 92.5%
To compare unit performance with similar units in peer hospitals 50 94.3%
For reporting (e.g., Joint Commission or CMS) 18 34.0%

26
Medication Questions and Response Options Frequency % Use
Question 45: Has your hospital completed the ISMP Medication Safety Self-Assessment for Hospitals?
Yes, the 2011 self-assessment 38 32.2%
Yes, in the last 1-5 years 33 28.0%
Yes, but more than 5 years ago 22 18.6%
Never 22 18.6%
No Response 3 2.5%
Question 46: What techniques does your hospital have to prevent harm from high-alert medications? (Check all that apply)
Standardized approach to treat patients with similar problems using order sets, preprinted order forms, and clinical protocols 104 88.1%
Standardizing concentrations and dose strengths to the minimal few needed 114 96.6%
Centralized pharmacist- or nurse-run anticoagulation services 38 32.2%
Use of reminders and information about appropriate monitoring parameters in the order sets, protocols, and flow sheets 100 84.7%
Protocols for vulnerable populations (e.g., the elderly and pediatric) 42 35.6%
Other 10 8.5%
Question 47: What error-reduction strategies are in place for administration of insulin products? (Check all that apply)
Limiting the variety of insulin products on the formulary 106 89.8%
Use of standardized protocols and formats for prescribing insulin 99 83.9%
Avoiding the use of abbreviations 111 94.1%
U500 insulin doses are prepared only in the pharmacy and are patient-specific 42 35.6%
Other 17 14.4%
Question 48: For diabetic patients is there a regular monitoring for signs and symptoms of hypoglycemia?
Yes, at least four times a day 62 52.5%
Yes,1-3 times per day 32 27.1%
Yes, but less than once per day 0 0.0%
No 17 14.4%
No Response 7 5.9%
Question 49: Does your hospital have checklist-driven protocols for the safe administration and monitoring of oxytocin for induction and augmentation of labor (e.g. Hospital Corporation of America’s Pre-Oxytocin checklist)?
Yes 42 35.6%
Yes, but checklists are used infrequently 1 0.8%

27
Questions and Response Options Frequency % Use
No 27 22.9%
Not applicable 41 34.7%
No Response 7 5.9%
Question 50: Are smart pump drug libraries developed by a multi-disciplinary team of clinicians (doctors, nurses, pharmacists)?
Yes 78 66.1%
Yes, but not by multidisciplinary team 5 4.2%
Not applicable 34 28.8%
No Response 1 0.8%
Question 51: Does your hospital have a protocol to address narcotic oversedation?
Yes 50 42.4%
Yes, but only for patients in a pain management program 11 9.3%
No 53 44.9%
Not applicable 2 1.7%
No Response 2 1.7%
Question 52: If "yes", OR "yes, but only patients in a pain management program", Does this protocol include specifications for patient monitoring? n=61
Yes 52 85.2%
No 7 11.5%
Question 53: What measures does your hospital include in its dashboard to track pharmacy performance? (Check all that apply)
Adverse drug reactions 97 82.2%
Adverse drug events 104 88.1%
Automated dispensing system discrepancies 84 71.2%
Bar code scanning compliance 50 42.4%
After hour medication use 34 28.8%
IV mixture competency of nursing staff 19 16.1%
Narcotic wasting compliance 71 60.2%
SCIP core measure compliance 87 73.7%
Overtime and medication error rate 22 18.6%
Other 9 7.6%

28
Purchasing Practice Questions and Response Options Frequency % Use
Question 54: Is there a process for identifying the 3,000+ recalls a year and assigning responsibility for addressing when appropriate?
Yes, there is a formal process to review every recall 105 89.0%
Yes, but only to evaluate high-risk recalls 10 8.5%
No, there is not 2 1.7%
No Response 1 0.8%
Question 55: Is there a procedure to notify patients when a product is recalled? Yes 90 76.3%
No 26 22.0%
No Response 2 1.7%
Question 56: Is there a process for tracking supply shortages affecting care and an
active program to reduce these shortages? Yes, and results are shared with nursing units and management regularly 88 74.6%
Yes 22 18.6%
No 6 5.1%
No Response 2 1.7%
Question 57: Which aspects of your hospital's evaluation of the safety of a device are
you aware of? (Check all that apply) Different aspects of the evaluation process (e.g., device failure, user errors, interface
design flaws, environmental factors, social factors) 94 79.7%
Staff responsible for safety evaluation 72 61.0%
Techniques used to evaluate safety 59 50.0%
Channels used to communicate evaluation results to management and different units (e.g., purchasing department) 70 59.3%
Actions taken (e.g., by purchasing department) based on results from safety evaluation of devices 77 65.3%
Other 5 4.2%
Question 58: Does your hospital regularly evaluate already-purchased devices for
safety and effectiveness (e.g. for ease of installation and user friendliness) and provide feedback to the purchasing department?
Yes, and it has impacted procurement decisions 80 67.8%
Yes, but it has not impacted procurement decisions 9 7.6%
No 27 22.9%
No Response 2 1.7%

29
Questions and Response Options Frequency % Use
Question 59: Which of the following does your hospital have to ensure safe and reliable purchases of medications? (Check all that apply)
Engagement by legal and risk management departments to better comprehend the differences between a legal and an illegal operation 26 22.0%
Development and communication of a policy for purchasing decisions and documentation of exceptions to the policy 63 53.4%
Confirmation of receipt of drug pedigree with all appropriate information 56 47.5%
Confirmation of wholesaler, distributor, and supplier licensure with authorities 88 74.6%
Keeping records of suspect suppliers 41 34.7%
Compare and scrutinize purchases and avoid using drug if there are concerns 72 61.0%
Reporting of any suspect suppliers to all appropriate authorities/hospitals (e.g., State Board of Pharmacy and the FDA’s MedWatch reporting site) 64 54.2%
Not applicable 5 4.2%
Other 13 11.0%
Question 60: Does your hospital regularly evaluate the performance of purchasing
managers and contractors? Yes, through 360 evaluations including front-line managers 19 16.1%
Yes, but only by top-level managers 71 60.2%
No 21 17.8%
Not applicable 5 4.2%
No Response 2 1.7%
Question 61: How strongly do you agree or disagree with the following statement?
“Patient safety considerations are incorporated into your hospital's purchasing decision of medical and nonmedical devices.”
Strongly Agree 52 44.1%
Agree 58 49.2%
Neither 5 4.2%
Disagree 2 1.7%
Strongly Disagree 0 0.0%
Not applicable 0 0.0%
No Response 1 0.8%
Question 62: Is your hospital's purchasing department routinely updated about
inpatient falls due to accidental/environmental reasons? Yes 59 50.0%
No 52 44.1%
Not applicable 6 5.1%
No Response 1 0.8%

30
Questions and Response Options Frequency % Use
Question 63: Is there a formal process for patient safety and risk involvement in equipment analysis and due diligence, selection, and purchasing?
Yes 78 66.1%
No 39 33.1%
No Response 1 0.8%

31
Procedural Questions and Response Options Frequency % Use
Question 64: Does your hospital have a system in place to monitor “hunting and gathering” behaviors among clinicians in general and RNs in particular?
Yes, and results are tracked by leadership 12 10.2%
Yes, but results are not tracked by leadership 9 7.6%
No 91 77.1%
No Response 6 5.1%
Question 65: What intervention strategies does your hospital have in place for hand
hygiene initiatives? (Check all that apply) Routine staff education and training on specific indications for hand hygiene 115 97.5%
Periodic performance measurement (audit) and comparative feedback on performance 109 92.4%
Visual or auditory reminders 110 93.2%
Use of multidisciplinary teams to analyze and improve hand hygiene processes 68 57.6%
Systematic performance improvement methods (e.g., establish goals, measure performance, investigate causes and contributing factors) using standard models (e.g., the plan-do-study-act (PDSA) rapid cycle improvement) 66 55.9%
Protocols for appropriate hand hygiene 105 89.0%
Guidelines for measurement and reporting of adherence to hand hygiene protocols 81 68.6%
Other 1 0.8%
Question 66: Does your hospital have a system (e.g. checklist, physician reminders, and
automatic stop orders) in place to ensure proper documentation of indication, catheter insertion, maintenance, and timely removal of urinary catheters?
Yes, in all applicable locations 68 57.6%
Yes, but in Emergency Department only 0 0.0%
Yes, but for Inpatient Department only 32 27.1%
No 18 15.3%
Not applicable 0 0.0%
Question 67: Do you have a multidisciplinary team or steering committee focused on
reaching VTE prophylaxis targets and reporting to key medical staff committees in both medicine and surgery?
Yes 59 50.0%
Yes, but only in medicine 0 0.0%
Yes, but only in surgery 18 15.3%
No 37 31.4%
Not applicable 3 2.5%
No Response 1 0.8%

32
Questions and Response Options Frequency % Use
Question 68: Does your hospital have a hospital-wide written thromboprophylaxis policy?
Yes, a fully-approved and implemented hospital-wide thromboprophylaxis policy 63 53.4%
Yes, but there is a considerable variability across units 13 11.0%
Yes, for specific patient groups, but not hospital wide 18 15.3%
No 23 19.5%
Not applicable 0 0.0%
No Response 1 0.8%
Question 69: Which of the following do you have in your hospital to ensure placement
of a mechanically ventilated patient's head between 30-45 degrees (unless medically contraindicated)? (Check all that apply)
A mechanism to ensure head-of-the-bed elevation 47 39.8%
A system for respiratory therapists to work collaboratively with nursing on positioning 81 68.6%
Education to caregivers and families about the importance of proper positioning and notify staff if supine positioning 77 65.3%
Visual cues to identify when the bed is in the proper position 45 38.1%
Include this intervention on order sets for initiation and weaning of mechanical ventilation, delivery of tube feedings, and provision of oral care 80 67.8%
Not applicable 11 9.3%
Other 5 4.2%
Question 70: Is the process of medication administration and reconciliation tracked by
management outside of pharmacy? Yes 86 72.9%
No 30 25.4%
No Response 2 1.7%
Question 71: Do you use radio opaque sponges and have clear rules for when an x-ray
is required before closing a surgical site? Yes 78 66.1%
Yes, but compliance is not audited 24 20.3%
No 8 6.8%
No Response 8 6.8%
Question 72: Which of the following is true regarding practices in your hospital to
ensure pressure ulcer assessment of all admitted patients? (Check all that apply) A system (e.g. checklists) to ensure that pressure ulcer risk assessment is conducted
within 4 hours of admission for all patients 56 47.5%
Use of a visual cue on each admission documentation record to indicate completion of a total risk assessment and reassessment 59 50.0%

33
Questions and Response Options Frequency % Use
A standard risk assessment tool (e.g. Braden scale) 115 97.5%
Methods to visually cue staff about at-risk patients (e.g. stickers on the patient chart or door) 29 24.6%
Sharing of pressure ulcer outcome measures with staff 78 66.1%
Not applicable 2 1.7%
Question 73: How often does the OB/GYN unit use a checklist (e.g. ACOG Patient Safety Checklist) to identify items/tasks that should be confirmed before or during the scheduling and performance of a procedure (e.g. elective induction and labor augmentation) AND to facilitate documentation of what was accomplished or utilized during a procedure?
Always 18 15.3%
Most of the time 9 7.6%
Sometimes 14 11.9%
Rarely 3 2.5%
Never 21 17.8%
Not applicable 46 39.0%
No Response 7 5.9%
Question 74: Your hospital has a protocol governing the timing and conditions for
elective delivery, adherence is monitored regularly, and compliance is part of re-granting privileges for physicians.
Yes 21 17.8%
Yes, but adherence is monitored infrequently 3 2.5%
Yes, but compliance is not part of re-granting privileges for physicians 31 26.3%
No 16 13.6%
Not applicable 42 35.6%
No Response 5 4.2%
Question 75: Does your hospital allow scheduling an elective delivery or c-section prior
to 39 weeks? No 35 29.7%
No, and we check gestational age 18 15.3%
Yes 16 13.6%
Not applicable 44 37.3%
No Response 5 4.2%
Question 76: Does your hospital have an active program to track and reduce elective
deliveries prior to 39 weeks? Yes 47 39.8%
No 16 13.6%
Not applicable 50 42.4%

34
Questions and Response Options Frequency % Use
No Response 5 4.2%
Question 77: Which of the following is available in your hospital to ensure a uniform
team management of shoulder dystocia? (Check all that apply) Drills 39 33.1%
Continuing medical education 46 39.0%
Interactive online courses and protocols that clarify the duties of each team member 21 17.8%
A system (e.g. checklist) to ensure appropriate documentation of the maneuvers utilized and avoided in the management of shoulder dystocia 26 22.0%
Not applicable 47 39.8%
Other 7 5.9%
Question78: Are patients who have fallen in your facility offered facilitated
environmental home assessments upon discharge? Yes 8 6.8%
Yes, but only to older patients 3 2.5%
No 107 90.7%
Question 79: Is there an automatic alarm reset when a critical alarm is turned off or
silenced (e.g. telemetry)? Yes 66 55.9%
No 35 29.7%
Not applicable 10 8.5%
No Response 7 5.9%
Question 80: Which of the following is true regarding the process and effect of
credentialing, privileging and peer review in your hospital? (Check all that apply)
Risk management is included in the peer review process of unexpected outcomes and issues relating to deviations from accepted standards of care and other risk exposures 94 79.7%
There is a process in place to support an adequate and objective medical staff and a nursing peer review process that demonstrates effectiveness for improvement 80 67.8%
Peer review has resulted in changes in protocol, purchasing, or practices 84 71.2%
Question 81: What does your hospital do to prevent recurrence of serious safety events? (Check all that apply)
Active involvement by the CEO in serious safety event prevention and apprised of effectiveness for prevention 72 61.0%
Active involvement by senior leadership in serious safety event prevention and apprised of effectiveness for prevention 108 91.5%

35
Questions and Response Options Frequency % Use
A measurement process that ensures RCA/FMEA actions are effective in preventing a repeat occurrence 84 71.2%
A system to track implementation and effectiveness of programs to reduce serious safety events 86 72.9%
Patient safety culture matrix 42 35.6%
A user friendly and "safe" reporting tool for front line staff 101 85.6%
Other 1 0.8%
Question 82: Which of the following is true regarding your hospital's patient safety practices to reduce OB adverse events? (Check all that apply)
Perinatal bundles are used for induction and vacuum extraction 26 22.0%
VBAC requirements that the entire team be in house during labor to perform immediate C/S if needed 35 29.7%
A structured process to manage shoulder dystocia should it occur 41 34.7%
Staff are certified in the ability to interpret EFM strips and the team is using the NICHD nomenclature and identification of the three-tier approach to FHT monitoring 41 34.7%
Regular simulation drills with the entire team regarding the high risk areas in OB (shoulder dystocia, timeliness of emergent C/S, post partum hemorrhage etc.) 36 30.5%
Staff training in advanced fetus monitoring 45 38.1%
Not applicable 44 37.3%
Other 5 4.2%

36
Risk Management Questions and Response Options Frequency % Use
Question 83: Which of the following is true regarding perioperative safety risk in your hospital? (Check all that apply)
There is a surgical/procedural verification protocol for patient identification, marking the site, and time out 106 89.8%
There is a count verification (i) before the procedure to establish a baseline, (ii) before the closure of a cavity within a cavity, (iii) before wound closure begins, at skin closure, at the time of permanent relief of either the scrub person or circulating nurse and wand technology 101 85.6%
There is a regular auditing for compliance of existing protocol to prevent retained foreign objects 67 56.8%
There have been no wrong site surgeries or RFBs in last 3 years 58 49.2%
There is a fire prevention program for the surgical suite, including, specific time out for laser use on ENT cases 80 67.8%
Not applicable 10 8.5%
Question 84: Are closing items in risk trend tied to leaders' performance evaluations?
Yes 16 13.6%
No 94 79.7%
No Response 8 6.8%
Question 85: Is there a patient safety incident dashboard for communicating risk management and 'lessons learned' information to senior management, the Board of Directors, and hospital staff?
Yes 48 40.7%
Yes, but only to senior management and Board of Directors 32 27.1%
No 36 30.5%
No Response 2 1.7%
Question 86: In your hospital’s staff performance reviews are staff asked about awareness of hospital quality improvement and patient safety initiatives?
Yes 44 37.3%
No 72 61.0%
No Response 2 1.7%
Question 87: How often are risk managers included during re-designing or addition of a new service (e.g. ED re-design), prior to the initiation of any physical plant work, or implementation of new service to proactively assess patient safety?
Always 17 14.4%
Frequently 38 32.2%

37
Questions and Response Options Frequency % Use
About half the time 18 15.3%
Seldom 27 22.9%
Never 14 11.9%
No Response 4 3.4%
Question 88: Are the board and governing body actively involved in risk management and patient safety decision making?
Yes 94 79.7%
No 23 19.5%
No Response 1 0.8%
Question 89: Does the board of your hospital actively participate in risk management, quality management, and patient safety?
Yes, directly and routinely 63 53.4%
Yes, but through a board risk management subcommittee 36 30.5%
No 17 14.4%
No Response 2 1.7%

38
Nursing Practice Questions and Response Options Frequency % Use
Question 90: Do nursing shifts overlap at least 30 minutes to allow adequate time for patient hand off?
Yes 111 94.1%
No 7 5.9%
Question 91: Which of the following is true regarding patient hand offs in your hospital? (Check all that apply)
They are done in front of the patient 56 47.5%
They are done face-to-face between staff 103 87.3%
They are done electronically 42 35.6%
Question 92: How often are nurses shadowed by an infection preventionist to ensure compliance with infection prevention protocols?
Weekly 44 37.3%
Monthly 18 15.3%
Quarterly 6 5.1%
Annually 10 8.5%
Never 39 33.1%
No Response 1 0.8%
Question 93: Does your hospital provide nurses with specialized training on the appropriate placement and management of urinary catheters and keep records on those who have and have not received training?
Yes 81 68.6%
No 36 30.5%
Not applicable 1 0.8%
Question 94: Are reports about the necessity of urinary catheters reviewed daily by nursing staff and trended data reviewed by hospital management?
Yes 79 66.9%
No 36 30.5%
Not applicable 2 1.7%
No Response 1 0.8%
Question 95: Do nursing protocols allow for removal of urinary catheters without physician order if criteria for necessity are not met?
yes 39 33.1%
No 76 64.4%
Not applicable 1 0.8%
No Response 2 1.7%

39
Questions and Response Options Frequency % Use
Question 96: Does the hospital have a nurse driven protocol for removing unnecessary urinary catheters?
Yes 47 39.8%
No 70 59.3%
Not applicable 1 0.8%
Question 97: Does the hospital have guidelines for nurse directed use of intermittent catheterization and use of bladder ultrasound scanners?
Yes 57 48.3%
No 58 49.2%
Not applicable 2 1.7%
No Response 1 0.8%
Question 98: Are nurses authorized to enforce use of a central line checklist to be sure all processes related to central line placement, including hand hygiene, are executed for each line placement?
Yes 97 82.2%
No 9 7.6%
Not applicable 9 7.6%
No Response 3 2.5%
Question 99: How often would physicians be stopped if they failed to comply with any portion of the central line checklist?
Always 20 16.9%
Frequently 49 41.5%
About half the time 17 14.4%
Seldom 11 9.3%
Never 4 3.4%
Not applicable 14 11.9%
No Response 3 2.5%
Question 100: Does your hospital have a process for evaluating staff competence in recognizing the signs and symptoms of sepsis and an evolving stroke?
Yes 32 27.1%
Yes, but only for sepsis 4 3.4%
Yes, but only for an evolving stroke 29 24.6%
No 50 42.4%
Not applicable 1 0.8%
No Response 2 1.7%

40
Questions and Response Options Frequency % Use
Question 101: Do staff regularly perform comfort rounds to assess and address patient needs for pain relief, toileting, and positioning?
Yes, hourly 74 62.7%
Yes, every 2 hours 32 27.1%
Yes, during shift changes 4 3.4%
Only when patients call for assistance 8 6.8%

41
Communication Questions and Response Options Frequency % Use
Question 102: Did your hospital have an event requiring a root cause analysis in the last two years where the root cause was determined to be lack of proper and timely communication between staff?
No serious event in the last 2 years 17 14.4%
Yes, but not sure how many 55 46.6%
Yes, we know how many cases we had 43 36.4%
No Response 3 2.5%
Question 103: If you asked five front line providers how many do you think would respond “I always use the repeat back technique with patients.”
0 9 7.6%
1 18 15.3%
2 31 26.3%
3 34 28.8%
4 13 11.0%
5 12 10.2%
No Response 1 0.8%
Question 104: How strongly do you agree or disagree with the following statement: “Staff follow a standardized and effective method of sharing information when handing off patients." Strongly Agree 14 11.9% Agree 77 65.3% Neither 18 15.3% Disagree 9 7.6% Strongly Disagree 0 0.0%
Question 105: Which of the following does your hospital do to ensure smooth and safe patient transition upon admission, during shift and unit changes, and/or at discharge? (Check all that apply)
Provide patients information about their medical conditions and treatment care plan in a way that is understandable to them 100 84.7% Inform patients and family members of the next steps in their care 99 83.9%
Inform patients who the responsible provider of care is during each shift and whom to contact if they have a concern about the safety or quality of care 86 72.9%
Create opportunities for patients and family members to address any medical care questions or concerns with their health care providers 94 79.7%
Involve patients and family members in decisions about their care at the level of involvement that they choose 98 83.1%

42
Questions and Response Options Frequency % Use
Use a standard handoff communication system, such as SBAR, and a verification process to ensure that information is both received and understood 77 65.3%
Effective communication of patient care to the next provider 94 79.7% Other 5 4.2%
Question 106: Which of the following is true regarding your hospital's hand off protocol during surgery? (Check all that apply) Limited interruptions during handoff 81 68.6%
Up-to-date information is communicated regarding patient identification, patients condition, care, treatment, medications, services and any recent or anticipated changes 98 83.1%
A method to verify the received information, including repeat-back or read-back techniques, is used 53 44.9%
There is an opportunity for the receiver of the handoff information to review relevant patient historical data, which may include previous care, treatment or services 76 64.4%
A system (e.g., an electronic medical record) to streamline the exchange of timely and accurate information is used 53 44.9%
Not applicable 12 10.2%
Question 107: Upon admission, do the physician, nurse, and pharmacist assess the patient together as a team and work collaboratively to develop a specific care plan for each patient? Yes 12 10.2% No 106 89.8%
Question 108: Is there an electronic medical record for each patient that allows staff to track the progress of a patient's care and share health information among providers from different service areas within the hospitals?
Yes 75 63.6%
No 43 36.4%
Question 109: Prior to discharging a patient at high risk of readmission is a face-to-face follow-up visit scheduled within 48 hours of discharge?
Yes 17 14.4% No 98 83.1%
Question 110: Prior to discharging a patient at moderate risk of readmission is a follow-up phone call scheduled within 48 hours of discharge?
Yes 40 33.9% No 76 64.4%

43
Questions and Response Options Frequency % Use
Question 111: How would your staff rate the support your hospital provides to a family/care taker of a patient in crisis? Excellent 39 33.1% Good 70 59.3% Fair 9 7.6% Poor 0 0.0%
Question 112: Which of the following is true regarding your hospital? (Check all that apply) There is at least one patient and family advisory council (PFAC) 18 15.3%
Patients and their family members serve on key service-based and hospital-wide committees 33 28.0%
The minutes of PFAC meetings and their accomplishments are provided to the hospital’s governing body and its Board of Trustees 14 11.9%
Patient and family care experiences are incorporated into the hospital’s planning and day-to-day operation 77 65.3%
Question 113: Are front-line workers trained in communication techniques to promote assertiveness?
Yes 42 35.6%
No 75 63.6%
No Response 1 0.8%
Question 114: Are patient rounds undertaken by interdisciplinary teams (e.g. physicians, nurses, pharmacist, patient advocates) to promote cross-communication under all settings?
Yes 56 47.5%
No 62 52.5%
Question 115: Are failures to meet antibiotic timing, selection, or discontinuation communicated to the staff physician? Yes, within 24 hours of occurrence 35 29.7% Yes, but not within 24 hours 72 61.0% No, they are not communicated 7 5.9% No Response 4 3.4%
Question 116: If you asked five front line staff on a unit about current blood stream infection rates, how many would know?
0 22 18.6%
1 19 16.1%
2 25 21.2%
3 22 18.6%

44
Questions and Response Options Frequency % Use
4 17 14.4%
5 11 9.3%
Not Applicable 2 1.7%
Question 117: Does your hospital provide information about the risk of VTE and its prevention to patients? Yes, 80% or more of all patients 38 32.2% Yes, at least 50% of patients 33 28.0%
Yes, at key patient encounter sites (e.g. admitting department, hospital lobbies, nursing units) 7 5.9% Not at all 36 30.5% Not applicable 1 0.8% No Response 3 2.5%
Question 118: Are visual indicators used to quickly communicate with the care team about patients at risk of fall or injury (e.g. use of colorful socks, colored wrist bands and/or blankets, or signage outside and inside the room to indicate fall and/or injury risk)?
Yes 116 98.3%
No 1 0.8%
No Response 1 0.8%
Question 119: Are patients and family members educated about risk of injury from a fall on admission and during hospital stay, and about what they can do to help prevent a fall using one of the following proven patient educational methods? (Check all that apply) Teach back 40 33.9% Return demonstration or show back 13 11.0%
“Ask Me 3” (Encourage patients to ask their providers three questions: What is my main problem? What do I need to do (for that problem)? Why is that important?) 11 9.3% Signed contract of expected behavior for families 6 5.1%
There is no formal process for communicating with patients/their families 35 29.7%
Other 39 33.1%
0.0%
Question 120: Which of the following is true about communication of critical values in your hospital? (Check all that apply)
There are protocols in place to alert physicians of critical values (e.g., laboratory, radiology) 117 99.2%
There is evidence of documentation of who was notified, by whom, time, response, and actions taken 115 97.5%
Loop is closed on labs ordered before discharge but results are not available until after discharge 44 37.3%

45
Infection Control Questions and Response Options Frequency % Use
Question 121: Does your hospital use CDC national healthcare safety network (NHSN) definitions for central line-associated blood stream infection in all locations and for all types of central venous catheters (PICC)? Yes 118 100.0% No 0 0.0% Not applicable 0 0.0%
Question 122: What is your hospital doing to ensure compliance with patient care practices to reduce the incidence of VAP? (Check all that apply)
Institute written policies, protocols, or pathways that describe the recommended practices for prevention of VAP 98 83.1%
Routinely collect data on process measures (e.g., hand hygiene compliance, sedation interruption, oral care, maintenance of 30-45 degrees positioning, and assessment of readiness to wean) related to VAP 80 67.8%
Assess if results based on collected process measures demonstrate compliance to recommended practices 72 61.0%
Report results from collected measures and assessment to senior leadership, nursing leadership, and care providers 74 62.7% Enforce QI initiatives targeted at addressing identified areas of improvement 74 62.7% Not applicable 11 9.3% Other 9 7.6%
Question 123: Does your hospital have a PICC team for PICC line placement and maintenance? Yes 55 46.6% Yes, outside contractual services 4 3.4% No 48 40.7% Not applicable 11 9.3%
Question 124: Are PICC line dressings routinely changed by a PICC team member
Yes 48 40.7%
No 42 35.6%
Not applicable 28 23.7%
Question 125: How often does your ICU/Clinical Care Area currently use a positive displacement needle-less connector valve for central venous catheters? Always 76 64.4% Frequently 12 10.2% About half the time 0 0.0% Seldom 2 1.7%

46
Questions and Response Options Frequency % Use Never 15 12.7% Not applicable 11 9.3% No Response 2 1.7%
Question 126: How often does your ICU/Clinical Care Area currently bathe patients in this clinical care area with chlorhexidine? Always 21 17.8% Frequently 7 5.9% About half the time 1 0.8% Seldom 23 19.5% Never 50 42.4% Not applicable 10 8.5% No Response 6 5.1%
Question 127: Do you routinely use ultrasound to place central venous catheters? (Check all that apply) Yes, for subclavian lines 38 32.2% Yes, for internal jugular lines 30 25.4% No 60 50.8% Not applicable 13 11.0%
Question 128: How often do you document the removal of urinary catheters post-operatively within 24-48 hours unless there are appropriate indications for continued use? Always 46 39.0% Frequently 53 44.9% About half the time 6 5.1% Seldom 1 0.8% Never 2 1.7% Not applicable 10 8.5%
Question 129: Is the use of proper aseptic technique and sterile equipment for urinary catheter insertion audited? Yes, in all applicable units and frequently 25 21.2% Yes, in all applicable units but not frequently 41 34.7% Never 52 44.1% Not applicable 0 0.0%
Audit urinary catheter insertion and aseptic technique for all units, frequently
Question 130: How often is systemic anti-microbial prophylaxis used for urinary catheters? Always 8 6.8% Frequently 6 5.1%

47
Questions and Response Options Frequency % Use About half the time 2 1.7% Seldom 22 18.6% Never 73 61.9% Not applicable 3 2.5% No Response 4 3.4%
Question 131: Does the hospital require a documented rationale for Foley catheter in all settings? Yes 72 61.0% No 44 37.3% Not applicable 1 0.8% No Response 1 0.8%
Question 132: How often does your hospital conduct checklist-driven monitoring of guidelines for appropriate perioperative catheter management (e.g. procedure-specific guidelines for catheter placement and postoperative catheter removal and management of postoperative urinary retention)? Always 27 22.9% Frequently 22 18.6% About half the time 2 1.7% Seldom 11 9.3% Never 40 33.9% Not applicable 12 10.2% No Response 4 3.4%
Question 133: Who inserts urinary catheters at your facility? (Check all that apply) RNs 118 100.0% LPNs 72 61.0% Nurse aides 11 9.3% Physicians 93 78.8% Medical Students 26 22.0% Not applicable 0 0.0% Other 16 13.6%
Question 134: Are urinary catheter days tracked? (Check all that apply) Yes, electronically 48 40.7% Yes, manually 77 65.3% No 3 2.5% Not applicable 0 0.0%

48
Questions and Response Options Frequency % Use
Question 135: Does your hospital have a comprehensive program to reduce CAUTI, including reducing catheter days, bladder bundle tracking, sterile technique placement, and reason for catheter at time of placement that is reviewed by senior leadership? Yes 64 54.2% Yes, but it is not comprehensive or linked to senior leadership 29 24.6% No 25 21.2% Not applicable 0 0.0%
Question 136: Do standard supply kits exist that include catheter and all necessary items? (Check all that apply) Yes, for indwelling (Foley) catheters 114 96.6% Yes, for central line catheters 102 86.4% No 4 3.4% Not applicable 0 0.0%
Question 137: Does your hospital utilize a surgical safety checklist (e.g. the World Health Organization Surgical Safety Checklist or an adaptation) prior to surgical procedures to verify (at a minimum) patient identity, allergies, and preoperative antibiotics (when required)? Yes, fully implemented throughout hospital 86 72.9% Yes, fully implemented in some areas 16 13.6% Yes, partially implemented in some or all areas 3 2.5% No, no plan to use surgical safety checklist 5 4.2% No, but is planning to use one 1 0.8% No Response 7 5.9%
Question 138: What does your hospital have in place to ensure proper endoscope processing/disinfecting? (Check all that apply)
A quality system program that covers all aspects of endoscopy procedure management 78 66.1%
A written procedure for monitoring adherence to the program and a chain of accountability 82 69.5%
A system to ensure that staff responsible for endoscope processing understand proper use and maintain proficiency in performing it 98 83.1% A routine monitoring to ensure compliance with recommended practices 81 68.6%

49
Resources and Toolkits
This section of the toolkit includes links to external sources that contain useful resources,
toolkits, and information that can be used once hospitals have prioritized their areas for
improvement, and are developing their action plans.
Implementation Support Packages
The following links will direct you to the Implementation Support Packages that were created by
the National Content Developer (NCD). The NCD created these Implementation Support
Packages to pull strategies, tools, and resources into a single package that hospitals can use when
working to build or enhance their organization’s safety culture. The first package includes
information on patient safety culture and the second package is focused on patient safety
leadership and board engagement.
Both packages are similarly structured and include an introduction, an improvement model,
information on measurement and quality improvement, strategies for patient safety culture and
leadership, tools & resources, and appendices. The tools and resources that are included in these
packages will be particularly helpful and meaningful to Pennsylvania hospitals after they analyze
their OAT results and begin developing their improvement plans.
Implementation Support Package: Patient Safety Culture
Implementation Support Package: Leadership/Board Engagement
Quality Curriculum for Trustees
The Hospital & Healthsystem Association of Pennsylvania (HAP) has partnered with the
American Hospital Association’s (AHA) Center for Healthcare Governance and the
Pennsylvania Patient Safety Authority to provide the Quality Curriculum for Trustees to hospital
boards in Pennsylvania.
As a governance resource, this curriculum offers unique guidance to boards and hospital
leadership to take a fresh look at quality program oversight, which is more important than ever
given the changes happening as a result of health care reform.
The curriculum is timely and relevant for any organization interested in improving quality
performance and more effectively driving quality and patient safety initiatives. The lessons that
boards will learn through this program will support the patient safety and quality improvement
projects that are being conducted in PA-HEN hospitals.
Please visit the Quality Curriculum for Trustees webpage, or contact Kelly Thompson, senior
director of regulatory advocacy at HAP, for more information.

50
PassKey: The PA-HEN Collaborative Workspace
PassKey, developed by the Pennsylvania Patient Safety Authority, is an electronic collaborative
workspace being utilized to support the PA-HEN Partnership for Patients (PfP) collaborative
projects. Through PassKey, hospital key contacts and hospital project team members have access
to educational materials, calendars, data portals, surveys, and informational libraries.
For more information and access to resources, please visit the PassKey website and enter your
PfP credentials to gain access to PassKey.
Comprehensive Changes to Foster a Culture of Safety
The following suggested practices have been compiled by the Institute for Healthcare
Improvement (IHI) and are suggested to facilitate a culture that embraces patient safety and that
sustains quality improvement efforts. To access greater detail on how to implement these
changes, click on the title of the change that you are interested in and you will be directed to the
IHI website.
1. Appoint a Safety Champion for Every Unit
Having a designated safety champion in every department and patient care unit
demonstrates the organization’s commitment to safety, and may make other staff
members feel more comfortable about sharing information and asking questions.
Champions must have proper training, resources, and authority.
2. Conduct Patient Safety Leadership WalkRoundsTM
Senior leaders wishing to demonstrate their commitment to safety and to learn about the
safety issues in their own organization can do so by making regular rounds for the sole
purpose of discussing safety with the staff. During the WalkRounds™, there should be
two-way communication, with both the executives and the staff talking honestly and
listening carefully.
3. Conduct Safety Briefings
Safety briefings in patient care units increase safety awareness among front-line staff and
foster a culture of safety. Based on concepts in aviation and other industries, briefings
make safety-consciousness part of the routine, 24 hours a day and seven days a week.
4. Create a Reporting System
In a culture of safety, staff members are aware of safety issues and are free to report
conditions that could lead to near misses or actual adverse events. This open exchange of
information requires the management to have a non-punitive response philosophy that
rewards reporting of safety issues and events, and does not punish staff members
involved in errors or adverse events related to system failures.

51
5. Create an Adverse Event Response Team
After any adverse event, members of the response team take prompt action to keep the
atmosphere in the unit calm; do whatever is possible to mitigate harm to the patient and
prevent further harm; curtail any undue punitive action; review details of the event; and
support the family, staff and physicians.
6. Designate a Patient Safety Officer
True commitment to patient safety requires action, not just statements about its
importance. Organizations fully committed to safety designate a dedicated patient safety
officer, an individual who promotes action through training of staff and implementation
of proven methods.
7. Develop a Culture of Safety
An organization can improve upon safety only when leaders are visibly committed to
change and when they enable staff to openly share safety information. When an
organization does not have such a culture, staff members are often unwilling to report
adverse events and unsafe conditions because they fear reprisal or believe reporting will
not result in any change.
8. Provide Feedback to Front-Line Staff
Feedback to the front-line staff demonstrates a commitment to safety and ensures that
staff members continue to report safety issues. If the leadership acts upon suggestions,
staff members should know their voices were heard and should be recognized for their
contributions, especially when the leadership’s response would otherwise be invisible
from the front lines.
9. Reenact Real Adverse Events from Your Hospital
Using staff members as actors, a simple skit or videotape of a reenacted adverse event or
near miss can raise safety awareness and teach both staff and management valuable
safety lessons. You can tell one true story or patch together real or plausible events to
create a fictional composite. A commentary from the patient safety officer, senior leader,
or the people involved in the real event can be a powerful ending that reinforces the
management’s non-punitive safety culture.
10. Relay Safety Reports at Shift Changes
Certain situations increase the risk of adverse events and should prompt staff to be even
more safety-conscious than usual. Examples include patients with the same last name,
trials of new equipment, and research protocols. Identifying these higher-risk situations
and bringing them to the attention of all staff members at the start of each shift decreases
the likelihood of errors and adverse events.

52
11. Simulate Possible Adverse Events
Many other industries, particularly aviation, use simulation to teach people to recognize
problems and understand the effects of their responses in a safe environment. The
technique is particularly helpful in preparing people for error-prone, high-risk, or unusual
situations. Simulation has many applications in health care, and an organization’s
investment of staff time in simulation or in a patient safety laboratory demonstrates the
leadership’s commitment to a culture of safety.

53
Thank you for joining the PA-HEN and for working so diligently to address quality and
patient safety in Pennsylvania. Transforming health care and integrating these changes
into everyday practice is not easy. We applaud your great efforts and dedication to
protecting patients and saving lives.
###

ORGANIZATIONAL ASSESSMENT TOOL (OAT)
This evidenced-based tool is being developed by the National Content Developer (NCD) as a resource for the Hospital Engagement Networks (HENs) and their partner hospitals to achieve the goals of the Partnership for Patients and support efforts to expand the use
of models shown to improve care. The first section includes questions to gather data on hospital location and other hospital-level characteristics. Subsequent sections are organized by 10 areas of focus: safety culture, leadership, measurement, medication,
purchasing practice, procedural, risk management, nursing practice, communication, and infection control. Completion of the OAT should be led by the hospital’s patient safety officer, quality improvement director, or equivalent. It is expected that this individual will
contact appropriate staff to complete the OAT. Only a single OAT should be completed for a hospital.
1. DEMOGRAPHICS
1. Hospital name UPMC St. Margaret 2. State
Alabama Alaska Arizona Arkansas California Colorado Connecticut Delaware District of Columbia Florida Georgia Hawaii Idaho Illinois Indiana Iowa

Kansas Kentucky Louisiana Maine Maryland Massachusetts Michigan Minnesota Mississippi Missouri Montana Nebraska Nevada New Hampshire New Jersey New Mexico New York North Carolina North Dakota Ohio Oklahoma Oregon Pennsylvania Rhode Island South Carolina South Dakota Tennessee Texas Utah Vermont Virginia Washington West Virginia Wisconsin

Wyoming 3. Zip code 15215 4. Region Rural Urban Suburban 5. Hospital type (Check all that apply) General For-profit Specialized Safety net Teaching Critical access Academic Community Non teaching Not-for-profit Other
Please specify
6. What service does your hospital provide to most of its patients? General medical and surgical Obstetrics and gynecology Surgical Orthopedic Psychiatric care Chronic disease care Tuberculosis and other respiratory diseases care Acute long-term care Cancer care Pediatrics Other Cardiac care Please specify
7. Hospital Identifier AHA ID 6232610
National Provider Identifier (NPI)
1790795359
Other Identifier

8. Title/Role of person completing the OAT Executive Director, Care Management/Quality 9. Total number of licensed beds in the hospital 249 10. Average daily census in the hospital 215 11. Average annual admissions per 100,000 population over the last 5 years 9185 12. Which Hospital Engagement Network (HEN) is your hospital associated with? American Hospital Association Ascension Health Carolinas HealthCare System Dignity Health (formerly known as Catholic Healthcare West) Dallas-Fort Worth Hospital Council Foundation Georgia Hospital Association Research and Education Foundation Healthcare Association of New York State Hospital & Healthsystem Association of Pennsylvania Intermountain Healthcare Iowa Healthcare Collaborative Joint Commission Resources, Inc. Lifepoint Hospitals, Inc. Michigan Health & Hospital Association Minnesota Hospital Association National Public Health and Hospital Institute New Jersey Hospital Association Nevada Hospital Association North Carolina Hospital Association Ohio Children’s Hospital Solutions for Patient Safety Ohio Hospital Association Premier Inc.

Tennessee Hospital Association Texas Center for Quality & Patient Safety UHC VHA Washington State Hospital Association 13. Does your hospital use an Electronic Health Records (EHR)? Yes No 14. Who is your hospital’s main Electronic Health Records (EHR) vendor? Cerner 15. Which of the following do you have in your hospital? (Check all that apply) Computerized provider order entry (CPOE) Automated checks for allergies and drug-drug interactions Patient- and disease-specific reminders Electronic nursing documentation 16. Have you evaluated whether and how an EHR is making a difference in your facility (e.g., on areas of patient care, business
practices, provider productivity, risk management, medical errors, and patient education)? Yes No No, but we plan to evaluate our EHR
2. SAFETY CULTURE
17. How strongly do you agree or disagree with the following statement? “Front-line staff perceive that hospital leadership is
committed to delivering necessary resources to achieve national benchmark standards on patient safety (e.g., qualified staff, appropriate medical equipment, information technology infrastructure, educational materials, laboratory).”
Strongly Agree Neither Strongly Disagree Agree Disagree
18. Which of the following is true about your hospital regarding adverse events? (Check all that apply)

There is a structure to triage and analyze adverse events There is frequent (monthly or more frequent) communication of adverse events to staff (e.g., through newsletter articles,
meetings, presentations) Leadership routinely seeks feedback from staff on reported events and on how to reduce adverse events in the future 19. How are results from your hospital’s survey of patient safety culture used? (Check all that apply) Develop quality improvement interventions Tied to unit score cards Tied to the hospital’s score card Compared to national standards or benchmarks To examine the effectiveness of safety programs Tracked over time to monitor hospital safety culture Not applicable Other Please specify
20. What percent of hospital staff respond to the safety culture survey? More than 90% 75% - 90% Less than 75% 21. What percent of physicians respond to the safety culture survey? More than 90% 75% - 90% Less than 75% 22. Does your hospital have a system to report serious adverse events? Yes No 23. Are all serious adverse events reported in the system within 24 hours of occurrence? Yes, every event in the past 2 years is reported No, but incident is logged and filled out later No, not always
24. Which of the following is true about the engagement of patients and their families in your hospital? (Check all that apply) They take part in multidisciplinary rounds

They are partners in monitoring for compliance with safety practices They actively participate on patient safety committees They participate in root cause analysis They sit on the board If patients and their families do not currently sit on the board, but you plan to add them, please specify month and year Unable to determine at this time 25. If five front-line staff were asked at random, how many do you think would be able to describe a reported incident, good catch,
near miss, and/or close call that led to a change (improvements in safety)? 0 1 2 3 4 5
3. LEADERSHIP
26. Does hospital leadership use a checklist to assess the priority of safety on strategic agendas of senior leadership team, high-level
operational meetings, and board meetings? Yes No 27. If five front-line staff were asked at random to describe how patient safety leadership rounds have led to changes that improved
safety, how many do you think could give a description? 0 3 No leadership rounds 1 4
2 5
28. Does your hospital have policies against disruptive and inappropriate behavior by staff? Yes No 29. How strongly do you think front line staff would agree with the following statement: “If any leader or physician violated the policy
against disruptive and inappropriate behavior, they would be removed from the hospital.” Strongly Agree Neither Strongly Disagree Agree Disagree
4. MEASUREMENT

30. How does your hospital measure improvements in health care workers' hand-hygiene adherence? (Check all that apply) Periodically monitor and record adherence (as the number of hand-hygiene episodes performed by personnel/number of
hand-hygiene opportunities) by ward or by service and provide feedback to personnel regarding their performance Monitor the volume of alcohol-based hand rub (or detergent used for hand washing or hand antisepsis) used per 1,000
patient-days Monitor adherence to policies dealing with wearing of artificial nails When outbreaks of infection occur, assess the adequacy of health care worker hand hygiene Other Please specify
31. Is it possible to identify patients in your hospital with each of the AHRQ Patient Safety Indicators (PSI)? Yes, within 24 hours but with 6-week lag due to billing Yes, but it would take a couple of weeks to obtain No feasible way to find this data 32. Would it be possible to identify patients with an International Normalized Ratio greater than 5 (INR>5)? Yes, this can be done electronically within minutes by the lab Yes, this can be done electronically with a 1-2 week delay Yes, this can be obtained with chart review No feasible way to find this data 33. Would it be possible to identify patients who received the drug Argatroban from the list of patients with INR>5? Yes, this can be done electronically within minutes Yes, this can be done electronically with a 1-2 week delay Yes, this can be done with INR>5, but would require chart review to remove Argatroban patients No feasible way to find this data 34. Is it possible in the hospital’s current system to page or email a caregiver when a patient has a lactate > 4 and is likely a septic
shock patient? Yes, this practice or something similar is used now Yes, but it is only used to identify research study patients Yes, the system allows for it but is not currently in place

No feasible way to do this 35. Is it possible to identify a particular group of patients (e.g., all patients with glucose below 50 ml/dL) based on lab work being done
within 12 hours of admission or the location of the patient? Yes, the hospital is able to identify patients’ location and length of time in a setting and integrate that information with other
data Yes, the hospital is able to find admission time but not location information No, these data cannot be retrieved from the current system Other Please specify
36. Which of the following practices is part of the hospital’s quality practices around measurement? (Check all that apply) A dashboard of key results is shared at all levels of the hospital from the board to the front-line staff The data are always presented in a manner that shows the trend over time The data comprehensively cover all settings and include more than mandated core measures The performance of leadership is tied to key safety and quality measures A significant subset of the results are shared with the public; data include both positive and negative results Other Please specify
37. Does your hospital have a linked perinatal database (that connects preconception information, maternal medical conditions, and
pediatric outcomes)? Yes No Not applicable 38. Is it possible to electronically obtain the timeliness of administration for specific drugs? Yes, it is possible to pull the time of any drug administration in any setting Yes, this can be pulled in some settings (e.g., ER) or for some special medications Yes, but information is used only by pharmacy and not by leadership No, can only be obtained with chart review

39. Does your hospital conduct checklist-assisted data collection on pressure ulcer (PU) rates (e.g., % of at-risk patients receiving full PU preventive care) and practices (e.g., frequent monitoring of PU incidence and prevalence, comprehensive skin assessment within 24 hours of admission)?
Yes Yes, but only for PU practices Not applicable Yes, but only for PU rates No
40. What does your hospital do to identify and minimize the risk of unexpected Emergency Department (ED) return visits? (Check all
that apply) Review/identify patients who returned unexpectedly to ED within 48 hours of discharge Immediate initiation of serious safety event investigations to prevent repeat occurrence (minimally within 24 hours of
occurrence) Collect and evaluate process of care quality measures routinely Use evaluation results to introduce QI initiatives Unexpected ED return visits are reviewed by leadership outside ED Unexpected ED return visits are not monitored Other Please specify
41. Which of the following is applicable to your hospital? (Check all that apply) Every unscheduled return to the OR is reviewed for quality of care issues Every unplanned transfer to a higher level of care (ICU, NICU, level 3 nursery, tertiary care hospital) is reviewed for quality of
care issues Review of unplanned transfer for quality of care issues have led to improvements in the last year 42. Does your hospital participate in the National Database for Nursing Quality Indicators (NDNQI)? Yes No Yes, currently a member but does not report data
43. Which hospital acquired condition does your hospital report to the National Database for Nursing Quality Indicators (NDNQI)?
(Check all that apply) Patient falls/Injury falls Pressure ulcers-unit acquired CLABSI Pressure ulcers-hospital
acquired
CAUTI VAP

44. How does your hospital use data from NDNQI reports? (Check all that apply) For quality improvement To compare unit performance with similar units in peer hospitals For reporting (e.g., Joint Commission or CMS)
5. MEDICATION
45. Has your hospital completed the ISMP Medication Safety Self-Assessment for Hospitals? Yes, the 2011 self-assessment Yes, but more than 5 years ago Yes, in the last 1-5 years Never 46. What techniques does your hospital have to prevent harm from high-alert medications? (Check all that apply) Standardized approach to treat patients with similar problems using order sets, preprinted order forms, and clinical protocols Standardizing concentrations and dose strengths to the minimal few needed Centralized pharmacist- or nurse-run anticoagulation services Use of reminders and information about appropriate monitoring parameters in the order sets, protocols, and flow sheets Protocols for vulnerable populations (e.g., the elderly and pediatric) Other Please specify inventory warning labels,speciality bin storage, and double witnessing 47. What error-reduction strategies are in place for administration of insulin products? (Check all that apply) Limiting the variety of insulin products on the formulary Use of standardized protocols and formats for prescribing insulin Avoiding the use of abbreviations U500 insulin doses are prepared only in the pharmacy and are patient-specific Other Please specify Switching over to insulin pens. Do not stock U-500 48. For diabetic patients, is there a regular monitoring for signs and symptoms of hypoglycemia? Yes, at least four times a day Yes, but less than once per day

Yes,1-3 times per day No 49. Does your hospital have checklist-driven protocols for the safe administration and monitoring of oxytocin for induction and
augmentation of labor (e.g., Hospital Corporation of America’s Pre-Oxytocin checklist)? Yes No Yes, but checklists are used infrequently Not applicable 50. Are smart pump drug libraries developed by a multidisciplinary team of clinicians (doctors, nurses, pharmacists)? Yes Not applicable Yes, but not by multidisciplinary team
51. Does your hospital have a protocol to address narcotic oversedation? Yes Yes, but only for patients in a pain management program No Not applicable 52. Does this protocol include specifications for patient monitoring? Yes No 53. What measures does your hospital include in its dashboard to track pharmacy performance? (Check all that apply) Adverse drug reactions IV mixture competency of nursing staff Adverse drug events Narcotic wasting compliance Automated dispensing system discrepancies SCIP core measure compliance Bar code scanning compliance Overtime and medication error rate After hour medication use Other Please specify POS dispensing machine overrides
6. PURCHASING PRACTICE
54. Is there a process for identifying the 3,000+ recalls a year and assigning responsibility for addressing when appropriate? Yes, there is a formal process to review every recall

Yes, but only to evaluate high-risk recalls No, there is not 55. Is there a procedure to notify patients when a product is recalled? Yes No 56. Is there a process for tracking supply shortages affecting care and an active program to reduce these shortages? Yes, and results are shared with nursing units and management regularly Yes No 57. Which aspects of your hospital’s evaluation of the safety of a device are you aware of? (Check all that apply) Different aspects of the evaluation process (e.g., device failure, user errors, interface design flaws, environmental factors,
social factors) Staff responsible for safety evaluation Techniques used to evaluate safety Channels used to communicate evaluation results to management and different units (e.g., purchasing department) Actions taken (e.g., by purchasing department) based on results from safety evaluation of devices Other Please specify
58. Does your hospital regularly evaluate already-purchased devices for safety and effectiveness (e.g., for ease of installation and
user friendliness) and provide feedback to the purchasing department? Yes, and it has impacted procurement decisions Yes, but it has not impacted procurement decisions No 59. Which of the following does your hospital have to ensure safe and reliable purchases of medications? (Check all that apply) Engagement by legal and risk management departments to better comprehend the differences between a legal and an illegal
operation Development and communication of a policy for purchasing decisions and documentation of exceptions to the policy Confirmation of receipt of drug pedigree with all appropriate information Confirmation of wholesaler, distributor, and supplier licensure with authorities

Keeping records of suspect suppliers Compare and scrutinize purchases and avoid using drug if there are concerns Reporting of any suspect suppliers to all appropriate authorities/hospitals (e.g., State Board of Pharmacy and the FDA’s
MedWatch reporting site) Not applicable Other Please specify Purchasing overseen by corporate owned drug wholesaler 60. Does your hospital regularly evaluate the performance of purchasing managers and contractors? Yes, through 360 evaluations including front-line managers Yes, but only by top-level managers No Not applicable 61. How strongly do you agree or disagree with the following statement? “Patient safety considerations are incorporated into your
hospital’s purchasing decision of medical and nonmedical devices.” Strongly Agree Neither Strongly Disagree Agree Disagree Not applicable 62. Is your hospital’s purchasing department routinely updated about inpatient falls due to accidental/environmental reasons? Yes No Not applicable 63. Is there a formal process for patient safety and risk involvement in equipment analysis and due diligence, selection, and
purchasing? Yes No
7. PROCEDURAL
64. Does your hospital have a system in place to monitor “hunting and gathering” behaviors among clinicians in general and RNs in
particular? Yes, and results are tracked by leadership Yes, but results are not tracked by leadership

No 65. What intervention strategies does your hospital have in place for hand hygiene initiatives? (Check all that apply) Routine staff education and training on specific indications for hand hygiene Periodic performance measurement (audit) and comparative feedback on performance Visual or auditory reminders Use of multidisciplinary teams to analyze and improve hand hygiene processes Systematic performance improvement methods (e.g., establish goals, measure performance, investigate causes and
contributing factors) using standard models (e.g., the plan-do-study-act (PDSA) rapid cycle improvement) Protocols for appropriate hand hygiene Guidelines for measurement and reporting of adherence to hand hygiene protocols Other Please specify
66. Does your hospital have a system (e.g., checklist, physician reminders, and automatic stop orders) in place to ensure proper
documentation of indication, catheter insertion, maintenance, and timely removal of urinary catheters? Yes, in all applicable locations Yes, but in Emergency Department only Yes, but for Inpatient Department only No Not applicable 67. Do you have a multidisciplinary team or steering committee focused on reaching VTE prophylaxis targets and reporting to key
medical staff committees in both medicine and surgery? Yes Yes, but only in surgery Not applicable Yes, but only in medicine No
68. Does your hospital have a hospital-wide written thromboprophylaxis policy? Yes, a fully-approved and implemented hospital-wide thromboprophylaxis policy Yes, but there is a considerable variability across units Yes, for specific patient groups, but not hospital wide No Not applicable

69. Which of the following do you have in your hospital to ensure placement of a mechanically ventilated patient’s head between
30-45 degrees (unless medically contraindicated)? (Check all that apply) A mechanism to ensure head-of-the-bed elevation A system for respiratory therapists to work collaboratively with nursing on positioning Education to caregivers and families about the importance of proper positioning and notify staff if supine positioning Visual cues to identify when the bed is in the proper position Include this intervention on order sets for initiation and weaning of mechanical ventilation, delivery of tube feedings, and
provision of oral care Not applicable Other Please specify
70. Is the process of medication administration and reconciliation tracked by management outside of pharmacy? Yes No 71. Do you use radio opaque sponges and have clear rules for when an x-ray is required before closing a surgical site? Yes No Yes, but compliance is not audited
72. Which of the following is true regarding practices in your hospital to ensure pressure ulcer assessment of all admitted patients?
(Check all that apply) A system (e.g., checklists) to ensure that pressure ulcer risk assessment is conducted within 4 hours of admission for all
patients Use of a visual cue on each admission documentation record to indicate completion of a total risk assessment and
reassessment A standard risk assessment tool (e.g., Braden scale) Methods to visually cue staff about at-risk patients (e.g., stickers on the patient chart or door) Sharing of pressure ulcer outcome measures with staff Not applicable

73. How often does the OB/GYN unit use a checklist (e.g., ACOG Patient Safety Checklist) to identify items/tasks that should be confirmed before or during the scheduling and performance of a procedure (e.g., elective induction and labor augmentation) AND to facilitate documentation of what was accomplished or utilized during a procedure?
Always Most of the time Sometimes Rarely Never Not applicable 74. Your hospital has a protocol governing the timing and conditions for elective delivery, adherence is monitored regularly, and
compliance is part of re-granting privileges for physicians. Yes Yes, but adherence is monitored infrequently Yes, but compliance is not part of re-granting privileges for physicians No Not applicable 75. Does your hospital allow scheduling an elective delivery or c-section prior to 39 weeks? No No, and we check gestational age Yes Not applicable 76. Does your hospital have an active program to track and reduce elective deliveries prior to 39 weeks? Yes No Not applicable 77. Which of the following is available in your hospital to ensure a uniform team management of shoulder dystocia? (Check all that
apply) Drills Continuing medical education Interactive online courses and protocols that clarify the duties of each team member A system (e.g., checklist) to ensure appropriate documentation of the maneuvers utilized and avoided in the management of
shoulder dystocia

Not applicable Other Please specify
78. Are patients who have fallen in your facility offered facilitated environmental home assessments upon discharge? Yes Yes, but only to older patients No 79. Is there an automatic alarm reset when a critical alarm is turned off or silenced (e.g., telemetry)? Yes No Not applicable 80. Which of the following is true regarding the process and effect of credentialing, privileging, and peer review in your hospital?
(Check all that apply) Risk management is included in the peer review process of unexpected outcomes and issues relating to deviations from
accepted standards of care and other risk exposures There is a process in place to support an adequate and objective medical staff and a nursing peer review process that
demonstrates effectiveness for improvement Peer review has resulted in changes in protocol, purchasing, or practices 81. What does your hospital do to prevent recurrence of serious safety events? (Check all that apply) Active involvement by the CEO in serious safety event prevention and apprised of effectiveness for prevention Active involvement by senior leadership in serious safety event prevention and apprised of effectiveness for prevention A measurement process that ensures RCA/FMEA actions are effective in preventing a repeat occurrence A system to track implementation and effectiveness of programs to reduce serious safety events Patient safety culture matrix A user-friendly and “safe” reporting tool for front-line staff Other Please specify
82. Which of the following is true regarding your hospital’s patient safety practices to reduce OB adverse events? (Check all that
apply) Perinatal bundles are used for induction and vacuum extraction VBAC requirements that the entire team be in house during labor to perform immediate C/S if needed

A structured process to manage shoulder dystocia should it occur Staff are certified in the ability to interpret EFM strips and the team is using the NICHD nomenclature and identification of the
three-tier approach to FHT monitoring Regular simulation drills with the entire team regarding the high-risk areas in OB (shoulder dystocia, timeliness of emergent
C/S, post partum hemorrhage, etc.) Staff training in advanced fetus monitoring Not applicable Other Please specify
8. RISK MANAGEMENT
83. Which of the following is true regarding perioperative safety risk in your hospital? (Check all that apply) There is a surgical/procedural verification protocol for patient identification, marking the site, and time out There is a count verification (i) before the procedure to establish a baseline, (ii) before the closure of a cavity within a cavity,
(iii) before wound closure begins, at skin closure, at the time of permanent relief of either the scrub person or circulating nurse and wand technology
There is a regular auditing for compliance of existing protocol to prevent retained foreign objects There have been no wrong site surgeries or RFBs in last 3 years There is a fire prevention program for the surgical suite, including specific time out for laser use on ENT cases Not applicable 84. Are closing items in risk trend tied to leaders’ performance evaluations? Yes No 85. Is there a patient safety incident dashboard for communicating risk management and “lessons learned” information to senior
management, the Board of Directors, and hospital staff? Yes No Yes, but only to senior management and Board of
Directors

86. In your hospital’s staff performance reviews, are staff asked about awareness of hospital quality improvement and patient safety initiatives?
Yes No 87. How often are risk managers included during re-designing or addition of a new service (e.g., ED re-design), prior to the initiation of
any physical plant work, or implementation of new service to proactively assess patient safety? Always About half the time Never Frequently Seldom
88. Are the Board and governing body actively involved in risk management and patient safety decision making? Yes No 89. Does the Board of your hospital actively participate in risk management, quality management, and patient safety? Yes, directly and routinely Yes, but through a Board risk management subcommittee No
9. NURSING PRACTICE
90. Do nursing shifts overlap at least 30 minutes to allow adequate time for patient handoff? Yes No 91. Which of the following is true regarding patient handoffs in your hospital? (Check all that apply) They are done in front of the patient They are done face-to-face between staff They are done electronically 92. How often are nurses shadowed by an infection preventionist to ensure compliance with infection prevention protocols? Weekly Quarterly Never
Monthly Annually
93. Does your hospital provide nurses with specialized training on the appropriate placement and management of urinary catheters
and keep records on those who have and have not received training?

Yes No Not applicable 94. Are reports about the necessity of urinary catheters reviewed daily by nursing staff and trended data reviewed by hospital
management? Yes No Not applicable 95. Do nursing protocols allow for removal of urinary catheters without physician order if criteria for necessity are not met? Yes No Not applicable 96. Does the hospital have a nurse-driven protocol for removing unnecessary urinary catheters? Yes No Not applicable 97. Does the hospital have guidelines for nurse-directed use of intermittent catheterization and use of bladder ultrasound scanners? Yes No Not applicable 98. Are nurses authorized to enforce use of a central line checklist to be sure all processes related to central line placement, including
hand hygiene, are executed for each line placement? Yes No Not applicable 99. How often would physicians be stopped if they failed to comply with any portion of the central line checklist? Always About half the time Never Frequently Seldom Not applicable 100. Does your hospital have a process for evaluating staff competence in recognizing the signs and symptoms of sepsis and an
evolving stroke? Yes Yes, but only for an evolving
stroke
Not applicable
Yes, but only for sepsis No
101. Do staff regularly perform comfort rounds to assess and address patient needs for pain relief, toileting, and positioning? Yes, hourly Yes, every 2 hours Yes, during shift changes Only when patients call for assistance

10. COMMUNICATION
102. Did your hospital have an event requiring a root cause analysis in the last 2 years where the root cause was determined to be lack
of proper and timely communication between staff? No serious event in the last 2 years Yes, but not sure how many Yes, we know how many cases we had Please specify the number of serious events
103. If you asked five front-line providers, how many do you think would respond “I always use the repeat back technique with
patients.” 0 1 2 3 4 5 104. How strongly do you agree or disagree with the following statement: “Staff follow a standardized and effective method of sharing
information when handing off patients." Strongly Agree Neither Strongly Disagree Agree Disagree
105. Which of the following does your hospital do to ensure smooth and safe patient transition upon admission, during shift and unit
changes, and/or at discharge? (Check all that apply) Provide patients information about their medical conditions and treatment care plan in a way that is understandable to them Inform patients and family members of the next steps in their care Inform patients who the responsible provider of care is during each shift and whom to contact if they have a concern about
the safety or quality of care Create opportunities for patients and family members to address any medical care questions or concerns with their health
care providers Involve patients and family members in decisions about their care at the level of involvement that they choose Use a standard handoff communication system, such as SBAR, and a verification process to ensure that information is both
received and understood Effective communication of patient care to the next provider Other

Please specify
106. Which of the following is true regarding your hospital's handoff protocol during surgery? (Check all that apply) Limited interruptions during handoff Up-to-date information is communicated regarding patient identification, patients condition, care, treatment, medications,
services and any recent or anticipated changes A method to verify the received information, including repeat-back or read-back techniques, is used There is an opportunity for the receiver of the handoff information to review relevant patient historical data, which may
include previous care, treatment or services A system (e.g., an electronic medical record) to streamline the exchange of timely and accurate information is used Not applicable 107. Upon admission, do the physician, nurse, and pharmacist assess the patient together as a team and work collaboratively to
develop a specific care plan for each patient? Yes No 108. Is there an electronic medical record for each patient that allows staff to track the progress of a patient's care and share health
information among providers from different service areas within the hospitals? Yes No 109. Prior to discharging a patient at high risk of readmission, is a face-to-face follow-up visit scheduled within 48 hours of discharge? Yes No 110. Prior to discharging a patient at moderate risk of readmission, is a follow-up phone call scheduled within 48 hours of discharge? Yes No 111. How would your staff rate the support your hospital provides to a family/caretaker of a patient in crisis? Excellent Good Fair Poor 112. Which of the following is true regarding your hospital? (Check all that apply) There is at least one patient and family advisory council (PFAC) Patients and their family members serve on key service-based and hospital-wide committees

The minutes of PFAC meetings and their accomplishments are provided to the hospital’s governing body and its Board of Trustees
Patient and family care experiences are incorporated into the hospital’s planning and day-to-day operation 113. Are front-line workers trained in communication techniques to promote assertiveness? Yes No 114. Are patient rounds undertaken by interdisciplinary teams (e.g., physicians, nurses, pharmacist, patient advocates) to promote
cross-communication under all settings? Yes No 115. Are failures to meet antibiotic timing, selection, or discontinuation communicated to the staff physician? Yes, within 24 hours of occurrence Yes, but not within 24 hours No, they are not communicated 116. If you asked five front-line staff on a unit about current blood stream infection rates, how many would know? 0 2 4 Not applicable 1 3 5
117. Does your hospital provide information about the risk of VTE and its prevention to patients? Yes, 80% or more of all patients Yes, at least 50% of patients Yes, at key patient encounter sites (e.g., admitting department, hospital lobbies, nursing units) Not at all Not applicable 118. Are visual indicators used to quickly communicate with the care team about patients at risk of fall or injury (e.g., use of colorful
socks, colored wristbands and/or blankets, or signage outside and inside the room to indicate fall and/or injury risk)? Yes No 119. Are patients and family members educated about risk of injury from a fall on admission and during hospital stay, and about what
they can do to help prevent a fall using one of the following proven patient educational methods? (Check all that apply) Teach back

Return demonstration or show back “Ask Me 3” (Encourage patients to ask their providers three questions: What is my main problem? What do I need to do (for
that problem)? Why is that important?) Signed contract of expected behavior for families There is no formal process for communicating with patients/their families Other Please specify Information is provided in hospital admission packet and nurse reinforces that information 120. Which of the following is true about communication of critical values in your hospital? (Check all that apply) There are protocols in place to alert physicians of critical values (e.g., laboratory, radiology) There is evidence of documentation of who was notified, by whom, time, response, and actions taken Loop is closed on labs ordered before discharge but results are not available until after discharge
11. INFECTION CONTROL
121. Does your hospital use CDC national healthcare safety network (NHSN) definitions for central line-associated blood stream
infection in all locations and for all types of central venous catheters (PICC)? Yes No Not applicable 122. What is your hospital doing to ensure compliance with patient care practices to reduce the incidence of VAP? (Check all that
apply) Institute written policies, protocols, or pathways that describe the recommended practices for prevention of VAP Routinely collect data on process measures (e.g., hand hygiene compliance, sedation interruption, oral care, maintenance of
30-45 degrees positioning, and assessment of readiness to wean) related to VAP Assess if results based on collected process measures demonstrate compliance to recommended practices Report results from collected measures and assessment to senior leadership, nursing leadership, and care providers Enforce QI initiatives targeted at addressing identified areas of improvement Not applicable Other Please specify

123. Does your hospital have a PICC team for PICC line placement and maintenance? Yes No Yes, outside contractual services Not applicable 124. Are PICC line dressings routinely changed by a PICC team member? Yes No Not applicable 125. How often does your ICU/Clinical Care Area currently use a positive displacement needle-less connector valve for central venous
catheters? Always About half the time Never Frequently Seldom Not applicable 126. How often does your ICU/Clinical Care Area currently bathe patients in this clinical care area with chlorhexidine?
Always About half the time Never Frequently Seldom Not applicable 127. Do you routinely use ultrasound to place central venous catheters? (Check all that apply) Yes, for subclavian lines No Yes, for internal jugular lines Not applicable 128. How often do you document the removal of urinary catheters post-operatively within 24-48 hours unless there are appropriate
indications for continued use? Always About half the time Never Frequently Seldom Not applicable 129. Is the use of proper aseptic technique and sterile equipment for urinary catheter insertion audited? Yes, in all applicable units and frequently Yes, in all applicable units but not frequently Never Not applicable 130. How often is systemic anti-microbial prophylaxis used for urinary catheters? Always About half the time Never

Frequently Seldom Not applicable 131. Does the hospital require a documented rationale for Foley catheter in all settings? Yes No Not applicable 132. How often does your hospital conduct checklist-driven monitoring of guidelines for appropriate perioperative catheter management
(e.g., procedure-specific guidelines for catheter placement and postoperative catheter removal and management of postoperative urinary retention)?
Always About half the time Never Frequently Seldom Not applicable 133. Who inserts urinary catheters at your facility? (Check all that apply) RNs LPNs Nurse aides Physicians Medical Students Not applicable Other Please specify Patient Care Technicians 134. Are urinary catheter days tracked? (Check all that apply) Yes, electronically No Yes, manually Not applicable 135. Does your hospital have a comprehensive program to reduce CAUTI, including reducing catheter days, bladder bundle tracking,
sterile technique placement, and reason for catheter at time of placement that is reviewed by senior leadership? Yes No Yes, but it is not comprehensive or linked to
senior leadership
Not applicable
136. Do standard supply kits exist that include catheter and all necessary items? (Check all that apply) Yes, for indwelling (Foley) catheters No

Yes, for central line catheters Not applicable 137. Does your hospital utilize a surgical safety checklist (e.g., the World Health Organization Surgical Safety Checklist or an
adaptation) prior to surgical procedures to verify (at a minimum) patient identity, allergies, and preoperative antibiotics (when required)?
Yes, fully implemented throughout hospital Yes, fully implemented in some areas Yes, partially implemented in some or all areas No, no plan to use surgical safety checklist No, but is planning to use one Please specify year and month you plan to start using surgical safety checklist
138. What does your hospital have in place to ensure proper endoscope processing/disinfecting? (Check all that apply) A quality system program that covers all aspects of endoscopy procedure management A written procedure for monitoring adherence to the program and a chain of accountability A system to ensure that staff responsible for endoscope processing understand proper use and maintain proficiency in
performing it A routine monitoring to ensure compliance with recommended practices
Thank you for taking your time to complete this assessment tool!