Upload
prima-eriawan-putra
View
51
Download
13
Embed Size (px)
DESCRIPTION
Neuro
Citation preview
Prima Eriawan Putra 1102012212 1
1. Anatomi Nervus Cranialis dan Jaras Motorik serta Sensorik
1.1. Nervus Kranialis
The cranial nerves are analogous in some ways to the spinal nerves, having both sensory and motor functions. Also, like the spinal cord, motor cranial nerve nuclei are located more ventrally, while sensory cranial nerve nuclei are located more dorsally. However, cranial nerve sensory and motor functions are more specialized because of the unique anatomy of the head and neck.
Brainstem I: Surface Anatomy and Cranial Nerves 495
Learning the cranial nerves initially requires some memorization. Over time,however, they become very familiar because of their important clinical rele-vance. The numbers, names, and main functions of the cranial nerves are listedin Table 12.1. Note that the cranial nerves have both sensory and motor func-tions. To learn the cranial nerves and their functions, two different reviewstrategies are useful. In one, the cranial nerves are listed in numerical sequenceand the sensory and motor functions of each nerve are discussed (see Table12.4). In the second, the different sensory and motor cranial nerve nuclei arelisted, and the functions and cranial nerves subserved by each nucleus are dis-cussed (see Table 12.3). Both approaches are clinically relevant, and we will useboth strategies at various points in these brainstem chapters to integrate knowl-edge of the peripheral and central course of the cranial nerves.
Surface Features of the BrainstemThe brainstem consists of the midbrain, pons, and medulla (see Figure 12.1). Itlies within the posterior fossa of the cranial cavity. The rostral limit of the brain-stem is the midbraindiencephalic junction (see Figure 12.1). Here the brainstemmeets thalamus and hypothalamus at the level of the tentorium cerebelli. Mid-brain joins pons at the pontomesencephalic junction, and pons meets medullaat the pontomedullary junction. The caudal limit of the brainstem is the cervi-comedullary junction, at the level of the foramen magnum and pyramidal de-cussation (see Figure 12.1, Figure 12.2A; see also Figure 6.8). The cerebellum isattached to the dorsal surface of the pons and upper medulla (see Figure 12.1).Although some authors have included the cerebellum or thalamus in the termbrainstem, we adopt common clinical usage here and take brainstem toimply only midbrain, pons, and medulla. We discuss the thalamus and cere-bellum at greater length elsewhere (see Chapters 7 and 15).
On the dorsal surface of the midbrain are two pairs of bumps called the su-perior colliculi and inferior colliculi (Figure 12.2B). Together, these form the tec-
TABLE 12.1 Cranial Nerve Names and Main Functions
CN NAME MAIN FUNCTION(S)
CN I Olfactory nerve OlfactionCN II Optic nerve VisionCN III Oculomotor nerve Eye movements; pupil constrictionCN IV Trochlear nerve Eye movementsCN V Trigeminal nerve Facial sensation; muscles of
masticationCN VI Abducens nerve Eye movementsCN VII Facial nerve Muscles of facial expression;
taste; lacrimation; salivationCN VIII Vestibulocochlear nerve Hearing; equilibrium senseCN IX Glossopharyngeal nerve Pharyngeal muscles; carotid body
reflexes; salivationCN X Vagus nerve Parasympathetics to most organs;
laryngeal muscles (voice);pharyngeal muscles (swallowing); aortic arch reflexes
CN XI Spinal accessory nerve Head turning (trapezius and ster-nomastoid muscles)
CN XII Hypoglossal nerve Tongue movement
REVIEW EXERCISECover the two right columns in Table 12.1. For each numberedcranial nerve, provide its name andmain functions.
REVIEW EXERCISEFor the midbrain, pons and medullain Figure 12.1 or 12.2C, point in therostral, caudal, dorsal, ventral, supe-rior, inferior, posterior and anteriordirections (see definitions in Figure2.4). How do these differ for pointsabove the midbraindiencephalicjunction?
BL2eBlum12.qxd 2/16/10 12:12 PM Page 495
500 Chapter 12
Sensory and Motor Organization of the Cranial NervesThe cranial nerves are analogous in some ways to the spinal nerves, havingboth sensory and motor functions. Also, like the spinal cord, motor cranialnerve nuclei are located more ventrally, while sensory cranial nerve nucleiare located more dorsally (Figure 12.4). However, cranial nerve sensory andmotor functions are more specialized because of the unique anatomy of thehead and neck. During embryological development, the cranial nerve nucleilie adjacent to the ventricular system (see Figure 12.4A). As the nervous sys-
REVIEW EXERCISECover the right column in Table 12.2.Name the exit foramina for each cra-nial nerve (see Figure 12.3).
TABLE 12.2 Cranial Nerve Exit Foramina
CN NAME EXIT FORAMEN
CN I Olfactory nerves Cribriform plateCN II Optic nerve Optic canalCN III Oculomotor nerve Superior orbital fissureCN IV Trochlear nerve Superior orbital fissureCN V Trigeminal nerve V1: Superior orbital fissure
V2: Foramen rotundumV3: Foramen ovale
CN VI Abducens nerve Superior orbital fissurea
CN VII Facial nerve Auditory canal (stylomastoid foramen)
CN VIII Vestibulocochlear nerve Auditory canalCN IX Glossopharyngeal nerve Jugular foramenCN X Vagus nerve Jugular foramenCN XI Spinal accessory nerve Jugular foramen (enters skull
via foramen magnum)CN XII Hypoglossal nerve Hypoglossal foramen (canal)
aThe abducens nerve first exits the dura through Dorellos canal (see Figure 12.3) and thentravels a long distance before exiting the skull at the superior orbital fissure.
(A)
Sulcus limitans
Fourthventricle
Visceral motornuclei
Somatic motornuclei
Motor nucleiSensory nuclei
Key
(B)
Somaticsensorynuclei
Visceralsensorynuclei
Sulcuslimitans
Branchialmotor: SVE(nucleusambiguus)
Parasympathetic:GVE (dorsalmotor nucleusof CN X)
Somatic motor:GSE (hypoglossal nucleus)
Visceral sensory:SVA and GVA(nucleussolitarius)
Special somaticsensory: SSA(vestibularnuclei)
General somaticsensory: GSA(spinaltrigeminalnucleus)
FIGURE 12.4 Development of CranialNerve Nuclei Sensory and Motor Lon-gitudinal Columns (A) Cross section ofhuman myelencephalon at 45 daysshowing locations of sensory and motorcranial nerve nuclei functional columns.(B) Adult medulla, with locations offunctional columns indicated. Examplesof the nuclei in these columns for a sec-tion at this level are indicated in paren-theses. (A after Tuchman-Duplessis H,Auroux M, and Haegel P. 1974. IllustratedHuman Embryology. Volume 3. NervousSystem and Endocrine Glands. Masson &Company, Paris. B after Martin JH. 1996.Neuroanatomy: Text and Atlas. 2nd Ed.McGraw-Hill, New York.)
BL2eBlum12.qxd 2/16/10 12:12 PM Page 500
Prima Eriawan Putra 1102012212 2
Cranial Nerve I: Olfactory Nerves
Olfactory stimuli are detected by specialized chemoreceptors on bipolar primary sensory neurons in the olfactory neuroepithelium of the upper nasal cavities. Axons of these neurons travel via short olfactory nerves that traverse the cribriform plate of the ethmoid bone to synapse in the olfactory bulbs. From the olfactory bulbs, information travels via the olfactory tracts, which run in the olfactory sulcus between the gyrus rectus and orbital frontal gyri to reach olfactory processing aeas. Note that although the olfactory bulbs and tracts are sometimes called CN I, these structures are actually not nerves, but are part of the central nervous system.
828 Chapter 18
ecule usually activates several olfactory receptors, enabling a virtually infinitenumber of different odors to be identified through combinatorial processing.Olfactory receptor neurons send unmyelinated axons in the olfactory nervesthrough the cribriform plate to reach the olfactory bulb (Figure 18.5). The olfac-tory bulb is part of the central nervous system that lies in a groove called theolfactory sulcus, between the gyrus rectus and orbitofrontal gyri (Figure 18.6).In the glomeruli of the olfactory bulb (see Figure 18.5), olfactory receptor neu-rons synapse onto mitral cells and tufted cells, both of which have long axonsthat enter the olfactory tract to reach the olfactory cortex. Collaterals in the ol-factory tract synapse onto scattered neurons, forming the anterior olfactory nu-
Mitral cell
Glomerulus
Olfactorynerve
Olfactoryreceptorneuron
Olfactory tract
To contralateral olfactory bulb
To olfactory areas (piriformcortex, periamygdaloid cortex,olfactory tubercle, amygdala)
Anteriorolfactorynucleus
Tufted cell
Cribriformplate
Olfactorymucosa
Olfactory bulb
FIGURE 18.5 Principal Neurons and Pathways of Olfactory Nervesand Olfactory Bulbs For simplicity, the periglomerular cells and gran-ule cells (the major interneurons of the olfactory bulb) are not shown.
Collateral sulcus
Parahippocampalgyrus
Parahippocampalcortex
Rhinal sulcus
Occipitotemporal(fusiform gyrus)
Orbitofrontalolfactory area
Amygdala(seen throughcortex)
Perirhinal cortex
Lateral olfactorystria
Medial olfactorystria
Entorhinal cortex
Piriform and periamygdaloidcortex (primary olfactory cortex)
Olfactory sulcus
Olfactory bulb
Olfactory tract
Orbital frontal cortex
Anterior perforatedsubstance
Gyrus rectus
Inferior temporal sulcus
FIGURE 18.6 Central Olfactory Structures and Other Components of the Parahippocampal Gyrus Inferior view.
BL2eCh18.qxd 2/16/10 12:49 PM Page 828
Brainstem I: Surface Anatomy and Cranial Nerves 501
tem matures, three motor columns and three sensory columns of cranial nervenuclei develop that run in an interrupted fashion through the length of thebrainstem (see Figure 12.4 and Figure 12.5). Each column subserves a differ-ent motor or sensory cranial nerve function, which can be classified as shownin Table 12.3. The color codes for each column used in Figures 12.4 and 12.5and in Table 12.3 will remain constant throughout this chapter. In another setof terminology described toward the end of this section (and listed in the fig-ures and tables) each column can also be described as general vs. special, so-matic vs. visceral, and afferent vs. efferent. Lets review each of these columnsin more detail, moving from medial to lateral.
Motor nuclei Sensory nuclei
EdingerWestphal nucleus (GVE: CN III)
Oculomotor nucleus (GSE: CN III)
Trochlear nucleus (GSE: CN IV)
Superior salivatory nucleus (GVE: CN VII)
Abducens nucleus (GSE: CN VI)
Trigeminal motor nucleus (SVE: CN V)
Trigeminal nuclei (GSA: CN V, VII, IX, X):
Mesencephalic nucleus of CN V
Chief sensory nucleus of CN V
Spinal trigeminal nucleus
Dorsal and ventral cochlear nuclei(SSA: CN VIII)
Vestibular nuclei (SSA: CN VIII)
Nucleus solitarius, rostral portion(SVA: CN VII, IX, X)
Nucleus solitarius, caudal portion(GVA: CN IX, X)
Facial nucleus (SVE: CN VII)
Dorsal motor nucleus of CN X (GVE: CN X)
Nucleus ambiguus (SVE: CN IX, X)
Hypoglossal nucleus (GSE: CN XII)
Spinal accessory nucleus (SVE: CN XI)
Branchial motor column = SVE Special somatic sensory column = SSA
General somatic sensory column = GSA
Visceral sensory column = SVA and GVA
Parasympathetic column = GVE
Somatic motor column = GSE
Inferior salivatory nucleus (GVE: CN IX)
FIGURE 12.5 FunctionalColumns of Brainstem Sensoryand Motor Cranial Nerve NucleiLongitudinal schematic. GSA,general somatic afferent; GSE,general somatic efferent; GVA,general visceral afferent; GVE,general visceral efferent; SSA, spe-cial somatic afferent; SVA, specialvisceral afferent; SVE, special vis-ceral efferent.
BL2eBlum12.qxd 2/16/10 12:12 PM Page 501
Prima Eriawan Putra 1102012212 3
The first neuron of the olfactory pathway is the bipolar ol- factory cell; the second neurons are the mitral and tufted cells of the olfactory bulb. The neurites of these cells form the olfactory tract (2nd neuron), which lies adjacent to and just below the frontobasal (orbitofrontal) cortex. The ol- factory tract divides into the lateral and medial olfactory striae in front of the anterior perforated substance; another portion of it terminates in the olfactory trigone, which also lies in front of the anterior perforated substance. The fibers of the lateral stria travel by way of the limen insulae to the amygdala, semilunar gyrus, and ambient gyrus (prepyriform area). This is the site of the 3rd neuron, which projects to the anterior portion of the parahippocampal gyrus (Brod- mann area 28, containing the cortical projection fields and association area of the olfactory system). The fibers of the medial stria terminate on nuclei of the septal area below the genu of the corpus callosum (subcallosal area) and in front of the anterior commissure. Fibers emerging from these nuclei project, in turn, to the opposite hemisphere and to the limbic system. The olfactory pathway is the only sensory pathway that reaches the cerebral cortex without going through a relay in the thalamus. Its central connections are complex and still incompletely known.
Cranial Nerve II: Optic Nerves The optic nerve carries visual information from the retina to the lateral geniculate nucleus of the thalamus and to the extrageniculate pathways. The retinal ganglion cells are actually part of the central nervous system, so the optic nerves are, strictly speaking, tracts and not nerves. Nevertheless, by widely accepted convention the portion of the visual pathway in front of the optic chiasm is called the optic nerve, and beyond this point it is referred to as the optic tract. The optic nerves travel from the orbit to the intracranial cavity via the optic canal
4129
Subcallosal area
Medial olfactorystria
Striae medullaresof the thalamus
Longitudinal striae
Habenulo-interpedun-
cular tract
Habenularnucleus
Inter-peduncular
nucleus
Medialforebrain
bundle
Tegmentalnuclei
Dorsallongitudinal
fasciculus
Reticularformation
Prepiriformarea
Area 28(entorhinalarea)
Uncus withamygdaloid body
Lateralolfactorystria
Olfactory epithelium
Olfactory bulb
bipolar olfactory cells
Olfactory bulb Olfactory tract
Temporal pole
Prepiriformarea
Amygdaloidbody
Diagonalband ofBroca
Uncus
Semilunargyrus
Ambient gyrus
Anteriorperforated substance
Medial olfactorystria
Limen insulae
Lateral olfactorystria
Fig. 4.7 The olfactory nerve and tract and the olfactory pathway
Fig. 4.8 The olfactory nerve and tract as seen from below
Cranial Nerves
Baehr, Duus' Topical Diagnosis in Neurology 2005 ThiemeAll rights reserved. Usage subject to terms and conditions of license.
Prima Eriawan Putra 1102012212 4
Visual information is transmitted centrally as follows. An object located in the left visual field gives rise to images on the nasal half of the left retina and the temporal half of the right retina. Optic nerve fibers derived from the nasal half of the left retina cross to the left side in the optic chiasm to join the fibers from the temporal half of the right retina in the right optic tract. These fibers then pass to a relay station in the right lateral geniculate body, and then by way of the right optic radiation into the right visual cortex. The right visual cortex is thus re- sponsible for the perception of objects in the left visual field; in analogous fash- ion, all visual impulses relating to the right visual field are transmitted through the left optic tract and radiation into the left visual cortex
Cranial Nerve III, IV, VI (Oculomotor, Trochlear, Abducens Nerves) These nerves, which are responsible for controlling the extraocular muscles, will be discussed in detail in Chapter 13. Briefly, CN VI abducts the eye later- ally in the horizontal direction; CN IV acts through a trochlea, or pulley-like, structure in the orbit, to rotate the top of the eye medially and move it down- ward; and CN III subserves all other eye movements. The oculomotor (CN III) and trochlear (CN IV) nuclei are located in the midbrain, and the abducens (CN VI) nucleus is in the pons (see Figures 12.5, 14.3, and 14.4C). Recall that CN III exits the brainstem ventrally in the interpeduncular fossa, CN IV exits dorsally from the inferior tectum, and CN VI exits ventrally at the pontomedullary junc- tion (see Figure 12.2). CN III, IV, and VI then traverse the cavernous sinus (see Figure 13.11), and exit the skull via the superior orbital fissure (see Figure 12.3A,C; Table 12.2) to reach the muscles of the orbit. CN III also carries parasympathetics to the pupillary constrictor and to the ciliary muscle of the lens. The preganglionic parasympathetic neurons are located in the EdingerWest- phal nucleus in the midbrain (see Figure 12.5). They synapse in the ciliary gan- glion located in the orbit (Figure 12.6). Postganglionic parasympathetic fibers then continue to the pupillary constrictor and ciliary muscles.
28 Visual pathways
296
ON
OT
OR
OT
OC
SC
PVC
LGB
ON
OR
Shield
Left eye
Meyers loop
Target cortex ofMeyers loop
Figure 28.10 Pathway from the visual field of the left eye to the primary visual cortex. T denotes the temporal (outer) half of the left visual field; N denotes the nasal (inner) half of the left visual field.
In the left retina and optic nerve (ON), the neural representation of the image is reversed side to side. It is also inverted top to bottom. The right retina and optic nerve are inactive because this eye is shielded.
At the optic chiasm (OC) the axons forming the nasal half of the left optic nerve cross the midline and form the medial half of the right optic tract (OT). Those forming the lateral half of the nerve form the lateral half of the left optic tract. Each set synapses in the corresponding lateral geniculate body (LGB).
The optic radiations (OR) are fan-like (cf. Figure 28.7), with the axons carrying the foveal input initially in the middle of the fan.As they approach the occipital pole, the foveal axons (red) in both hemispheres move to the back and enter the posterior part
of the primary visual cortex (PVC). Note the striped pattern of delivery to the cortex on both sides. The blank intervals between are the same width and contain the axons and cortex responsible for the visual field of the right eye. SC, superior colliculus.
Prima Eriawan Putra 1102012212 5
The nuclei of the oculomotor and trochlear nerves lie in the midbrain teg- mentum, while the nucleus of the abducens nerve lies in the portion of the pontine tegmentum underlying the floor of the fourth ventricle.
Cranial Nerve V: Trigeminal Nerve
The name trigeminal was given to this nerve because it has three major branches: the ophthalmic division (V1), maxillary division (V2), and mandibular division (V3) (Figure 12.7). The trigeminal nerve provides sensory innervation to the face and should be distinguished from the facial nerve, which controls the muscles of facial expression
506 Chapter 12
KEY CLINICAL CONCEPT
12.1 ANOSMIA (CN I)Patients with unilateral anosmia, or olfactory loss, are rarely aware of thedeficit because olfaction in the contralateral nostril can compensate. There-fore, when testing olfaction, the examiner must test each nostril separately(see neuroexam.com Video 24). Patients are often aware of bilateral anosmiaand may complain of decreased taste because of the important contributionof olfaction to the perception of flavor.
Loss of the sense of smell can be caused by head trauma, which damagesthe olfactory nerves as they penetrate the cribriform plate of the ethmoid. Inaddition, viral infections can damage the olfactory neuroepithelium. Ob-struction of the nasal passages can impair olfaction. Bilateral anosmia is alsocommon in patients with certain neurodegenerative conditions such asParkinsons disease and Alzheimers disease.
Intracranial lesions that occur at the base of the frontal lobes near the olfac-tory sulci can interfere with olfaction. Possible lesions in this location includemeningioma, metastases, basal meningitis or less commonly, sarcoidosis, a gran-ulomatous inflammatory disorder that occasionally involves the nervous sys-tem, often causing cranial neuropathies. As we will discuss in KCC 19.11, frontallobe deficits are often difficult to detect clinically, especially with small lesions.Therefore, lesions at the base of the frontal lobes can sometimes grow to a verylarge size, causing little obvious dysfunction other than anosmia. Large lesionsof the olfactory sulcus region (typically meningiomas) can also sometimes pro-duce a condition called Foster Kennedy syndrome, in which there is anosmia to-gether with optic atrophy in one eye (caused by ipsilateral tumor compression)and papilledema in the other eye (caused by elevated intracranial pressure).!
CN II: Optic Nerve
FUNCTIONAL CATEGORY FUNCTION
Special somatic sensory Vision
As we discussed in Chapter 11, the optic nerve carries visual informationfrom the retina to the lateral geniculate nucleus of the thalamus and to theextrageniculate pathways (see Figures 11.6, 11.15, and 12.2A). The retinalganglion cells are actually part of the central nervous system, so the opticnerves are, strictly speaking, tracts and not nerves. Nevertheless, by widelyaccepted convention the portion of the visual pathway in front of the opticchiasm is called the optic nerve, and beyond this point it is referred to as theoptic tract. The optic nerves travel from the orbit to the intracranial cavityvia the optic canal (see Figure 12.3A,C; Table 12.2). The anatomy and disor-ders of visual pathways are discussed in greater detail in Chapter 11.
CN III, IV, and VI: Oculomotor, Trochlear, and Abducens Nerves
NERVE FUNCTIONALCATEGORY FUNCTION
CN III Somatic Levator palpebrae superior and all extraocularmotor muscles, except for superior oblique and lateral
rectusParasym- Parasympathetics to pupil constrictor and ciliary
pathetic muscles for near visionCN IV Somatic motor Superior oblique muscle; causes depression motor
and intorsion of the eyeCN VI Somatic motor Lateral rectus muscle; causes abduction of the eye
Olfaction
BL2eBlum12.qxd 2/16/10 12:12 PM Page 506
Brainstem I: Surface Anatomy and Cranial Nerves 507
These nerves, which are responsible for controlling the extraocular muscles,will be discussed in detail in Chapter 13. Briefly, CN VI abducts the eye later-ally in the horizontal direction; CN IV acts through a trochlea, or pulley-like,structure in the orbit, to rotate the top of the eye medially and move it down-ward; and CN III subserves all other eye movements. The oculomotor (CN III)and trochlear (CN IV) nuclei are located in the midbrain, and the abducens (CNVI) nucleus is in the pons (see Figures 12.5, 14.3, and 14.4C). Recall that CN IIIexits the brainstem ventrally in the interpeduncular fossa, CN IV exits dorsallyfrom the inferior tectum, and CN VI exits ventrally at the pontomedullary junc-tion (see Figure 12.2). CN III, IV, and VI then traverse the cavernous sinus (seeFigure 13.11), and exit the skull via the superior orbital fissure (see Figure12.3A,C; Table 12.2) to reach the muscles of the orbit. CN III also carriesparasympathetics to the pupillary constrictor and to the ciliary muscle of the lens.The preganglionic parasympathetic neurons are located in the EdingerWest-phal nucleus in the midbrain (see Figure 12.5). They synapse in the ciliary gan-glion located in the orbit (Figure 12.6). Postganglionic parasympathetic fibersthen continue to the pupillary constrictor and ciliary muscles.
Other cranial nerve parasympathetics are also summarized in Figure 12.6.
Pupillaryconstrictor
Otic ganglion
Sphenopalatineganglion
Ciliaryganglion
CN III
CN IX
CN X
EdingerWestphalnucleus
Superiorsalivatory nucleus
Greater petrosalnerve
Parotid gland
Submandibular ganglion
Submandibular gland
Sublingual gland
Lesser petrosalnerve
Chorda tympani
Inferiorsalivatory nucleus
CN IX
CN X(to parasympatheticganglia of thoracoabdominalviscera)
Dorsal motornucleus of CN X
Lacrimal glands
CN VII
Ciliary muscleof lens
FIGURE 12.6 Summary of CranialNerve Parasympathetic Pathways
BL2eBlum12.qxd 2/16/10 12:12 PM Page 507
508 Chapter 12
CN V: Trigeminal Nerve
FUNCTIONAL CATEGORY FUNCTION
General somatic sensory Sensations of touch, pain, temperature, joint position,and vibration for the face, mouth, anterior two-thirds of tongue, nasal sinuses, and meninges
Branchial motor Muscles of mastication and tensor tympani muscle
The name trigeminal was given to this nerve because it has three majorbranches: the ophthalmic division (V1), maxillary division (V2), and mandibulardivision (V3) (Figure 12.7). The trigeminal nerve provides sensory innervationto the face and should be distinguished from the facial nerve, which controlsthe muscles of facial expression. The trigeminal nerve also has a small
Trigeminal ganglionin Meckels cave
Trigeminalsensory nuclei
Trigeminalmotor nucleus
Temporalismuscle
V1
V2
C2
C3
Superior orbital fissure
(A)
(ophthalmic)
(maxillary)
MassetermuscleMassetermuscle
Tensor tympanimuscle
Foramenrotundum
Foramenovale
Anterior belly ofdigastric muscle
Motor root of CN V
(B)
V1
V2
V3
C3
CN VII, IX, X
C2
V3(mandibular)
FIGURE 12.7 Trigeminal Nerve (CN V)(A) Summary of trigeminal sensory andmotor pathways. (B) General somaticsensory innervation to the face is pro-vided by the trigeminal nerve as well asby CN VII, IX, and X. These inputs alltravel to the trigeminal nuclei (see Figure12.8). The occiput and neck, on the otherhand, are supplied by cervical nerveroots C2 and C3. Sensory innervation ofthe supratentorial dura is provided byCN V (not shown).
BL2eBlum12.qxd 2/16/10 12:12 PM Page 508
Prima Eriawan Putra 1102012212 6
Trigeminal somatosensory functions
The trigeminal nuclei (Figure 12.8 and Figure 12.9) receive general somatic sen- sory inputs from CN V and other cranial nerves (see Table 12.3). The main in- puts are carried by CN V and, as we just mentioned, provide sensation for the face, mouth, anterior two-thirds of the tongue, nasal sinuses, and supratentor- ial dura. Smaller inputs from CN VII, IX, and X provide sensation for part of the external ear (see Figure 12.7B; Table 12.4). In addition, CN IX provides sen- sation to the middle ear, posterior one-third of the tongue, and pharynx. CN X additionally provides sensation for the infratentorial dura and probably also contributes to pharyngeal sensation (see Table 12.4).
Trigeminal motor functions
The trigeminal motor nucleus mediates the branchial motor functions of the trigeminal nerve (see Figure 12.7). This nucleus is located in the upper-to- mid pons (see Figures 12.5 and 14.4B), near the level where the trigeminal nerve exits the brainstem. The branchial motor root of the trigeminal nerve runs inferomedial to the trigeminal ganglion along the floor of Meckels cave and then joins V3 to exit via the foramen ovale (see Figure 12.3A). It then supplies the muscles of mastication (see neuroexam.com Video 38), including the masseter, temporalis, and medial and lateral pterygoid muscles, as well as several smaller muscles, such as the tensor tympani, tensor veli palatini, mylohyoid, and anterior belly of the digastric. The upper motor neuron con- trol reaching the trigeminal motor nucleus is predominantly bilateral, so uni- lateral lesions in the motor cortex or corticobulbar tract usually cause no deficit in jaw movement. Bilateral upper motor neuron lesions, however, can cause hyperreflexia manifested in a brisk jaw jerk reflex
508 Chapter 12
CN V: Trigeminal Nerve
FUNCTIONAL CATEGORY FUNCTION
General somatic sensory Sensations of touch, pain, temperature, joint position,and vibration for the face, mouth, anterior two-thirds of tongue, nasal sinuses, and meninges
Branchial motor Muscles of mastication and tensor tympani muscle
The name trigeminal was given to this nerve because it has three majorbranches: the ophthalmic division (V1), maxillary division (V2), and mandibulardivision (V3) (Figure 12.7). The trigeminal nerve provides sensory innervationto the face and should be distinguished from the facial nerve, which controlsthe muscles of facial expression. The trigeminal nerve also has a small
Trigeminal ganglionin Meckels cave
Trigeminalsensory nuclei
Trigeminalmotor nucleus
Temporalismuscle
V1
V2
C2
C3
Superior orbital fissure
(A)
(ophthalmic)
(maxillary)
MassetermuscleMassetermuscle
Tensor tympanimuscle
Foramenrotundum
Foramenovale
Anterior belly ofdigastric muscle
Motor root of CN V
(B)
V1
V2
V3
C3
CN VII, IX, X
C2
V3(mandibular)
FIGURE 12.7 Trigeminal Nerve (CN V)(A) Summary of trigeminal sensory andmotor pathways. (B) General somaticsensory innervation to the face is pro-vided by the trigeminal nerve as well asby CN VII, IX, and X. These inputs alltravel to the trigeminal nuclei (see Figure12.8). The occiput and neck, on the otherhand, are supplied by cervical nerveroots C2 and C3. Sensory innervation ofthe supratentorial dura is provided byCN V (not shown).
BL2eBlum12.qxd 2/16/10 12:12 PM Page 508
Prima Eriawan Putra 1102012212 7
Cranial Nerve VII: Facial Nerves
The main function of the facial nerve is to control the muscles of facial ex- pression (see neuroexam.com Video 40); however, it has several other impor- tant functions as well. The main nerve trunk carries the branchial motor fibers controlling facial expression, while a smaller branch called the nervus intermedius carries fibers for the parasympathetic (tears and salivation), vis- ceral sensory (taste), and general somatosensory functions (Figure 12.10; see also Figures 12.6 and 12.14).
The facial nucleus is located in the branchial motor column, more caudally in the pons than the trigeminal motor nucleus (see Figure 12.5; see also Figure 14.4B,C). The fascicles of the facial nerve loop dorsally around the abducens nucleus, forming the facial colliculus on the floor of the fourth ventricle
Brainstem I: Surface Anatomy and Cranial Nerves 513
CN VII: Facial Nerve
FUNCTIONAL CATEGORY FUNCTION
Branchial motor Muscles of facial expression, stapedius muscle, and part of digastric muscle
Parasympathetic Parasympathetics to lacrimal glands, and to sublingual, submandibular, and all other salivary glands except parotid
Visceral sensory (special) Taste from anterior two-thirds of tongueGeneral somatic sensory Sensation from a small region near the external
auditory meatus
The main function of the facial nerve is to control the muscles of facial ex-pression (see neuroexam.com Video 40); however, it has several other impor-tant functions as well. The main nerve trunk carries the branchial motorfibers controlling facial expression, while a smaller branch called the nervusintermedius carries fibers for the parasympathetic (tears and salivation), vis-ceral sensory (taste), and general somatosensory functions (Figure 12.10; seealso Figures 12.6 and 12.14).
The facial nucleus is located in the branchial motor column, more caudally inthe pons than the trigeminal motor nucleus (see Figure 12.5; see also Figure14.4B,C). The fascicles of the facial nerve loop dorsally around the abducensnucleus, forming the facial colliculus on the floor of the fourth ventricle (see Fig-ure 12.2B and Figure 12.11). The nerve then exits the brainstem ventrolaterallyat the pontomedullary junction (see Figure 12.2A,C). Upper motor neuron con-trol of the facial nucleus is discussed in KCC 12.3 (see Figure 12.13). Briefly, le-sions in the cortex or corticobulbar tracts cause contralateral face weakness thatspares the forehead, while lesions of the facial nucleus, nerve fascicles in thebrainstem, or peripheral nerve cause ipsilateral weakness of the entire face.
The facial nerve exits the brainstem ventrolaterally at the pontomedullaryjunction, lateral to CN VI in a region called the cerebellopontine angle (see Fig-ure 12.2A,C). It then traverses the subarachnoid space and enters the internalauditory meatus (see Figure 12.3A; see also Figure 4.13C) to travel in the audi-tory canal of the petrous temporal bone together with the vestibulocochlearnerve (see Figure 12.14). At the genu of the facial nerve, the nerve takes a turnposteriorly and inferiorly in the temporal bone to run in the facial canal, justmedial to the middle ear (see Figures 12.10 and 12.14). The geniculate ganglionlies in the genu and contains primary sensory neurons for taste sensation inthe anterior two-thirds of the tongue, and for general somatic sensation in aregion near the external auditory meatus (see Table 12.5; Figure 12.7B). Themain portion of the facial nerve exits the skull at the stylomastoid foramen (seeFigures 12.3B and 12.10). It then passes through the parotid gland and dividesinto five major branchial motor branches to control the muscles of facial ex-pression: the temporal, zygomatic, buccal, mandibular, and cervical branches(see Figure 12.10). Other smaller branchial motor branches innervate thestapedius (see Figures 12.10 and 12.15), occipitalis, posterior belly of the digas-tric, and stylohyoid muscles. The cranial nerves controlling the middle earmuscles can be recalled by the mnemonic Trigeminal for Tensor Tympani andSeventh for Stapedius. Both the tensor tympani and the stapedius dampenmovements of the middle ear ossicles (see the section on CN VIII later in thischapter), providing feedback modulation of acoustic signal intensity.
The preganglionic parasympathetic fibers of the facial nerve originate in thesuperior salivatory nucleus (see Figure 12.10) and are carried by two smallbranches off the main trunk of the facial nerve. The greater petrosal nerve takesoff at the genu of the facial nerve (see Figure 12.14) to reach the sphenopalatine
Facial muscles
MNEMONIC
BL2eBlum12.qxd 2/16/10 12:12 PM Page 513
514 Chapter 12
(pterygopalatine) ganglion, where postganglionic parasympathetic cells projectto the lacrimal glands and nasal mucosa (see Figure 12.10). The chorda tympanileaves the facial nerve just before the stylomastoid foramen and travels backupward to traverse the middle ear cavity before exiting the skull at thepetrotympanic fissure (see Figures 12.3B and 12.10), just medial and posterior tothe temporomandibular joint. The chorda tympani then joins the lingual nerve(a branch of CN V3) to reach the submandibular ganglion (also called the sub-maxillary ganglion), where postganglionic parasympathetics arise to supplythe submandibular (submaxillary) and sublingual salivary glands as well asother minor salivary glands aside from the parotid. Note that the majority(~70%) of saliva production arises from the submandibular salivary glands.
The lingual nerve and chorda tympani also carry special visceral sensoryfibers mediating taste sensation (see neuroexam.com Video 41) for the ante-rior two-thirds of the tongue (see Figure 12.10). The primary sensory tastefibers have their cell bodies in the geniculate ganglion (Figure 12.12; see alsoFigure 12.14 and Table 12.5). These cells synapse onto secondary sensory
Sphenopalatineganglion
Sublingualgland
Submandibulargland
Submandibularganglion
Lacrimalglands
Taste, anterior2/3 of tongue
Greater petrosalnerve
Stapediusmuscle
GeniculateganglionGeniculateganglion
Internalacousticmeatus
Nervusintermedius
Superior salivatorynucleus
Mandibular branchMandibular branch
Cervical branchCervical branch
Buccal branchBuccal branch
Zygomatic branchZygomatic branch
TemporalbranchTemporalbranch
Chorda tympani
Facial nucleus
Nucleus solitarius
Spinal trigeminalnucleus
Stylomastoidforamen
Petrotympanicfissure
Lingual nerve
Posterior auricularbranch
FIGURE 12.10 Facial Nerve(CN VII) Summary of facialnerve sensory and motorpathways.
Taste
BL2eBlum12.qxd 2/16/10 12:12 PM Page 514
Prima Eriawan Putra 1102012212 8
Facial Nerve Lesion
Cranial Nerve VIII: Vestibulocochlear Nerves This nerve carries the special somatic sensory functions of hearing and vestibu- lar sense from the structures of the inner ear. The vestibulocochlear nerve exits the brainstem at the pontomedullary junction just lateral to the facial nerve, in a region called the cerebellopontine angle
Auditory informa- tion throughout these pathways is tonotopically organized. Primary sensory neurons in the spiral ganglion send their axons in the cochlear division of CN VIII to reach the dorsal and ventral cochlear nuclei, which are wrapped around the lateral aspect of the inferior cerebellar peduncle at the pontomedullary junc- tion (see Figures 12.16 and 12.17C). The hearing pathways then ascend through the brainstem bilaterally through a series of relays to reach the inferior colliculi, medial geniculate nuclei, and, ultimately, the auditory cortex. Because auditory information from each ear ascends bilaterally in the brainstem, with decussations oc- curring at multiple levels, unilateral hearing loss is not seen in le- sions in the central nervous system proximal to the cochlear nuclei.
Brainstem I: Surface Anatomy and Cranial Nerves 517
tion, patients may suffer from dry eye, resulting from decreased lacrimationwith parasympathetic involvement (see Figure 12.10). Neurologic examinationis notable for unilateral lower motor neurontype facial weakness, sometimesassociated with loss of taste on the ipsilateral tongue (test with mustard orsugar applied with a cotton swab; see neuroexam.com Video 41). The remain-der of the exam should be normal in Bells palsy. The presence of hand weak-ness, sensory loss, dysarthria, or aphasia suggests an upper motor neuron le-sion. In clinically typical cases, imaging studies are usually normal, however,most practitioners will order an MRI scan to exclude a structural lesion andblood studies including a blood count, glucose, and Lyme titer.
Treatment of Bells palsy has been controversial, but recent evidence sug-gests that a 10-day course of oral steroids started soon after onset improveschances for full recovery. The possible role of antiviral agents in treating Bellspalsy remains uncertain. Incomplete eye closure and decreased tearing cancause corneal ulcerations. Therefore, patients should be given lubricating eye-drops and instructions to tape the eye shut at night. About 80% of patients re-cover fully from Bells palsy within 3 weeks, although some are left with vari-able degrees of residual weakness. During recovery, regenerating facial nerve
R L
R L
Region of weakness
R L
Contralateralprimary motorcortex
Ipsilateralprimary motorcortex
Lesion A
Lower motorneurontypefacial weakness
Lesion B
Pons
CN VII
Lower motorneuron
Upper motorneuron
A
B
Upper motorneurontypefacial weakness
FIGURE 12.13 Upper Motor Neuron versus Lower MotorNeuron Facial Weakness With an upper motor neuron le-sion (Lesion A), the upper face is spared because both hemi-spheres contribute to movement of the upper face, and the unaffected hemisphere can compensate. With a lower motorneuron lesion (Lesion B), the entire face is affected on one side.
BL2eBlum12.qxd 2/16/10 12:12 PM Page 517
Prima Eriawan Putra 1102012212 9
Nervus Cranialis IX: Glossopharyngeal Nerves
The branchial motor portion of the nerve supplies one muscle, the sty- lopharyngeus (Figure 12.20), which elevates the pharynx during talking and swallowing and contributes (with CN X) to the gag reflex. The branchial motor component of CN IX arises from the nucleus ambiguus in the medulla. The general visceral sensory portion of the glossopharyngeal nerve con- veys inputs from baroreceptors and chemoreceptors in the carotid body. These aerents travel to the caudal nucleus solitarius of the medulla, also known as the cardiorespiratory nucleus (see Figure 12.20). Glossopharyngeal special visceral sensation mediates taste for the posterior one-third of the tongue, which reaches the rostral nucleus solitarius, or gustatory nucleus (see Figures 12.5, 12.12, and 12.20). General somatic sensory functions of CN IX are the sensation of touch, pain, and temperature from the posterior one- third of the tongue, pharynx, middle ear, and a region near the external au- ditory meatus
Brainstem I: Surface Anatomy and Cranial Nerves 521
nerve (see Figures 12.14 and 12.15). The hair cells of the cochlea, togetherwith their supporting cells, are called the organ of Corti. There is a tonotopicrepresentation determined by structural width and stiffness along the lengthof the organ of Corti such that higher-frequency sounds activate hair cellsnear the oval window, while lower-frequency sounds activate hair cells nearthe apex of the cochlea (see Figure 12.15).
Lets follow the pathways for hearing centrally, from the cochlear nuclei tothe primary auditory cortex (Figure 12.16 and Figure 12.17). Auditory informa-tion throughout these pathways is tonotopically organized. Primary sensoryneurons in the spiral ganglion send their axons in the cochlear division of CNVIII to reach the dorsal and ventral cochlear nuclei, which are wrapped aroundthe lateral aspect of the inferior cerebellar peduncle at the pontomedullary junc-tion (see Figures 12.16 and 12.17C). The hearing pathways then ascend through
Superior temporal gyrus
Heschls transversegyri (area 41)
Insula
CN VIII
Ventral cochlearnucleus
Superior olivarynuclear complex
Trapezoid body
Inferior cerebellarpeduncles
Lateral lemniscus
Brachium ofinferior colliculus
Medial geniculatenucleus (MGN)
Dorsalcochlearnucleus
Spiralganglioncells
A
B
C
Inferior colliculus Cochlea
FIGURE 12.16 Central Auditory Pathways Mainnuclei and pathways are shown from the cochlearnerve to the auditory cortex. Levels of sections for Figure 12.17 are indicated.
BL2eBlum12.qxd 2/16/10 12:12 PM Page 521
530 Chapter 12
CN IX: Glossopharyngeal Nerve
FUNCTIONAL CATEGORY FUNCTION
Branchial motor Stylopharyngeus muscleParasympathetic Parasympathetics to parotid glandGeneral somatic sensory Sensation from middle ear, region near the external
auditory meatus, pharynx, and posterior one-third of tongue
Visceral sensory (special) Taste from posterior one-third of tongueVisceral sensory (general) Chemoreceptors and baroreceptors of carotid body
The glossopharyngeal nerve was named for its role in sensation for the pos-terior tongue and pharynx; however, it has additional functions as well. Itexits the brainstem as several rootlets along the upper ventrolateral medulla,just below the pontomedullary junction and just below CN VIII, between theinferior olive and the inferior cerebellar peduncle (see Figure 12.2A,C). Thenerve traverses the subarachnoid space to exit the skull via the jugular fora-men (see Figure 12.3A,B; Table 12.2).
The branchial motor portion of the nerve supplies one muscle, the sty-lopharyngeus (Figure 12.20), which elevates the pharynx during talking andswallowing and contributes (with CN X) to the gag reflex. There is evidencethat the glossopharyngeal nerve may provide some innervation to otherpharyngeal muscles; however, most pharyngeal muscles are supplied pri-marily by the vagus (see the next section). The branchial motor componentof CN IX arises from the nucleus ambiguus in the medulla (see Figure 12.20).Ambiguus is Latin for ambiguous, and this name can be rememberedbecause the nucleus is difficult to discern on conventional stained sections(see Figure 14.5A,B). Parasympathetic preganglionic fibers in the glossopha-ryngeal nerve arise from the inferior salivatory nucleus in the pons (see Fig-ure 12.20). These parasympathetic fibers leave the glossopharyngeal nervevia the tympanic nerve and then join the lesser petrosal nerve to synapse inthe otic ganglion, providing postganglionic parasympathetics to the parotidgland.
The general visceral sensory portion of the glossopharyngeal nerve con-veys inputs from baroreceptors and chemoreceptors in the carotid body.These afferents travel to the caudal nucleus solitarius of the medulla, alsoknown as the cardiorespiratory nucleus (see Figure 12.20). Glossopharyngealspecial visceral sensation mediates taste for the posterior one-third of thetongue, which reaches the rostral nucleus solitarius, or gustatory nucleus (seeFigures 12.5, 12.12, and 12.20). General somatic sensory functions of CN IXare the sensation of touch, pain, and temperature from the posterior one-third of the tongue, pharynx, middle ear, and a region near the external au-ditory meatus (see Figure 12.7B). The glossopharyngeal nerve has two sen-sory ganglia located within or just below the jugular foramen (see Table12.5). General and special visceral sensation are conveyed by primary sen-sory neurons in the inferior (petrosal) glossopharyngeal ganglion. General so-matic sensation is conveyed by primary sensory neurons in both the inferiorand superior (jugular) glossopharyngeal ganglion.
MNEMONIC
REVIEW EXERCISEWhich cranial nerve contributes tothe greater petrosal nerve? Whichcontributes to the lesser petrosalnerve? (See Figure 12.6.)
BL2eBlum12.qxd 2/16/10 12:12 PM Page 530
Prima Eriawan Putra 1102012212 10
Nervus Cranialis X: Vagus Nerves
The largest part of the vagus nerve provides parasympathetic innervation to the heart, lungs, and digestive tract, extending nearly to the splenic flexure (see Figures 6.13 and 12.21). Parasympathetic preganglionic fibers arise from the dorsal motor nucleus of CN X, which runs from the rostral to the caudal medulla (see Figure 14.5A,B). The dorsal motor nucleus of CN X forms the vagal trigone on the floor of the fourth ventricle, just lateral to the hypoglos- sal trigone, near the obex (see Figure 12.2B).
The branchial motor component of the vagus (Figure 12.21) controls nearly all pharyngeal and upper esophageal muscles (swallowing and gag reflex) and the muscles of the larynx (voice box). The nucleus ambiguus supplies branchial motor fibers that travel in the vagus nerve to the muscles of the palate, pharynx, upper esophagus, and larynx, and in the glossopharyngeal nerve (CN IX) to the stylopharyngeus (see Figure 12.20).
A branch of the vagus called the recurrent laryngeal nerve (see Figure 12.21) loops back upward from the thoracic cavity to control all intrinsic la- ryngeal muscles except for the cricothyroid, which is innervated by another branch of the vagus, the superior laryngeal nerve. The fibers in the recurrent laryngeal nerve arise from the caudal portion of the nucleus ambiguus. After they exit the brainstem, these fibers travel briefly with CN XI before joining CN X (see the next section).
General somatic sensory fibers of the vagus (see Figure 12.21) supply the pharynx, larynx, meninges of the posterior fossa, and a small region near the external auditory meatus (see Figure 12.7B). Note that below the larynx and pharynx, conscious (general somatic) sensation from the viscera is carried by spinal, not cranial, nerves. However, unconscious, general visceral
Brainstem I: Surface Anatomy and Cranial Nerves 531
Oticganglion
Carotid sinus
Carotid body
Parotid gland
Inferior salivatorynucleus
Superiorglosso-pharyngealganglion
Rostralnucleus solitarius(gustatory nucleus)
Caudal nucleussolitarius(cardiorespiratorynucleus)
Lesserpetrosalnerve
Inferiorglosso-pharyngealganglion Spinal trigeminal
nucleus
Nucleus ambiguus
Sensation from middleear and external ear
Sensation frompharynx and posteriorone-third of tongue
Stylopharyngeus muscle
Jugular foramen
Taste, posteriorone-third of tongue
CN IX
CN IX
FIGURE 12.20 Glossopharyngeal Nerve (CN IX)Summary of glossopharyngeal nerve sensory andmotor pathways.
BL2eBlum12.qxd 2/16/10 12:12 PM Page 531
532 Chapter 12 CN X: Vagus Nerve
FUNCTIONAL CATEGORY FUNCTION
Branchial motor Pharyngeal muscles (swallowing) and laryngeal muscles (voice box)
Parasympathetic Parasympathetics to heart, lungs, and digestive tractdown to the splenic flexure
General somatic sensory Sensation from pharynx, meninges, and a small region near the external auditory meatus
Visceral sensory (special) Taste from epiglottis and pharynxVisceral sensory (general) Chemoreceptors and baroreceptors of the aortic arch
The vagus nerve derives its name from the wandering course it takes in pro-viding parasympathetic innervation to organs throughout the body(vagus means wandering in Latin). Other important functions are alsoserved by the vagus, as we will discuss here. The vagus nerve exits the ven-trolateral medulla as several rootlets just below CN IX, between the inferiorolive and the inferior cerebellar peduncle (see Figure 12.2A,C). It crosses thesubarachnoid space and then leaves the cranial cavity via the jugular fora-men (see Figures 12.3A,B and 12.21).
The largest part of the vagus nerve provides parasympathetic innervationto the heart, lungs, and digestive tract, extending nearly to the splenic flexure(see Figures 6.13 and 12.21). Parasympathetic preganglionic fibers arise fromthe dorsal motor nucleus of CN X, which runs from the rostral to the caudalmedulla (see Figure 14.5A,B). The dorsal motor nucleus of CN X forms thevagal trigone on the floor of the fourth ventricle, just lateral to the hypoglos-sal trigone, near the obex (see Figure 12.2B). Postganglionic parasympatheticneurons innervated by the vagus are found in terminal ganglia located withinor near the effector organs. Recall that parasympathetics to the gastrointesti-nal tract beyond the splenic flexureand to the urogenital systemare pro-vided by parasympathetic nuclei in the sacral spinal cord (see Figure 6.13).
The branchial motor component of the vagus (Figure 12.21) controls nearlyall pharyngeal and upper esophageal muscles (swallowing and gag reflex)and the muscles of the larynx (voice box). The nucleus ambiguus suppliesbranchial motor fibers that travel in the vagus nerve to the muscles of thepalate, pharynx, upper esophagus, and larynx, and in the glossopharyngealnerve (CN IX) to the stylopharyngeus (see Figure 12.20).
A branch of the vagus called the recurrent laryngeal nerve (see Figure12.21) loops back upward from the thoracic cavity to control all intrinsic la-ryngeal muscles except for the cricothyroid, which is innervated by anotherbranch of the vagus, the superior laryngeal nerve. The fibers in the recurrentlaryngeal nerve arise from the caudal portion of the nucleus ambiguus. Afterthey exit the brainstem, these fibers travel briefly with CN XI before joiningCN X (see the next section). Some texts consider these caudal fibers of thenucleus ambiguus to be part of CN XI and refer to the caudal nucleus am-biguus as the cranial nucleus of CN XI. However, we include these fiberswith CN X because they spend the majority of their course traveling withCN X, not CN XI. Upper motor neuron innervation to the nucleus ambiguuscontrolling the voice and voluntary swallowing is from bilateral motor cor-tex (see Figure 6.2), except for the palate, which receives unilateral innerva-tion from the contralateral cortex (for example, see Case 6.5).
General somatic sensory fibers of the vagus (see Figure 12.21) supply thepharynx, larynx, meninges of the posterior fossa, and a small region near theexternal auditory meatus (see Figure 12.7B). Note that below the larynx andpharynx, conscious (general somatic) sensation from the viscera is carried byspinal, not cranial, nerves. However, unconscious, general visceral sensationfrom chemoreceptors and baroreceptors of the aortic arch, cardiorespiratorysystem, and digestive tract is carried to the brainstem by the vagus nerve.
REVIEW EXERCISEList the branchial motor, parasympa-thetic, general somatic sensory, andvisceral sensory functions of CN IXand CN X. Name the nucleus sub-serving each function. (See Figures12.20 and 12.21.)
BL2eBlum12.qxd 2/16/10 12:12 PM Page 532
Prima Eriawan Putra 1102012212 11
sensation from chemoreceptors and baroreceptors of the aortic arch, cardiorespiratory system, and digestive tract is carried to the brainstem by the vagus nerve.
Cranial Nerve XI: Accessory Nerves The spinal accessory nucleus (also known as the accessory spinal nu- cleus) protrudes laterally between the dorsal and ventral horns of the spinal cord central gray matter (see Figure 14.5D), providing branchial motor* fibers to this nerve. CN XI then exits the cranium again via the jugular foramen to supply the sternomastoid and upper portions of the trapezius muscle. The sternomastoid muscle turns the head toward the opposite side, and the trapezius is involved in elevating the shoulder. The lower portions of the trapez- ius are usually supplied mainly by cervical nerve roots C3 and C4.
Cranial Nerve XII: Hypoglossal Nerves
The hypoglossal nerve exits the ventral medulla as multiple rootlets be- tween the pyramid and inferior olivary nucleus (see Figure 12.2A,C). This nerve exits through its own foramen, the hypoglossal foramen (see Figure 12.3A,B), and provides somatic motor innervation to all intrinsic and extrin- sic tongue muscles except for the palatoglossus, which is supplied by CN X (see neuroexam.com Video 47). The hypoglossal nucleus is located near the midline on the floor of the fourth ventricle in the medulla (see Figure 14.5A,B), forming the hypoglossal trigone, just medial to the dorsal nucleus of CN X (see Figures 12.2B, 12.4B, and 12.5).
1.2. Jaras Motorik
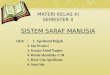
Functional mapping and lesion studies have demonstrated that the primary motor and somatosensory cortices are somatotopically organized (Figure 6.2). That is, adjacent regions on the cortex correspond to adjacent areas on the body surface. The cortical maps are classically depicted by a motor homunculus and a sensory homunculus (homunculus means little man in Latin)
Many of these general visceral afferents reach the caudal nucleus solitarius(cardiorespiratory nucleus; see Figures 12.5 and 14.5B). The vagus nerve alsocontains a small number of special visceral sensory fibers that carry taste sen-sation from the epiglottis and posterior pharynx to the rostral nucleus solitar-ius (gustatory nucleus) (see Figures 12.5 and 14.5A).
The primary sensory neuron cell bodies for CN X general and special vis-ceral sensation are located in the inferior (nodose) vagal ganglion (Table 12.5),located just below the jugular foramen. Cell bodies for general somatic sen-sation are located in both the inferior vagal ganglion and the superior (jugu-lar) vagal ganglion, which lies within or just below the jugular foramen.
Jugular foramen
Aortic archreceptors
To thoracoabdominalviscera (vagus nerve)
Recurrentlaryngealnerve
Superiorlaryngealnerve
Cricothyroidmuscle
Taste, epiglottis
Pharyngeal nerve(sensory andmotor plexus)
Soft palate
Sensation,meninges ofposterior fossa
Spinal trigeminalnucleus
Nucleus solitarius
Dorsal motornucleus of CN X
Nucleus ambiguus
Superior vagalganglion
Inferior vagalganglion
Sensation,external ear
CN X
FIGURE 12.21 Vagus (CN X)Summary of vagal sensory andmotor pathways.
Brainstem I: Surface Anatomy and Cranial Nerves 533
BL2eBlum12.qxd 2/16/10 12:12 PM Page 533
Prima Eriawan Putra 1102012212 12
Corticospinal Tract and Other Motor Pathways 225
Premotor cortex
Supplementarymotor area
Primary motorcortex
Central sulcus Primarysomatosensorycortex
Parietalassociationcortex
Secondarysomatosensoryarea (in parietaloperculum)
Supplementarymotor area
Primary motorcortex
Primarysomatosensorycortex
Parietalassociationcortex
(A)
(B)
66
65, 7
4
4 3, 1, 2
3,1,2
5, 7
FIGURE 6.1 Motor and Somatosen-sory Cortical Areas(A) Lateral view showing primary andassociation cortical areas of the sensoryand motor cortex and reciprocal connec-tions between these regions. Numbersindicate corresponding Brodmann areas(see Figure 2.15). (B) Medial view.
BL2eBlum06.qxd 2/12/10 8:42 AM Page 225
226 Chapter 6
somatotopic organization along their entire length, which can be traced fromone level to the next in the nervous system.
A useful generalization for remembering the somatotopic representationsis: The arms are medial to the legs with two exceptions: the primary sensorimotorcortices and the posterior columns (see, for example, Figures 6.2, 6.10, and 7.3).
Basic Anatomy of the Spinal CordThe spinal cord contains a butterfly-shaped central gray matter surrounded byascending and descending white matter columns, or funiculi (Figure 6.3A). Sen-sory neurons in the dorsal root ganglia have axons that bifurcate. One branchconveys sensory information from the periphery, and the other carries thisinformation through the dorsal nerve root filaments into the dorsal aspect ofthe spinal cord. The central gray matter has a dorsal (posterior) horn that is in-volved mainly in sensory processing, an intermediate zone that contains in-terneurons and certain specialized nuclei (Table 6.2), and a ventral (anterior)horn that contains motor neurons. Motor neurons send their axons out of thespinal cord via the ventral nerve root filaments. The spinal gray matter can alsobe divided into nuclei or, using a different nomenclature, into laminae namedby Bror Rexed (Figure 6.3B; see also Table 6.2), with different functions that
MNEMONIC
Leg
Hip
Neck
HeadArmElbow
ForeamHandFingersThumb
EyeNose
Face
Lips
Teeth
Gums
Tongue
Jaw
Pharynx
Abdome
n
Genitals Toes
Motor cortexSomatosensory cortex
Midline
Trunk Kne
e
Hip
Shou
lder
Arm
Elbo
w
Wris
tH
and
Fing
ers
Thum
b
Eye
Neck
Brow
Face
Lips
TonguePharynxLarynx
Jaw
Trun
k
Left Right
FIGURE 6.2 Somatosensory and Motor Homunculi Note that the size ofeach region of the homunculi is relatedto its importance in sensory or motorfunction, resulting in a distorted-appear-ing map (see also Figure 10.1).
REVIEW EXERCISEIs a patient with face and arm weak-ness more likely to have a lesion onthe lateral cortical surface or in theinterhemispheric fissure? Is a patientwith leg weakness more likely tohave a lesion on the lateral corticalsurface or in the interhemisphericfissure?
BL2eBlum06.qxd 2/12/10 8:42 AM Page 226
Prima Eriawan Putra 1102012212 13
Anatomy of Spinal Cord The spinal cord contains a butterfly-shaped central gray matter surrounded by ascending and descending white matter columns, or funiculi (Figure 6.3A). Sen- sory neurons in the dorsal root ganglia have axons that bifurcate. One branch conveys sensory information from the periphery, and the other carries this information through the dorsal nerve root filaments into the dorsal aspect of the spinal cord. The central gray matter has a dorsal (posterior) horn that is in- volved mainly in sensory processing, an intermediate zone that contains in- terneurons and certain specialized nuclei (Table 6.2), and a ventral (anterior) horn that contains motor neurons. Motor neurons send their axons out of the spinal cord via the ventral nerve root filaments. The spinal gray matter can also be divided into nuclei or, using a dierent nomenclature, into laminae named by Bror Rexed
Corticospinal Tract and Other Motor Pathways 227
we will discuss in this chapter and in Chapter7. The spinal cord white matter consists of dor-sal (posterior) columns, lateral columns, and ven-tral (anterior) columns (see Figure 6.3A).
The spinal cord does not appear the same atall levels (Figure 6.4). The white matter is thick-est in the cervical levels (see Figure 6.4C), wheremost ascending fibers have already entered thecord and most descending fibers have not yetterminated on their targets, while the sacral cordis mostly gray matter (see Figure 6.4F). In ad-dition, the spinal cord has two enlargements(see Figure 6.4A). The cervical enlargement andthe lumbosacral enlargement give rise to thenerve plexuses for the arms and legs. The spinalcord has more gray matter at the cervical andlumbosacral levels (see Figure 6.4C,E,F) than
(A)
Intermediate zone
Ventral (anterior) horn
Spinalnerve
Sensoryneuron
Ventral root(motor)
Dorsal root(sensory)
Motor neuron
Ventralcolumn
Dorsalcolumn
Dorsal (posterior) horn
Lateralcolumn
Dorsal rootganglion
I IIIII
IV
V
VI
VII
VIII
IX
(B)
Rexeds laminae:
Medial and lateralmotor nuclei
Nuclei:
Intermediatezone
Nucleusproprius
Substantiagelatinosa
Marginalzone
X
FIGURE 6.3 Basic Spinal CordAnatomy (A) Gray matter, white matter, and dorsal and ventral roots. (B) Spinal cord nuclei (left) and Rexedslaminae (right). (See also Table 6.2.) (B from DeArmond SJ, Fusco MM, May-nard MD. 1989. Structure of the HumanBrain: A Photographic Atlas. 3rd Ed. Ox-ford, New York.)
TABLE 6.2 Nuclei and Laminae of the Spinal Cord
REGION NUCLEI REXEDS LAMINAE
Dorsal horn Marginal zone IDorsal horn Substantia gelatinosa IIDorsal horn Nucleus proprius III, IVDorsal horn Neck of dorsal horn VDorsal horn Base of dorsal horn VIIntermediate zone Clarkes nucleus, VII
intermediolateral nucleusVentral horn Commissural nucleus VIIIVentral horn Motor nuclei IXGray matter Grisea centralis X
surrounding central canal
BL2eBlum06.qxd 2/12/10 8:42 AM Page 227
3 60
Precentral gyrus
From area 8
Caudatenucleus
(tail)
Thalamus
Lentiformnucleus
Internal capsule
Caudate nucleus (head)
Cortico-mesencephalic tract
Corticonuclear tract
Corticospinal(pyramidal) tract
Pyramid
Decussation of the pyramids
Anterior corticospinaltract (uncrossed)
Midbrain
Corticopontine tract
Cerebral peduncle( = crus cerebri)
Pons
Medulla
Lateral corticospinaltract (crossed)
Motor end plate
T
IIIIV
V
VI
VII
IXXXIIXI
C1
Multiform layer
Molecular layer
Externalgranular layer
Externalpyramidal layer
Internalgranular layer
Internalpyramidal layer
Fig. 3.3 Microarchitectureof the motor cortex(Golgi stain)
Fig. 3.4 Course of the pyramidal tract
3 Motor System
Baehr, Duus' Topical Diagnosis in Neurology 2005 ThiemeAll rights reserved. Usage subject to terms and conditions of license.
Prima Eriawan Putra 1102012212 14
Corticospinal Tract The corticospinal tractmore specifically, the lateral corticospinal tractis the most clinically important descending motor pathway in the nervous system. This pathway controls movement of the extremities, and lesions along its course produce characteristic deficits that often enable precise clinical localiza- tion. Because of its clinical importance, we will discuss the corticospinal tract in greater detail than the other descending motor systems.
Over half of the corticospinal tract fibers originate in the primary motor cor- tex (Brodmanns area 4) of the precentral gyrus. The remainder arise from the premotor and supplementary motor areas (area 6) or from the parietal lobe (ar- eas 3, 1, 2, 5, and 7) (Figure 6.9A). The primary motor cortex neurons contribut- ing to the corticospinal tract are located mostly in cortical layer 5 (see Figure 2.14B).
This tract originates in the motor cortex and travels through the cerebral white matter (corona radiata), the posterior limb of the internal capsule (where the fibers lie very close together), the central portion of the cerebral peduncle (crus cerebri), the pons, and the base (i.e., the anterior portion) of the medulla, where the tract is externally evident as a slight protrusion called the pyramid. The medullary pyramids (there is one on either side) give the tract its name. At the lower end of the medulla, 80-85% of the pyramidal fibers cross to the other side in the so-called decussation of the pyramids. The fibers that do not cross here descend the spinal cord in the ipsilateral anterior funiculus as the anterior corticospinal tract; they cross farther down (usually at the level of the segment that they supply) through the anterior commissure of the spinal cord (cf. Fig. 3.6). At cervical and thoracic levels, there are probably also a few fibers that remain uncrossed and innervate ipsilateral motor neurons in the anterior horn, so that the nuchal and truncal musculature receives a bilateral cortical inner- vation.
The majority of pyramidal tract fibers cross in the decussation of the py- ramids, then descend the spinal cord in the contralateral lateral funiculus as the lateral corticospinal tract. This tract shrinks in cross-sectional area as it travels down the cord, because some of its fibers terminate in each segment along the way. About 90 % of all pyramidal tract fibers end in synapses onto interneurons, which then transmit the motor impulses onward to the large motor neurons of the anterior horn, as well as to the smaller motor neurons
Corticospinal Tract and Other Motor Pathways 231
the spinal cord. Lateral motor systems travel in the lat-eral columns of the spinal cord and synapse on themore lateral groups of ventral horn motor neuronsand interneurons (Figure 6.7). Medial motor systemstravel in the anteromedial spinal cord columns tosynapse on medial ventral horn motor neurons andinterneurons.
The two lateral motor systems are the lateral corti-cospinal tract and the rubrospinal tract (Table 6.3). These
FIGURE 6.7 Somatotopic Organization of Medial and Lat-eral Motor System Projections to Anterior Horn Cells Lateralmotor systems (corticospinal and rubrospinal tracts) project to lateralanterior horn cells, while medial motor systems (anterior corticospinal,vestibulospinal, reticulospinal, and tectospinal tracts) project to medial an-terior horn cells. Lateral anterior horn cells control distal muscles of the ex-tremities, while medial anterior horn cells control proximal trunk muscles. (Spinal cord section from DeArmond SJ, Fusco MM, Maynard MD. 1989. Structure of the Human Brain: A Photographic Atlas. 3rd Ed. Oxford University Press, New York.)
TABLE 6.3 Lateral and Medial Descending Motor Systems
SITE OF DECUSSATION LEVELS OF TRACT SITE OF ORIGIN (WHERE RELEVANT) TERMINATION FUNCTION
LATERAL MOTOR SYSTEMS
Lateral corticospinal tract Primary motor cortex Pyramidal decussation, Entire cord (pre- Movement ofand other frontal and at the cervicomedullary dominantly at contralateral parietal areas junction cervical and limbs
lumbosacral enlargements)
Rubrospinal tract Red nucleus, Ventral tegmental decus- Cervical cord Movement ofmagnocellular sation, in the midbrain contralateral division limbs (function
is uncertain in humans)
MEDIAL MOTOR SYSTEMS
Anterior corticospinal tract Primary motor cortex Cervical and Control of and supplementary upper thoracic bilateral axial motor area cord and girdle
musclesVestibulospinal tracts Medial VST: medial Medial VST: Medial VST:
(VSTs)a and inferior vestibular Cervical and positioning ofnuclei; lateral VST: upper thoracic head and neck;lateral vestibular cord; Lateral lateral VST:nucleus VST: entire cord balance
Reticulospinal tracts Pontine and medullary Entire cord Automatic reticular formation posture and
gait-related movements
Tectospinal tract Superior colliculus Dorsal tegmental Cervical cord Coordination of decussation, in head and eye the midbrain movement
(uncertain in humans)
aDespite their names, both medial and lateral VSTs are medial motor systems.
Dorsal
Ventral
Medial motor systems
Anterior horncells for proximalmuscles
Anterior horncells for distalmuscles
Lateral motor systems
BL2eBlum06.qxd 2/12/10 8:42 AM Page 231
Prima Eriawan Putra 1102012212 15
Corticospinal Tract and Other Motor Pathways 233
Lateralgeniculatenucleus
Frontopontine and othercorticofugal fibers
Anterior thalamic radiation
Anterior limb
Corticospinal andcorticobulbar tractsCorticospinal andcorticobulbar tracts
6
3,1,2
5,7
4
Pyramid
Posterior limbof internal capsule
Basis pedunculi
(A)
(B)
Posterior limbCorticopontine and othercorticofugal fibers
Superior thalamic radiation(includes somatosensoryradiation)
Corticospinal tract
Auditory radiation(inferior thalamicpeduncle)
Optic radiation(posterior thalamicpeduncle)
Thalamus
Medialgeniculatenucleus
Head ofcaudatenucleus
Corticobulbartract
Genu
Glob
us
pallid
us
Putam
en
AT
L
F
Lateralcorticospinaltract (crossed)
Dorsal
Ventral
Pyramidal (motor) decussation
Anteriorcorticospinaltract (uncrossed)
Pyramidaldecussation
Pyramid
FIGURE 6.9 Internal Capsule (A) Three-dimensional representation of the internalcapsule. Corticospinal and corticobulbarfibers arising from the primary motor cor-tex and adjacent regions form part of the in-ternal capsule. Corticobulbar fibers projectto lower motor neurons in the brainstem.About 85% of corticospinal fibers cross overat the pyramidal decussation to form thelateral corticospinal tract, while the remain-ing fibers form the anterior corticospinaltract. (B) Horizontal section through inter-nal capsule showing the anterior limb,genu, and posterior limb in relation to thethalamus, head of the caudate, andlentiform nucleus (putamen and globus pal-lidus). Major fiber pathways of the internalcapsule are indicated.
BL2eBlum06.qxd 2/12/10 8:42 AM Page 233
Neuroanatomy Overview and Basic Definitions 33
Motor neurons that project from the cortex down to the spinal cord orbrainstem are referred to as upper motor neurons (UMNs). UMNs formsynapses onto the lower motor neurons (LMNs), which are located in the ante-rior horns of the central gray matter of the spinal cord (see Figure 2.16B) or inbrainstem motor nuclei. The axons of LMNs project out of the CNS via theanterior spinal roots or via the cranial nerves to finally reach muscle cells inthe periphery. Lesions affecting UMNs and LMNs have certain distinct clini-cal features, which we will learn about in Chapter 3.
(A) (B)
Precentral gyrus(motor cortex)
Primarymotor cortex
Posterior limbof internalcapsule
Pyramidaldecussation
Cervical
Thoracic
Lumbar
Sacral
Lateral corticospinal tract
Anterior horn
Skeletalmuscle
Upper motor neuron
Lower motor neuron
FIGURE 2.16 Overview of Cortico-spinal Tract (A) Pathway of upper mo-tor neuron from motor cortex to lowermotor neuron in contralateral spinalcord. (B) Representative sections throughthe cerebral cortex, pyramidal decussa-tion, and spinal cord showing corti-cospinal tract.
BL2e02.qxd 2/11/10 4:12 PM Page 33
Prima Eriawan Putra 1102012212 16
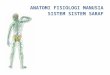
Corticonuclear (corticobulbar) Tract Some of the fibers of the pyramidal tract branch o from the main mass of the tract as it passes through the midbrain and then take a more dorsal course toward the motor cranial nerve nuclei (Figs. 3.4 and 4.54, p. 212). The fibers supplying these brainstem nuclei are partly crossed and partly uncrossed (for further details, cf. Chapter 4, section 4.4 Cranial Nerves). The nuclei receiving pyramidal tract input are the ones that mediate voluntary movements of the cranial musculature through cranial nerves V (the trigeminal nerve), VII (the facial nerve), IX, X, and XI (the glossopharyngeal, vagus, and accessory nerves), and XII (the hypoglossal nerve).
236 Chapter 6
Pons
Midbrain
Rostralmedulla
Cervicomedullaryjunction(decussation)
Spinal cord
Pyramid
Basispedunculi
Pyramidaldecussation Lateral cortico-
spinal tract
Internal capsule(posterior limb)
Cortex
(A) Lateral corticospinal tract
Basispontis
Pons
Midbrain
Rostralmedulla
Caudalmedulla
Spinal cord
Cortex
(B) Rubrospinal tract
Red nucleus(magnocellulardivision)
Ventral tegmentaldecussation
Lateral column
Lateral intermediatezone and lateralmotor nuclei
Lateral inter-mediate zoneand lateralmotor nuclei
BL2eBlum06.qxd 2/12/10 8:42 AM Page 236
Prima Eriawan Putra 1102012212 17
1.3. Jaras Sensorik
The term somatosensory generally refers to bodily sensations of touch, pain, tem- perature, vibration, and proprioception (limb or joint position sense). There are two main pathways for somatic sensation (see Table 7.1 and Figures 7.1 and 7.2):
The posterior columnmedial lemniscal pathway conveys proprioception, vibration sense, and fine, discriminative touch (see Figure 7.1).
The anterolateral pathways include the spinothalamic tract and other asso- ciated tracts that convey pain, temperature sense, and crude touch (see Figure 7.2). Since some aspects of touch sensation are carried by both pathways, touch sen- sation is not eliminated in isolated lesions to either pathway. Four types of sensory neuron fibers are classified according to axon diam- eter (Table 7.2). These dierent fiber types have specialized peripheral recep- tors that subserve dierent sensory modalities. Larger-diameter, myelinated axons conduct faster than smaller-diameter or unmyelinated axons. Sensory neuron cell bodies are located in the dorsal root ganglia (see Figures 7.1 and 7.2). Each dorsal root ganglion cell has
Corticospinal Tract and Other Motor Pathways 237
Pons
Midbrain
Medulla
Cervicalspinal cord
(C) Anterior corticospinal tract (D) Vestibulospinal tracts
Basispedunculi
Pyramid
Ventral column
Medial intermediate zoneand medial motor nuclei
Pons
Midbrain
Rostralmedulla
Cervicalspinal cord
Medialvestibularnucleus
Medialvestibulospinaltracts
Lateralvestibulospinaltract
Lateral vestibularnucleus
Medial intermediatezone and medialmotor nuclei
Cortex Cortex
FIGURE 6.11 Descending Motor Pathways Illustrated on this page, overleaf, andpage 238 (see also Table 6.3).
BL2eBlum06.qxd 2/12/10 8:42 AM Page 237
276 Chapter 7
IN CHAPTER 6, WE DISCUSSED the anatomy of the corticospinal tract and otherdescending motor pathways. In this chapter we will discuss the other twomajor long tracts of the nervous system (Table 7.1). These are the so-matosensory pathways: the posterior columnmedial lemniscal system and theanterolateral systems. Like the corticospinal tract, these pathways are somato-topically organized (see Figure 6.2). Understanding the functions and pointsof decussation of the three major long tracts (see Table 7.1) is fundamental toclinical neuroanatomical localization.
In the sections that follow, we will learn to use the anatomy of the three ma-jor long tracts to localize lesions in the nervous system. We will discuss com-mon disorders of the spinal cord and other locations that affect these pathways.In addition, brainstem and spinal cord mechanisms of pain modulation willbe addressed. The organization of the thalamus, serving as the major relayfor sensory and other information traveling to the cortex, will be reviewed aswell. Finally, we will discuss the roles of sensory and motor pathways in bowel,bladder, and sexual function.
Main Somatosensory PathwaysThe term somatosensory generally refers to bodily sensations of touch, pain, tem-perature, vibration, and proprioception (limb or joint position sense). There aretwo main pathways for somatic sensation (see Table 7.1 and Figures 7.1 and 7.2):
The posterior columnmedial lemniscal pathway conveys proprioception,vibration sense, and fine, discriminative touch (see Figure 7.1).
The anterolateral pathways include the spinothalamic tract and other asso-ciated tracts that convey pain, temperature sense, and crude touch (seeFigure 7.2).
Since some aspects of touch sensation are carried by both pathways, touch sen-sation is not eliminated in isolated lesions to either pathway.
Four types of sensory neuron fibers are classified according to axon diam-eter (Table 7.2). These different fiber types have specialized peripheral recep-tors that subserve different sensory modalities. Larger-diameter, myelinatedaxons conduct faster than smaller-diameter or unmyelinated axons.
Sensory neuron cell bodies are located in the dorsal root ganglia (see Figures7.1 and 7.2). Each dorsal root ganglion cell has a stem axon that bifurcates, re-sulting in one long process that conveys sensory information from the periph-
ery and a second process that carries informationinto the spinal cord through the dorsal nerve roots.A peripheral region innervated by sensory fibersfrom a single nerve root level is called a dermatome.The dermatomes for the different spinal levels forma map over the surface of the body (see Figure 8.4)that can be useful in localizing lesions of the nerveroots or spinal cord. In Chapters 8 and 9 we will dis-cuss localization based on dermatome and periph-eral nerve patterns of sensory and motor loss. In thischapter we will focus on the central course of the so-matosensory pathways in the spinal cord and brain.Just as our knowledge that the corticospinal tractcrosses over at the pyramidal decussation helps uslocalize CNS lesions (see Figure 6.11A), it is equally
ANATOMICAL AND CLINICAL REVIEW
TABLE 7.1 Main Long Tracts of the Nervous System
NAME (AND LEVEL) PATHWAY(S) FUNCTION OF DECUSSATION
Lateral Motor Pyramidal decus-corticospinal sation (cervico-tract medullary junction)
Posterior column Sensory (vibration, Internal arcuate fibers medial lemniscal joint position, (lower medulla)pathway fine touch)
Anterolateral Sensory (pain, Anterior commissure pathways temperature, (spinal cord)
crude touch)
BL2eBlum07.qxd 2/12/10 8:45 AM Page 276
Prima Eriawan Putra 1102012212 18
a stem axon that bifurcates, re- sulting in one long process that conveys sensory information from the periph- ery and a second process that carries information into the spinal cord through the dorsal nerve roots. A peripheral region innervated by sensory fibers from a single nerve root level is called a dermatome.
Individual somatosensory fibers enter the spinal cord at the dorsal root entry zone (DREZ; also called the RedlichOber- steiner zone) and then give o numerous collaterals that make synaptic con- tact with other neurons within the cord. Fibers subserving dierent sensory modalities occupy dierent positions in the spinal cord (Fig. 2.15). It is impor- tant to note that the myelin sheaths of all aerent fibers become considerably thinner as the fibers traverse the root entry zone and enter the posterior horn. The type of myelin changes from peripheral to central, and the myelinating cells are no longer Schwann cells, but rather oligodendrocytes.
Somatosensory information is sequentially transmitted over three types of neurons: first- order neurons, which transmit information from sensory receptors to dorsal horn neurons; second-order CNS association neurons, which communicate with various reflex circuits and transmit information to the thalamus; and third- order neurons, which forward the information from the thalamus to the sensory cortex.
227
C2C3
C4
C5
C6
C7C8
L1
L 2
L 3
L 4
L5
S1
S1
S2
T2T3T4T5T6T7T8
T9
T10
T11
T12
Ophthalmic n.
Maxillary n.
Mandibular n.
Trigeminal n.C 2
C 3
C 4
C5
C6
C7
C8
T2T3T4T5T6T7T8T9
T 10T 11T 12
L1L 2
L 3
L 4
L 5
L5L4
S 1
S1
S2
S 3
S5S 4
T 1
T1
Fig. 2.6 Segmental innervation of the skin (after HansenSchliack). a Anterior view. b Posteriorview.
cent roots, a dermatomal deficit of touch is generally hard to demonstrate,while one of pain and temperature sensation is more readily apparent. Thus,nerve root lesions can be more sensitively detected by testing for hypalgesia oranalgesia, rather than hypesthesia or anesthesia.
Sensory deficits due to peripheral nerve lesions. It is easy to see why a lesionaffecting a nerve plexus or a peripheral nerve produces a sensory deficit of anentirely different type than a radicular lesion. As plexus lesions usually cause a
Peripheral Components of the Somatosensory System and Peripheral Regulatory Circuits
Baehr, Duus' Topical Diagnosis in Neurology 2005 ThiemeAll rights reserved. Usage subject to terms and conditions of license.
320 Chapter 8
IN THE PRECEDING TWO CHAPTERS, we studied the three main motor andsensory pathways in the central nervous system (see Table 7.1). Wewill now follow these somatic sensory and somatic motor pathwaysinto the peripheral nervous system (see Figure 2.1) to explore theanatomy and clinical disorders of the peripheral nerves. In this chap-ter, we will concentrate on the anatomy of spinal nerve roots and theirrelation to the vertebral structures, regions of innervation, and commonclinical disorders. Peripheral autonomic functions were already dis-cussed in Chapter 6. In Chapter 9, we will follow the nerves further intothe periphery, and we will discuss the brachial and lumbosacral plexusesand peripheral nerve branches.
Segmental Organization of the Nervous SystemLike their invertebrate ancestors, humans retain some degree of segmen-tal organization, especially in the spinal cord. There are 8 cervical (C1C8),12 thoracic (T1T12), 5 lumbar (L1L5), 5 sacral (S1S5), and 1 coccygeal(Co1) spinal segments (Figure 8.1). During development, the bones ofthe spine continue to grow after the spinal cord has reached its fullsize. Therefore, in adults the spinal cord normally ends with the conusmedullaris at the level of the L1 or L2 vertebral bones. The nerve roots (seeFigure 8.1; see also Figure 6.3) travel downward to reach their exit pointsat the appropriate level. Below the L1 or L2 vertebral bones, the spinalcanal contains nerve roots with no spinal cord, forming the cauda equina,meaning horses tail (see Figures 8.1A and 8.3C). The conus medullaristapers into the filum terminale, a thin strand of connective tissue runningin the center of the cauda equina. The roots of the cauda equina are or-ganized such that the most centrally located roots are from the most cau-dal segments of the spinal cord (see Figure 8.3C).
8
C1(A)
C2
C3
C4
C5
C6
C7
C8
T1
T2
T3
T4
T5
T6
T7
T8
T9
T10
T11
T12
L1
L2
L3
L4
S1S2
S3
S4S5
Co1
L5
T1
T2
T3
T4
T5
T6
T7
T8
T9
T10
T11
T12
12L12345
11
10
9
8
7
6
5
4
3
2
T1
76
5
4
3
2
1
L1
L2
L3
L4
L5
S
C2
C3
C4
C5
C6
C7
Conus medullaris
Cauda equina
Lumbar cord
Sacral cord
Cervical cord
Thoracic cord
(B)
Dorsal median septum
Central canal
Intermediate zone
Ventral (anterior) horn
White matter
Gray matter
Spinalnerve
Ventral root(motor)
Dorsal root(sensory)
Ventral median fissure
Ventralcolumn
Dorsalcolumn
Dorsal (posterior) horn
Lateralcolumn
C1
FIGURE 8.1 Spinal Cord and Nerve Roots in Relation to the Vertebral Spinal Canal(A) Sagittal view. The cervical (C5T1) and lumbosacral (L1S3) spinal cord enlarge-ments supply nerves to the arms and legs, respectively. At the level of the L1 or L2 ver-tebral bones the spinal cord ends, and nerve roots continue as the cauda equina. (B) Mo-tor (ventral) roots and sensory (dorsal) roots join at each segment to form spinal nerves.
ANATOMICAL AND CLINICAL REVIEW
BL2eBlum08.qxd 1/1/70 12:53 AM Page 320
Somatosensory SystemsSensory systems can be conceptualized as a series of neu-rons consisting of first-order, second-order, and third-order neurons. First-order neurons transmit sensoryinformation from the periphery to the CNS. Second-orderneurons communicate with various reflex networks andsensory pathways in the spinal cord and travel directly tothe thalamus. Third-order neurons relay informationfrom the thalamus to the cerebral cortex (Fig. 35-1).
This organizing framework corresponds with thethree primary levels of neural integration in thesomatosensory system: the sensory units, which containthe sensory receptors; the ascending pathways; and thecentral processing centers in the thalamus and cerebralcortex. Sensory information usually is relayed andprocessed in a cephalad (toward the head) direction bythe three orders of neurons. Many interneurons processand modify the sensory information at the level of thesecond- and third-order neurons, and many more par-ticipate before coordinated and appropriate learned-movement responses occur. The number of participatingneurons increases exponentially from the primarythrough the secondary and the secondary through thetertiary levels.
The Sensory UnitThe somatosensory experience arises from informationprovided by a variety of receptors distributed throughoutthe body. These receptors monitor four major types ormodalities of sensation: discriminative touch, which isrequired to identify the size and shape of objects andtheir movement across the skin; temperature sensation;sense of movement of the limbs and joints of the body;and nociception, or pain.
Each of the somatosensory modalities is mediated bya distinct system of receptors and pathways to the brain;however, all somatosensory information from the limbs
and trunk shares a common class of sensory neuronscalled dorsal root ganglion neurons. Somatosensoryinformation from the face and cranial structures is trans-mitted by the trigeminal sensory neurons, which func-tion in the same manner as the dorsal root ganglionneurons. The cell body of the dorsal root ganglion neu-ron, its peripheral branch (which innervates a small areaof periphery), and its central axon (which projects to theCNS) form what is called a sensory unit.
The fibers of different dorsal root ganglion neurons con-duct impulses at varying rates, ranging from 0.5 to 120 m/second. This rate depends on the diameter of the nervefiber. There are three types of nerve fibers that transmitsomatosensory information: types A, B, and C. Type Afibers, which are myelinated, have the fastest rate of con-duction.1,2 Type A fibers convey cutaneous pressure andtouch sensation, cold sensation, mechanical pain, and heatpain. Type B fibers, which also are myelinated, transmitinformation from cutaneous and subcutaneous mechano-receptors. The unmyelinated type C fibers have the small-est diameter and the slowest rate of conduction. Theyconvey warmhot sensation and mechanical and chemi-cal as well as heat- and cold-induced pain sensation.
Dermatomal Patt