Embed Size (px)
Citation preview

Acta Anaesthesiol Scand 2002; 46: 160–165 Copyright C Acta Anaesthesiol Scand 2002Printed in Denmark. All rights reserved
ACTA ANAESTHESIOLOGICA SCANDINAVICA
0001-5172
Sympathetic nervous activation following subarachnoidhemorrhage: Influence of intravenous clonidine
G. LAMBERT1, S. NAREDI2,4, E. EDEN2, B. RYDENHAG3 and P. FRIBERG1
1Department of Clinical Physiology, Sahlgrenska University Hospital, 2Department of Anesthesia and Intensive Care, Institute of Surgical Sciences and3Department of Neurosurgery, Institute of Neurosciences, Sahlgrenska University Hospital, Göteborg; 4Department of Anesthesia and Intensive Care,Institute of Surgical and Perioperative Sciences, Umeå University Hospital, Umeå, Sweden
Background: Subarachnoid hemorrhage is often accompaniedby systemic complications and cerebral vasospasm. Elevatedlevels of circulating catecholamines may be involved in thepathophysiology behind these events. The alpha-2-agonistclonidine inhibits sympathetic outflow by a central mechan-ism. Unrestricted sympathoexcitation may be detrimental andadministration of clonidine may be beneficial in these patients.Methods: Using isotope dilution methodology, norepinephrinekinetic determinations, comprising determination of arterialnorepinephrine concentration and rates of norepinephrinespillover to and removal, or clearance, from plasma, were per-formed on three occasions during the first week after sub-arachnoid hemorrhage in 25 patients. Eleven of these patientsreceived clonidine (continuous i.v. infusion 5.8∫0.7mg¡kgª1¡24hª1) and the remainder, standard therapy. Initialresults were compared with 17 healthy age-matched subjectsand eight patients suffering from severe traumatic brain injurywithout traumatic subarachnoid hemorrhage.Results: Subarachnoid hemorrhage patients exhibited mark-edly elevated arterial plasma norepinephrine concentrations[3.74∫0.48, P,0.001 vs. healthy subjects (1.59∫0.11nmol/L)and P,0.05 vs. head trauma patients (1.94∫0.29nmol/L)].The rate of clearance of norepinephrine from plasma in thesubarachnoid patients was also significantly greater than that
SUBARACHNOID hemorrhage is characterized by ahigh level of morbidity and mortality, largely as a
consequence of rebleeding, but also due to the devel-opment of cerebral vasospasm and systemic compli-cations, such as: electrocardiographic abnormalitiesand elevated plasma troponin levels consistent withthe development of left ventricular dysfunction andmyocardial ischaemia and pulmonary edema (1–4).Elevated levels of circulating catecholamines (5, 6)arising due to an elevation in the rate of spillover ofnorepinephrine to plasma may be involved in thepathogenesis behind these events (7). Moreover, in-creased levels of circulating catecholamines coupledwith an abnormal sensitivity of the cerebral vascula-
160
observed in the healthy subjects (2.66∫0.15 vs. 2.14∫0.15L/min, P,0.05) and the head trauma patients (2.00∫0.12L/min,P,0.05). Compared with both control groups, on admissionthe rate of spillover of norepinephrine to plasma followingsubarachnoid hemorrhage was markedly elevated (9.11∫1.12,P,0.001). Clonidine treatment (continuous i.v. infusion 5.8∫0.7mg¡kgª1¡24hª1) did not reduce the increased rate ofspillover of norepinephrine to plasma following subarachnoidhemorrhage.Conclusion: Sympathetic nervous activity is markedly elev-ated following subarachnoid bleeding. Clonidine had no effecton the rate of norepinephrine spillover to, or clearance from,plasma in these patients. Clearly, further studies are requiredto elucidate the mechanisms responsible for generating sym-pathetic nervous activation following subarachnoid hemor-rhage.
Received 9 March, accepted for publication 27 August 2001
Key words: a-adrenoreceptors; human; norepinephrine;spillover
c Acta Anaesthesiologica Scandinavica 46 (2002)
ture to norepinephrine (8) may partly generate cer-ebral vasospasm.
We wondered whether administration of the sym-pathoinhibitory alpha-2-agonist, clonidine, could beof benefit following subarachnoid hemorrhage.Using isotope dilution methodology to examine therate of spillover of norepinephrine to plasma, wetested the impact of intravenous administration ofclonidine on the degree of sympathetic nervous acti-vation in patients with subarachnoid bleeding.Given that the plasma concentration of norepineph-rine is the net result of the bidirectional flux of theneurotransmitter into and out of plasma, the kineticdetermination of norepinephrine spillover and clear-

Sympathoexcitation and subarachnoid bleeding
ance provides a well-documented, robust and moreuseful index of sympathetic function than doesmeasurement of arterial norepinephrine alone (9).
Methods
SubjectsResults obtained from 25 patients following non-trau-matic subarachnoid hemorrhage (14 females and 11males, aged 51 ∫ 1 years), 17 healthy control subjects(8 females and 9 males, aged 53 ∫ 2 years) and 8 pa-tients suffering from severe traumatic brain injurywithout traumatic subarachnoid hemorrhage (3 fe-males and 5 males, aged 33 ∫ 12 years) form the basisof this report. All patients were admitted and treatedat the Neurointensive Care Unit of the SahlgrenskaUniversity Hospital within 24 h after the onset of sub-arachnoid hemorrhage or head trauma. Diagnosis wasmade by computerized tomography scan. Estimationof the amount of blood in the subarachnoid space wasdetermined according to the criteria proposed byFisher (10). The median Hunt & Hess classification(11) of the subarachnoid patients was 3 (range 1–5).None of these patients had a history of myocardialdisease. The healthy subjects were recruited by localadvertisement and underwent a comprehensivephysical examination to screen for possible con-founding medical illness prior to their inclusion in theexperimental procedure. The local ethical and isotopecommittees at the Sahlgrenska University Hospitalapproved all study protocols. All subjects or their nextof kin gave their written informed consent to partici-pate in the study.
MonitoringAll patients had central venous and arterial lines forcontinuous monitoring of central venous and sys-temic arterial blood pressures, respectively. Oxygensaturation was determined by pulsoximetry (DatexCardiocap 2). In 14 of the subarachnoid hemorrhagepatients the development of hydrocephalus necessi-tated the insertion of an intraventricular catheter (Stil-le EDN v-kat 20 cm, set: Monitor ICP). This catheterwas used for monitoring intracranial pressure and fordrainage of cerebrospinal fluid. The limit for drainageof cerebral spinal fluid was normally set at 20 cmH2Oabove forehead level. Zero pressure baseline for intra-cranial pressure was set at forehead level and zeropressure baseline for systemic pressure at heart level(pressure monitor: Datex Cardiocap 2). The drainagesystem was closed every hour to measure the actualintracranial pressure and to calculate the cerebral per-fusion pressure.
161
TreatmentIn 22 of the patients, bleeding was associated with thepresence of an aneurysm. In three patients, the causeof the bleeding remained unknown; neither an aneu-rysm nor an arterio-venous malformation could befound on repeated angiograms. The treatment of theaneurysms was either by surgical clipping or by em-bolization with platina coils. All patients underwentprophylactic treatment with the calcium-blockingagent nimodepine in order to limit cerebral vaso-spasm.
Experimental protocol and blood samplingIn order to assess sympathetic nervous function, nor-epinephrine kinetic determinations were made by iso-tope dilution during a steady state infusion of a tracerdose of norepinephrine as previously described (12).At steady-state, the total body norepinephrinespillover to plasma and the total body clearance rateof norepinephrine from plasma were determined ac-cording to the following formulas:
Total Spillover Rate Ω [3H] Norepinephrine InfusionRate (dpm/min)/Plasma Norepinephrine SpecificRadioactivity (dpm/pmol)
and
Total Body Clearance Ω [3H] Norepinephrine InfusionRate (dpm/min)/Arterial [3H] Norepinephrine con-centration (dpm/ml)
This procedure allowed measurement of norepineph-rine clearance from plasma and calculation of totalbody norepinephrine spillover. Assessment of both ofthese parameters enables a more accurate assessmentof sympathetic nervous function than does measure-ment of plasma norepinephrine levels alone, giventhat the arterial plasma concentration of norepineph-rine is the net result of the bidirectional flux of theneurotransmitter.
Initial norepinephrine kinetic measurements weremade within 48 h after subarachnoid hemorrhage, andfollow-up studies were performed 24 h subsequent toand on day 7–10 post-trauma. In 11 patients, followingthe initial measurements, made within 48 h of sub-arachnoid bleeding, a continuous intravenous infusionof the alpha2 adrenergic agonist clonidine (5.8 ∫ 0.7mg¡kgª1¡24 hª1) was commenced (Table 1). Clonidinetreatment remained in place for the duration of the ex-perimental period (8 ∫ 1 day). In order to maintain cer-ebral perfusion and not to predispose patients to cer-ebral ischaemia, the drug was titrated in order not toreduce mean blood and cerebral perfusion pressuresbelow 75 and 70 mmHg, respectively. The dose of cloni-

G. Lambert et al.
dine used was based on our previous experience intreating head injury patients according to the ‘Lundconcept’ (13). Retrospective examination of records ob-tained from 34 consecutive head injury patients admit-ted to Sahlgrenska University Hospital between 1993and 1994 indicated that a clonidine dose of 5.3 ∫ 0.3mg¡kgª1¡24 h– (maximun dose 8 mg¡kgª1¡24 hª1) wasassociated with good survival (14). In the healthy sub-jects, resting determinations were made in the morningafter an overnight fast and in the head trauma patients,determinations were made on a single occasion within48 h of admission to hospital.
On each experimental occasion blood samples wereobtained from indwelling arterial catheters and im-mediately placed in chilled tubes containing an anti-coagulant/antioxidant mixture. At the completion ofthe study and within 30 min of sampling, the bloodsamples were centrifuged (approximately 1000 g for30 min at 4 æC) and the plasma stored at ª80 æC untilassayed. Within 1 month of obtaining blood samples,norepinephrine was extracted from 1 ml of plasmaand samples of radiotracer infusate (10 ml) using alu-mina adsorption, separated and quantified by highperformance liquid chromatography with coulometricdetection (15). Timed collection of tritiated eluateleaving the electrochemical cell permitted separationof the tritium-labeled norepinephrine for subsequentcounting by liquid scintillation spectroscopy.
StatisticsAll results, unless otherwise specified, are expressedas mean ∫ standard error of the mean and tests of sig-nificance were carried out using distribution-free non-parametric tests. Evaluation of the effect of clonidinewas evaluated using Wilcoxon’s signed rank test forpaired samples. Values less than 0.05 were consideredto be statistically significant.
Table1
Clonidine dosage.
Patient Mean clonidine dose Clonidine doseID (mg¡kgª1¡24hª1) (mg/24h)
14 4.8 28815 5.3 29216 3.4 23817 4.3 30118 3.5 28019 5.8 70820 3.0 18024 10.4 72826 4.1 35728 8.6 68830 5.5 440Mean∫SEM 5.8∫0.7 409∫61
162
Results
On admission to the neurointensive care unit and ir-respective of whether they were sedated or not, thesubarachnoid hemorrhage patients exhibited mark-edly elevated arterial plasma norepinephrine concen-trations, being more than two times that seen inhealthy subjects (3.74 ∫ 0.48 vs. 1.59 ∫ 0.11 nmol/L, P, 0.001) and 48% greater than in patients followinghead trauma (1.94 ∫ 0.29 nmol/L, P ,0.05). The rateof clearance of norepinephrine from plasma in thesubarachnoid patients was significantly greater thanthat observed in the healthy control subjects (2.66 ∫0.15 vs. 2.14 ∫ 0.15 L/min, P , 0.05) and the headtrauma patients (2.00 ∫ 0.12 L/min, P , 0.05). The pro-nounced elevation in arterial norepinephrine, coupledwith the increase in norepinephrine plasma clearance,translated into an approximately 3-fold increase in therate of spillover of norepinephrine to plasma in pa-tients following-non-traumatic subarachnoid hemor-rhage compared with that of the two control groups(Fig. 1).
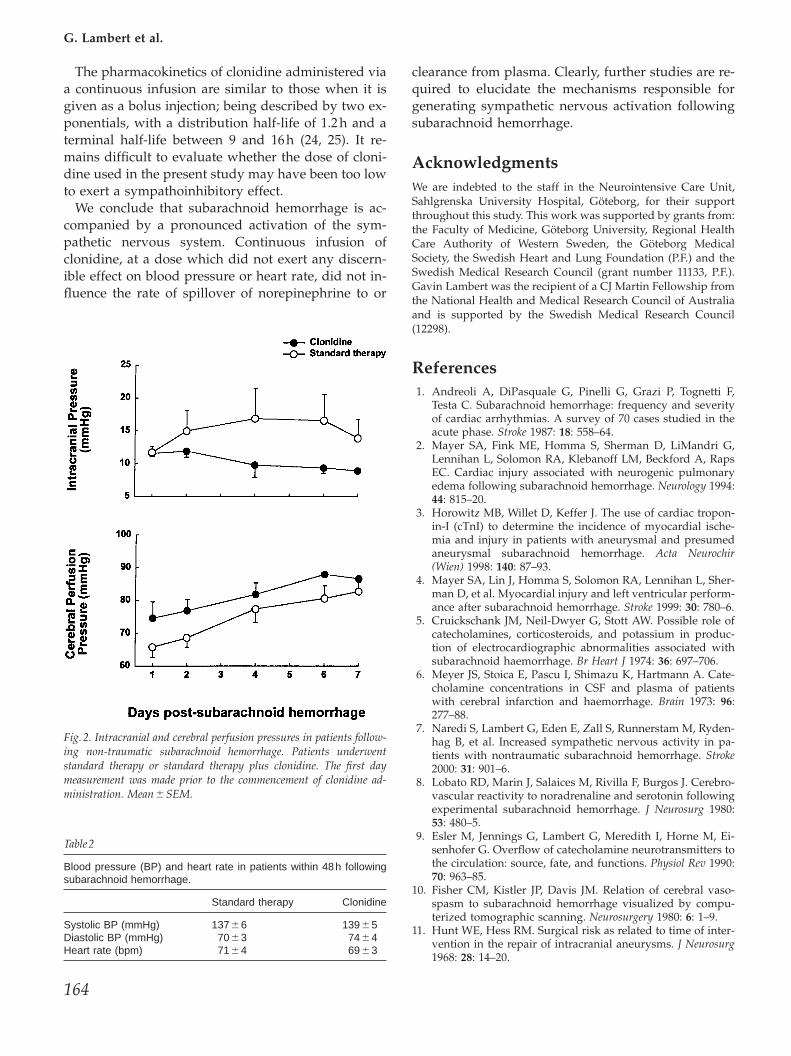
Following baseline measurements the patient groupwas divided, group 1 (n Ω 14) continued to receivestandard therapy and group 2 (n Ω 11) received stan-dard therapy plus intravenous clonidine. Within 48 hof subarachnoid hemorrhage there was no differencebetween the rate of spillover of norepinephrine toplasma in the two groups of patients (Fig. 1). Plasmanorepinephrine concentrations were not significantlydifferent (3.74 ∫ 0.76 nmol/L pre-clonidine v 2.84 ∫0.44 nmol/L post-clonidine) Baseline blood pressureand heart rates were similar in the two groups (Table2). Administration of the alpha-2-adrenergic agonistclonidine did not reduce total body norepinephrinespillover and was without effect on the plasma clear-ance of norepinephrine (Fig. 1). Clonidine did not in-fluence blood pressure, heart rate or cerebral per-fusion pressure throughout the experimental period(Fig. 2). Intracranial pressure tended to remain lowerin those patients treated with clonidine (Fig. 2).
Discussion
In agreement with our previous clinical (7) and ex-perimental studies (16), a marked activation of thesympathetic nervous system occurs following sub-arachnoid hemorrhage. Intravenous infusion of the al-pha-2-adrenergic agonist clonidine at a dose of ap-proximately 6 mg¡kgª1¡24 hª1 did not reduce the rateof total body spillover of norepinephrine in this study.
The lack of effect of clonidine in reducing sym-pathetic nervous activity was surprising. Clonidine is

Sympathoexcitation and subarachnoid bleeding
Fig.1. Rates of spillover of norepinephrine to, and clearance from, plasma in patients following non-traumatic subarachnoid hemorrhage and therate of spillover of norepinephrine to plasma in patients suffering from severe traumatic brain injury without traumatic subarachnoid hemorrhageand in healthy subjects. Subarachnoid hemorrhage patients underwent standard therapy or standard therapy plus clonidine (continuous iv infusion5.8∫0.7mg¡kgª1¡24hª1). The first day measurement was made prior to the commencement of clonidine administration. Mean∫SEM.
a centrally acting suppressant of sympathetic nervoussystem activity known to inhibit the firing rate of lo-cus coeruleus neurons (17) and to reduce multiunitpostganglionic sympathetic activity in the muscle-supplying fascicles of the peroneal nerve (18), brainnorepinephrine turnover and whole body nor-epinephrine spillover to plasma (19). In patients fol-lowing head injury, clonidine has been demonstratedto reduce plasma catecholamine levels (20). The so-called ‘Lund therapy’ (21) utilizes clonidine to reducecapillary hydrostatic pressure and, presumably, the‘stress-response’. While the tendency for intracranialpressure to remain lower in those treated with cloni-dine is encouraging, and perhaps relates to the drug’sability to diminish capillary hydrostatic pressure,clearly, as our results indicate, when it comes to thesympathetic nervous system, comparisons between
163
patients with subarachnoid hemorrhage and thosewith head injury per se are perhaps unwise.
The lack of effect of intravenous clonidine in thisstudy could be due to the route of administration, thedose or the patient group studied. When administeredintravenously at a dose of 0, 2, 4, or 6 mg/kg over a15-min period 30 min prior to induction of anesthesiaprior to heart surgery, clonidine therapy was associ-ated with a reduction in plasma catecholamine levelsand a small reduction or even unchanged arterialblood pressure (22). While the sedative effects ofclonidine seem to be related to the plasma concen-trations of the drug, blood pressure seems to be in-fluenced in a more complex manner. At lower drugconcentrations there exists a positive relation betweendose and blood pressure but at higher doses this cor-relation becomes negative (23).
G. Lambert et al.
The pharmacokinetics of clonidine administered viaa continuous infusion are similar to those when it isgiven as a bolus injection; being described by two ex-ponentials, with a distribution half-life of 1.2 h and aterminal half-life between 9 and 16 h (24, 25). It re-mains difficult to evaluate whether the dose of cloni-dine used in the present study may have been too lowto exert a sympathoinhibitory effect.
We conclude that subarachnoid hemorrhage is ac-companied by a pronounced activation of the sym-pathetic nervous system. Continuous infusion ofclonidine, at a dose which did not exert any discern-ible effect on blood pressure or heart rate, did not in-fluence the rate of spillover of norepinephrine to or
Fig.2. Intracranial and cerebral perfusion pressures in patients follow-ing non-traumatic subarachnoid hemorrhage. Patients underwentstandard therapy or standard therapy plus clonidine. The first daymeasurement was made prior to the commencement of clonidine ad-ministration. Mean∫SEM.
Table2
Blood pressure (BP) and heart rate in patients within 48h followingsubarachnoid hemorrhage.
Standard therapy Clonidine
Systolic BP (mmHg) 137∫6 139∫5Diastolic BP (mmHg) 70∫3 74∫4Heart rate (bpm) 71∫4 69∫3
164
clearance from plasma. Clearly, further studies are re-quired to elucidate the mechanisms responsible forgenerating sympathetic nervous activation followingsubarachnoid hemorrhage.
AcknowledgmentsWe are indebted to the staff in the Neurointensive Care Unit,Sahlgrenska University Hospital, Göteborg, for their supportthroughout this study. This work was supported by grants from:the Faculty of Medicine, Göteborg University, Regional HealthCare Authority of Western Sweden, the Göteborg MedicalSociety, the Swedish Heart and Lung Foundation (P.F.) and theSwedish Medical Research Council (grant number 11133, P.F.).Gavin Lambert was the recipient of a CJ Martin Fellowship fromthe National Health and Medical Research Council of Australiaand is supported by the Swedish Medical Research Council(12298).
References1. Andreoli A, DiPasquale G, Pinelli G, Grazi P, Tognetti F,
Testa C. Subarachnoid hemorrhage: frequency and severityof cardiac arrhythmias. A survey of 70 cases studied in theacute phase. Stroke 1987: 18: 558–64.
2. Mayer SA, Fink ME, Homma S, Sherman D, LiMandri G,Lennihan L, Solomon RA, Klebanoff LM, Beckford A, RapsEC. Cardiac injury associated with neurogenic pulmonaryedema following subarachnoid hemorrhage. Neurology 1994:44: 815–20.
3. Horowitz MB, Willet D, Keffer J. The use of cardiac tropon-in-I (cTnI) to determine the incidence of myocardial ische-mia and injury in patients with aneurysmal and presumedaneurysmal subarachnoid hemorrhage. Acta Neurochir(Wien) 1998: 140: 87–93.
4. Mayer SA, Lin J, Homma S, Solomon RA, Lennihan L, Sher-man D, et al. Myocardial injury and left ventricular perform-ance after subarachnoid hemorrhage. Stroke 1999: 30: 780–6.
5. Cruickschank JM, Neil-Dwyer G, Stott AW. Possible role ofcatecholamines, corticosteroids, and potassium in produc-tion of electrocardiographic abnormalities associated withsubarachnoid haemorrhage. Br Heart J 1974: 36: 697–706.
6. Meyer JS, Stoica E, Pascu I, Shimazu K, Hartmann A. Cate-cholamine concentrations in CSF and plasma of patientswith cerebral infarction and haemorrhage. Brain 1973: 96:277–88.
7. Naredi S, Lambert G, Eden E, Zall S, Runnerstam M, Ryden-hag B, et al. Increased sympathetic nervous activity in pa-tients with nontraumatic subarachnoid hemorrhage. Stroke2000: 31: 901–6.
8. Lobato RD, Marin J, Salaices M, Rivilla F, Burgos J. Cerebro-vascular reactivity to noradrenaline and serotonin followingexperimental subarachnoid hemorrhage. J Neurosurg 1980:53: 480–5.
9. Esler M, Jennings G, Lambert G, Meredith I, Horne M, Ei-senhofer G. Overflow of catecholamine neurotransmitters tothe circulation: source, fate, and functions. Physiol Rev 1990:70: 963–85.
10. Fisher CM, Kistler JP, Davis JM. Relation of cerebral vaso-spasm to subarachnoid hemorrhage visualized by compu-terized tomographic scanning. Neurosurgery 1980: 6: 1–9.
11. Hunt WE, Hess RM. Surgical risk as related to time of inter-vention in the repair of intracranial aneurysms. J Neurosurg1968: 28: 14–20.

Sympathoexcitation and subarachnoid bleeding
12. Esler M, Jackman G, Bobik A, Kelleher D, Jennings G, Leon-ard P, Skews H, Korner P. Determination of norepinephrineapparent release rate and clearance in humans. Life Sci 1979:25: 1461–70.
13. Asgeirsson B, Grande PO, Nordstrom CH. A new therapyof post-trauma brain oedema based on haemodynamic prin-ciples for brain volume regulation. Intensive Care Med 1994:20: 260–7.
14. Naredi S, Eden E, Zall S, Stephensen H, Rydenhag B. A stan-dardized neurosurgical neurointensive therapy directed to-ward vasogenic edema after severe traumatic brain injury:clinical results. Intensive Care Med 1998: 24: 446–51.
15. Medvedev OS, Esler MD, Angus JA, Cox HS, Eisenhofer G.Simultaneous determination of plasma noradrenaline andadrenaline kinetics, responses to nitroprusside-induced hy-potension and 2-deoxyglucose-induced glucopenia in therabbit. Naunyn Schmiedebergs Arch Pharmacol 1990: 341: 192–9.
16. Lambert E, Lambert G, Fassot C, Friberg P, Elghozi J-L. Sub-arachnoid haemorrhage induced sympathoexcitation arisesdue to a change in endothelin and/or nitric oxide activity.Cardiovascular Res 2000: 45: 1046–53.
17. Foote SL, Bloom FE, Aston-Jones G. Nucleus locus ceruleus.new evidence of anatomical and physiological specificity.Physiol Rev 1983: 63: 844–914.
18. Kirnö K, Lundin S, Elam M. Epidural clonidine depressessympathetic nerve activity in humans by a supraspinalmechanism. Anesthesiology 1993: 78: 1021–7.
19. Lambert GW, Kaye DM, Thompson JM, Turner AG, Cox HS,Vaz M, et al. Internal jugular venous spillover of noradren-aline and metabolites and their association with sympatheticnervous activity. Acta Physiol Scand 1998: 163: 155–63.
165
20. Payen D, Quintin L, Plaisance P, Chiron B, Lhoste F. Headinjury: clonidine decreases plasma catecholamines. Crit CareMed 1990: 18: 392–5.
21. Asgeirsson B, Grande PO, Nordstrom CH, Berntman L, Mes-seter K, Ryding E. Effects of hypotensive treatment with al-pha 2-agonist and beta 1-antagonist on cerebral haemodyn-amics in severely head injured patients. Acta AnaesthesiolScand 1995: 39: 347–51.
22. Kulka PJ, Tryba M, Zenz M. Dose–response effects of intra-venous clonidine on stress response during induction ofanesthesia in coronary artery bypass graft patients. AnesthAnalg 1995: 80: 263–8.
23. Reid JL, Panfilov V, MacPhee G, Elliott HL. Clinical pharma-cology of drugs acting on imidazoline and adrenergic recep-tors. Studies with clonidine, moxonidine, rilmenidine, andatenolol. Ann N Y Acad Sci 1995: 763: 673–8.
24. Reid JL. The clinical pharmacology of clonidine and relatedcentral antihypertensive agents. Br J Clin Pharmacol 1981: 12:295–302.
25. Fauler J, Verner L. The pharmacokinetics of clonidine in highdosage. Eur J Clin Pharmacol 1993: 45: 165–7.
Address:Dr Gavin LambertBaker Medical Research InstitutePO Box 6492St Kilda Road CentralMelbourne Vic 8008Australiae-mail: gavin.lambert/baker.edu.au