Embed Size (px)
Citation preview

7/30/2019 Subarachnoid Hemorrhage With Negative Initial Catheter Angiography
http://slidepdf.com/reader/full/subarachnoid-hemorrhage-with-negative-initial-catheter-angiography 1/7
Subarachnoid Hemorrhage With Negative InitialCatheter Angiography: A Review of 254 CasesEvaluating Patient Clinical Outcome and Efficacy of Short- and Long-term Repeat Angiography
BACKGROUND: Subarachnoid hemorrhage (SAH) is found to have no vascular originby initial catheter angiography in approximately 15% of cases. The most appropriatecourse for the type and frequency of additional diagnostic workup remains contro-versial.OBJECTIVE: To retrospectively assess the diagnostic yield of short-term and long-termrepeat catheter angiography in the era of advanced imaging.METHODS: Between 2003 and 2011, 254 consecutive patients diagnosed with SAH had
negative initial angiography. SAH was perimesencephalic (PM) in 46.5% and non-perimesencephalic (NPM) in 53.5%. Angiography was repeated at 1-week (short-term)and 6-week (long-term) intervals from the initial negative angiogram.RESULTS: Ten of 254 patients had a vascular source of hemorrhage on short-termfollow-up angiography with a diagnostic yield of 3.9%. One hundred seventy-fourpatients with negative findings on the first 2 angiograms received a third angiogram,and 7 of these patients were found to have a vascular abnormality. The estimated yieldof this third angiogram was 4.0%. The overall diagnostic yield of repeat angiographywas 0% in the PM group and 12.5% in the NPM group. The diagnostic yield of short-term and long-term follow-up angiography in patients with NPM SAH was 7.3% and7.8%, respectively. NPM patients were more likely to experience vasospasm andhydrocephalus requiring external ventricular drainage or cerebrospinal fluid diversion
than PM patients.CONCLUSION: Our results support a protocol of short-term and long-term angio-graphic follow-up in patients with NPM SAH and negative initial angiography.Aggressive protocols of follow-up angiography may not be necessary in patients withPM SAH.
KEY WORDS: Aneurysms, Digital subtraction angiography, Occult vascular lesions, Subarachnoid hemorrhage
Neurosurgery 72:646–652, 2013 DOI: 10.1227/NEU.0b013e3182846de8 www.neurosurgery-online.com
Subarachnoid hemorrhage (SAH) is a devas-tating neurological condition, accounting for approximately 3% to 5% of all strokes
and affecting 30 000 North Americans annu-ally.1,2 It is associated with a 30-day mortality ratethat can reach 45%.2 Catheter digital subtraction
angiography (DSA) remains the gold standard for the detection of a cerebral aneurysm or other vascular source of the hemorrhage. However,
nearly 15% of patients suffering from SAH havea negative initial DSA.3-15 Previous reports haveestimated that vascular abnormalities could beidentified in 2% to 24% of these cases on repeatDSA.3-7,10,12-14,16 However, many of thesereports precede the era of more advanced imaging techniques such as 3-dimensional (3-D)rotational angiography, magnetic resonance angi-ography (MRA), and computed tomography (CT) angiography (CTA) imaging.17,18
Richard Dalyai, MD
Nohra Chalouhi, MD
Thana Theofanis, BS
Pascal M. Jabbour, MD
Aaron S. Dumont, MD
L. Fernando Gonzalez, MD
David S. Gordon, MD
Robert H. Rosenwasser, MD
Stavropoula I. Tjoumakaris, MD
Department of Neurosurgery, Thomas
Jefferson University and Jefferson Hos-
pital for Neuroscience, Philadelphia,
Pennsylvania
Correspondence:
Stavropoula I. Tjoumakaris, MD,
Assistant Professor,
Department of Neurological Surgery,
Division of Neurovascular Surgery and
Endovascular Neurosurgery,
Thomas Jefferson University Hospital,
901 Walnut St, 3rd Floor,
Philadelphia, PA 19107.
E-mail: [email protected]
Received, May 24, 2012.
Accepted, December 10, 2012.
Published Online, December 28, 2012.
Copyright ª 2012 by the
Congress of Neurological Surgeons
SANS LifeLong Learning and
NEUROSURGERY offer CME for subscribers
that complete questions about featured
articles. Questions are located on the SANS
website (http://sans.cns.org/). Please read
the featured article and then log into SANS
for this educational offering.
ABBREVIATIONS: CTA, computed tomographicangiography; DSA, digital subtraction angiogra-phy; HH, Hunt and Hess; MRA, magnetic resonanceangiogram; NPM, nonperimesencephalic; PM, peri-mesencephalic; SAH, subarachnoid hemorrhage
RESEARCH—HUMAN—CLINICAL STUDIES
TOPIC RESEARCH —HUMAN —CLINICAL STUDIES
646 | VOLUME 72 | NUMBER 4 | APRIL 2013 www.neurosurgery-online.com
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

7/30/2019 Subarachnoid Hemorrhage With Negative Initial Catheter Angiography
http://slidepdf.com/reader/full/subarachnoid-hemorrhage-with-negative-initial-catheter-angiography 2/7
SAH with negative cerebral angiography can be categorized asperimesencephalic (PM) and nonperimesencephalic (NPM) typeson thebasis of the blood distribution on noncontrast head CT. PMhemorrhage is limited to the ambient, crural, and quadrigeminalcisterns without significant extension into the sylvian or inter-hemispheric fissures. This hemorrhage type has been reported to
have a more benign clinical course and is mostly nonaneurysmal inorigin.5,6,8,19 Conversely, patients with a more diffuse SAHpattern on initial head CT are more likely to have a positiverepeat angiography and to have worse clinical outcomes.19 NPMSAH was found to have 10% associated morbidity and mortality rate in a recent series of 180 patients.20 Given the uncertainty surrounding the yield of repeat DSA in patients with negativeinitial angiography, protocols have varied widely across differentinstitutions. Because of the dreaded complications related tountreated ruptured cerebral aneurysms, our neurovascular center undertakes a diagnostic protocol of repeat DSA at 1- and 6-week intervals after negative initial DSA. In addition, all patientscomplete an magnetic resonance image (MRI) of the brain and cervical spine and MRA of the head within 24 hours of thenegative catheter angiography.
The purpose of this study was to investigate the diagnostic yield of short (1 week) and long-term (6 weeks) catheter angiography inatraumatic SAH with negative initial angiography in an era of advanced noninvasive imaging technologies. Furthermore, weevaluated the clinical outcome of 254 patients with SAH and negative initial catheter angiography. We also analyzed and discussed the complications, outcomes, and discovered origins of occult SAH based on the hemorrhage pattern on initial CT.
PATIENTS AND METHODS
Approval from the Institutional Review Board was filed and granted for the retrospective data review of our study. From a prospectively collected database, we reviewed 254 consecutive patients with atraumatic SAHadmitted to our institution from2003 to 2011 who hadno vascularsourceidentified on initial 6-vessel DSA. Hemorrhage patterns on initial head CT were carefully reviewed and categorized by a radiologist and a neurosurgeon as PM or NPM on the basis of criteria established by van Gijn et al.14 Patients with a traumatic source of SAH weresystematically excluded from the analysis.
All patients underwent biplane DSA within 24 hours of admission that was negative for a vascular source of SAH. Angiography included a thorough inspection of all 6 vessels—bilateral internal, external, and vertebral arteries— with selective catheterization of all 6 vessels. Three-
dimensional reconstruction of intracranial vessels was obtained onfollow-up angiography. MRI of the brain and cervical spine and MRA of the brain were performed in all patients within 24 hours from the initialangiography in search for a vascular source for the bleeding. MRI wasperformed outside the 24-hour window only in patients who could nottolerate the study because of high intracranial pressures when lying flatfor extended periods of time. Negative MRI/MRA reports were thenfollowed by repeat 6-vessel DSA at the 1-week interval. Patients withpositive findings on the first follow-up angiography were treated immediately. Patients with another negative DSA received a third and final catheter angiogram at an approximately 6-week interval from the
initial study. Catheter angiography yield was determined for every subsequent angiogram. CTA was not routinely used as part of our institutional protocol. Besides their hemorrhage pattern, patients werefurther categorized on the basis of their Hunt and Hess (HH) grade, and the incidence of hydrocephalus, rehemorrhage, vasospasm, and shunting
was determined by the attending neurosurgeon of record.
RESULTS
A total of 254 patients met the study criteria. Of those, 118(46.5%) were PM-type SAH on initial head CT and 136 (53.5%) were NPM-type SAH (Table 1). The HH scores were as follows:grade I in 147 patients (57.8%), grade II in 10 patients (3.9%),grade III in 78 patients (30.7%), grade IV in 17 patients (6.7%),and grade V in 2 patients (0.8%) initially, which improved toa lower grade after external ventriculostomy. Patients withadvanced HH scores (III-V) included 23 patients (23.7%) withPM SAH and 74 patients (76.3%) with NPM SAH. A
comparison between NPM and PM SAH patients showed thatthe latter had a lower incidence of rehemorrhage (1.5% vs 0%),radiographic vasospasm (13.2% vs 8.5%), need for externalventriculostomy (37.5% vs 16%), and hydrocephalus requiring ventriculoperitoneal shunting (21.3% vs 6.8%; Table 1).
A vascular source for the SAH was identified in 17 patients(6.7%) with initially negative DSA. In no patient with follow-upangiography was MRI diagnostic for an aneurysmal source of SAH. Of those, 10 were identified with the first follow-up DSA,and the diagnostic yield of short-term repeat angiography in 1 week was found to be 3.9% (Table 2). All 10 patients were in theNPM group (Figures 1 and 2). One hundred seventy-four patients (85 with PM SAH and 89 with NPM SAH) with 2
negative DSA procedures underwent long-term follow-up angi-ography at 6 weeks, which revealed a vascular source in 7 patientsfor a yield of 4% (Table 3). All 7 patients were also in the NPMgroup. The overall diagnostic yield of repeat angiography was 0%in the PM group and 12.5% in the NPM group. The diagnosticyield of short-term and long-term repeat DSA in patients withNPM SAH was 7.3% and 7.8%, respectively.
TABLE 1. Patient Characteristics of Initial Hemorrhagic Patterna
NPM, n (%) PM, n (%)
Total patients 136 118HH grade III-V 74 (54.4) 23 (19.5)IVH 66 (48.5) 0EVD required 51 (37.5) 19 (16)VPS 29 (21.3) 8 (6.8)Radiographic vasospasm 18 (13.2) 10 (8.5)Rebleed 2 (1.5) 0
aEVD, external ventricular drain; HH, Hunt and Hess; IVH, intraventricular
hemorrhage; NPM, nonperimesencephalic; PM, perimesencephalic; VPS,
ventriculoperitoneal shunt.
ANGIOGRAM NEGATIVE SAH: YIELD OF REPEAT DSA
NEUROSURGERY VOLUME 72 | NUMBER 4 | APRIL 2013 | 647
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

7/30/2019 Subarachnoid Hemorrhage With Negative Initial Catheter Angiography
http://slidepdf.com/reader/full/subarachnoid-hemorrhage-with-negative-initial-catheter-angiography 3/7
The reasons for missing the lesion on the initial negativeangiograms were as follows: lesion not filling with contrast (n = 5),vasospasm (n = 2), suboptimal angiographic projection (n = 4),partially thrombosed aneurysm (n = 3), and larger protuberance(n = 3). Of note, 9 of the 17 patients did not have 3-Dreconstruction of the initial DSA. In 4 of 17 patients, 1-week or 6-week DSA was performed in a more thorough manner than thefirst DSA.
DISCUSSIONKey Results
The results of this study show that, in the patient population with initial negative catheter angiography, NPM patients experi-ence a higher incidence of neurological complicationsand sequelae
related to SAH compared with their PM counterparts. The overallyield of repeat catheter angiography in SAH with initial negativeangiography was 6.7%. Specifically, NPM patients had a highyield of repeat DSA (12.5%), whereas PM patients had a 0% yield of repeat DSA. The yield of short- and long-term repeatangiography was grossly similar (approximately 4%).
Interpretation
SAH with negative initial catheter angiography accounts for approximately 10% to 20% of all atraumatic SAH.20-36 Thisrepresents a significant patient population with limited data onthe natural history, prognosis, or diagnostic workup. Tradition-ally, angiogram-negative SAH was thought to portend a benignnatural history.22,24 Case series have investigated the outcome of angiogram-negative SAH on the basis of the initial noncontrasthead CT.6,8,10,11 Most patients with PM-type hemorrhages havefavorable clinical outcomes, which questions the need for aggressive diagnostic workup.6,7,11 This study proposes a thor-ough and aggressive diagnostic follow-up of these patients withboth short- and long-term catheter angiography. It also providesparticular insight into the diagnostic yield of repeat angiograms inboth angiogram-negative PM hemorrhages and those with a morediffuse bleeding pattern.
Rinkel and colleagues32,33 were among the first to differentiatePM hemorrhages from the remaining SAH population, demon-strating a benign medical course and low probability of associated vascular abnormalities. Recent evidence suggests a venous originfor most of these hemorrhages.34 A small cavernoma wasconsidered the source of hemorrhage in a recent case report.36
The prevalence of this subpopulation was estimated at 66% of all
angiogram-negative patients.
13
Although traditionally considered benign, PM hemorrhage has recently been associated with severalneurological complications of SAH. Hui et al26 have reported that 9.6% of PM SAH patients required a ventriculostomy and a similar percentage was medically treated for clinical vasospasm.These patients are further subject to complex neuropsychological
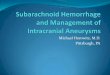
FIGURE 1. A 54-year-old female patient presented with Hunt and Hess grade III nonperimesencephalic hemorrhage on initial head computed tomography. Negative initial
angiography in the frontal projection ( A ) with 3-dimensional reconstruction ( B ). Magnetic resonance imaging/angiography was nondiagnostic for vascular source. Short-term
angiography at 7 days in the frontal projection ( C ) and 3-dimensional reconstruction ( D ) identified a 3-mm anterior communicating artery aneurysm that was successfully treated with coil embolization.
TABLE 2. Short-term Angiographic Positive Findingsa
Patient Angiograms, n Source Treatment
1 2 P1 aneurysm Stent/coil2 2 Anterior choroidal
aneurysmClip/wrap
3 2 Distal PICAaneurysm
WDOC/notreatment
4 2 Vertebral arteryaneurysm
Coil
5 2 Basilarpseudoaneurysm
Clip
6 2 ACOM aneurysm Clip7 2 ACOM aneurysm Coil8 2 Pericallosal aneurysm Clip9 2 PICA aneurysm Onyx 34
10 2 ACOM aneurysm Clip
aACOM, anterior communicating artery; DHC, decompressive hemicraniectomy;
ICA, internal carotid artery; PICA, posterior inferior cerebellar artery; WDOC,
withdrawal of care.
DALYAI ET AL
648 | VOLUME 72 | NUMBER 4 | APRIL 2013 www.neurosurgery-online.com
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

7/30/2019 Subarachnoid Hemorrhage With Negative Initial Catheter Angiography
http://slidepdf.com/reader/full/subarachnoid-hemorrhage-with-negative-initial-catheter-angiography 4/7
deficits from SAH sequelae.30 Overall, they reported favorableclinical outcomes in 96% of this patient population with returnto independent living. The risk of rebleeding from PM SAHis minimal and documented in few case reports.31
DSA is known to have an average sensitivity of 99% and negative predictive value of 96% to 98%.10,16-18 Studies havefound that 10% to 16% of posterior circulation skull baseruptured aneurysms present with a PM pattern on initial head CT.2,17,18,27 These statistics suggest the need for vascular imaging with the highest accuracy to promptly diagnose and treat patients with a potentially identifiable vascular source for SAH.
Among the 118 patients with PM SAH in our series,a significant percentage required intensive medical and, at times,
surgical interventions as a result of SAH-related morbidities.Twenty-three patients (19.5%) initially presented as HH grade IIIor greater with an altered mental status. Although Ildan et al5
reported a 1% incidence of shunt-dependent hydrocephalus inpatients with PM SAH, we found that 19 of 118 patients (16%)required a ventriculostomy for hydrocephalus or poor clinicalgrade. Furthermore, 8 patients (6.8%) with PM hemorrhage
eventually required permanent cerebrospinal fluid diversion, and 10 patients (8.5%) had increased middle cerebral artery velocities(.200 cm/s and Lindegaard ratio .3) and radiographicvasospasm on repeat angiograms. However, none required endovascular angioplasty or other procedural interventions for the treatment of clinical vasospasm. The rate of vasospasm after PM SAH was found to be 2.2% by Andaluz and Zuccarello.3 Thesame authors found positive findings on DSA for a vascular source in 13.9% of patients with PM SAH. However, their protocol was not standardized with regard to follow-up angiog-raphy, and only 35 of 45 patients received a second angiogramafter a negative initial DSA. These findings suggested that PMSAH and its neurological sequelae should be diagnosed and
treated aggressively, similar to other SAH. We found no patient with PM SAH and negative initial angiography to harbor anoccult vascular source on short- or long-term repeat angiography, which may call into question the necessity of subsequentangiography (DSA or CTA) in this patient population.
Generally, patients with a more diffuse pattern of hemorrhageon head CT (NPM SAH) and no vascular source on initialangiogram have a clinical course similar to that of patients withSAH from known ruptured aneurysms. Andaluz and Zuccarello3
reported poor outcomes in 36% of these patients. Similarly,Ruigrok et al8 reported worse conditions on arrival, clinicalcourse, morbidities, and long-term outcomes compared withpatients with PM hemorrhages.
Our findings with regard to this patient population were largely similar. We found a 12.5% yield of short- andlong-term follow-upangiography in NPM SAH patients. NPM SAH patientspresented with a Hunt and Hess grade between III and V in54% of cases and were more likely to experience radiographicvasospasm and hydrocephalus requiring external ventriculostomy/cerebrospinal fluid diversion compared with their PM counter-parts. Most worrisome, 2 patients with NPM SAH had clinically significant rebleeding episodes (1 patient after 1 week, and theother after 2 weeks). These patients are of great concern and
TABLE 3. Long-term Angiographic Positive Findingsa
Patient Angiograms, n Source Treatment
1 3 ACOM aneurysm Clip/wrap
2 3 Basilarpseudoaneurysm
Stent/coil
3 3 PICA AVF NBCA embolization4 3 Distal PCA aneurysm Coil5 3 MCA aneurysm Clip6 3 MCA aneurysm Clip7 3 Vertebral aneurysm Clip
aACOM, anterior communicating artery; AVF, arteriovenous fistula; MCA, middle
cerebral artery; NBCA, N-butyl cyanoacrylate; PCA, posterior cerebral artery; PICA,
posterior inferior cerebellar artery.
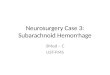
FIGURE 2. A 57-year-old female patient presented with Hunt and Hess grade III nonperimesencephalic hemorrhage on initial head computed tomography ( A ). Lateral
projection ( B ) of negative initial angiography of posterior circulation. Lateral projection ( C ) of short-term follow-up angiography identifying a 5-mm right posterior inferior cerebellar artery (PICA) aneurysm. Lateral projection ( D ) of right PICA aneurysm after successful Onyx 34 embolization.
ANGIOGRAM NEGATIVE SAH: YIELD OF REPEAT DSA
NEUROSURGERY VOLUME 72 | NUMBER 4 | APRIL 2013 | 649
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

7/30/2019 Subarachnoid Hemorrhage With Negative Initial Catheter Angiography
http://slidepdf.com/reader/full/subarachnoid-hemorrhage-with-negative-initial-catheter-angiography 5/7
provide the rationale for a complete diagnostic workup for a vascular source to prevent such potentially life-devastating events.
Repeat imaging for initial angiogram-negative SAH is contro-versial because of the various diagnostic modalities and lack of a clear consensus on yield. Some centers have proposed the use of
CTA to triage all SAH patientsanddefer the use ofDSA in patients with a PM SAH.25 Ruigrok et al7 suggested a mathematical modelto estimate the utility of the diagnostic workup for PM SAH and recommend CTA imaging only. However, the analysis focused on a low prevalence (4%) of vertebrobasilar aneurysms in PMSAH while potentially overestimating the sensitivity of CTA (97%) for detecting aneurysms in this patient population.Furthermore, their reported complication rate for catheter angiography was 2.5%, whereas reports have shown that inmost high-volume vascular centers it is ,1%.23 In PM SAH, Agid et al21 reported a CTA false-negative rate of 10%, but all of these presented with a diffuse pattern of blood on initial head CT. Westerlaan et al35 similarly reported 60 patients with negativefindings on CTA and found 5 of 17 patients (29%) with NPMSAH to have a vascular source on DSA. Other case series haveinvestigated a paradigm similar to the one in this study but witha single short-term repeat angiography. Our series proposesa second long-term repeat catheter angiogram, especially for patients with NPM-type SAH. Delayed SAH resorption and resolution of radiographic vasospasm could explain the 12.5%diagnostic yield of follow-up angiography.
The diagnostic yield of repeat vascular imaging has varied greatly in the literature, and many reports predate the common useof 3-D rotational angiography and advanced MRI (contrast-enhanced circle of Willis, 4-dimensional tracks). Studies have
reported a 20% incidence of positive vascular findings on repeatangiography for NPM hemorrhage.3 The incidence of positivefindings on a third long-term follow-up DSA has been reported to be between 7% and 10%.3,5,8,12,13 These studies contribute toour understanding of this population, which is still limited by study protocols predating 3-D rotational angiography,27-29,37
small sample sizes,26,38 inconsistent imaging protocols,39 or lack of long-term angiographic follow-up for most patients.3,40,41 Our protocol ultimately identified a 7.3% yield for short-term follow-up angiography and 7.8% yield for long-term 6-week follow-upDSA in patients with NPM SAH. This significant yield on long-term follow-up angiography highlights the need for aggressiveangiographic follow-up in NPM SAH patients.
The results of this study propose a systematic approach toSAH patients with initially negative catheter angiography. Ina neurointerventional era when angiography complicationrates are #1%, further aggressive work-up of patients withNPM is strongly indicated.23 Our recommendations consistof repeat angiography in 1 week after initially negativeangiography in these patients. We also recommend long-term follow-up angiography at 6 weeks, outside the period of cerebral vasospasm, considering the reported 7.8% yield onfinal long-term angiography.
Limitations
We recognize the inherent limitations of this study based on itsretrospective data collection. Because 3-D reconstruction was notperformed on theinitial angiogram in a fewpatients, some aneurysmscould have potentially been missed initially, and this may haveslightly overestimated the diagnostic yield of repeat angiography.
Generalizability
Our results reflect the experience of a single institution and may not be generalizable to other centers. Our protocol does notinclude a preoperative or postoperative CTA in patients withangiogram-negative SAH. As a result, we cannot contrast the yield of CTA in the same patient series or compare our results witha CTA series. Because catheter angiography has been reported tohave higher diagnostic power compared with conventional CTA, we believe that CTA after initially negative DSA carries additionalrisk of dye-related renal toxicity with little or no additionaldiagnostic benefit. Additional studies comparing newer diagnostic
techniques such as subtraction 320-detector CTA and conven-tional angiography are required to further investigate diagnosticimaging in this patient population.
CONCLUSION
We found that, in the patient population with initial negativecatheter angiography, NPM patients experience a higher inci-dence of neurological complications andsequelaerelated to SAHcompared with their PM counterparts, including hydrocephalusrequiring external ventriculostomy or permanent cerebrospinalfluid diversion and radiographic vasospasm on repeat angiogra-phy. We report the overall yield of repeat catheter angiography in
SAH with initial negative angiography to be 6.7%. Thisincludesshort-term (1 week) and long-term (6 weeks) repeat angiogra-phy. Patients with NPM SAH had a high yield of repeat DSA (12.5%), whereas patients with PM SAH had a 0% yield of repeat DSA. Therefore, we propose follow-up catheter angiog-raphy at both intervals only in patients with NPM hemorrhage.This proposed protocol should be carried out in institutions withlow angiographic complication rates. Our results, however, donot support an aggressive protocol of repeat angiography inpatients with PM SAH.
Disclosures
Dr Jabbour has been a consultant forev3, Codman, and Mizuho. Dr Tjoumakarishas been a consultant for Stryker. Dr Gonzalez has been a consultant for ev3.
Dr Dumont has been a consultant for ev3 and Stryker. Dr Rosenwasser has been
a consultant forBostonScientific. Theother authorshave no personal financialor
institutional interest in any of the drugs, materials, or devices described in this
article.
REFERENCES
1. Abu Bakar I, Shuaib IL, Mohd Ariff AR, Naing NN, Abdullah JM. Diagnostic
cerebral angiography in spontaneous intracranial haemorrhage: a guide for developing countries. Asian J Surg. 2005;28(1):1-6.
DALYAI ET AL
650 | VOLUME 72 | NUMBER 4 | APRIL 2013 www.neurosurgery-online.com
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

7/30/2019 Subarachnoid Hemorrhage With Negative Initial Catheter Angiography
http://slidepdf.com/reader/full/subarachnoid-hemorrhage-with-negative-initial-catheter-angiography 6/7
2. Bederson JB, Connolly ES Jr, Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionalsfrom a special writing group of the Stroke Council, American Heart Association.Stroke . 2009;40(3):994-1025.
3. Andaluz N, Zuccarello M. Yield of further diagnostic work-up of cryptogenicsubarachnoid hemorrhage based on bleeding patterns on computed tomographicscans. Neurosurgery . 2008;62(5):1040-1046; discussion 1047.
4. Hashimoto H, Iida J, Hironaka Y, Okada M, Sakaki T. Use of spiral computerized tomography angiography in patients with subarachnoid hemorrhage in whomsubtraction angiography did not reveal cerebral aneurysms. J Neurosurg. 2000;92(2):278-283.
5. Ildan F, Tuna M, Erman T, Gocer AI, Cetinalp E, Burgut R. Prognosis and prognostic factors for unexplained subarachnoid hemorrhage: review of 84 cases.Neurosurgery . 2002;50(5):1015-1024; discussion 1024-1025.
6. Rinkel GJ, Velthuis BK. Long term follow up after perimesencephalic sub-arachnoid haemorrhage. J Neurol Neurosurg Psychiatry. 2001;70(3):419-420.
7. Ruigrok YM, Rinkel GJ, Buskens E, Velthuis BK, van Gijn J. Perimesencephalichemorrhage and CT angiography: a decision analysis. Stroke . 2000;31(12):2976-2983.
8. Ruigrok YM, Rinkel GJ, Van Gijn J. CT patterns and long-term outcome inpatients with an aneurysmal type of subarachnoid hemorrhage and repeatedly negative angiograms. Cerebrovasc Dis. 2002;14(3-4):221-227.
9. Schievink WI, Wijdicks EF, Spetzler RF. Diffuse vasospasm after pretruncalnonaneurysmal subarachnoid hemorrhage. AJNR Am J Neuroradiol. 2000;21(3):521-523.
10. Schwartz TH, Farkas J. Quadrigeminal non-aneurysmal subarachnoid hemor-rhage: a true variant of perimesencephalic subarachnoid hemorrhage: case report.Clin Neurol Neurosurg. 2003;105(2):95-98.
11. Schwartz TH, Solomon RA. Perimesencephalic nonaneurysmal subarachnoid hemorrhage: review of the literature. Neurosurgery . 1996;39(3):433-440; discus-sion 440.
12. Topcuoglu MA, Ogilvy CS, Carter BS, Buonanno FS, Koroshetz WJ, Singhal AB.Subarachnoid hemorrhage without evident cause on initial angiography studies:diagnostic yield of subsequent angiography and other neuroimaging tests. J Neurosurg. 2003;98(6):1235-1240.
13. Urbach H, Zentner J, Solymosi L. The need for repeat angiography insubarachnoid haemorrhage. Neuroradiology . 1998;40(1):6-10.
14. van Gijn J, van Dongen KJ, Vermeulen M, Hijdra A. Perimesencephalichemorrhage: a nonaneurysmal and benign form of subarachnoid hemorrhage.Neurology . 1985;35(4):493-497.
15. Velthuis BK, Rinkel GJ, Ramos LM, Witkamp TD, van Leeuwen MS.Perimesencephalic hemorrhage: exclusion of vertebrobasilar aneurysms with CTangiography. Stroke . 1999;30(5):1103-1109.
16. Schievink WI, Wijdicks EF. Pretruncal subarachnoid hemorrhage: an anatomically correct description of the perimesencephalic subarachnoid hemorrhage. Stroke .1997;28(12):2572.
17. Luo Z, Wang D, Sun X, et al. Comparison of the accuracy of subtraction CTangiography performed on 320-detector row volume CT with conventional CTangiography for diagnosis of intracranial aneurysms. Eur J Radiol. 2012;81(1):118-122.
18. Yeung R, Ahmad T, Aviv RI, de Tilly LN, Fox AJ, Symons SP. Comparison of CTA to DSA in determining the etiology of spontaneous ICH. Can J Neurol Sci.2009;36(2):176-180.
19. Weyerbrock A, Woznica M, Rosahl SK, Berlis A. Aneurysmal and non-aneurysmal SAH: is initial computed tomography predictive? Rofo . 2009;181(9):881-887.
20. Maslehaty H, Barth H, Petridis AK, Doukas A, Maximilian Mehdorn H. Specialfeatures of subarachnoid hemorrhage of unknown origin: a review of a series of 179cases. Neurol Res. 2012;34(1):91-97.
21. Agid R, Andersson T, Almqvist H, et al. Negative CT angiography findings inpatients with spontaneous subarachnoid hemorrhage: when is digital subtractionangiography still needed? AJNR Am J Neuroradiol. 2010;31(4):696-705.
22. Bradac GB, Bergui M, Ferrio MF, Fontanella M, Stura G. False-negativeangiograms in subarachnoid haemorrhage due to intracranial aneurysms.Neuroradiology . 1997;39(11):772-776.
23. Cloft HJ, Joseph GJ, Dion JE. Risk of cerebral angiography in patients withsubarachnoid hemorrhage, cerebral aneurysm, and arteriovenous malformation:a meta-analysis. Stroke . 1999;30(2):317-320.
24. Giombini S, Bruzzone MG, Pluchino F. Subarachnoid hemorrhage of unexplained cause. Neurosurgery . 1988;22(2):313-316.
25. Guevara-Dondé JE, Rogel-Ortiz F. Subarachnoid hemorrhage with negativeangiography [in Spanish]. Gac Med Mex. 1999;135(2):107-112.
26. Hui FK, Tumialán LM, Tanaka T, Cawley CM, Zhang YJ. Clinicaldifferences between angiographically negative, diffuse subarachnoid hemor-rhage and perimesencephalic subarachnoid hemorrhage. Neurocrit Care. 2009;11(1):64-70.
27. Inamasu J, Nakamura Y, Saito R, et al. “Occult” ruptured cerebral aneurysmsrevealed by repeat angiography: result from a large retrospective study. Clin Neurol Neurosurg. 2003;106(1):33-37.
28. Jafar JJ, Weiner HL. Surgery for angiographically occult cerebral aneurysms. J Neu rosu rg. 1993;79(5):674-679.
29. Jung JY, Kim YB, Lee JW, Huh SK, Lee KC. Spontaneous subarachnoid haemorrhage with negative initial angiography: a review of 143 cases. J ClinNeurosci. 2006;13(10):1011-1017.
30. Madureira S, Canhão P, Guerreiro M, Ferro JM. Cognitive and emotionalconsequences of perimesencephalic subarachnoid hemorrhage. J Neurol. 2000;247(11):862-867.
31. Reynolds MR, Blackburn SL, Zipfel GJ. Recurrent idiopathic perimesencephalicsubarachnoid hemorrhage. J Neurosurg. 2011;115(3):612-616.
32. Rinkel GJ, van Gijn J, Wijdicks EF. Subarachnoid hemorrhage without detectableaneurysm: a review of the causes. Stroke . 1993;24(9):1403-1409.
33. Rinkel GJ, Wijdicks EF, Hasan D, et al. Outcome in patients with subarachnoid
haemorrhage and negative angiography according to pattern of haemorrhage oncomputed tomography. Lancet . 1991;338(8773):964-968.
34. van der Schaaf IC, Velthuis BK, Gouw A, Rinkel GJ. Venous drainage inperimesencephalic hemorrhage. Stroke . 2004;35(7):1614-1618.
35. Westerlaan HE, Gravendeel J, Fiore D, et al. Multislice CT angiography in theselection of patients with ruptured intracranial aneurysms suitable for clipping or coiling. Neuroradiology . 2007;49(12):997-1007.
36. Yaghi S, Oomman S, Keyrouz SG. Non-aneurysmal perimesencephalic sub-arachnoid hemorrhage caused by a cavernous angioma. Neurocrit Care. 2011;14(1):84-85.
37. Pathirana N, Refsum SE, McKinstry CS, Bell KE. The value of repeat cerebralangiography in subarachnoid haemorrhage. Br J Neurosurg. 1994;8(2):141-146.
38. Kokkinis C, Vlychou M, Zavras GM, Hadjigeorgiou GM, Papadimitriou A,Fezoulidis IV. The role of 3D-computed tomography angiography (3D-CTA) ininvestigation of spontaneous subarachnoid haemorrhage: comparison with digitalsubtraction angiography (DSA) and surgical findings. Br J Neurosurg. 2008;22(1):
71-78.39. van Rooij WJ, Peluso JP, Sluzewski M, Beute GN. Additional value of 3D rotational
angiography in angiographically negative aneurysmal subarachnoid hemorrhage: how negative is negative? AJNR Am J Neuroradiol. 2008;29(5):962-966.
40. Ishihara H, Kato S, Akimura T, Suehiro E, Oku T, Suzuki M. Angiogram-negativesubarachnoid hemorrhage in the era of three dimensional rotational angiography. J Clin Neurosci. 2007;14(3):252-255.
41. Whiting J, Reavey-Cantwell J, Velat G, et al. Clinical course of nontraumatic,nonaneurysmal subarachnoid hemorrhage: a single-institution experience. Neuro- surg Focus. 2009;26(5):E21.
COMMENTS
This article is a retrospective review of patients presenting with sub-arachnoid hemorrhage with an initial negative angiogram. The
authors have broken down the subarachnoid hemorrhage into peri-mesencephalic and nonperimesencephalic type of hemorrhage and havelooked at the importance of performing repeat angiography in 1 week and again in 6 weeks. As this article nicely points out, peri-mesencephalic-type hemorrhage is a more benign entity, and the risk of subsequent shuntingand vasospasmand the chance of finding an arterialsource of the hemorrhage are low. On the other hand, when the sub-arachnoid hemorrhage extends beyond the perimesencephalic area, therisks of needing a ventriculoperitoneal shunt and of vasospasm and thechance of finding, for instance, an aneurysm in a delayed fashionincrease. This article reinforces our belief that nonperimesencephalic
ANGIOGRAM NEGATIVE SAH: YIELD OF REPEAT DSA
NEUROSURGERY VOLUME 72 | NUMBER 4 | APRIL 2013 | 651
Copyright © Congress of Neurological Surgeons. Unauthorized reproduction of this article is prohibited.

7/30/2019 Subarachnoid Hemorrhage With Negative Initial Catheter Angiography
http://slidepdf.com/reader/full/subarachnoid-hemorrhage-with-negative-initial-catheter-angiography 7/7
type of subarachnoid hemorrhage with negative angiogram findingsneeds more short- and long-term angiographic follow-up. At our insti-tution, the long-term angiogram tends to be a computed tomography angiogram because it is less invasive than the conventional catheter angiogram, and with 3-dimensional reconstruction, the sensitivity of this imaging modality is very high.
Roham Moftakhar Chicago, Illinois
This is a retrospective review of patients presenting with subarachnoid hemorrhage with an initial negative angiogram. The authors analyze
the outcome of 258 consecutive patients between 2003-2011. The
authors divide the patients into 2 groups perimesencephalic and non-perimesencephalic type of hemorrhage. Angiograms were performed atthetimeof initial hemorrhage, oneweek, andagain in 6 weeks.Theoveralldiagnostic yield of repeat angiography in the perimesencephalic group was0% and 15% in the nonperimesencephalic group. This article reinforcesthat short and long-term angiographic follow-up is not needed for peri-mesencephalic hemorrhage. The diagnostic yield on the initial angiogramsmay have been higher in the nonperimesencephalic group if 3-dimen-sional imaging was performed in all cases and 2 staff had reviewed theimages.
Joseph Gemmete Ann Arbor, Michigan
DALYAI ET AL
652 | VOLUME 72 | NUMBER 4 | APRIL 2013 www.neurosurgery-online.com