Embed Size (px)
Citation preview

RESEARCH AND EDUCATION
aClinical AssibProfessor EmcClinical ProfdProfessor, D
904
The accuracy of virtual interocclusal registration duringintraoral scanning
Faraj Edher, DDS, MSc, Dip. Pros, FRCD(C),a Alan G. Hannam, BDS, PhD, FDSRCS,b
David L. Tobias, BSc, DMD, MSc,c and Chris C. L. Wyatt, DMD, MSc, Dip. Pros, FRCD(C)d
ABSTRACTStatement of problem. Evidence on the accuracy and reproducibility of the virtual interocclusalregistration procedure and recommendations as to how to make a virtual interocclusal record arelacking.
Purpose. The purpose of this in vitro study was to assess whether virtual interocclusal registrationrecords made at different locations around the arch affect the alignment of virtual casts, and toassess whether quadrant and complete arch scans have different effects on cast alignment whenthey are articulated with virtual interocclusal records.
Material and methods. Three sites of close proximity (SCPs) and 3 sites of clearance (SCs) wereidentified in each sextant of mounted zirconia master models. The SCPs and SCs were confirmed byusing shimstock foil and the transillumination of an interocclusal impression. Complete-arch andquadrant scans of the master models were made with an intraoral scanner and registered withdifferent virtual interocclusal registration records. The SCPs and SCs indicated by the scanner’ssoftware and by independent software were compared according to the sensitivity, specificity,and predictive values of each method.
Results. Changed locations of SCPs were found depending on the location of the virtualinterocclusal registration record. The intraoral scanner’s software contacts had a higher sensitivity of92.86% and a negative predictive value of 84.21% than the contacts revealed by the independentsoftware that exhibited a sensitivity of 69.05% and a negative predictive value of 70.45%. However,the intraoral scanner software had a lower specificity of 41.03% and a positive predictive value of62.90% compared with the independent software, which exhibited a specificity of 79.49% and apositive predictive value of 78.38%. The quadrant scans had a higher sensitivity than did thecomplete-arch scans.
Conclusions. Different occlusal contacts are obtained from interocclusal registration scans indifferent segments of the dental arch. The difference is more obvious in complete-arch scans, wherea tilting effect toward the site of the interocclusal registration scan was observed. Occlusal contactsobtained from interocclusal registration scans for quadrant scans had a higher sensitivity than didthose for complete-arch scans. (J Prosthet Dent 2018;120:904-12)
Recording, storing, and trans-ferring occlusal information in apredictable way is importantin the analysis and restorationof dentitions.1,2 Despite theabsence of a universallyaccepted standard for identi-fying occlusal contacts and theinaccuracies inherent in most ofthe materials used to indicatethem, patient feedback andocclusal examination remain themost prevalent clinical ap-proaches to identifying them.Consequently, the selection anduse of any contact indicator re-quires caution, interpretation,and clinical judgement.3,4
The transillumination of asilicone interocclusal recordcan be used to quantifyocclusal contacts, becauselight transmission varies withmaterial thickness. Owenset al5 considered any materialthicknesses at or below 50 mmas dental contacts and thick-nesses greater than 50 mm but
less than 350 mm as near contacts. Silicone interocclusalrecords have been shown to be more reliable forrevealing occlusal contacts than other occlusalstant Professor, Department of Oral Health Sciences, Faculty of Dentistry,eritus, Faculty of Dentistry, University of British Columbia, Vancouver, Ca
essor, Department of Oral Health Sciences, Faculty of Dentistry, Universityepartment of Oral Health Sciences, Faculty of Dentistry, University of Briti
indicators6-10; therefore, the transillumination approachoffers a standard against which other methods can betested.11
University of British Columbia, Vancouver, Canada.nada.of British Columbia, Vancouver, Canada.
sh Columbia, Vancouver, Canada.
THE JOURNAL OF PROSTHETIC DENTISTRY

Clinical ImplicationsQuadrant scans are indicated for single-unitrestorations because they provide the mostaccurate occlusal representation. Multiple virtualinterocclusal registration records appear necessaryfor articulating complete arches to reduce the tiltingeffect of a single localized interocclusal registrationrecord. If the scanning software prevents the use ofmultiple records, single records should be made asclose as possible to areas of interest (such as a toothpreparation or implant). If complete-arch scans areused without a site of interest for diagnostic orrecord purposes, virtual interocclusal records shouldpreferably be made in the anterior region becausethis results in more accurate reproduction of mostocclusal contacts.
December 2018 905
Intraoral scanning systems and their associated soft-ware are now widely used in clinical practice. Virtualdental arches can be acquired by scanning dental im-pressions and physical casts, or by directly scanning thearches intraorally. In the virtual environment, meshregistration commonly involves the initial alignment of atleast 4 designated landmarks followed by a least-squarescomputational fit of the 2 meshes, and is usuallyaccompanied by expression of the iterative closest pointsbetween them. Details of how most commercial intraoralscanning software platforms actually register theopposing dentition are difficult to find. Virtual castsaligned with virtual interocclusal records should permitthe accurate identification and quantification of any re-gions of contact between the meshes representing thevirtual arches.
Although intraoral virtual records are frequently usedto fabricate single and multiunit restorations thatconform with the patient’s existing occlusal scheme, ev-idence regarding the accuracy or reproducibility of thisprocess is sparse. Solaberrieta et al12 attempted to vali-date this virtual procedure by comparing the predictedvirtual occlusal contact points with the contacts obtainedby occlusion recording paper on mounted casts. Theyfound that virtual registration is a valid procedure forlocating the mandibular cast and that contacts observedin the virtual environment are significantly more accuratethan those of the physical ones. However, the study usedan industrial 3-dimensional scanner to digitize the castsand to obtain the virtual interocclusal records, so theresults do not necessarily equate with those obtainable byintraoral scanning.
Stavness et al13 used an intraoral scanner to digitizemaxillary and mandibular casts and an industrial
Edher et al
3-dimensional scanner to obtain the virtual interocclusalrecords. They found that digital simulation with virtualinterocclusal records can closely replicate the occlusalcontacts and primary movements of mounted casts on asemi-adjustable articulator. Solaberrieta et al,14,15 by us-ing an industrial 3-dimensional scanner and intraoralscanners, have shown that intraoral virtual occlusalrecording is a valid procedure for locating a mandibularcast on a virtual articulator. They concluded that the bestcombination for obtaining virtual occlusal records were 2lateral and frontal sections, or both left- and right-sideocclusal records. The best results were found when thedistance between the registration sections was maxi-mized. Iwaki et al16 assessed the dimensional accuracy ofoptical interocclusal registration by using an intraoralscanner and compared this with a conventional physicalmethod in vitro. They found that optical interocclusalregistration was more effective in single posterior resto-rations compared with the conventional method,although for multiple preparations, the optical methodshowed significantly more discrepancies. The accuracy ofan intraoral scanner in reproducing the occlusal contactsof a cast was assessed by Arslan et al.17 The highestpercentages of virtual occlusal contacts identical to thoseof the physical casts were found in the nonpreparedcomplete-arch digital scans. They recommended makinga complete-arch digital scan when there is no posteriorantagonist contact after tooth preparation.
The current study was carried out because informa-tion is lacking on the efficacy of the current intraoralscanning and interocclusal registration used for articu-lating virtual dental casts, in particular, the reliability ofthe approach for predicting occlusal contacts. The pur-pose of this study was to assess whether virtual inter-occlusal records made at different locations on the archaffect the alignment of virtual casts and whether quad-rant scans and complete-arch scans affect the alignmentof virtual casts when articulated by using virtual inter-occlusal records. The null hypotheses of the study werethat the use of virtual interocclusal records made atdifferent locations on the arch do not affect the alignment(assessed by the presence or absence of occlusal contacts)of virtual casts and that the use of virtual interocclusalrecords results in no difference between the alignment(assessed by the presence or absence of occlusal contacts)of complete-arch scans and quadrant scans.
MATERIAL AND METHODS
Maxillary and mandibular zirconia were hand-articulatedand mounted in maximum intercuspal position (MIP) ona semi-adjustable articulator (Denar Mark 330; Whip MixCorp). Occlusal adjustments were made to achievebilaterally distributed sites of close proximity (SCPs) inMIP on a minimum of 3 teeth in each sextant. SCPs and
THE JOURNAL OF PROSTHETIC DENTISTRY
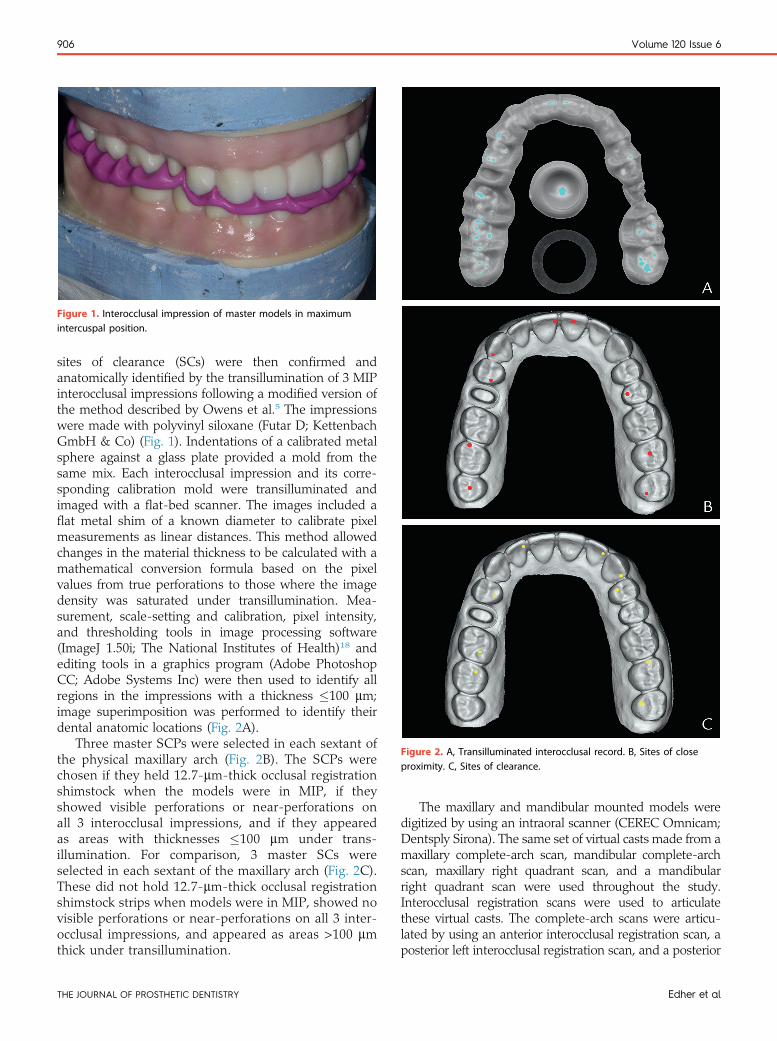
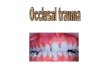
Figure 1. Interocclusal impression of master models in maximumintercuspal position.
Figure 2. A, Transilluminated interocclusal record. B, Sites of closeproximity. C, Sites of clearance.
906 Volume 120 Issue 6
sites of clearance (SCs) were then confirmed andanatomically identified by the transillumination of 3 MIPinterocclusal impressions following a modified version ofthe method described by Owens et al.5 The impressionswere made with polyvinyl siloxane (Futar D; KettenbachGmbH & Co) (Fig. 1). Indentations of a calibrated metalsphere against a glass plate provided a mold from thesame mix. Each interocclusal impression and its corre-sponding calibration mold were transilluminated andimaged with a flat-bed scanner. The images included aflat metal shim of a known diameter to calibrate pixelmeasurements as linear distances. This method allowedchanges in the material thickness to be calculated with amathematical conversion formula based on the pixelvalues from true perforations to those where the imagedensity was saturated under transillumination. Mea-surement, scale-setting and calibration, pixel intensity,and thresholding tools in image processing software(ImageJ 1.50i; The National Institutes of Health)18 andediting tools in a graphics program (Adobe PhotoshopCC; Adobe Systems Inc) were then used to identify allregions in the impressions with a thickness �100 mm;image superimposition was performed to identify theirdental anatomic locations (Fig. 2A).
Three master SCPs were selected in each sextant ofthe physical maxillary arch (Fig. 2B). The SCPs werechosen if they held 12.7-mm-thick occlusal registrationshimstock when the models were in MIP, if theyshowed visible perforations or near-perforations onall 3 interocclusal impressions, and if they appearedas areas with thicknesses �100 mm under trans-illumination. For comparison, 3 master SCs wereselected in each sextant of the maxillary arch (Fig. 2C).These did not hold 12.7-mm-thick occlusal registrationshimstock strips when models were in MIP, showed novisible perforations or near-perforations on all 3 inter-occlusal impressions, and appeared as areas >100 mmthick under transillumination.
THE JOURNAL OF PROSTHETIC DENTISTRY
The maxillary and mandibular mounted models weredigitized by using an intraoral scanner (CEREC Omnicam;Dentsply Sirona). The same set of virtual casts made from amaxillary complete-arch scan, mandibular complete-archscan, maxillary right quadrant scan, and a mandibularright quadrant scan were used throughout the study.Interocclusal registration scans were used to articulatethese virtual casts. The complete-arch scans were articu-lated by using an anterior interocclusal registration scan, aposterior left interocclusal registration scan, and a posterior
Edher et al

Figure 3. Screenshots of intraoral scanner outputs.
December 2018 907
right interocclusal registration scan. The right quadrantscans were virtually articulated by using a canine inter-occlusal scan, a molar interocclusal scan, and a quadrantinterocclusal scan. Every interocclusal registration scan wasrepeated once under the same conditions. This produced atotal of 6 complete-arch articulated virtual casts and 6quadrant articulated virtual casts.
The Omnicam software provided images of the castswith color-coded markings identifying SCPs �100 mmand apparent perforations. These are shown in Figure 3,where according to the manufacturer, red represents 100mm of contact or greater, yellow represents 50 to 100 mmof contact, green represents 0 to 50 mm of contact, darkblue represents 0 to 50 mm of occlusal clearance, royalblue represents 50 to 100 mm of occlusal clearance, andlight blue represents 100 mm of clearance.
The articulated virtual casts were then exported instandard tessellation language (STL) file format anduploaded to 3D point cloud and triangular mesh editingand processing software (CloudCompare v2.7; http://www.cloudcompare.org). This software platformallowed the identification and measurement of actualmesh separations and perforations between the virtualcasts. By setting thresholds for the program’s distancemap settings, all distances �100 mm and perforationscould be identified. These are shown in Figure 4, wheregreen represents areas with 0 to 100 mm of occlusalclearance and blue represents areas of mesh perforation.
The Master SCPs and SCs were then compared withthe color-coded virtual casts produced by the intraoral
Edher et al
scanner and the color-coded virtual casts produced bythe independent software. The sites were classified asnegative clearance (clearance >100 mm), positiveclearance (clearance �100 mm), and positive perfora-tion (perforations of the virtual casts). True positive,true negative, false positive, and false negative calcu-lations were also identified for each cast. The sensi-tivity, specificity, positive predictive value (PPV), andnegative predictive value (NPV) were then determined,similar to the approach used by Delong et al19 andSolaberrieta et al.14,15
RESULTS
The results of the SCP analysis are visually displayed inFigure 5, which illustrates changes in the location of thepositive clearances and positive perforations according totheir locations on the virtual interocclusal record. Thecombined data for SCPs (including both positiveclearances �100 mm and positive perforations) and SCsare displayed in Figure 6. The true positive, true negative,false positive, and false negative contacts calculated foreach virtually articulated cast, and the sensitivity, speci-ficity, PPVs, and NPVs are summarized in Tables 1 and 2.
The CEREC software contacts showed higher sensi-tivity and NPV (92.86% and 84.21%, respectively)compared with the contacts found with CloudComparesoftware (69.05% and 70.45%, respectively). However,the CEREC software had lower specificity and PPV(41.03% and 62.90%, respectively) compared with
THE JOURNAL OF PROSTHETIC DENTISTRY

Figure 4. Screenshots of CloudCompare software outputs.
908 Volume 120 Issue 6
CloudCompare (79.49% and 78.38%, respectively). TheQuadrant scans revealed a higher sensitivity comparedwith the complete-arch scans.
DISCUSSION
Few studies have specifically addressed virtual inter-occlusal records, and to date, coordinate measuring ma-chine scanners have mostly been used for this pur-pose.12,13,15 The few studies that have assessedinterocclusal records made with intraoral scanners sug-gest that this procedure can be accurate if used inparticular situations.14,16,17
SCPs were defined and determined where materialthickness was �100 mm and confirmed on 3 differenttransilluminated interocclusal records. In addition,occlusal adjustment, visual inspection for perforations ornear perforations, and physical confirmation with shimstock foil were done as additional validation, providing ahigh level of confidence in the selection of 3 SCPs in eachsextant, and to overcome the present lack of a universalgold standard for identifying and quantifying trueocclusal contacts.20
Arch scanning and stitching of the scanned segmentscan introduce errors affecting the results of studies suchas ours,21 and other data (Straga RW, unpublished data,2009) have shown that fewer digital captures can result in
THE JOURNAL OF PROSTHETIC DENTISTRY
increased occlusal contact accuracy. To reduce the influ-ence of stitching errors and to maintain those present asconstants, we used the same single maxillary andmandibular complete-arch scan and single maxillary andmandibular right quadrant scan for all 12 virtually artic-ulated casts. Thus, the only variable factor among themwas the interocclusal registration scan.
Interocclusal perforations are phenomena that cannotexist in natural dentitions or conventional casts. Theyexist between virtual casts and can theoretically introduceocclusal errors. In this study, more contacts and perfo-rations were seen in the region closest to the virtualinterocclusal record, and more contacts were missed inthe sections farthest from it. Because virtual casts areoriented 3-dimensionally, the above observation can bethought of as a tilting of the virtual casts, in one or moreplanes, toward the region where the virtual interocclusalrecord was made. The effect was clearly visible in thecomplete-arch scans but minimized in the quadrantscans. This can be attributed to the fact that teeth in thequadrant scans were all closer to where the virtualinterocclusal record was made. These findings suggestthat multiple virtual interocclusal records may be neededto articulate complete-arch scans. This has already beensuggested by others, who have advocated taking multiplebuccal scans as far apart as possible.16,17 In situations inwhich the software does not allow multiple interocclusal
Edher et al

ThirdMolarComplete Arch Scans
Quadrant Scans
AIO1AIO1
AIO2AIO2
LIO1LIO1
LIO2LIO2
RIO1RIO1
CIO1CIO1
MIO1MIO1
QIO1QIO1
QIO2QIO2
Legend AIOLIORIOCIOMIOQIO
≤100μm
>100μm
Positive ClearancePositive Perforation
NegativeOmnicam Output
CloudCompare Output
MIO2MIO2
CIO2CIO2
RIO2RIO2
SecondMolar
FirstPremolar
CanineCentralIncisor
CentralIncisor
SecondPremolar
SecondMolar
ThirdMolar
Master Sites of Close Proximity
Anterior Interocclusal ScanLeft Interocclusal Scan
Right Interocclusal ScanRight Canine Interocclusal ScanRight Molar Interocclusal Scan
Full Right Quadrant Interocclusal Scan
Figure 5. Sites of close proximity analysis.
ThirdMolar
1 1 1 1 1 1 1 0 0 0 0 0 0 0 1 0 0 01 1 1 1 1 1 1 1 1 1 1 1 0 0 1 1 0 0
1 1 1 1 1 1 0 0 0 0 0 0 0 0 0 0 0 01 1 1 1 1 1 1 1 1 1 1 1 0 0 1 1 0 0
0 0 0 0 1 1 1 1 0 0 0 0 0 0 0 1 1 00 1 0 1 1 1 1 1 1 0 0 0 0 0 1 1 1 1
0 0 0 1 1 1 1 1 0 0 0 0 0 0 0 1 1 11 1 0 1 1 1 1 1 1 0 0 0 0 0 1 1 1 1
1 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 01 1 1 1 1 1 1 1 0 1 1 1 0 0 1 1 0 0
1 1 1 1 1 1 1 0 0 0 0 0 0 0 1 0 0 01 1 1 1 1
0 1 1 1 11 1 1 1 1
0 1 1 1 11 1 1 1 1
1 1 1 1 11 1 1 1 1
1 1 1 1 11 1 1 1 1
1 1 1 1 01 1 1 1 1
1 1 1 1 01 1 1 1 1
1 1 0 0 1 1 1 0
0 0 0 01 1 1 0
0 0 0 01 1 1 0
0 0 0 01 1 1 0
1 0 0 01 1 1 0
1 0 0 01 1 1 0
1 0 0 01 1 1 0
0 1 1 0 0
CompleteArch Scans
AIO1AIO1
AIO2AIO2
LIO1LIO1
LIO2LIO2
RIO1RIO1
RIO2RIO2
SecondMolar
FirstPremolar
CanineCentralIncisor
CentralIncisor
SecondPremolar
SecondMolar
ThirdMolar
SecondMolar
FirstMolar
FirstPremolar
LateralLateralIncisor
CanineFirst
PremolarSecondMolar
ThirdMolar
Master Sites of Close Proximity Master Sites of Clearance
Quadrant Scans
CIO1CIO1
CIO2CIO2
MIO1MIO1
MIO2MIO2
QIO1QIO1
QIO2QIO2
Legend AIOLIORIOCIOMIOQIO
≤100μm
>100μm
Positive ClearancePositive Perforation
NegativeOmnicam Output
CloudCompare Output
Anterior Interocclusal ScanLeft Interocclusal Scan
Right Interocclusal ScanRight Canine Interocclusal ScanRight Molar Interocclusal Scan
Full Right Quadrant Interocclusal Scan
Figure 6. Sites of close proximity and sites of clearance analysis.
December 2018 909
Edher et al THE JOURNAL OF PROSTHETIC DENTISTRY

Table 1. CEREC software output analysis
CEREC Software Output
True Positive False Positive False Negative True Negative Sensitivity Specificity PPV NPV
AIO1 9 5 0 4 100.00 44.44 64.29 100.00
AIO2 9 5 0 4 100.00 44.44 64.29 100.00
LIO1 7 4 2 5 77.78 55.56 63.64 71.43
LIO2 8 4 1 5 88.89 55.56 66.67 83.33
RIO1 8 5 1 4 88.89 44.44 61.54 80.00
RIO2 7 5 2 4 77.78 44.44 58.33 66.67
Complete arch total 48 28 6 26 88.89 48.15 63.16 81.25
CIO1 5 3 0 1 100.00 25.00 62.50 100.00
CIO2 5 3 0 1 100.00 25.00 62.50 100.00
MIO1 5 3 0 1 100.00 25.00 62.50 100.00
MIO2 5 3 0 1 100.00 25.00 62.50 100.00
QIO1 5 2 0 2 100.00 50.00 71.43 100.00
QIO2 5 3 0 1 100.00 25.00 62.50 100.00
Quadrant total 30 18 0 6 100.00 25.00 62.50 100.00
Total 78 46 6 32 92.86 41.03 62.90 84.21
NPV, negative predictive value; PPV, positive predictive value.
Table 2. CloudCompare software output analysis
CloudCompare Software Output
True Positive False Positive False Negative True Negative Sensitivity Specificity PPV NPV
AIO1 7 1 2 8 77.78 88.89 87.50 80.00
AIO2 6 0 3 9 66.67 100.00 100.00 75.00
LIO1 4 2 5 7 44.44 77.78 66.67 58.33
LIO2 5 3 4 6 55.56 66.67 62.50 60.00
RIO1 3 0 6 9 33.33 100.00 100.00 60.00
RIO2 7 1 2 8 77.78 88.89 87.50 80.00
Complete arch total 32 8 22 46 59.26 85.19 80.00 67.65
CIO1 4 0 1 4 80.00 100.00 100.00 80.00
CIO2 4 0 1 4 80.00 100.00 100.00 80.00
MIO1 5 0 0 4 100.00 100.00 100.00 100.00
MIO2 5 1 0 3 100.00 75.00 83.33 100.00
QIO1 4 1 1 3 80.00 75.00 80.00 75.00
QIO2 4 2 1 2 80.00 50.00 66.67 66.67
Quadrant total 26 8 4 16 86.67 66.67 76.47 80.00
Total 58 16 26 62 69.05 79.49 78.38 70.45
NPV, negative predictive value; PPV, positive predictive value.
910 Volume 120 Issue 6
records, we suggest the interocclusal record be made asclose as possible to the area of interest. If complete-archscans are made for diagnostic or record purposes andthere is no specific area of interest, virtual interocclusalrecords made in the anterior region appear to producemore accurate reproductions of the occlusal contacts thanleft- or right-side scans. Patients with increased verticaloverlap are an exception to this, as registration of therelationship between the anterior teeth is often notpossible.
The clinical consequence of any interocclusal perfo-rations on definitive restorations should always beconsidered. A restoration designed and fabricated withperforated virtual casts will theoretically always be inlight, or likely out of, occlusal contact once in a patient’smouth. Although restorations in light or out of occlusion
THE JOURNAL OF PROSTHETIC DENTISTRY
reduce the need for adjustments, it is less than ideal if thegoal is to stabilize the occlusion. The potential for theintermesh penetration problem inherent in virtual castarticulation can, however, be addressed by collision res-olution in software algorithms, as demonstrated byStavness et al.13
The contacts displayed by using the CEREC softwareshowed higher sensitivity and NPV compared with thecontacts displayed with the CloudCompare software; thatis, the intraoral scanner software identified more of themaster SCPs. The regions it displayed greater than 100 mmapart were also more likely to be true negatives (SCs). Theapparent high sensitivity of the intraoral scanner softwareis encouraging, as it will likely lead to restorations requiringless occlusal adjustment. However, the intraoral scannersoftware had a lower specificity and PPV compared with
Edher et al

December 2018 911
CloudCompare. A possible explanation for these findingscould be that the intraoral scanner software’s distancethresholds for color-coding are actually larger thandescribed, leading to more areas being categorized ascontacts or near contacts. If this were true, it would havethe advantage of producing restorations that require lessocclusal adjustment but would increase the likelihood ofrestorations being out of occlusion.
Solaberrieta et al14 have shown that knowing the ac-curacy of best-fit operational algorithms used in softwareplatforms is useful because it accounts for any cumulativeerror produced. CloudCompare was used because itsmethod for measuring intermesh distances is known (theplatform uses available mesh-vertices as points and thenmeasures the distance between the point-cloud and theclosest opposing mesh-face), whereas the intraoral scan-ner’s algorithm for virtual registration was unknown to us.Therefore, some of the differences observed in the studymay be due to different algorithms used by the intraoralscanner and CloudCompare.
The quadrant scans showed higher sensitivity whencompared with complete-arch scans. This means thatcontacts (SCPs) are more likely to be identified inquadrant scans, which can be attributed to a reducedtilting effect. This differs from the findings of Arslanet al,17 who reported that half-arch digital scans showedsignificantly lower percentages of identical contacts whencompared with complete-arch digital scans. This may bebecause, in their study, 2 posterior fixed dental prosthesisabutments were prepared, which significantly reducedthe occlusal contacts observed on a quadrant scan. Iwakiet al16 also found that for multiple preparations, thevirtual interocclusal records showed significantly largerdiscrepancies. In their study, there was only 1 tooth-bound prepared abutment in the quadrant scans.Quadrant scans also showed higher NPV compared withcomplete-arch scans, which means that areas displayedas more than 100 mm apart are more likely to truly beSCs. Surprisingly, complete-arch scans displayed higherspecificity than quadrant scans, implying that complete-arch scans were better at identifying SCs.
The present study was conducted in vitro by using 1set of articulated zirconia ceramic casts, which does notsimulate the biological environment of the oral cavity northe physiological intrusion of natural teeth with anocclusal force. The use of the intraoral scanner extraorallycould also be considered a limitation because scanningoutside the mouth has been shown to produce virtualcasts with higher resolutions and accuracies than thoseobtained by intraoral scanning. Finally, although theanalytic approach used is a common way to estimatepredictive accuracy for clinical relevance, the small sam-ple size (that is, the number of different scans) could beconsidered a limitation because small differences can
Edher et al
amplify into significant changes when the numeric re-sults are analyzed.
CONCLUSIONS
Based on the findings of this in vitro study, the followingconclusions were drawn:
1. A difference was found in the occlusal contactsobtained from interocclusal scans made in differentsegments of the opposing dental arches. The dif-ference was most obvious in complete-arch scans, inwhich there was a tilting effect toward the site of theinterocclusal scan. Based on these results, multiplevirtual interocclusal records used to articulate com-plete arch scans may reduce the “tilting effect”produced by taking a single virtual interocclusalrecord. In cases in which the software does notpermit multiple virtual interocclusal records forregistration, the single virtual interocclusal recordshould be made as close as possible to the area ofinterest (tooth preparation or implant).
2. Single anterior interocclusal scans showed moreaccurately distributed occlusal contacts in compari-son to single right or left interocclusal scans.Therefore, if complete arch scans are made fordiagnostic or record purposes without a specifiedsite of interest, virtual interocclusal records made inthe anterior region (canine to canine) would pro-duce more accurate reproduction of the overallocclusal contacts.
3. Occlusal contacts obtained from interocclusal scansfor virtual quadrants showed a higher sensitivitythan those obtained from scans for complete virtualarches. Based on these results, quadrant scans usedin single-unit cases can reproduce the most accurateocclusal representation.
REFERENCES
1. Davies S, Al-Ani Z, Jeremiah H, Winston D, Smith P. Reliability of recordingstatic and dynamic occlusal contact marks using transparent acetate sheet.J Prosthet Dent 2005;94:458-61.
2. DeLong R, Knorr S, Anderson GC, Hodges J, Pintado MR. Accuracy ofcontacts calculated from 3D images of occlusal surfaces. J Dent 2007;35:528-34.
3. Forrester SE, Presswood RG, Toy AC, Pain MT. Occlusal measurementmethod can affect SEMG activity during occlusion. J Oral Rehabil 2011;38:655-60.
4. Millstein P, Maya A. An evaluation of occlusal contact marking in-dicators. A descriptive quantitative method. J Am Dent Assoc 2001;132:1280-6; quiz 319.
5. Owens S, Buschang PH, Throckmorton GS, Palmer L, English J. Masticatoryperformance and areas of occlusal contact and near contact in subjects withnormal occlusion and malocclusion. Am J Orthod Dentofacial Orthop2002;121:602-9.
6. Yamashita S, Igarashi Y, Ai M. Tooth contacts at the mandibular retrudedposition, comparison of two different methods for bite registration. J OralRehabil 2002;29:823-6.
7. Gazit E, Lieberman MA. Occlusal contacts following orthodontic treat-ment. Measured by a photocclusion technique. Angle Orthod 1985;55:316-20.
THE JOURNAL OF PROSTHETIC DENTISTRY

912 Volume 120 Issue 6
8. Durbin DS, Sadowsky C. Changes in tooth contacts following orthodontictreatment. Am J Orthod Dentofacial Orthop 1986;90:375-82.
9. Razdolsky Y, Sadowsky C, BeGole EA. Occlusal contacts following ortho-dontic treatment: a follow-up study. Angle Orthod 1989;59:181-5.
10. Sakaguchi RL, Anderson GC, DeLong R. Digital imaging of occlusal contactsin the intercuspal position. J Prosthodont 1994;3:193-7.
11. Baba K, Tsukiyama Y, Clark GT. Reliability, validity, and utility of variousocclusal measurement methods and techniques. J Prosthet Dent 2000;83:83-9.
12. Solaberrieta E, Otegi JR, Goicoechea N, Brizuela A, Pradies G. Com-parison of a conventional and virtual occlusal record. J Prosthet Dent2015;114:92-7.
13. Stavness IK, Hannam AG, Tobias DL, Zhang X. Simulation of dental colli-sions and occlusal dynamics in the virtual environment. J Oral Rehabil2016;43:269-78.
14. Solaberrieta E, Garmendia A, Brizuela A, Otegi JR, Pradies G, Szentpetery A.Intraoral Digital impressions for virtual occlusal records: section quantity anddimensions. Biomed Res Int 2016;2016:7173824.
15. Solaberrieta E, Arias A, Brizuela A, Garikano X, Pradies G. Determining therequirements, section quantity, and dimension of the virtual occlusal record.J Prosthet Dent 2016;115:52-6.
16. Iwaki Y, Wakabayashi N, Igarashi Y. Dimensional accuracy of optical biteregistration in single and multiple unit restorations. Oper Dent 2013;38:309-15.
17. Arslan Y, Bankoglu Gungor M, Karakoca Nemli S, Kokdogan Boyaci B,Aydin C. Comparison of maximum intercuspal contacts of articulated castsand virtual casts requiring posterior fixed partial dentures. J Prosthodont2017;26:594-8.
Noteworthy Abstracts of
Passivity of fit of a novel prefabricated implareconstruction: a comparative in vitro study
Karl M, Carretta R, Higuchi KWInt J Prosthodont 2018;31:440-2
Purpose. To quantify the strain development of a new prefareconstruction.
Material and methods. Five resin models reflecting edentuaminal implants and prefabricated frameworks with a novelcomputer-aided design/computer-assisted manufacturing (Cduring superstructure fixation. Statistical analyses (analysis ofdistribution of misfit.
Results. Cast restorations showed significantly higher levelsof misfit compared to prefabricated and CAD/CAM restoratiCAD/CAM frameworks showed a similar low level and distr
Conclusions. The compensation mechanism of the prefabriCAD/CAM superstructures.
Reprinted with permission of Quintessence Publishing.
THE JOURNAL OF PROSTHETIC DENTISTRY
18. Schneider CA, Rasband WS, Eliceiri KW. NIH Image to ImageJ: 25 years ofimage analysis. Nat Methods 2012;9:671-5.
19. DeLong R, HeinzenM, Hodges JS, Ko CC, DouglasWH. Accuracy of a system forcreating 3D computer models of dental arches. J Dent Res 2003;82:438-42.
20. Delong R, Ko CC, Anderson GC, Hodges JS, Douglas WH. Comparingmaximum intercuspal contacts of virtual dental patients and mounted dentalcasts. J Prosthet Dent 2002;88:622-30.
21. Patzelt SB, Emmanouilidi A, Stampf S, Strub JR, Att W. Accuracy of full-archscans using intraoral scanners. Clin Oral Investig 2014;18:1687-94.
Corresponding author:Dr Faraj EdherFaculty of DentistryUniversity of British Columbia2199 Wesbrook MallVancouver, BC V6T 1Z3CANADAEmail: [email protected]
AcknowledgmentsThe authors thank Aurum Ceramic Dental Laboratories Canada for fabricatingand mounting the casts and assisting in the conversion of the digital files. Also, athank-you to Patterson Dental for providing access to the CEREC Omnicamintraoral scanner.
Copyright © 2018 by the Editorial Council for The Journal of Prosthetic Dentistry.https://doi.org/10.1016/j.prosdent.2018.01.024
the Current Literature
nt-supported mandibular full-arch
bricated implant-supported mandibular full-arch
lous mandibles were each restored with three interfor-compensation mechanism, cast frameworks, andAD/CAM)-fabricated frameworks. Strains were recordedvariance, t tests; a=.05) were based on level of misfit and
of misfit and a significantly more uneven distributionons (P<.05 for all comparisons). Prefabricated andibution of misfit (P=.24145 and P=.2837, respectively).
cated frameworks provides a level of fit comparable to
Edher et al