Embed Size (px)
Citation preview

Pergamon
Int. J. Radiation Oncology Biol. Phys., Vol. 30, No. 3, pp. 551-556, 1994 Copyright 0 1994 Elscvier Science Ltd Printed in the USA. All rights reserved
0360-3016/94 $6.00 + .OO
0360-3016(94)00265-7
??Clinical Original Contribution
PATTERN OF RECURRENCE OF MEDULLOBLASTOMA AFTER LOW-DOSE CRANIOSPINAL RADIOTHERAPY
WILLIAM M. WARA, M.D.,* QUYNH-THU X. LE, M.D.,* PENNY K. SNEED, M.D.,* DAVID A. LARSON, M.D.,* MICHAEL D. PRADOS, M.D.,+ VICTOR A. LEVIN, M.D.,$
MICHAEL S. B. EDWARDS, M.D.+ AND MICHAEL D. WEIL, M.D.*
*Departments of Radiation Oncology and +Neurologic Surgery, University of California, San Francisco, CA 94 143 *Department of Neuro-Oncology, M. D. Anderson Cancer Center, Houston, TX 77030
Purpose: We retrospectively evaluated relapse of medullobhrstoma after low- or high-dose craniospinal radiotherapy, and after conventional or hyperfractionated posterior fossa irradiation. Methods and Materials: Ninety-two pediatric patients were treated postoperatively since 1970 at the University of California, San Francisco. Until 1989, we employed conventional fractionation with low (I 30 Gy) or high-dose craniospinal fields and low-dose (I 56 Gy) posterior fossa boosts. Recently, hyperfractionation delivered low- or high-dose to the craniospinal axis and high-dose to the posterior fossa. Most patients treated after 1979 received chemotherapy. Results: Median follow-up was 70 months. Five-year disease-free survival was 36% (22% for poor-risk vs. 59% for good-risk patients). Five-year overall survival was 52% (43% for poor vs. 68% for good-risk). Neither the dose to the posterior fossa nor the craniospinal axis was statistically related to recurrence. Failure in the posterior fossa occurred despite boosts greater than 56 Gy. Females, over the age of 6 years, had significantly better relapse-free survival than males of the same age. Six of the 54 patients who relapsed were long-term survivors. Conclusions: Low-dose craniospinal radiotherapy, where the majority of patients received chemotherapy, was not associated with increased failure. High-dose posterior fossa hyperfractionation did not improve control. Long-term survival was noted in a number of patients after relapse. We recommend 60 Gy or greater with conventional fractions to the primary area, and continued study of low-dose craniospinal irradiation with adjuvant chemotherapy.
Medulloblastoma, Craniospinal, Radiotherapy, Radiotherapy dosage, Hyperfractionation, Recurrence.
INTRODUCTION
Reported survival for medulloblastoma has improved over the past several decades. Bloom reported a 32% survival rate with radiotherapy for a period between 1950 and 1964, during which time the operative mortality rate was 25% (1). Trials by the International Society of Pediatric Oncology (SIOP) and the Children’s Cancer Study Group (CCSG), which closed in 1979 and 198 1, respectively, added chemotherapy to high-dose radiotherapy of the posterior fossa and craniospinal axis (6, 14). Five-year survival was 53% and 65% with no statistically significant difference in survival between patients treated after surgery with radiotherapy alone or radiotherapy plus chemother- apy. However, Packer showed a significant improvement in survival in patients treated after 1982 with platinum-
based chemotherapy and radiotherapy ( 12). In those pa- tients with a median follow-up of 40 months, a five-year actuarial disease-free survival of 82% overall was reported (88% in poor-risk patients). Halberg most recently updated the results for treatment of adult and pediatric medullo- blastoma at the University of California, San Francisco (UCSF) (8). There was no difference in the rate of recur- rence in the craniospinal axis after reducing the dose to this area. Five-year actuarial survival for all patients was 73%.
We performed a retrospective analysis of the pattern of relapse of pediatric medulloblastoma patients in an attempt to discern a benefit of “high-dose” hyperfrac- tionated radiotherapy to the posterior fossa, and to reassess “low-dose” radiotherapy to the craniospinal axis. Most of the patients received adjuvant chemotherapy. The sites
Presented at the 35th Annual Meeting of ASTRO, New Or- leans, LA, October 1 l-l 5, 1993.
Reprint requests to: Michael D. Weil, M.D., Department of Radiation Oncology, Room L-75 (Box 0226), University ofCal- ifornia, San Francisco, CA 94 143-0226.
Acknowledgements-The authors thank Lea Conlu and Marion Thornton for manuscript preparation.
Accepted for publication 6 May 1994.
551

552 I. J. Radiation Oncology 0 Biology 0 Physics Volume 30, Number 3, 1994
of failure were categorized in relation to the extent of disease and the intensity of the dose of radiation admin- istered.
METHODS AND MATERIALS
We evaluated all patients with primary medulloblas- toma, I 21 years of age, treated with postoperative ra- diotherapy at UCSF between 1970 and 1992. Extent of surgical resection was assessed by the surgeon’s report and, more recently, by examination with magnetic resonance imaging (MRI). All patients had a pathologic diagnosis of medulloblastoma from UCSF. Most patients underwent spinal evaluation with myelogram (4), examination of the cerebrospinal fluid (CSF), MRI, or a combination of these tests. Risk stage was assigned based on the age at diagnosis, the type of surgical procedure (gross total resection vs. biopsy or subtotal resection), and evidence of tumor be- yond the primary area. We did not attempt to subdivide patients by the degree of subtotal resection. Patients were assigned to a good risk category if they were greater than 3 years of age, had undergone a gross total resection, and had negative evaluation of the craniospinal axis. Poor- risk patients were considered to be children 3 years old or less, or those who had undergone a subtotal resection, or patients found to have evidence of microscopic or gross disease outside of the posterior fossa.
diation at reduced craniospinal doses; 36 Gy to the whole brain and 25 Gy to the spine (Brain Tumor Research Center protocol 7922) (10). Between 1984 and 1992, postoperative chemotherapy was procarbazine, 1-(2- chloroethyl)-3-cyclohexyl- 1 -nitrosourea (CCNU), vin- cristine, 6-thioguanine (6-TG), and dibromodulcitol, fol- lowed by radiotherapy with hydroxyurea (Brain Tumor Research Center protocol 8422). Patients received 54 Gy to the posterior fossa, and 24 Gy to the craniospinal axis. After 1990, most poor-risk patients, over 3 years old, were treated with hyperfractionated radiotherapy followed by cisplatinum, CCNU, and vincristine (Brain Tumor Re- search Center protocol 9023). Patients were treated with 1 Gy twice daily, and received 72 Gy to the posterior fossa, and 30 Gy to the craniospinal axis.
Tumor volumes were localized on the simulation films with the aid of computed tomography (CT), beginning in the mid- 1970s and later with MR imaging. All patients were treated with linear accelerators using 4 or 6 MV photons. The brain was treated with opposed lateral fields and, except for several infants, patients were treated prone. The spinal field was treated directly from the posterior to the level of S2-S3 without a “spade flair” at the lower border of the portal. Divergence between the brain and spinal fields was accounted for by appropriate rotation of the collimator and angling of the treatment table towards the lateral field. The match line between the fields was shifted 1 cm every 10 Gy of treatment. Until 1989, ra- diation was delivered to the posterior fossa in single daily fractions of 1.8 Gy to 56 Gy or less (“low dose”). Since 1989, patients were treated at 1 Gy twice daily to a total dose of 72 Gy to the posterior fossa (“high dose”). Patients treated once a day received an average dose of 36 Gy to the craniospinal axis and those treated twice daily received 24-40 Gy. Six infants received radiation to the posterior fossa only.
No patients were lost to follow-up. After treatment, patients were followed with regular examination of the primary site and craniospinal axis using CT or MR scans and CSF cytology. Disease-free survival was measured from the start of radiotherapy until relapse; patients who expired without evidence of disease at the time of death were censored. Duration of survival was measured from the start of radiotherapy until last follow-up or death. Es- timates of disease-free survival and survival were com- puted using the method of Kaplan and Meier (9). Differ- ences among patient groups were evaluated by the Mantel- Haenzel log rank test (11). Univariate and multivariate analyses were performed with the Cox proportional haz- ards regression model (3) using statistical software.’
Combinations of chemotherapeutic agents changed over time. Prior to 1979, adjuvant therapy was radiation only; 54 Gy to the posterior fossa, 40 Gy to the brain, and 36 Gy to the spine. Subsequently, procarbazine was given postoperatively, followed by hydroxyurea plus ra-
Ninety-two patients were treated from 1970- 1992 (Ta- ble 1). The mean age of the patients was 8 years and 27% were 3 years of age or less. Fifty patients were male and 42 were female. Eighty-seven percent had evaluation of the spine with a myelogram, MRI, and/or examination of the spinal fluid. Both radiographic and cytological studies of the craniospinal axis were performed in 69 of the 92 patients. Gross total resection was performed on over one-half of the group (53%), while 36% underwent a subtotal resection, and 11% had a biopsy only. Thirty- five of the 92 patients were assigned to the good-risk group and 57 to the poor-risk group. There were eight patients assigned to the poor-risk category solely on the basis of their age being 3 years old or less at the time of diagnosis. No significant change, in the distribution of good vs. poor- risk patients over the different treatment eras, was noted. Twenty-three patients, treated between 1970 and 1979, received postoperative radiation only. Subsequently, ad- juvant chemotherapy was used in 46 poor-risk patients and in 15 good-risk patients. Seventeen patients in the early 1980s were treated with procarbazine, followed by
RESULTS
’ Stata software (Computing Resource Center, Santa Monica, CA).

Medulloblastoma recurrence after craniospinal radiotherapy 0 W. M. WARA et a/. 553
Table 1. Patient characteristics
Age: 11 months-21 years (median 8 years) (27% 5 3 year-old)
Sex: 50 male/42 female Cranio-spinal 87% had MRI or myelogram or CSF
evaluation: cytology
MRI = magnetic resonance imaging. CSF = cerebrospinal fluid.
hydroxyurea plus radiation at reduced craniospinal doses. Between 1984 and 1990, there were 27 patients who received postoperative chemotherapy (procarbazine, CCNU, vincristine, 6-TG, and dibromodulcitol), followed by radiotherapy with hydroxyurea. After 1990, most poor- risk patients were treated with hyperfractionated radio- therapy, followed by cisplatinum, CCNU, and vincristine.
Treatment of the posterior fossa with I 56 Gy was defined as “low-dose” therapy and > 56 Gy was consid- ered “high dose.” Radiotherapy doses ranged from 22- 56 Gy to the posterior fossa, O-54 Gy to the brain, and O-50 Gy to the spine for standard fractionation. Hyper- fractionation doses ranged from 60-72 Gy to the posterior fossa and 24-40 Gy to the craniospinal axis. Conventional fractionation given to the posterior fossa was, therefore, low dose, and the hyperfractionated posterior fossa treat- ments were high dose. Low (I 30 Gy) and high-dose (> 30 Gy) therapy to the craniospinal axis used conven- tional or hyperfractionated regimens. The median low dose was 54 Gy to the posterior fossa (with conventional fractions) and 25 Gy to the craniospinal axis. The median high-dose was 70 Gy to the posterior fossa ( via hyper- fractionation) and 40 Gy to the craniospinal axis. In pa- tients without evidence of relapse, the mean dose to the posterior fossa was 57.7 Gy. In patients who failed, the mean dose was 56.18 Gy. Mean dose to the brain in pa- tients who failed in that area was 28.16 vs. 3 1.60 Gy in patients who were without brain relapse. Patients who were disease-free in the spinal cord received a mean dose of 27.50 Gy as opposed to a mean dose of approximately 32.00 Gy for those who failed in the spine.
The median follow-up was 70 months and the median time to relapse was 22 months. The actuarial 5-year dis- ease-free survival was 36% (59% for good-risk patients and 22% for poor-risk patients: p = 0.002). There were relapses in 54 patients; 15 of these patients were considered good risk, and 39 were considered poor risk. Median sur- vival was 69 months. Five-year survival was 68% for the good-risk patients vs. 43% for the poor-risk patients (p = 0.015), and 52% overall (Fig. 1). Of the 54 patients who failed, 6 have survived for at least 5 years after relapse. Actuarial analysis of 5-year survival after recurrence was 25%.
Prognostic factors that were significant for disease-free survival by univariate analysis included stage (good risk vs. poor risk) (p = 0.002), sex (p = O.OlO), extent of sur- gical resection (p = 0.017), and whether or not adjuvant
chemotherapy was given (p = 0.046). Female gender and greater extent of resection were associated with improved disease-free survival. Of note, the use of chemotherapy was associated with decreased disease-free survival, but chemotherapy was more commonly given to poor-risk patients. Multivariate analysis, including stage, gender, and use of adjuvant chemotherapy, showed that stage and gender were significant determinants of disease-free sur- vival (p < 0.01 and a = 0.040, respectively) and che- motherapy was not. Thirty-six of 50 (72%) boys have re- lapsed and 18 of 42 (43%) girls have relapsed.
Prognostic factors that were significant for overall sur- vival by univariate analysis included stage (good risk vs. poor risk) (p = 0.015), sex (p = 0.013), and extent of surgical resection (p = 0.00 1). A multivariate analysis in- cluding stage and gender yielded p = 0.023 for gender and p = 0.027 for stage. When the analysis was performed including gender and extent of surgical resection, gender remained a significant determinant of survival (p = 0.040 for gender and p = 0.002 for surgery). Females over 6 years of age had a highly-significant survival advantage (p < 0.00 1): 82% for girls compared to 36% 5-year survival for boys. There was no significant difference in relapse rate or survival detected over the varying diagnostic and treatment eras.
We evaluated the sites of failure to try to correlate treatment with relapse patterns. In the good-risk group, only single sites of failure were noted. This is in distinction to the poor-risk group where patients relapsed concur- rently in multiple areas (Fig. 2). Multiple sites of relapse occurred in 11 of 39 (28%) poor-risk failures. Overall, there were 28 total failures in the posterior fossa, 18 of which were single failures (Table 2). Nineteen patients failed in the brain and 11 of these were the only sites of failure. The spinal cord was the only site of failure in 12 patients, and an additional 6 patients failed in the cord and simultaneously elsewhere. There was no statistical correlation between dose and the site of failure. Subgroup analysis was performed. Good-risk patients who received
Median OS = 70 mo.
b 3b 6b CIO l?O Time (months)
Fig. 1. Kaplan-Meier survival for all patients.
554 I. J. Radiation Oncology 0 Biology 0 Physics Volume 30, Number 3, 1994
PF Dose I 56 Gy
CSA Dose I 30 Gy
PF Dose > 56 Gy
CSA Dose > 30 Gy
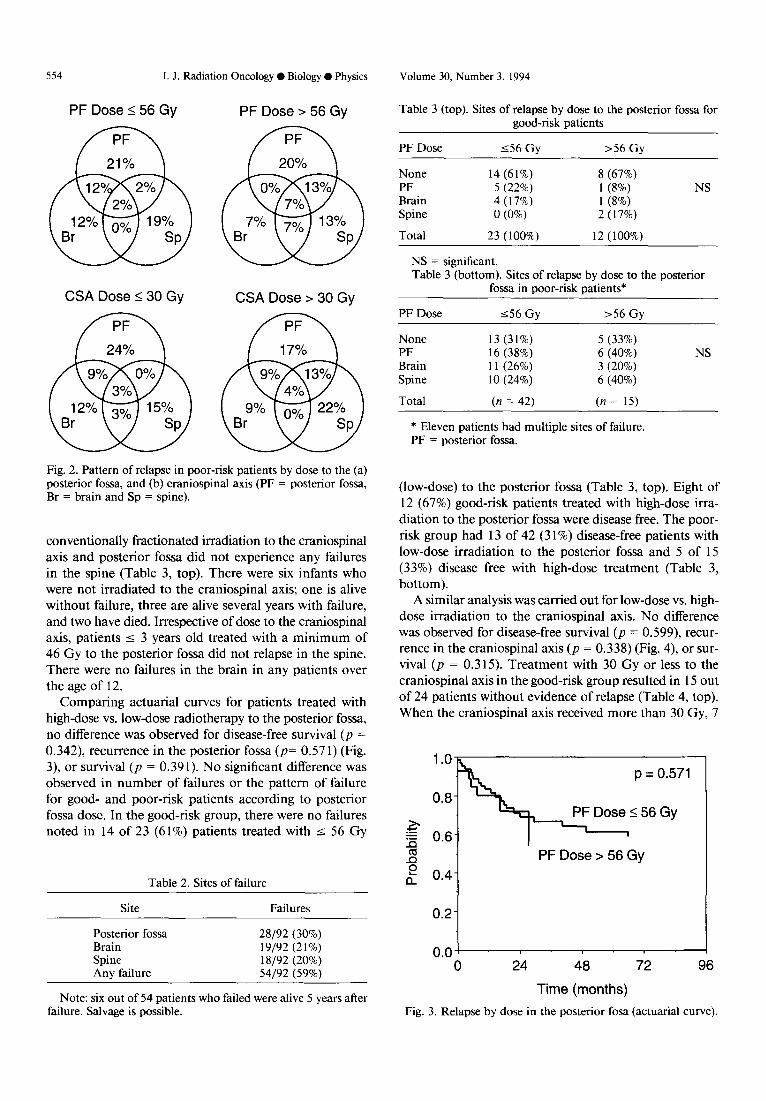
Fig. 2. Pattern of relapse in poor-risk patients by dose to the (a) posterior fossa, and (b) craniospinal axis (PF = posterior fossa, Br = brain and Sp = spine).
conventionally fractionated irradiation to the craniospinal axis and posterior fossa did not experience any failures in the spine (Table 3, top). There were six infants who were not irradiated to the craniospinal axis; one is alive without failure, three are alive several years with failure, and two have died. Irrespective of dose to the craniospinal axis, patients I 3 years old treated with a minimum of 46 Gy to the posterior fossa did not relapse in the spine. There were no failures in the brain in any patients over the age of 12.
Comparing actuarial curves for patients treated with high-dose vs. low-dose radiotherapy to the posterior fossa, no difference was observed for disease-free survival (p = 0.342), recurrence in the posterior fossa (p= 0.571) (Fig. 3), or survival (a = 0.39 1). No significant difference was observed in number of failures or the pattern of failure for good- and poor-risk patients according to posterior fossa dose. In the good-risk group, there were no failures noted in 14 of 23 (6 1%) patients treated with I 56 Gy
Table 2. Sites of failure
Site Failures
Posterior fossa 28/92 (30%) Brain 19/92 (21%) Spine 18/92 (20%) Any failure 54192 (59%)
Note: six out of 54 patients who failed were alive 5 years after failure. Salvage is possible.
Table 3 (top). Sites of relapse by dose to the posterior fossa for good-risk natients
PF Dose 156 Gv >56 Gv
None 14 (61%) 8 (67%) PF 5 (22%) 1 (8%) NS Brain 4 (17%) 1 (8%) Spine 0 (0%) 2 (17%)
Total 23 (100%) 12 (100%)
NS = significant. Table 3 (bottom). Sites of relapse by dose to the posterior
fossa in poor-risk patients*
PF Dose
None PF Brain Spine
Total
556 Gy >56 Gy
13 (31%) 5 (33%) 16 (38%) 6 (40%) NS 11 (26%) 3 (20%) 10 (24%) 6 (40%)
(n = 42) (n = 15)
* Eleven patients had multiple sites of failure. PF = posterior fossa.
(low-dose) to the posterior fossa (Table 3, top). Eight of 12 (67%) good-risk patients treated with high-dose irra- diation to the posterior fossa were disease free. The poor- risk group had 13 of 42 (3 1%) disease-free patients with low-dose irradiation to the posterior fossa and 5 of 15 (33%) disease free with high-dose treatment (Table 3, bottom).
A similar analysis was carried out for low-dose vs. high- dose irradiation to the craniospinal axis. No difference was observed for disease-free survival (p = 0.599), recur- rence in the craniospinal axis (p = 0.338) (Fig. 4) or sur- vival (p = 0.3 15). Treatment with 30 Gy or less to the craniospinal axis in the good-risk group resulted in 15 out of 24 patients without evidence of relapse (Table 4, top). When the craniospinal axis received more than 30 Gy, 7
p = 0.571
PF Dose > 56 Gy
0.2
1 0.0 !
0 24 48 72 96
Time (months)
Fig. 3. Relapse by dose in the posterior fosa (actuarial curve).

Medulloblastoma recurrence after craniospinal radiotherapy 0 W. M. WARA et al. 555
$ 0.6 ‘I CSA Dose > 30 Gy
0.0 ! I 0 24 48 72 96
Time (months)
Fig. 4. Relapse by dose in the craniospinal axis (actuarial curve).
of 11 good-risk patients were disease free. In the poor-risk patients, low-dose vs. high-dose craniospinal radiotherapy resulted in control for 12 of 34 (35%) compared to 6 of 23 patients (26%) (Table 4, bottom). It is possible that a relationship between radiation dose and relapse was ob- scured by nonrandom assignment of therapy and the al- teration in radiation dose when chemotherapy was used. Significant differences in relapse rate or survival were not seen when combined chemotherapy and radiation were compared to radiation alone.
DISCUSSION
A recent study by the Pediatric Oncology Group (POG) and CCSG randomized medulloblastoma patients to 23.4 Gy vs. 36 Gy craniospinal radiotherapy, without che-
Table 4 (top). Sites of relapse by dose to the craniospinal axis in good-risk patients
CSA dose
None PF Brain Spine
Total
130 Gy >30 Gy
15 (63%) I (64%) 3 (13%) 3 (27%) 4 (17%) 1 (9%) 2 (8%) 0 (0%) NS
24 (100%) 11 (100%)
CSA = craniospinal axis. Table 4 (bottom). Sites of relapse by dose to the craniospinal
axis in poor-risk patients*
CSA dose 130 Gy >30 Gy
None PF Brain Spine
Total
12 (35%) 6 (26%) 12 (35%) 10 (43%) 9 (26%) 5 (22%) 7 (21%) 9 (39%)
(n = 34) (n = 23)
* Eleven patients had multiple sites of failure. CSA = craniospinal axis.
motherapy (5). An interim analysis reported an increase in failures in the low-dose regimen. We found no statis- tically significant relationship between radiotherapy dose and the pattern of recurrence of medulloblastoma. Some of our patients received high-dose irradiation to the pos- terior fossa and low-dose radiotherapy to the brain and spine. We analyzed the control vs. relapse in a site by the dose given to that site. Neither posterior fossa dose nor craniospinal dose was correlated with any model of failure or with overall survival. In an attempt to decrease the morbidity of giving craniospinal radiotherapy to children, treatment with high-dose radiation to the craniospinal axis was replaced, over the years, by combined modality ther- apy. In our patients, radiation doses were decreased and the treatment was supplemented by drug therapy. Signif- icant differences in relapse rate or survival were not seen for combined chemotherapy and low-dose radiation compared to high-dose radiation alone. Because many of our patients received adjuvant chemotherapy, it is possible that this treatment was of benefit in treating microscopic residual (7) and thereby enhanced the effect of a given radiation dose. As a result, a relationship between radia- tion dose and relapse could have been obscured when chemotherapy was used. In addition, the assignment of dosage to the craniospinal axis was not randomized and this might confound the differences between low and high- dose treatment. Low-dose craniospinal radiotherapy with chemotherapy and careful follow-up needs to be contin- ued in an attempt to minimize morbidity of treating chil- dren with medulloblastoma (2, 13, 15).
Prior studies suggested that survival after failure is dis- mal in medulloblastoma ( 10). Ton-es et al. recently re- ported no survivors after relapse, and questioned the value of surveillance scanning of children after treatment for medulloblastoma (16). However, 6 of 54 patients in this study are long-term survivors after relapse. It is tempting to speculate that improvements in imaging, treatment planning, and surgical techniques during the study altered the results. Surprisingly, we did not detect a significant change in the distribution of good vs. poor-risk patients over the different treatment eras. In addition, there was no significant difference in relapse rate or survival detected over the varying diagnostic and treatment eras. MR im- aging and precision planning should decrease morbidity and marginal misses of tumor (8). We are now using triple- dose contrast with spine MR imaging to better evalu- ate the craniospinal axis in primary patients and in follow-up.
Survival after medulloblastoma is still not satisfactory. Age of greater than 6 years, gender, extent of resection, and classification as good risk or high risk correlated with relapse-free and overall survival. Girls over the age of 6 years had significantly better 5-year survival than boys of the same age, 82% vs. 36%. The basis for this finding eludes us. There are few developmental differences in the lower portion of this age range to explain the result (not seen in other brain tumors). It might be that precocious puberty

556 I. J. Radiation Oncology 0 Biology 0 Physics Volume 30, Number 3, 1994
is induced by the therapy, and this confers a survival ad- a higher biologically equivalent dose was necessary. We vantage (P. K. Duffner, oral communication, March, currently recommend treating the posterior fossa with 59.4 1994). In this analysis, high-dose radiotherapy to the pos- Gy at 1.8 Gy per daily fraction with consideration of a terior fossa with hyperfractionation was no better than radiosurgery boost to gross disease and continued study conventional low-dose radiotherapy. It is possible that 72 of low-dose craniospinal irradiation with adjuvant che- Gy given at 1 Gy twice daily was an inadequate dose and motherapy.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
Bloom, H. J. G.; Wallace, E. N. K.; Henk, J. M. The treat- ment and prognosis of medulloblastoma in children. Am. J. Radiol. 105:43-62; 1969. Brown, I. H.; Lee, T. J.; Eden, 0. B.; Bullimore, J. A.; Savage, D. C. Growth and endocrine function after treatment for medulloblastoma. Arch. Dis. Child. 58:722-727; 1983. Cox, D. R. Regression models and life tables. J. R. Stat. Sot. 34: 187-220; 1972. Deutsch, M.; Reigel, D. H. The value of myelography in the management of childhood medulloblastoma. Cancer 45: 2194-2197; 1980. Deutsch, M.; Thomas, P.; Boyett, J.; Krischer, J. P.; Finlay, J.; Kun, L. et al. Low stage medulloblastoma: A children’s cancer study group (CCSG) and pediatric oncology group (POG) randomized study of standard vs. reduced neuraxis irradiation [abstract]. Proc. A.S.C.O. 10: 124; 199 1. Evans, A. E.; Derek, R.; Jenkin, T.; Sposto, R.; Ortega, J. A.; Wilson, C. B.; Wara, W.; Ertel, I. J.; Kramer, S.; Chang, C. H.; Leikin, S. L.; Hammond, G. D. Results of a pro- spective randomized trial of radiation therapy with and without CCNU, vincristine, and prednisone. J. Neurosurg. 721572-582; 1990. Goldwein, J. W.; Radcliffe, J.; Packer, R. J.; Sutton, L. N.; Lange, B.; Rorke, L. B.; D’Angio, G. J. Results of a pilot study of low-dose craniospinal radiation therapy plus che- motherapy for children younger than 5 years with primitive neuroectodermal tumors. Cancer 71:2647-2652; 1993. Halberg, F. E.; Wara, W. M.; Fippin, L. F.; Edwards, M. S. B.; Levin, V. A.; Davis, R. L. Low-dose craniospinal radiation for medulloblastoma. Int. J. Radiat. Oncol. Biol. Phys. 20:65 I-654; 199 1.
9. Kaplan, E. S.; Meier, P. Non-parametric estimations from
10.
11.
12.
13.
14.
15.
16
incomplete observations. Am. Stat. Assoc. J. 53:457-482; 1958. Levin, V. A.; Rodriguez, L. A.; Edwards, M. S. B.; Wara, W. M.; Liu, A. C.; Fulton, D.; Davis, R. L.; Wilson, C. R.; Silver, P. Treatment of medulloblastoma with procarbazine hydroxyurea, and reduced radiation does to whole brain and spine. J. Neurosurg. 68:383-387; 1988. Mantel, N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Che- mother. Rep. 50: 163- 170; 1966. Packer, R. J.; Sutton, L. N.; Goldwein, J. W.; Perilongo, G.; Bunin, G.; Ryan, J.; Cohen, B. H.; D’Angio, G.; Kramer, E.; Zimmerman, R. A.; Rorke, L. B.; Evans, A. E.; Schut, L. Improved survival with the use of adjuvant chemotherapy in the treatment of medulloblastoma. J. Neurosurg. 74:433- 440; 1991. Raimondi, A. J.; Tomita, T. The advantage of total resection of medulloblastoma and disadvantages of whole brain post- operative radiation therapy. Childs Brain 5:585-590; 1979. Tait, D. M.; Thornton-Jones, H.; Bloom, H. J. G.; Lemerle, J.; Morris-Jones, P. Adjuvant chemotherapy for medullo- blastoma: The first multi-centre control trial of the inter- national society of paediatric oncology (SIOP I). Eur. J. Cancer 26:464-469; 1990. Tomita, T.; Mclone, D. G. Medulloblastoma in childhood results of radical resection and low dose neuroaxis radiation therapy. J. Neurosurg. 64:238-243; 1986. Torres, C. F.; Rebsamen, S.; Silber, J. H.; Sutton, L. N.; Bilaniuk, L. T.; Zimmerman, R. A.; Goldwein, J. W.; Phil- lips, P. C.; Lange, B. J. Surveillance scanning of children with medulloblastoma. N. Engl. J. Med. 330:892-895; 1994.
![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://img.dokumen.tips/doc/110x75/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)



![Medulloblastoma: [Print] - eMedicine Neurology · accounts for approximately 7-8% of all intracranial tumors and 30% of ... Incidence of medulloblastoma is 1.5-2 cases per ... Medulloblastoma:](https://img.dokumen.tips/doc/110x75/5b7fc2317f8b9ae6088caa0e/medulloblastoma-print-emedicine-accounts-for-approximately-7-8-of-all.jpg)



![Spinal Metastasis of Medulloblastoma in Adults: A Case Report · 2015. 1. 6. · systemic metastasis [1]. Our patient had neither tumor recurrence in the posterior fossa nor systemic](https://img.dokumen.tips/doc/110x75/5fda06f185061512a942751d/spinal-metastasis-of-medulloblastoma-in-adults-a-case-2015-1-6-systemic-metastasis.jpg)




















