Embed Size (px)
Citation preview

Journal of Clinical Neuroscience 18 (2011) 678–682
Contents lists available at ScienceDirect
Journal of Clinical Neuroscience
journal homepage: www.elsevier .com/ locate/ jocn
Neuroanatomical study
Neuronavigation-based quantitative study of the far-lateral keyhole approachfollowing partial removal of the occipital condyle and jugular tubercle
Hengzhu Zhang a, Qing Lan b,⇑, Xiaodong Wang a
a Department of Neurosurgery, Clinical Medical College, Yangzhou University, Yangzhou, Jiangsu Province, Chinab Department of Neurosurgery, Second Affiliated Hospital, Soochow University, 1055 Sanxiang Road, Suzhou, Jiangsu Province 215004, China
a r t i c l e i n f o
Article history:Received 2 May 2010Accepted 19 August 2010
Keywords:KeyholeNeurosurgical anatomyOperation approachSkull base
0967-5868/$ - see front matter � 2010 Elsevier Ltd. Adoi:10.1016/j.jocn.2010.08.031
⇑ Corresponding author. Tel.: +86 512 67783937; faE-mail address: [email protected] (Q. Lan).
a b s t r a c t
We aimed to quantitate the exposure of the petroclival area after partial removal of the occipital condyle(OC) and tuberculum jugular (JT) using the far-lateral keyhole approach. Navigation data were obtainedfor six cadaveric heads, and the OC and jugular tubercle were outlined with different colours. After theretro-condylar keyhole approach was performed, 1/3 and then 1/2 of the OC and then the JT wereresected stepwise using neuronavigation. Simultaneously, anatomic structures were observed and thelateral visual field angle (LVFA), exposed clival area and surgical freedom were measured. Themean ± standard deviation (SD) of the LVFA were: 39.2 ± 3.29� (before drilling the OC); 51.46 ± 2.45�(1/3 of the OC drilled); and 57.52 ± 2.66� (1/2 of the OC drilled); these values were significantly different(p < 0.01). Exposure of the petroclival area increased significantly after JT removal (p < 0.01), whereas sur-gical freedom increased significantly after removal of both partial OC and JT (p < 0.05).We concluded thatin the far-lateral keyhole approach, the LVFA is increased by partial drilling of the OC; the middle clivus isfurther exposed following JT drilling, and surgical freedom is improved significantly after partial removalof the OC and JT.
� 2010 Elsevier Ltd. All rights reserved.
1. Introduction
Lesions located along the lower clivus and the anterior portionof the foramen magnum have always been surgically challenging.The far-lateral approach has been considered suitable because itcan provide access to the upper ventral spinal canal, the anteriorportion of the foramen magnum, the lower and middle clivusand the jugular foramen.1 In recent years, the advantages of thekeyhole approach have been described by an increasing numberof neurosurgeons.2 We combined a keyhole exposure with the tra-ditional far-lateral approach and designed several new far-lateralkeyhole approaches aimed at different exposure demands. Theretro-condylar keyhole approach,3 using a 7 cm longitudinal‘‘S’’-shaped skin incision, can expose cranial nerves VII to XII, thevertebral artery (VA), a branch of the posterior inferior cerebellarartery (PICA), and the ventrolateral medulla oblongata, allowingsurgery on lesions therein.
Only a narrow slit-like area can be exposed at the level of theforamen magnum because of the medulla oblongata mediallyand the occipital condyle (OC) laterally – leaving a limited fieldfor the neurosurgeon.4,5 Several reports4,6 suggest that the surgicalfield can be enlarged via partial resection of the OC or the jugular
ll rights reserved.
x: +86 512 68284303.
tubercle (JT). More anatomical structures and space can be exposedin the far-lateral transcondylar transtubercular keyhole approach.7
The main purpose of this study was to quantitate the exposureof the petroclival area after 1/3 and 1/2 of the OC, and then the JT,were removed successively with the assistance of neuronavigation.We were therefore able to assess the effects of partial resection ofthe OC and JT in the far-lateral keyhole approach.
2. Materials and methods
The study was performed on six bilaterally dissected cadaverspecimens in which the intracranial blood vessels had been in-jected with coloured latex. The dissections were performed usinga Stryker neuronavigation system (Stryker Navigation, Kalamazoo,MI, USA; software version 6000-600-000 SW90-0001), a LeicaOHS-1 microscope (Leica, Wetzlar, Germany), high-speed drill(Aesculap, Tuttlingen, Germany), a Nikon 4500 digital camera(Nikon, Tokyo, Japan), and bayonet-shaped instruments specifi-cally designed for keyhole surgery.
Cadaver heads fixed with six to eight navigation markers under-went continuous 3 mm thin-slice CT scans and three-dimensional(3D) reconstruction (1 mm). Before exposure of the petroclivalarea, the scan data were entered into the neuronavigation systemand 1/3 and 1/2 of the medioposterior OC and the JT were circum-scribed in different colours using the contour function of the
H. Zhang et al. / Journal of Clinical Neuroscience 18 (2011) 678–682 679
navigation system (Supplementary Fig. 1). The head was placed inthe lateral position, which placed the ear and the mastoid upper-most. A 7 cm longitudinal ‘‘S’’-shaped skin incision began 2 cm be-hind the middle point of the mastoid. Using neuronavigation, theincision curved downward, ending at the level of C23 in the cadaverhead (Fig. 1). The muscle tissues were reflected layer by layer.3 Asmall, approximately 3-cm-diameter suboccipital craniotomy wasmade with its lateral border at the sigmoid sinus; a ‘‘doubleY’’-shaped dural flap was made with its base towards the sigmoidsinus (Fig. 2). After the cisterna magna was opened and thecerebellar hemisphere retracted medially and superiorly, manyanatomic structures could be partially observed via the keyholebone window by adjusting the head position and microscope angle.Successive neuronavigation-based removal of 1/3 and then 1/2 ofthe OC and then the JT was then conducted, and measurementstaken at each step (Figs. 3–6).
Four parameters were measured as follows.
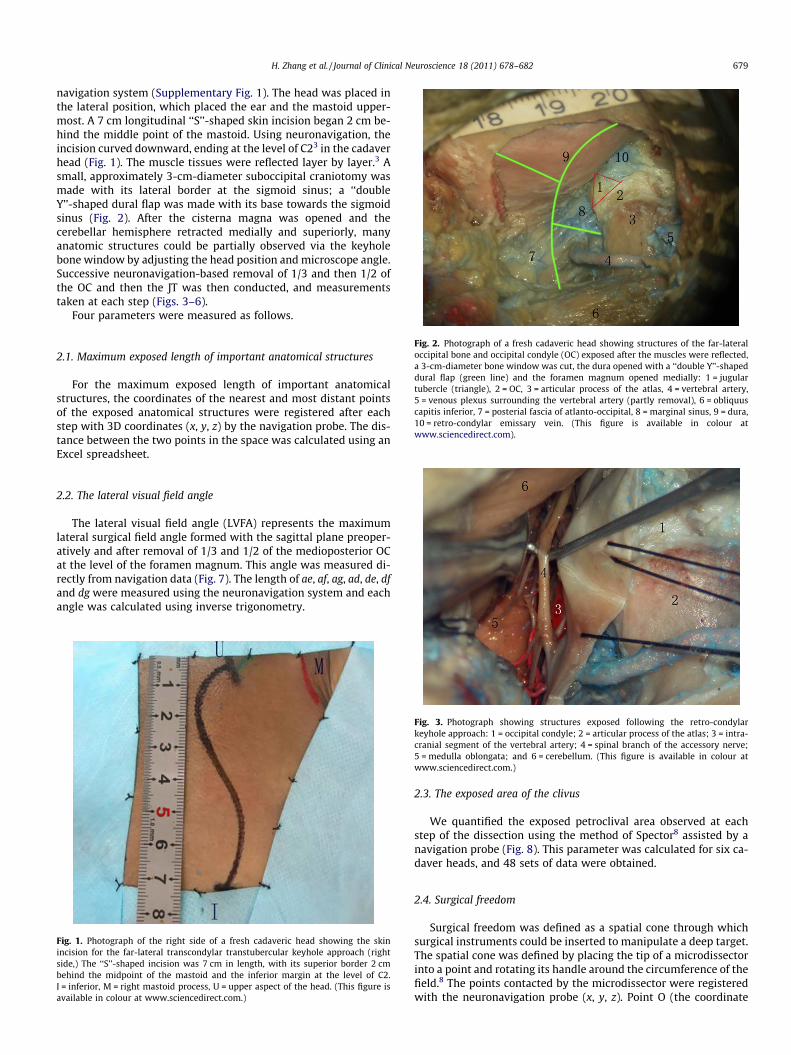
Fig. 2. Photograph of a fresh cadaveric head showing structures of the far-lateraloccipital bone and occipital condyle (OC) exposed after the muscles were reflected,a 3-cm-diameter bone window was cut, the dura opened with a ‘‘double Y’’-shapeddural flap (green line) and the foramen magnum opened medially: 1 = jugulartubercle (triangle), 2 = OC, 3 = articular process of the atlas, 4 = vertebral artery,5 = venous plexus surrounding the vertebral artery (partly removal), 6 = obliquuscapitis inferior, 7 = posterial fascia of atlanto-occipital, 8 = marginal sinus, 9 = dura,10 = retro-condylar emissary vein. (This figure is available in colour atwww.sciencedirect.com).
2.1. Maximum exposed length of important anatomical structures
For the maximum exposed length of important anatomicalstructures, the coordinates of the nearest and most distant pointsof the exposed anatomical structures were registered after eachstep with 3D coordinates (x, y, z) by the navigation probe. The dis-tance between the two points in the space was calculated using anExcel spreadsheet.
2.2. The lateral visual field angle
The lateral visual field angle (LVFA) represents the maximumlateral surgical field angle formed with the sagittal plane preoper-atively and after removal of 1/3 and 1/2 of the medioposterior OCat the level of the foramen magnum. This angle was measured di-rectly from navigation data (Fig. 7). The length of ae, af, ag, ad, de, dfand dg were measured using the neuronavigation system and eachangle was calculated using inverse trigonometry.
Fig. 1. Photograph of the right side of a fresh cadaveric head showing the skinincision for the far-lateral transcondylar transtubercular keyhole approach (rightside,) The ‘‘S’’-shaped incision was 7 cm in length, with its superior border 2 cmbehind the midpoint of the mastoid and the inferior margin at the level of C2.I = inferior, M = right mastoid process, U = upper aspect of the head. (This figure isavailable in colour at www.sciencedirect.com.)
Fig. 3. Photograph showing structures exposed following the retro-condylarkeyhole approach: 1 = occipital condyle; 2 = articular process of the atlas; 3 = intra-cranial segment of the vertebral artery; 4 = spinal branch of the accessory nerve;5 = medulla oblongata; and 6 = cerebellum. (This figure is available in colour atwww.sciencedirect.com.)
2.3. The exposed area of the clivus
We quantified the exposed petroclival area observed at eachstep of the dissection using the method of Spector8 assisted by anavigation probe (Fig. 8). This parameter was calculated for six ca-daver heads, and 48 sets of data were obtained.
2.4. Surgical freedom
Surgical freedom was defined as a spatial cone through whichsurgical instruments could be inserted to manipulate a deep target.The spatial cone was defined by placing the tip of a microdissectorinto a point and rotating its handle around the circumference of thefield.8 The points contacted by the microdissector were registeredwith the neuronavigation probe (x, y, z). Point O (the coordinate

Fig. 4. Photograph showing the structures exposed following the retro-condylarkeyhole approach and neuronavigation-based removal of 1/3 of the posteriormedial occipital condyle (OC): 1 = jugular tubercle (triangle), 2 = OC, 3 = articularprocess of the atlas, 4 = hypoglossal nerve, 5 = cerebellum, 6 = dura. (This figure isavailable in colour at www.sciencedirect.com.)
Fig. 5. Photograph showing structures exposed following the retro-condylarkeyhole approach and neuronavigation-based removal of 1/2 of the occipitalcondyle and jugular tubercle: 1 = ipsilateral vertebral artery, 2 = contralateralvertebral artery, 3 = hypoglossal nerve, 4 = spinal root of nervus accessorius,5 = medulla oblongata, 6 = cerebellum. (This figure is available in colour atwww.sciencedirect.com.)
Fig. 6. Photograph (view from inferior) of a skull showing the relationship betweenthe occipital condyle (OC), hypoglossal canal and jugular tubercle (JT): 1 = OC,2 = hypoglossal canal, 3 = JT, 4 = internal acoustic foramen. (This figure is availablein colour at www.sciencedirect.com.)
Fig. 7. An axial neuronavigation data image of the occipital condyle (OC) showingthe lateral visual field angle (LVFA, \): \eab, the LVFA before removal of the OC;\fab, the LVFA angle after removal of 1/3 of the OC; and \gab, the LVFA afterremoval of 1/2 of the OC. A = anterior, P = posterior. (This figure is available incolour at www.sciencedirect.com.)
680 H. Zhang et al. / Journal of Clinical Neuroscience 18 (2011) 678–682
origin at the edge of the foramen magnum) was set (x = y = z = zero)and was connected to each of the contact points; thus, a heptagonalarea was created by taking a slice through the polygonal cone at aheight of 10 cm on the z axis. Data for each coordinate followingeach step of the resection were collected; 48 sets of data were ob-tained for six cadaver heads (Fig. 9).
Based on the coordinate values of the seven points (S1–S7), theexposed area of the clivus and surgical freedom could be measureddirectly using the in-house-developed software Med-area (devel-oped by Mr Nan Li, Nanjing University). The software rotated thecoordinate system and ignored the z variable for the seven points
in the new coordinate system to obtain the projected coordinatesof these points in the OBC plane (Fig. 9). The software then deter-mined the coordinates of the focal point O’ for the seven points;thus, seven triangles were generated and the combined area ofthese seven triangles was considered the sum of the projectionarea. Surgical freedom was calculated similarly. Data were givenas the mean ± standard deviation (SD) and were statistically ana-lysed using the Statistical Package for the Social Sciences version11.5 software (SPSS, Chicago, IL, USA). The paired t-test was usedfor statistical analysis.
3. Results
The PICA and hypoglossal nerve (cranial nerve XII) were furtherexposed after removal of 1/3 of the OC (p < 0.05 and p < 0.01,respectively); the intracranial segment of the VA was further ex-posed after removal of 1/2 of the OC (p < 0.01). Drilling of the JT re-sulted in dramatic exposure of the basilar artery (p < 0.01), anteriorinferior cerebellar artery (AICA) (p < 0.01), and accessory nervespinal branch (p < 0.05) (Table 1).
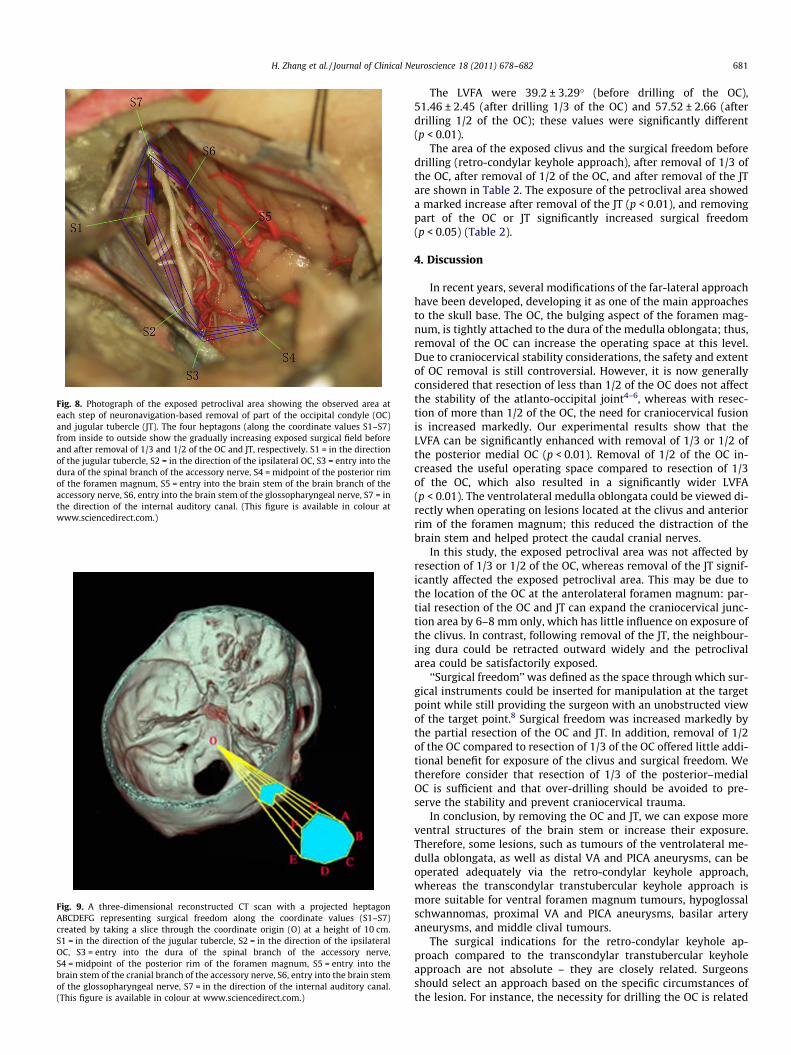
Fig. 9. A three-dimensional reconstructed CT scan with a projected heptagonABCDEFG representing surgical freedom along the coordinate values (S1–S7)created by taking a slice through the coordinate origin (O) at a height of 10 cm.S1 = in the direction of the jugular tubercle, S2 = in the direction of the ipsilateralOC, S3 = entry into the dura of the spinal branch of the accessory nerve,S4 = midpoint of the posterior rim of the foramen magnum, S5 = entry into thebrain stem of the cranial branch of the accessory nerve, S6, entry into the brain stemof the glossopharyngeal nerve, S7 = in the direction of the internal auditory canal.(This figure is available in colour at www.sciencedirect.com.)
Fig. 8. Photograph of the exposed petroclival area showing the observed area ateach step of neuronavigation-based removal of part of the occipital condyle (OC)and jugular tubercle (JT). The four heptagons (along the coordinate values S1–S7)from inside to outside show the gradually increasing exposed surgical field beforeand after removal of 1/3 and 1/2 of the OC and JT, respectively. S1 = in the directionof the jugular tubercle, S2 = in the direction of the ipsilateral OC, S3 = entry into thedura of the spinal branch of the accessory nerve, S4 = midpoint of the posterior rimof the foramen magnum, S5 = entry into the brain stem of the brain branch of theaccessory nerve, S6, entry into the brain stem of the glossopharyngeal nerve, S7 = inthe direction of the internal auditory canal. (This figure is available in colour atwww.sciencedirect.com.)
H. Zhang et al. / Journal of Clinical Neuroscience 18 (2011) 678–682 681
The LVFA were 39.2 ± 3.29� (before drilling of the OC),51.46 ± 2.45 (after drilling 1/3 of the OC) and 57.52 ± 2.66 (afterdrilling 1/2 of the OC); these values were significantly different(p < 0.01).
The area of the exposed clivus and the surgical freedom beforedrilling (retro-condylar keyhole approach), after removal of 1/3 ofthe OC, after removal of 1/2 of the OC, and after removal of the JTare shown in Table 2. The exposure of the petroclival area showeda marked increase after removal of the JT (p < 0.01), and removingpart of the OC or JT significantly increased surgical freedom(p < 0.05) (Table 2).
4. Discussion
In recent years, several modifications of the far-lateral approachhave been developed, developing it as one of the main approachesto the skull base. The OC, the bulging aspect of the foramen mag-num, is tightly attached to the dura of the medulla oblongata; thus,removal of the OC can increase the operating space at this level.Due to craniocervical stability considerations, the safety and extentof OC removal is still controversial. However, it is now generallyconsidered that resection of less than 1/2 of the OC does not affectthe stability of the atlanto-occipital joint4–6, whereas with resec-tion of more than 1/2 of the OC, the need for craniocervical fusionis increased markedly. Our experimental results show that theLVFA can be significantly enhanced with removal of 1/3 or 1/2 ofthe posterior medial OC (p < 0.01). Removal of 1/2 of the OC in-creased the useful operating space compared to resection of 1/3of the OC, which also resulted in a significantly wider LVFA(p < 0.01). The ventrolateral medulla oblongata could be viewed di-rectly when operating on lesions located at the clivus and anteriorrim of the foramen magnum; this reduced the distraction of thebrain stem and helped protect the caudal cranial nerves.
In this study, the exposed petroclival area was not affected byresection of 1/3 or 1/2 of the OC, whereas removal of the JT signif-icantly affected the exposed petroclival area. This may be due tothe location of the OC at the anterolateral foramen magnum: par-tial resection of the OC and JT can expand the craniocervical junc-tion area by 6–8 mm only, which has little influence on exposure ofthe clivus. In contrast, following removal of the JT, the neighbour-ing dura could be retracted outward widely and the petroclivalarea could be satisfactorily exposed.
‘‘Surgical freedom’’ was defined as the space through which sur-gical instruments could be inserted for manipulation at the targetpoint while still providing the surgeon with an unobstructed viewof the target point.8 Surgical freedom was increased markedly bythe partial resection of the OC and JT. In addition, removal of 1/2of the OC compared to resection of 1/3 of the OC offered little addi-tional benefit for exposure of the clivus and surgical freedom. Wetherefore consider that resection of 1/3 of the posterior–medialOC is sufficient and that over-drilling should be avoided to pre-serve the stability and prevent craniocervical trauma.
In conclusion, by removing the OC and JT, we can expose moreventral structures of the brain stem or increase their exposure.Therefore, some lesions, such as tumours of the ventrolateral me-dulla oblongata, as well as distal VA and PICA aneurysms, can beoperated adequately via the retro-condylar keyhole approach,whereas the transcondylar transtubercular keyhole approach ismore suitable for ventral foramen magnum tumours, hypoglossalschwannomas, proximal VA and PICA aneurysms, basilar arteryaneurysms, and middle clival tumours.
The surgical indications for the retro-condylar keyhole ap-proach compared to the transcondylar transtubercular keyholeapproach are not absolute – they are closely related. Surgeonsshould select an approach based on the specific circumstances ofthe lesion. For instance, the necessity for drilling the OC is related

Table 1The exposed length of anatomic structures (mean ± standard deviation) measured before and after the removal of the occipital condyle (OC) and the jugular tubercle (JT)
Item VA (mm) PICA (mm) Basilar artery (mm) Accessory nerve spinal branch (mm) Cranial nerve XII (mm) AICA
Before removal of the OC 14.34 ± 0.97� 20.48 ± 2.03� – 17.20 ± 1.53�� 6.83 ± 0.81§ 12.34 ± 0.81��
Removal of 1/3 of the OC 20.77 ± 2.32 26.88 ± 2.72� 6.51 ± 1.13– 22.22 ± 0.80 9.05 ± 1.43§ 14.16 ± 0.63Removal of 1/2 of the OC 25.77 ± 1.44� 27.26 ± 2.33 9.82 ± 2.47 23.92 ± 0.77 12.33 ± 1.41 15.07 ± 1.90Removal of the JT 26.88 ± 0.35 26.96 ± 2.74 15.65 ± 1.34– 26.56 ± 1.35�� 12.45 ± 1.26 20.36 ± 4.18��
Drilling of the JT resulted in increased exposure of the: –, basilar artery (p < 0.01); ��, anterior inferior cerebellar artery (AICA; p < 0.01); ��, accessory nerve spinal branch(p < 0.05).� The intracranial segment of the VA was exposed after removal of 1/2 of the OC (p < 0.01).� The posterior inferior cerebellar artery (PICA) was exposed after removal of 1/3 of the OC (p < 0.05).§ Cranial nerve XII was exposed after removal of 1/3 of the OC (p < 0.01).
Table 2The exposed petroclival area and surgical freedom at each step of the far-lateral transcondylar transtubercular keyhole approach
Step of the approach Exposed petroclival area Surgical freedom
Mean ± SD (mm2) Mean% of final exposure ± SD Mean area ± SD (mm2) Mean% of final surgical freedom ± SD
Retro-condylar keyhole approach 188.1 ± 32.5a 43.9 ± 17.3 340.2 ± 112.6c 34.6 ± 33.1Removal of 1/3 of the OC 208.5 ± 28.4a 48.6 ± 13.6 654.6 ± 154.7d 66.6 ± 23.6Removal of 1/2 of the OC 236.4 ± 30.2a 55.2 ± 12.8 762.1 ± 182.4d 77.5 ± 24.0Removal of the JT 428.6 ± 28.7b 100 983.4 ± 235.2e 100
The exposure of the petroclival area increased significantly after removal of the JT (ab: p < 0.01); drilling part of the OC and JT can significantly increase surgical freedom (cd:p < 0.01; de: p < 0.05).JT = jugular tubercle, OC = occipital condyle, SD = standard deviation.
682 H. Zhang et al. / Journal of Clinical Neuroscience 18 (2011) 678–682
to many factors including the size of the OC, the shape and size ofthe foramen magnum, the distance between the ventral side of thebrain stem and the clivus, the amount of cerebrospinal fluid re-leased, the displacement of the brain stem and cranial nerves,the interface between the lesion and brain tissue, the course ofthe VA through the dura, the vertebro basilar artery confluence,and the size of the JT. For patients who have a foramen magnumthat is small or an OC that is large, or those for whom the spacingbetween the brain stem and the clivus is short, the transcondylarkeyhole approach has obvious advantages over the retro-condylarkeyhole approach. In addition, the selection of the approach isrelated to the lesion; for example, for a tumour located ventral tothe medulla oblongata, if the shape of the lesion is flat and broadlyconnected with the dura, the transcondylar keyhole approach maybe more appropriate even if the tumour is small; in contrast, if thetumour is spherical, soft and less attached to the dura, total resec-tion without drilling of the OC or JT may be achieved even for largetumours.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.jocn.2010.08.031.
References
1. Mintelis A, Sameshima T, Bulsara KR, et al. Jugular tubercle: morphometricanalysis and surgical significance. J Neurosurg 2006;105:753–7.
2. Lan Q. Clinical application of keyhole techniques in minimally invasiveneurosurgery. Chin Med J 2006;119:1327–30.
3. Zhang HZ, Lan Q. Design and microsurgical anatomy of the retrosigmoid–retrocondylar keyhole approach without condyle removal. Minim InvasNeurosurg 2006;49:49–54.
4. Rhoton AL. The far-lateral approach and its transcondylar, supracondylar, andparacondylar extensions. Neurosurgery 2000;47:195–209.
5. Salas E, Sekhar LN, Ziyal IM, et al. Variations of the extreme-lateral craniocervicalapproach: anatomical study and clinical analysis of 69 patients. J Neurosurg1999;90:206–19.
6. Banerji D, Behari S, Jain VK, et al. Extreme lateral transcondylar approach to theskull base. Neurol India 1999;47:22–30.
7. Zhang HZ, Lan Q. Anatomic study on the design of the far-lateral transcondylartranstubercular keyhole approach assisted by neuro-navigation. Chin Med J2006;86:736–9.
8. Spektor S, Anderson GJ, McMenomey SO, et al. Quantitative description of thefar-lateral transcondylar transtubercular approach to the foramen magnum andclivus. J Neurosurg 2000;92:824–31.





























