Embed Size (px)
Citation preview

Supra ten to ria I Recurrences in Me d ullo blas to ma
BERTA JEREB, MD, NARAYAN SUNDARESAN, MD, BRUCE HORTEN, MD, ANN REID, BSc, AND JOSEPH H. GALICICH, MD
Four children with medulloblastoma had massive supratentorial recurrences in the region of the cribriform plate after adequate craniospinal irradiation. The pathogenesis of these recurrences is probably related to underdosage to this region caused by shielding of the eyes. This hypothesis was corroborated by autopsy findings in two other patients in whom subfrontal implants were histologically different from recurrences elsewhere. Two possible solutions to avoid this problem in the future are suggested.
Cancer 47:806-809, 1981.
EDULLOBLASTOMAS REPRESENT approximately M 20% of childhood intracranial tumors and are the second most common posterior fossa tumors en- countered in The major improvement in cure rate of children with medulloblastoma occurred with the introduction of whole neuraxis irradiation. l9
Increasing the dose to the posterior fossa further im- proved the survival rate; however, there appears to be an optimum level above which results d e t e r i ~ r a t e . ~ Neither the use of more sophisticated techniques of radiation nor adjuvant chemotherapy has influenced the outcome of the disease significantly. More recent reports on improvement of survival rates may be related to diagnosis at an earlier stage of the disease, and more complete removal of the primary t ~ m o r . ~ * l ~ Two main causes of treatment failure are local recur- rences in the posterior fossa and diffuse meningeal seeding through the cerebrospinal fluid (CSF) path- ways.1.4*8,16,'7 In addition, extracranial metastases have also been reported, especially to the skeleton and occasionally to lung and other v i s ~ e r a . ~ + ~ ~ ~ Supra- tentorial recurrences that appear as mass lesions are uncommon. We wish to report on four cases in which massive recurrences occurred in the region of the cribriform plate after craniospinal radiation. We sug- gest a possible pathogenesis for their occurrence at this particular site.
From the Departments of Radiation Therapy, Neuropathology, the Neurosurgical Service, and the Medical Physics Department, Memorial Sloan-Kettering Cancer Center, New York, New York.
Address reprints: Berta Jereb, MD 1275 York Avenue. New York, NY 10021.
Accepted for publication March 12, 1980.
Case Reports
Case 1
In January 197 1, a six-year-old female underwent posterior fossa craniotomy with partial resection of a medulloblastoma. Her postoperative treatment consisted of craniospinal radia- tion (3500 rads to whole brain, 3500 rads to spinal cord, and an additional 1500 rads to the posterior fossa) over eight weeks, supplemented by six weekly courses of vin- cristine (0.5 mg/m'). The calculated dose to the cribriform plate area was approximately 350 rads. She was symptom- free until August 1972 when she experienced a generalized seizure. Examination revealed some swelling about the right orbit and exophthalmos. Tomography showed destruction of the medial orbital wall and the cribriform plate. Following confirmation of recurrent tumor by aspiration biopsy, she was treated with an additional 4000 rads to the area ofrecur- rence. Clinical evidence of tumor regression was noted. In November 1972, metastases to the lumbar spine, ilium, and femur were treated with local radiation. She died in July 1973 of progressive disease in the central nervous system. No autopsy was performed.
Case 2
In February 1971, a six-year-old boy underwent posterior fossa craniotomy and subtotal resection of a rnedulloblastoma. This was followed by craniospinal radiation (4000 rads to the entire neuraxis) in six weeks. The cribriform plate was estimated to have received a total dose of 400 rads. In March, 1975 he had tumor recurrence in the subfrontal region. He underwent subtotal resection of the tumor, followed by an additional 2000 rads to the frontal lobes. In addition, three courses of 1,3-bis(2-chloroethyl)- 1- nitrosourea (BCNU) (80 mg/kg) were given. In June 1976, he was reevaluated because of persistent seizures. Computed
0008-543X/8 1/02 15/0806 $0.70 0 American Cancer Society
806

No. 4 SUPRATENTORIAL RECURRENCE . Jereb et al. 807
tomography (CT scan) revealed a large right frontal lesion and hydrocephalus. Meningeal seeding was also documented by myelography. The patient received an additional 600 rads to the spinal cord, and chemotherapy consisting of high-dose methotrexate (400 mg/kg), vincristine (2 mg/m2), and BCNU (90 mg/m2). In January 1977, he underwent a right frontal craniotomy and total excision of a subfrontal recurrence that was attached to the cribriform plate. Fol- lowing temporary improvement, he died of progressive disease in June 1977.
Case 3
In August 1972, a five-year-old girl underwent posterior fossa craniotomy and gross total resection of a medul- loblastoma. This was followed by craniospinal radiation (3,500 rads to the whole brain, 4000 rads to the spinal cord, and an additional 1500 rads to the posterior fossa) over eight weeks. The dose to the cribriform plate was estimated to be 350 rads. She was symptom-free until July 1974 when she had a large subfrontal tumor. Following resection of the tumor, which was attached to the cribriform plate, an ad- ditional 2000 rads to the anterior cribriform plate were given following surgery. In September 1974, bony metastases developed in the lumbar spine, and cytologic analysis was positive. Accordingly, the patient received further local radiation therapy to the lumbosacral region and combination chemotherapy consisting of vincristine (1.5 mg/m2), 1-(2- chloroethyl)-3(4-methylcyclohexyl)-l-nitrosourea (Me- CCNU) (120 mg/m2), and high dose methotrexate (500 mg/kg) for a total of seven doses. In July 1975, she died of progressive central nervous system disease. No autopsy was performed.
Cuse 4
In April 1977, a five-year-old girl underwent posterior fossa craniotomy and biopsy of a medulloblastoma. This was followed by craniospinal radiation (3000 rads to the cranium and 2000 rads to the spine) in four weeks. The dose to the cribriform plate was estimated to be 900 rads. Sixteen months later, a large subfrontal recurrence of tumor developed. She underwent craniotomy and resection of a subfrontal medulloblastoma attached to the cribriform plate. She has done well following this resection and has no further signs of CNS relapse at six months follow-up.
Discussion
During the past two decades, several series of medulloblastomas have been reported showing five- year survival rates of 30-50%.3,13,14,18,23 BI oom has suggested that local recurrence in the posterior fossa is the main cause of death.3,4 McFarland noted that metastatic nodules caused by CSF seeding occurred mainly in the spinal canal, and he postulated that this was caused by the predominantly downward flow of
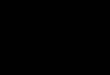
POSTERIOR
15 X 16
RT
'%o
SHIELD
FIG. 1. Composite dose distribution within the skull with posterior and two oblique portals. With insertion of the blocks for eye shielding. The dose in the frontal and ethmoidal area reduced to <30% of the tumor dose.
accounted for only 6% of recurrences in his compre- hensive review. Recently, however, it is becoming apparent that supratentorial recurrences may be more common than previously assumed. lo Periodic evalua- tion by computed tomography of patients who have been treated for medulloblastoma has shown sub- clinical recurrences along the walls of the ventricular system and in the subarachnoid cisterns.
Three problems are encountered in attempting to deliver a homogeneous radiation dose to the whole neuraxis. These are 1) attaining the long narrow fields required for the spine; 2) achieving an adequate dose distribution to the whole brain, particularly at the region of the cribriform plate; and 3) joining these two regions.
A variety of methods has been suggested to achieve a uniform dose to the head.6,13,23,25 These include lateral fields (with or without wedges), anterior and posterior fields, and the technique of using anterior oblique fields combined with a posterior field (used at this Institution). To avoid radiation damage to the eyes, some have chosen either a baseline for these fields so that the eyes lie below the field^,^ or they have shielded the eyes should they be included in the treatment ports. In either case, the dose distribution in the region of the cribriform plate is low.
Figure 1 shows the anterior oblique field technique in the region of the eye; the resulting dose to the
CSF from the cisterna magna.17 Supratentorial lesions cribriform plate is approximately 20%. If the head is

808 CANCER February 15 1981 Vol. 41
treated with lateral fields the estimated dose to this region will depend on where the baselines of the fields are drawn. If they are drawn above the eye level, the cribriform plate will receive a dose of less than 10% (Fig. 2). If they are drawn below the level of the eyes, and appropriate shielding is then employed, the dose in the cribriform plate will again be in the range of 10% (Fig. 3). We believe that this factor is responsible for the subfrontal recurrences noted in our patients.
Hardy has previously noted extradural recurrences in this region in three patients." Since his patients were operated on in the prone position. he suggested that the region of the cribriform plate represented the most dependent portion of the brain where tumor cells might be expected to pool. In addition, he considered radiation underdosage to be a contributing factor. Since
FIG. 2. Beam film of a lateral brain field with the inferior border above the eyes.
our patients were operated upon in the sitting position, the former explanation would not apply in our patients. The prone position is used during radiation treatment, and if tumor cells tend to pool along the dependent portions of the brain, they may seed by gravity to the region of the cribriform plate.
Our own experience at autopsy indicates that the majority of these deposits are found in the dependent portions of the subarachnoid space, inparticular the dorsal surface of the spinal cord and the ventral sur- faces of the cranial compartment. If undertreated, this site may represent a sanctuary for the tumor. Although this would not explain why medulloblastomas recur in the majority of cases, it is interesting to speculate that the subfrontal area may harbor a pool of tumor cells that are capable of seeding throughout the CSF pathways.
FIG. 3. Beam film of a lateral brain field with the inferior border below the eyes. The eyes are shielded.

No. 4 SUPRATENTORIAL RECURRENCE * Jereb et al. 809
Autopsy examination of patients with medulloblas- toma and subfrontal tumor implants has occasionally provided further insight into the nature of these supra- tentorial recurrences. It is now generally accepted that the medulloblastoma is a primitive neuroecto- dermal tumor, which may show differentiation along neuronal or glial lines.21 In two recent cases studied at our Institution, tumor in the posterior fossa and along the spinal axis displayed in one patient abundant Homer-Wright rosettes (neuronal differentiation), and in the other patient, a mixture of astrocytoma and medulloblastoma (glial differentiation). Examination of the subfrontal tumor implants in these two cases, however, revealed primitive undifferentiated medullo- blastoma. 'This histologic disparity between the sub- frontal implants and the remainder of the tumor sug- gests that the subfrontal region in these patients provided a site for tumor growth that differed in some factor from, that provided elsewhere in the brain. Such a factor might well be focal suboptimal radiation, which would permit an overgrowth of mitotically active cells at the expense of less proliferative, maturing tumor cells.
To avoid subfrontal recurrence of medulloblastoma in the future, we are considering two possible tech- niques. One is the use of an 11 MeV electron beam with a small field between the eyes to boost the region of underdosage. This technique, however, does not ensure uniformity of dose particularly at the edges of the electron beam field. Another method would be the use of belt-driven gravity oriented blocks (Proimos device) that would involve a moving beam technique adapted for a portion of the head field.I5 Neither of these alternatives offers an easy solution, and both re- quire extensive cooperation between the therapist and the physicist. Treatment of these recurrences with radiation, chemotherapy, or surgery may produce useful palliation in some patient^.^.'^.'^
REFERENCES
I . Aron BS. Medulloblastorna in children. Am J Dis Child 1971; 121:314-317.
2. Banna A , Lassrnan LP, Pearce GW. Radiological study of skeletal metastases from cerebellar medulloblastoma. Br J Radiol 1970; 43: 173- 179.
3 . Bloom HJG. Combined modality therapy for intracranial tumors. Cancer 1975; 35:111- 120.
4. Bloom HJG, Wallace ENK, Henk JM. The treatment and prognosis of medulloblastoma in children. Am J Roentgenol 1969;
5 . Brutschin P, Culver GJL. Extracranial metastases from medulloblastoma. Radiology 1973; 107:359-362.
6. Bottrill DO, Rogers RT, Hope-Stone HF. A composite filter technique and special patient jig for treatment of the whole brain and spinal cord. Br J Radiol 1965; 38:122-130.
7. Chang CH, Honsepian EM, Herbert C. An operative staging system and a megavoltage radiotherapeutic technic for cerebellar medulloblastoma. Radiology 1969; 93: 1351- 1359.
8. Chatty EM, Earle KM. Medulloblastoma. A report of 201 cases with emphasis on the relationship of histological variants to survival. Cancer 1971; 28:977-983.
9 . Christ WM. Ragab AH, Vietti JJ, Ducos R, Chu JY. Chemo- therapy of childhood medulloblastoma. A m J Dis Child 1976; 130: 639- 642.
10. Clark EE, Hattner RS. Brain scintigraphy in recurrent rnedulloblastoma. Radiology 1976; I 19:633-636.
1 1 . Hardy DG, Hope-Stone HF, McKenzie CG, Scholtz CL. Recurrence of medulloblastoma after monogenous field radio- therapy. Report of three cases. J Neurosurg 1978; 49:434-440.
12. Harisiadis L, Chang CH. Medulloblastoma in children: a correlation of staging and results of treatment. lnt J Radial Oncol Biol Phys 1977; 2:833-841.
13. Hope-Stone HF. Results of treatment of medulloblastoma. J Neurosurg 1970; 32:83-88.
14. Jenkin RDT. Medulloblastoma in childhood. Radiation Therapy. Can Med Assoc J 1969; 100:51-53.
15. Kelley CD, Reid A, Simpson L, Hilaris B. The Proimos device: a gravity oriented blocking system for use in external radiation therapy. Bull Mem Sloan-Kerf 1976; 6: 107- 113.
16. King GA, Sagerrnan RH. Late recurrence in rnedulloblastoma. Am J Roentgenol Radium Ther Nucl Med 1975; 123:7- 12.
17. McFarland DR, Horowitz H, Saenger EL, Bahr GK. Medulloblastoma. A review of prognosis and survival. Br J Radio/ 1969; 42: 198-214.
18. Mealey J, Hall PV. Medulloblastoma in children. Survival and treatment. J Neurosurg 1977; 46:50-64.
19. Paterson E, Farr RF. Cerebellar rnedulloblastoma: Treatment of the whole central nervous system. Acfa Rudiol 1953; 39:323-336.
20. Quest DO, Brisman R, Antunes JL, Housepian EM. Period of risk for recurrence in medulloblastorna. J Neurosurg 1978; 48:
21. Russell DS, Rubinstein LJ. Pathology of Tumours of the Nervous System, 4th ed. Baltimore: Williams & Wilkins Co., 1977.
22. Smith CE, Long DM, JonesTK, Levitt SH. Medulloblastoma: an analysis of time-dose relationships and recurrence patterns. Cancer 1973; 32:722-728.
23. Tokars RP, Sutton HG, Griem ML. Cerebellar medullo- blastoma. Results of a new method of radiation treatment. Cancer
24. Wilson GB. Medulloblastoma. Current views regarding the tumor and treatment. Oncology 1970; 24:273-290.
25. Van Dyk J, Jenkin DT, Leung PMK, Cunningham JR. Medulloblastoma. Treatment technique and radiation dosimetry. Inf J Rndiaf Oncol Biol Phys 1977; 2:993- 1005.
105~43-62.
159- 163.
1979; 43: 129- 136.

![Medulloblastoma: [Print] - eMedicine Neurology · accounts for approximately 7-8% of all intracranial tumors and 30% of ... Incidence of medulloblastoma is 1.5-2 cases per ... Medulloblastoma:](https://img.dokumen.tips/doc/110x75/5b7fc2317f8b9ae6088caa0e/medulloblastoma-print-emedicine-accounts-for-approximately-7-8-of-all.jpg)