Embed Size (px)
Citation preview

Feasibility of Spinal Neuronavigation and Evaluation of Registration and Application Error Modalities Using Optical
Topographic Imaging
by
Daipayan Guha
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Institute of Medical Science University of Toronto
© Copyright by Daipayan Guha (2018)

ii
Feasibility of Spinal Neuronavigation and Evaluation of
Registration and Application Error Modalities Using Optical
Topographic Imaging
Daipayan Guha
Doctor of Philosophy
Institute of Medical Science
University of Toronto
2018
Abstract
Intra-operative navigation began with the localization of subsurface structures in cranial
neurosurgery using frame-based stereotaxy. Advances in imaging and computing power have led
to the development of modern frameless three-dimensional (3D) computer-assisted navigation
(CAN), employed across multiple surgical disciplines. In spinal surgery, CAN may guide
implant placement, bony decompression and soft-tissue resection. However, adoption of 3D
CAN by spinal surgeons has been limited by cumbersome registration protocols, workflow
disruption, high capital cost, and questionable quantitative and clinical utility. A novel technique
for image-to-patient registration has recently been developed, based on optical topographic
imaging (OTI). Whether OTI-based CAN is able to provide accurate intra-operative image-
guidance for common spinal procedures, while addressing current limitations of CAN
techniques, warrants study. First, we explored the current paradigms of reporting CAN accuracy
in the context of spinal procedures, finding that quantitative application accuracy and
radiographic screw placement do not correlate. We therefore proposed a combined quantitative
and radiographic system of reporting CAN accuracy. Second, we examined the registration
workflow and accuracy of OTI-CAN in open posterior thoracolumbar instrumentation, in pre-

iii
clinical swine and cadaveric models and subsequently in clinical in-vivo testing. We found that
OTI-CAN is comparably accurate to but significantly faster than existing 3D CAN techniques.
We subsequently found that OTI-CAN was similarly accurate, with maintained workflow
improvements, in minimally-invasive (MIS) thoracolumbar and open cervical approaches.
Finally, we explored mechanisms by which current CAN and specifically surface-based
registration techniques, including OTI, may fail. We found that navigation error increases with
greater working distance to the dynamic reference frame (DRF), and with greater geometric
symmetry over the osseous posterior elements. Taken together, this body of work demonstrates
that OTI is a feasible technique for spinal CAN, and may alleviate the primary issues plaguing
current systems to allow increased adoption into settings where CAN may be most useful.

iv
Acknowledgments
I owe my sincerest gratitude to Dr. Victor Yang for this opportunity and for continued guidance
and mentorship throughout my residency. It has been my utmost honour to be able to observe
and work with you on your journey developing novel surgical applications of optical imaging
devices. What has struck me most, and what I hope to be able to replicate in my own career, is
how incredibly you have been able to balance your clinical, research and entrepreneurial interests
with your family life.
I would like to thank Dr. Albert Yee, as a member of my thesis committee, for your invaluable
guidance and support. Despite a hectic schedule you never ceased to take time out to discuss
approaches for a new study, or to go out of your way to assist in my progression as a clinician.
I also wish to thank Dr. Michael Fehlings, as a member of my thesis committee, without whom
this work would not be possible. Your keen interest and attention to detail, as well as knowledge
of how to plan, perform and communicate scientific work, was instrumental in raising the quality
of this work.
I would like to extend my sincerest thanks also to Dr. Nir Lipsman, for personifying scientific
curiosity and levelheadedness from our initial interactions at the conclusion of my medical
training, to our clinical rotations as junior/senior residents, and finally now as a member of my
thesis committee.
Numerous other advisors, colleagues and friends, impossible to name individually here, have
contributed significantly to my research training. In particular, I would like to thank the
University of Toronto’s Department of Surgery and Division of Neurosurgery for prioritizing the
Surgeon-Scientist Training Program. In this, a number of individuals have made notable
contributions: Chairman of the Department of Surgery Dr. James Rutka, Chairman of the
Division of Neurosurgery Dr. Andres Lozano, Program Director Dr. Abhaya Kulkarni, Sandi
Amaral, Val Cabral, and my fellow clinical and research trainees.
Curiosity, passion, work ethic, and a drive to improve upon the status quo are key tenets of the
life and career I am striving to build. For instilling these qualities in me and for raising me with

v
these very values at the forefront, with no sacrifice spared so that I could have every opportunity
to succeed and grow, I owe my absolute deepest gratitude to my parents Abhijit and Soma. I also
thank my sister, Tanya, for always remaining lighthearted, never allowing me to lose sight of the
truly important moments, and for always being available to lend an ear in our shared journey
towards our doctorates. Finally, thank you to my fiancée, Shatabdi, for your continual
encouragement and unyielding love throughout the long hours spent composing and writing this
thesis.
I would also like to acknowledge the following granting/scholarship programs, without whom
this work would not have been possible: Canadian Institutes of Health Research (CIHR), Natural
Sciences and Engineering Research Council of Canada (NSERC), Postgraduate Medical
Education at the University of Toronto, Surgeon Scientist Training Program at the University of
Toronto, Clinician Investigator Program at the Royal College of Physicians and Surgeons of
Canada, and the International Society for Optics and Photonics (SPIE).

vi
Contributions
Daipayan Guha (author) solely prepared this thesis. All aspects of this body of work, including
the planning, execution, analysis, and writing of all original research and publications, was
performed in whole or in part by the author. The following individual contributions are formally
acknowledeged:
Dr. Victor X.D. Yang (Primary Supervisor, Thesis Committee Member) – mentorship;
laboratory resources; guidance and assistance in the planning, execution and analysis of
experiments as well as manuscript and thesis preparation
Dr. Albert Yee (Thesis Committee Member) – mentorship; laboratory resources; guidance and
assistance in the planning, execution and analysis of experiments as well as manuscript and
thesis preparation
Dr. Michael G. Fehlings (Thesis Committee Member) – mentorship; guidance and assistance in
the planning and analysis of experiments as well as manuscript and thesis preparation
Dr. Nir Lipsman (Thesis Committee Member) – mentorship; guidance and assistance in the
interpretation of results as well as thesis preparation
Dr. Todd G. Mainprize – mentorship; laboratory resources, study supervision
Dr. Raphael Jakubovic – assistance with the quantitative engineering analysis in Chapters 4 and
5, and with the image processing for quantitative analysis in Chapters 4-9
Shaurya Gupta – assistance with the quantitative engineering analysis in Chapters 4 and 5, and
with execution of the experiments in Chapter 6-8
Joel Ramjist – assistance with the execution of experiments in Chapters 4, 5, 7 and 8
Michael K. Leung – assistance with the image processing and software development/refinement
of OTI in Chapter 5, and execution of experiments in Chapter 9

vii
Ryan Deorajh – assistance with the execution of experiments in Chapters 5-7
Dr. Naif M. Alotaibi – assistance with the interpretation of results in Chapters 3, 4, 6, 7
Jamil Jivraj – assistance with the execution of experiments in Chapter 5
Michael Lu – assistance with the execution of experiments in Chapter 5
Dr. Ali Moghaddamjou – assistance with statistical analysis in Chapter 3
Zaneen H. Jiwani – assistance with the execution of experiments in Chapter 3
Dr. David W. Cadotte – assistance with the execution of experiments in Chapters 4-5
Dr. Leodante B. da Costa – assistance with the execution of experiments in Chapters 4-5
Dr. Rajeesh George – assistance with radiographic analysis in Chapters 4-5
Dr. Chris Heyn – assistance with radiographic analysis in Chapters 4-5
Dr. Peter Howard – assistance with radiographic analysis in Chapters 4-5
Dr. Anish Kapadia – assistance with radiographic analysis in Chapter 4
Dr. Jesse M. Klostranec – assistance with radiographic analysis in Chapter 4
Dr. Nicolas Phan – assistance with the execution of experiments in Chapters 4-5
Dr. Gamaliel Tan – assistance with radiographic analysis in Chapters 4-5
Dr. Beau Standish – assistance with the hardware and software development of OTI in Chapter 5
Dr. Adrian Mariampillai – assistance with the hardware and software development of OTI in
Chapter 5
Dr. Kenneth Lee – assistance with the hardware and software development of OTI in Chapter 5
Dr. Peter Siegler – assistance with the hardware and software development of OTI in Chapter 5
Patrick Skowron – assistance with quantitative engineering analysis in Chapter 5

viii
Hamza Farooq – assistance with quantitative engineering analysis in Chapter 5
Nhu Nguyen – assistance with quantitative engineering analysis in Chapter 5
Joseph Alarcon – assistance with quantitative engineering analysis in Chapter 5
Dr. Michael Ford – assistance with the execution of experiments in Chapter 5
Dr. Sidharth Saini – assistance with radiographic analysis in Chapter 6
Dr. Howard J. Ginsberg – assistance with the interpretation of results in Chapter 9

ix
Table of Contents
ACKNOWLEDGMENTS ...................................................................................................................... IV
CONTRIBUTIONS .............................................................................................................................. VI
TABLE OF CONTENTS ........................................................................................................................ IX
LIST OF ABBREVIATIONS ................................................................................................................. XIV
LIST OF TABLES .............................................................................................................................. XVI
LIST OF FIGURES ............................................................................................................................ XVII
CHAPTER 1 GENERAL INTRODUCTION .................................................................................................1
1.1 THESIS ORGANIZATION ......................................................................................................................1
CHAPTER 2 INTRA-OPERATIVE SPINAL NAVIGATION ...........................................................................2
INTRODUCTION .........................................................................................................................2
2.1 EVOLUTION OF COMPUTER-ASSISTED NAVIGATION ................................................................................2
2.1.1 History of Frameless Stereotaxy ..............................................................................................4
2.1.2 History of Spinal Computer-Assisted Navigation .....................................................................5
2.1.3 Current Applications of Spinal Computer-Assisted Navigation................................................9
2.1.3.1 Rationale for Spinal Computer-Assisted Navigation .................................................................................. 12
2.2 REGISTRATION, IMAGING AND ACTUATION TECHNIQUES IN SPINAL COMPUTER-ASSISTED NAVIGATION ....... 21
2.2.1 2D Navigation ....................................................................................................................... 21
2.2.2 3D Navigation ....................................................................................................................... 23
2.2.2.1 Imaging Techniques ................................................................................................................................... 23
2.2.2.2 Registration Techniques ............................................................................................................................. 28
2.2.2.2.1 Paired-Point Matching .......................................................................................................................... 29
2.2.2.2.2 Surface Contour Matching .................................................................................................................... 32
2.2.2.2.3 Hybrid Matching ................................................................................................................................... 36
2.2.2.2.4 Automatic Registration ......................................................................................................................... 37
2.2.2.2.5 Optical Topographic Imaging ................................................................................................................ 38
2.2.3 Instrument Tracking and Actuation ...................................................................................... 44
2.3 EVALUATION OF NAVIGATION ACCURACY .......................................................................................... 50
2.4 THESIS AIMS AND HYPOTHESES ........................................................................................................ 53
CHAPTER 3 SPATIO-TEMPORAL TRENDS IN SPINAL CAN IMPLEMENTATION ....................................... 56
PREAMBLE ............................................................................................................................... 56

x
3.1 ABSTRACT .................................................................................................................................... 57
3.2 INTRODUCTION ............................................................................................................................. 58
3.3 METHODS .................................................................................................................................... 60
3.3.1 Study Design ......................................................................................................................... 60
3.3.2 Database – Patient Selection ................................................................................................ 60
3.3.3 Database – Data Extraction .................................................................................................. 61
3.3.4 Database – Statistical Analysis ............................................................................................. 61
3.3.5 Online Survey ........................................................................................................................ 62
3.4 RESULTS ....................................................................................................................................... 63
3.4.1 Spatio-Temporal Trends in Spinal CAN Usage ...................................................................... 63
3.4.2 Impact of CAN Usage on Revision Surgery Rates.................................................................. 66
3.4.3 Survey of Surgical Trainees – Demographics ........................................................................ 68
3.4.4 Utilization of CAN by Trainees .............................................................................................. 69
3.4.5 Impact of CAN on Trainee Proficiency .................................................................................. 71
3.5 DISCUSSION .................................................................................................................................. 73
3.6 CONCLUSIONS ............................................................................................................................... 76
3.7 SUPPLEMENTAL | DIAGNOSTIC AND FEE CODING ................................................................................ 77
3.8 SUPPLEMENTAL | ONLINE SURVEY.................................................................................................... 80
CHAPTER 4 CORRELATION BETWEEN CLINICAL AND ABSOLUTE ENGINEERING ACCURACY IN SPINAL
COMPUTER-ASSISTED NAVIGATION .................................................................................................. 84
PREAMBLE ............................................................................................................................... 84
4.1 ABSTRACT .................................................................................................................................... 85
4.2 INTRODUCTION ............................................................................................................................. 86
4.3 METHODS .................................................................................................................................... 88
4.3.1 Patient Selection ................................................................................................................... 88
4.3.2 Intra-Operative Navigation ................................................................................................... 88
4.3.3 Clinical Grading ..................................................................................................................... 88
4.3.4 Quantitative Navigation Application Accuracy ..................................................................... 90
4.3.5 Statistical Analysis ................................................................................................................ 92
4.4 RESULTS ....................................................................................................................................... 93
4.4.1 Clinical Accuracy ................................................................................................................... 93
4.4.2 Absolute Application Accuracy ............................................................................................. 94

xi
4.4.3 Clinical-Engineering Correlation ........................................................................................... 94
4.4.4 Surgeon Compensation for Navigation Error ........................................................................ 97
4.5 DISCUSSION .................................................................................................................................. 99
4.6 CONCLUSIONS ............................................................................................................................. 103
CHAPTER 5 OPTICAL TOPOGRAPHIC IMAGING WITH EFFICIENT REGISTRATION TO CT FOR SPINAL
INTRA-OPERATIVE THREE-DIMENSIONAL NAVIGATION ................................................................... 104
PREAMBLE ............................................................................................................................. 104
5.1 ABSTRACT .................................................................................................................................. 105
5.2 INTRODUCTION ........................................................................................................................... 106
5.3 METHODS .................................................................................................................................. 109
5.3.1 OTI System Design .............................................................................................................. 109
5.3.2 Specimen/Patient Selection ................................................................................................ 112
5.3.3 Pre-Clinical Testing ............................................................................................................. 112
5.3.4 Human Clinical Testing ....................................................................................................... 113
5.3.5 Clinicoradiographic Accuracy Assessment .......................................................................... 116
5.3.6 Quantitative Application/Engineering Accuracy ................................................................ 117
5.3.7 Statistical Analysis .............................................................................................................. 119
5.4 RESULTS ..................................................................................................................................... 120
5.4.1 Pre-Clinical Validation ......................................................................................................... 120
5.4.2 Human Clinical Validation................................................................................................... 120
5.5 DISCUSSION ................................................................................................................................ 125
5.6 CONCLUSIONS ............................................................................................................................. 128
CHAPTER 6 OPTICAL TOPOGRAPHIC IMAGING FOR SPINAL INTRA-OPERATIVE THREE-DIMENSIONAL
NAVIGATION IN MINI-OPEN APPROACHES ...................................................................................... 129
PREAMBLE ............................................................................................................................. 129
6.1 ABSTRACT .................................................................................................................................. 130
6.2 INTRODUCTION ........................................................................................................................... 131
6.3 METHODS .................................................................................................................................. 133
6.3.1 Specimen/Patient Selection ................................................................................................ 133
6.3.2 Surgical Technique .............................................................................................................. 133
6.3.3 Registration and Intra-Operative Navigation ..................................................................... 136
6.3.4 Evaluation of Navigation Accuracy ..................................................................................... 137

xii
6.3.5 Statistical Analysis .............................................................................................................. 138
6.4 RESULTS ..................................................................................................................................... 139
6.4.1 Image-to-Patient Registration ............................................................................................ 139
6.4.2 Quantitative Navigation Application Accuracy ................................................................... 140
6.4.3 Radiographic Navigation Accuracy ..................................................................................... 143
6.5 DISCUSSION ................................................................................................................................ 145
6.6 CONCLUSIONS ............................................................................................................................. 148
CHAPTER 7 OPTICAL TOPOGRAPHIC IMAGING FOR SPINAL INTRA-OPERATIVE THREE-DIMENSIONAL
NAVIGATION IN THE CERVICAL SPINE ............................................................................................. 149
PREAMBLE ............................................................................................................................. 149
7.1 ABSTRACT .................................................................................................................................. 150
7.2 INTRODUCTION ........................................................................................................................... 151
7.3 METHODS .................................................................................................................................. 152
7.3.1 Specimen/Patient Selection ................................................................................................ 152
7.3.2 Surgical Technique .............................................................................................................. 153
7.3.3 Registration and Intra-Operative Navigation ..................................................................... 153
7.3.4 Evaluation of Navigation Accuracy ..................................................................................... 155
7.3.5 Statistical Analysis .............................................................................................................. 157
7.4 RESULTS ..................................................................................................................................... 158
7.4.1 Quantitative Navigation Application Accuracy ................................................................... 159
7.4.2 Radiographic Navigation Accuracy ..................................................................................... 159
7.5 DISCUSSION ................................................................................................................................ 162
7.6 CONCLUSIONS ............................................................................................................................. 164
CHAPTER 8 ERROR PROPAGATION IN SPINAL INTRA-OPERATIVE THREE-DIMENSIONAL NAVIGATION
FROM NON-SEGMENTAL REGISTRATION ........................................................................................ 165
PREAMBLE ............................................................................................................................. 165
8.1 ABSTRACT .................................................................................................................................. 166
8.2 INTRODUCTION ........................................................................................................................... 168
8.3 METHODS .................................................................................................................................. 170
8.3.1 Specimen/Patient Selection ................................................................................................ 170
8.3.2 Quantification of Navigation Error from Proximity to DRF ................................................. 170
8.3.3 Quantification of Navigation Error from Surgical Manipulation ........................................ 171

xiii
8.3.4 Quantification of Navigation Error from Respiration-Induced Motion............................... 171
8.3.5 Statistical Analyses ............................................................................................................. 174
8.4 RESULTS ..................................................................................................................................... 175
8.4.1 Navigation Error from Proximity to DRF ............................................................................. 175
8.4.2 Navigation Error from Surgical Manipulation .................................................................... 176
8.4.3 Navigation Error from Respiration-Induced Motion ........................................................... 179
8.5 DISCUSSION ................................................................................................................................ 182
8.6 CONCLUSIONS ............................................................................................................................. 185
CHAPTER 9 GEOMETRIC CONGRUENCE IN SURFACE REGISTRATION FOR SPINAL INTRA-OPERATIVE
THREE-DIMENSIONAL NAVIGATION ................................................................................................ 186
PREAMBLE ............................................................................................................................. 186
9.1 ABSTRACT .................................................................................................................................. 187
9.2 INTRODUCTION ........................................................................................................................... 188
9.3 METHODS .................................................................................................................................. 190
9.3.1 Specimen/Patient Selection ................................................................................................ 190
9.3.2 OTI Registration .................................................................................................................. 190
9.3.3 Computational Modelling of Geometric Congruence ......................................................... 192
9.3.4 Statistical Analysis .............................................................................................................. 194
9.4 RESULTS ..................................................................................................................................... 195
9.4.1 Geometric Congruence by Spinal Region ............................................................................ 195
9.4.2 Geometric Congruence by Laterality .................................................................................. 198
9.4.3 Geometric Congruence by Inclusion of the Spinous Process ............................................... 201
9.5 DISCUSSION ................................................................................................................................ 204
9.6 CONCLUSIONS ............................................................................................................................. 208
CHAPTER 10 CONCLUDING SUMMARY, GENERAL DISCUSSION, AND FUTURE DIRECTIONS ............... 209
PREAMBLE ............................................................................................................................. 209
10.1 CONCLUDING SUMMARY .............................................................................................................. 210
10.2 UNIFYING DISCUSSION.................................................................................................................. 214
10.3 FUTURE DIRECTIONS .................................................................................................................... 218
REFERENCES .................................................................................................................................. 223

xiv
List of Abbreviations
2D Two-dimensional
3D Three-dimensional
ANOVA Analysis of variance
AP Antero-posterior
AR Augmented reality
BBL Biophotonics and Bioengineering Laboratory
BRW Brown-Roberts-Wells
CAN Computer-assisted navigation
CB Cone-beam
CC Cranio-caudal
CRW Cosman-Roberts-Wells
CT Computed tomography
DICOM Digital Imaging and Communications in Medicine
DRF Dynamic reference frame
EM Electromagnetic
EMG Electromyography
FB Fan-beam
FLE Fiducial localization error
FRE Fiducial registration error
GPU Graphics processing unit
ICP Iterative closest-point
IGS Image-guided surgery
II Image-intensifier
IQR Interquartile range

xv
IR Infra-red
LED Light-emitting diode
LITT Laser interstitial thermal therapy
LM Lateral mass
MIS Minimally-invasive
ML Medio-lateral
MPR Multiplanar reconstruction
MRI Magnetic resonance imaging
OR Operating room
OTI Optical topographic imaging
OTS Optical tracking system
RMS Root-mean-square
TL Trsanslaminar
TRE Target registration error
VR Virtual reality
XR X-ray

xvi
List of Tables
TABLE 2-1. STUDIES OF PEDICLE SCREW ACCURACY. .......................................................................... 14
TABLE 2-2. STUDIES OF PEDICLE SCREW MISPLACEMENT. .................................................................. 16
TABLE 2-3. INTRAOPERATIVE OUTCOMES WITH ROBOTIC GUIDANCE. ............................................... 50
TABLE 3-1. UNIVARIATE ANALYSIS WITH REVISION SURGERY AS OUTCOME. ..................................... 67
TABLE 4-1. HEARY CLASSIFICATION FOR PEDICLE SCREW PLACEMENT. .............................................. 89
TABLE 4-2. 2MM CLASSIFICATION FOR PEDICLE SCREW PLACEMENT. ................................................ 89
TABLE 4-3. CLINICORADIOGRAPHIC GRADES OF 209 PEDICLE SCREWS. .............................................. 94
TABLE 5-1. NAVIGATION ERROR AS A FUNCTION OF SPINE REGION AND NAVIGATION TECHNIQUE.. 124
TABLE 6-1. CHARACTERISTICS OF CADAVERIC OTI REGISTRATIONS THROUGH MINI-OPEN EXPOSURES.
...................................................................................................................................................... 141
TABLE 7-1. KELLGREN CLASSIFICATION OF RADIOGRAPHIC CERVICAL SPONDYLOSIS. ....................... 157
TABLE 7-2. NUMBER OF SCREWS IN CADAVERIC AND CLINICAL TESTING, BY LEVEL AND KELLGREN
GRADE. .......................................................................................................................................... 158
TABLE 9-1. GEOMETRIC CONGRUENCE FOR UNILATERAL REGISTRATIONS BY SPINAL LEVEL. ............. 197

xvii
List of Figures
FIGURE 2-1. THE EARLIEST FRAME-BASED STEREOTAXY. ......................................................................3
FIGURE 2-2. AN EARLY FRAMELESS STEREOTACTIC NAVIGATION SYSTEM. ...........................................5
FIGURE 2-3. INTRA-OPERATIVE BIPLANE FLUOROSCOPY. .....................................................................7
FIGURE 2-4. THE FIRST SPINAL INTRA-OPERATIVE NAVIGATION SYSTEM..............................................9
FIGURE 2-5. RADIOGRAPHIC ACCURACY OF PEDICLE SCREWS. ........................................................... 13
FIGURE 2-6. ‘VIRTUAL’ (2D) FLUOROSCOPY. ...................................................................................... 22
FIGURE 2-7. INTRA-OPERATIVE IMAGING TECHNQIUES FOR 3D CAN. ................................................. 27
FIGURE 2-8. PAIRED-POINT IMAGE-TO-PATIENT REGISTRATION. ....................................................... 30
FIGURE 2-9. MANUAL SURFACE MAPPING. ....................................................................................... 34
FIGURE 2-10. ITERATIVE CLOSEST-POINT REGISTRATION. .................................................................. 36
FIGURE 2-11. COMPONENTS AND COORDINATE SYSTEMS OF AUTOMATIC REGISTRATION
TECHNIQUES. ................................................................................................................................... 38
FIGURE 2-12. PASSIVE STEREOVISION AND CORRESPONDENCE. ........................................................ 40
FIGURE 2-13. STRUCTURED LIGHT 3D SCANNING............................................................................... 42
FIGURE 2-14. STRUCTURED LIGHT ILLUMINATION PATTERNS. ........................................................... 42
FIGURE 2-15. OPTICAL INSTRUMENT TRACKING SYSTEMS. ................................................................ 46
FIGURE 2-16. ELECTROMAGNETIC INSTRUMENT TRACKING. .............................................................. 48
FIGURE 2-17. ROBOTIC INSTRUMENTATION GUIDANCE. .................................................................... 50
FIGURE 2-18. CLASSIFICATION OF ERRORS IN FRAMELESS STEREOTACTIC NAVIGATION. .................... 52
FIGURE 3-1. COHORT DEMOGRAPHICS. ............................................................................................. 63
FIGURE 3-2. TEMPORAL TRENDS IN SPINAL CAN USAGE. ................................................................... 65
FIGURE 3-3. SURVEY DEMOGRAPHICS. .............................................................................................. 69
FIGURE 3-4. TRAINEE-REPORTED CAN USAGE. ................................................................................... 70
FIGURE 3-5. TRAINEE PROFICIENCY IN CAN. ...................................................................................... 72

xviii
FIGURE 4-1. QUANTIFICATION OF NAVIGATION APPLICATION ACCURACY. ........................................ 91
FIGURE 4-2. ABSOLUTE NAVIGATION APPLICATION ACCURACY FOR 209 PEDICLE SCREWS. ................ 95
FIGURE 4-3. CORRELATION BETWEEN ABSOLUTE NAVIGATION APPLICATION ERROR AND
CLINICORADIOGRAPHIC GRADE. ....................................................................................................... 96
FIGURE 4-4. POTENTIAL MECHANISM FOR SURGEON COMPENSATION. ............................................. 98
FIGURE 4-5. CORRELATION BETWEEN TRANSLATIONAL AND ANGULAR NAVIGATION ERRORS. .......... 98
FIGURE 5-1. IDEAL THORACIC PEDICLE SCREW PLACEMENT. ............................................................ 108
FIGURE 5-2. CLINICAL PROTOTYPE OF AN EXPERIMENTAL OTI NAVIGATION SYSTEM. ...................... 110
FIGURE 5-3. OPTICAL TOPOGRAPHIC IMAGING (OTI) EXPERIMENTAL NAVIGATION TECHNIQUE. ...... 111
FIGURE 5-4. FLOW DIAGRAM OF OTI HUMAN CLINICAL TRIALS. ....................................................... 114
FIGURE 5-5. QUANTIFICATION OF ABSOLUTE NAVIGATION APPLICATION ACCURACY. ..................... 118
FIGURE 5-6. BLAND-ALTMAN ANALYSIS COMPARING BENCHMARK AND OTI NAVIGATION ACCURACY.
...................................................................................................................................................... 123
FIGURE 6-1. CADAVERIC MINI-OPEN EXPOSURE. ............................................................................. 134
FIGURE 6-2. IN-VIVO HUMAN CLINICAL MINI-OPEN EXPOSURES. ..................................................... 135
FIGURE 6-3. PROTOTYPE OTI CONFIGURATION. .............................................................................. 137
FIGURE 6-4. CORRELATION OF REGISTERED POINTS TO EXPOSURE SIZE AND SPINAL LEVEL. ............. 142
FIGURE 6-5. NAVIGATION APPLICATION ACCURACY, BY SPINAL LEVEL, IN CADAVERIC TESTING. ....... 142
FIGURE 6-6. NAVIGATION APPLICATION ACCURACY, BY SPINAL LEVEL, IN CLINICAL TESTING. ........... 143
FIGURE 6-7. REPRESENTATIVE INTENTIONAL PLACEMENT OF A POORLY-GRADED SCREW. ............... 144
FIGURE 7-1. TRACKED CERVICAL DRILL GUIDE NAVIGATED WITH OTI. .............................................. 154
FIGURE 7-2. QUANTIFICATION OF ABSOLUTE NAVIGATION APPLICATION ACCURACY. ..................... 156
FIGURE 7-3. ABSOLUTE NAVIGATION APPLICATION ACCURACY IN CADAVERIC TESTING. .................. 160
FIGURE 7-4. ABSOLUTE NAVIGATION APPLICATION ACCURACY IN CLINICAL TESTING. ...................... 161
FIGURE 8-1. RESPIRATORY MOTION TRACKING WITH A CUSTOM SPINOUS PROCESS CLAMP............ 172
FIGURE 8-2. VERTEBRAL RESPIRATORY MOTION TRACKING. ............................................................ 173

xix
FIGURE 8-3. TRANSLATIONAL NAVIGATION ERROR FROM DISTANCE TO DRF. .................................. 177
FIGURE 8-4. TRANSLATIONAL NAVIGATION ERROR WITH SURGICAL MANIPULATION. ..................... 178
FIGURE 8-5. RESPIRATION-INDUCED VERTEBRAL MOTION. .............................................................. 180
FIGURE 8-6. RESPIRATORY CYCLES WITH CLINICALLY SIGNIFICANT VERTEBRAL MOTION. ................. 181
FIGURE 9-1. CADAVERIC MIDLINE EXPOSURES FOR OTI. .................................................................. 191
FIGURE 9-2. RECONSTRUCTION OF OTI SURFACE MAP POINT CLOUDS. ............................................ 193
FIGURE 9-3. FITTING OF SYMMETRICAL GEOMETRIES TO OTI POINT CLOUDS. .................................. 193
FIGURE 9-4. GEOMETRIC CONGRUENCE BY SPINE REGION. .............................................................. 196
FIGURE 9-5. GEOMETRIC CONGRUENCE BY REGISTRATION LATERALITY. .......................................... 199
FIGURE 9-6. REDUCTION IN GEOMETRIC CONGRUENCE WITH BILATERAL REGISTRATION. ................ 200
FIGURE 9-7. GEOMETRIC CONGRUENCE BY SPINOUS PROCESS INCLUSION. ..................................... 202
FIGURE 9-8. REDUCTION IN GEOMETRIC CONGRUENCE WITH INCLUSION OF IPSILATERAL SPINOUS
PROCESS BASE. .............................................................................................................................. 203
FIGURE 9-9. PROTOCOL FOR MANUAL REGISTRATION VERIFICATION. ............................................. 207

1
Chapter 1 General Introduction
1.1 Thesis Organization
This thesis is organized in a ‘paper’ format rather than the traditional ‘continuous’ structure,
using primarily peer-reviewed content that has either already been published, or is in submission
for publication. Each chapter addresses a unique component of a novel technique for spinal intra-
operative three-dimensional navigation, including assessing the current climate of navigation
usage, existing paradigms of evaluating navigation techniques, and subsequently multiple routes
of investigation on the merits and pitfalls of this navigation technique. Chapter 2 represents a
comprehensive review of the existing work on spinal navigation and intra-operative imaging
techniques. The final section of this chapter outlines the research questions and hypotheses
addressed in the remainder of the thesis. Chapters 3-9 present original research addressing each
of these objectives, each as a self-contained manuscript. Chapter 3 is a reformatted version of a
manuscript currently in submission for publication. Chapter 4 is a reformatted version of a paper
published in The Spine Journal.(Guha, Jakubovic, Gupta, Alotaibi, et al., 2017) Chapters 5-9 are
reformatted versions of manuscripts submitted for journal publication. The discussion sections in
each of the data chapters (3-9) are complemented by Chapter 10, in which a general summary
and discussion of the thesis findings are presented, along with ongoing and specific future
directions for this work.

2
Chapter 2 Intra-Operative Spinal Navigation
Introduction
This review chapter is divided into 4 primary sections. The first (Section 2.1) discusses the
history and evolution of intra-operative computer-assisted navigation, beginning with a brief
introduction of frame-based stereotaxis and subsequently exploring the development of frameless
techniques and their extension to spinal applications. Section 2.1 concludes by delineating the
clinical rationale as well as limits to adoption of spinal navigation techniques. Section 2.2 briefly
summarizes current imaging and registration techniques for contemporary navigation systems,
including their relative merits and drawbacks. Section 2.3 describes how navigation systems are
currently evaluated in the literature. Finally, Section 2.4 outlines the specific hypotheses and
objectives addressed by the original research in this thesis.
2.1 Evolution of Computer-Assisted Navigation
Navigation, the “process or activity of accurately ascertaining one’s position and planning and
following a route” as defined by the Oxford English Dictionary, began in its earliest forms
through nautical charts and instruments used by sailors for guidance. In surgery, maintaining the
complex 3D relationships between anatomical targets and instruments is paramount to safe and
effective interventions. The earliest surgical navigation systems were developed in neurosurgery,
to correlate external cranial anatomy to underlying internal structures intra-operatively. In 1908
Horsley and Clarke coined the term ‘stereotactic’ in describing a novel device allowing the
placement of intracranial electrodes into precise targets in an animal model, using a rigid frame
(Figure 2-1).(E. A. C. Pereira, Green, Nandi, & Aziz, 2008)

3
The first human clinical application of frame-based stereotaxy was by Spiegel and Wycis in the
1940s, using a Cartesian coordinate system.(Spiegel, Wycis, Marks, & Lee, 1947) Subsequent
development for use with emerging cross-sectional imaging modalities, including computed
tomography (CT) and magnetic resonance imaging (MRI), led to the introduction of rigid frame
and arc localization systems including the eponymous Leksell frame, Brown-Roberts-Wells
(BRW) and Cosman-Roberts-Wells (CRW) systems, and the lesser-used Zamorano-Dujovny and
Patil frames.(Patil, 1984; T. Roberts, 1998; L. Zamorano, 1999) In each of these systems, the
rigid frames are affixed to the skull using pins under local anesthesia, to establish a fixed
relationship between the patient’s skull and the frame ± arc localizer, allowing the rapid and
accurate targeting of intracranial structures due to the known and constant relationship between
skull anatomy and frame system.
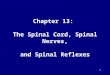
Figure 2-1. The earliest frame-based stereotaxy. Clarke and Horsley’s primate stereotactic apparatus. Reprinted
from Pereiera et al., Stereotactic Neurosurgery in the United Kingdom: The Hundred Years from Horsley to Hariz.
Neurosurgery 2008;63(3):594-607, by permission of Oxford University Press.

4
2.1.1 History of Frameless Stereotaxy
With rapid advances in imaging and computing power over the past three decades, frameless
stereotaxy, also termed image-guided surgery (IGS), neuronavigation, or computer-assisted
navigation (CAN), was pioneered again first in a neurosurgical context. While frame-based
stereotaxy is still used for biopsies and implantation of depth electrodes for neuronal recording,
stimulation or ablation, the development and iterative improvement in frameless stereotaxy has
allowed the extension of stereotactic guidance to craniotomies for a variety of indications, as
well as to spinal procedures, the focus of this thesis. The use of CAN is particularly critical in
neurosurgical applications, as delicate neuronal tissues limit the corridors of direct visualization
available in many other surgical disciplines.
Frameless stereotaxy, by virtue of its lack of a rigid mechanical linkage between the patient
anatomic space and the instrument space, as accomplished by frame ± arc localizers, therefore
requires the matching of patient and device (or image) spaces, a process termed registration. The
first clinical application of frameless stereotaxy was by Friets and Roberts et al. in the 1980s,
where an operating microscope with ultrasonic emitters was placed in an operating room (OR)
with surrounding microphones outside the operating field to localize the position of the
microscope in relation to the patient, allowing the injection of a target point on cross-sectional
imaging into the microscope oculars (Figure 2-2).(Friets, Strohbehn, Hatch, & Roberts, 1989;
David W. Roberts, Strohbehn, Hatch, Murray, & Kettenberger, 1986; D W Roberts, Hartov,
Kennedy, Miga, & Paulsen, 1998) Groundwork for subsequent integration of cross-sectional
imaging into the patient anatomic space, a pre-requisite for modern CAN, was laid by the work
of Kelly and others, by reconstructing volumetric data from CT and later MRI into 3D
space.(Kelly, 1990) The first frameless CAN devices, tracking pointers initially using ultrasonic
emitters and subsequently magnetic sources and infra-red (IR) light-emitting diodes (LEDs),
were developed in the late 1980s and early 1990s for intracranial and otolaryngologic
applications, first with arm-based systems and subsequently with armless devices.(Kato et al.,
1991; Kosugi et al., 1988; Mösges & Schlöndorff, 1988; Reinges, Spetzger, Rohde, Adams, &
Gilsbach, 1998; H. Reinhardt, Meyer, & Amrein, 1988; Watanabe, Mayanagi, Kosugi, Manaka,

5
& Takakura, 1991; Watanabe, Watanabe, Manaka, Mayanagi, & Takakura, 1987; L. J.
Zamorano, Nolte, Kadi, & Jiang, 1993)
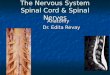
Figure 2-2. An early frameless stereotactic navigation system. Photograph of one of the first clinical frameless
stereotactic navigation systems, employing an operating microscope (top right) fitted with an array of spark-gap
ultrasonic emitters (top left) for tracking of the microscope position relative to the patient, to allow injection of a target
into the microscope oculars using a beam-splitting device (bottom right). Reprinted from Roberts et al., A Frameless
Stereotaxic Integration of Computerized Tomographic Imaging and the Operating Microscope. JNS 1986;65(4):545-9,
by permission of the JNS Publishing Group.
2.1.2 History of Spinal Computer-Assisted Navigation
Prior to the advent of CAN, intra-operative navigation in the spine was typically performed using
a combination of anatomic knowledge as well as radiographic feedback from serial XR (X-rays)

6
or fluoroscopy. Additional feedback on the integrity of adjacent neural elements was, and
continues to be, obtained with the use of various electromyography (EMG) and direct
stimulation-based neuromonitoring techniques.(Holly & Foley, 2003) While plain XR remains
useful for the initial localization of a skin incision or vertebral levels, it is associated with a
significant time lag particularly when digital radiograph processing units are unavailable, and
provides only a single temporal snapshot. Poor image quality due to metallic artifact, bony
obstruction or large patient body habitus, requires repeated XR and therefore increases this time
cost. C-arm fluoroscopy has therefore traditionally been the imaging modality of choice for
many spinal surgeons for intra-operative guidance. C-arms may provide a single XR snapshot for
incision and anatomic level localization, and may also acquire continuous images to allow for
real-time localization of instruments in the operative field. However, this practice is associated
with significant occupational radiation exposure, particularly to the surgical team. Extensive
investigation has been performed on the cumulative radiation dose from C-arm fluoroscopy to
various parts of the surgeon’s body, at various positions around the operative table (i.e. on the
side of the detector vs. emitter), with varying patient body habitus, and with the duration of
fluoroscopy.(Mroz, Abdullah, Steinmetz, Klineberg, & Lieberman, 2011; Mulconrey, 2016;
Rampersaud, Foley, Shen, Williams, & Solomito, 2000; H. E. Smith, Welsch, Sasso, & Vaccaro,
2008) Moreover, standard C-arm fluoroscopy only provides a single in-plane view, with multiple
planes possible only with the introduction of a second orthogonally-positioned C-arm or by
moving the single C-arm back and forth to the required planes, a cumbersome and
ergonomically-disruptive exercise (Figure 2-3).(Tjardes et al., 2010; Xu et al., 2014)

7
Figure 2-3. Intra-operative biplane fluoroscopy. Typical operating room setup when two C-arm units are required
concurrently for biplane (antero-posterior and lateral) views for spinal instrumentation guidance. Reprinted from Xu et
al., A Method of Percutaneous Vertebroplasty Under the Guidance of Two C-Arm Fluoroscopes. Pak J Med Sci
2014;30(2):335-8, under the Open Access Creative Commons Attribution License 3.0.
Extension of computer-assisted navigation from cranial to spinal procedures was therefore a
natural target. The evolution from early arm-based CAN techniques to armless systems was
enabled by the development of dynamic reference frames (DRFs), consisting of an
electromagnetic coil or active or passive IR-LED arrays affixed to rigid bony anatomy. This
allowed the tracking of instruments in the patient space without rigid anatomic fixation, as is
typically accomplished in cranial neurosurgery with the use of rigid head fixation devices such as
the Mayfield or Sugita clamps, but is not feasible in spinal approaches.(Grunert, Darabi,
Espinosa, & Filippi, 2003) Kalfas et al. were the first to adapt frameless stereotaxy for clinical
use in the spine in the mid-1990s, using a wand fitted with ultrasonic emitters allowing tracking
using sonic digitizers placed around the operating field, registered to a pre-operatively-acquired
volumetric CT dataset (Figure 2-4).(Kalfas et al., 1995; Murphy, McKenzie, Kormos, & Kalfas,

8
1994) Subsequent development in the late 1990s expanded the scope of spinal CAN to include
updating of imaging in real-time intra-operatively using C-arm fluoroscopy, termed ‘virtual
fluoroscopy’.(Foley, Simon, & Rampersaud, 2001; T.-S. Fu et al., 2004) Unfortunately, virtual
fluoroscopy systems remained limited to 2D projection images, without true multiplanar views in
the axial, sagittal and coronal planes.(Helm, Teichman, Hartmann, & Simon, 2015) 3D CAN
systems, based initially on pre-operative CT imaging and subsequently on intra-operative mobile
CT as as well as isocentric C-arm fluoroscopy, therefore arose to the forefront starting in the
early 2000s.(Euler, Heining, Fischer, Pfeifer, & Mutschler, 2002; Nolte et al., 2000; Waschke et
al., 2013) These early imaging devices remained limited by poor image quality and cumbersome
workflow. A major step forward in spinal intra-operative imaging and navigation was taken in
2006, with the introduction of the O-Arm™ by Breakaway Imaging (now Medtronic), allowing
360° cone-beam CT-quality imaging with a breakable gantry facilitating movement around the
operating table, and automatic registration to the patient spinal anatomy.(Helm et al., 2015) A
full discussion of contemporary spinal CAN imaging and registration techniques is presented in
Section 2.2 of this chapter.

9
Figure 2-4. The first spinal intra-operative navigation system. Photograph of the acoustic frameless stereotactic
navigation system devised by Kalfas et al. for spinal pedicle screw guidance. The black sonic digitizer is mounted on
a platform next to the operating table. Reprinted from Kalfas et al., Application of Frameless Stereotaxy to Pedicle
Screw Fixation of the Spine. JNS 1995;83(4):641-7, by permission of the JNS Publishing Group.
2.1.3 Current Applications of Spinal Computer-Assisted Navigation
The first spinal CAN systems were used to guide the placement of lumbar pedicle
instrumentation.(Kalfas et al., 1995; Murphy et al., 1994) In the two decades following,
instrumentation placement remains the primary application of contemporary spinal image-
guidance systems, with a body of literature encompassing over 10,000 pooled pedicle
screws.(Overley, Cho, Mehta, & Arnold, 2017) CAN systems have been used to guide pedicle
screws from the atlantoaxial (C1-C2) and subaxial cervical spine,(Shimokawa & Takami, 2016b;
J. D. Smith, Jack, Harn, Bertsch, & Arnold, 2016) down to the sacrum and pelvis.(Ray,
Ravindra, Schmidt, & Dailey, 2013; J. H. Shin, Hoh, & Kalfas, 2012) While there is literature to
suggest that the freehand placement of standard posterior thoracolumbar and sacral pedicle

10
screws may be safe in highly-trained hands, CAN systems have expanded the accessibility of
accurate and safe placement of instrumentation at these levels, particularly in revision and
deformity-correction cases where typical anatomic landmarks are distorded, as discussed in
greater detail in Section 2.1.3.1 of this chapter.(Fridley, Fahim, Navarro, Wolinsky, & Omeis,
2014; Y. J. Kim, Lenke, Bridwell, Cho, & Riew, 2004) CAN has also facilitated novel
instrumentation approaches that are otherwise feasible only with repeated fluoroscopy, including
odontoid screw placement at C2,(Pisapia et al., 2017) oblique prepsoas and extreme lateral
transpsoas approaches to the lumbar spine,(DiGiorgio, Edwards, Virk, Mummaneni, & Chou,
2017; Joseph, Smith, Patel, & Park, 2016) as well as percutaneous and minimally-invasive
instrumentation at all spinal levels.(T. T. Kim, Drazin, Shweikeh, Pashman, & Johnson, 2014; T.
T. Kim, Johnson, Pashman, & Drazin, 2016; Komatsubara, Tokioka, Sugimoto, & Ozaki, 2016;
Nakashima, Sato, Ando, Inoh, & Nakamura, 2009)
The utility of modern CAN techniques has expanded from instrumentation to guidance and
confirmation of the extent of decompression. Navigation guidance for anterior transoral
approaches to the craniocervical junction, for inflammatory and neoplastic etiologies, has been
reported as early as 2003 by Vougioukas et al..(Vougioukas, Hubbe, Schipper, & Spetzger,
2003) More recently, anterior CAN-guided subaxial cervical transcorporal tunnel approaches to
treat focal pathology underlying cervical myelopathy, have been reported.(Quillo-Olvera, Lin,
Suen, Jo, & Kim, 2017) Ligamentous decompression with MIS epiduroscopic laser ablation in
the lumbar spine may also be guided by modern CAN techniques.(Jeon et al., 2015) Osteotomies
for correction of spinal alignment, with or without instrumentation, may also be guided by CAN
techniques in order to precisely plan, pre-operatively, and subsequently execute, intra-
operatively, the specific bony extirpations required to achieve a desired alignment.(Metz &
Burch, 2008) In an oncologic context, the extent of osseous and soft-tissue tumour
decompression may be guided and confirmed by intra-operative CAN, particularly when coupled
with CT/MRI fusion techniques and intra-operative imaging.(Bandiera et al., 2013) CAN
guidance may facilitate less invasive ‘separation surgery’ for metastatic epidural disease,
whereby a transpedicular approach is used to resect sufficient tumour lateral and ventral to the
spinal cord to allow safe high-dose fractionated radiation therapy with minimal
neurotoxicity.(Nasser et al., 2018) At the extremes of minimally-invasive surgery, CAN may

11
guide percutaneous catheters for laser interstitial thermal therapy (LITT), with the purpose of
ablating epidural tumour similar to ‘separation surgery’.(Tatsui et al., 2017) By merging pre-
operative MRI and intra-operative 3D fluoroscopic images, CAN may also be facilitate the
resection of intradural tumours, by minimizing the extent of soft-tissue and bony exposure and,
for intrinsic spinal cord tumours, centering the tumour to more precisely localize the midline
myelotomy.(Stefini, Peron, Mandelli, Bianchini, & Roccucci, 2017)
While infusion and neuromodulatory therapies for spinal chronic pain conditions are typically
performed safely and easily freehand, such as with the implantation of dorsal root ganglion
stimulation electrodes, CAN may be useful in cases of severely distorted or disrupted anatomy,
such as in one series of intrathecal baclofen pump catheter implantation in cerebral palsy patients
with severe neuromuscular scoliosis.(Robinson et al., 2017)
Finally, CAN may play a significant role in trainee surgeon education. While expert spine
surgeons are able to place instrumentation safely freehand or with fluoroscopic guidance, the
real-time visualization and verification of anatomic landmarks and proposed trajectories that is
afforded by intra-operative CAN may be a useful adjunctive pedagogic tool. To date, seven
studies have reported on the use of CAN for surgical resident and clinical fellow education, all in
the context of ex-vivo virtual reality (VR) or cadaveric or phantom simulations.(Gasco et al.,
2014; Michael B. Gottschalk, Yoon, Park, Rhee, & Mitchell, 2015; Lorias-Espinoza, Carranza,
de León, Escamirosa, & Martinez, 2016; Luciano et al., 2011; Podolsky et al., 2010; Rambani,
Ward, & Viant, 2014; Sundar et al., 2016) The consensus from these studies, through self-
reported surveys, is that CAN simulation is a useful exercise for training novice learners.
Objective improvement, however, in simulation performance such as the placement of
instrumentation, with CAN guidance, remains less well established. Gasco et al., Rambani et al.,
and Sundar et al. found significant improvements in simulation performance for screw placement
with CAN-based simulation training, while Gottschalk et al. found improvement only in screw
trajectory but not in entry point placement, and Podolsky et al. found no improvement in
radiographic screw accuracy.

12
2.1.3.1 Rationale for Spinal Computer-Assisted Navigation
CAN was applied to spinal procedures initially for the guidance of lumbar pedicle screws.
Instrumentation guidance remains the primary application for CAN by most spinal surgeons,
with multiple systematic reviews and meta-analyses reporting on the radiographic accuracy of
pedicle screws in the cervical, thoracic and lumbosacral spine, and in multiple clinical contexts
including minimally-invasive percutaneous instrumentation as well as in adolescent idiopathic
scoliosis patients.(L. P. Amiot, Lang, Putzier, Zippel, & Labelle, 2000; Austin C Bourgeois et
al., 2015; Chan, Parent, Narvacan, San, & Lou, 2017; Du et al., 2018; Gelalis et al., 2012;
Luther, Iorgulescu, Geannette, Gebhard, Saleh, Tsiouris, & Härtl, 2015; Mason et al., 2014; B. J.
Shin, James, Njoku, Hartl, & Härtl, 2012; N. F. Tian et al., 2011; Verma, Krishan, Haendlmayer,
& Mohsen, 2010) Comparison of radiographic accuracy of pedicle screw placement between
navigated and freehand, or conventional fluoroscopy, technqiues was made most recently in a
meta-analysis by Mason et al..(Mason et al., 2014) This analysis found an overall radiographic
accuracy rate, across all spinal regions, of 68.1% for freehand techniques, vs. 84.3% for 2D
navigation and 95.5% for 3D navigation, with all 3D techniques pooled (isocentric fluoroscopy,
cone-beam CT, fan-beam CT). Primary studies included in this meta-analysis are shown in Table
2-1, and a stratification of accuracy by spinal region is shown in Figure 2-5. Further stratification
of navigated pedicle screw accuracy was made most recently by Du et al., in a meta-analysis
comparing specifically 3D fan-beam CT vs. 3D isocentric fluoroscopy (Table 2-2).(Du et al.,
2018) Interestingly, although the diagnostic accuracy of isocentric fluoroscopy for intra-
operative pedicle breach identification has compared favourably to post-operative CT in prior
studies,(Qureshi, Lu, McAnany, & Baird, 2014) the analysis by Du et al. found greater
radiographic screw accuracy with isocentric fluoroscopy rather than CT-based navigation. This
has potential implications from a hospital/departmental purchasing perspective, whereby less-
costly isocentric fluoroscopy units may become more attractive in the context of spinal
navigation. Within CT-based systems, there does not appear to be a significant difference in
accuracy between systems registering to pre- vs. intra-operatively-acquired CT, however in
current paradigms the intra-operative CT-based systems register significantly faster due to

13
automatic registration protocols.(Francesco Costa et al., 2011) Nooh et al. report that differences
in accuracy may exist even across manufacturers of CAN devices employing similar registration
and imaging modalities.(Nooh et al., 2017)
Figure 2-5. Radiographic accuracy of pedicle screws. Boxplots comparing the accuracy of pedicle screws across
all regions (A), and specifically in the thoracic spine (B) and lumbosacral spine (C). placed using
freehand/conventional fluoroscopy guidance vs. 2D navigation vs. 3D navigation. Boxes represent the interquartile
range; black lines within boxes represent the mean screw accuracy; error bars represent minimum and maximum
values. Reprinted from Mason et al., The Accuracy of Pedicle Screw Placement Using Intraoperative Image
Guidance Systems. JNS: Spine 2014;20(2):196-203, by permission of the JNS Publishing Group.

14
Table 2-1. Studies of pedicle screw accuracy. Articles are stratified by spine region and insertion technique.
Reprinted from Mason et al., The Accuracy of Pedicle Screw Placement Using Intraoperative Image Guidance
Systems. JNS: Spine 2014;20(2):196-203, by permission of JNS Publishing Group.

15

16
Table 2-2. Studies of pedicle screw misplacement. Articles are stratified by insertion technique, specifically with
distinction among 3D CT vs. fluoroscopic guidance. Reprinted from Du et al., Accuracy of Pedicle Screw Insertion
Among 3 Image-Guided Navigation Systems: Systematic Review and Meta-Analysis. World Neurosurg 2018;109:24-
30, by permission of Elsevier.

17
As the benefits of CAN are most evident in MIS and deformity-correcting procedures, where
anatomic landmarks are less readily identifiable, the advantage of CAN in potentially reducing
intra-operative fluoroscopy and its associated radiation cost in MIS procedures, has also come
under significant investigation. Intra-operative fluoroscopy, the current gold-standard for the
evaluation of real-time instrument positioning and spinal alignment, is associated with an
average dose to the surgeon of 53.3 mrem/min at the torso in one study, greater in the hand and
less in the neck, with variation in dose based on distance from the beam source and patient body
habitus.(Rampersaud et al., 2000) A multitude of subsequent studies has demonstrated reduced
occupational radiation dose, i.e. to OR personnel, with 3D fluoroscopy-based navigation,(Foley
et al., 2001; Izadpanah, Konrad, Südkamp, & Oberst, 2009; Schafer et al., 2011) as well as with
intra-op CBCT,(Abdullah et al., 2012; Bandela et al., 2013; Mendelsohn et al., 2016) relative to
standard C-arm fluoroscopy. However, while CAN reduces the radiation exposure to surgical
and OR personnel, it does appear that this is more a result of shifting the burden of radiation to
the patient rather than a reduction in overall radiation exposure. Early spinal CAN systems
registered to pre-operative CT imaging, with the radiation cost to the patient of dedicated spinal
imaging exceeding that of any other non-spinal musculoskeletal CT imaging by 10-12
fold.(Biswas et al., 2009) With the development of more advanced CAN techniques registered to
intra-operative imaging, the argument has been made that intra-operative 3D fluoroscopy or
CBCT can both guide instrumentation as well as provide post-implantation imaging to check
hardware accuracy, as a replacement for the otherwise obligate post-operative CT scan.
However, particularly with larger patients, with longer instrumentation constructs, or with any
inadvertent shifting of the DRF intra-operatively or other source of navigation error, multiple
intra-operative imaging sequences may be required. Lange et al. have estimated that 3 or more
intra-operative O-Arm imaging cycles, at standard manufacturer-recommended dosing, results in
patient radiation exposure equivalent to that one of standard abdominal CT scan.(Lange et al.,
2013) Therefore, while CAN techniques may reduce occupational radiation exposure for OR
personnel, particularly in traditionally fluoroscopy-heavy procedures including MIS and
deformity corrections, the burden of radiation exposure remains, and in the current paradigm of
CAN techniques is shifted to the patient rather than eliminated entirely.(Bandela et al., 2013)

18
With an increasing focus on value-based health care and efficiency optimization, CAN
techniques have also been purported to improve surgical temporal workflow thereby reducing
costly OR time.(G. Fan et al., 2017) Prolonged operative times have been associated with
increased blood loss and more frequent infectious and ischemic complications,(Baig et al., 2007)
though certainly there remains significant equipoise on this point in the literature, and the
majority of surgical morbidity likely remains secondary to patient comorbidities and the treated
pathology rather than operative time alone.(Fogarty, Khan, Ashall, & Leonard, 1999) While
perhaps not dramatically reducing operative times compared to traditional fluoroscopy-guided or
freehand techniques, the use of CAN appears to be at least time-equivalent. In a comparative
study of O-Arm (3D cone-beam CT) vs. fluoroscopy guidance for MIS lateral interbody lumbar
fusions, Zhang et al. demonstrated a statistically-insignificant increase in operative time with
CAN guidance.(Y.-H. Zhang, White, Potts, Mobasser, & Chou, 2017) However, Sasso et al.
demonstrated a statistically-significant time savings in posterior L5-S1 fusions with 3D
fluoroscopy vs. serial XR.(Sasso & Garrido, 2007) In a cadaveric setting, Webb et al. found total
operative time-equivalence for CAN-guided lateral interbody thoracolumbar fusion vs.
fluoroscopy.(Webb, Regev, Garfin, & Kim, 2010) In larger in-vivo comparative studies, both
Rajasekaran et al. and Tabaraee et al. found time-equivalence for 3D CBCT-based navigation vs.
fluoroscopy for the placement of posterior thoracolumbar pedicle screws.(Rajasekaran,
Vidyadhara, Ramesh, & Shetty, 2007; Tabaraee et al., 2013) While a temporal efficiency benefit
to CAN has yet to be demonstrated with current paradigms of navigation, there does appear to be
a significant learning curve, with increased operative times early in the curve followed by time
equivalence or even modest savings once sufficient familiarity has been achieved. While no
specific number of cases to achieve ‘competence’ has been postulated in the literature, a
significant improvement in radiographic instrumentation accuracy was observed by Wood et al.
after 50 cases of CT CAN-guided MIS lumbar pedicle screw placement.(Wood & McMillen,
2014) Ryang et al. demonstrated substantial and statistically-significant continual improvements
in both temporal efficiency and radiographic instrumentation accuracy with 3D-fluoroscopy
guided open thoracolumbar pedicle screw placement.(Ryang et al., 2015) In fact, the learning
curve in Ryang et al.’s study extended to the radiology technicians operating the 3D-fluoroscopy
CAN system, with continual improvements in scan time over the duration of the study. It
therefore appears from the body of literature that while the current paradigm of spinal CAN does
not offer significant workflow improvements relative to traditional fluoroscopy, time-

19
equivalence can typically be achieved following a significant learning curve for both surgeons
and involved OR personnel.
In part from purported time savings, and in greater part from a potential reduction in
complications and subsequent reoperations from misplaced instrumentation, an argument in
favour of spinal CAN usage has been made from an economic and cost-effectiveness
perspective. The literature on this subject is only recently beginning to expand, partly because
comparative data on clinical complications and reoperation rates from CAN vs. traditionally-
guided instrumentation has required long-term follow-up for adequate analysis. In the earliest
economic analysis of CAN guidance, Watkins et al. found a non-statistically-significant
reduction in revision surgeries for misplaced hardware with 3D-fluoroscopy guidance (0.2%, vs.
3% with traditional fluoroscopy), with an associated cost of revision surgery of USD $23,762
assuming a hospital stay of two nights.(Watkins, Gupta, & Watkins, 2010) Their navigation
system of choice, a 3D-fluoroscopy unit, had an upfront cost of USD $475,000, not including
annualized maintenance costs. In more recent studies, Hodges et al. approximated a 1% rate of
revision surgery for thoracolumbar pedicle screws placed with traditional C-arm fluoroscopy, vs.
0% with O-Arm CBCT guidance, at an average revision surgery cost of $17,650.(Hodges, Eck,
& Newton, 2012) Sanborn et al. concluded that intra-operative O-Arm CBCT imaging was a
cost-effective alternative to neuromonitoring or post-operative CT scanning for the confirmation
of screw placement, albeit with a flawed analysis that accounted only for personnel costs of the
imaging or monitoring techniques, and therefore attributed a cost of zero to O-Arm imaging.(M
R Sanborn et al., 2012) Costa et al. compared OR costs of instrumented fusion procedures using
a pre-operative CT-based CAN device vs. an O-Arm CBCT-based device, and concluded a non-
significant cost savings of only 3.8% with CBCT due entirely to an average time savings of 27
minutes using intra-operative imaging as a result of the automated registration protocol, with no
difference in clinical complications.(F Costa et al., 2014) In the most thorough analysis to date,
Dea et al. performed a retrospective comparative study of a prospectively-maintained cohort of
patients undergoing posterior spinal instrumentation with either O-Arm CBCT-CAN or standard
C-arm fluoroscopy. They concluded a cost of reoperation of CAD $12,618, and a statistically-
significant reduction in revision surgery rate of 5.2% with CAN guidance, thereby concluding
cost-effectiveness of the CAN technique if more than 254 instrumented cases per year are

20
performed at a given institution.(Dea et al., 2016) In this study, as a result of higher revision
surgery costs, cost-effectiveness in the United States was achieved at a fewer number of cases,
168 per year. Recent data supports improved short-term clinical outcomes with CAN usage, with
reduced 30-day reoperation rates for hardware malposition-related neurovascular complications
as well as wound infections.(Fichtner et al., 2017; Luther, Iorgulescu, Geannette, Gebhard,
Saleh, Tsiouris, & Härtl, 2015; Xiao et al., 2017) When long-term complications of misplaced
hardware, including poor osseous fusion and construct loading leading to junctional failure, are
taken into account, the economic argument in favour of CAN likely becomes more
robust.(Acikbas, Arslan, Tuncer, Matge, & Muciejczak, 2003)
Despite the increasing range of applications for spinal CAN described in the literature,
summarized in Section 2.1.3, adoption of CAN among spinal surgeons remains limited, without
establishment of the technology as standard of care.(Schröder & Wassmann, 2006) In the only
study to date quantifying the current state of navigation usage, Hartl et al. surveyed a worldwide
population of 3348 spinal surgeons, predominantly based in Europe, Latin America and the Asia
Pacific region, and found a worldwide CAN usage rate of only 11%.(Hartl et al., 2013) By
contrast, 78% of surgeons in the same survey reported using fluoroscopy as their primary method
of intra-operative image guidance. In separate surveys by Hartl et al. and Choo et al., the
predominant barriers to spinal CAN adoption were a definitive lack of evidence supporting
improved accuracy, workflow disruption primarily from cumbersome registration protocols, high
capital costs, increased radiation exposure to either the patient and/or OR personnel, and steep
learning curves.(Choo, Regev, Garfin, & Kim, 2008; Hartl et al., 2013) With a body of literature
reporting the safe and accurate placement of thoracic pedicle screws with freehand technique in
highly-experienced hands,(Y. J. Kim et al., 2004) and lack of definitive clinical benefit and
complication reduction with the use of CAN, albeit in short-term follow-up,(Wagner et al., 2017)
it is unsurprising that significant barriers remain to the widespread of adoption of CAN.

21
2.2 Registration, Imaging and Actuation Techniques in Spinal Computer-Assisted Navigation
The basic tenet of intra-operative computer-assisted image guidance is real-time correlation of
cross-sectional imaging data to patient anatomy, to provide surgeons with a view of structures
that cannot otherwise be visualized directly. A unifying requirement for any frameless
stereotactic navigation technique, in the spine or elsewhere, is registration of the imaging and
patient spaces. The imaging dataset to be registered to, and the technique for registration itself,
vary widely among various CAN techniques. A brief summary of imaging and registration
techniques in contemporary CAN systems is presented in this section.
2.2.1 2D Navigation
While the first published spinal CAN system provided 3D navigation based on a preoperative CT
(see Section 2.1.2),(Kalfas et al., 1995) the prevalence and relative compactness of C-arm
fluoroscopy units rendered 2D navigation, or ‘virtual fluoroscopy’, the next step in evolution.
Imaging in 2D navigation is performed using a standard C-arm fluoroscope modified with an
attached calibration target. In typical workflow, a dynamic reference frame (DRF) is affixed to
rigid patient anatomy, and XR images are taken with the C-arm in the planes desired for
navigation (typically a cross-table lateral for sagittal views, and an antero-posterior (AP) view).
As most ‘virtual fluoroscopy’ systems rely on optical instrument tracking (discussed further in
Section 2.2.3), a separate IR camera tracks the relative position of the C-arm (specifically the
attached calibration target) and patient-mounted DRF during XR imaging, and automatically
computes the transformation matrix required to register patient and image spaces. The position of
tracked instruments can then be overlaid on the multiplanar XR images to allow for real-time
navigated surgery with only the single fluoroscope(Figure 2-6).(Foley et al., 2001)
Unfortunately, as their name belies, 2D navigation systems are hampered by their inability to
display reconstructed axial views, leaving surgeons to mentally reconstruct the imaged planes
into a 3D structure. Moreover, as with all plain radiographs, the quality of navigation images is

22
entirely dependent on the quality of the initial acquisition XR, leaving much to be desired in
obese or osteopenic patients.(Helm et al., 2015; Holly & Foley, 2003) As 2D navigation
techniques have largely fallen out of favour due to their lack of multiplanar (MPR)
reconstruction, the remainder of this thesis will focus fully on 3D CAN technqiues.
Figure 2-6. ‘Virtual’ (2D) fluoroscopy. Navigation screenshot of an odontoid screw guided by virtual fluoroscopy.
Navigated instrument trajectory (grey + white lines) is overlaid on lateral (left) and antero-posterior (right) XR views.
Reprinted from Holly et al., Intraoperative Spinal Navigation. Spine 2003;28(15S):S54-61, by permission of Wolters
Kluwer Health, Inc.

23
2.2.2 3D Navigation
By definition, 3D CAN techniques provide full multiplanar reconstruction of cross-sectional
imaging, displaying the relevant anatomy in axial, sagittal and coronal planes and, depending on
the software package used, in a 3D reconstruction. All current spinal 3D CAN techniques are
reliant on a DRF for maintaining image-to-patient registration and instrument tracking. The
imaging modalities and techniques used to register this imaging to real-world anatomy vary
among systems, and are discussed further in this section.
2.2.2.1 Imaging Techniques
Imaging for navigation in 3D CAN techniques may be acquired either pre- or intra-operatively.
Among systems registering to pre-operative imaging, the most common imaging dataset is spiral
CT, best if acquired at high-resolution thin slices of thickness <2mm.(Herz, Franz, Giacomuzzi,
Bale, & Krismer, 2003) The typical workflow for pre-operative CT-based techniques involves
transferring of Digital Imaging and Communications in Medicine (DICOM) files to the CAN
workstation pre-operatively. A DRF is affixed to the patient, and manual registration of the pre-
operative CT dataset to patient anatomy is then performed using one of three techniques,
described in greater detail in Section 2.2.2.2. Following successful image-to-patient registration,
MPR views of the registered anatomy are displayed on a screen, and image-guided surgery may
proceed. Pre-operative CAN systems remain of value as they obviate the need for bulky intra-
operative imaging devices, particularly in the case of intra-operative CT scanners, that are costly
to both acquire and maintain, often require specially-trained personnel to operate, and image at
lower resolution than the fan-beam medical-grade scanners used for pre-operative imaging.
However, the manual registration protocol of current CAN systems registering to pre-operative
imaging significantly increases operative times,(Parker et al., 2011) and necessitates a pre-
operative CT scan with its associated cost and patient radiation exposure.(A C Bourgeois,
Faulkner, Pasciak, & Bradley, 2015; Holly & Foley, 2003) The accuracy of the initial
registration is also highly operator-dependent, as the quality of selected points for paired-point

24
matching can significantly impact the robustness of the resultant transformation matrix.(Tamura
et al., 2005) Moreover, as these systems rely on an imaging dataset acquired with the patient in a
supine position, whereas most navigated spinal procedures are performed in the prone position,
intervertebral spinal mobility due to positioning may result in significant navigation inaccuracy,
particularly when operating at levels distant to which the DRF is affixed.(A C Bourgeois et al.,
2015; Holly & Foley, 2003; Kalfas et al., 1995; Ringel, Villard, Ryang, & Meyer, 2014) The
lack of associated intra-operative imaging also eliminates the ability to assess instrumentation
placement or spinal alignment without a separate intra-operative imaging device, or a dedicated
post-operative CT scan with its associated cost and patient radiation exposure.
In an effort to overcome some of these drawbacks associated with registration to pre-operative
imaging, 3D CAN systems with intra-operative imaging devices were developed. 3D intra-
operative imaging techniques include isocentric fluoroscopy, or ‘3D fluoroscopy’, cone-beam
CT (CBCT), and fan-beam CT (FBCT)(Figure 2-7). Isocentric fluoroscopy devices employ a C-
arm which is motorized to automatically rotate a fixed amount (typically 190°), centred about a
point in the spine chosen by the operator (hence ‘isocentric’). A DRF is affixed to patient
anatomy, as with all modern CAN techniques, and imaging proceeds with subsequent automatic
transferring of images to the CAN workstation and image-to-patient registration. The first CBCT
device, the O-Arm™ (Medtronic Sofamor Danek; Memphis, TN, USA), was introduced in 2006
and employs a similar fluoroscopy unit with flat-panel detector as isocentric fluoroscopy
devices.(Helm et al., 2015) The O-Arm is differentiated from isocentric fluoroscopy by its ability
to rotate a full 360°, optimizing volume sampling and minimizing reconstruction artifacts due to
limited projection views that are prominent with isocentric fluoroscopy devices. This is
permitted by its toroid form factor, with a breakable gantry allowing lateral access to the
operating table. DRF placement and automatic image transfer and registration otherwise
proceeds similar to isocentric fluoroscopy devices. The latest evolution in intra-operative
imaging devices is mobile multi-row fan-beam CT imagers, more similar in design to the fixed
scanners found in radiology departments than to the O-Arm.(Helm et al., 2015) These devices,
examples of which include the BodyTom™ (Samsung Electronics America; Ridgefield Park, NJ,
USA) and Airo™ (Brainlab AG; Munich, Germany), offer significantly better contrast resolution
than flat-panel cone-beam devices (isocentric fluoroscopy and CBCT) with comparable imaging

25
times. With a pre-calibrated relationship between CT gantry and operating table (and therefore
patient) position, image transfer and registration are automatic as with isocentric fluoroscopy and
CBCT devices. However, FBCT systems are associated with significantly greater capital cost,
due in part to the requirement for a dedicated operating room with proprietary attached operating
table to facilitate ingress/egress from the CT gantry. Without flat-panel detectors as with
standard C-arm fluoroscopes, FBCT devices also lack real-time fluoroscopy capabilities that are
useful for initial incision and vertebral level localization.(A C Bourgeois et al., 2015; Helm et al.,
2015) The adoption of FBCT systems has therefore been limited largely to highly-specialized
academic institutions, with an unclear role in the future of spinal CAN. Nonetheless, each of the
three intra-operative imaging technqiues has advanced spinal CAN, by improving workflow
through automated registration protocols, and providing real-time feedback on intra-operative
spinal alignment and hardware placement through repeat imaging cycles.
There is ample evidence in the literature to suggest that all intra-operative imaging techniques
reduce cumulative radiation dose to the surgeon and OR staff, as these personnel are typically
able to leave the OR while navigation and verification scans are being performed via automated
motorized actuation. Villard et al. demonstrated that the use of isocentric fluoroscopy, to guide
lumbar pedicle instrumentation as well as verify hardware position post-implantation intra-
operatively, reduces surgeon radiation exposure by almost 10-fold relative to standard
fluoroscopy.(Villard et al., 2014) They also found that the cumulative radiation dose to the
patient was halved, largely due to avoidance of a post-operative CT to verify screw position. In
more recent studies of CBCT systems, Costa et al. found an intra-operative radiation dose to
surgical staff that was essentially negligible, however with increased intra-operative exposure to
the patient relative to standard fluoroscopy.(Francesco Costa et al., 2016) Similarly, Mendelsohn
et al. found increased patient radiation exposure by 2.77 fold with CBCT navigation relative to
literature values for fluoroscopy-guided thoracolumbar instrumentation, however with negligible
surgeon radiation exposure.(Mendelsohn et al., 2016) Interestingly, they also found no difference
in the need for post-operative XR or CT in patients who had undergone a navigated vs. non-
navigated procedure, although their institution did not routinely perform intra-operative post-
implantation verification CBCT scans, which might otherwise have reduced the need for post-
operative scanning in the navigated cohort. Nonetheless, while all intra-operative imaging

26
devices reduce radiation exposure to OR personnel, the burden of exposure is shifted somewhat
to patients, to a significantly greater extent for CBCT/FBCT systems than with isocentric
fluoroscopy, with the tradeoff of improved image quality and potentially navigation accuracy
with CT systems.

27
Figure 2-7. Intra-operative imaging technqiues for 3D CAN. Photographs demonstrating the intra-operative setup
of mobile cone-beam CT (top left), isocentric fluoroscopy (top right), and fan-beam multidetector CT (bottom). Each
technique is associated with significant bulk and cumbersome additional draping requirements for the patient and/or
the imaging device. Top images reprinted from Bourgeois et al., The Evolution of Image-Guided Lumbosacral Spine
Surgery. Ann Trans Med 2015;3(5):69, by permission of the Society for Translational Medicine. Bottom image
reprinted from Tormenti et al., Intraoperative Computed Tomography Image-Guided Navigation for Posterior
Thoracolumbar Spinal Instrumentation in Spinal Deformity Surgery. Neurosurg Focus 2010;28(3):E11, by permission
of the JNS Publishing Group.

28
2.2.2.2 Registration Techniques
A fundamental requirement for any frameless stereotaxis is to identify a fixed relationship
between patient and image spaces, a process termed registration. A transformation must be
computed, which allows the mapping of any point in anatomical (real-world) space to its
corresponding point in image space, thereby allowing instrument tracking in both
environments.(Grunert et al., 2003) Broadly, the transformation (φ) linking corresponding points
or surfaces in imaging and patient spaces consists of a linear translation (�⃗�) and a rotational
matrix (B), which will align every point in the patient space (𝑄𝑖⃗⃗ ⃗⃗ ) to a corresponding point in the
imaging space (𝑃𝑖⃗⃗⃗) (Equation 1) (Eggers, Mühling, & Marmulla, 2006)
Equation 1: 𝜑(�⃗⃗�𝑖) = 𝐵 ∙ �⃗⃗�𝑖 + �⃗� = �⃗⃗�𝑖
Multiple techniques for image-to-patient registration have been proposed and iteratively refined
over the past three decades, and are described in greater detail in this section. Early CAN
techniques relied on paired-point matching, surface mapping, or a hybrid of these two techniques
for registration. The advent of intra-operative imaging suites, including isocentric fluoroscopy,
CBCT and FBCT, have allowed for automatic registration protocols. Regardless of registration
technique, in the current paradigm all techniques of spinal CAN first require a DRF to be rigidly
affixed to patient anatomy in the operative position, followed by execution of the relevant
registration process or intra-operative imaging with automatic registration. A given
transformation linking patient and imaging spaces would remain valid only while the patient
remained in the initial position; any movement of the patient or operating table following
registration would render the initial transformation obsolete, and a repeat calibration would have
to be performed. The presence of a patient- or operating table-affixed DRF therefore allows
some patient motion to be compensated for, with only movement relative to the DRF
unaccounted for by the initial registration transformation.

29
2.2.2.2.1 Paired-Point Matching
Paired-point transformation represents the earliest technique used to register imaging and patient
spaces, and was employed in the first cranial and spinal CAN systems.(Kalfas et al., 1995) Points
in the image space, a minimum of three, are matched to corresponding readily-identifiable points
in the patient space.(Eggers et al., 2006) Points in patient space may be anatomic bony or skin-
surface landmarks, adhesive skin-surface fiducials, or internal bone-affixed fiducials (Figure 2-
8). In spinal surgery, anatomic bony landmarks are most commonly used for paired-point
registration, due to the mobility and lack of adhesion of skin fiducials for posterior approaches,
in contrast to the relative immobility of the scalp for skin-adhesive fiducials in cranial
applications. Where skin-surface fiducials have been employed in spinal navigation, registration
errors have been unacceptably large, up to 2 cm at the level of the disc space.(Roessler et al.,
1997) Bone-implanted fiducials are demonstrably superior in registration accuracy to anatomic
or skin-marker fiducials, however are rarely used in spinal surgery due to their
invasiveness.(Mascott et al., 2006)

30
Figure 2-8. Paired-point image-to-patient registration. Demonstration of paired-point techniques for image-to-
patient registration in cranial neuronavigation. Points in the image space (bottom row) may be registered to
corresponding points in the patient anatomic space (top row), chosen using anatomic surface landmarks (A), skin-
adhesive fiducials (B), bone-implanted cranial fiducials (C), or manual surface mapping (D). Reprinted from Mascott
et al., Quantification of True In-Vivo (Application) Accuracy in Cranial Image-Guided Surgery: Influence of Mode of
Patient Registration. Neurosurgery 2006;59(1):ONS146-56, by permission from Oxford University Press.
The basic equation for a transformation matrix (T) linking the patient space (X) and image space
(X*) can be expressed in matrix notation (Equation 2)(Helm et al., 2015).
Equation 2: (
𝑥1 𝑦1 𝑧1
𝑥2 𝑦2 𝑧2
𝑥3 𝑦3 𝑧3
) ∗ (
𝑡11 𝑡12 𝑡13
𝑡21 𝑡22 𝑡23
𝑡31 𝑡32 𝑡33
) = (
𝑥1∗ 𝑦1
∗ 𝑧1∗
𝑥2∗ 𝑦2
∗ 𝑧2∗
𝑥3∗ 𝑦3
∗ 𝑧3∗)
The matrix (X) consists of the (x,y,z) coordinates of each of the three fiducial markers in the
patient space, while the matrix (X*) consists of the (x*, y*, z*) coordinates of the corresponding
points in the image space. The transformation matrix (T) consists of 9 parameters t which are to
(X) (T) (X*)

31
be calculated in the registration process. Using matrix multiplication, the registration protocol
must solve a set of linear equations to compute each variable of t (Equation 3)(Helm et al.,
2015).
{
𝑥1𝑡11 + 𝑦1𝑡21 + 𝑧1𝑡31 = 𝑥1∗
𝑥2𝑡11 + 𝑦2𝑡21 + 𝑧2𝑡31 = 𝑥2∗
𝑥3𝑡11 + 𝑦3𝑡21 + 𝑧3𝑡31 = 𝑥3∗
{
𝑥1𝑡12 + 𝑦1𝑡22 + 𝑧1𝑡32 = 𝑦1∗
𝑥2𝑡12 + 𝑦2𝑡22 + 𝑧2𝑡32 = 𝑦2∗
𝑥3𝑡12 + 𝑦3𝑡22 + 𝑧3𝑡32 = 𝑦3∗
{
𝑥1𝑡13 + 𝑦1𝑡23 + 𝑧1𝑡33 = 𝑧1∗
𝑥2𝑡13 + 𝑦2𝑡23 + 𝑧2𝑡33 = 𝑧2∗
𝑥3𝑡13 + 𝑦3𝑡23 + 𝑧3𝑡33 = 𝑧3∗
Once the transformation matrix (T), with each value for its component variables t, has been
computed in the registration protocol, the matrix (T) may be applied to any point in the patient
space (x, y, z) to map it to its corresponding point in the image space (x*, y*, z*), allowing real-
time image guidance. A minimum of three fiducial markers are required for this paired-point
registration, though certainly more may be used, with subsequent mathematics to use either the
best three fiducials which minimize the root-mean-square (RMS) error between the patient and
image spaces, or to use all fiducials and reduce the resulting overestimated linear equation
system to a set of three new computed coordinates.
In practice, while paired-point registration works well in principle with readily-identifiable
corresponding landmarks in both the patient and image spaces, it is time consuming intra-
operatively and often tedious if the desired anatomic landmarks cannot be localized precisely,
Equation 3:

32
and prone to error whenever fiducials other than radiolucent implanted markers are used,
impractical in most common procedures.(Mascott et al., 2006)
2.2.2.2.2 Surface Contour Matching
An alternative method of manual registration, attempting to overcome some of the drawbacks of
paired-point methodologies, is surface-based registration, described first by Pelizzari et al. in
1987.(Pelizzari & Chen, 1987) Fundamentally, surface registration techniques attempt to align
two surfaces, assumed to be rigid bodies, by iteratively applying scaling, translational and
rotational transformations until a particular distance or other error metric is minimized or
otherwise optimized.(Eggers et al., 2006; Helm et al., 2015) Scaling transformations are
represented by simple multiplication of an original surface, described by (X), by a scaling factor
(m), to generate the appropriately scaled surface (X*)(Equation 4).
Equation 4: 𝑋∗ = 𝑚(𝑋)
Translation in 3D space is defined by a vector transformation of every point in the original
surface, with coordinates (x, y, z), by a vector V consisting of three coordinates defining the
magnitude and direction of the translation (a, b, c), resulting in a surface at a novel position, with
coordinates for each point represented by (x*, y*, z*)(Equation 5).
Equation 5: (𝑥, 𝑦, 𝑧) + �⃗⃗�(𝑎, 𝑏, 𝑐) = (𝑥∗, 𝑦∗, 𝑧∗)

33
Rotational transformations may be described either by 3 (3x3) Euler matrices using Euler angles
corresponding to each of the 3 axes in Cartesian space, or by a single (3x3) matrix of unit
quaternions.(Helm et al., 2015; Stéphane Lavallee, 1996)
Surfaces in the imaging space are typically isolated from cross-sectional imaging by contouring
and thresholding algorithms, which are beyond the scope of this discussion. Surfaces in the
patient space may be acquired by a number of differing techniques. The earliest methods
acquired surfaces point by point using a tracked tool, a highly time-intensive and laborious
exercise (Figure 2-9).(Eggers et al., 2006) Laser contouring devices may also be used to scan
surfaces and are often used in commercial applications, however in their current form are
typically less accurate than marker-based point-matching techniques.(Schlaier, Warnat, &
Brawanski, 2002) Automated optical surface scanning via deformation of a projected structured-
light pattern may also be applied towards acquiring depth information in the patient
space.(Hoppe, Däuber, Kübler, Raczkowsky, & Wörn, 2002) This technique is the basis for
optical topographic imaging (OTI), described in greater detail in Section 2.2.2.2.5.

34
Figure 2-9. Manual surface mapping. Navigation display screenshot of a typical registration procedure using a
tracked pointer (blue) to manually select individual points (green dots) over the posterior osseous elements of a
lumbar vertebra, to generate a rudimentary surface map for subsequent image-to-patient registration. Reprinted from
Costa et al., Computed Tomography-Based Image-Guided System in Spinal Surgery: State of the Art Through 10
Years of Experience. Neurosurgery 2015;11(Suppl 2):59-67, by permission of Oxford University Press.
Registration of the surfaces in the imaging and patient spaces requires minimization of some
distance or error function between the two, with iterative applications of translational, scaling
and rotational transformations. Common error metrics include the Euclidean surface distance,
voxel congruence, information entropy, and mutual information functions.(S Lavallee, Szelisky,
& Brunie, 1996; van Herk & Kooy, 1994; Zeilenhofer et al., 1997) The most widespread and
best-established mathematical realizations in surgical navigation systems are variants of the
Iterative Closest-Point (ICP) algorithm, first described by Besi and Mackay and separately by
Chen and Medioni in the early 1990s (Figure 2-10).(Besi & Mckay, 1992; Y. Chen & Medioni,
1991) The original ICP algorithm minimized the point-to-point RMS distance error between the
two surfaces; subsequent variants have minimized point-to-plane RMS error or a combination of
the two. Any iterative technique is prone to failure by falling into local minima, that is, settling
on a solution for aligning the two surfaces that is relatively appropriate by some parameters but
is not the best possible match.(Helm et al., 2015) ICP algorithms in particular are also prone to

35
numerous other pitfalls, including failed registration from poor initial pose estimation due to
error in localizing fiducials or due to soft-tissue deformation,(Clements, Chapman, & Dawant,
2008; Maurer, Aboutanos, Dawant, Maciunas, & Fitzpatrick, 1996; Xin & Pu, 2010)
susceptibility to mismatched outliers,(Pomerleau, Colas, Siegwart, & Magnenat, 2013) and
inability to account for scaling differences between the initial point set alignments.(Ying, Peng,
Du, & Qiao, 2009) This has resulted in hundreds of variants of the original ICP algorithm
published in the past two decades.(Pomerleau et al., 2013) An outstanding pitfall of ICP variants
that remains unsolved is that of geometric congruence, that is, failure of the algorithm to
converge on a solution, or falling into local minima, in the presence of significant geometric
symmetry (congruence) in any number of configurations.(Armesto, Minguez, & Montesano,
2010; Gelfand, Ikemoto, Rusinkiewicz, & Levoy, 2003; Pottmann & Hofer, 2003) While
multiple proposed solutions to this error mechanism have been proposed, none have the required
accuracy or temporal efficiency to be feasible for intra-operative navigation.(Armesto et al.,
2010; Berner, Bokeloh, Wand, Schilling, & Seidel, 2008) Navigation error from ICP non-
convergence in geometrically-congruent surfaces therefore remains an ongoing potential pitfall.

36
Figure 2-10. Iterative Closest-Point registration. Simplified illustration of the iterative closest-point (ICP) method of
reconciling and aligning two surfaces or lines (blue and red). A set of points is chosen along each surface/line, and
the target surface/line (blue) iteratively scaled, translated and rotated until a cumulative distance error metric between
the point sets (black lines) is minimized. Reprinted from Smistad et al., Medical Image Segmentation on GPUs – A
Comprehensive Review. Med Image Anal 2015;20(1):1-18, under the Open Access Creative Commons Attribution
License 3.0.
2.2.2.2.3 Hybrid Matching
The accuracy of surface scanning techniques is known to diminish with distance from the
mapped surface.(Maurer, Jr. et al., 1995) A hybrid registration technique incorporating surface
mapping for initial registration, followed by refinement with paired-point matching using deeper
anatomic fiducials, has been proposed by Maurer et al.. Deep point-matching has been described
using a standard optically-tracked pointer, or with one-dimensional ultrasonic sensors applied
percutaneously to reduce invasiveness.(Schmerber et al., 1997) As navigation accuracy at
significant depth is most relevant in cranial procedures, hybrid tehcniques have not been widely
explored in the spine, and will not be discussed in any greater detail in this chapter.

37
2.2.2.2.4 Automatic Registration
The development of sophisticated intra-operative imaging devices, coupled with the tedious and
time-consuming nature of manual registration procedures, has driven significant improvements
in automatic image transfer and registration techniques. In the context of spinal surgery, the first
automatic algorithms were developed to allow registration of patient anatomy to a pre-operative
CT using multiple intra-operative C-arm XR images (typically one lateral and multiple oblique
views).(Nolte et al., 2000) Fundamentally, all automatic registration algorithms employ a known
relationship between the intra-operative imaging device and the output images, based on
manufacturer/laboratory calibration of the imaging device, to allow subsequent automatic
registration of the imaged patient anatomy to the imaging space dataset. Nolte et al. applied
multiple 2D XR images for automatic registration to a 3D pre-operatively-acquired CT dataset.
In their system, 2D to 3D transformation is accomplished by laboratory calibration of the C-arm
using a calibration plate with a grid of metallic markers. Using a linear cone beam projection
model, the virtual projection of a tracked instrument in the image-intensifier (II) coordinate
system can be transformed into the C-arm image coordinate system (Figure 2-11). This
calibration is accurate for a given C-arm in a specific position; as the C-arm position changes
intra-operatively however, deformation of the C-arm frame itself may lead to errors as a result of
millimetric movement of the XR source relative to the II detector. Therefore, the C-arm itself
also requires a calibration set of LEDs to be mounted to it to control the deformation in real-time
via a spatial calibration correction function.(Nolte et al., 2000)
Similar techniques of automatic registration are applied to contemporary intra-operative imaging
devices, including CBCT and FBCT systems. With FBCT systems the operating table is fixed to
the CT toroid, allowing for factory calibration of the relationship between the CT imaging plane
and the operating table, with real-time adjustments made if the gantry angle is altered for the
intra-operative scan. This relationship is updated intra-operatively using a patient-affixed DRF
and an LED tracking array mounted to the scanner itself. Automatic registration techniques with
modern intra-operative imaging systems have been demonstrated to be more time-efficient than
existing paradigms of registration to pre-operative imaging,(T. Kotani et al., 2014) however still

38
requiring on average 8-9 minutes for a complete registration cycle, from initial clamping of the
DRF to being ready to navigate.(Eric W. Nottmeier & Crosby, 2009) Moreover, these
registrations remain accurate only for the patient and DRF position at the time of intra-operative
imaging; any subsequent manipulation or deformation of either patient anatomy or the DRF
necessitates a repeat scan, with its associated time and patient radiation cost, as no rapid and
radiation-free technique of updating a registration exists to date.
Figure 2-11. Components and coordinate systems of automatic registration techniques. Illustration of a
representative setup (left) for automatic registration to intra-operatively-acquired fluoroscopic images. Local
coordinate systems (COSs) for each of the image source (here, image-intensifier (II)), surgical object/dynamic
reference frame (SO), tool (T) and C-arm image (CI) are shown. Automatic registration necessitates
laboratory/factory calibration to model the virtual projection of an imaged instrument from the II coordinate system to
the CI coordinate system (right). Reprinted from Nolte et al., A New Approach to Computer-Aided Spine Surgery:
Fluoroscopy-Based Surgical Navigation. Eur Spine J 2000;9(Suppl 1):S078-88, by permission of Springer Nature.
2.2.2.2.5 Optical Topographic Imaging
Despite workflow improvements afforded by automatic registration to intra-operatively-acquired
imaging, the radiation exposure to patients and OR personnel with intra-operative imaging
devices remains of concern. Conversely, while this radiation exposure is minimized by
registration to pre-operative CT or MRI with conventional techniques, these remain so

39
cumbersome and time-consuming as to deter the widespread adoption of navigation for spinal
procedures.(E W Nottmeier, 2012) Intra-operative stereoscopic optical imaging, or computer
stereovision, is one technique that has been explored to allow radiation-free registration of a pre-
operative imaging dataset to an optically-acquired surface map of intra-operative anatomy. In
neurosurgical navigation applications, stereovision was first explored for the automated
resolution of brain shift for updating of registrations for intra-cranial navigation.(DeLorenzo et
al., 2010; Paul, Morandi, & Jannin, 2009; Sun et al., 2005) Applications for open posterior spinal
surgery were investigated more recently in the mid-2010s.(Ji et al., 2015)
In isolation, passive stereovision with visible-wavelength cameras is able to generate 3D spatial
information, i.e. depth, from two 2D images. This may be accomplished through one of two
mechanisms, distinctly or in combination, based on the modes of information provided by
reconstructed stereoscopic images: texture intensity and 3D geometry. 3D spatial reconstruction
from two 2D images taken contemporaneously by two cameras spaced a known distance apart, is
accomplished by first eliminating lens distortion from each 2D image based on known attributes
of each optical setup, to allow simplification to an ideal pinhole projection. Subsequently, the
two 2D images are rectified into a common image plane, and the positions of a given element in
each image compared and triangulated to compute the position of the element in 3D space
relative to the camera positions (Figure 2-12).(Sun et al., 2005) Passive stereovision requires
imaged points to be distinctly visible in both 2D images. It therefore encounters significant
difficulty when imaging highly reflective or smooth surfaces, or in poor ambient lighting
conditions.(C. Chen & Zheng, 1995)

40
Figure 2-12. Passive stereovision and correspondence. Illustration depicting the ‘correspondence problem’ in
passive stereovision, modelled using ideal pinhole cameras (Cl and Cr). The image of a single point (X, Y, Z) is
projected onto the image planes of both cameras, (xl, yl) and (xr, yr), respectively. Triangulation of the location of (X,
Y, Z) in 3D space requires rectification of both image planes (solid lines, left) onto a plane (solid lines, right)
coincident with the epipolar lines (dotted lines, right) from both image projections. Reprinted from Sun et al.,
Stereopsis-Guided Brain Shift Compensation. IEEE Transactions on Medical Imaging 2005;24(8):1039-52, by
permission of © 2005 IEEE.
Active 3D imaging, or ranging technqiues, involve the addition of a surface-scanning projection
in addition to optical cameras, to identify the 3D geometry of a scanned surface.(Geng, 2011)
The fundamental principles of triangulation for spatial reconstruction apply equally to both
active and passive stereovision, however the features extracted from the images acquired by each
camera are created or enhanced by the addition of an active surface-scanning projection, to
minimize the difficulties faced by passive systems with textureless surfaces.(C. Chen & Zheng,
1995) Common active projection techniques include time-of-flight techniques, laser range
scanning, which may be coupled to stereo or monocular vision systems, as well as structured-
light scanning.(Mirota, Ishii, & Hager, 2011) Structured light involves the illumination of a
surface with a 2D spatially-varying pattern of known periodicity and intensity, made possible by
the development of digital micromirror devices. Monocular or stereovision imaging is then
applied to acquire a 2D image of the scene under structured light illumination. The deformation
of the projected structured-light pattern by a surface with varying 3D geometry, is then employed
to extract depth information from the surface, allowing the generation of a 3D surface map of the
scanned scene (Figure 2-13).(Geng, 2011) Techniques for structured-light spatial and temporal
variation have been studied extensively. A detailed examination of projection and coding

41
techniques is beyond the scope of this thesis. Broadly, structured-light projection patterns may be
classified as single-shot or sequential (multi-shot), requiring spatial or temporal multiplexing,
respectively. While sequential projection patterns may provide more accurate surface mapping
due to a greater number of reconstructed points, they are often unsuitable for moving targets as a
snapshot of the surface at a single point in time cannot be acquired.(Salvi, Fernandez, Pribanic,
& Llado, 2010) A simplified summary and classification of structured-light illumination patterns
is shown in Figure 2-14. Numerous studies of projection patterns and coding have been
published over the past two decades, aiming to strike a balance between resolution (point cloud
density of the reconstructed surface), noise, spatial accuracy, ability to code for coloured
surfaces, handling of dynamic surfaces, and computational time. Sequential projection patterns
have been demonstrated to have greater resolution and therefore spatial accuracy,(Pribanić,
Džapo, & Salvi, 2009; Salvi et al., 2010) whereas binary single-shot spatial multiplexing patterns
have the poorest spatial resolution.(Carrihill & Hummel, 1985; Salvi et al., 2010) Conversely,
the computational power and time required for sequential temporal multiplexing patterns is
significantly greater, due to the need to compute vastly greater numbers of 3D points. Color
calibration requires additional computational time.(Salvi et al., 2010) The use of stereovision
rather than a single camera partly minimizes the computational load for decoding depth
information from the structured light illumination pattern.(Mirota et al., 2011) The optimal
technique for medical/surgical applications therefore depends on the type of tissue being imaged,
i.e. whether it is relatively static or dynamic, as well as the accessibility of the tissue to imaging
devices, i.e. whether endoscopic or open approaches are required.(Schmalz, Forster, Schick, &
Angelopoulou, 2012) With advances in modern digital light projection technology as well as
increases in computing power afforded by graphics processing units (GPUs), sequential
projection techniques have been applied even to dynamic tissues including the myocardium and
bioprosthetic cardiac valves, at accuracies on the order of <100 µm.(Laughner, Zhang, Li, Shao,
& Efimov, 2012)

42
Figure 2-13. Structured light 3D scanning. Illustration of structured light illumination-based 3D surface mapping. A
monocular setup is depicted, with a structured light projection of a light pattern of known pattern and periodicity onto
the 3D object in the scene. The deformation of the reflected light pattern is seen by the camera, allowing computation
of a surface map based on known parameters of the optical setup, including the distance between camera and
projector (B) and incident angles (α, θ). Reprinted from Geng et al., Structured-Light 3D Surface Imaging: A Tutorial.
Adv Opt Photonics 2011;3(2):128-60, under Open Access by permission of the © 2011 Optical Society of America.
Figure 2-14. Structured light illumination patterns. A summary classification of structured light illumination
patterns described to date. Reprinted from Geng et al., Structured-Light 3D Surface Imaging: A Tutorial. Adv Opt
Photonics 2011;3(2):128-60, under Open Access by permission of the © 2011 Optical Society of America.

43
Computer vision-based image-guidance techniques have been developed in medicine for
numerous applications, most prominently facial prosthetics, joint arthroplasty, as well as
endoscopic and laparoscopic applications for rhinoscopy, bronchoscopy and intra-abdominal
surgery.(Helferty & Higgins, 2001; Keller & Ackerman, 2000; Mirota et al., 2011) Applications
of stereovision to surgical navigation have been explored more recently, predominantly with
passive stereovision in the context of cranial neurosurgery for the compensation of intra-
operative brain shift following craniotomy.(DeLorenzo et al., 2010; Paul et al., 2009; Sun et al.,
2005) Further advances have led to automated segmentation and registration protocols to update
registrations to pre-operative MRI.(X. Fan, Ji, Hartov, Roberts, & Paulsen, 2012, 2014; Ji, Fan,
Roberts, Hartov, & Paulsen, 2014) Stereovision for spinal procedures has been explored in only
one study to date, with a passive technique described by Ji et al., employing readily-available
stereoscopically-aligned grayscale cameras mounted rigidly to a surgical microscope.(Ji et al.,
2015) In clinical in-vivo testing in 8 patients, Ji et al. demonstrated a reconstruction accuracy of
stereovision-acquired surface maps of 2.21 mm, far greater than the <100 µm accuracies
described with active surface-scanning techniques.(Laughner et al., 2012) Registration accuracy
to a standard optically-tracked navigation system was 1.43 mm, within the described tolerances
for modern neuronavigation systems, typically considered to be <2 mm. The mean computational
time for stereovision-based reconstruction and registration was 95.8 seconds. While passive
stereovision represents a novel, contactless and radiation-free mechanism for intra-operative
image-to-patient registration of spinal anatomy, its clinical accuracy remains unproven, and
workflow improvements perhaps not sufficiently significant to promote widespread adoption
among spinal surgeons.
Our laboratory has developed a technique for active structured light illumination-based surface
mapping, coupled with thresholding algorithms to appropriately isolate scanned bony anatomy.
This technique may therefore be applied to registration of optically-imaged anatomy to a CT
dataset. We have termed this combination of structured light-based surface scanning and
automated segmentation and thresholding, optical topographic imaging (OTI). For the remainder
of this thesis, the term OTI will be used to refer to active computer stereovision for image-to-
patient registration.

44
2.2.3 Instrument Tracking and Actuation
Regardless of the method by which image-to-patient registration is achieved, all contemporary
intra-operative navigation suites aim to subsequently track instruments in the merged coordinate
system, to facilitate a given surgical maneuver. Instrument tracking may be accomplished
through a number of techniques; while a detailed discussion of tracking methodologies is beyond
the scope of this thesis, the topic merits some discussion as tool tracking itself is associated with
a quantifiable error, termed ‘jitter’, which contributes to the final application accuracy of a
navigation system.(Khadem et al., 2000) Furthermore, the process of intra-operative instrument
calibration and tracking contributes significantly to the overall usability and workflow of any
CAN system; inadvertent bumping of the DRF required for optical instrument tracking, for
instance, is a commonly cited pain point in current CAN workflows.(Choo et al., 2008)
Instruments in the earliest frameless CAN systems were tracked by mechanical articulated arms,
in which multi-directional position sensors at each articulation enabled computation of the
location and orientation of the instrument at the end effector of the arm, in all 6 possible degrees
of freedom (x, y, z for position, and roll, pitch, yaw for orientation).(Alshail et al., 1998; Carney,
Patel, Baldwin, Coakham, & Sandeman, 1996; Guthrie & Adler, 1992) While accurate, these
systems were bulky to position and operate, difficult to modify to track multiple instruments, and
were unable to track the motion of anything not directly attached to and calibrated for the arm.
The initial era of tracking systems devoid of mechanical linkages began with microscopes and
tools equipped with ultrasonic spark-gap emitters, whose pose and position were computed based
on an array of acoustic recorders situated around the operative field (Figures 2-2 and 2-4).(Kalfas
et al., 1995; H. F. Reinhardt, Horstmann, & Gratzl, 1993) Due to relative inaccuracy and
sensitivity to ambient noise from other operating room equipment as well as to air temperature,
acoustic tracking was largely abandoned in favour of optical or electromagnetic tracking, the two
primary paradigms in current use.(Tatar et al., 2002)

45
Contemporary optical tracking systems (OTS) rely on an infra-red camera typically mounted on
a mobile platform in the operating room. In a passive OTS, an IR emitter is also located on the
camera unit, and the reflection of the IR light from reflective markers on the tracked instruments
and DRF are used to triangulate the pose and position of each tool. In an active OTS, IR LEDs
are situated on both the DRF and each tracked instrument, with the IR light detected by the
mobile camera unit and used to calculate the pose and position of each tool (Figure 2-15).(N. D.
Glossop, 2009) Both active and passive OTS devices are currently available commercially. There
has been some suggestion, particularly among early-generation technologies, that active OTS
provides lower tracking error and greater consistency than passive systems; Khadem et al.
compared both active and passive OTS units from the same manufacturer, and found RMS jitter
of 0.058 ± 0.037 mm with active OTS and 0.115 ± 0.075 mm with passive.(Khadem et al., 2000)
These differences have been mitigated in modern devices largely through more powerful IR
emitters and improved filtering techniques for the IR cameras; current optical systems are able to
track individual markers with an accuracy of approximately 0.25 mm, and instrument tips at
accuracies of 1-2 mm.(Wiles, Thompson, & Frantz, 2004) However, OTS tool tracking relies on
a pre-calibrated relationship between the IR tracker array mounted on an instrument (either
passive reflective markers, or active LEDs) and the instrument tip, hence is unable to track
needles and other non-rigid tools. More importantly, and of greater relevance in day-to-day use,
accurate and real-time optical tracking necessitates constant line-of-sight between the IR camera
± emitter platform, and the DRF as well as the tracking array on each monitored instrument.
Clutter in the surgical field, and even the physical position of OR personnel and the hand
position of the tool operator, can greatly influence optical instrument tracking. Moreover, the
relative positioning of the DRF, tracker arrays on each tool, and the camera unit can influence
the tracking error of the system; Khadem et al. demonstrated that the majority of OTS tracking
error arises in the z-axis, that is, pointing directly away from the IR camera. Finally, the number
of tracker markers (reflective spheres or active LEDs) visible to the IR camera, as well as the
distance from the tool tip to the centroid of its tracker array, also influence tracking error; Wiles
et al. demonstrated a doubling of RMS tracking error with an increase in the tool tip distance of
100 mm.(Wiles et al., 2004) It is also known that optical instrument tracking accuracy in-vivo
degrades over time as well as with increasing distance from the DRF.(Quiñones-Hinojosa,
Robert Kolen, Jun, Rosenberg, & Weinstein, 2006) Operator-dependent mechanisms to reduce
optical tracking error therefore include situating the IR cameras as close to the surgical field as

46
possible, and moreover aligning the camera z-axis with the direction in which clinical accuracy is
least important, as well as ensuring that as many markers as possible are visible to the camera
when affixing the DRF and tracking a given surgical instrument.
Figure 2-15. Optical instrument tracking systems. Photographs of passive (left) and active (right) optical tracking
systems. In passive OTS, reflective spheres on both the reference frame (B) and instrument (C) are used for tool
tracking. In active OTS, LEDs on the reference frame and tracker are used for the same purpose, with a minimum of
three visible to the camera system (extreme right, yellow lines) for accurate tracking. Left image reprinted from Kral et
al., Comparison of Optical and Electromagnetic Tracking for Navigated Lateral Skull Base Surgery. Int J Med
Robotics Comp Assist Surg 2013;9(2):247-52, by permission of John Wiley and Sons. Right images reprinted from
Glossop et al., Advantages of Optical Compared with Electromagnetic Tracking. JBJS 2009;91(Suppl 1):23-8, by
permission of Wolters Kluwer Health, Inc.
Electromagnetic (EM) tracking systems were developed earlier than OTS technologies, however
have come into widespread clinical use only recently due in part to their lack of reliance on line-
of-sight as with optical systems. EM systems are composed of an electromagnetic field generator
or emitter, typically a bulky device positioned near the operative field in non-sterile fashion, a
DRF and a tracked instrument. Both the DRF and instrument contain sensor coils in which a
voltage is produced within the electromagnetic field generated by the emitter; the magnitude and
direction of the voltage generated in these cylindrical coils are used to compute the relative
position and two-dimensional orientation of the instrument (pitch, yaw). Computation of the
third dimension of orientation (roll, around the sensor coil’s longitudinal axis) requires a
combination of coils oriented orthogonally.(Milne, Chess, Johnson, & King, 1996) The primary
advantage of EM tracking is that the coil sensors are small, on the order of <1 mm in diameter
and <10 mm in length (Figure 2-16). They may therefore be embedded directly into instrument

47
tips, including rigid and flexible needles, catheters and endoscopes; as the instrument tip is
tracked directly given that no line-of-sight to an external detector is required, this enables the
tracking of flexible instruments within tissue cavities where line-of-sight is unobtainable.(N. D.
Glossop, 2009) However, EM tracking, particularly in older generation units, has been hindered
by significant interference from surrounding ferromagnetic materials, including most standard
surgical instruments and operating tables. EM tracking, as with OTS, relies on the presence of a
fixed DRF for relative tracking of instruments, and therefore is prone to the same disruptions as
OTS from inadvertent manipulation or displacement of the DRF. Accuracy degradation over
time and distance from the DRF, as has been demonstrated with OTS, has not however been
shown comparably in EM systems. Nonetheless, the accuracy of EM tracking has typically been
and continues to be slightly worse than that achieved by OTS, with tracking accuracy of an
individual sensor of approximately 0.9 mm and tool-tip accuracy of 1.5-2.5 mm, as reported in
the datasheets of an EM tracking device by a manufacturer also producing OTS systems.(NDI,
2018a) In a clinical comparative study of EM vs OTS tracking in skull-base neurosurgical
applications, Kral et al. found tracking accuracy of 0.99 mm with EM tracking, vs. 0.22 mm with
OTS.(Kral, Puschban, Riechelmann, & Freysinger, 2013) However, in applications where
needles or other fine-diameter catheters are tracked, part of the accuracy deficit of EM trackers is
mitigated by their ability to track the tool tip directly, as opposed to requiring an optical tracking
array at some distance from the tool tip, which itself introduces errors.

48
Figure 2-16. Electromagnetic instrument tracking. Photographs of a representative setup (left) with an
electromagnetic field generator (A) and reference coil (C) affixed rigidly into a skull. Representative photograph of a
tracked biopsy needle stylet (right), with sensor coil (green, circled in yellow) embedded at the tip of the instrument.
Left image reprinted from Kral et al., Comparison of Optical and Electromagnetic Tracking for Navigated Lateral Skull
Base Surgery. Int J Med Robotics Comp Assist Surg 2013;9(2):247-52, by permission of John Wiley and Sons. Right
image reprinted from Glossop et al., Advantages of Optical Compared with Electromagnetic Tracking. JBJS
2009;91(Suppl 1):23-8, by permission of Wolters Kluwer Health, Inc.
In all current navigation techniques, with instruments tracked either optoelectronically or
electromagnetically, the surgical instruments are typically actuated or manipulated freehand by
the surgeon, with continuous visual feedback from a display placing the tracked instrument in the
shared coordinate space with the registered imaging dataset. Initial CAN suites tracked only a
pointer or similar probe-type instrument; in the context of spinal surgery, the surgeon would then
be required to manually follow the trajectory planned with the navigated pointer using untracked
instruments for pedicle cannulation, tract preparation and screw placement. As a result, some
error of the final screw placement could result from slight deviations in manually-actuated
trajectory or entry point from that planned with the tracked pointer non-contemporaneously.
Subsequent generations of CAN devices have spawned instrument sets to match evolving
capabilities of modern trackers and intra-operative imaging devices, with dedicated tracked
instruments for pedicle cannulation, tract tapping as well as screw placement. This may
potentially minimize the final application error of navigated screw placement, however still
relies on freehand actuation of the navigated instrument by the operator, with continuous visual
feedback from a navigation display. The latest advance in instrument actuation, in an effort to
minimize the component of application error resulting from freehand manipulation of a tracked

49
instrument, is robotic guidance. Multiple systems have been developed and are commercially
available for spinal applications, all of which rely on optical IR tracking similar to freehand OTS
techniques. A mobile platform with a robotically-actuated arm is situated adjacent to the patient
and, using an affixed optical tracking array, is registered into the same coordinate system as the
patient anatomy and imaging dataset. The robotic end-effector, which may include a guide for
instruments for pedicle drilling/cannulation, tract preparation and screw placement, is
subsequently moved into the appropriate trajectory automatically with navigation guidance
(Figure 2-17).(Overley et al., 2017) 25 series studying the accuracy of spinal instrumentation
placement with various robotic guidance systems have been published to date, demonstrating
radiographic accuracy rates of 85.0-100%.(Joseph, Smith, Liu, & Park, 2017) Comparative
studies have demonstrated significant improvement in radiographic accuracy, as well as decrease
in intra-operative patient and surgeon radiation exposure, with robotic guidance vs. freehand or
fluoroscopically-guided instrumentation placement. However, only one study to date has
compared robotically-actuated to freehand-actuated navigated pedicle screw placement. In a
three-armed prospective trial of freehand vs. freehand-navigated vs. robotic-navigated
thoracolumbar pedicle screw placement, Roser et al. demonstrated no significant difference in
screw placement accuracy with standard navigation or robotic guidance, but with significantly
greater pre-operative preparation time and greater intra-operative radiation dose with robotic vs.
standard navigation (Table 2-3).(Roser, Tatagiba, & Maier, 2013) While robotic guidance may
represent the next step in evolution of intra-operative CAN systems, particularly as integration
with intra-operative imaging devices improves, in their current form there does not appear to be
any discernible benefit relative to freehand-actuated navigation techniques.

50
Figure 2-17. Robotic instrumentation guidance. Illustration of the Rosa© robotic guidance system (Medtech
S.A./Zimmer Biomet) with end-effector sleeve for pedicle cannulation. Reprinted from Overley et al., Navigation and
Robotics in Spinal Surgery: Where Are We Now? Neurosurgery 2017;80(3S):S86-99, by permission of Oxford
University Press.
Table 2-3. Intraoperative outcomes with robotic guidance. Operative times and intra-operative radiation time and
exposure are compared among freehand, freehand-navigation and robotic-navigation techniques for thoracolumbar
pedicle screw insertion. Reprinted from Roser et al., Spinal Robotics: Current Applications and Future Perspectives.
Neurosurgery 2013;72(Suppl 1):12-18, by permission of Oxford University Press.
2.3 Evaluation of Navigation Accuracy
Classically, Fitzpatrick et al. have classified errors in frameless stereotactic navigation into three
categories, the fiducial localization error (FLE), fiducial registration error (FRE), and target
registration error (TRE)(Figure 2-18).(Fitzpatrick, West, & Maurer, 1998) FLE represents the
error in localizing the points marked for registration in the patient space, which depends on the

51
error in the OTS or EM tracking system, the number and arrangement of fiducials, and the spatial
resolution and geometric accuracy of the imaging dataset, which is known to be greater for CT
than MRI.(M. N. Wang & Song, 2011) As discussed in Section 2.2.3 for instance, the tracking
error of EM systems is known to be greater than for OTS. FRE is the error in matching
corresponding fiducials in the patient and imaging spaces, represented by a distance metric
which is typically reported by commercial CAN systems as the ‘registration error’, somewhat
misleadingly. The true navigation error at a given target, however, is represented by the TRE, the
most clinically-relevant metric for end-users and also the most variable, as it differs for unique
targets. For paired-point registration technqiues, it is well documented that TRE increases with
distance from the centroid of the selected fiducial markers, as well as in areas of lower fiducial
concentration.(Fitzpatrick et al., 1998) While registration accuracy, or more appropriately FRE,
has been described for various surface-scanning techniques as well as differing algorithms for
registering two surfaces (see Section 2.2.2.2.2), the characteristics of TRE in surface-mapping
techniques in an in-vivo setting have not yet been elucidated. As unique errors arise in differing
techniques of patient and image space acquisition and registration, quantification of these errors
remains critical in the development of novel registration and neuronavigation techniques.

52
Figure 2-18. Classification of errors in frameless stereotactic navigation. Illustration depicting the classically-
described registration errors in frameless stereotaxis. (A) arrows indicate fiducial localization error (FLE). (B) arrows
indicate fiducial registration error (FRE). (C) arrows indicate target registration error (TRE) for the target, represented
by a square. Reprinted from Eggers et al., Image-to-Patient Registration Techniques in Head Surgery. Int J Oral
Maxillofac Surg 2006;35(12):12-5, by permission of Elsevier.
While TRE is the most clinically-relevant of the classic registration errors described by
Fitzpatrick et al., the concept of application accuracy is perhaps even more relevant to end-users,
as it accounts not only for errors inherent in the registration process and instrument tracking (as
with TRE), but also in how the tracked tools are applied to perform a given surgical maneuver.
In spinal procedures, in earlier generations of CAN a tracked pointer was used to visualize the
approximate ideal trajectory and entry point, which subsequently were followed manually with
untracked drills, pedicle finders and screwdrivers. Later generations of spinal CAN instruments

53
added tracked drills/awls, pedicle finders and screwdrivers. Nonetheless, the ultimate aim of
CAN guidance in this context is to place instrumentation accurately, hence the application
accuracy reflects how closely the final screw position approximates its intended navigated
position. As spine instrumentation is readily visualized on post-implantation XR or CT imaging,
final screw positions may therefore be compared readily to planned trajectories on intra-
operative navigation, as a measure of application accuracy. The radiographic grading systems
used in the literature to quantify pedicle screw accuracy, as a measure of application accuracy,
are highly heterogeneous. Some measures quantify only the magnitude of breach of the pedicle
wall, others assess the position of the screw tip alone without regard for the shaft position, and
only some identify the important of directionality of breach rather than magnitude alone.(Aoude
et al., 2015; Gertzbein & Robbins, 1990; Güven, Yalçin, Karahan, & Sevinç, 1994; Heary, Bono,
& Black, 2004; O’Brien et al., 2000) Quantification of absolute navigation application accuracy
in a standardized, reproducible fashion, is essential for the valid comparison of novel
neuronavigation techniques, and remains a knowledge gap in the current literature.
2.4 Thesis Aims and Hypotheses
Taken together, the body of literature suggests that surgical spinal pathologies, from
predominantly degenerative and neoplastic etiologies, constitute a significant and growing health
care burden, and that computer-assisted navigation techniques have an important and burgeoning
role in a variety of procedures to treat these ailments. While there is substantial evidence
supporting increased radiographic accuracy with spinal CAN, significant heterogeneity within
this literature results in unclear practical benefits from the perspective of the end-user,
particularly given that data on clinically-relevant outcomes in navigated spinal procedures is only
recently beginning to emerge. Inconsistencies in literature reporting standards render the results
of comparative studies on various CAN techniques onerous to interpret. As data on complication
avoidance with CAN emerges, however, cost-utility arguments for spinal CAN can subsequently
be investigated appropriately. A multitude of 3D CAN techniques exist currently, each with their
relative merits and drawbacks. Universal to essentially all current CAN methodologies is a
disruption in spatial and temporal workflow, significant upfront and ongoing capital costs, and a

54
considerable mental cost in the form of steep learning curves. These current hindrances to
adoption lead us to the overarching question of whether the capital and intellectual investment in
CAN is worthwhile. As with any medical technology, there may exist certain demographics
which are more suited to, or better able to maximize the benefits of, spinal navigation techniques.
However, these current usage patterns of spinal CAN remain undefined. Moreover, concerns
over workflow disruption and temporal efficiency remain unaddressed, and potential pitfalls and
application errors associated with CAN, which constitute part of their learning curve, remain
poorly transparent to the end-user. Each of these issues may contribute to a lack of adoption of
these technologies in key demographics. With optical topographic imaging (OTI), the potential
exists for disruption of the current paradigm of spinal navigation, with significant improvements
in spatial and temporal workflow that may alleviate some of the roadblocks to adoption. These
improvements must be demonstrated in clinical practice, however, and the remaining hindrances
affecting all spinal CAN techniques concomitantly addressed.
With this in mind, this thesis aims to test the following hypotheses:
1) Neuronavigation for spinal procedures, using optical topographic imaging (OTI), is at
least comparably accurate to and faster than existing neuronavigation techniques, across
all spinal regions, and in all high-yield applications for current navigation paradigms
2) Registration and navigation errors associated with OTI may be different in character and
magnitude from those associated with typical paired-point or automatic registration
These hypotheses will be addressed in the following 5 research objectives:
1) To evaluate current trainee and surgeon practice patterns with spinal CAN
2) To assess current methods of evaluating navigation error in spinal surgery, including
clinical, radiographic and quantitative metrics of navigation accuracy

55
3) To quantify the accuracy of OTI-CAN in the thoracolumbar spine, for both open and
minimally-invasive (MIS) approaches, and assess the impact of OTI-CAN on intra-
operative workflow
4) To quantify the accuracy of OTI-CAN in the mobile cervical spine, and assess the impact
of OTI-CAN on intra-operative workflow
5) To identify and characterize mechanisms of error in surface-based registration for intra-
operative CAN, and identify modifiable and non-modifiable anatomical and
computational predictors of increased navigation error

56
Chapter 3 Spatio-Temporal Trends in Spinal CAN Implementation
Preamble
This chapter is modified from the following:
Guha D, Moghaddamjou A, Jiwani ZH, Alotaibi NM, Fehlings MG, Mainprize TG, Yee A,
Yang VXD (2017). Utilization of spinal intra-operative three-dimensional navigation by
Canadian surgeons and trainees: a population based time trend study. Manuscript in submission.

57
3.1 Abstract
Computer-assisted navigation (CAN) is a useful adjunct to improve the accuracy of spinal
instrumentation as well as bony and soft-tissue resection. However, the widespread adoption of
CAN by spinal surgeons has been limited due partly to lack of training, high capital costs, and
workflow hindrances. The purpose of this study is to characterize the spatiotemporal use of
spinal CAN in a single-payer health care system and assess the impact of intra-operative CAN
use on trainee proficiency. We retrospectively reviewed a prospectively-maintained provincial
database of patients undergoing spinal instrumentation or percutaneous
vertebroplasty/kyphoplasty. Data was collected on treated pathology, spine region, surgical
approach, institution type, surgeon specialty, the use of 2D or 3D-CAN, and revision surgeries
within 2 years of the index procedure. Predictors of CAN usage as well as revision surgery were
identified. Trainee comfort with CAN and its impact on technical proficiency were assessed
using an electronic questionnaire distributed to all Canadian orthopedic surgical and
neurosurgical trainees across 15 nationwide training programs. 16.8% of instrumented fusions in
our provincial cohort were CAN-guided, predominantly by 3D-CAN. Navigation was employed
more frequently in academic institutions (15.9% vs. 12.3%, p<0.001) and by neurosurgeons
more than orthopedic surgeons (21.0% vs. 12.4%, p<0.001). Revision surgery was required in
6.4% of patients undergoing instrumented fusion, more frequently for trauma and deformity
cases, for cases performed at academic centers, and for cases performed without CAN guidance.
34.1% of residents reported being fully comfortable in the setup and use of spinal CAN, greater
for neurosurgical than orthopedic surgical trainees (48.1% vs. 11.8%, p=0.008). The use of CAN
for thoracic instrumentation increased the mean self-reported proficiency rank across all trainees
by 11.0% (p=0.036), with orthopedic residents also reporting an increase in mean proficiency
rank of 18.0% for atlantoaxial instrumentation (p=0.014) with CAN guidance. In current
practice, spinal CAN is employed most frequently by neurosurgeons and in academic centers.
The use of CAN is associated with a significant decrease in associated revision surgeries. Most
spine surgical trainees are not fully comfortable with the setup and use of intra-operative CAN,
but do report an increase in technical comfort with CAN guidance particularly for thoracic
instrumentation. Increased education in spinal CAN starting at the trainee level, particularly for
orthopedic surgery, may improve adoption.

58
3.2 Introduction
Spinal instrumentation is performed routinely for internal stabilization to promote osseous fusion
in traumatic, degenerative, metabolic and neoplastic spinal pathologies. With an aging
population, the North American burden particularly of degenerative and osteoporotic spinal
injuries is increasing, with tremendous societal and economic costs.(Baaj et al., 2010; Burge et
al., 2007; Cadarette & Burden, 2011; Martin et al., 2009) Instrumentation misplacement can
result, acutely, in injury to adjacent neurovascular structures and, in the longer term, to hardware
failure and non-union from poor load-bearing properties.(Acikbas et al., 2003; Xiao et al., 2017)
The placement of spinal instrumentation is traditionally performed freehand, or with guidance
from intra-operative X-rays resulting in significant radiation exposure to operating room (OR)
personnel.(Nelson, Monazzam, Kim, Seibert, & Klineberg, 2014; Villard et al., 2014) Three-
dimensional computer-assisted navigation (CAN), standard of care in cranial neurosurgery for
subsurface localization, has been shown to improve the accuracy of screw placement and reduce
surgeon radiation exposure, across all spinal levels.(T. S. Fu et al., 2008; G. Y. Lee, Massicotte,
& Rampersaud, 2007; Mason et al., 2014; Mirza et al., 2003; Nelson et al., 2014) Recent
evidence supports improved short and long-term clinical outcomes with the use of spinal CAN,
with reduced reoperation for hardware malposition-related complications as well as wound
infections.(Fichtner et al., 2017; Luther, Iorgulescu, Geannette, Gebhard, Saleh, Tsiouris, & Ha,
2015; Xiao et al., 2017) CAN usage is also cost-effective in high-volume centres.(Dea et al.,
2015; Matthew R Sanborn et al., 2012) However, CAN is used routinely by only 10-15% of
spinal surgeons.(Choo et al., 2008; Hartl et al., 2013; Schröder & Wassmann, 2006) A
worldwide survey of spinal surgeons, representing predominantly Europe, Asia and Latin
America, revealed multiple barriers to CAN adoption, principally cost, lack of training, and
unproven clinical benefit.(Hartl et al., 2013) The potential benefit of intra-operative CAN for
trainee education is also poorly represented in assessments of spinal CAN utility.(Gasco et al.,
2014; M B Gottschalk, Yoon, Park, Rhee, & Mitchell, 2015; Lorias-Espinoza et al., 2016;
Luciano et al., 2011; Podolsky et al., 2010; Rambani et al., 2014; Sundar et al., 2016)

59
Given differences in health care economics in Canada relative to the United States and Europe,
with potentially different barriers to CAN adoption, in the current study we characterize spinal
CAN utilization across a cohort of Canadian institutions. We also explore the utility of intra-
operative spinal CAN for trainee education.

60
3.3 Methods
3.3.1 Study Design
Assessment of spatiotemporal trends in spinal CAN utilization was performed by retrospective
review of a prospectively maintained provincial database of diagnostic and fee codes. The utility
of spinal CAN for trainee education was explored through an online survey, administered to a
nationwide cohort of neurosurgical and orthopedic surgical residents and clinical spine fellows.
3.3.2 Database – Patient Selection
The Ontario Health Insurance Plan (OHIP) database was searched through the Institute of
Clinical and Evaluative Sciences (ICES), at Sunnybrook Health Sciences Centre, for records
from 1 January 2005 to 31 December 2014 (REB# 380-2015). Patients meeting the following
criteria were included: ≥18 years of age; undergoing instrumented spinal fusion from either an
anterior or posterior approach at any spinal region; or undergoing percutaneous or open
vertebroplasty or kyphoplasty. Patients undergoing non-instrumented spinal fusion, or spinal
decompression without instrumentation, were excluded.
To detect a difference in the rate of revision surgery between navigated and non-navigated cases,
with literature estimates of 1% revision for navigated screws and 5-6% for non-navigated screws,
at α=0.05 and β=0.2, 376 patients were required in each group.(Dea et al., 2015). All sample size
calculations were performed using the ‘pwr’ package in R (Version 3.4.1; R Project for
Statistical Computing).

61
3.3.3 Database – Data Extraction
All data were extracted from the OHIP database by ICES analysts. Revision procedures were
identified by a combination of International Classification of Diseases, Ninth Revision, Clinical
Modification (ICD-9-CM) code, as well as date. Revision procedures were limited to within 2
years of the index procedure, to attempt to better capture revisions due to acute complications or
progressive hardware failure rather than ongoing degenerative processes.
Procedures were classified by pathology as trauma, degenerative, deformity, infection, tumor,
and vertebroplasty/kyphoplasty, based on a combination of OHIP fee and ICD-9-CM codes.
Within each pathology, procedures were subclassified by spine region
(cervical/thoracic/lumbosacral) and surgical approach (anterior/posterior), using a combination
of fee and ICD-9-CM codes. The use of two-dimensional (2D) or three-dimensional (3D) spinal
CAN for each procedure was identified using fee codes (E379/E378). A full description of
coding for data extraction is given in Supplemental – Section 3.7
For each identified procedure, the following demographic data were extracted: patient age,
gender, institution type (academic/rural), and surgeon specialty (orthopedic
surgery/neurosurgery).
3.3.4 Database – Statistical Analysis
Univariate comparison of categorical variables, including the proportion of procedures
undertaken with 2D or 3D CAN, were performed using Pearson Chi-squared or Fisher Exact
tests, depending on data distribution, with computation of Pearson’s correlation coefficients.
Continuous variables were compared using independent-samples t-tests or Mann-Whitney-U

62
tests, depending on data distribution. Predictors of CAN usage as well as revision surgical
procedures were explored using binary multiple logistic regression modelling, as well as
hierarchical mixed-effects logistic regression to account for surgeon specialty and institution
type as random effects. Significance levels for all tests were set at <0.05. All statistical analyses
were performed in SAS (Version 9.3; SAS Institute Inc., Cary, NC, USA).
3.3.5 Online Survey
The utility of spinal CAN for Canadian surgical trainees was assessed using a 22-item
anonymized online questionnaire distributed through GoogleForms (Supplemental - Section 3.8).
The survey was disseminated in September 2015 by email to 241 orthopedic surgical and
neurosurgical residents across 15 Canadian training programs, as well as 31 clinical adult and
pediatric spine fellows. A follow-up request for completion was emailed at 1 month; responses
were collected for a total of 4 months.
Responses to questions with multiple-choice ordinal options were converted to ordinal numerical
variables for analysis. All other responses were converted to nominal categorical variables.
Comparisons between categorical variables were made using Pearson Chi-squared tests or Fisher
Exact tests, depending on data distribution. Comparisons between multiple proportions were
made using partitioned Chi-squared analyses with Bonferroni correction. User comfort with
instrumentation techniques with versus without navigation guidance was assessed using
Wilcoxon signed-rank tests. Statistical analyses for the online survey were performed in SPSS
(version 21; IBM, Chicago, IL, USA).

63
3.4 Results
3.4.1 Spatio-Temporal Trends in Spinal CAN Usage
4607 cases of spinal instrumentation were identified in the OHIP database from 2005-2014,
35.8% with temporary percutaneous instrumentation (vertebroplasty/kyphoplasty) and the
remainder with permanent hardware for fusion (Figure 3-1). 45.9 % of cases were performed at
an academic institution, with 67.7% of instrumented fusions performed by orthopedic surgeons
and the remainder by neurosurgeons.
Figure 3-1. Cohort demographics. Pie chart demonstrating the demographics of the prospectively-monitored cohort
of patients undergoing spinal instrumentation, stratified by pathology.

64
Intra-operative computer-assisted navigation was employed in 14.0% of cases, and 16.8% of
instrumented fusions. Navigated cases were guided predominantly by 3D-CAN, with 27.1%
employing 2D-CAN. In this cohort, CAN was employed most frequently for trauma (41.8%,
with 32.1% 3D-CAN), followed by degenerative pathologies (19.8%, with 94.6% 3D-CAN) and
deformity corrections (2.5%, with 66.7% 3D-CAN). CAN was employed in only 0.5% of
vertebroplasties/kyphoplasties. In univariate analysis, CAN was employed more frequently in
academic institutions (15.9% vs 12.3%, p<0.001), and by neurosurgeons more than orthopedic
surgeons (21.0% vs 12.4%, p<0.001). Temporal trends in CAN usage are shown in Figure 3-2.

65
Figure 3-2. Temporal trends in spinal CAN usage. Histograms demonstrating temporal trends in spinal CAN usage
for a provincial cohort of patients undergoing spinal instrumentation, overall (A), and stratified by pathology (B),
surgeon specialty (C), 2D vs. 3D-CAN (D), and by institution type (E).

66
In hierarchical logistic regression, accounting for patient age, gender, pathology, and surgical
approach as fixed effects, and individual institutions and surgeons as random effects, surgeon
specialty and institution type were not independently associated with increased CAN usage. The
intraclass correlation coefficients for individual institutions and surgeons were 24% and 64%,
respectively. That is, the majority of variation in CAN usage is based on hospital and surgeon
individual preference.
3.4.2 Impact of CAN Usage on Revision Surgery Rates
In our cohort, revision surgery was required in 6.4% of patients undergoing instrumented fusion,
at an average (95%-CI) of 15.55 months (13.16-17.94 months) after the index procedure. In
univariate analyses, revisions were required more frequently for trauma and deformity cases, for
cases performed at academic centers and by orthopedic surgeons, and for cases performed
without CAN guidance (Table 3-1).

67
Table 3-1. Univariate analysis with revision surgery as outcome.
OR = odds ratio for repeat surgery. CI = confidence interval. (*) denotes significance at p<0.05.
Variables Repeat Surgery (%) OR (95%-CI) p-value
Yes No
CAN Use
Yes 0.023 13.6 0.48 (0.31-0.76) 0.001*
No 5.9 80.0
Surgeon
Specialty
Neurosurgery 1.5 29.3
0.55 (0.37-0.81) 0.002* Orthopedic
Surgery 5.4 56.9
Institution Type
Academic 3.4 42.3
1.37 (1.07-1.75) 0.011* Non-
Academic 3.0 51.3
Pathology
Degenerative 2.1 51.5
- - Deformity 4.4 37.1
Trauma 0.6 4.2

68
In hierarchical logistic regression, trauma and deformity pathologies remained independently
associated with increased revision. Intraclass correlation coefficients for individual institutions
and surgeons, as random effects, were 1% for both, indicating only 1% of the variation in
revision surgery rate was related to the individual institution and surgeon.
3.4.3 Survey of Surgical Trainees – Demographics
Of 272 residents and clinical spine fellows polled, complete responses were obtained from 60,
for a response rate of 22.1% (Figure 3-3). Orthopedic surgery and neurosurgery were represented
equally at 50% each. Respondents were located predominantly in Ontario (55.0%), followed by
Quebec (20.0%) and Alberta (10.0%); the remaining respondents were located in British
Columbia, Saskatchewan, Manitoba, Nova Scotia and Newfoundland.
Among surgical residents, the average time spent on a dedicated spine service was 5.50 ± 6.71
months, significantly greater for neurosurgery (7.37 ± 8.62 months) than orthopedics (3.30 ±
1.82 months)(p=0.024).

69
Figure 3-3. Survey demographics. Pie chart demonstrating the demographics of a surveyed national cohort of
neurosurgical and orthopedic surgical trainees, stratified by training level.
3.4.4 Utilization of CAN by Trainees
73.3% of trainees identified CAN as being available at their institution. Across all case types,
CAN was used >40% of the time by only 34.1% of respondents, with no differences between
surgical specialties.
In subgroup analyses looking at open fusions, minimally-invasive (MIS) fusions, deformity
corrections and revision fusions, CAN was used in >40% of cases by 38.6%, 36.6%, 32.1% and

70
38.6% of respondents, respectively, with no differences between surgical specialties (Figure 3-
4). In partitioned Chi-squared analysis, there was no significant difference in CAN usage
between case types.
Figure 3-4. Trainee-reported CAN usage. Histograms depicting trainee-reported CAN usage at their respective
institutions, for open instrumented fusions (A), minimally-invasive instrumented fusions (B), deformity corrections (C),
and revision instrumented fusions (D), stratified by trainee specialty.

71
34.1% of residents identified as being fully capable in the setup and intra-operative use of the
CAN system available at their institution, either independently or with minimal supervision,
significantly greater among neurosurgical than orthopedic trainees (48.1% vs. 11.8%, p=0.008).
Instruction on CAN setup/use was provided by surgical faculty for 75.0% of respondents, by
CAN product representatives for 52.3%, by fellows for 22.7%, by senior residents for 20.5%,
and by self-teaching for 22.7%.
3.4.5 Impact of CAN on Trainee Proficiency
Self-reported trainee proficiency with instrumentation in the atlantoaxial, subaxial cervical,
thoracic and lumbosacral spine was compared with and without CAN guidance (Appendix A,
Questions #13-20). An 11.0% increase in mean proficiency rank (2.93 vs 2.64, p=0.036) was
seen for thoracic pedicle screws with vs. without CAN guidance, across all respondents (Figure
3-5).

72
Figure 3-5. Trainee proficiency in CAN. Histogram demonstrating mean self-reported proficiency rank of trainees
for the placement of atlantoaxial, subaxial cervical, thoracic and lumbosacral instrumentation, with vs. without CAN
guidance. Proficiency was self-reported as 1 = not at all competent, 2 = somewhat competent, requiring extensive
supervision; 3 = very competent, with supervision; 4 = fully independent, without supervision. (*) denotes significant
difference at p<0.05.
When stratified by specialty, neurosurgical residents reported improved but statistically
insignificant gains in proficiency with CAN guidance for thoracic instrumentation (2.85 vs 2.59,
p=0.198), whereas orthopedic surgical residents reported an 18.0% increase in mean proficiency
rank with atlantoaxial instrumentation (2.29 vs 1.94, p=0.014) as well as a 12.9% increase in
mean proficiency with thoracic instrumentation, just missing statistical significance (3.06 vs
2.71, p=0.058).

73
3.5 Discussion
The adoption of spinal CAN remains limited by steep learning curves with potentially prolonged
operating times initially, and significant workflow disturbances primarily from registration
protocols.(Choo et al., 2008; Hartl et al., 2013; Ryang et al., 2015; Wood & McMillen, 2014)
Increasing the uptake of a technology proven to improve accuracy and patient outcomes requires
an understanding of current practice patterns and barriers to adoption. To our knowledge, our
study represents the first to explore the use of spinal CAN in a single-payer health care system.
We show here that spinal CAN is used predominantly by neurosurgeons and in academic
institutions. This conclusion is unsurprising given that intra-operative frameless stereotactic
CAN was developed originally for intracranial tumor localization.(David W. Roberts et al.,
1986) Two-year revision surgery rates were increased for trauma and deformity cases, for those
performed by orthopedic surgeons, at academic institutions, and when performed without CAN
guidance. Increased revisions for trauma and deformity cases, particularly at academic centers,
are to be expected given their relatively greater complexity. Only pathology remained
independently associated with revision in hierarchical mixed-effects modelling, with minimal
variability due to institutions and providers, suggesting additional variables, including case
complexity, operative time, and patient-level co-morbidities, as potential contributors which
were unaccounted for in our models.
While surgical technique, beyond anterior vs. posterior approaches, was not captured in the
database review, our online survey of Canadian surgical trainees revealed that CAN was used
equally for open fusions, MIS fusions, revision fusions and deformity cases. This contrasts with
the trend seen in the United States, where CAN appears to be used most often in high-volume
MIS practices, and may reflect a lack of deployment of CAN, in Canada, in the settings in which
it is clinically most useful.(Hartl et al., 2013) Conversely, the relative deficiency of CAN in MIS
and deformity procedures in Canada may reflect a relatively lower volume of these cases overall,

74
due in part to prolonged operating times and increased OR radiation exposure with MIS cases
compared to equivalent open procedures.(Bindal et al., 2008; Funao et al., 2014) Both issues are
addressed by current and emerging CAN techniques; willingness of institutions and practitioners
to adopt CAN technology may encourage safer, more efficient, and less invasive spinal
procedures for patients.(Jakubovic et al., 2016)
Real-time CAN feedback on anatomic landmark identification may also be beneficial for trainees
in learning spinal anatomy and nuances of instrumentation. A review of the literature revealed 7
studies assessing the utility of CAN for trainee education, all in an ex-vivo virtual-reality or
cadaveric/phantom setting.(Gasco et al., 2014; Michael B. Gottschalk et al., 2015; Lorias-
Espinoza et al., 2016; Luciano et al., 2011; Podolsky et al., 2010; Rambani et al., 2014; Sundar et
al., 2016) To our knowledge, our study represents the first to explore the utility of CAN intra-
operatively for trainee comfort and proficiency in placing instrumentation.
In our online survey, only one-third of residents reported being fully capable of setting up and
using a CAN system without or with minimal supervision, greater among neurosurgical than
orthopedic surgical trainees. The lack of comfort in CAN use among residents overall is reflected
in the similar lack of comfort and training for current faculty, one of the major barriers to
adoption that may be addressable through improved practical education at the trainee level.(Choo
et al., 2008; Hartl et al., 2013) The relative lack of comfort with CAN for orthopedic surgical
trainees compared to their neurosurgical counterparts may be due in part to a lack of familiarity
with CAN from non-spinal procedures, as well as significantly less time spent on a dedicated
spine service. However, the intra-operative use of CAN appears to improve the self-reported
proficiency of all trainees, in fact to a greater degree for orthopedic surgical trainees. This is in
keeping with the findings of ex-vivo laboratory studies.(Sundar et al., 2016) Given that
orthopedic surgeons performed most of the instrumented spinal fusions in our retrospectively-
reviewed Ontario cohort, it may be prudent to increase education in spinal CAN techniques at the
trainee level, to improve adoption particularly within the orthopedics community and thereby
maximize the potential benefits of CAN. Most respondents in our cohort reported being
instructed on CAN use by their attendings; improvement in trainee CAN education thus requires

75
increased adoption amongst faculty, by addressing known concerns with CAN such as workflow
and registration hindrances.(Choo et al., 2008; Hartl et al., 2013; Jakubovic et al., 2016) As
trainees and future faculty increase familiarity with CAN techniques and maximize their
benefits, the cost-effectiveness of CAN, currently greatest in high-volume academic centers, may
well trickle down to community institutions where a greater number of patients are treated.
Our retrospective database review is subject to the typical limitations of using an administrative
database, including inconsistent coding particularly for pathology, and for the indication for
revision surgery. Case complexity was not captured in the administrative database. Traumatic
pathologies were heavily under-represented in this dataset, at <5% of all cases. Our electronic
survey of surgical trainees captured self-reported proficiency in spinal instrumentation. Future
studies may assess the impact of intra-operative CAN on trainee proficiency with more objective
metrics, such as quantitative screw accuracy and/or time required per screw.

76
3.6 Conclusions
In a large provincial cohort, intra-operative navigation was employed for less than one-fifth of
instrumented spinal fusions, more frequently by neurosurgeons than orthopedic spinal surgeons,
and more often in academic than community institutions. The use of spinal CAN was associated
with a significant reduction in revision surgery. At a trainee level, almost two-thirds of
orthopedic surgical and neurosurgical trainees are not fully comfortable with the setup and use of
CAN. The use of CAN improves self-reported trainee proficiency in placing thoracic
instrumentation. Increasing practical education in spinal CAN from a trainee stage, particularly
in orthopedic surgery, may increase adoption and maximize the benefits of CAN for the greatest
population of patients.

77
3.7 Supplemental | Diagnostic and Fee Coding
The following combination of fee (OHIP) and diagnostic (ICD-9-CM) codes were applied to flag
patients stratified by pathology (trauma, degenerative, deformity, infection, tumour,
vertebroplasty/kyphoplasty), spine region (cervical, thoracic, lumbosacral), and approach
(anterior, posterior):
Trauma:
- Cervical:
o Anterior:
▪ OHIP code: N573/N516/E365
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 805.0x/805.1x/806.0x/806.1x/952.0x
o Posterior:
▪ OHIP code: (N572 + E370) OR (N572 + E384):
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 805.0x/805.1x/806.0x/806.1x/952.0x
- Thoracic:
o Anterior:
▪ OHIP code: N517/N518/E365:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 805.2/805.3/806.2x/806.3x/952.1x
o Posterior:
▪ OHIP code: (N572 + E370):
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 805.2/805.3/806.2x/806.3x/952.1x
- Lumbosacral:
o Anterior:
▪ OHIP code: N559/N580/E365:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above:
805.4/805.5/805.6/805.7/806.4/806.5/806.6x/806.7x/952.2/952.3/952.4
o Posterior:
▪ OHIP code: (N572 + E370):
▪ Flag if one of the following ICD-9-CM code is associated with the records
above:
805.4/805.5/805.6/805.7/806.4/806.5/806.6x/806.7x/952.2/952.3/952.4

78
Degenerative:
- Cervical:
o Anterior:
▪ OHIP code: N573/N516/N526/E365:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 721.0/721.1/722.0/722.4/723.x/722.71/722.81/722.91
o Posterior:
▪ OHIP code: N532/N515/N513/N528/E370/E384:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 721.0/721.1/722.0/722.4/723.x/722.71/722.81/722.91
- Thoracic:
o Anterior:
▪ OHIP code: N517/N518/E365:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 721.2/721.41/722.51/722.11/722.72/722.82/722.92/724.01/724.1
o Posterior:
▪ OHIP code: N513/N515/N526/E370:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 721.2/721.41/722.51/722.11/722.72/722.82/722.92/724.01/724.1
- Lumbosacral:
o Anterior:
▪ OHIP code: N559/N580/E365:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above:
721.3/721.42/722.1/722.52/722.83/722.10/722.73/722.93/724.02/724.03/7
24.2/724.3/724.6/724.7
o Posterior:
▪ OHIP code: N513/N582/N533/N526/E370/E387/E372:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above:
721.3/721.42/722.1/722.52/722.83/722.10/722.73/722.93/724.02/724.03/7
24.2/724.3/724.6/724.7
- Unspecified:
o OHIP code: N532/N515/N513/N526/N528/N533/N582/E370/E384/E387/E372:
o Flag if one of the following ICD-9-CM code is associated with the records above:
714.x/720.x/721.6/721.7/721.9x/722.2/722.6/722.7
Deformity:
o Anterior:
▪ OHIP code: N539:
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 737.x
o Posterior:
▪ OHIP code: N540:

79
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 737.x
o Unspecified osteotomy:
▪ OHIP code: (N574/N575/N576 + E370):
▪ Flag if one of the following ICD-9-CM code is associated with the records
above: 737.x
Infection:
- By OHIP code only (please provide primary ICD-9 code for manual confirmation)
- OHIP code: (N548/N549/N550 + E370)
Tumour:
- by OHIP code only (please provide primary ICD-9 code for manual confirmation)
- OHIP code: (N560/N561/N553/N554/E386 + E370), WITHOUT any combination from
the ‘Infection’ label (above)(b/c the E386 code covers both tumour and infection)
Vertebroplasty/Kyphoplasty:
- by OHIP code only (please provide primary ICD-9 code for manual confirmation)
- OHIP code: N570/N583/E388/E392
Other:
- OHIP code E370, plus:
- ICD-9-CM code: 336.x/741.x
Navigation usage was identified by OHIP code, flagged as either 2D-CAN (E379) or 3D-CAN
(E378). Revision fusions were identified by OHIP code, flagged by the billing of E375 for the
same patient ID within 2 years of the index procedure.

80
3.8 Supplemental | Online Survey
1) What is your current training level?
a. PGY-1
b. PGY-2
c. PGY-3
d. PGY-4
e. PGY-5
f. PGY-6
g. Clinical spine fellow
2) Which residency program are you enrolled in/have you completed?
a. Neurosurgery
b. Orthopedic surgery
3) In which province are you currently training?
a. British Columbia
b. Alberta
c. Saskatchewan
d. Manitoba
e. Ontario
f. Quebec
g. Nova Scotia
h. Newfoundland
4) How many months of residency did you spend on a full-time spine service?
5) Do you have computer-assisted 3D navigation capabilities for spinal surgery at your
institution? If ‘yes’, please complete the remaining questions.
a. Yes
b. No
6) In what percent of overall spine cases at your institution is computer-assisted 3D
navigation utilized?
a. 0-20%
b. 21-40%
c. 41-60%
d. 61-80%
e. 81-100%

81
7) In what percent of open spinal fusions at your institution is computer-assisted 3D
navigation utilized?
a. 0-20%
b. 21-40%
c. 41-60%
d. 61-80%
e. 81-100%
8) In what percent of minimally-invasive spinal fusion cases at your institution is computer-
assisted 3D navigation utilized?
a. 0-20%
b. 21-40%
c. 41-60%
d. 61-80%
e. 81-100%
f. N/A (minimally-invasive cases not performed at this institution)
9) In what percent of deformity correction cases at your institution is computer-assisted 3D
navigation utilized?
a. 0-20%
b. 21-40%
c. 41-60%
d. 61-80%
e. 81-100%
f. N/A (deformity cases not performed at this institution)
10) In what percent of revision spinal fusion cases at your institution is computer-assisted 3D
navigation utilized?
a. 0-20%
b. 21-40%
c. 41-60%
d. 61-80%
e. 81-100%
11) From which sources do you receive your primary teaching/instruction on the use of
computer-assisted 3D navigation in spinal surgery? Select all that apply.
a. Senior resident
b. Clinical spine fellow
c. Staff surgeon
d. Navigation company/product representatives
e. Self-taught
f. Other: __________

82
12) Please rate your current level of comfort in the setup and intraoperative use of the
computer-assisted 3D navigation available at your institution, for spinal surgery.
(includes transferring of images, intraoperative registration, navigation)
a. Fully able to set up and use, independently
b. Fully able to set up and use, with supervision
c. Able to set up and use most intraoperative features, with supervision
d. Able to perform minimal setup and use some intraoperative features, with
extensive supervision
e. No concept of setup or intraoperative use
13) Please rate your confidence, at your current level of training, in placing atlantoaxial
screws (C1 and/or C2) WITHOUT computer-assisted 3D navigation (X-ray/fluoroscopy
may be used, if required).
a. Fully independent, without supervision
b. Very competent, with supervision
c. Somewhat competent, requiring extensive supervision
d. Not at all competent
14) Please rate your confidence, at your current level of training, in placing atlantoaxial
screws (C1 and/or C2) WITH computer-assisted 3D navigation.
a. Fully independent, without supervision
b. Very competent, with supervision
c. Somewhat competent, requiring extensive supervision
d. Not at all competent
15) Please rate your confidence, at your current level of training, in placing subaxial cervical-
spine screws (C3-7) WITHOUT computer-assisted 3D navigation (X-ray/fluoroscopy
may be used, if required).
a. Fully independent, without supervision
b. Very competent, with supervision
c. Somewhat competent, requiring extensive supervision
d. Not at all competent
16) Please rate your confidence, at your current level of training, in placing subaxial cervical-
spine screws (C3-7) WITH computer-assisted 3D navigation.
a. Fully independent, without supervision
b. Very competent, with supervision
c. Somewhat competent, requiring extensive supervision
d. Not at all competent

83
17) Please rate your confidence, at your current level of training, in placing thoracic-spine
pedicle screws WITHOUT computer-assisted 3D navigation (X-ray/fluoroscopy may be
used, if required).
a. Fully independent, without supervision
b. Very competent, with supervision
c. Somewhat competent, requiring extensive supervision
d. Not at all competent
18) Please rate your confidence, at your current level of training, in placing thoracic-spine
pedicle screws WITH computer-assisted 3D navigation.
a. Fully independent, without supervision
b. Very competent, with supervision
c. Somewhat competent, requiring extensive supervision
d. Not at all competent
19) Please rate your confidence, at your current level of training, in placing lumbosacral
pedicle screws WITHOUT computer-assisted 3D navigation (X-ray/fluoroscopy may be
used, if required).
a. Fully independent, without supervision
b. Very competent, with supervision
c. Somewhat competent, requiring extensive supervision
d. Not at all competent
20) Please rate your confidence, at your current level of training, in placing lumbosacral
pedicle screws WITH computer-assisted 3D navigation.
a. Fully independent, without supervision
b. Very competent, with supervision
c. Somewhat competent, requiring extensive supervision
d. Not at all competent
21) How has your use of computer-assisted 3D navigation, for spinal surgery, changed your
likelihood of pursuing specialized (i.e. fellowship) spine training?
a. Significantly increased
b. Slightly increased
c. Unchanged
d. Slightly decreased
e. Significantly decreased
22) How has your use of computer-assisted 3D navigation, for spinal surgery, changed your
likelihood of incorporating spine cases into your fuure practice?
a. Significantly increased
b. Slightly increased
c. Unchanged
d. Slightly decreased
e. Significantly decreased

84
Chapter 4 Correlation Between Clinical and Absolute Engineering Accuracy
in Spinal Computer-Assisted Navigation
Preamble
This chapter is modified from the following:
Guha D, Jakubovic R, Gupta S, Alotaibi NM, Cadotte D, da Costa LB, George R, Heyn C,
Howard P, Kapadia A, Klostranec JM, Phan N, Tan G, Mainprize TG, Yee A, Yang VXD.
Spinal intra-operative three-dimensional navigation: correlation between clinical and absolute
engineering accuracy. Spine J 2017;17(4):489-98.

85
4.1 Abstract
Spinal intra-operative computer-assisted navigation (CAN) may guide pedicle screw placement.
CAN techniques have been reported to reduce pedicle screw breach rates across all spinal levels.
However, definitions of screw breach vary widely across studies, if reported at all. The absolute
quantitative error of spinal navigation systems is theoretically a more precise and generalizable
metric of navigation accuracy. It has also been computed variably, and reported in fewer than a
quarter of clinical studies of CAN-guided pedicle screw accuracy. Here, we aim to characterize
the correlation between clinical pedicle screw accuracy, based on post-operative imaging, and
absolute quantitative navigation accuracy. We reviewed a prospectively-collected series of 209
pedicle screws placed in 30 patients with CAN guidance. Each screw was graded clinically by
multiple independent raters using the Heary and 2mm classifications. Clinical grades were
dichotomized per convention. The absolute accuracy of each screw was quantified by the
translational and angular error in each of the axial and sagittal planes. Acceptable screw accuracy
was achieved for significantly fewer screws based on 2mm grade vs. Heary grade (92.6% vs.
95.1%, p = 0.036), particularly in the lumbar spine. Inter-rater agreement was good for the Heary
classification and moderate for the 2mm grade, significantly greater among radiologists than
surgeon raters. Mean absolute translational/angular accuracies were 1.75 mm/3.13 and 1.20
mm/3.64 in the axial and sagittal planes, respectively. There was no correlation between clinical
and absolute navigation accuracy, as surgeons appear to compensate for navigation registration
error. Future studies of navigation accuracy should report absolute translational and angular
errors. Clinical screw grades based on post-operative imaging may be more reliable if performed
in multiple by radiologist raters.

86
4.2 Introduction
Intra-operative three-dimensional computer-assisted navigation (CAN) is used routinely in
cranial neurosurgery for the localization of subsurface structures. While not employed as
frequently, navigation for spinal procedures may guide implant placement and bony
decompression, particularly in minimally-invasive and complex deformity-correcting procedures
where anatomic landmarks are less readily identifiable.(Bandiera et al., 2013; Hartl et al., 2013;
Sakai et al., 2008)
Modern spinal CAN techniques employ two-dimensional (2D) guidance using “virtual”
fluoroscopy, or three-dimensional (3D) guidance based on either pre-operative or intra-operative
computed tomography (CT) imaging, as discussed in Chapter 2.(A C Bourgeois et al., 2015) The
accuracy of spinal navigation systems is most easily studied for pedicle screw placement, as
instrumentation is reliably localized on post-operative imaging. CAN techniques have been
widely reported to reduce pedicle screw breach rates, from 12-40% under freehand or
fluoroscopic guidance to under 5% with 3D CAN.(L. P. Amiot et al., 2000; M Bydon et al.,
2014; Castro et al., 1996; Eric W Nottmeier, Seemer, & Young, 2009; Rajasekaran et al., 2007;
B. J. Shin et al., 2012; Y Wang et al., 2013) Improved instrumentation accuracy is seen across all
3D CAN techniques, in each of the cervical, thoracic, lumbar and sacral regions.(Barsa, Frőhlich,
Šercl, Buchvald, & Suchomel, 2016; Austin C Bourgeois et al., 2015; Hecht et al., 2010; Mason
et al., 2014; N. F. Tian et al., 2011)
The clinical accuracy of spinal CAN for pedicle screw placement is variably reported. Up to half
of studies assessing pedicle screw accuracy do not define methods of determining screw
‘breach’, and no consistent grading system is used by those that do.(Aoude et al., 2015; B. J.
Shin et al., 2012) The absolute accuracy of spinal navigation systems, quantified most commonly
by the target registration error (TRE), has been reported to varying extent in fewer than ten
human clinical studies since 2000, while more than forty studies on CAN-guided pedicle screw

87
placement have been published in the same period.(Belmont, Klemme, Dhawan, & Polly, 2001;
Haberland, Ebmeier, Grunewald, Hliscs, & Kalff, 2000; Kleck et al., 2016; Y. Kotani et al.,
2007; Mason et al., 2014; Mathew, Mok, & Goulet, 2013; Oertel, Hobart, Stein, Schreiber, &
Scharbrodt, 2011; Scheufler, Franke, Eckardt, & Dohmen, 2011a, 2011b; N. F. Tian et al., 2011)
Unsurprisingly, the absolute accuracy requirements of spinal CAN systems, and their
relationship to radiographic screw position and clinical outcomes, remain poorly
defined.(Rampersaud, Simon, & Foley, 2001)
Here, we therefore review a prospectively-collected series of 209 pedicle screws placed with 3D
CAN guidance, with clinical accuracy grading using two established scoring systems, as well as
quantitation of absolute translational and angular navigation accuracy, to identify any correlation
between clinical and engineering accuracies.

88
4.3 Methods
4.3.1 Patient Selection
Thirty patients enrolled in a prospective comparative trial of our research group’s optical
topographic 3D CAN system (Chapter 5) against two commercially-available 3D CAN systems,
were retrospectively reviewed. All patients underwent posterior cervical/thoracic/lumbar/sacral
instrumented fusion with pedicle screw constructs, with or without decompression, for
predominantly traumatic, degenerative, or neoplastic pathologies. Procedures were performed at
Sunnybrook Health Sciences Centre by a single surgeon (VXDY), with or without trainee
assistance, from May 2014 – February 2015.
4.3.2 Intra-Operative Navigation
All screws were placed with 3D CAN guidance using either the NAV3/3i (Stryker; Portage, MI,
USA), registered to pre-operative imaging with point-matching followed by surface refinement,
or the StealthStation S7 (Medtronic Sofamor Danek; Memphis, TN, USA), registered to intra-
operative imaging using the O-Arm™ (Medtronic). Pre-operative CT scans were performed at a
slice thickness of 0.625mm, on a GE LightSpeed VCT scanner. All patients underwent post-
operative CT imaging of the instrumented region, using the same scanner at a slice thickness of
0.625mm.
4.3.3 Clinical Grading

89
Clinical grading of pedicle screw accuracy was performed on post-operative CT imaging using
two established methods, the Heary and 2mm classifications.(Belmont et al., 2001; Heary et al.,
2004) Summaries of each scoring system are shown in Tables 4-1 and 4-2, respectively. Heary
grading was performed for all screws independently by one neurosurgeon (DC), two orthopedic
surgeons (RG, GT) and two radiologists (CH, PH). 2mm grading was performed for all screws
independently by two neurosurgeons (NMA, DG) and two radiologists (AK, JMK). Reviewers
for each scoring system were blinded to the results of the other. Clinical grades were
dichotomized as acceptable (Heary grade ≤ 2, or 2mm grade ≤ 2) or poor (Heary grade >2, or
2mm grade >2), as has been previously reported.(Aoude et al., 2015; Belmont et al., 2001; Heary
et al., 2004)
Table 4-1. Heary Classification for pedicle screw placement.
Grade Definition
1 Shaft + tip contained entirely within pedicle
2 Shaft violates lateral pedicle, but tip entirely contained within vertebral body
3 Tip penetrates anterior or lateral vertebral body
4 Shaft breaches medial or inferior pedicle wall
5 Tip or shaft violates pedicle or vertebral body, and endangers spinal cord, nerve
root(s) or great vessels, requiring immediate revision
Table 4-2. 2mm classification for pedicle screw placement.
Grade Definition
1 Shaft contained entirely within pedicle
2 Shaft violates pedicle cortical wall by <2mm
3 Shaft violates pedicle cortical wall by 2-4mm
4 Shaft violates pedicle cortical wall by >4mm

90
4.3.4 Quantitative Navigation Application Accuracy
Absolute navigation accuracy was measured by comparing the final screw position, on post-
operative CT imaging, to a screenshot of the planned screw entry point and trajectory, as seen by
the navigation system intra-operatively. Translational and angular deviation from the planned
entry point and trajectory were than quantified, in both the axial and sagittal planes, using
multiplanar reformatting of both pre- and post-operative CT imaging. The method of absolute
navigation error quantification is adapted from those described by Mathew et al. and Kotani et al.
(Figure 4-1).(Y. Kotani et al., 2007; Mathew et al., 2013) In the axial plane, positive translational
deviations denote a lateral deflection of the entry point, and positive angular deviations denote a
more lateral trajectory. In the sagittal plane, positive translational deviations denote a superior
deflection of the entry point, and positive angular deviations denote a more cranial trajectory.
All image processing and measurements were performed using an Osirix 64-bit workstation
(version 10.9.5; PIXMEO SARL, Switzerland).

91
Figure 4-1. Quantification of navigation application accuracy. Measurement of absolute navigation accuracy, in
the axial (A+C) and sagittal (B+D) planes. Comparison is made between intra-operative navigation screenshots of
planned entry points and trajectories (A+B), to final screw positions on post-operative CT (C+D). Reference lines
(dashed) are drawn, in the axial plane, in the mid-sagittal line (bisecting the vertebral body, spinal canal and spinous
process) and, in the sagittal plane, along the inferior endplate. Translational error is computed as (d1-d); angular error
is computed as (1-).

92
4.3.5 Statistical Analysis
Inter-rater reliabilities (IRR) of Heary and 2mm grades were computed using two-way
consistency average-measures intraclass correlation coefficients (ICC), appropriate for a fully-
crossed design.(Shrout & Fleiss, 1979) As an approximation, ICC values between 0.60 and 0.74
were reflective of moderate agreement, 0.75 to 0.89 good agreement, and 0.90-1.00 excellent
agreement.(Cicchetti, 1994) Frequencies of categorical data were analysed using Fisher’s exact
tests. For paired categorical data, including the frequencies of poor-grade screws on both Heary
and 2mm grading scales, McNemar-Bowker tests of marginal homogeneity were used.
Correlation of clinical grading with absolute navigation errors were performed by independent-
samples t-tests as well as generalized linear regression models. Regression models were first
tested for nonlinearity with three cubic splines, with subsequent elimination of all nonsignificant
nonlinear terms from the final model. Significance levels for all tests were set at < 0.05.
All statistical analyses were performed in SPSS Statistics (version 21; IBM, Chicago, IL, USA).

93
4.4 Results
A total of 209 pedicle screws from 30 patients were included in our analysis. 3 screws were
placed in the cervical spine (all at C7), 138 in the thoracic spine, 64 in the lumbar spine, and 4 in
the sacrum (all at S1).
4.4.1 Clinical Accuracy
Of 209 screws, with 932 combined Heary grades from five independent reviewers, 95.1% were
rated as acceptable. On the 2mm grading scale, from four independent reviewers assessing the
same dataset, significantly fewer screws were rated as acceptable, at 92.6%. These differences
did not persist when thoracic screws were analyzed independently, however the Heary grading
system was significantly more generous in the lumbar spine. Cervical and sacral screws were not
analyzed independently due to inadequate sample size. A summary of clinical grades is presented
in Table 4-3.
The intraclass correlation coefficient, a measure of inter-rater reliability, was 0.763 (95%-CI
0.665-0.809) for Heary grade, 0.428 among the three surgeon raters and 0.781 among the two
radiologist raters. For the 2mm grade, overall ICC was 0.611 (95%-CI 0.517-0.690), 0.21 among
the two surgeon raters and 0.678 among the two radiologist raters.

94
Table 4-3. Clinicoradiographic grades of 209 pedicle screws.
Heary Grade
(# of ratings)
2mm Grade
(# of ratings)
Difference
(absolute value)
Significance
All screws
Acceptable 886 (95.1%) 774 (92.6%) 2.48% p = 0.036*
Poor 46 (4.9%) 62 (7.4%)
Thoracic screws
Acceptable 584 (93.4%) 509 (92.2%) 1.23% p = 0.43
Poor 41 (6.6%) 43 (7.8%)
Lumbar screws
Acceptable 272 (98.6%) 240 (93.8%) 4.80% p = 0.005*
Poor 4 (1.4%) 16 (6.2%)
(*) denotes significance at < 0.05
4.4.2 Absolute Application Accuracy
The absolute translational and angular errors of all screws in our cohort, in both axial and sagittal
planes, are shown in Figure 4-2. For all screws, axial and sagittal translational errors were (1.8 ±
3.6 mm) and (1.2 ± 1.1 mm), respectively, while axial and sagittal angular errors were (3.1 ±
2.9) and (3.6 ± 3.4), respectively (mean ± SD). Axial angular errors were greater in the lumbar
vs. thoracic spine (mean 3.7 vs. 2.6, respectively; p = 0.018); all other errors were equivalent
across spinal regions.
4.4.3 Clinical-Engineering Correlation
In a generalized linear regression model, there was no correlation between any absolute
navigation error parameter, and the mean Heary grade across all raters (Figure 4-3). Comparison
of absolute navigation errors between ‘poor’ and ‘acceptable’ dichotomized Heary grades also
revealed no significant differences. Similarly, no correlation was observed between absolute
navigation errors and the mean 2mm grade (Figure 4-3). Comparison of absolute navigation

95
errors between ‘poor’ and ‘acceptable’ dichotomized 2mm grades revealed no significant
differences.
Figure 4-2. Absolute navigation application accuracy for 209 pedicle screws. Standard boxplots demonstrating
the translational (A) and angular (B) absolute navigation errors in axial and sagittal planes. Boxplot height
corresponds to the interquartile range (IQR), whiskers correspond to 1.5xIQR, circular points are those outside
1.5xIQR, asterisked points are those outside 3xIQR.

96
Figure 4-3. Correlation between absolute navigation application error and clinicoradiographic grade.
Scatterplots of mean Heary grade (top row) and mean 2mm grade (bottom row), vs. each of axial and sagittal
translational and angular errors. No correlation is seen between Heary grade or 2mm grade, and any absolute
navigation error parameter.

97
4.4.4 Surgeon Compensation for Navigation Error
We theorized that the lack of observed correlation between clinical screw grade and absolute
navigation accuracy may be due, in part, to surgeon compensation for perceived misalignment of
virtual and anatomic intended screw entry points, based on surgeon visualization and knowledge
of anatomic landmarks. For instance, a ‘perfect’ entry point as shown by the navigation system,
that is felt by the surgeon to be excessively lateral based on anatomic knowledge, may lead the
surgeon to compensate by medializing their screw trajectory (Figure 4-4). In this situation, the
signed axial translational error is expected to be positive, with a corresponding negative axial
angular error.
Linear regression models were therefore generated between signed translational and angular
errors, in the axial and sagittal planes, respectively. Negative linear correlations were observed
for both axial (p < 0.001) and sagittal (p < 0.001) errors, suggestive of surgeon compensation
occurring in both planes, greater in the axial than sagittal plane (Figure 4-5).

98
Figure 4-4. Potential mechanism for surgeon compensation. Visualization of potential mechanism of surgeon
compensation for perceived navigation registration error. In the axial plane (A), a lateral translational error may lead
the surgeon to medialize the screw trajectory, leading to inversely-signed translational and angular errors (d2-d1 > 0;
2-1 < 0). In the sagittal plane (B), a rostral translational error may lead the surgeon to direct the screw more
caudally, with similar inversely-signed translational and angular errors.
Figure 4-5. Correlation between translational and angular navigation errors. Scatterplots of angular vs.
translational errors in the axial (A) and sagittal (B) planes. Least-squares regression lines (solid) and 95% confidence
intervals (dashed) are shown, along with regression coefficients (ß).

99
4.5 Discussion
The primary purported benefit of CAN for spinal procedures is improved instrumentation
accuracy and, in theory, minimization of complications from breached screws. Clinical sequelae
of screw breach include, acutely, neurologic and vascular injury and, in the longer term,
pseudoarthrosis due to poor osseous purchase and load-bearing.(Verma et al., 2010) As CAN
techniques evolve, from 2D-fluoro to 3D-fluoro to intra-operative CT-based registration, from
surgeon-manipulated to robotically-actuated instruments, the body of literature on navigation
accuracy is rapidly expanding. In an era of fiscally-responsible health care, the cost-effectiveness
of various CAN techniques, in relation to their purported accuracy, is also being explored.(Dea et
al., 2015; Watkins et al., 2010)
The grading systems used to quantify navigation accuracy for pedicle screw insertion remain
highly heterogeneous.(Aoude et al., 2015) Some, such as the 2mm grading system, are based on
screw shaft relation to the pedicle wall alone, while others, such as the Heary classification,
include the relation of the screw tip to the vertebral body.(Gertzbein & Robbins, 1990; Heary et
al., 2004) Similarly, while most scales quantify only the amount of pedicle wall breach, others
have demonstrated the importance of directionality, with lateral breaches less likely to be
clinically significant.(Güven et al., 1994; O’Brien et al., 2000) As assessments of in vivo screw
accuracy are based on post-operative CT imaging, metallic artefact may also contribute to the
reliability of accuracy ratings, though the type of screw material has been shown not to impact
inter-rater reliability.(Lavelle et al., 2014)
The commonest grading system in current use is the 2mm classification, with variations in the
grade cutoffs ranging from >4mm breach to >6mm breach for Grade IV screws.(Gertzbein &
Robbins, 1990; Neo, Sakamoto, Fujibayashi, & Nakamura, 2005) The increasingly-popular
Heary classification accounts for tip position relative to the vertebral body, and emphasizes
medial/inferior breaches over less clinically-relevant lateral breaches, regardless of magnitude. In

100
our series, the Heary classification was significantly more conservative than the 2mm grade in
identifying poorly-placed screws, but only among lumbar pedicle screws. While the Heary grade
was developed for thoracic pedicle screws and has not formally been validated in the lumbar
spine, it can reasonably be expected to perform similarly as its emphasis is to prioritize breaches
more likely to be symptomatic.(Heary et al., 2004) Anterior, medial and inferior perforations are
given greater weight in the Heary classification due to risk of injury to the
esophagus/trachea/lungs, spinal cord and nerve roots, respectively, in the thoracic spine. In the
lumbar spine, perforations in similar directions may injure the iliac vessels/bowel, conus
medullaris/cauda equina, and nerve roots, respectively. Therefore, the relatively aggressive
identification of poor-grade screws by the 2mm grading system in the lumbar spine, is likely
reflective of the larger pedicles and screw diameters relative to the thoracic spine. A breach of
2mm for a 7mm-diameter lumbar pedicle screw is far more likely to be tolerated by a surgeon
than the same 2mm breach for a 4.5mm-diameter thoracic screw. While the 2mm increment in
this classification is appropriately justified, and the grade cutoffs in our study are those used
most commonly in the literature, adjustment of grade cutoffs may be required across spinal
levels.(Abe et al., 2011; Belmont et al., 2001; Bledsoe, Fenton, Fogelson, & Nottmeier, 2009;
Cui et al., 2012; Gertzbein & Robbins, 1990; Kleck et al., 2016) For instance, ‘Grade IV: >4mm
breach’ may be appropriate for the thoracic spine, while ‘Grade IV: >6mm breach’ may be more
appropriate in the lumbar spine, as described originally by Gertzbein and Robbins.(Gertzbein &
Robbins, 1990)
Good inter-rater agreement was demonstrated in our series for the Heary classification, and
moderate agreement for the 2mm scale. For both scales, inter-rater reliability was significantly
higher amongst radiologists than surgeons. For the 2mm system, using the same grade cutoffs as
our study, ICC has been reported to vary from 0.45 to 0.69, in concordance with our results.(Bai
et al., 2013; Cho, Chan, Lee, & Lee, 2012; M.-C. Kim, Chung, Cho, Kim, & Chung, 2011;
Schizas, Thein, Kwiatkowski, & Kulik, 2012) To our knowledge, this is the first study reporting
on inter-rater reliability of the Heary classification. It is also the first to compare IRR between
radiologist and surgeon raters. Given the difficulty in distinguishing metallic screw artefact from
pedicle cortex on CT imaging, it is unsurprising that radiology-trained raters are more consistent.
It may therefore be prudent for future studies of navigation accuracy to employ multiple

101
radiologists for rating clinical screw accuracy, rather than a single rater as has been done in more
than half of studies to date.(Aoude et al., 2015)
Absolute navigation accuracy, commonly quantified as the target registration error (TRE), likely
represents the most generalizable method of reporting navigation accuracy. The TRE of novel
navigation techniques is commonly quantified ex vivo using specialized fiducial-implanted
phantoms.(Koivukangas, Katisko, & Koivukangas, 2011; Uneri et al., 2015) However, in vivo
absolute navigation accuracy has been reported in only seven human clinical studies since
2000.(Haberland et al., 2000; Kleck et al., 2016; Y. Kotani et al., 2007; Mathew et al., 2013;
Oertel et al., 2011; Scheufler et al., 2011a, 2011b) Quantitation of absolute accuracy in these
studies is highly variable, with the majority reporting only angular error. Given that surgeons
employing CAN intra-operatively modulate both the position and angulation of their instruments,
in both the axial and sagittal planes based on in-plane views on the navigation display, error
tolerances in each of these parameters should be reported in future studies of navigation
accuracy.
We have shown here furthermore that clinical grading, on two commonly used scales, does not
correlate with absolute quantitative navigation accuracy. Using a novel technique of measuring
both translational and angular error in axial and sagittal planes, we have also demonstrated
quantitatively for the first time that surgeon compensation may lead to clinically-acceptable
screw placement despite navigation registration error. While the absolute accuracy requirements
for surgical navigation systems remain uncertain, in trained hands they are likely to be less
stringent than the submillimeter tolerances suggested by rigid mathematical models.(Rampersaud
et al., 2001) Conversely, while CAN is a useful intra-operative adjunct, it cannot and should not
replace dedicated subspecialty training, which affords the experience and anatomic knowledge
required to identify and compensate for navigation registration errors.

102
Given the heterogeneity and inter-rater discordance in clinical grading scales, along with their
lack of correlation with engineering accuracy, reporting of absolute navigation accuracy along
with a summary of clinical sequelae may be a reasonable standard for future studies of
navigation accuracy. Acute neurovascular injury from breached screws are rare events, however,
and long-term pseudoarthrosis-related complications are difficult to attribute specifically to
breached screws.(Mason et al., 2014) Clinical screw grading based on post-operative imaging
will therefore continue to be of value in identifying breaches likely to cause significant sequelae.

103
4.6 Conclusions
Radiographic grading scales of pedicle screw accuracy are highly heterogeneous, with variability
in performance across spinal levels, as well as in inter-rater reliability. Correlation between
clinical screw grade and absolute navigation accuracy is poor, in part due to surgeon
compensation for navigation error. Future studies of navigation accuracy should therefore report
absolute translational and angular navigation accuracy, along with relevant clinical sequelae of
any placed screws. If used, clinical screw grades based on post-operative imaging should ideally
be generalizable, validated, and include the directionality of breach, and may be more reliable if
performed in multiple by radiologist raters. Navigation systems are not intended to replace
quality surgical training, which affords the experience and anatomic knowledge required to
identify and compensate for navigation errors.

104
Chapter 5 Optical Topographic Imaging with Efficient Registration to CT for
Spinal Intra-Operative Three-Dimensional Navigation
Preamble
This chapter is modified from the following:
Jakubovic R*, Guha D*, Gupta S, Lu M, Jivraj J, Standish BA, Leung MK, Mariampillai A, Lee
K, Siegler P, Skowron P, Farooq H, Nguyen N, Alarcon J, Deorajh R, Ramjist J, Ford M,
Howard P, Phan N, da Costa L, Heyn C, Tan G, George R, Cadotte DW, Mainprize TG, Yee A,
Yang VXD. High speed, high density intraoperative 3D optical topographical imaging with
efficient registration to MRI and CT for craniospinal surgical navigation. Manuscript in
submission.
*co-first authors

105
5.1 Abstract
Intraoperative image-guided surgical navigation for craniospinal procedures has significantly
improved accuracy by providing an avenue for surgeons to visualize underlying internal
structures corresponding to exposed surface anatomy. Despite the obvious benefits of surgical
navigation, surgeon adoption remains relatively low due to long setup and registration times,
steep learning curves, high capital costs, and workflow disruptions. We introduce an
experimental navigation system utilizing optical topographic imaging (OTI) to acquire the 3D
surface anatomy of the surgical cavity, enabling visualization of internal structures relative to
exposed surface anatomy from registered pre-operative images. Our OTI approach includes near
instantaneous and accurate optical measurement of >250,000 surface points, computed at
>52,000 points-per-second for considerably faster patient registration than commercially
available benchmark computer-assisted navigation (CAN) systems, without compromising
spatial accuracy. Our experience of 162 pedicle screws placed with OTI-CAN demonstrated
significant workflow improvement relative to benchmark spinal computer-assisted navigation
systems, on the order of 6-20 fold faster, without compromising absolute application accuracy.
Our advancements provide the cornerstone for widespread adoption of image guidance
technologies for faster and safer surgeries without intraoperative CT or MR imaging. This work
represents a major workflow improvement for navigated spinal procedures, with readily-
conceivable extension to cranial as well as non-neurosurgical image-guided applications.

106
5.2 Introduction
Intraoperative surgical navigation has become the standard-of-care in cranial neurosurgery for
the localization of subsurface structures, including neoplasms and vascular lesions, and for
targeting of electrical implants to specific nuclei. While not as ubiquitous, navigation for spinal
surgery has undergone significant evolution over the past decade. This technological
advancement has been driven by need, with 410,000 spinal fusion procedures performed in the
United States in 2008, a number expected to rise significantly over the next decades with an
aging population.(Ciol, Deyo, Howell, & Kreif, 1996; Rajaee, Bae, Kanim, & Delamarter, 2012)
While instrumentation is often used to facilitate osseous fusion, breach of screws outside the
intended trajectory occurs in 12-40% of screws (Figure 5-1).(Mohamad Bydon et al., 2014;
Castro et al., 1996; Rajasekaran et al., 2007; Yingsong Wang et al., 2013) This may result,
acutely, in neurovascular injury and, in the longer term, mechanical construct failure, causing
potentially life or limb-threatening complications which may require costly revision
surgery.(Verma et al., 2010; Watkins et al., 2010) Computer-assisted navigation has been
developed to improve the accuracy of screw placement at all spinal levels, reducing breach rates
to under ten percent (see Section 2.1.3.1).(L. P. Amiot et al., 2000; Arand, Schempf, Fleiter,
Kinzl, & Gebhard, 2006; Laine, Lund, Ylikoski, Lohikoski, & Schlenzka, 2000; G. Y. F. Lee,
Massicotte, & Raja Rampersaud, 2007; Eric W Nottmeier et al., 2009; Rajasekaran et al., 2007)
Navigation is also increasingly being applied to non-neurosurgical procedures, including hip and
knee arthroplasties, oral and maxillofacial reconstructions, delicate otologic drilling, and open
abdominal surgery.(L.-P. Amiot & Poulin, 2004) We demonstrate a new surgical navigation
technology, developed in our Biophotonics and Bioengineering Laboratory (BBL), using optical
topographical imaging (OTI) to create virtual 3D surfaces of open surgical cavities, allowing
surgeons to visualize internal structures relative to exposed surface anatomy (Figures 5-2, 5-3).
Our system completes full bony surface registration using graphics processing units (GPUs)
considerably faster than current systems, with comparable spatial resolution, sparing the patient
from additional radiation exposure, reducing operating room time and costs, and minimizing
disruption to surgical workflow.

107
Despite the apparent benefit of spinal surgical navigation in reducing breach rates, adoption of
navigation as standard of care has been slow due to lengthy setup/registration times, steep
learning curves, and interruption of surgical workflow.(Wood & McMillen, 2014) Contemporary
benchmark navigation systems employ a paired-point registration protocol relying on surgeons to
drag a pointed probe across exposed bony anatomy to map to a pre-operative computed
tomography (CT) scan. These protocols have steep learning curves and take three to five-fold
longer per screw than traditional fluoroscopy, necessitating additional anesthetic and operating
room time.(Assaker, Reyns, Vinchon, Demondion, & Louis, 2001; Mirza et al., 2003; N. F. Tian
et al., 2011) Current registration protocols are unable to account for variances in spinal anatomy
due to changes in patient positioning from CT gantry to operating table, critical in trauma and
deformity cases. While this may be overcome with intra-operative 3D fluoroscopy or CT, it is at
the cost of significantly increased radiation to the patient, particularly with multilevel fusions,
and adds substantial setup time.(Manbachi, Cobbold, & Ginsberg, 2014; Nelson et al., 2014) Our
experimental navigation system confers significant benefit over currently available navigation
systems, implementing a simple point-picking protocol for initial approximate alignment
followed by rapid optical imaging registration to fuse the intra-operative surface anatomy with
the pre-operative CT. Rapid repeat registration allows for sequential segmental registration,
minimizing intersegmental deviation from pre-operative imaging to intra-operative positioning.
While we validate our system here for spinal navigation, the technology is immediately
applicable to cranial as well as non-neurosurgical navigation applications, with rapid repeat
registration lending itself well to future soft-tissue applications.

108
Figure 5-1. Ideal thoracic pedicle screw placement. sIdeal thoracic pedicle screw entry point (dark red circle) and
trajectory (dashed red cylinder) in the coronal (A), axial (B) and sagittal (C) planes. Ideal entry point distance (d) and
trajectory angle () shown on axial and sagittal planes. Example of a misplaced thoracic pedicle screw via freehand
technique (D), Heary Grade V, with tip (arrowhead) abutting the aorta.

109
5.3 Methods
5.3.1 OTI System Design
Our experimental OTI navigation system consists of a small camera gantry integrated with
surgical lighting. The camera gantry is composed of two grayscale visible-band cameras, a
digital micromirror pico-projector and an infra-red (IR) optical tracking system (Figure 5-2A-B).
The projector illuminates a structured light of known structure and periodicity (repeating bars)
sequentially, that is recorded by the cameras and used to reconstruct the 3D surface of the patient
(Figure 5-3A).(Geng, 2011) The patterns enable image correspondence between the stereo
cameras to be established, regardless of the natural texture of the scanned surface. With
calibrated cameras, the stereo images allow for 3D mapping of the surface correlating to the
various height disparities. The experimental navigation system registers the acquired 3D-point
cloud to pre-acquired imaging data (i.e. CT, MRI) using a surface registration algorithm that is
based on the iterative closest-point (ICP) algorithm (Figure 5-3C-D). The experimental
navigation system also utilizes a passive IR tracking system containing two IR cameras
surrounded by IR light-emitting diodes (LEDs) to illuminate the tracking volume. The IR system
is employed to track surgical tools using passive-reflective markers (Figure 5-3D).

110
Figure 5-2. Clinical prototype of an experimental OTI navigation system. (A) Computer design model of the
surgical light head with embedded navigation. Designed to inconspicuously serve as traditional boom-supported
surgical light head comprised of 64 high intensity surgical light LEDs to provide standard lighting with minimal spectral
overlap with the navigation optics. Binocular infrared cameras utilizing provide real-time tracking of passive-reflective
markers mounted on surgical tools. A digital mirror device centered around binocular structured light cameras forming
an epipolar baseline provide intra-operative surface imaging for registration to the pre-operative images. Co-ordinates
of the tracked tools are easily matched to the acquired structured light surface image. (B) Computer design model of
the field of view of the infrared tracking volume (outer pyramid) and the structured light imaging volume (inner
pyramid). All measurements are in millimeters. (C) Prototype navigation system in clinical use. (D) Comparison of
total setup time (median and IQR) for cranial and spine applications of experimental (OTI) and benchmark navigation
systems.

111
Figure 5-3. Optical topographic imaging (OTI) experimental navigation technique. (A) Structured light
illumination of the open surgical field. Structured light pattern deformations reflect height variations (along the optical
axis) of the surface. (B) Registered reconstructed surface data to pre-acquired imaging data with tool tracking
capabilities. (C) Grayscale stereoscopic cameras acquire surface images (left). Deformation of structured light
patterns are used to create 3D reconstructions and thresholded point-clouds representing the bony surface of the
spine (right). (D) Registration of the acquired 3D point cloud (left) to pre-acquired imaging data (right) using an
iterative closest point (ICP) algorithm based on a three point picking protocol for initial alignment.

112
5.3.2 Specimen/Patient Selection
Pre-clinical technical development and validation was performed first ex-vivo in 6 adult human
formalin-fixed cadavers, and subsequently in-vivo in 10 anesthetized and ventilated adult swine.
All cadavers had no history of prior spinal surgery. All cadavers and porcine specimens
underwent pre- and post-operative helical CT imaging at 0.5 mm slice thickness for image-to-
patient registration (pre-operative) and quantitation of application accuracy (post-operative).
Institutional ethics and animal control board approvals were obtained (Mount Sinai Hospital
REB# 260-2011; Sunnybrook Health Sciences Centre AUP# 13-512).
Human clinical testing was performed in 92 adult patients, >18 years of age, without history of
prior spinal surgery. Institutional ethics board approval was obtained (Sunnybrook Health
Sciences Centre REB# 177-2013, 309-2014, 004-2015, 406-2015, 288-2016).
5.3.3 Pre-Clinical Testing
In all pre-clinical testing, both cadaveric and porcine, cadavers/specimens were positioned prone
on a standard operating table. Standard midline open posterior exposures were fashioned using a
combination of sharp dissection and, in-vivo, electrocautery. Exposures were performed to mimic
those typically required in open midline posterior instrumentation approaches clinically, that is,
with adequate exposure bilaterally of the medial half of the transverse process (thoracic spine)
and facet capsule (lumbar spine).
Ex-vivo cadaveric testing was employed for initial prototyping of an OTI-CAN system,
transitioning from stereocameras and a digital micromirror projector mounted on optical stages
to a unified design integrating all components into a surgical overhead lighting unit (Figure 5-2).
Subsequent in-vivo porcine work assessed interference between optical illumination for surgical
lighting and structured light illumination for OTI, as both are in the visible electromagnetic

113
spectrum, for optimization and minimization. Porcine work was also required to establish the
required timing for 3D optical imaging, that is the time available to acquire a surface map of the
operative field within the limits of typical suctioning to clear pooling blood within the cavity.
Navigation application accuracy was also assessed first in in-vivo porcine trials, to include the
effect of ventilatory motion on final application accuracy. Following OTI registration to the
exposed posterior osseous spinal anatomy, OTI-CAN guidance was employed using a tracked
awl and gearshift probe for pedicle cannulation, followed by the placement of standard
appropriately-sized titanium thoracic and lumbar pedicle screws. All in-vivo procedures were
performed by a single surgeon (VXDY).
5.3.4 Human Clinical Testing
In-vivo human clinical validation was performed in a prospective comparative trial of OTI-CAN
against two benchmark spinal CAN systems, the NAV3/3i (Stryker; Portage, MI, USA) using a
paired-point and manual surface tracing registration protocol, and the StealthStation S7 coupled
with O-Arm for automatic registration to intra-operative imaging (Medtronic Sofamor Danek;
Memphis, TN, USA). Open posterior instrumented fusions were performed for stabilization
following either trauma, discoligamentous degeneration, or decompression of bony and epidural
tumor. All patients were positioned prone on a Wilson frame or four-post Jackson operating
table. Standard open midline exposures were performed similar to human cadaveric testing. All
in-vivo procedures were performed by a single surgeon (VXDY), with trainee assistance.
To maximize safety, human clinical trials began with a lead-in phase (Phase I) whereby OTI was
used to generate a 3D surface map of exposed anatomy and perform registration only, however
with instrumentation guidance by benchmark CAN or traditional freehand or fluoroscopic
techniques (Figure 5-4). This was followed by two validation phases: in the first (Phase II), both
a benchmark and an OTI-CAN system were available in the operating room, initially with
instrumentation guidance by benchmark CAN and measurement of established trajectories by
OTI, and subsequently with a cross-over whereby instrumentation guidance was by OTI-CAN;

114
in the second (Phase III), OTI-CAN continued to be employed as the primary image-guidance,
but as a standalone device without secondary confirmation from a benchmark CAN system.
Figure 5-4. Flow diagram of OTI human clinical trials. Phase I: Lead-in phase, with screws placed using standard-
of-care freehand/fluoroscopic techniques or with image-guidance from benchmark CAN systems. OTI used to assess
feasibility of registration and subjectively verify accuracy, for further engineering refinement. Phase II: Initial validation
of OTI prototype system. In first half of phase II, instrumentation guided by benchmark CAN techniques with OTI used
for registration and verification of trajectory, with quantification of accuracy for verification. In second half of phase II,
instrumentation guided by OTI but with benchmark CAN used for verification of accuracy. Phase III: Final validation of
OTI prototype system, with OTI used as primary guidance system without benchmark CAN verification.
For OTI registrations, a custom dynamic reference frame (DRF) with passive-reflective optical
tracking array was clamped onto the spinous process of the level to be registered (‘segmental’
registration). Structured light illumination was then applied to generate a 3D surface of the
surgical cavity, which was automatically registered to the pre-operative CT dataset after
selection of three rough points on both hemilaminae and the spinous process of the vertebra to be
registered, to provide an initial alignment for the ICP algorithm (Figure 5-3). Following
registration, manual verification of registration accuracy was performed by dragging a tracked

115
pointer/awl along known anatomic landmarks and assessing the quality of correlation in the
imaging space. If manual verification deemed the registration acceptable, navigation or trajectory
confirmation could proceed. If the registration was unacceptably inaccurate for navigation
purposes, as deemed by the operator, the registration protocol was repeated.
For registrations using either benchmark CAN suite, the respective proprietary DRF was affixed
segmentally to the spinous process of the level to be registered. Where the NAV3/3i was used,
points corresponding to readily-identifiable landmarks had been pre-selected on the pre-operative
CT dataset. These were matched intra-operatively using a tracked pointer to complete a paired-
point registration. The tracked pointer was then dragged along the exposed hemilaminae and
spinous process as a manual surface tracing for refinement of the registration, the accepted
practice for this class of device. Where the O-Arm was used, following DRF fixation the O-Arm
gantry was opened and the imaging device moved over the operating table in sterile fashion. An
intra-operative cone-beam CT scan was taken, and automatically registered to the patient
anatomy using the companion StealthStation S7 CAN system. Manual verification of registration
accuracy was performed for both benchmark systems in the same manner as for OTI-CAN, with
repetition of the respective registration sequences in cases of inaccurate or failed initial
registration.
For both benchmark and OTI-CAN systems, following successful registration a tracked awl and
gearshift probe were used to cannulate the target pedicle. A screenshot of the navigation
trajectory was taken with the gearshift probe in-situ at its deepest point in the cannulated pedicle
tract, to most accurately represent the planned navigation trajectory down the cannulated pedicle,
for assessments of navigation accuracy. For both benchmark and OTI systems, registration time
was recorded as the time from DRF fixation to completion of manual registration accuracy
verification, that is, being ready to navigate instrumentation. For procedures guided by the O-
Arm, this therefore included the time required for intra-operative imaging. Navigation accuracy
was graded both clinicoradiographically and quantitatively for screws placed with all systems
(see Sections 5.3.5 and 5.3.6).

116
Prospective human trials were commenced with a goal of non-inferiority for quantitative
accuracy relative to benchmark CAN systems. While translational technical accuracy in a
laboratory phantom setting has been described for some current CAN systems including the O-
Arm cone-beam CT with StealthStation,(Koivukangas et al., 2011) translational application error
remains unknown, but is typically accepted to be ~2 mm. This is borne out by reported
translational application errors for cranial navigation systems, on the order of (2 ± 0.5) mm
(mean ± SD).(Steinmeier et al., 2000) Angular application error for thoracolumbar pedicle
screws has been reported in one study to be (2.8 ± 1.9)°,(Oertel et al., 2011) and in another to
range from (3.09 ± 2.12)° to (4.02 ± 2.63)°, depending on whether a navigated screwdriver was
used or not, respectively, to place instrumentation.(Kleck et al., 2016) Assuming a translational
error of (2.0 ± 0.5) mm and angular error of (3.0 ± 2.0)° for current spinal CAN systems, at α =
0.05 and β = 0.20 (i.e. power = 0.80), for two independent samples with continuous outcomes,
and a non-inferiority limit difference of 0.5 mm and 1.0°, 50 screws per group will be required.
All sample size calculations were performed in R (Version 3.4.1; R Project for Statistical
Computing).
5.3.5 Clinicoradiographic Accuracy Assessment
For all pedicle screws placed in pre-clinical porcine testing, as well as in Phase II + III of human
clinical in-vivo testing under both benchmark and OTI guidance, radiographic accuracy was
graded on post-operative CT imaging using the Heary classification (Table 4-1). Briefly, Grade I
denotes the screw is entirely contained within pedicle; Grade II the screw violates lateral pedicle
but screw tip is contained within the vertebral body; Grade III indicates the screw tip penetrates
anterior or lateral vertebral body; Grade IV indicates a medial or inferior breach of the pedicle;
Grade V involves a violation of the pedicle or vertebral body endangering the spinal cord, nerve
root, or great vessels. Heary grades were dichotomized per convention, into no breach/minor
breach (Heary Grade ≤ 2) vs. major breach (Heary Grade > 2). Radiographic grading was
performed independently by two neuroradiologists (CH, PH), three neurosurgeons (DWC, NP, &
LC) and two orthopedic spine surgeons (RG, GT). Any adverse clinical events intra or post-

117
operatively, that is any neurovascular sequelae or any other instrumentation-related
complications, were also recorded.
5.3.6 Quantitative Application/Engineering Accuracy
For all pedicle screws placed in pre-clinical porcine testing, as well as in Phase II + III of human
clinical in-vivo testing under both benchmark and OTI guidance, pre- and post-operative CT
images were resliced to 0.3 mm thickness and dynamically resliced using multiplanar
reconstruction (MPR) corresponding to the axial and sagittal co-ordinates of the intra-operative
and post-operative screw trajectories. Deviations of each screw from planned navigation
trajectories were then computed by comparing the position of the screw on post-operative MPR
CT imaging, to a screenshot of the navigation trajectory taken intra-operatively. Deviations are
reported as the translational and angular errors in each of the axial and sagittal planes, based on
our reporting scheme devised in Chapter 4. Briefly, the distance from the axis of symmetry
perpendicular to the point of entry (translational error), as well as the angle between the screw
trajectory and the perpendicular distance of the entry point (angular error), were recorded. In the
axial plane, the axis of symmetry was the mid-vertebral line; in the sagittal plane, either the
superior or inferior endplate, consistent across levels (Figure 5-5). The entry point of the screw
was determined as the point where the center of the screw comes into contact with the vertebral
body. All measurements were performed using an OSIRIX 64-bit workstation (Version 10.9.5,
PIXMEO SARL, Switzerland).

118
Figure 5-5. Quantification of absolute navigation application accuracy. Example shown of a patient with
hypoplastic pedicles at L2. (A) Intraoperative predicted screw trajectory (red) as visualized on a pre-operative axial
CT. (B) Postoperative actual screw trajectory (red) as visualized on a multiplanar reformatted post-operative CT. Axial
distances (d) were measured at 90° relative to mid-sagittal axis (green line). Angle (Ø) represents corresponding
trajectory angles. (C) Intra-operative predicted screw trajectory (red) as visualized on a pre-operative sagittal CT. (D)
Post-operative actual screw trajectory (red) as visualized on a multiplanar reformatted post-operative CT. Sagittal
distances (d) were measured at 90° relative to the inferior or superior endplate (green line). Angle (Ø) represents
corresponding trajectory angles. Errors in each plane were calculated as d1-d (translational) and Ø1-Ø (angular).

119
5.3.7 Statistical Analysis
For absolute navigation application accuracy, translational and angular deviation in the axial and
sagittal planes in the benchmark spine cohort were compared with the corresponding deviations
in the OTI navigation system cohort, in Phases II + III of human clinical trials. Statistical
analysis was not performed on the lead-in phase as the experimental navigation system was not
used for guidance. The distributions of translational and angular deviations were assessed and, as
an assumption of normality was not met, were compared using the non-parametric Kruskal-
Wallis one-way analysis of variance (ANOVA) test and visualized on Bland-Altman plots.
Predictors of increased navigation application error were identified and tested using a
generalized linear model, with age, gender, screw location, and guidance method (navigation,
fluoroscopy, or freehand) considered as covariates. For clinicoradiographic grading, Heary
grades were assessed for inter-rater reliability using the intra-class correlation coefficient, and
reliability of agreement measured using the Fleiss’ kappa test. A p-value of <0.05 was
considered statistically significant for all tests.
All statistical analyses were performed in SPSS Statistics (version 21; IBM, Chicago, IL, USA).

120
5.4 Results
5.4.1 Pre-Clinical Validation
Ex-vivo feasibility of our experimental optical navigation technology was studied in 6 adult
human cadavers, resulting in the integrated design of navigation with surgical lighting. In- vivo
proof-of-principle validation of OTI was performed on 10 anaesthetized ventilated adult swine
models, where interference between optical illumination for surgical lighting and OTI, both in
the visible spectrum, were studied and minimized. In porcine testing, optical imaging of
subperiosteal dissection planes between soft and bony tissues, cluttered by bleeding and
carbonization effects from electrocautery using standard surgical techniques, was performed to
demonstrate pre-clinical applicability and refine software to appropriately segment osseous
anatomy and eliminate soft tissue using thresholding algorithms. Porcine testing also established
a specification for 3D imaging speed, of <0.5 seconds to acquire the entire operative field using
standard surgical suction to clear pooling blood.
To study navigation accuracy, 71 thoracic and lumbar pedicle screws were inserted and
quantified by comparing intra-operative trajectory data to true screw placement based on
postoperative CT imaging. Median (95%) translational and angular error of the experimental
navigation system in the adult swine model was 1.7 mm (5.1 mm) and 4.4° (13.0°) in the axial
plane, and 1.6 mm (7.8 mm) and 6.5° (17.8°) in the sagittal plane.
5.4.2 Human Clinical Validation
162 thoracolumbar pedicle screws were placed using OTI guidance in human in-vivo clinical
trials, along with 209 pedicle screws by benchmark CAN systems. In radiographic grading, 5.7%
of all navigated screws using either benchmark or OTI systems were graded as a major breach

121
(Heary III-IV), with strong intraclass correlation (ICC 0.725; p < 0.001) and fair inter-rater
agreement (Fleiss’ Kappa (95% CI) 0.248 (0.243 – 0.254); p < 0.0001). There were no
significant differences in major screw breaches rates between OTI and combined benchmark
systems (6.8% vs. 5.3%, p = 0.99). No screws required revision either intra-operatively or
immediately post-operatively during the hospital course, and there were no neurovascular
complications from any instrumentation.
With respect to quantitative navigation application accuracy, median (95%) translational and
angular errors for benchmark systems were 1.1 mm (3.9 mm) and 2.4° (9.0°) in the axial plane,
and 0.8 mm (3.6 mm) and 2.6° (10.1°) in the sagittal plane. For OTI guided screws, median
(95%) translational and angular errors of 1.2 mm (3.4 mm) and 2.2° (8.1°) in the axial plane, and
1.1 mm (4.2 mm) and 2.3° (8.6°) in the sagittal plane, were obtained (Figure 5-6).
In early human clinical testing, in Phase I and the beginning of Phase II, relative displacement
drift between the stereo cameras over time was found to degrade navigation accuracy during the
validation phase, aggravated by the larger thermal expansion coefficients of the 3D printed
plastic material used in the prototype OTI system. An active calibration protocol was therefore
developed to account for camera drift in real-time, implemented after 50 screws had been placed
using OTI guidance. Without active calibration for spinal screw navigation (n=50), the median
(95%) translational and angular errors were 1.3 mm (3.0 mm) and 1.9° (7.6°) in the axial plane,
and 1.6 mm (4.4 mm) and 2.3° (8.2°) in the sagittal plane, vs. 1.0 mm (3.4 mm) and 2.3° (8.1°)
and 0.9 mm (2.6 mm) and 2.5° (7.8°) following implementation of active calibration (n=112).
These differences did not reach statistical significance.
Univariate analysis, accounting for age, gender, surgical navigation method (i.e. benchmark
navigation, experimental OTI navigation) and spine region (cervical, thoracic, lumbar, sacral),
identified age as a predictor for increased axial translational error, and sacral spine region as a
predictor of increased axial angular error vs. the thoracic and lumbar spine. Generalized linear

122
regression confirmed sacral screw location as an independent predictor of increased axial angular
error (p = 0.009; Table 5-1) and advanced age as a predictor of increased axial translational error
(p = 0.005).
With respect to temporal efficiency and workflow, for spinal procedures, the time from DRF
fixation to registration completion with the OTI experimental navigation system was a median
(IQR) of 41s (25 – 68), vs. 258s (143 – 355) for paired-point based benchmark CAN (p < 0.001)
and 794s (609 – 1136) for intra-operative CBCT benchmark CAN (p = 0.001) (Figure 5-2D).
This suggests that intra-operative navigation confers significant accuracy benefit compared to
freehand and fluoroscopy techniques, and that the remarkable gains in surgical workflow
facilitated by the experimental OTI system do not come at the expense of surgical accuracy.

123
Figure 5-6. Bland-Altman analysis comparing benchmark and OTI navigation accuracy. (Left) Correlation plots
with corresponding boxplots comparing predicted intra-operative screw trajectory with actual post-operative screw
trajectory for benchmark (blue) and experimental (red) navigation systems. (Right) Bland-Altman plots comparing
actual screw trajectory with translational and angular deviations for (A) axial translation, (B) sagittal translation, (C)
axial angle, (D) sagittal angle. No statistically significant differences were found.

124
Table 5-1. Navigation error as a function of spine region and navigation technique. Generalized linear model of
navigation error vs. spine region and navigation method. No significant differences between experimental (OTI) and
benchmark techniques were found. (*) denotes significance at < 0.05
Clinical Variables Spine Region and Error
Median (95 percentile)
Navigation Method
Median (95 percentile)
Cervical
N = 10
Thoracic
N = 225
Lumbar
N = 130
Sacral
N = 6
P-Value Benchmark
N = 209
OTI
N = 162
P-Value
Axial Translational
Error (mm)
1.0 (1.7) 1.0 (3.7) 1.5 (3.9) 1.0 (1.9) 0.381 1.1 (3.9) 1.2 (3.4) 0.597
Axial Angular
Error (deg)
2.8 (4.3) 2.1 (8.1) 2.5 (9.5) 6.0 (11.6)* 0.009* 2.4 (9.0) 2.2 (8.1) 0.839
Sagittal
Translational
Error (mm)
1.3 (2.2) 0.9 (1.3) 1.3 (4.1) 0.8 (2.1) 0.437 0.8 (3.6) 1.1 (4.2) 0.214
Sagittal Angular
Error (deg)
1.6 (4.2) 2.6 (9.8) 2.5 (9.5) 3.9 (10.8) 0.485 2.6 (10.1) 2.3 (8.6) 0.492

125
5.5 Discussion
This work represents a major shift in the current surgical paradigm through the introduction of
ultra-fast optical topographic imaging and registration. We have demonstrated the
implementation of an optical topographic imaging modality in spinal surgery, with thorough
clinical and engineering data analysis to ensure surgical accuracy. By using optical imaging
based surface point acquisition and GPU based parallel computing processing, we perform
registration of intra-operative anatomy to pre-operative CT imaging at speed orders of magnitude
faster than current paired-point or automatic registration-based navigation systems. The form
factor of our experimental surgical navigation system has been designed to integrate into the
existing operating room environment, with the benefit of performing imaging and registration
tasks considerably faster than existing technologies. We believe these significant innovations
eliminate the workflow restrictions that have traditionally led somes surgeons to forgo navigation
in favour of freehand approaches.
While the utility of the present study is apparent in the context of spinal procedures, the same
optical topographical imaging technology is suitable for a variety of applications. In particular,
rapid optical topographic imaging allows for frequent repeat registrations, minimizing the
significant target registration errors seen with existing neuronavigation technologies as a result of
progressive brain shift during the procedure.(V. M. Pereira et al., 2015) Frameless stereotactic
navigation is also employed routinely in otolaryngology, with growing applications in
orthopedic, abdominal, and craniomaxillofacial procedures.(L.-P. Amiot & Poulin, 2004;
Hassfeld & Mühling, 2001; Okamoto, Onda, Yanaga, Suzuki, & Hattori, 2015; Peterhans et al.,
2011) The utility of optical topographic imaging techniques is evident in these non-neurosurgical
applications, particularly in those with significant soft-tissue manipulation or deformation, where
rapid repeat registration is required to maintain accurate correlation to pre-operative imaging.
High frequency re-acquisition of intra-operative optical images also lends itself well to
augmented reality, with co-registered images overlaid onto operating microscopes or other
displays employed commonly in multiple surgical disciplines.

126
The salient findings of our study are, first, that intra-operative navigation based on OTI is
accomplished significantly faster than existing technologies. These differences are particularly
pronounced when compared to newer-generation devices employing intra-operative cone-beam
CT scanning, relative to techniques requiring point-matching registration to pre-operative
imaging (Figure 5-2D). Such benefit was enabled by the efficient GPU algorithm, as
demonstrated by the computation time for optical image acquisition and registration at 5.07±1.83
seconds measured over 476 spinal registrations, each consisting of over 250,000 surface points,
with average throughput of over 52,000 points per second, representing an improvement on the
current clinical paradigm, whereby spatial accuracy is maintained while vastly improving
registration time and workflow. Second, for spinal procedures, absolute translational and angular
accuracy of intraoperative navigation is comparable to benchmark technologies (Figure 5-6).
The accuracy measured in this study is the total surgical application accuracy, encompassing
both the navigation system’s technical accuracy with the surgeon’s ability to utilize 3D
navigation data in placing pedicle screws, to which the ease of use of the surgical instruments,
the surgeon’s experience and anatomical knowledge also contribute.(Guha, Jakubovic, Gupta,
Alotaibi, et al., 2017)
The introduction of active calibration protocol is crucial as it facilitates rapid intra-operative re-
registration without exposing the patient to additional radiation. While the exact cause of camera
drift is unknown, several possible factors have been identified including thermal expansion of the
aluminum and acrylonitrile-butadiene-styrene camera housing due to heat produced by the LED
surgical lights, optical drift occurring within the cameras, and torsion stemming from the
structural design of the experimental system and various screw connection sites. These
inaccuracies, while still present in spine though without significant impact on final application
accuracy, are more prominent in cranial applications based on our preliminary unpublished
experiments, where a significant time lag between registration and screw placement exists,
during which surgical steps such as mechanical drilling, cutting, musculocutaneous flap traction,
and patient movement can all introduce navigation error due to relative displacement between
the patient's cranium and the navigation reference. The active calibration protocol obviates the
need for additional intra-operative imaging while maintaining the required surgical accuracy.
While the current analysis comprises the experience of a number of surgeons, the majority of

127
screws navigated with the experimental system were either directly placed or supervised by one
surgeon (VXDY), representing a single-surgeon influence. Larger studies, involving multiple
surgeons, are therefore underway to fully evaluate the evolution of a novice user to a skilled
operator using the experimental navigation system, with multicenter studies representing the
subsequent logical progression.

128
5.6 Conclusions
Optical topographic imaging is a novel and rapid technique for image-to-patient registration,
which has been applied here to intra-operative 3D spinal navigation. We demonstrate in pre-
clinical and human clinical testing that OTI is safe, feasible and comparably accurate to current
commercial navigation techniques for the image-guidance of spinal instrumentation. However,
OTI imparts no intra-operative radiation and permits rapid repeat registration, and does so with a
temporal workflow an order of magnitude faster than existing navigation techniques. OTI may
therefore obviate one of the primary roadblocks to routine usage of navigation for spinal
procedures, paving the way for greater adoption among spinal surgeons.

129
Chapter 6 Optical Topographic Imaging for Spinal Intra-Operative Three-
Dimensional Navigation in Mini-Open Approaches
Preamble
This chapter is modified from the following:
Guha D, Jakubovic R, Alotaibi NM, Klostranec JM, Saini S, Deorajh R, Gupta S, Fehlings MG,
Mainprize TG, Yee A, Yang VXD. Optical topographic imaging for spinal intra-operative three-
dimensional navigation in mini-open approaches: a prospective cohort study of initial pre-
clinical and clinical feasibility. Manuscript in submission.

130
6.1 Abstract
Computer-assisted three-dimensional navigation (CAN) may guide spinal instrumentation.
Optical topographic imaging (OTI) offers comparable accuracy and significantly faster
registration relative to current navigation systems, in open posterior thoracolumbar exposures
(Chapter 5). Here, we aim to validate the utility and accuracy of OTI in minimally-invasive
(MIS) spinal approaches. We conducted a prospective pre-clinical cadaveric and clinical cohort
study. Mini-open midline posterior exposures were performed in four human cadavers. Square
exposures of size 25, 30, 35, and 40mm were registered to preoperative CT imaging. Screw
tracts were fashioned using a tracked awl and probe, and instrumentation placed. Navigation data
were compared to screw positions on postoperative CT imaging, and absolute translational and
angular deviations computed. In-vivo validation was performed in eight patients, with mini-open
thoracolumbar exposures and percutaneous placement of navigated instrumentation. For 37
cadaveric screws, absolute translational errors were (1.8±1.4mm) and (1.8±1.5mm) in the axial
and sagittal planes, respectively; absolute angular deviations were (3.8±2.9) and (3.4±2.8),
respectively (mean±SD). The number of surface points registered by the navigation system, but
not exposure size, correlated positively with the likelihood of successful registration (OR=1.02,
95%-CI 1.009-1.024, p<0.001). 55 in-vivo thoracolumbar pedicle screws were analyzed. Overall
(mean±SD) axial and sagittal translational errors were (1.8±1.4 mm) and (2.7±2.3 mm), while
axial and sagittal angular errors were (3.6±2.9) and (4.6±3.4), respectively. There were no
radiographic breaches >2mm, nor any neurovascular complications. We conclude that OTI has
comparable accuracy for mini-open MIS exposures. The likelihood of successful registration is
affected more by the geometry of the exposure than its size.

131
6.2 Introduction
Intra-operative three-dimensional computer-assisted navigation (CAN) has become standard-of-
care in cranial neurosurgery for the localization of subsurface anatomy. Spinal CAN may guide
instrumentation placement and tissue resection, however adoption has been limited by
cumbersome and lengthy registration protocols, workflow hindrances, steep learning curves and
high costs.(Choo et al., 2008; Hartl et al., 2013; Hecht et al., 2015; Rivkin & Yocom, 2014;
Ryang et al., 2015; Wood & McMillen, 2014)
The utility of CAN is most apparent in minimally-invasive surgery (MIS) and deformity-
correcting procedures, where anatomic landmarks are not directly visible or are significantly
distorted.(Bandiera et al., 2013; Choo et al., 2008; Hartl et al., 2013; Sakai et al., 2008) MIS
techniques, through mini-open, tubular and/or endoscopic approaches, have been shown to
shorten hospital length-of-stay, minimize intra-operative blood loss and improve short-term
patient-reported outcomes, with indeterminate impact on operative time and post-operative
complications, relative to comparable open spinal procedures.(Al-Khouja et al., 2015; Dea et al.,
2015; Goldstein, Macwan, Sundararajan, & Rampersaud, 2016; Hu, Tang, Wu, Zhang, & Ke,
2016; McAnany et al., 2015; Phan & Mobbs, 2016) However, MIS approaches have typically
been guided by intra-operative fluoroscopy or computed tomography. These techniques are
associated with substantial radiation exposure and workflow disruption (Chapter 2).(Francesco
Costa et al., 2016)
Optical topographic imaging (OTI) is a novel technique for 3D surface acquisition, patient-to-
image registration and intra-operative navigation, developed by our research group. OTI registers
significantly faster than current CAN systems with comparable accuracy and without intra-
operative radiation exposure (Chapter 5). This technology obviates many of the limitations of
current CAN techniques.(Choo et al., 2008; Hartl et al., 2013) In its current iteration, OTI
requires line-of-sight to exposed bony anatomy, to allow machine-vision cameras to generate a

132
virtual 3D surface for patient-to-image registration. To date, OTI has been validated only in open
posterior thoracolumbar approaches (Chapter 5).
Here, we assess the ability of OTI to perform successful patient-to-image registration and
accurate intra-operative navigation in mini-open spinal procedures. We explore predictors of
successful registration and their correlation with quantitative navigation accuracy.

133
6.3 Methods
Reporting of all methodology is performed in accordance with the criteria for STrengthening the
Reporting of OBservational studies in Epidemiology (STROBE – www.strobe-statement.org).
6.3.1 Specimen/Patient Selection
Pre-clinical validation was performed in four human cadavers. All cadavers underwent pre- and
post-operative helical CT imaging at 0.5mm slice thickness. Institutional ethics board approval
was obtained (Mount Sinai Hospital REB# 16-0051-E).
For human in-vivo clinical testing, eight patients without history of prior spinal surgery were
enrolled in an ongoing trial of OTI navigation at Sunnybrook Health Sciences Centre (REB#
309-2014 and 086-2015). All patients underwent pre- and post-operative helical CT imaging,
reformatted at 0.625mm slice thickness. To demonstrate non-inferiority of OTI-MIS vs. open
OTI navigation, given standard deviations of 0.6 mm and 1.0° for translational and angular error,
respectively (Chapter 5), and a non-inferiority limit difference of 0.5 mm and 1.0°, respectively,
at α = 0.05 and β = 0.20 (power = 0.80), a minimum sample size of 18 screws is required. All
sample size calculations were performed in R (Version 3.4.1; R Project for Statistical
Computing).
6.3.2 Surgical Technique
Cadavers were placed prone on a standard operating table, with head fixed in a Mayfield clamp.
Mini-open midline posterior exposures of the spinous process and medial bilateral hemilaminae

134
were performed at T2, T6, T10 and L3 (Figure 6-1). A bladed self-retaining retractor was placed.
All cadaveric procedures were performed by a single surgeon (DG).
In human in-vivo clinical testing, posterior instrumented fusions were performed for stabilization
following either trauma, or decompression of bony and epidural tumor. All patients were
positioned prone on a Wilson frame. Mini-open midline exposures were performed for OTI
registration as well as laminectomy (Figure 6-2). All in-vivo procedures were performed by a
single surgeon (VXDY), with trainee assistance.
Figure 6-1. Cadaveric mini-open exposure. Representative cadaveric mini-open posterior midline exposure at T2.
Dynamic reference frame for OTI navigation is clamped to the T2 spinous process. Exposure size of 25x25 mm has
been simulated with sterile towels.

135
Figure 6-2. In-vivo human clinical mini-open exposures. Mini-open posterior midline exposure at T8-9 for Patient
A (A), T10-11 for Patient B (B), and L2 for Patient C (C) in clinical in-vivo validation. Dynamic reference frame
(arrowhead) is clamped to an exposed spinous process in (A), (B) and (C). A tracked drill guide (arrow) and K-wires
were used for percutaneous placement of instrumentation (D).

136
6.3.3 Registration and Intra-Operative Navigation
In cadaveric studies, the retractor width was increased serially to create square exposures of size
25x25, 30x30, 35x35, and 40x40 mm (Figure 6-1). At each level, the exposed anatomy at each
exposure size was registered to pre-operative CT using OTI. Technical details of OTI registration
are described fully in Chapter 5. Briefly, a structured-light pattern is projected onto the exposed
anatomy and recorded by stereoscopic cameras to reconstruct a 3D surface (Figure 6-3). This is
automatically aligned to pre-operative CT imaging using a registration algorithm in real-time.
Registration accuracy was verified manually by placing an optically-tracked awl on bony
landmarks and assessing correlation to the navigation display. Registration was deemed
successful if the OTI system captured sufficient anatomy for patient-to-image registration (≥100
surface points), and if manual verification by the operator demonstrated acceptable accuracy
using identifiable anatomic landmarks with visual and tactile feedback. The number and location
of surface points used by the OTI system for registration were also recorded. At each level, the
30x30 mm exposure was used to place instrumentation. A tracked awl and gearshift probe were
used to fashion pedicle screw tracts at each registered level. Cortical trajectory tracts were also
fashioned at L3. Titanium screws were placed at each level.
In human in-vivo studies, midline mini-open exposures were used for OTI registration, with
similar registration verification as in cadaveric specimens, especially using tactile feedback from
a tracked awl percutaneously on bony landmarks. Screw tracts were then fashioned
percutaneously using the tracked awl, gearshift probe and/or drill-guide, followed by placement
of Kirschner wires. Appropriately-sized cannulated titanium pedicle screws were placed
percutaneously over the Kirschner wires using a standard untracked screwdriver (Figure 6-2D).

137
Figure 6-3. Prototype OTI configuration. Computer-assisted design model of OTI navigation unit integrated into
surgical light head. Structured-light projector (arrow), stereoscopic cameras for 3D surface mapping (arrowheads)
and infrared cameras for tool tracking (*) are shown.
6.3.4 Evaluation of Navigation Accuracy
Absolute quantitative navigation accuracy was measured by comparing the final screw position,
on post-operative CT imaging, to a screenshot of the planned screw trajectory on the navigation
system intra-operatively. Translational and angular deviations from the planned entry point and
trajectory were quantified, in the axial and sagittal planes, using multiplanar reformatting of both
pre- and post-operative CT imaging. The method of absolute navigation error quantification has
been described in Chapter 5 (Figure 5-5).
Radiographic accuracies of all in-vivo screws were graded independently by two radiologists
(JMK, SS), using both the 2mm and Heary classifications.(Heary et al., 2004; W. Zhang et al.,
2016) Screws were dichotomized as acceptable (2mm grade ≤2; Heary grade ≤2) or poor (2mm

138
grade >2; Heary grade >2) per convention.(Guha, Jakubovic, Gupta, Alotaibi, et al., 2017; W.
Zhang et al., 2016)
All image processing and measurements were performed using an OsiriX 64-bit workstation
(version 10.9.5; PIXMEO SARL. Geneva, Switzerland).
6.3.5 Statistical Analysis
Differences in absolute navigation errors between spinal levels were quantified with one-way
ANOVA, with Tukey’s Honest-Significant-Difference test for post-hoc comparisons. Correlation
between the likelihood of successful registration, and the number of surface points used for
patient-to-image registration as well as the size of the exposed anatomy, were performed using
multiple logistic regression models. Hierarchical mixed-effects general linear modelling was
employed to adjust for second-order differences between cadavers/patients, where required based
on univariate analyses. In-vivo MIS cases were matched 1:2 based on age/gender/spinal level,
and separately based on mean pedicle diameter, to patients who had undergone open
thoracolumbar instrumentation using OTI guidance in our prior trial (Chapter 5). Significance
levels for all tests were set at < 0.05.
All statistical analyses were performed in SPSS Statistics (version 21; IBM. Chicago, IL, USA).

139
6.4 Results
For the four cadavers used in pre-clinical validation, mean age at death was 91.4 years (range 83-
96). 37 screws from the four cadavers were included in our analysis: 8 pedicle screws at T2, 10
at T6, 9 at T10, and 4 pedicle and 6 cortical screws at L3.
In-vivo clinical feasibility was assessed in eight patients, with mean age 57.2 years. 55
thoracolumbar pedicle screws placed with CAN from mini-open OTI registrations were
analyzed, bilaterally at T8-9 for Patient A, T6-11 for Patient B, T12-L4 for Patient C, T12-L1 for
Patient D, T11-L3 for Patient E, T10-L2 for Patients F and G, and T9-11 for Patient H. Mean (±
SD) pedicle diameter was 4.4 ± 3.5 mm.
6.4.1 Image-to-Patient Registration
In the cadaveric study, we systematically studied the attributes of successful registrations with
OTI and compared them to unsuccessful registrations. A total of 131 registration attempts were
made through mini-open exposures of varying sizes, with 71.8% verified by the operator as
successful based on correlation between imaging and anatomic bony landmarks (Table 6-1). The
likelihood of successful registration was greater at T2 than at any other tested spinal level
(OR=6.02, 95%-CI 1.47-24.63, p=0.013). The minimum tested exposure of 25x25 mm allowed
successful registration in 66.7% of attempts at T2, 80.0% of attempts at T6, 33.3% of attempts at
T10, and 25.0% of attempts at L3. Successful registration in more than 70% of attempts
necessitated a minimum exposure of 25x25 mm at T6, 30x30 mm at T2 and T10, and 35x35 mm
at L3. The mean wound depths at T2 (5.89 cm) and L3 (5.68 cm) were significantly greater than
at T6 (3.23 cm) or T10 (3.50 cm) (p<0.001), however wound depth did not correlate with the
likelihood of successful registration.

140
Overall, (431 ± 235) surface points (mean ± SD) were used by the OTI system for patient-to-
image registration, (502 ± 231) points for successful registrations and (250 ± 120) for
unsuccessful registrations. Significantly fewer points were acquired and used by the system at
the smallest exposure of 25x25 mm (mean 303 points, p=0.039), with no significant differences
in the number of points registered at 30x30, 35x35 or 40x40 mm exposures (Figure 6-4).
In multiple logistic regression modelling, the number of surface points registered by the OTI
system correlated positively with the likelihood of successful registration, independent of spinal
level, exposure size and wound depth (OR=1.02, 95%-CI 1.009-1.024, p<0.001).
In human clinical testing, 9 registrations through MIS exposures were performed, 2 in Patient B
for the placement of T6-8 and T9-11 screws, respectively, and 1 registration each for all other
patients. All registrations were successful on the first attempt, using the representative exposures
demonstrated in Figure 6-2.
6.4.2 Quantitative Navigation Application Accuracy
In cadaveric testing, overall (mean ± SD) axial and sagittal translational errors were (1.8 ± 1.4
mm) and (1.8 ± 1.5 mm), while axial and sagittal angular errors were (3.8 ± 2.9) and (3.4 ±
2.8), respectively. There were no significant differences in errors between levels, nor between
pedicle and cortical trajectory screws (Figure 6-5). The number of points registered by OTI did
not significantly correlate with any metric of absolute navigation error.
From in-vivo testing, overall (mean ± SD) axial and sagittal translational errors were (1.8 ± 1.4
mm) and (2.7 ± 2.3 mm), while axial and sagittal angular errors were (3.6 ± 2.9) and (4.6 ±
3.4), respectively (Figure 6-6). In univariate analyses, there were no statistically-significant

141
differences in absolute navigation errors between cadaveric and clinical studies. MIS screws
showed increased quantitative error, relative to matched open thoracolumbar controls, in axial
translation (1.8 ± 1.4 mm vs. 1.0 ± 0.9 mm, p=0.004), axial angle (3.6 ± 2.9 vs. 2.7 ± 2.1,
p=0.032), sagittal translation (2.7 ± 2.3 mm vs. 1.0 ± 0.9 mm, p<0.001), and sagittal angle (4.6 ±
3.4 vs. 2.8 ± 2.3, p=0.006). These differences persisted when matching was performed by
pedicle diameter rather than age/gender/spinal level. However, in general linear modelling
including distance from the registered level as a covariate, there were no significant differences
in any quantitative errors between MIS and open thoracolumbar cases. All in-vivo screws were
placed 0, 1 or 2 vertebral levels from the registered level. Increasing distance between the
instrumented and registered levels correlated positively with increased axial translational error
(Pearson correlation coefficient 0.534, p = 0.007).
Table 6-1. Characteristics of cadaveric OTI registrations through mini-open exposures.
Level Successful registrations (%
of total)
Number of registered
points (mean ± SD)
T2 85.7% 355 ± 152
T6 82.1% 608 ± 288
T10 67.6% 440 ± 234
L3 58.5% 353 ± 173
Overall 71.8% 431 ± 235

142
Figure 6-4. Correlation of registered points to exposure size and spinal level. Standard boxplots demonstrating
the number of surface points registered by OTI stratified by exposure size (A), and by registered level (B), in
cadaveric testing. Boxes represent the first, median and third quartiles. Whiskers represent 1.5x the interquartile
range. * represents significance at p<0.05.
Figure 6-5. Navigation application accuracy, by spinal level, in cadaveric testing. Standard boxplots
demonstrating the absolute translational (A) and angular (B) navigation errors in the axial and sagittal planes,
stratified by registered level and screw trajectory, in cadaveric testing. Boxes represent the first, median and third
quartiles. Whiskers represent 1.5x the interquartile range.

143
Figure 6-6. Navigation application accuracy, by spinal level, in clinical testing. Standard boxplot demonstrating
the absolute translational (A) and angular (B) navigation errors in the axial and sagittal planes, in clinical in-vivo MIS
testing. Boxes represent the first, median and third quartiles. Whiskers represent 1.5x the interquartile range.
6.4.3 Radiographic Navigation Accuracy
From two independent raters, an average of 94.5% of in-vivo screws were rated as acceptable on
the 2mm grade, and 100% rated acceptable by the Heary classification. Three screws were rated
as poor (Grade >2) on the 2mm classification by one or both raters. All three screws were placed
in lumbar vertebrae (L3 or L4) intentionally with a more lateral starting point, at the junction of
the transverse process and superior articular process (Figure 6-7). This is a well-documented
technique allowing docking of the awl against the transverse process/facet junction for tactile
feedback in a percutaneous procedure, to reduce the profile of the screw heads, and to avoid
damaging the superior facet capsule.(Wong et al., 2014)
There were no critical radiographic breaches, and no neurovascular or other clinical
complications from any in-vivo instrumentation.

144
Figure 6-7. Representative intentional placement of a poorly-graded screw. Axial (A) and sagittal (B)
multiplanar-reformatted CT imaging demonstrating a percutaneously-inserted right L4 screw, with starting point
intentionally at the junction of the transverse process and superior articular process, and graded as ‘poor’ by the 2mm
classification.

145
6.5 Discussion
The primary purported benefit of CAN for spinal procedures is improved instrumentation
accuracy and, in theory, minimization of acute and long-term complications from misplaced
screws. CAN has been shown to reduce pedicle screw breach rates from 12-40%, under freehand
or fluoroscopic guidance, to under 5% with 3D CAN.(L. P. Amiot et al., 2000; M Bydon et al.,
2014; Castro et al., 1996; E W Nottmeier, Seemer, & Young, 2009; B. J. Shin et al., 2012; Y
Wang et al., 2013) Improved instrumentation accuracy is seen across all 3D CAN techniques,
registering to pre- or intra-operative imaging, in each of the cervical, thoracic, lumbar and sacral
regions.(Barsa et al., 2016; Austin C Bourgeois et al., 2015; Hecht et al., 2010; Mason et al.,
2014; N. F. Tian et al., 2011)
Workflow disturbances continue to limit the usage of CAN among spinal surgeons, though the
technology has been adopted more readily by specialists in MIS and complex deformity surgery,
where bony landmarks may not be readily identifiable. While OTI has been validated previously
as a comparably accurate yet significantly faster technique of intra-operative navigation relative
to current CAN systems, its utility in mini-open procedures, with limited line-of-sight to exposed
anatomy, has been unproven to date.
Our group has previously quantified absolute navigation accuracy, for the first time, in current
CAN techniques registered to pre- or intra-operative imaging, as well as in OTI for open
thoracolumbar exposures.(Jakubovic et al., 2016) In our current analysis, while not reaching
statistical significance, there was a trend towards increased translational and angular errors for
MIS exposures in clinical testing relative to pre-clinical cadaveric validation. This is likely due
in part to the placement of in-vivo screws percutaneously over K-wires, but without a navigated
screwdriver, which may have led to deviation of the final screw placement from the original
navigated tract. Furthermore, in-vivo screws were placed percutaneously at up to 2 levels distant
from the registered level, potentially introducing error due to intersegmental mobility.

146
Corroborating this theory, absolute translational and angular errors for in-vivo MIS exposures
were slightly greater, in both axial and sagittal planes, than those obtained using OTI for open
thoracolumbar exposures, but not significantly once distance from the registered level was
accounted for in general linear modelling. The literature on the impact of non-segmental
registration on navigation accuracy is heterogeneous, both in outcomes as well as in the metrics
used to quantify navigation accuracy.(Elias C Papadopoulos, Girardi, Sama, Sandhu, &
Cammisa; Scheufler et al., 2011b; Shimizu et al., 2014) The quantitative translational accuracy
of OTI for MIS remains within 2-3mm, comparing favorably to the accuracy of current
commercial CAN systems. Moreover, the radiographic accuracy of screws placed following
MIS-OTI registrations was 100% by the Heary classification, with no clinical complications. The
slightly greater quantitative inaccuracy in MIS vs. open OTI procedures is likely related to the
percutaneous placement of screws rather than the registration itself, as the lack of visual
anatomic feedback and the unavailability of a tracked screwdriver, with an untapped screw tract,
allow for increased error in screw placement relative to the intended navigation-guided
trajectory.
The ability of OTI to perform patient-to-image registration is contingent on the acquisition of
sufficient exposed points that can be correlated, using an iterative closest-point algorithm, to
corresponding points on a pre-operative image set. As this is most readily performed on bony
anatomy, standard midline mini-open exposures were chosen for this initial demonstration of
feasibility for MIS approaches. Cadaveric registrations were performed in the upper, middle and
lower thoracic spine as well as lumbar spine, where the bulk of current MIS procedures are
performed.(Banczerowski et al., 2015; Z. A. Smith & Fessler, 2012) Pedicle screws were
inserted at all levels. Concurrent cortical-trajectory screws were placed at L3, as cortical screws
are commonly placed in MIS midline decompression and fusion procedures to achieve greater
bony purchase with minimal muscle dissection and soft-tissue retraction.(Phan, Hogan, Maharaj,
& Mobbs, 2015; Wray et al., 2015)
We found that the number of surface points acquired and registered by the navigation system
correlated positively with the likelihood of successful registration. The first quartile of registered

147
points for successful registrations and the third quartile for unsuccessful registrations converged
at approximately 325 points. The number of registered points did not, however, correlate with
any absolute navigation error. In this iteration of OTI, 325 registered points should therefore be
targeted as the minimum for successful registration through an MIS exposure, with more points
increasing the likelihood of successful registration but not final navigation accuracy.
While the number of surface points registered by OTI was correlated with the likelihood of
successful registration, the size of the exposure itself was not an independent predictor of
registration success. Therefore, while smaller exposures are considered the definition of
‘minimally-invasive’, it is the quality of the exposed anatomy rather than the size itself which
most affects the likelihood of successful registration with OTI. Regions with more geometric
variability, and hence a greater number of unique points that may be used for patient-to-image
registration, are more likely to be registered successfully even with a smaller skin opening, than
regions with geometric homogeneity. For instance, to achieve a minimum 70% likelihood of
registration success, a minimum 35x35 mm exposure was required in the lumbar spine, while
25x25 mm and 30x30 mm exposures were sufficient in the thoracic spine. This may be due in
part to geometric symmetry in the medial lumbar hemilaminae, and in part to the increased depth
of lumbar surgical cavities, resulting in increased shadowing and fewer captured points for an
optically-based acquisition system. The latter represents a known technical challenge with OTI,
one that is readily rectifiable with modified camera and projector alignments.
There are multiple limitations to our analysis. The armamentarium of MIS spinal surgeons
includes tubular ports and retractors, which were unavailable in the cadaveric study for
systematic testing of registration success. Percutaneous placement of instrumentation is
performed best with a tracked screwdriver to ensure no deviation from the navigated screw tract.
Future studies of OTI for MIS applications should include percutaneous placement of
instrumentation distant from the level of registration and reference-frame fixation, while
accounting for the additional sources of navigation error arising from non-segmental registration.

148
6.6 Conclusions
Optical machine-vision is a novel navigation technique previously validated for open posterior
exposures. OTI is feasible for mini-open MIS exposures in pre-clinical and initial clinical testing,
with comparable radiographic accuracy to that achieved by OTI in open exposures. The
likelihood of successful registration is dependent on the number of points acquired and registered
by the navigation system, but not exposure size. With the exception of sagittal angular deviation,
absolute navigation accuracy is unaffected by the size of the MIS exposure, or by the number of
registered points. Future work exploring the feasibility of OTI registration through tubular
minimal-access approaches is warranted.

149
Chapter 7 Optical Topographic Imaging for Spinal Intra-Operative Three-
Dimensional Navigation in the Cervical Spine
Preamble
This chapter is modified from the following:
Guha D, Jakubovic R, Alotaibi NM, Deorajh R, Gupta S, Fehlings MG, Mainprize TG, Yee A,
Yang VXD. Optical topographic imaging for spinal intra-operative three-dimensional navigation
in the cervical spine: initial pre-clinical and clinical feasibility. Manuscript in submission.

150
7.1 Abstract
Computer-assisted three-dimensional navigation may guide spinal instrumentation. Optical
topographic imaging (OTI) offers comparable accuracy and significantly faster registration
workflow relative to current navigation systems. It has previously been validated in open
posterior thoracolumbar exposures. Here, we aim to validate the utility and accuracy of OTI in
the cervical spine. We conducted a prospective pre-clinical cadaveric and clinical cohort study,
on 4 human formalin-fixed cadavers, and 15 patients undergoing first-time posterior cervical
decompression and instrumented fusion, guided by intra-operative OTI navigation. In both pre-
clinical and clinical validation, standard midline open posterior cervical exposures were
performed, with segmental OTI registration. In cadaveric testing, a tracked drill guide was used
to cannulate screws tracts in the lateral mass at C1, pars at C2, lateral mass at C3-6, and pedicle
at C7. In clinical testing, translaminar screws at C2 were also analyzed in addition. Navigation
data were compared to screw positions on post-operative CT imaging, and absolute translational
and angular deviations computed. In cadaveric testing, (mean ± SD) axial and sagittal
translational errors were (1.7 ± 1.2 mm) and (2.1 ± 2.2 mm), while axial and sagittal angular
errors were (4.1 ± 3.8) and (7.0 ± 5.4), respectively. In clinical validation, (mean ± SD) axial
and sagittal translational errors were (1.9 ± 1.4 mm) and (1.3 ± 1.0 mm), while axial and sagittal
angular errors were (3.7 ± 2.6) and (3.5 ± 2.9), respectively. There were no radiographic facet,
canal or foraminal violations, nor any neurovascular complications. We conclude that optical
machine-vision is a novel navigation technique allowing efficient initial and repeat registration.
Accuracy even in the more-mobile cervical spine is comparable to current spinal neuronavigation
systems.

151
7.2 Introduction
Intra-operative three-dimensional computer-assisted navigation (CAN) has become standard-of-
care in cranial neurosurgery for the localization of subsurface anatomy. CAN in spinal surgery
may guide instrumentation placement as well as bony and soft-tissue resection, however
adoption has been limited by cumbersome and lengthy registration protocols, spatial and
temporal workflow hindrances, steep learning curves and high costs. (Choo et al., 2008; Hartl et
al., 2013; Hecht et al., 2015; Rivkin & Yocom, 2014; Ryang et al., 2015; Wood & McMillen,
2014)
In current practice, the utility of CAN is most apparent in minimally-invasive and deformity-
correcting procedures in the thoracolumbar spine, where anatomic landmarks are not directly
visible or are significantly distorted.(Bandiera et al., 2013; Choo et al., 2008; Hartl et al., 2013;
Sakai et al., 2008) Navigation may play an increasing role in the cervical spine, for the
placement of minimally-invasive instrumentation in the setting of acute trauma, for fixation of
the atlantoaxial spine and craniocervical junction, and for the placement of cervical pedicle
screws which are biomechanically superior to lateral mass fixation.(Komatsubara et al., 2016;
Shimokawa & Takami, 2016a; J. D. Smith et al., 2016) However, the cervical spine is inherently
more mobile than the thoracolumbar spine, with narrower pedicles and tighter tolerances, hence
navigation inaccuracy due to intersegmental mobility is of significant concern with most current
CAN systems. Unsurprisingly, the reported radiographic accuracy of current 3D-CAN systems is
typically lower in the cervical than in the thoracolumbar spine.(Mason et al., 2014; N. F. Tian et
al., 2011)
Optical topographic imaging (OTI) is a novel technique for 3D surface anatomy acquisition,
patient-to-image registration and intra-operative navigation, developed by our research group.
OTI registers significantly faster than current CAN systems, without intra-operative radiation
exposure and with comparable accuracy in open thoracolumbar approaches (Chapter 5). This

152
technology obviates many of the limitations of current CAN techniques.(Choo et al., 2008; Hartl
et al., 2013) Here, we assess the ability of OTI to perform successful patient-to-image
registration and accurate intra-operative navigation in the mobile cervical spine, in pre-clinical
cadaveric models and in initial human clinical testing.
7.3 Methods
Reporting of all methodology is performed in accordance with the criteria for STrengthening the
Reporting of OBservational studies in Epidemiology (STROBE – www.strobe-statement.org).
7.3.1 Specimen/Patient Selection
Pre-clinical validation was performed in four human cadavers. All cadavers underwent pre- and
post- operative helical CT imaging at 0.5mm slice thickness. Institutional ethics board approval
was obtained (IRB# 16-0051-E).
In human in-vivo clinical validation, 15 patients without history of prior spinal surgery were
enrolled in an ongoing prospective trial of OTI navigation at Sunnybrook Health Sciences Centre
(IRB# 309-2014 and 086-2015). All patients underwent pre- and post- operative helical CT
imaging, reformatted at 0.625mm slice thickness. To demonstrate non-inferiority of OTI for
open cervical vs. thoracolumbar approaches, given standard deviations of 0.6 mm and 1.0° for
thoracolumbar translational and angular error, respectively (Chapter 5), and a non-inferiority
limit difference of 0.5 mm and 1.0°, respectively, at α = 0.05 and β = 0.20 (power = 0.80), a
minimum sample size of 18 screws is required. All sample size calculations were performed in R
(Version 3.4.1; R Project for Statistical Computing).

153
7.3.2 Surgical Technique
Cadavers were positioned prone on a standard operating table, with head fixed in a Mayfield
clamp. Standard midline posterior exposures were performed from occiput to the cervicothoracic
junction, with exposure of the medial 1.5 cm of the posterior arch of C1, and the entire lateral
masses of C3-7. All cadaveric procedures were performed by a single surgeon (DG).
In human in-vivo testing, all patients underwent open posterior cervical instrumented fusion for
traumatic or degenerative pathologies. All patients were positioned prone on a Wilson frame,
with head fixed in a Mayfield clamp. Standard midline open posterior exposures were used for
all cases. In-vivo procedures were performed by a single surgeon (VXDY), with trainee
assistance.
7.3.3 Registration and Intra-Operative Navigation
In cadaveric testing, the exposed anatomy at each level was individually registered to pre-
operative CT using OTI, with the dynamic reference frame (DRF) clamped to the spinous
process of the registered level. Registration at C1 was performed segmentally, but with the DRF
clamped on C2 due to the lack of a C1 spinous process. Technical details of OTI registration are
described separately.(Jakubovic et al., 2016) Briefly, a structured-light pattern is projected onto
the exposed anatomy and recorded by stereoscopic visible-band cameras to reconstruct a 3D
surface point cloud. This is automatically aligned to pre-operative CT imaging using a
segmentation and registration algorithm in real-time.
Registration accuracy was verified manually by placing an optically-tracked awl on bony
landmarks and assessing correlation to the navigation display. Registration was deemed

154
successful if the OTI system captured sufficient anatomy for patient-to-image registration (≥100
surface points), and if manual verification by the operator demonstrated acceptable accuracy
with visual and tactile feedback.
An optically-tracked drill guide (Medtronic Sofamor Danek; Memphis, TN, USA) was used with
OTI navigation to fashion pilot holes for screw tracts in the C1 lateral mass, C2 pars, and C3-6
lateral mass (Figure 7-1). A tracked awl and gearshift probe were used to fashion tracts for C7
pedicle screws. Appropriately-sized titanium instrumentation was then placed using an untracked
screwdriver. Screw holes were not tapped.
In human in-vivo validation, segmental OTI registration, tract cannulation, and instrumentation
placement were performed similar to cadaveric testing.
Figure 7-1. Tracked cervical drill guide navigated with OTI. (A) Tracked drill guide used to cannulate all cervical
screw tracts with OTI navigation guidance. (B) OTI navigation (rectangle) integrated into surgical light head, guiding
placement of a C4 lateral mass screw.

155
7.3.4 Evaluation of Navigation Accuracy
Absolute quantitative navigation accuracy was measured by comparing the final screw position,
on post-operative CT, to a screenshot of the planned screw trajectory on the navigation system
intra-operatively. Translational and angular deviations from the planned entry point and
trajectory were quantified, in the axial and sagittal planes, using multiplanar reformatting of both
pre- and post- operative CT imaging. The method of absolute navigation error quantification has
been described by our group previously in Chapters 5 and 6, and adapted for use in the cervical
spine (Figure 7-2).(Guha, Jakubovic, Gupta, Alotaibi, et al., 2017; Y. Kotani et al., 2007;
Mathew et al., 2013)
Radiographic accuracy of all in-vivo screws were graded using the 2mm classification of Neo et
al..(Neo, Sakamoto, & Fujibayashi, 2005) Screws were dichotomized as acceptable (deviation
≤2mm) or unacceptable (deviation >2mm) per convention.
All image processing and measurements were performed using an OsiriX 64-bit workstation
(version 10.9.5; PIXMEO SARL. Geneva, Switzerland).

156
Figure 7-2. Quantification of absolute navigation application accuracy. Measurement of absolute navigation
accuracy, in the axial (A+B) and sagittal (C+D) planes. Comparison is made between intra-operative navigation
screenshots of planned entry points and trajectories (A+C), to final screw placement on post-operative CT (B+D).
Reference lines (dashed) are drawn, in the axial plane in the mid-sagittal line, and in the sagittal plane along the
superior endplate. Translational error is computed as (d1-d); angular error is computed as (1-).

157
7.3.5 Statistical Analysis
Differences in absolute navigation errors between spinal levels, and between the cervical cohort
in this study and the thoracolumbar cohort from our prior trial of OTI, were quantified with one-
way ANOVA with Tukey’s Honest-Significant-Difference test for post-hoc comparisons.
Correlation between radiographic cervical spondylosis, based on Kellgren grade (Table 7-1), and
navigation errors were assessed using general linear modelling.(Ofiram et al., 2009) Hierarchical
mixed-effects general linear modelling was employed to adjust for second-order differences
between cadavers/patients, where required based on univariate analyses. In-vivo cases were
matched 1:1 based on age and gender, to patients who had undergone open thoracolumbar
instrumentation using OTI guidance in our prior trial.(Jakubovic et al., 2016) Significance levels
for all tests were set at < 0.05.
All statistical analyses were performed in SPSS Statistics (version 21; IBM. Chicago, IL, USA).
Table 7-1. Kellgren classification of radiographic cervical spondylosis.
Grade Definition
0 No anterior osteophytes
0-25% disc space narrowing
No endplate sclerosis
No olisthesis
1 Minimal anterior osteophyte formation (<2mm)
25-50% disc space narrowing
Minimal endplate sclerosis
Olisthesis <3mm
2 Moderate anterior osteophyte formation (2-4mm)
50-75% disc space narrowing
Moderate endplate sclerosis
Olisthesis 3-5mm
3 Large anterior osteophyte formation (>4mm)
75-100% disc space narrowing
Severe endplate sclerosis
Olisthesis >5mm

158
7.4 Results
For the four cadavers used in pre-clinical validation, mean age at death was 91.4 years (range 83-
96). No significant cervical deformity was evident in any cadaver, however significant
osteophyte bridging across the lateral masses was seen in two (Kellgren Grade 3). 53 screws
from 4 cadavers were included in our analysis, encompassing C1 lateral mass, C2 pars, C3-6
lateral mass and C7 pedicle screws (Table 7-2).
In-vivo clinical feasibility was assessed in 15 patients, with mean age 61.1 years (range 34-78).
74 cervical screws placed with OTI guidance were analyzed, lateral mass at C1, pars and
translaminar at C2, lateral mass at C3-6, and pedicle at C7 (Table 7-2).
Table 7-2. Number of screws in cadaveric and clinical testing, by level and Kellgren grade.
Abbreviations: LM – lateral mass; TL – translaminar
Level
C1 LM C2 pars C2 TL C3-6 LM C7 pedicle TOTAL
Cadaveric
Kellgren Grade 0 0 0 0 0 0
1 2 4 0 16 4
2 0 0 0 0 0
3 3 4 0 16 4
5 8 0 32 8 53
In-vivo
Kellgren Grade 0 0 0 0 5 0
1 0 6 0 19 5
2 0 2 2 12 4
3 0 0 0 19 0
0 8 2 55 9 74
5 16 2 87 17 127

159
7.4.1 Quantitative Navigation Application Accuracy
In pre-clinical cadaveric testing, overall (mean ± SD) axial and sagittal translational errors were
(1.7 ± 1.2 mm) and (2.1 ± 2.2 mm), while axial and sagittal angular errors were (4.1 ± 3.8) and
(7.0 ± 5.4), respectively (Figure 7-3). There were no significant differences in errors between
levels, nor any correlation between radiographic cervical degeneration, based on Kellgren
classification, and any metric of absolute navigation error.
In clinical validation, overall (mean ± SD) axial and sagittal translational errors were (1.9 ± 1.4
mm) and (1.3 ± 1.0 mm), while axial and sagittal angular errors were (3.7 ± 2.6) and (3.5 ±
2.9), respectively (Figure 7-4). There were no significant differences in errors between levels,
nor correlation with radiographic cervical spondylosis. In univariate analyses, sagittal
translational and angular error were significantly greater in cadaveric than in-vivo testing
(p<0.001). There were no differences in any error metric between matched cervical cases and
open thoracolumbar controls.
7.4.2 Radiographic Navigation Accuracy
No radiographic breach was observed in any cadaveric or in-vivo C1, C2 or C7 screws (Neo
Grade 0). There were no unintentional facet violations for any lateral mass screws placed at C3-
6. There were no neurovascular or other clinical sequelae of any placed screws in clinical testing.

160
Figure 7-3. Absolute navigation application accuracy in cadaveric testing. Standard boxplots demonstrating the
translational (top) and angular (bottom) absolute navigation errors, in cadaveric testing. Boxes represent the first,
median and third quantiles. Whiskers represent 1.5x the interquartile range.

161
Figure 7-4. Absolute navigation application accuracy in clinical testing. Standard boxplots demonstrating the
translational (A) and angular (B) absolute navigation errors, in clinical in-vivo testing. Boxes represent the first,
median and third quantiles. Whiskers represent 1.5x the interquartile range.

162
7.5 Discussion
We demonstrate here that application accuracy in the cervical spine of optical topographic
imaging, a novel technique for image-to-patient registration and intra-operative navigation, is
comparable to that in open thoracolumbar procedures and to currently-available navigation
devices.(Jakubovic et al., 2016) The workflow advantages associated with OTI in the
thoracolumbar spine are maintained with comparable accuracy in the cervical spine.
The most frequently cited benefit of CAN for spinal procedures is improved instrumentation
accuracy, and minimization of associated acute and long-term complications from misplaced
hardware. CAN has been shown to reduce pedicle screw breach rates from 12-40%, under
freehand or fluoroscopic guidance, to under 10% with 3D CAN.(L. P. Amiot et al., 2000; M
Bydon et al., 2014; Castro et al., 1996; Eric W Nottmeier et al., 2009; B. J. Shin et al., 2012; Y
Wang et al., 2013) Improved instrumentation accuracy is seen across all 3D CAN techniques,
registering to pre- or intra-operative imaging.(Mason et al., 2014) In one of the most recent meta-
analyses on CAN-guided instrumentation accuracy, 3D-CAN was shown to result in pedicle
screw accuracy of 96.7% in the lumbosacral spine, 93.2% in the thoracic spine, and 90.3% in the
cervical spine, with the finding of reduced CAN accuracy in the cervical spine echoed in an
earlier review.(Mason et al., 2014; N. F. Tian et al., 2011)
The reduced accuracy of cervical CAN in the literature is likely due in part to the focus of
previous publications on navigated subaxial pedicle screws specifically, rather than the more
common lateral mass and C2 pars/translaminar implants. Radiographic accuracy has also been
evaluated purely on ordinal classifications based on some variant of 2mm gradients, which is not
necessarily reflective of quantitative application accuracy.(Guha, Jakubovic, Gupta, Alotaibi, et
al., 2017; Neo, Sakamoto, & Fujibayashi, 2005) In addition, navigation for cervical procedures is
often performed with non-segmental registration. That is, the dynamic reference frame (DRF) is
affixed to either a head clamp or to the cervicothoracic junction, distant from the level being

163
instrumented to avoid the DRF obstructing the surgeon’s hands as may often occur with C1/2
instrumentation, where CAN guidance is most useful. As intersegmental mobility is typically
greater in the cervical spine, this practice may lead to increased navigation error.(Tauchi et al.,
2013) In our analysis, we demonstrate equivalent navigation accuracy with OTI in our cervical
cohort and our prior open thoracolumbar cases. This is likely due largely to our practice of
registering each instrumented level segmentally, a technique facilitated by the rapid registration
workflow of OTI, which thereby eliminates error from intersegmental mobility.
Sagittal translational and angular errors in our clinical cohort were significantly lower than those
observed in pre-clinical cadaveric testing. This is likely due in part to the significantly older age
of the cadaveric specimens, with commensurately greater degenerative cervical spondylosis. Half
of the cervical screws in cadaveric testing were placed in severely degenerated spines (Kellgren
Grade 3), whereas only 19 of 74 screws (25.6%) in clinical testing were placed in Kellgren
Grade 3 spines. Facet arthrosis in the more severely degenerated cadaveric cervical spines,
resulting in poorer vertebral segmentation with machine vision, is a likely contributor to the
increased sagittal-plane errors observed in cadaveric testing, however without ultimate
radiographic misplacement. In the setting of severe facet arthrosis, therefore, clinicians should be
cognizant to carefully verify navigation accuracy manually based on correspondence to known
anatomic landmarks.
There are multiple limitations to our analysis. 87 of the 127 screws analyzed in combined
cadaveric and clinical testing were lateral mass implants at C3-6. While it is well-documented
that freehand placement of C3-6 lateral mass instrumentation is safe, obviating the need for
navigation, these screws were analyzed here to quantitatively assess OTI application
accuracy.(H.-S. H.-S. Kim et al., 2014) Future studies of OTI may include larger prospective
cohorts of C1/2 instrumentation.

164
7.6 Conclusions
Optical topographic imaging is a novel navigation technique previously validated for open
posterior thoracolumbar exposures. We show here that OTI is feasible and comparably accurate
in open posterior cervical approaches. Accuracy is not dependent on the instrumented spinal
level. Careful manual verification of navigation accuracy should be performed particularly with
severe facet arthrosis, to minimize the likelihood of navigation error.

165
Chapter 8 Error Propagation in Spinal Intra-Operative Three-Dimensional
Navigation from Non-Segmental Registration
Preamble
This chapter is modified from the following:
Guha D, Jakubovic R, Gupta S, Fehlings MG, Mainprize TG, Yee A, Yang VXD. Intra-operative
error propagation in three-dimensional spinal navigation from non-segmental registration: a
prospective cadaveric and clinical study. Manuscript in submission.

166
8.1 Abstract
Spinal instrumentation may be guided by intra-operative computer-assisted navigation (CAN).
Current systems rely on a dynamic reference frame (DRF) for image-to-patient registration and
tool tracking. Working distant to a DRF may generate inaccuracy from intrinsic limitations of
optical tool tracking, and from intersegmental mobility during surgical manipulation and patient
respiration. Our aim in this study was to quantitate and identify predictors of absolute navigation
error as a function of distance from the registered vertebral level, and from intersegmental
mobility due to surgical manipulation and patient respiration. We conducted a prospective pre-
clinical and clinical cohort study involving 4 human formalin-fixed cadavers, and 10 patients
undergoing first-time posterior cervical/thoracic/lumbar instrumented fusion ± decompression,
guided by intra-operative three-dimensional CAN. Navigation error from working distant to the
level to which the DRF is affixed, and from surgical manipulation, was quantified in four human
cadavers. The 3D position of a tracked tool tip at 0-5 levels from the DRF, and during the
targeting of a pedicle screw tract, was captured in real-time by an optical navigation system.
Respiration-induced vertebral motion was quantified from 10 clinical cases of open posterior
instrumented fusion. The 3D position of a custom spinous-process clamp was tracked over 12
respiratory cycles using an optical navigation system. Data on patient and ventilator parameters
were collected. Absolute quantitative translational navigation error was computed in 3D, and in
each of the component medio-lateral (ML), antero-posterior (AP), and cranio-caudal (CC) axes.
We observed an increase in mean quantitative 3D navigation error of ≥ 2 mm from baseline at ≥2
levels distant from the DRF in the cervical and lumbar spine, due predominantly to increased
error in the AP axis. (Mean ± SD) displacement due to surgical manipulation was 1.6 ± 1.1 mm
in 3D across all levels, ≥ 2 mm in 17.4%, 19.2% and 38.5% of levels in the cervical, thoracic and
lumbar spine, respectively. (Mean ± SD) absolute respiration-induced 3D motion was 2.0 ± 1.3
mm, greatest in the lower thoracic spine (p<0.001). TV and PEEP correlated positively with
increased vertebral displacement. We concluded therefore that vertebral motion is unaccounted
for during image-guided surgery when performed at levels distant from the DRF. Navigating
instrumentation within 2 levels of the DRF is likely to minimize the risk of navigation error.
While respiration- and manipulation-induced vertebral motion is typically small, there is
significant variability in magnitude, particularly with spinal region and ventilator parameters.

167

168
8.2 Introduction
Intra-operative three-dimensional computer-assisted navigation (CAN) in spinal procedures may
guide instrumentation placement as well as bony and soft-tissue resection. Contemporary
navigation systems register patient anatomy to an imaging dataset, allowing real-time instrument
tracking and/or robotic guidance in the virtualized environment. Whether the imaging data is
acquired pre-operatively, as CT or MRI, or intra-operatively, as 2D/3D-fluoroscopy or CT,
current CAN systems rely on a dynamic reference frame (DRF) for maintaining the image-to-
patient registration and tool tracking (Chapter 2). The accuracy of spinal CAN systems has been
studied extensively, and varies by registration and imaging technique as well as spinal
region.(Du et al., 2017; Laudato, Pierzchala, & Schizas, 2017; Mason et al., 2014; N. F. Tian et
al., 2011) Concern over registration accuracy is one of several reasons for the relative lack of
widespread adoption of CAN amongst spinal surgeons.(Choo et al., 2008; Hartl et al., 2013)
Displacement of vertebral levels distant to the DRF may generate navigation inaccuracy from
intersegmental mobility, which is seen to varying extents across the cervical, thoracic and lumbar
spines.(Tauchi et al., 2013) While intersegmental motion due to patient positioning, for instance
between supine pre-operative CT imaging and intra-operative prone positioning, is accounted for
by CAN systems registering to intra-operative imaging, there are multiple sources of intra-
operative post-imaging intersegmental motion. These include patient respiration-induced
vertebral motion, as well as displacement from surgeon manipulation during the placement of
instrumentation.(N. Glossop & Hu, 1997; Liu et al., 2015) In long-segment deformity corrections
and minimally-invasive lumbosacral procedures, or in some cases of posterior cervical
instrumentation, with DRF fixation to the pelvis or Mayfield clamp, respectively, navigation
inaccuracy due to intersegmental mobility can become particularly pronounced. However, the
current literature on the extent and significance of navigation inaccuracy due to intersegmental
mobility is conflicted.(N. Glossop & Hu, 1997; Liu et al., 2015; E C Papadopoulos, Girardi,
Sama, Sandhu, & Cammisa Jr., 2005; Scheufler et al., 2011a, 2011b; Takahashi, Hirabayashi,
Hashidate, Ogihara, & Kato, 2010; Uehara et al., 2017)

169
Here, we perform a prospective cadaveric and in-vivo human clinical study to quantify intra-
operative vertebral motion from patient respiration and surgical manipulation, using continuous
tracking enabled by a novel in-house navigation technology based on optical topographic
imaging (OTI), described in greater detail in Chapter 5.

170
8.3 Methods
8.3.1 Specimen/Patient Selection
Pre-clinical testing was performed in four formalin-fixed human cadavers. All cadavers
underwent pre- and post-operative helical CT imaging at 0.5mm slice thickness, for registration
using an OTI navigation system. Institutional ethics board approval was obtained (REB# 16-
0051-E).
In-vivo testing was performed in 10 clinical cases of open posterior instrumented fusion, for
degenerative, traumatic or neoplastic etiologies. All patients had no history of prior spinal
surgery at the operated levels. All patients underwent pre-operative helical CT imaging,
reformatted at 0.625mm slice thickness, for registration using an OTI navigation system as part
of an ongoing trial of OTI at Sunnybrook Health Sciences Centre (REB# 309-2014 and 086-
2015).
8.3.2 Quantification of Navigation Error from Proximity to DRF
Navigation error due to working at a level distant from that to which the DRF is affixed, was
assessed in four human cadavers. Cadavers were placed prone on a standard operating table, and
a standard midline posterior exposure performed from C1 to S1. Bone screws were implanted
into the superolateral edges of the laminae at each level as internal fiducials, to approximate the
entry point of typical pedicle screws. The DRF was clamped at various levels in the
cervical/thoracic/lumbar spine, and OTI navigation registered. The tip of a tracked awl was then
placed into the head of the bone screws at 0-5 levels away from that to which the DRF was
affixed. The three-dimensional location of the tool tip as seen by the OTI navigation system was
recorded at each point, and compared using image-processing software to the actual position of

171
the center of the bone screw head on post-operative CT imaging. All image processing and
measurements were performed using a 64-bit OsiriX workstation (version 10.9.5; PIXMEO
SARL. Geneva, Switzerland).
8.3.3 Quantification of Navigation Error from Surgical Manipulation
Using the same midline exposures and laminar fiducials in four human cadavers, the tip of a
tracked awl (thoracolumbar) or tracked drill guide (cervical) was placed into the heads of the
bone screws at each level, and pressure exerted with the appropriate force and trajectory to
simulate the creation of pedicle screw tracts. The 3D position of the tracked tool tip prior to and
following the exertion of force was recorded by the OTI navigation system.
8.3.4 Quantification of Navigation Error from Respiration-Induced Motion
Respiration-induced vertebral motion was quantified in-vivo in 10 human patients. Patients were
positioned prone on a Wilson frame, with Mayfield head clamp for cervical fusions. Following
standard midline open posterior exposure, OTI image-to-patient registration was performed. A
custom spinous-process clamp with passive-reflective infrared (IR) tracking spheres, fabricated
in-house, was clamped to the level adjacent to the level to which the DRF was affixed, to 2-5
levels distant from the DRF, or to a stationary anatomic target supported by pelvic bolsters or a
Mayfield head clamp on the operating table (Figure 8-1). The 3D position of the spinous-process
clamp was tracked at 20 Hz over ~12 respiratory cycles. Tracked levels were categorized into
cervical, upper thoracic (T1-T6), lower thoracic (T7-T12), and lumbar. Data were collected on
multiple parameters that may influence respiration-induced motion, including patient age,
gender, body-mass index (BMI), spinal level, respiratory rate (RR), heart rate (HR), mean
arterial pressure (MAP), tidal volume (TV), positive end-expiratory pressure (PEEP) and
ventilator mode.

172
Motion during each respiratory cycle was quantified as the ‘peak-to-peak’ displacement (i.e.
from end-expiration to end-inspiration) in each of the antero-posterior, cranio-caudal, and medio-
lateral axes (Figure.8-2)
Figure 8-1. Respiratory motion tracking with a custom spinous process clamp. In-vivo surgical field with DRF
for in-house OTI navigation system (arrowhead), and custom spinous-process infrared tracking clamp to quantify
vertebral motion (arrow).

173
Figure 8-2. Vertebral respiratory motion tracking. Representative tracking of the 3D displacement of a cervical
vertebra over ~14 respiratory cycles, spanning 72 seconds. ‘Peak-to-peak’ displacement is computed as the change
in displacement from end-expiration to end-inspiration within one respiratory cycle, indicated by the red arrow.

174
8.3.5 Statistical Analyses
Differences in absolute navigation errors between spinal levels were quantified with one-way
ANOVA, with Tukey’s Honest-Significant-Difference test for post-hoc comparisons.
Differences in error dispersion were computed using Levene’s test of homogeneity of variances.
Predictors of increased vertebral motion from distance from the DRF, surgical manipulation, or
respiratory motion were assessed using multiple linear regression models. Variables were entered
simultaneously into a full model, with nonlinearity checked using 3 cubic splines. Models were
assessed for collinearity as well as quality of fit. Hierarchical mixed-effects general linear
modelling was employed to adjust for second-order differences between cadavers/patients, where
required based on univariate analyses.
All statistical analyses were performed in SPSS Statistics (version 21; IBM. Chicago, IL, USA).

175
8.4 Results
In cadaveric testing, 132 laminar fiducials were implanted from C2-S1, 46 cervical, 47 thoracic,
and 39 lumbar. 583 respiratory cycles were tracked in 10 patients in-vivo, 136 in the cervical
spine, 167 upper thoracic, 74 lower thoracic, and 206 lumbar.
8.4.1 Navigation Error from Proximity to DRF
(Mean ± SD) quantitative navigation error at the level of the DRF was 1.1 ± 0.3 mm in the
antero-posterior (AP) axis, 1.3 ± 0.2 mm in the medio-lateral (ML) axis, and 1.6 ± 0.4 mm in the
cranio-caudal (CC) axis, for an overall 3D error of 2.7 ± 0.4 mm, representing the baseline
navigation error.
An increase in mean quantitative navigation error of ≥ 2 mm was seen in 3D in the cervical and
lumbar spine at ≥ 2 levels distant from the DRF, driven largely by an equivalent increase in error
in the AP axis at ≥ 2 levels distant from the DRF, and in the ML axis at ≥ 3 levels distant (Figure
8-3). An increase in error of ≥ 4 mm was seen in 3D at 5 levels from the DRF, driven by an
equivalent increase in AP error at ≥ 4 levels from the DRF. No significant increases in error in
the CC axis were seen up to 5 levels from the DRF (Figure 8-3).
The variability in navigation error increased significantly in the AP axis at ≥ 2 levels from the
DRF (SD 0.41 vs. 0.27 mm, p = 0.026), and in the ML axis at ≥ 1 level from the DRF (SD 0.53
vs. 0.18 mm, p < 0.001), by Levene’s test of homogeneity of variances. No significant increases
in error dispersion in the CC axis were observed.

176
8.4.2 Navigation Error from Surgical Manipulation
(Mean ± SD) displacement due to surgical manipulation was 1.6 ± 1.1 mm in 3D across all
levels, non-significantly greater in the lumbar spine (1.8 ± 1.5 mm) than in the thoracic (1.5 ± 1.0
mm) and cervical (1.3 ± 0.8 mm) spine. Displacement in the ML axis was significantly greater in
the thoracic spine relative to the cervical spine (1.0 ± 0.9 mm vs. 0.4 ± 0.3 mm; p<0.001), and in
the CC axis in the lumbar spine relative to both the cervical and thoracic spine (1.4 ± 1.1 mm vs.
0.9 ± 0.8 mm and 0.8 ± 0.7 mm, respectively; p<0.001).
Deviation of ≥ 2 mm was observed in 3D in 17.4% of cervical levels, 19.2% of thoracic levels,
and 38.5% of lumbar levels. 3D displacement of ≥ 3 mm was recorded in 6.5% of cervical levels,
10.7% of thoracic levels, and 10.3% of lumbar levels (Figure 8-4).

177
Figure 8-3. Translational navigation error from distance to DRF. Standard boxplots demonstrating the increase
in translational error from baseline, as a function of the number of levels distant from the DRF, in 3D (A) and each of
the medio-lateral (B), antero-posterior (C) and cranio-caudal (D) axes. Boxes represent the first, median and third
quartiles. Whiskers represent 1.5x the interquartile range. * represents significant difference from baseline error, at
p<0.05.

178
Figure 8-4. Translational navigation error with surgical manipulation. Histograms demonstrating the percentage
of screw tracts with ≥ 2 mm, ≥ 3 mm and ≥ 4 mm deviation with surgeon manipulation, in 3D and in each of the
medio-lateral (ML), antero-posterior (AP) and cranio-caudal (CC) axes. Manipulation-induced displacement is shown
in each of the cervical (A), thoracic (B) and lumbar (C) spines.

179
8.4.3 Navigation Error from Respiration-Induced Motion
Respiration-induced motion was quantified as absolute motion, or motion relative to a DRF
clamped 1-5 levels adjacent. In general linear modelling, accounting for spinal level, there were
no differences in relative vertebral motion in any axis between the DRF at any of 1-5 levels
distant, hence these are pooled for subsequent analysis as ‘relative motion’.
(Mean ± SD) absolute 3D vertebral motion across all levels was 2.0 ± 1.3 mm, significantly
greater in the lower thoracic spine than in the cervical, upper thoracic or lumbar spine (4.3 ± 0.4
mm vs. 2.6 ± 1.2 mm, 1.7 ± 0.5 mm, and 1.1 ± 0.4 mm, respectively; p<0.001). Absolute motion
was greatest in the AP axis vs. the ML and CC axes (2.4 ± 1.8 mm vs. 0.8 ± 0.6 mm and 0.9 ±
0.6 mm, respectively; p<0.001)(Figure 8-5). Absolute 3D motion was greater than 2 mm in
32.9% of cases and greater than 4 mm in 11.6%, significantly more frequently in the lower
thoracic spine (p<0.001)(Figure 8-6). (Mean ± SD) relative respiration-induced 3D displacement
across all levels was 0.5 ± 0.1 mm, significantly greater in the lumbar spine and in the AP and
CC axes (Figure 8-5).
In general linear modelling, TV (r = 0.263, p=0.032), PEEP (r = 0.756, p<0.001) and MAP (r =
0.150, p<0.001) were positively correlated with absolute 3D and AP respiration-induced motion
(r – Pearson correlation coefficient). Age, gender, and BMI did not significantly correlate with
any respiration-induced displacement.

180
Figure 8-5. Respiration-induced vertebral motion. Standard boxplots demonstrating absolute (top) and relative
(bottom) respiration-induced vertebral motion, in 3D and in each of the ML, AP and CC axes, stratified by spinal
region. Boxes represent the first, median and third quartiles. Whiskers represent 1.5x the interquartile range. *
represents significant difference, at p<0.05.

181
Figure 8-6. Respiratory cycles with clinically significant vertebral motion. Histograms demonstrating the
percentage of respiratory cycles with ≥ 2 mm and ≥ 4 mm of displacement, in 3D and in each of the ML, AP and CC
axes, in the cervical (A), upper thoracic (B), lower thoracic (C), and lumbar (D) spine.

182
8.5 Discussion
While modern 3D-CAN has demonstrably increased instrumentation accuracy across all spinal
levels, widespread enthusiasm for the technology has been tempered by high costs as well as
workflow disruption.(Barsa et al., 2016; Austin C Bourgeois et al., 2015; Hartl et al., 2013;
Hecht et al., 2010; Mason et al., 2014; W. Tian et al., 2013; Wagner et al., 2017) Initial 3D CAN
systems employing registration of patient anatomy to pre-operative imaging, using either point-
or surface-matching techniques, were highly cumbersome to register. Advances in intra-
operative imaging, either 3D fluoroscopy or cone- or fan-beam CT, have allowed for faster
automatic patient registration to intra-operatively-acquired imaging.(F Costa et al., 2014) Intra-
operative imaging devices have concurrently eliminated one source of navigation error due to
intersegmental mobility, from positional changes from a supine pre-operative scan to a prone
operating position. However, all contemporary 3D-CAN systems, whether registering to pre- or
intra-operative imaging, retain dependence on a DRF to maintain patient-to-image registration
and allow tool tracking. Navigation errors may therefore arise by virtue of distance from the
DRF, a limitation largely of the infra-red optical tracking technology used by most current CAN
devices, as well as due to intersegmental mobility, from surgical manipulation and patient
respiration-induced motion at levels distant to the DRF. Using an OTI navigation system
developed in-house, allowing granular control and root-level system access, we quantify and
identify predictors of these errors for the first time in the literature.
The impact of working distance from a DRF on navigation error has been studied
heterogeneously in the limited literature to date. In the cervical spine, using point-matching
registration to pre-operative CT, Tauchi et al. demonstrated a 17% increase in cervical pedicle
screw perforation rate when working one level distant from the DRF, with greater distance
correlated with larger error.(Tauchi et al., 2013) The literature in the thoracolumbar spine is
more controversial. Using point-matching registration to pre-operative CT in the setting of
adolescent scoliosis, Uehara et al. demonstrated significantly increased pedicle screw perforation
rates at 3 or more levels distant to the DRF, while Takahashi et al. showed pedicle violation rates
of 1.5% at up to 3 levels distant from the DRF, though without comparison to segmental

183
registration.(Takahashi et al., 2010; Uehara et al., 2017) Papadopoulos et al. demonstrated no
significant increases in computer-reported registration error, known to correlate poorly with true
application error, at up to 4 levels from the DRF.(Guha, Jakubovic, Gupta, Alotaibi, et al., 2017;
E C Papadopoulos et al., 2005) Scheufler et al. claimed safe instrumentation up to 12 levels from
the DRF with registration to an intra-operative fan-beam CT, based on radiographic pedicle
screw grading, though requiring 3 intra-operative CT spins and with an additional 2.5% rate of
K-wire revision.(Scheufler et al., 2011b) Here, we show quantitatively that an increase in
navigation error of ≥ 2mm, corresponding to the difference between an ‘acceptable’ and an
‘unacceptable’ pedicle screw in common radiographic grading classifications, occurs at 2 or
more levels distant from the DRF in the medio-lateral and antero-posterior axes.(Gertzbein &
Robbins, 1990; Neo, Sakamoto, & Fujibayashi, 2005) While antero-posterior accuracy, i.e. screw
depth, may be less important due to typically greater tolerances, inaccuracy in the medio-lateral
axis may lead to neural or vascular injury. Our study, performed in a cadaveric setting, also
eliminates respiration-related motion as a confounder for error due to distance from the DRF.
Intersegmental mobility may also lead to error during surgical manipulation at levels distant
from the DRF. This has been studied only once in the literature to our knowledge, with Glossop
et al. demonstrating up to 12mm of 3D movement in the lumbar spine with paraspinal muscle
dissection and pedicle targeting in an in-vivo setting.(N. Glossop & Hu, 1997) We show absolute
3D movement of only 1.55mm across all levels, due in part to the rigid formalin-fixed cadaveric
setting, as well as because only pedicle targeting was assessed, whereas typically more force may
be applied for paraspinal tissue dissection. However, the key point is that while absolute
manipulation-related motion is typically small in our study, variability in motion is high
particularly in the lumbar spine, and may be expected to be even greater in an in-vivo setting
with more pliable tissues, as well as a range of degenerative pathologies with greater
intersegmental mobility.
Vertebral motion from patient respiration may result in navigation inaccuracy distant to a DRF,
due to intersegmental mobility. In the limited literature to date, respiratory motion has been
reported up to 1.6mm in the lumbar spine, with no direct quantification of vertebral motion at

184
other levels.(N. Glossop & Hu, 1997; Liu et al., 2015) In our study, we demonstrate via direct
measurement that while respiration-induced vertebral motion averages only 0.48 mm at 1-5
levels from a DRF, absolute motion with respect to a DRF affixed to a remote fixed anatomical
site may be as large as 10 mm in the AP axis and 6 mm in the ML axis. The attenuation of
respiration-induced error with an adjacent DRF, even though we demonstrate increased error in
optical tracking at 2 or more levels distant from the DRF, is likely due to temporal averaging of
errors which does not occur at a single time point. Caution should therefore be exercised when
performing navigated procedures with a DRF affixed to the pelvis or Mayfield head clamp, as is
commonly done in long-segment lumbosacral or cervical procedures, respectively. Furthermore,
greater respiration-induced displacement is correlated with larger TV and PEEP; apnea or
modification of ventilator parameters may therefore be warranted at critical stages of a navigated
procedure where accuracy is paramount.
There are multiple limitations to our analysis. Pre-clinical testing was conducted in formalin-
fixed cadavers, with far more rigid tissues and therefore underestimated vertebral motion than
might be expected in clinical application. Respiration-induced motion was assessed up to 5 levels
distant to a DRF, due to the limited exposure in most procedures in this series. Further work is
therefore required to assess the impact of working at greater distances from a DRF on mitigation
of respiration-induced vertebral motion.

185
8.6 Conclusions
Vertebral motion is unaccounted for during image-guided surgery when performed at levels
distant from the DRF. Navigating instrumentation within 2 levels of the DRF is likely to
minimize the risk of navigation error. While respiration- and manipulation-induced vertebral
motion is typically small, there may be significant variability in magnitude, particularly with
spinal region and ventilator parameters. Surgeons may mitigate these errors intra-operatively by
placing the DRF adjacent to the registered level, rather than on a Mayfield head clamp or pelvis,
to minimize respiration-induced error. If performing work distant to a DRF, temporary apnea or
adjustment of ventilator parameters may be warranted at critical stages of the procedure, to
minimize respiration-induced error. Surgeons should also take care to cease manipulation of
bony elements when actively using navigation guidance. Future generations of image-guidance
systems should compensate for these errors in real-time to minimize navigation inaccuracy.

186
Chapter 9 Geometric Congruence in Surface Registration for Spinal Intra-
Operative Three-Dimensional Navigation
Preamble
This chapter is modified from the following:
Guha D, Jakubovic R, Leung MK, Ginsberg HJ, Fehlings MG, Mainprize TG, Yee A, Yang
VXD. Quantification of computational geometric congruence in surface-based registration for
spinal intra-operative three-dimensional navigation. Manuscript in submission.

187
9.1 Abstract
Computer-assisted navigation (CAN) may guide spinal instrumentation, and requires alignment
of patient anatomy to imaging. Iterative closest-point (ICP) algorithms register anatomical and
imaging surface datasets, which may fail in the presence of significant geometric symmetry
(congruence), leading to failed registration or inaccurate navigation. In this study, we therefore
strove to computationally quantify geometric congruence in posterior spinal exposures, and
identify predictors of potential navigation inaccuracy. Midline posterior exposures were
performed from C1-S1 in four human cadavers. CAN based on optical topographic imaging
(OTI) generated surface maps of the posterior elements at each level. Maps were reconstructed to
include bilateral hemilamina, or unilateral hemilamina with/without the base of the spinous
process. Maps were fitted to symmetrical geometries (cylindrical/spherical/planar) using
computational modelling, and the degree of model fit quantified based on the ratio of model
inliers to total points. Geometric congruence in a clinical setting was assessed similarly, in 11
patients undergoing midline exposures in the cervicsal/thoracic/lumbar spine for posterior
instrumented fusion. In cadaveric testing, increased cylindrical/spherical/planar symmetry was
seen in the subaxial cervical spine relative to the high-cervical and thoracolumbar spine
(p<0.001). Extension of unilateral exposures to include the ipsilateral base of the spinous
process, or to a central bilateral exposure, decreased symmetry independent of spinal level
(p<0.001). In clinical testing, increased cylindrical/spherical/planar symmetry was again seen in
the subaxial cervical spine relative to the thoracolumbar spine (p<0.001), and in the thoracic
spine relative to the lumbar spine (p<0.001). Symmetry in all geometric configurations in
unilateral exposures was decreased by 20% with inclusion of the ipsilateral base of the spinous
process. We concluded that geometric congruence is most evident at C1 and the subaxial cervical
spine, warranting greater vigilance in navigation accuracy verification. At all levels, inclusion of
the base of the spinous process in unilateral registration decreases the likelihood of geometric
symmetry and navigation error. This work is important to allow the extension of line-of-sight
based registration techniques, including OTI, to minimally-invasive unilateral approaches.

188
9.2 Introduction
Spinal instrumentation traditionally has been placed freehand based on anatomic landmarks,
which may be highly variable, or with fluoroscopic guidance resulting in significant radiation
exposure to operating room personnel.(Nelson et al., 2014; Robertson, Novotny, Grobler, &
Agbai, 1998; Villard et al., 2014) Computer-assisted navigation (CAN) may guide spinal
instrumentation placement, significantly improving accuracy and minimizing acute and long-
term malposition related complications.(Fichtner et al., 2017; Luther, Iorgulescu, Geannette,
Gebhard, Saleh, Tsiouris, & Härtl, 2015; Xiao et al., 2017) Image guidance in CAN may be
based on pre-operative imaging, typically CT, or intra-operatively-acquired 3D fluoroscopy or
CT; in all cases, navigation requires registration of the image and patient spaces. Our laboratory
has developed a novel technique for image-to-patient registration, based on optical topographic
imaging (OTI), which rapidly acquires a surface map of exposed spinal anatomy under direct
vision and automatically registers to pre-operative CT in real-time, minimizing workflow
disturbance (Chapter 5). Registration of three-dimensional point sets in contemporary surface-
based navigation techniques, including OTI, is typically performed using variants of the iterative
closest-point (ICP) algorithm, in which two meshes are aligned using an initial rigid-body pose
estimation, followed by iterative refinement of the translational and rotational transformations to
minimize a distance error metric between the two meshes.(Besi & Mckay, 1992; Y. Chen &
Medioni, 1991) ICP algorithms may be prone to instability when too many point pairs arise from
unconstrained symmetrical, or congruent, geometries, including cylinders, spheres, and
planes.(Armesto et al., 2010; Gelfand et al., 2003; Pottmann & Hofer, 2003) While multiple
variations of ICP have attempted to address the stability of the final alignment between meshes,
non-convergence from geometric congruence remains a potential source of registration error in
image-guided surgery, leading to failed registration or, worse, successful registration with
inaccurate navigation. ICP convergence is particularly critical in surface-based registration
techniques, such as OTI, especially when applied to minimally-invasive (MIS) exposures with
fewer available points to increase the variance in input geometry and specify the initial alignment
pose. Here, we therefore quantify geometric congruence, or symmetry, in posterior spinal
exposures using computational modelling, and identify predictors of potential navigation
inaccuracy from this error mechanism. This understanding is essential to allow the safe and

189
efficient translation of any surface-based navigation technique requiring line-of-sight to exposed
anatomy, to minimally-invasive spinal exposures.

190
9.3 Methods
9.3.1 Specimen/Patient Selection
Surface geometry of posterior spinal exposures was assessed initially in four human cadavers, as
part of pre-clinical validation of our OTI navigation system. All cadavers underwent pre-
operative helical CT imaging at 0.5mm slice thickness. Institutional ethics board approval was
obtained (REB# 16-0051-E).
Surface geometry of posterior spinal anatomy was subsequently assessed in-vivo in 11 patients,
undergoing midline exposures in the cervical/thoracic/lumbar spine for OTI-guided posterior
instrumented fusion as part of an ongoing trial of OTI navigation at Sunnybrook Health Sciences
Centre (REB# 309-2014 and 086-2015). All patients underwent pre-operative helical CT
imaging, reformatted at 0.625mm slice thickness.
9.3.2 OTI Registration
Cadavers were positioned prone on a standard operating table. Midline posterior exposures were
performed bilaterally from C1-S1 in four human cadavers, extending to the lateral edge of the
lateral masses in the cervical spine, and to the transverse processes in the thoracolumbar spine.
3D surface maps of the posterior elements were generated using OTI at each level (Figure 9-1).
Technical details of OTI registration are described separately, in Chapter 5.(Jakubovic et al.,
2016) Briefly, structured light is projected onto the exposed anatomy and its deformation
recorded by stereoscopic cameras to generate a 3D surface point cloud, followed by automatic
registration via an iterative closest-point (ICP) algorithm to the pre-operative CT.

191
In clinical testing, all patients were positioned prone on a Wilson frame. Patients undergoing
cervical instrumentation were also placed in a Mayfield head clamp. Standard midline posterior
exposures sufficient for open instrumentation placement were performed, with OTI surface
acquisition and registration similar to cadaveric testing.
Figure 9-1. Cadaveric midline exposures for OTI. (A) Representative standard midline posterior spinal exposure in
cadaveric testing. (B) OTI 3D surface map of a midline posterior cervical spine exposure.

192
9.3.3 Computational Modelling of Geometric Congruence
3D surface maps generated from each vertebral level were thresholded to isolate the vertebra.
The point clouds comprising each surface map were subsequently reconstructed to capture the
bilateral hemilaminae including spinous process (Group A), each unilateral hemilamina
including the ipsilateral base of the spinous process (Group B), and each unilateral hemilamina
excluding the spinous process (Group C)(Figure 9-2). All thresholding and reconstruction was
performed in an open-source data visualization package (ParaView 5.2.0. Kitware, Inc.; Clifton
Park, NY, USA).
Reconstructed point clouds from each group at each registered level were subsequently fitted to
symmetrical geometries (cylindrical, spherical, planar) in a computing package (MATLAB
R2016b. The MathWorks, Inc.; Natick, MA, USA) using a random sample consensus
(RANSAC) algorithm, iterated 100 times (Figure 9-3).
The degree of fit of each point cloud to a geometrically-symmetric shape was quantified using
two metrics, the mean-adjusted coefficient of variation in the root-mean-square error (CoV-
RMSE) of the point cloud to the fitted shape, as well as the proportion of total points fitted to the
symmetric shape (inliers-to-points ratio, ITPR). Increased fit to a symmetric geometry, and
therefore increased likelihood of navigation error, is denoted by decreased CoV-RMSE and
increased ITPR. As the CoV-RMSE is highly dependent on the user-specified maximum inlier
error for the RANSAC algorithm, sensitivity analyses were performed for each geometry with
the maximum inlier error set to 0.1mm, 0.5mm, 1.0mm and 2.0mm, and the maximum inlier
error resulting in the lowest CoV-RMSE chosen for subsequent ITPR analyses; a maximum
inlier error of 0.5mm was selected for all analyses in this study.

193
Figure 9-2. Reconstruction of OTI surface map point clouds. Reconstructed surface map point clouds, capturing
the bilateral hemilaminae including spinous process (Group A) viewed from above (top) and axially (bottom),
unilateral hemilamina including base of the spinous process (Group B), and unilateral hemilamina excluding the
spinous process (Group C).
Figure 9-3. Fitting of symmetrical geometries to OTI point clouds. (A) Point cloud of an L2 unilateral hemilamina
including base of spinous process (Group B). Fitting of a cylinder (B), sphere (C), and plane (D) to the L2 point cloud.
Red dots represent points included in the fitted model (inliers); green dots represent points excluded from the fitted
model (outliers).

194
9.3.4 Statistical Analysis
Predictors of increased fit to symmetric geometries were explored using univariate and multiple
linear regression modelling. For univariate analyses, RMSE and ITPR were compared between
spinal levels and between point cloud reconstruction groups using one-way analysis of variance
(ANOVA), with Tukey’s Honest-Significant-Difference test for post-hoc comparisons.
Differences in CoV-RMSE were compared using Levene’s test of homogeneity of variances.
Hierarchical mixed-effects general linear modelling was employed for multivariate analyses to
adjust for second-order differences between cadavers/patients. Significance levels for all tests
were set at α < 0.05.
All statistical analyses were performed in SPSS Statistics (version 21; IBM. Chicago, IL, USA).

195
9.4 Results
For the four cadavers used in pre-clinical testing, mean age at death was 91.4 years (range 83-
96). In-vivo clinical testing was performed in eleven patients, with mean age 58.3 years (range
42-71).
9.4.1 Geometric Congruence by Spinal Region
In cadaveric testing, for unilateral registrations (Group C), C1 was found to have greater
cylindrical and planar symmetry than C2, the subaxial cervical spine, as well as the thoracic,
lumbar and sacral spines, based on ITPR (p<0.001)(Figure 9-4). C2 demonstrated increased
symmetry in all configurations relative to the thoracolumbar and sacral spines, while the subaxial
cervical spine showed greater planar symmetry than the thoracolumbar and sacral spines
(p<0.001). ITPR stratified by individual spinal levels are shown in Table 9-1.
In unilateral in-vivo registrations (Group C), the subaxial cervical spine again demonstrated
greater symmetry, in all configurations, relative to the thoracic and lumbar spine
(p<0.001)(Figure 9-4). Uniquely, the posterior elements of thoracic vertebrae also showed
greater symmetry in all configurations relative to the lumbar spine (p<0.001).

196
Figure 9-4. Geometric congruence by spine region. (Top) Standard boxplot of the ITPR stratified by spine region
(C1, C2, subaxial cervical, T - thoracic, L – lumbar, S – sacrum), for each of cylindrical, spherical and planar
geometries, in cadaveric testing. (Bottom) Standard boxplot of the ITPR stratified by spine region, in clinical testing.
Error bars represent 1.5xIQR. * denotes significance at p<0.05.

197
Table 9-1. Geometric congruence for unilateral registrations by spinal level. Inliers-to-points ratio (ITPR) for
unilateral registrations (Group C) for each symmetrical configuration, stratified by spinal level, in cadaveric testing. All
values reported as (mean±SD).
Level Cylinder Sphere Plane
C1 0.541 ± 0.092 0.555 ± 0.091 0.529 ± 0.072
C2 0.499 ± 0.081 0.541 ± 0.066 0.510 ± 0.064
C3 0.414 ± 0.100 0.494 ± 0.125 0.433 ± 0.100
C4 0.527 ± 0.125 0.645 ± 0.165 0.553 ± 0.150
C5 0.618 ± 0.150 0.727 ± 0.155 0.669 ± 0.186
C6 0.513 ± 0.088 0.591 ± 0.067 0.535 ± 0.060
C7 0.507 ± 0.108 0.560 ± 0.076 0.522 ± 0.091
T1 0.491 ± 0.089 0.582 ± 0.079 0.530 ± 0.066
T2 0.524 ± 0.104 0.603 ± 0.122 0.561 ± 0.123
T3 0.468 ± 0.088 0.514 ± 0.090 0.468 ± 0.108
T4 0.474 ± 0.110 0.529 ± 0.107 0.495 ± 0.116
T5 0.472 ± 0.096 0.546 ± 0.093 0.521 ± 0.084
T6 0.448 ± 0.088 0.521 ± 0.090 0.503 ± 0.099
T7 0.442 ± 0.101 0.507 ± 0.102 0.486 ± 0.095
T8 0.438 ± 0.091 0.513 ± 0.111 0.478 ± 0.106
T9 0.409 ± 0.100 0.473 ± 0.140 0.444 ± 0.132
T10 0.432 ± 0.083 0.454 ± 0.105 0.429 ± 0.102
T11 0.472 ± 0.097 0.539 ± 0.097 0.485 ± 0.089
T12 0.458 ± 0.086 0.517 ± 0.094 0.479 ± 0.109
L1 0.434 ± 0.093 0.510 ± 0.097 0.462 ± 0.106
L2 0.417 ± 0.091 0.483 ± 0.084 0.455 ± 0.084
L3 0.452 ± 0.073 0.486 ± 0.035 0.466 ± 0.042
L4 0.492 ± 0.099 0.518 ± 0.073 0.479 ± 0.052
L5 0.510 ± 0.098 0.599 ± 0.130 0.521 ± 0.077
S1 0.449 ± 0.091 0.537 ± 0.144 0.503 ± 0.095

198
9.4.2 Geometric Congruence by Laterality
In cadaveric testing, extension of the registered anatomy from a unilateral exposure (Groups
B+C) to a bilateral acquisition (Group A) resulted in significant reduction in symmetry in all
geometric configurations (Figures 9-5, 9-6). ITPR for cylindrical configurations, i.e. cylindrical
symmetry, was decreased by 47.9% (0.436 ± 0.107 vs. 0.227 ± 0.055, p<0.001)(mean ± SD),
spherical symmetry by 42.0% (0.493 ± 0.121 vs. 0.286 ± 0.082, p<0.001), and planar symmetry
by 48.6% (0.438 ± 0.119 vs. 0.225 ± 0.063, p<0.001), for unilateral vs. bilateral registrations
(Groups B+C vs. Group A).
In clinical testing, absolute ITPRs were decreased for all geometric configurations relative to
cadaveric data (p<0.001), but with similar reductions in symmetry by extending unilateral
acquisitions (Groups B+C) to a bilateral registration (Group A)(Figure 9-5). Cylindrical
symmetry was reduced by 50.0% (0.366 ± 0.111 vs. 0.183 ± 0.037, p<0.001), spherical
symmetry by 47.7% (0.451 ± 0.136 vs. 0.236 ± 0.069, p<0.001), and planar symmetry by 50.8%
(0.390 ± 0.144 vs. 0.192 ± 0.048, p<0.001), in Group A vs. Groups B+C.

199
Figure 9-5. Geometric congruence by registration laterality. (Top) Standard boxplot of the ITPR stratified by
unilateral vs. bilateral registrations, for each of cylindrical, spherical and planar geometries, in cadaveric testing.
(Bottom) Standard boxplot of the ITPR stratified by unilateral vs. bilateral registrations, in clinical testing. Error bars
represent 1.5xIQR. * denotes significance at p<0.05.

200
Figure 9-6. Reduction in geometric congruence with bilateral registration. (Top row) Fitting of a cylinder (A),
sphere (B), and plane (C) to a unilateral L2 registration (D). Inliers are denoted by red dots, outliers by green dots.
(Bottom row) Significant reduction in symmetry, i.e. ratio of inliers (red dots) to outliers (green dots), by extension to a
bilateral L2 registration (H), in each of cylindrical (E), spherical (F), and planar (G) geometries.

201
9.4.3 Geometric Congruence by Inclusion of the Spinous Process
In cadaveric testing, extension of the registered anatomy from a unilateral exposure (Group C) to
include the ipsilateral base of the spinous process (Group B) reduced symmetry significantly in
all configurations (Figures 9-7, 9-8). Cylindrical symmetry was reduced by 16.5% (0.472 ±
0.107 vs. 0.394 ± 0.089, p<0.001)(mean ± SD), spherical symmetry by 18.4% (0.539 ± 0.119 vs.
0.440 ± 0.099, p<0.001), and planar symmetry by 26.1% (0.498 ± 0.111 vs. 0.368 ± 0.087,
p<0.001), for unilateral registrations including the ipsilateral spinous process base vs. without
(Group B vs. Group C).
For in-vivo registrations, absolute ITPRs were decreased for all configurations relative to
cadaveric testing (p<0.001). Inclusion of the ipsilateral spinous process base in the registration
reduced cylindrical symmetry by 24.6% (0.418 ± 0.116 vs. 0.315 ± 0.078, p<0.001), spherical
symmetry by 28.8% (0.527 ± 0.136 vs. 0.375 ± 0.082, p<0.001), and planar symmetry by 40.2%
(0.488 ± 0.138 vs. 0.292 ± 0.054, p<0.001), relative to registrations excluding the spinous
process (Group B vs. Group C).

202
Figure 9-7. Geometric congruence by spinous process inclusion. (A) Standard boxplot of the ITPR stratified by
inclusion of the spinous process (SP) base, for unilateral registrations, in cadaveric testing. (B) Standard boxplot of
the ITPR stratified by inclusion of the spinous process base, in clinical testing. Error bars represent 1.5xIQR. *
denotes significance at p<0.05.

203
Figure 9-8. Reduction in geometric congruence with inclusion of ipsilateral spinous process base. (Top row)
Fitting of a cylinder (A), sphere (B), and plane (C) to a unilateral L2 registration excluding the base of the ipsilateral
spinous process (D). Inliers are denoted by red dots, outliers by green dots. (Bottom row) Significant reduction in
symmetry, i.e. ratio of inliers (red dots) to outliers (green dots), by extension of the unilateral registration to include
the base of the ipsilateral spinous process (H), in each of cylindrical (E), spherical (F), and planar (G) geometries.

204
9.5 Discussion
While CAN has been shown to improve instrumentation accuracy across all spinal levels,
widespread adoption has been limited by high capital costs and workflow disruptions.(Barsa et
al., 2016; Austin C Bourgeois et al., 2015; Hartl et al., 2013; Hecht et al., 2010; Mason et al.,
2014; N. F. Tian et al., 2011; Wagner et al., 2017) OTI for spinal navigation significantly
streamlines registration workflow by employing rapid optical 3D scanning to generate a high-
density surface point cloud.(Jakubovic et al., 2016) However, OTI requires direct vision of bony
anatomy for registration, limiting its applicability to some current paradigms of minimally-
invasive approaches. Extension of OTI, and other efficient surface-based registration techniques,
to minimally-invasive approaches requires an understanding of mechanisms of registration
failure. OTI, along with every current navigation technique applying surface-based registration
to pre-operative imaging, employs an ICP algorithm to register point sets. Some pitfalls of ICP
algorithms are known, including failed registration due to poor initial pose estimation from large
rigid-body fiducial localization errors or soft tissue deformation, susceptibility to mismatched
outliers, and inability to account for differences in scale between point sets, resulting in hundreds
of variants of the original ICP algorithm published in the past 20 years.(Clements et al., 2008;
Maurer et al., 1996; Pomerleau et al., 2013; Xin & Pu, 2010; Ying et al., 2009) A lack of
convergence, i.e. failed or inaccurate registration, of ICP algorithms in the presence of geometric
congruence has been demonstrated in the context of 3D scanned shapes, with multiple variants
attempting to minimize the associated rotational error, albeit with a target translational error of
<25mm as a definition of ‘successful registration’, far too large for surgical navigation.(Armesto
et al., 2010) Other variants have attempted to use a similar RANSAC-algorithm based approach
as used in our study, to detect geometric symmetry in the point sets to be aligned, however
requiring a computational time of 10 minutes, again unacceptable for real-time surgical
navigation.(Berner et al., 2008) To date, geometric homogeneity has not been demonstrated in
the context of surgical navigation; in spinal surgery, geometric congruence is likely to arise in
unilateral or minimal-exposure registrations. While CAN techniques employing intra-operative
3D imaging do eliminate this potential error, it comes with significant capital expense, operating
time, and workflow hindrance. To allow the workflow improvements of surface-scanning

205
techniques such as OTI to be fully realized, with their significantly greater point density, it is
paramount to characterize their potential limitations and failure mechanisms.
Here, we show first that geometric instability, or congruence, is greatest at C1 and in the subaxial
cervical spine, in both cadaveric and in-vivo settings. This is certainly intuitive given the
relatively smooth and symmetric nature of the C1 posterior arch, disrupted minimally by the
posterior tubercle. In the subaxial cervical spine, facets are relatively flat and smooth relative to
those in the thoracolumbar spine, again resulting in significant geometric congruence that may
lead to potential navigation error when registered through minimal exposures. In the literature on
navigated pedicle screw placement, breach rates are consistently greater in the cervical spine
than in the thoracolumbar spine, although the relatively smaller diameter of cervical pedicles
may certainly contribute to this.(Mason et al., 2014) In our own clinical validation of OTI
navigation, quantitative navigation accuracy has been comparable in the cervical vs.
thoracolumbar spine, albeit with statistically insignificantly-greater translational and angular
errors in the cervical spine.(Guha, Jakubovic, Gupta, Fehlings, et al., 2017; Jakubovic et al.,
2016)
For unilateral registrations using surface-based navigation techniques, geometric instability can
be improved significantly by extending the registration to a bilateral exposure, intuitive as three-
dimensionally-unique geometry in the form of the spinous process and contralateral hemilamina
is now included in the surface dataset to be registered by ICP. More practically, however, we
show that geometric instability may also be improved in a unilateral registration by simply
including the adjacent base of the ipsilateral spinous process in the registered anatomy. While the
absolute values of ITPR were greater in our cadaveric vs. clinical testing, due likely to larger and
more rounded osteophytes in the significantly older cadaveric population, improvement in
symmetry by including the ipsilateral spinous process base was seen in both cadaveric and
clinical settings, in fact more so in the in-vivo population. Clinically, this has relevance in
performing for instance minimally-invasive TLIFs with surface-based navigation guidance,
whereby a unilateral exposure is required for the interbody work, and slight medialization of the
exposure to include the ipsilateral spinous process base can significantly improve the likelihood

206
of successful navigation registration and implant accuracy. It is important to note, however, that
geometric symmetry is minimized but not eliminated with these maneuvers, hence manual
verification of navigation accuracy by the surgeon remains paramount to the safe and efficient
performance of navigated spinal procedures. We propose a systematic technique of manual
registration verification to account for all dimensions in which geometric congruence may lead
to navigation error (Figure 9-9).
Our findings may be extended to surface imaging and navigation for cranial and non-
neurosurgical procedures. In cranial navigation, while initial surface-based registrations prior to
patient draping are likely to be accurate due to the unique geometry offered by variant facial
features, intra-operative updating of registrations on the external skull requires caution
particularly over the convexity, where significant cylindrical and spherical symmetry may be
expected.
While our study was conducted using an OTI navigation system, our findings may be
generalized to those of any surface-based navigation techniques. Our study is limited by its
simulation of unilateral exposures, as our surface scanning was performed on fully-open bilateral
exposures, and reconstructed to simulate unilateral registration post-hoc. Future studies of in-
vivo MIS surgery using tubular retractors are warranted, to assess registration quality in true
unilateral exposures.

207
Figure 9-9. Protocol for manual registration verification. (A) Representative point cloud of an open bilateral
posterior lumbar exposure. Manual accuracy verification should be performed with a tracked sharp-tip tool statically at
the superior and inferior facet joints (*), and dynamically by sliding axially (1) and sagittally (2) along the hemilaminae
as well as along the spinous process tip (3). Verification steps shown on orthogonal sagittal (B) and axial (C) CT
reconstructions as seen on typical navigation displays, with static verification points (*) and dynamic sliding
maneuvers (1, 2, 3).

208
9.6 Conclusions
Geometric congruence may lead to failed or inaccurate registration with surface-based surgical
navigation techniques. Congruence is most evident at C1 and the subaxial cervical spine,
warranting greater vigilance in navigation accuracy verification in these regions. At all spinal
levels, medial extension of a unilateral exposure to include the base of the ipsilateral spinous
process, or to a central bilateral exposure, decreases the likelihood of geometric symmetry and
therefore improves the likelihood of successful and accurate navigation in minimally-invasive
approaches.

209
Chapter 10 Concluding Summary, General Discussion, and Future Directions
Preamble
Chapter 10.3 (Future Directions) is modified from the following:
Guha D, Yang VXD. Perspective review on applications of optics in spinal surgery. Journal of
Biomedical Optics 2018, in press.

210
10.1 Concluding Summary
Neurosurgery as a surgical discipline has, by necessity, long been at the forefront of image-
guided technologies. Computer-assisted intra-operative navigation (CAN) represented a
significant leap forward in spatial planning, and has become standard of care in cranial
neurosurgery. Applications of CAN have been transitioned from cranial neurosurgery to spinal
approaches since the mid-1990s. While techniques used for tracking instruments in a surgical
field have evolved significantly, from early acoustic devices to subsequent electromagnetic and
now passive/active optoelectronic tracking, registration techniques have evolved less
substantially. Nonetheless, the accuracy of spinal CAN techniques has collectively improved to
the point that a substantial body of literature exists supporting improved radiographic outcomes
relative to pre-CAN methodologies. However, adoption of spinal CAN remains limited, with
well-defined barriers: questionable accuracy and clinical benefit, significant workflow
disruption, steep learning curves, and high capital costs. In this thesis our objectives were to
identify settings and populations in which spinal CAN is most usefully applied, and examine
how a novel registration technique, optical topographic imaging (OTI), could obviate many of
the concerns plaguing current CAN techniques. To this end, we characterized practice patterns in
spinal CAN usage in a representative Canadian cohort, and additionally investigated the utility of
CAN intra-operatively as a training adjunct. This set the stage for subsequent work assessing the
feasibility of OTI for spinal image guidance in a number of common-use clinical settings.
Finally, as an exercise in translating not just OTI but other navigation techniques to clinical
fruition, we first explored and quantified error modalities afflicting all current navigation
techniques, and subsequently those pertinent to surface mapping techniques alone, and outlined
steps to be taken both by surgeons intra-operatively, and engineers in the
development/refinement phases, to identify and mitigate these errors.
While barriers to the adoption of CAN have been explored in a small number of surveys of
selected spinal surgeons, real-world practice patterns in spinal CAN usage have not been
investigated thoroughly. The gains in radiographic accuracy with CAN techniques are not often
sufficient to overcome poor workflow and high capital cost in many settings, however there may

211
be specific applications and demographics for which the yields of CAN guidance may be
maximized. In a retrospective review of a prospectively-maintained database of patients
undergoing spinal instrumentation or percutaneous vertebroplasty/kyphoplasty, we found that
spinal CAN guidance was applied for less than one fifth of instrumented spinal fusions,
significantly more frequently by neurosurgeons than orthopedic spinal surgeons, and more often
in academic than community institutions. The use of CAN was associated with a reduction in the
need for revision surgery, though this conclusion is limited by the constraints of reviewing an
administrative database. Assessing the impact of spinal CAN on trainee education may provide
an additional application to justify the work needed to overcome typical barriers to adoption. In a
nationwide survey of spinal trainees, we found that almost two-thirds of orthopedic surgical and
neurosurgical trainees are not fully comfortable with the setup and use of spinal CAN, however
self-reported proficiency in instrumentation improves when CAN is applied, more so for
orthopedic surgical trainees. From a public health and resource allocation perspective, therefore,
these conclusions suggest that maximal clinical benefit of spinal CAN for patients may be
achieved if barriers to adoption are overcome among the primary practitioners performing the
bulk of instrumentation, orthopedic surgeons in the community. This requires significant
education at the trainee level, with additional emphasis on CAN operation for orthopedic and
neurosurgical spine fellows perhaps a worthwhile investment to improve adoption and ultimately
clinical outcomes.
Once we identified that, at least in the context of a single-payer health care system such as in
Canada, opportunities exist to maximize the utility of spinal CAN if specific barriers can be
overcome, we turned our attention to the translation of OTI for spinal CAN. As one of the
primary barriers to adoption is the unclear radiographic and clinical benefit relative to expert
freehand placement, we first explored how current CAN techniques are evaluated in the
literature, to allow optimal comparison with a novel technique, OTI, as well as guide future
studies of subsequent new technologies. We found that while most studies of spinal CAN assess
instrumentation accuracy as their primary outcome, less than half report radiographic accuracy,
with heterogeneous classification schemes used by those that do. Somewhat surprisingly, we
found that radiographic accuracy does not correlate with absolute quantitative engineering
accuracy, a more objective measure that can allow direct comparison between CAN techniques.

212
This finding emphasized that CAN is an adjunct tool but is not a replacement for knowledge of
surgical anatomy, as we demonstrated quantitatively that surgeons compensate for navigation
error based on this knowledge. These conclusions also led us to propose that reproducible
literature comparisons among CAN techniques must therefore be made by reporting of both
engineering accuracy, as a measure of relative technical merit, as well as radiographic accuracy
coupled with clinical sequlae, as a measure of application accuracy.
To then explore OTI as a feasible alternate technique for spinal neuronavigation, we assessed the
accuracy and workflow of OTI-CAN in multiple common-use clinical contexts. In open posterior
thoracolumbar approaches, the most commonly applied portal for spinal instrumentation, we
quantified engineering accuracies of less than 2 mm translationally, and 2.5° angularly, in each
of the axial and sagittal planes, in keeping with reported values for current commercial CAN
techniques. Total time from registration to navigation averaged less than one minute,
significantly faster than existing techniques. We subsequently extended our analysis to
minimally-invasive thoracolumbar instrumentation, and found comparable accuracy in both
cadaveric and clinical studies with similar workflow benefits. Finally, we validated the accuracy
of OTI in the more mobile cervical spine, and found comparable translational and angular
accuracy to our thoracolumbar cohort, again with similar workflow.
Finally, we set about characterizing error modalities that arise first with all spinal navigation
techniques, and subsequently those unique to range scanning methodologies such as OTI. Errors
from non-segmental registrsation arise in all techniques dependent on a dynamic reference frame
(DRF), including OTI. We categorized non-segmental registration errors as those arising by
virtue of distance from the DRF alone, from surgical manipulation of elements distant to the
DRF, and from patient respiration-induced motion. We found that the largest of these errors
arose from distance to the DRF, with an increase in mean three-dimensional translational error of
more than 2 mm at 2 or more levels distant from the DRF in the cervical and lumbar spine. Error
from surgical manipulation and respiration-induced motion was less than 2 mm on average,
however with a not-insignificant proportion greater than 2 mm, the threshold commonly cited for
clinical significance. Errors unique to high-density surface scanning techniques, of which OTI is

213
essentially the only example among current CAN techniques, relate to geometric congruence,
and were quantified for the first time as part of this thesis as being greater in the atlantoaxial and
subaxial cervical spine. Intra-operative maneuvers to avoid this pitfall, including bilateral
registration or extension of a unilateral exposure to include the base of the ipsilateral spinous
process, were identified.

214
10.2 Unifying Discussion
The ‘multiple paper’ format of this thesis has allowed for the pertinent discussion around each
set of experimental work to be included within the corresponding data chapter (see Sections 3.5,
4.5, 5.5, 6.5, 7.5, 8.5, 9.5). In order to minimize redundancy, these final unifying thoughts are
directed towards the overarching theme and goal of this body of work: the knowledge translation
of a novel surgical technique, and paradigm for the interaction of operators with image guidance
systems.
This journey began with the realization that, in general terms, for spinal pathologies which
constitute a significant and growing health care burden, a technology exists, in the form of
computer-assisted navigation, which has largely been shown to improve the accuracy of a given
set of surgical procedures, however with a highly heterogeneous body of evidence that renders
the results questionable and difficult to interpret. This technology is also associated with other
drawbacks, particularly in workflow and efficiency, and requires a steep capital and mental cost
in the form of a significant learning curve, all of which beg the question of whether the capital
and intellectual investment are worthwhile for nebulous benefit. The aim of this thesis was
therefore to first clarify, for spinal pathologies, where the concept of computer-assisted
navigation is best applied. We know intuitively and from limited surveys that minimally-invasive
and deformity cases are likely the best surgical procedures to take advantage of CAN.(Choo et
al., 2008; Hartl et al., 2013) However, from a broader perspective, the question of which
populations are most likely to benefit from and maximize the advantages of CAN, must be
posed. This is the primary focus of the experimental work in Chapter 3. We identified for the
first time in the literature that, at least in a Canadian cohort, most spinal instrumentations are
performed in a community setting by orthopedic surgeons, thereby pinpointing a key
demographic which may be able to maximize the benefits of CAN for patients. Barriers to spinal
CAN adoption must be overcome particularly in this population; while multiple surveys have
identified barriers in sample groups biased towards orthopedic surgeons, they are largely
reflective of academic practitioners, and therefore do not necessarily reflect barriers experienced
by community orthopedic surgeons in Canada.(Hartl et al., 2013) Nonetheless, what these prior

215
studies have suggested is that the largest impediments to adoption include a lack of proven and
readily-comparable accuracy, high capital cost, daunting training requirements, and intra-
operative radiation exposure. From a cost perspective, the utility of OTI for spinal image
guidance is not yet clear, as our work involved predominantly a research prototype system.
However, as dedicated intra-operative imaging devices, which constitute at least half of the cost
of a typical navigation setup, are avoided with this system, it is likely that overall capital
expenditure will be decreased. This remains to be demonstrated in future endeavours, however,
once commercialization of OTI platforms begins in earnest. We do know that OTI represents a
radiation-free technology intra-operatively, with therefore no exposure to both OR personnel and
intra-operatively to patients. However, one must be mindful that the total radiation cost to the
patient includes not only intra-operative exposure, but also any associated pre-operative imaging
for planning, and post-procedure imaging for instrumentation checks and follow up evaluation.
The experimental work in this thesis has not assessed or definitely shown lower overall radiation
cost to the patient relative to current CAN techniques. In our research paradigms assessing OTI
feasibility, a post-operative CT scan was required for accuracy quantification with high
precision. In routine clinical practice, however, a plain intra-operative XR following
instrumentation placement might often suffice for placement verification without quantification
of millimetric accuracy. Future studies of OTI in a more routine clinical workflow are therefore
required to assess whether this technique reduces the overall burden of radiation to the patient
during their entire clinical course. With regards to onerous training requirements as a barrier to
adoption of current CAN techniques, several studies have demonstrated significant learning
curves for navigation systems, with improvement in efficiency and accuracy demonstrated after
35-50 cases though with no robust assessment of whether improvement might have occurred at a
lower case volume.(Ryang et al., 2015; Wood & McMillen, 2014) In our initial analysis of OTI
feasibility for open posterior thoracolumbar exposures (Chapter 5), no significant operator
learning curve was demonstrated with regards to accuracy or efficiency. However, our studies
were performed by a single surgeon and trainee with involvement in the development of the
technology, hence it is not unfathomable that these trialists had greater upfront expertise than
might otherwise be expected from a truly novice user. The other possible perspective, of course,
is that the workflow improvements in the registration process significantly flattern the learning
curve of OTI relative to other CAN techniques. This remains to be addressed experimentally in
future multicenter comparative studies of commercialized OTI systems.

216
The primary rationale for CAN systems remains, however, improved accuracy through virtual
visualization of subsurface structures. The decision by a clinician to adopt any novel technique,
be it a diagnostic tool or therapeutic modality, is made by careful comparison of relative merits
and drawbacks. Meaningful comparisons can be made only on a level playing field, that is, with
homogeneity in classification and reporting mechanisms for the parameters relevant to
benchmarking. To date, uniformity in classification systems have not existed in the context of
spinal CAN systems. For the first time in the literature, we devised and demonstrated
quantitatively the rationale for a mechanism of reporting navigation accuracy based on both
engineering and clinicoradiographic parameters which, if applied readily in future investigations,
will allow practitioners to easily compare between novel navigation techniques. One immediate
potential application of this proposed reporting scheme is to compare the accuracy of robotically-
actuated navigation with freehand-actuated navigation. As discussed in Chapter 2, robotic
systems are on the immediate horizon of current CAN paradigms, with demonstrated
improvements in accuracy relative to traditional freehand techniques but minimal evidence to
demonstrate any additional utility over the current standard of freehand image guidance.(Roser et
al., 2013) However, uniform reporting remains a significant barrier, with new subjective
classification schemes being proposed even as of this writing.(Rajasekaran, Bhushan, Aiyer,
Kanna, & Shetty, 2018) Nonetheless, using our proposed reporting mechanism we demonstrated
for the first time in the literature that OTI is a faster yet comparably accurate and therefore
feasible CAN technique in relation to the current complement of technologies.
Another barrier to the routine usage of CAN has been its role in trainee education. While
multiple studies exist integrating CAN into phantom/cadaveric/virtual-reality simulators, with
evidence supporting subjective acceptance by trainees as an educational tool, if not significant
objective improvement in assessment metrics, there have been no studies to date assessing the
intra-operative utility of CAN for training. Anecdotally, CAN is often derided particularly by
non-adopters, as being a ‘crutch’ for inexperienced surgeons, hindering the acquisition of tactile
and visual landmarks for safe freehand instrumentation as is often the capability of expert senior
surgeons. However, an alternative perspective is that CAN, when applied correctly with

217
pedagogical intent as a verification tool rather than first-line guidance, may be a useful training
adjunct.(Manbachi et al., 2014) We demonstrate this for the first time in a nationwide survey of
surgical trainees, however with only self-reported metrics rather than true objective assessments.
Part of the process of training new CAN users and flattening their learning curve involves
identifying pitfalls of navigation systems, and knowing how to avoid them or otherwise correct
for them pre- and intra-operatively. To this end, common errors associated with all CAN
techniques including OTI (Chapter 8), as well as to OTI uniquely (Chapter 9), were identified.
More importantly, predictors of increased error from these modalities were characterized, to
allow surgeons to identify them and subsequently engage in mechanisms to address them. While
some of these error modalities may be considered common sense on a trial-and-error basis for
some surgeons, characterization by absolute quantification is often necessary to appreciate their
magnitude and mechanisms for avoidance, and we have done so for the first time here.
It is my hope that, collectively, the body of work presented in this thesis demonstrates the
feasibility of OTI as a safe and efficient technique for spinal CAN to allow increased adoption
amongst key players, and ultimately improved outcomes for their patients. Moreover, I hope to
have demonstrated that barriers to the knowledge translation of any novel medical technologies
can be overcome with a similar set of analyses, beginning with characterization of existing usage
patterns to identify key demographics for adoption, along with exploration and quantification of
specific shortcomings, and standardization of reporting schema where significant heterogeneity
exists.

218
10.3 Future Directions
Several avenues of largely epidemiological experimental work have presented themselves based
on limitations of our existing analyses. We explored usage patterns of spinal CAN among
Ontario surgeons, identifying specific demographics for which barriers to adoption must be
overcome by OTI and other future technologies. While we demonstrate that OTI-CAN represents
a significant improvement in workflow efficiency and therefore likely cost-effectiveness relative
to current systems, particularly given the lack of a requirement for intra-operative imaging
devices, this will need to be investigated definitively in a larger prospective cohort, accounting
for complications and reoperation costs following OTI-guided procedures. Similarly, while OTI
has no explicit radiation cost intra-operatively to patient or surgeon, the overall radiation
exposure to the patient including pre- and post-surgical imaging has not yet been evaluated, and
must be done with prospective observational dosimetric cohort studies. Comparison of the
learning curve between OTI and other CAN techniques also requires prospective multi-center,
multi-surgeon comparative cohorts.
The ability of structured light imaging to rapidly generate three-dimensional topographic maps of
a scanned surface lends itself well to numerous other avenues for potential future exploration. In
the current paradigm of open spinal surgery, possibilities include the application of OTI for real-
time continuous anatomical and instrument tracking, for machine learning-based adaptation to
level localization, and for the scanning of non-osseous surfaces to eliminate the need for intra-
operative imaging. Longer term possibilities include the natural extension of OTI-based
techniques to other non-spinal surgical applications.
In all current paradigms of frameless stereotactic navigation, a dynamic reference frame (DRF) is
required for relative instrument tracking and for maintenance of the initial registration. If the
pose of exposed surgical anatomy could be tracked in real-time, however, this would permit
updating of the initial registration simultaneously. Similar principles have already been applied

219
in the use of structured light illumination to update cranial registrations to compensate for intra-
operative brain shift, albeit at non-contiguous intervals (Chapter 2).(DeLorenzo et al., 2010; Paul
et al., 2009; Sun et al., 2005) With increases in the refresh rates of the visible-band cameras
responsible for capturing the deformed structured light illumination, and with appropriate
computing power, an exposed surface could be tracked at a frequency on the order of 10-30 Hz.
More intriguingly, surgical tools within the detection range of stereocameras could also be
tracked at the same frequency using the same visible band cameras, using object identification
algorithms to isolate and track a given surgical instrument. Modern infra-red (IR) optical
instrument tracking systems update at a frequency of 20-60 Hz,(NDI, 2018b) hence direct
visible-band instrument tracking at a comparable frequency would not result in any appreciable
lag to the operator. If computing power is insufficient to update registrations at this frequency, a
hybrid system of IR tool tracking within the visible-band camera volume may also be
considered, requiring an additional calibration to mesh the coordinate spaces of the IR and
visible cameras. Either technique would eliminate the need for a DRF and thereby obviate one of
the major pain points identified in current navigation workflows, as well as eliminate a
significant source of instrument-tracking error (Chapter 8).(Choo et al., 2008; Hartl et al., 2013)
The ability of OTI to segment and track vertebral levels individually may also be applied to the
real-time tracking of alignment intra-operatively. Particularly in long-segment deformity
correction procedures, a common-use scenario for spinal CAN, the final desired alignment is
decided a priori based on pre-operative imaging parameters and the necessary operative
maneuvers planned accordingly, i.e. what type of osteotomies may be required and at which
levels to achieve the desired correction. Intra-operative confirmation of achievement of the
desired alignment, however, remains a mainstay of traditional fluoroscopy, with repeated
imaging required to iteratively confirm the required correction at each operated level in order to
attain the desired global alignment. Real-time optical tracking of each segmental vertebral level
allows independent registration to the corresponding imaging dataset; changes in intervertebral
alignment may therefore be computed by repeat OTI registration, obviating the need for ongoing
fluoroscopic imaging. Changes in global alignment may then be computed by summating the
segmental changes in intervertebral alignment, to provide a radiation-free snapshot of global
alignment. Particularly in the context of adolescent idiopathic scoliosis, extension of OTI to real-

220
time segmental alignment tracking has the potential to significantly reduce radiation burden as
well as time cost, major topics of ongoing investigation in the adolescent spine field.(Presciutti,
Karukanda, & Lee, 2014; Ughwanogho, Patel, Baldwin, Sampson, & Flynn, 2012)
Another feasible application of vertebral imaging using OTI involves the localization of levels
for surgical site identification. The target level to be operated on is typically identified using
some combination of intra-operative localization, using fluoroscopy or mobile XR, and pre-
operative placement of radio-opaque markers which are then captured on pre-operative
imaging.(Hsiang, 2011; Hsu et al., 2008) Localization remains most challenging in the mid-
thoracic region or with poor visibility on XR imaging, as levels must be counted from the
occipito-cervical junction (‘top-down’) or lumbosacral junction (‘bottom-up’). The rate of
wrong-level surgery in the United States is approximately 0.03% which, while small, remains
unacceptably high for what should be a ‘never’ incidence.(Mody et al., 2008) With advances in
machine learning algorithms for object recognition,(Nasrabadi, 2007) as seen most evidently in
the consumer electronics arena with applications such as Google Lens, an opportunity exists for
a potential application of OTI in target level identification. A library of structured light-based
surface maps of various spinal levels may be constructed, with computation of relevant
differentiating parameters such as laminar and spinous process dimensions, and incident angles
of the lamina relative to cranial and caudal levels as well as to the spinous process; free
parameters would also be available, to allow application of a standard neural network
framework. Deep learning algorithms may then be applied to identify a set of parameters reliably
and uniquely identifying spinal levels, with testing and validation performed on a distinct set of
scanned vertebrae. OTI imaging might then be applied to an open posterior exposure to identify
the level without additional fluoroscopic imaging, or as a confirmatory measure if fluoroscopic
identification is equivocal or difficult. This is likely most appropriate only in larger open
exposures; in most minimally-invasive approaches, the skin incision must be tailored to the
target of interest, hence XR target localization prior to exposure remains a requirement. Certainly
this approach may be feasible, however, with precedent set by a similar algorithm employing a
2D-3D registration of intra-operative lateral XR to pre-operative CT for automatic level
confirmation, once levels had been reliably identified on the CT initially as the ‘gold
standard’.(Lo et al., 2015)

221
Continuing along the established path of spinal surgery, OTI may also be applied to image other
instruments in the operative field. A major limitation of OTI-CAN in its current form is the lack
of integrated verification of instrumentation placement accuracy; automatically-registered CAN
techniques require an intra-operative imaging device, which may be used post-instrumentation to
assess the accuracy of placed hardware, and revise intra-operatively if necessary. A scenario can
easily be envisioned however, with minimal software modification, whereby structured light
illumination may be applied to scan a pedicle screw as it is partially inserted into a target
cannulated tract. If the known screw diameter and length are specified, a virtual projection of the
imaged screw may then be placed onto the concomitantly-registered spine imaging, and
automatically advanced into final position in the imaging space to provide a real-time ‘virtual’
check on implant placement accuracy. The trajectory of pedicle screws is unlikely to change
significantly after the screw has been partially threaded into the cannulated tract, particularly if
the tract has been tapped previously,(Erkan et al., 2010) hence errors in the virtual projection can
reasonably be assumed to be minimal. Instrumentation verification may therefore be performed
in a radiation-free fashion, obviating the need for a bulky and costly intra-operative imaging
device or post-operative CT, with its associated radiation burden.
Adaption of OTI for the scanning of soft-tissues in the context of spinal surgery is also within the
realm of short-term possibility. Registration in its current prototype format is performed via
scanning of rigid osseous anatomy which, while readily accessible for open (Chapter 5) and even
mini-open MIS (Chapter 6) approaches, precludes fully percutaneous approaches to the spine.
Structured light-based 3D scanning of the back has already been described in the context of non-
invasive methods for evaluating patients with idiopathic scoliosis,(Mínguez et al., 2007) using
surface maps of the dorsal skin to compute metrics of axial deformity and global symmetry as
surrogates for traditional radiographic alignment parameters. One can imagine performing a
similar maneuver on a patient positioned prone on an operating table, or even coupling an OTI
scanner to a motorized rotatory frame similar to those in isocentric fluoroscopy or cone-beam CT
devices, to generate a partially circumferential surface map of the dorsal skin anatomy. Applying
a correction function to adjust for skin shift from supine pre-operative imaging to prone

222
operative positioning, registration may then theoretically be achieved using the skin surfaces
alone, allowing image-guided fully percutaneous procedures. With these advancements, there
would remain no limitations to OTI for spinal applications relative to current CAN techniques.
It is without question that OTI can readily be translated to other non-spinal surgical applications
as well. Our group is in the process of developing and validating OTI for cranial
neuronavigation; further developments will integrate real-time brain-shift compensation
algorithms on a much more efficient scale than those described previously in the literature
(Chapter 2). Applications in oromaxillofacial reconstruction have been described,(Kau,
Richmond, Incrapera, English, & Xia, 2007) as well as in facial morphology assessment for
infants with cleft palates.(Li et al., 2013) Our group is fortunate to have access to one of the
largest pediatric neurosurgical and plastic surgical units in Canada. One can imagine the practical
applications of OTI in, for instance, real-time updating of cephalometric parameters in patients
undergoing reconstruction for craniosynostoses, obviating the need for costly patient-specific
templates and moulds to guide intra-operative repair. 3D scanning in these patients has already
been described for post-operative routine follow up; it is but a small leap to extend this
application intra-operatively for real-time updates.(Tenhagen et al., 2016) Miniaturized
structured light-based 3D range scanning has also been described for laparoscopic applications to
intra-abdominal organ mapping, of significant utility in guiding liver resections.(Maurice,
Albitar, Doignon, & de Mathelin, 2012)
Looking to the more distant future, robotic actuation of instruments traditionally guided freehand
has begun to take hold particularly in spinal surgery (see Section 2.2.3). While no clear benefit
over freehand navigation has yet been demonstrated, one prevalent perspective is that robotic
actuation flattens the learning curve and maximizes the efficiency of image guidance for non-
CAN users, with perhaps negligible benefit for operators already proficient in freehand
navigation. With increasing advancements in OTI and other machine vision technologies
however, automated robotic instrument actuation using machine vision for real-time bony and
soft-tissue tracking and registration may represent a possible view of the future operating room.

223
References
Abdullah, K. G., Bishop, F. S., Lubelski, D., Steinmetz, M. P., Benzel, E. C., & Mroz, T. E.
(2012). Radiation Exposure to the Spine Surgeon in Lumbar and Thoracolumbar Fusions
With the Use of an Intraoperative Computed Tomographic 3-Dimensional Imaging System.
Spine, 37(17), E1074–E1078. http://doi.org/10.1097/BRS.0b013e31825786d8
Abe, Y., Ito, M., Abumi, K., Kotani, Y., Sudo, H., & Minami, A. (2011). A novel cost-effective
computer-assisted imaging technology for accurate placement of thoracic pedicle screws.
Journal of Neurosurgery. Spine, 15(5), 479–85. http://doi.org/10.3171/2011.6.SPINE10721
Acikbas, S. C., Arslan, F. Y., Tuncer, M. R., Matge, G., & Muciejczak, A. (2003). The effect of
transpedicular screw misplacement on late spinal stability. Acta Neurochirurgica, 145(11),
949–955. http://doi.org/10.1007/s00701-003-0116-0
Al-Khouja, L., Shweikeh, F., Pashman, R., Johnson, J. P., Kim, T. T., & Drazin, D. (2015).
Economics of image guidance and navigation in spine surgery. Surg Neurol Int, 6(Suppl
10), S323-6. http://doi.org/10.4103/2152-7806.159381
Alshail, E., Rutka, J. T., Drake, J. M., Hoffman, H. J., Humphreys, R., Phillips, J., … Holowka,
S. (1998). Utility of frameless stereotaxy in the resection of skull base and Basal cerebral
lesions in children. Skull Base Surgery, 8(1), 29–38.
Amiot, L.-P., & Poulin, F. (2004). Computed tomography-based navigation for hip, knee, and
spine surgery. Clinical Orthopaedics and Related Research, (421), 77–86.
Amiot, L. P., Lang, K., Putzier, M., Zippel, H., & Labelle, H. (2000). Comparative results
between conventional and computer-assisted pedicle screw installation in the thoracic,
lumbar, and sacral spine. Spine (Phila Pa 1976), 25(5), 606–614.
Aoude, A. A., Fortin, M., Figueiredo, R., Jarzem, P., Ouellet, J., & Weber, M. H. (2015).
Methods to determine pedicle screw placement accuracy in spine surgery: a systematic
review. European Spine Journal : Official Publication of the European Spine Society, the
European Spinal Deformity Society, and the European Section of the Cervical Spine
Research Society, 24(5), 990–1004. http://doi.org/10.1007/s00586-015-3853-x
Arand, M., Schempf, M., Fleiter, T., Kinzl, L., & Gebhard, F. (2006). Qualitative and
quantitative accuracy of CAOS in a standardized in vitro spine model. Clin Orthop Relat
Res, 450, 118–128. http://doi.org/10.1097/01.blo.0000218731.36967.e8
Armesto, L., Minguez, J., & Montesano, L. (2010). A generalization of the metric-based iterative
closest point technique for 3D scan matching. Proceedings - IEEE International Conference
on Robotics and Automation, 1367–1372. http://doi.org/10.1109/ROBOT.2010.5509371
Assaker, R., Reyns, N., Vinchon, M., Demondion, X., & Louis, E. (2001). Transpedicular screw
placement: image-guided versus lateral-view fluoroscopy: in vitro simulation. Spine (Phila
Pa 1976), 26(19), 2160–2164.
Baaj, A. A., Uribe, J. S., Nichols, T. A., Theodore, N., Crawford, N. R., Sonntag, V. K. H., &
Vale, F. L. (2010). Health care burden of cervical spine fractures in the United States:
analysis of a nationwide database over a 10-year period. Journal of Neurosurgery: Spine,
13(1), 61–66. http://doi.org/10.3171/2010.3.SPINE09530

224
Bai, Y.-S., Niu, Y.-F., Chen, Z.-Q., Zhu, X.-D., Gabriel, L. K. P., Wong, H. K., & Li, M. (2013).
Comparison of the pedicle screws placement between electronic conductivity device and
normal pedicle finder in posterior surgery of scoliosis. Journal of Spinal Disorders &
Techniques, 26(6), 316–20. http://doi.org/10.1097/BSD.0b013e318247f21d
Baig, M. N., Lubow, M., Immesoete, P., Bergese, S. D., Hamdy, E.-A., & Mendel, E. (2007).
Vision loss after spine surgery: review of the literature and recommendations.
Neurosurgical Focus, 23(5), E15. http://doi.org/10.3171/FOC-07/11/15
Banczerowski, P., Czigléczki, G., Papp, Z., Veres, R., Rappaport, H. Z., & Vajda, J. (2015).
Minimally invasive spine surgery: systematic review. Neurosurgical Review, 38(1), 11–26.
http://doi.org/10.1007/s10143-014-0565-3
Bandela, J. R., Jacob, R. P., Arreola, M., Griglock, T. M., Bova, F., & Yang, M. (2013). Use of
CT-Based Intraoperative Spinal Navigation: Management of Radiation Exposure to
Operator, Staff, and Patients. World Neurosurgery, 79(2), 390–394.
http://doi.org/10.1016/j.wneu.2011.05.019
Bandiera, S., Ghermandi, R., Gasbarrini, A., Barbanti Brodano, G., Colangeli, S., & Boriani, S.
(2013). Navigation-assisted surgery for tumors of the spine. Eur Spine J, 22 Suppl 6, S919-
24. http://doi.org/10.1007/s00586-013-3032-x
Barsa, P., Frőhlich, R., Šercl, M., Buchvald, P., & Suchomel, P. (2016). The intraoperative
portable CT scanner-based spinal navigation: a viable option for instrumentation in the
region of cervico-thoracic junction. European Spine Journal : Official Publication of the
European Spine Society, the European Spinal Deformity Society, and the European Section
of the Cervical Spine Research Society. http://doi.org/10.1007/s00586-016-4476-6
Belmont, P. J., Klemme, W. R., Dhawan, A., & Polly, D. W. (2001). In vivo accuracy of thoracic
pedicle screws. Spine, 26(21), 2340–6.
Berner, A., Bokeloh, M., Wand, M., Schilling, A., & Seidel, H.-P. (2008). A Graph-Based
Approach to Symmetry Detection. Symposium on Volume and Point-Based Graphics, 1–8.
Besi, P. J., & Mckay, N. D. (1992). A Method for Registration of 3-D Shapes. SPIE - Sensor
Fusion IV, 1611, 586–606. http://doi.org/10.1117/12.57955
Bindal, R. K., Glaze, S., Ognoskie, M., Tunner, V., Malone, R., & Ghosh, S. (2008). Surgeon
and patient radiation exposure in minimally invasive transforaminal lumbar interbody
fusion. Journal of Neurosurgery. Spine, 9(6), 570–3.
http://doi.org/10.3171/SPI.2008.4.08182
Biswas, D., Bible, J. E., Bohan, M., Simpson, A. K., Whang, P. G., & Grauer, J. N. (2009).
Radiation Exposure from Musculoskeletal Computerized Tomographic Scans. The Journal
of Bone and Joint Surgery-American Volume, 91(8), 1882–1889.
http://doi.org/10.2106/JBJS.H.01199
Bledsoe, J. M., Fenton, D., Fogelson, J. L., & Nottmeier, E. W. (2009). Accuracy of upper
thoracic pedicle screw placement using three-dimensional image guidance. The Spine
Journal, 9(10), 817–821. http://doi.org/10.1016/j.spinee.2009.06.014
Bourgeois, A. C., Faulkner, A. R., Bradley, Y. C., Pasciak, A. S., Barlow, P. B., Gash, J. R., &
Reid, W. S. (2015). Improved Accuracy of Minimally Invasive Transpedicular Screw
Placement in the Lumbar Spine With 3-Dimensional Stereotactic Image Guidance: A

225
Comparative Meta-Analysis. Journal of Spinal Disorders & Techniques, 28(9), 324–9.
http://doi.org/10.1097/BSD.0000000000000152
Bourgeois, A. C., Faulkner, A. R., Pasciak, A. S., & Bradley, Y. C. (2015). The evolution of
image-guided lumbosacral spine surgery. Ann Transl Med, 3(5), 69.
http://doi.org/10.3978/j.issn.2305-5839.2015.02.01
Burge, R., Dawson-Hughes, B., Solomon, D. H., Wong, J. B., King, A., & Tosteson, A. (2007).
Incidence and Economic Burden of Osteoporosis-Related Fractures in the United States,
2005-2025. Journal of Bone and Mineral Research, 22(3), 465–475.
http://doi.org/10.1359/jbmr.061113
Bydon, M., Mathios, D., Macki, M., De la Garza-Ramos, R., Aygun, N., Sciubba, D. M., …
Wolinksy, J. P. (2014). Accuracy of C2 pedicle screw placement using the anatomic
freehand technique. Clin Neurol Neurosurg, 125, 24–27.
http://doi.org/10.1016/j.clineuro.2014.07.017
Bydon, M., Mathios, D., Macki, M., De La Garza-Ramos, R., Aygun, N., Sciubba, D. M., …
Wolinksy, J. P. (2014). Accuracy of C2 pedicle screw placement using the anatomic
freehand technique. Clinical Neurology and Neurosurgery, 125, 24–27.
http://doi.org/10.1016/j.clineuro.2014.07.017
Cadarette, S. M., & Burden, A. M. (2011). The Burden of Osteoporosis in Canada. Canadian
Pharmacists Journal / Revue Des Pharmaciens Du Canada, 144(1_suppl), S3–S3.e1.
http://doi.org/10.3821/1913-701X-144.SUPPL1.S3
Carney, A. S., Patel, N., Baldwin, D. L., Coakham, H. B., & Sandeman, D. R. (1996). Intra-
operative image guidance in otolaryngology--the use of the ISG viewing wand. The Journal
of Laryngology and Otology, 110(4), 322–7.
Carrihill, B., & Hummel, R. (1985). Experiments with the intensity ratio depth sensor. Computer
Vision, Graphics, and Image Processing, 32(3), 337–358.
http://doi.org/https://doi.org/10.1016/0734-189X(85)90056-8
Castro, W. H., Halm, H., Jerosch, J., Malms, J., Steinbeck, J., & Blasius, S. (1996). Accuracy of
pedicle screw placement in lumbar vertebrae. Spine (Phila Pa 1976), 21(11), 1320–1324.
Chan, A., Parent, E., Narvacan, K., San, C., & Lou, E. (2017). Intraoperative image guidance
compared with free-hand methods in adolescent idiopathic scoliosis posterior spinal
surgery: a systematic review on screw-related complications and breach rates. The Spine
Journal. http://doi.org/10.1016/j.spinee.2017.04.001
Chen, C., & Zheng, Y. F. (1995). Passive and Active Stereo Vision for Smooth Surface
Detection of Deformed Plates. IEEE TRANSACTIONS ON INDUSTRIAL ELECTRONICS,
42(3).
Chen, Y., & Medioni, G. (1991). Object modeling by registration of multiple range images. In
Proceedings. 1991 IEEE International Conference on Robotics and Automation (pp. 2724–
2729). IEEE Comput. Soc. Press. http://doi.org/10.1109/ROBOT.1991.132043
Cho, J. Y., Chan, C. K., Lee, S. H., & Lee, H. Y. (2012). The accuracy of 3D image navigation
with a cutaneously fixed dynamic reference frame in minimally invasive transforaminal
lumbar interbody fusion. Comput Aided Surg, 17(6), 300–309.
http://doi.org/10.3109/10929088.2012.728625

226
Choo, A. D., Regev, G., Garfin, S. R., & Kim, C. W. (2008). Surgeons’ Perceptions of Spinal
Navigation: Analysis of Key Factors Affecting the Lack of Adoption of Spinal Navigation
Technology. SAS Journal, 2(4), 189–194. http://doi.org/10.1016/S1935-9810(08)70038-0
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and
standardized assessment instruments in psychology. Psychological Assessment, 6(4), 284.
Ciol, M. A., Deyo, R. A., Howell, E., & Kreif, S. (1996). An assessment of surgery for spinal
stenosis: time trends, geographic variations, complications, and reoperations. J Am Geriatr
Soc, 44(3), 285–290.
Clements, L. W., Chapman, W. C., & Dawant, B. M. (2008). Robust surface registration using
salient anatomical features for image-guided liver surgery : Algorithm and validation, 2528–
2540. http://doi.org/10.1118/1.2911920
Costa, F., Cardia, A., Ortolina, A., Fabio, G., Zerbi, A., & Fornari, M. (2011). Spinal navigation:
standard preoperative versus intraoperative computed tomography data set acquisition for
computer-guidance system: radiological and clinical study in 100 consecutive patients.
Spine, 36(24), 2094–8. http://doi.org/10.1097/BRS.0b013e318201129d
Costa, F., Porazzi, E., Restelli, U., Foglia, E., Cardia, A., Ortolina, A., … Banfi, G. (2014).
Economic study: a cost-effectiveness analysis of an intraoperative compared with a
preoperative image-guided system in lumbar pedicle screw fixation in patients with
degenerative spondylolisthesis. Spine J, 14(8), 1790–1796.
http://doi.org/10.1016/j.spinee.2013.10.019
Costa, F., Tosi, G., Attuati, L., Cardia, A., Ortolina, A., Grimaldi, M., … Fornari, M. (2016).
Radiation exposure in spine surgery using an image-guided system based on intraoperative
cone-beam computed tomography: analysis of 107 consecutive cases. Journal of
Neurosurgery: Spine, 25(5), 654–659. http://doi.org/10.3171/2016.3.SPINE151139
Cui, G., Wang, Y., Kao, T.-H., Zhang, Y., Liu, Z., Liu, B., … Xiao, S. (2012). Application of
intraoperative computed tomography with or without navigation system in surgical
correction of spinal deformity: a preliminary result of 59 consecutive human cases. Spine,
37(10), 891–900. http://doi.org/10.1097/BRS.0b013e31823aff81
Dea, N., Fisher, C. G., Batke, J., Strelzow, J., Mendelsohn, D., Paquette, S. J., … Street, J. T.
(2015). Economic evaluation comparing intraoperative cone beam CT-based navigation and
conventional fluoroscopy for the placement of spinal pedicle screws: a patient-level data
cost-effectiveness analysis. The Spine Journal : Official Journal of the North American
Spine Society. http://doi.org/10.1016/j.spinee.2015.09.062
Dea, N., Fisher, C. G., Batke, J., Strelzow, J., Mendelsohn, D., Paquette, S. J., … Street, J. T.
(2016). Economic evaluation comparing intraoperative cone beam CT-based navigation and
conventional fluoroscopy for the placement of spinal pedicle screws: A patient-level data
cost-effectiveness analysis. Spine Journal, 16(1), 23–31.
http://doi.org/10.1016/j.spinee.2015.09.062
DeLorenzo, C., Papademetris, X., Staib, L. H., Vives, K. P., Spencer, D. D., & Duncan, J. S.
(2010). Image-Guided Intraoperative Cortical Deformation Recovery Using Game Theory:
Application to Neocortical Epilepsy Surgery. IEEE Transactions on Medical Imaging,
29(2), 322–338. http://doi.org/10.1109/TMI.2009.2027993
DiGiorgio, A. M., Edwards, C. S., Virk, M. S., Mummaneni, P. V., & Chou, D. (2017).

227
Stereotactic navigation for the prepsoas oblique lateral lumbar interbody fusion: technical
note and case series. Neurosurgical Focus, 43(2), E14.
http://doi.org/10.3171/2017.5.FOCUS17168
Du, J. P., Fan, Y., Wu, Q. N., Wang, D. H., Zhang, J., & Hao, D. J. (2017). Accuracy of Pedicle
Screw Insertion among Three Image-Guided Navigation Systems: A Systematic Review
and Meta-Analysis. World Neurosurgery. http://doi.org/10.1016/j.wneu.2017.07.154
Du, J. P., Fan, Y., Wu, Q. N., Wang, D. H., Zhang, J., & Hao, D. J. (2018). Accuracy of Pedicle
Screw Insertion Among 3 Image-Guided Navigation Systems: Systematic Review and
Meta-Analysis. World Neurosurgery, 109(January), 24–30.
http://doi.org/10.1016/j.wneu.2017.07.154
Eggers, G., Mühling, J., & Marmulla, R. (2006). Image-to-patient registration techniques in head
surgery. International Journal of Oral and Maxillofacial Surgery, 35(12), 1081–1095.
http://doi.org/10.1016/j.ijom.2006.09.015
Erkan, S., Hsu, B., Wu, C., Mehbod, A. A., Perl, J., & Transfeldt, E. E. (2010). Alignment of
pedicle screws with pilot holes: can tapping improve screw trajectory in thoracic spines?
European Spine Journal, 19(1), 71–77. http://doi.org/10.1007/s00586-009-1063-0
Euler, E., Heining, S., Fischer, T., Pfeifer, K. J., & Mutschler, W. (2002). Initial Clinical
Experiences with the SIREMOBIL Iso-C^ 3^ D. ELECTROMEDICA-ERLANGEN-, 70(1),
48–51.
Fan, G., Han, R., Gu, X., Zhang, H., Guan, X., Fan, Y., … He, S. (2017). Navigation improves
the learning curve of transforamimal percutaneous endoscopic lumbar discectomy.
International Orthopaedics, 41(2), 323–332. http://doi.org/10.1007/s00264-016-3281-5
Fan, X., Ji, S., Hartov, A., Roberts, D., & Paulsen, K. (2012). Registering stereovision surface
with preoperative magnetic resonance images for brain shift compensation. In D. R. Holmes
III & K. H. Wong (Eds.), Proc. SPIE (Vol. 8316, p. 83161C). International Society for
Optics and Photonics. http://doi.org/10.1117/12.911081
Fan, X., Ji, S., Hartov, A., Roberts, D. W., & Paulsen, K. D. (2014). Stereovision to MR image
registration for cortical surface displacement mapping to enhance image-guided
neurosurgery. Medical Physics, 41(10), 102302. http://doi.org/10.1118/1.4894705
Fichtner, J., Hofmann, N., Rienmüller, A., Buchmann, N., Gempt, J., Kirschke, J. S., … Ryang,
Y.-M. (2017). Revision Rate of Misplaced Pedicle Screws of the Thoracolumbar Spine -
Comparison of 3D Fluoroscopy Navigated with Freehand Placement - A Systematic
Analysis and Review of the Literature. World Neurosurgery.
http://doi.org/10.1016/j.wneu.2017.09.091
Fitzpatrick, J. M., West, J. B., & Maurer, C. R. (1998). Predicting error in rigid-body point-based
registration. IEEE Transactions on Medical Imaging, 17(5), 694–702.
http://doi.org/10.1109/42.736021
Fogarty, B. J., Khan, K., Ashall, G., & Leonard, A. G. (1999). Complications of long operations:
a prospective study of morbidity associated with prolonged operative time (> 6 h).
British Journal of Plastic Surgery, 52(1), 33–6. http://doi.org/10.1054/bjps.1998.3019
Foley, K. T., Simon, D. A., & Rampersaud, Y. R. (2001). Virtual fluoroscopy: computer-assisted
fluoroscopic navigation. Spine, 26(4), 347–51.

228
Fridley, J., Fahim, D., Navarro, J., Wolinsky, J., & Omeis, I. (2014). Free-hand placement of
iliac screws for spinopelvic fixation based on anatomical landmarks: technical note.
International Journal of Spine Surgery, 8(1), 3–3. http://doi.org/10.14444/1003
Friets, E. M., Strohbehn, J. W., Hatch, J. F., & Roberts, D. W. (1989). A frameless stereotaxic
operating microscope for neurosurgery. IEEE Transactions on Biomedical Engineering,
36(6), 608–617. http://doi.org/10.1109/10.29455
Fu, T.-S., Chen, L.-H., Wong, C.-B., Lai, P.-L., Tsai, T.-T., Niu, C.-C., & Chen, W.-J. (2004).
Computer-assisted fluoroscopic navigation of pedicle screw insertion: an in vivo feasibility
study. Acta Orthopaedica Scandinavica, 75(6), 730–5.
Fu, T. S., Wong, C. B., Tsai, T. T., Liang, Y. C., Chen, L. H., & Chen, W. J. (2008). Pedicle
screw insertion: computed tomography versus fluoroscopic image guidance. Int Orthop,
32(4), 517–521. http://doi.org/10.1007/s00264-007-0358-1
Funao, H., Ishii, K., Momoshima, S., Iwanami, A., Hosogane, N., Watanabe, K., … Matsumoto,
M. (2014). Surgeons’ Exposure to Radiation in Single- and Multi-Level Minimally Invasive
Transforaminal Lumbar Interbody Fusion; A Prospective Study. PLoS ONE, 9(4), e95233.
http://doi.org/10.1371/journal.pone.0095233
Gasco, J., Patel, A., Ortega-Barnett, J., Branch, D., Desai, S., Kuo, Y. F., … Roitberg, B. Z.
(2014). Virtual reality spine surgery simulation: an empirical study of its usefulness.
Neurological Research, 36(11), 968–973. http://doi.org/10.1179/1743132814Y.0000000388
Gelalis, I. D., Paschos, N. K., Pakos, E. E., Politis, A. N., Arnaoutoglou, C. M., Karageorgos, A.
C., … Xenakis, T. A. (2012). Accuracy of pedicle screw placement: a systematic review of
prospective in vivo studies comparing free hand, fluoroscopy guidance and navigation
techniques. Eur Spine J, 21(2), 247–255. http://doi.org/10.1007/s00586-011-2011-3
Gelfand, N., Ikemoto, L., Rusinkiewicz, S., & Levoy, M. (2003). Geometrically Stable Sampling
for the ICP Algorithm. Proceedings of the Fourth International Conference on 3-D Digital
Imaging and Modeling - IEEE.
Geng, J. (2011). Structured-light 3D surface imaging: a tutorial. Advances in Optics and
Photonics, 3(2), 128. http://doi.org/10.1364/AOP.3.000128
Gertzbein, S. D., & Robbins, S. E. (1990). Accuracy of pedicular screw placement in vivo.
Spine, 15(1), 11–4.
Glossop, N. D. (2009). Advantages of optical compared with electromagnetic tracking. Journal
of Bone and Joint Surgery - Series A, 91(SUPPL. 1), 23–28.
http://doi.org/10.2106/JBJS.H.01362
Glossop, N., & Hu, R. (1997). Assessment of vertebral body motion during spine surgery. Spine,
22(8), 903–9.
Goldstein, C. L., Macwan, K., Sundararajan, K., & Rampersaud, Y. R. (2016). Perioperative
outcomes and adverse events of minimally invasive versus open posterior lumbar fusion:
meta-analysis and systematic review. Journal of Neurosurgery: Spine, 24(3), 416–427.
http://doi.org/10.3171/2015.2.SPINE14973
Gottschalk, M. B., Yoon, S. T., Park, D. K., Rhee, J. M., & Mitchell, P. M. (2015). Surgical
training using three-dimensional simulation in placement of cervical lateral mass screws: a
blinded randomized control trial. The Spine Journal, 15(1), 168–175.

229
http://doi.org/10.1016/j.spinee.2014.08.444
Gottschalk, M. B., Yoon, S. T., Park, D. K., Rhee, J. M., & Mitchell, P. M. (2015). Surgical
training using three-dimensional simulation in placement of cervical lateral mass screws: a
blinded randomized control trial. Spine J, 15(1), 168–175.
http://doi.org/10.1016/j.spinee.2014.08.444
Grunert, P., Darabi, K., Espinosa, J., & Filippi, R. (2003). Computer-aided navigation in
neurosurgery. Neurosurgical Review, 26(2), 73–99. http://doi.org/10.1007/s10143-003-
0262-0
Guha, D., Jakubovic, R., Gupta, S., Alotaibi, N. M., Cadotte, D., da Costa, L. B., … Yang, V. X.
D. (2017). Spinal intraoperative three-dimensional navigation: correlation between clinical
and absolute engineering accuracy. The Spine Journal, 17(4), 489–498.
http://doi.org/10.1016/j.spinee.2016.10.020
Guha, D., Jakubovic, R., Gupta, S., Fehlings, M., Yee, A., & Yang, V. (2017). 0127: Optical
topographic imaging for intraoperative 3d navigation in the cervical spine. Canadian
Journal of Surgery, 60(3), S104.
Guthrie, B. L., & Adler, J. R. (1992). Computer-assisted preoperative planning, interactive
surgery, and frameless stereotaxy. Clinical Neurosurgery, 38, 112–131.
Güven, O., Yalçin, S., Karahan, M., & Sevinç, T. T. (1994). Postoperative evaluation of
transpedicular screws with computed tomography. Orthopaedic Review, 23(6), 511–6.
Haberland, N., Ebmeier, K., Grunewald, J. P., Hliscs, R., & Kalff, R. L. (2000). Incorporation of
intraoperative computerized tomography in a newly developed spinal navigation technique.
Computer Aided Surgery : Official Journal of the International Society for Computer Aided
Surgery, 5(1), 18–27. http://doi.org/10.1002/(SICI)1097-0150(2000)5:1<18::AID-
IGS3>3.0.CO;2-T
Hartl, R., Lam, K. S., Wang, J., Korge, A., Kandziora, F., & Audige, L. (2013). Worldwide
survey on the use of navigation in spine surgery. World Neurosurg, 79(1), 162–172.
http://doi.org/10.1016/j.wneu.2012.03.011
Hassfeld, S., & Mühling, J. (2001). Computer assisted oral and maxillofacial surgery--a review
and an assessment of technology. International Journal of Oral and Maxillofacial Surgery,
30(1), 2–13. http://doi.org/10.1054/ijom.2000.0024
Heary, R. F., Bono, C. M., & Black, M. (2004). Thoracic pedicle screws: postoperative
computerized tomography scanning assessment. Journal of Neurosurgery, 100(4 Suppl
Spine), 325–31.
Hecht, N., Kamphuis, M., Czabanka, M., Hamm, B., König, S., Woitzik, J., … Hospital, B. J. B.
C. (2010). Intraoperative Iso-C C-Arm Navigation in Craniospinal Surgery: The First 60
Cases. Journal of Neurosurgery: Spine, 36(3), E1. http://doi.org/10.3171/SPI.2008.9.11.450
Hecht, N., Kamphuis, M., Czabanka, M., Hamm, B., König, S., Woitzik, J., … Vajkoczy, P.
(2015). Accuracy and workflow of navigated spinal instrumentation with the mobile
AIRO(®) CT scanner. European Spine Journal : Official Publication of the European Spine
Society, the European Spinal Deformity Society, and the European Section of the Cervical
Spine Research Society. http://doi.org/10.1007/s00586-015-3814-4
Helferty, J. P., & Higgins, W. E. (2001). Technique for registering 3D virtual CT images to

230
endoscopic video. In Proceedings 2001 International Conference on Image Processing
(Cat. No.01CH37205) (Vol. 2, pp. 893–896). IEEE.
http://doi.org/10.1109/ICIP.2001.958638
Helm, P. A., Teichman, R., Hartmann, S. L., & Simon, D. (2015). Spinal Navigation and
Imaging: History, Trends, and Future. IEEE Transactions on Medical Imaging, 34(8),
1738–1746. http://doi.org/10.1109/TMI.2015.2391200
Herz, T., Franz, A., Giacomuzzi, S. M., Bale, R., & Krismer, M. (2003). Accuracy of Spinal
Navigation for Magerl Screws. Clinical Orthopaedics and Related Research, 409(409),
124–130. http://doi.org/10.1097/01.blo.0000053345.97749.a6
Hodges, S. D., Eck, J. C., & Newton, D. (2012). Analysis of CT-based navigation system for
pedicle screw placement. Orthopedics, 35(8), e1221-4. http://doi.org/10.3928/01477447-
20120725-23
Holly, L. T., & Foley, K. T. (2003). Intraoperative Spinal Navigation. Spine, 28(supplement),
S54–S61. http://doi.org/10.1097/01.BRS.0000076899.78522.D9
Hoppe, H., Däuber, S., Kübler, C., Raczkowsky, J., & Wörn, H. (2002). A new, accurate and
easy to implement camera and video projector model. Studies in Health Technology and
Informatics, 85, 204–6.
Hsiang, J. (2011). Wrong-level surgery: A unique problem in spine surgery. Surgical Neurology
International, 2, 47. http://doi.org/10.4103/2152-7806.79769
Hsu, W., Sciubba, D. M., Daniel Sasson, A., Khavkin, Y., Wolinsky, J.-P., Gailloud, P., …
Murphy, K. (2008). Intraoperative Localization of Thoracic Spine Level With Preoperative
Percutaneous Placement of Intravertebral Polymethylmethacrylate. Journal of Spinal
Disorders & Techniques, 21(1), 72–75. http://doi.org/10.1097/BSD.0b013e3181493194
Hu, W., Tang, J., Wu, X., Zhang, L., & Ke, B. (2016). Minimally invasive versus open
transforaminal lumbar fusion: a systematic review of complications. International
Orthopaedics, 40(9), 1883–1890. http://doi.org/10.1007/s00264-016-3153-z
Izadpanah, K., Konrad, G., Südkamp, N. P., & Oberst, M. (2009). Computer Navigation in
Balloon Kyphoplasty Reduces the Intraoperative Radiation Exposure. Spine, 34(12), 1325–
1329. http://doi.org/10.1097/BRS.0b013e3181a18529
Jakubovic, R., Guha, D., Lu, M., Gupta, S., Cadotte, D. W., Heyn, C., … Yang, V. X. D. (2016).
A.709: Design and development of a novel, fast, extensive intraoperative registration
technique of optical machine vision to pre-operative imaging for cranial and spinal
neurosurgical procedures: clinical feasibility and comparison with existing neuronavi.
Journal of Neurosurgery, 124(4), A1146-209.
http://doi.org/10.3171/2016.4.JNS.AANS2016abstracts
Jeon, S., Lee, G. W., Jeon, Y. D., Park, I.-H., Hong, J., & Kim, J.-D. (2015). A preliminary study
on surgical navigation for epiduroscopic laser neural decompression. Proceedings of the
Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, 229(10),
693–702. http://doi.org/10.1177/0954411915599801
Ji, S., Fan, X., Paulsen, K. D., Roberts, D. W., Mirza, S. K., & Lollis, S. S. (2015). Patient
Registration Using Intraoperative Stereovision in Image-guided Open Spinal Surgery. IEEE
Transactions on Biomedical Engineering, 62(9), 2177–2186.

231
http://doi.org/10.1109/TBME.2015.2415731
Ji, S., Fan, X., Roberts, D. W., Hartov, A., & Paulsen, K. D. (2014). Cortical surface shift
estimation using stereovision and optical flow motion tracking via projection image
registration. Medical Image Analysis, 18(7), 1169–83.
http://doi.org/10.1016/j.media.2014.07.001
Joseph, J. R., Smith, B. W., Liu, X., & Park, P. (2017). Current applications of robotics in spine
surgery: a systematic review of the literature. Neurosurgical Focus, 42(5), E2.
http://doi.org/10.3171/2017.2.FOCUS16544
Joseph, J. R., Smith, B. W., Patel, R. D., & Park, P. (2016). Use of 3D CT-based navigation in
minimally invasive lateral lumbar interbody fusion. Journal of Neurosurgery: Spine,
25(September), 339–344. http://doi.org/10.3171/2016.2.SPINE151295.
Kalfas, I. H., Kormos, D. W., Murphy, M. A., McKenzie, R. L., Barnett, G. H., Bell, G. R., …
Weisenberger, J. P. (1995). Application of frameless stereotaxy to pedicle screw fixation of
the spine. J Neurosurg, 83(4), 641–647. http://doi.org/10.3171/jns.1995.83.4.0641
Kato, A., Yoshimine, T., Hayakawa, T., Tomita, Y., Ikeda, T., Mitomo, M., … Mogami, H.
(1991). A frameless, armless navigational system for computer-assisted neurosurgery.
Journal of Neurosurgery, 74(5), 845–849. http://doi.org/10.3171/jns.1991.74.5.0845
Kau, C. H., Richmond, S., Incrapera, A., English, J., & Xia, J. J. (2007). Three-dimensional
surface acquisition systems for the study of facial morphology and their application to
maxillofacial surgery. The International Journal of Medical Robotics and Computer
Assisted Surgery, 3(2), 97–110. http://doi.org/10.1002/rcs.141
Keller, K., & Ackerman, J. D. (2000). Real-time structured light depth extraction. Proc. SPIE,
3958, 11–19. http://doi.org/10.1117/12.380037
Kelly, P. J. (1990). Stereotactic craniotomy. Neurosurgery Clinics of North America, 1(4), 781–
99.
Khadem, R., Yeh, C. C., Sadeghi-Tehrani, M., Bax, M. R., Johnson, J. A., Welch, J. N., …
Shahidi, R. (2000). Comparative Tracking Error Analysis of Five Different Optical
Tracking Systems. Computer Aided Surgery, 5(2), 98–107.
http://doi.org/10.3109/10929080009148876
Kim, H.-S. H.-S., Suk, K.-S. K.-S., Moon, S.-H. S.-H., Lee, H.-M. H.-M., Kang, K. C., Lee, S.-
H. S.-H., & Kim, J.-S. J.-S. (2014). Safety evaluation of freehand lateral mass screw
fixation in the subaxial cervical spine: Evaluation of 1256 screws. Spine.40 (1) ()(Pp 2-5),
2014.Date of Publication: 01 Jan 2015., 40(1), 2–5.
http://doi.org/10.1097/BRS.0000000000000667
Kim, M.-C., Chung, H.-T., Cho, J.-L., Kim, D.-J., & Chung, N.-S. (2011). Factors affecting the
accurate placement of percutaneous pedicle screws during minimally invasive
transforaminal lumbar interbody fusion. European Spine Journal : Official Publication of
the European Spine Society, the European Spinal Deformity Society, and the European
Section of the Cervical Spine Research Society, 20(10), 1635–43.
http://doi.org/10.1007/s00586-011-1892-5
Kim, T. T., Drazin, D., Shweikeh, F., Pashman, R., & Johnson, J. P. (2014). Clinical and
radiographic outcomes of minimally invasive percutaneous pedicle screw placement with

232
intraoperative CT (O-arm) image guidance navigation. Neurosurgical Focus, 36(3), E1.
http://doi.org/10.3171/2014.1.FOCUS13531
Kim, T. T., Johnson, J. P., Pashman, R., & Drazin, D. (2016). Minimally Invasive Spinal Surgery
with Intraoperative Image-Guided Navigation. BioMed Research International, 2016, 1–7.
http://doi.org/10.1155/2016/5716235
Kim, Y. J., Lenke, L. G., Bridwell, K. H., Cho, Y. S., & Riew, K. D. (2004). Free hand pedicle
screw placement in the thoracic spine: is it safe? Spine, 29(3), 333–42; discussion 342.
Kleck, C. J., Cullilmore, I., LaFleur, M., Lindley, E., Rentschler, M. E., Burger, E. L., … Patel,
V. V. (2016). A new 3-dimensional method for measuring precision in surgical navigation
and methods to optimize navigation accuracy. European Spine Journal : Official
Publication of the European Spine Society, the European Spinal Deformity Society, and the
European Section of the Cervical Spine Research Society, 25(6), 1764–74.
http://doi.org/10.1007/s00586-015-4235-0
Koivukangas, T., Katisko, J. P. A., & Koivukangas, J. P. (2011). Technical accuracy of an O-arm
registered surgical navigator. In 2011 Annual International Conference of the IEEE
Engineering in Medicine and Biology Society (pp. 2148–2151). IEEE.
http://doi.org/10.1109/IEMBS.2011.6090402
Komatsubara, T., Tokioka, T., Sugimoto, Y., & Ozaki, T. (2016). Minimally Invasive Cervical
Pedicle Screw Fixation by a Posterolateral Approach for Acute Cervical Injury. Clinical
Spine Surgery. http://doi.org/10.1097/BSD.0000000000000421
Kosugi, Y., Watanabe, E., Goto, J., Watanabe, T., Yoshimoto, S., Takakura, K., & Ikebe, J.
(1988). An articulated neurosurgical navigation system using MRI and CT images. IEEE
Transactions on Biomedical Engineering, 35(2), 147–152. http://doi.org/10.1109/10.1353
Kotani, T., Akazawa, T., Sakuma, T., Koyama, K., Nemoto, T., Nawata, K., … Minami, S.
(2014). Accuracy of Pedicle Screw Placement in Scoliosis Surgery: A Comparison between
Conventional Computed Tomography-Based and O-Arm-Based Navigation Techniques.
Asian Spine Journal, 8(3), 331. http://doi.org/10.4184/asj.2014.8.3.331
Kotani, Y., Abumi, K., Ito, M., Takahata, M., Sudo, H., Ohshima, S., & Minami, A. (2007).
Accuracy analysis of pedicle screw placement in posterior scoliosis surgery: comparison
between conventional fluoroscopic and computer-assisted technique. Spine, 32(14), 1543–
50. http://doi.org/10.1097/BRS.0b013e318068661e
Kral, F., Puschban, E. J., Riechelmann, H., & Freysinger, W. (2013). Comparison of optical and
electromagnetic tracking for navigated lateral skull base surgery. The International Journal
of Medical Robotics and Computer Assisted Surgery, 9(2), 247–252.
http://doi.org/10.1002/rcs.1502
Laine, T., Lund, T., Ylikoski, M., Lohikoski, J., & Schlenzka, D. (2000). Accuracy of pedicle
screw insertion with and without computer assistance: a randomised controlled clinical
study in 100 consecutive patients. European Spine Journal : Official Publication of the
European Spine Society, the European Spinal Deformity Society, and the European Section
of the Cervical Spine Research Society, 9(3), 235–40.
Lange, J., Karellas, A., Street, J., Eck, J. C., Lapinsky, A., Connolly, P. J., & DiPaola, C. P.
(2013). Estimating the Effective Radiation Dose Imparted to Patients by Intraoperative
Cone-Beam Computed Tomography in Thoracolumbar Spinal Surgery. Spine, 38(5), E306–

233
E312. http://doi.org/10.1097/BRS.0b013e318281d70b
Laudato, P. A., Pierzchala, K., & Schizas, C. (2017). Pedicle Screw Insertion Accuracy Using O-
Arm, robotic guidance or freehand technique. SPINE, 1.
http://doi.org/10.1097/BRS.0000000000002449
Laughner, J. I., Zhang, S., Li, H., Shao, C. C., & Efimov, I. R. (2012). Mapping cardiac surface
mechanics with structured light imaging. American Journal of Physiology-Heart and
Circulatory Physiology, 303(6), H712–H720. http://doi.org/10.1152/ajpheart.00269.2012
Lavallee, S. (1996). Registration for computer-integrated surgery: methodology, state of the art.
In R. Taylor, S. Lavallee, G. Burdea, & R. Mosges (Eds.), Computer-Integrated Surgery:
(pp. 77–97). Cambridge: MIT Press.
Lavallee, S., Szelisky, R., & Brunie, L. (1996). Anatomy-based registration of three-dimensional
medical images, range images, X-ray projections, and three-dimensional models using
octree-splines. In R. Taylor, S. Lavallee, G. Burdea, & R. Mosges (Eds.), Computer-
Integrated Surgery. (pp. 115–143). Cambridge: MIT Press.
Lavelle, W. F., Ranade, A., Samdani, A. F., Gaughan, J. P., D’Andrea, L. P., & Betz, R. R.
(2014). Inter- and intra-observer reliability of measurement of pedicle screw breach
assessed by postoperative CT scans. International Journal of Spine Surgery, 8.
http://doi.org/10.14444/1011
Lee, G. Y. F., Massicotte, E. M., & Raja Rampersaud, Y. (2007). Clinical Accuracy of
Cervicothoracic Pedicle Screw Placement. Journal of Spinal Disorders & Techniques,
20(1), 25–32. http://doi.org/10.1097/01.bsd.0000211239.21835.ad
Lee, G. Y., Massicotte, E. M., & Rampersaud, Y. R. (2007). Clinical accuracy of cervicothoracic
pedicle screw placement: a comparison of the “open” lamino-foraminotomy and computer-
assisted techniques. Journal of Spinal Disorders & Techniques, 20(1), 25–32.
http://doi.org/10.1097/01.bsd.0000211239.21835.ad
Li, G., Wei, J., Wang, X., Wu, G., Ma, D., Wang, B., … Feng, X. (2013). Three-dimensional
facial anthropometry of unilateral cleft lip infants with a structured light scanning system.
Journal of Plastic, Reconstructive & Aesthetic Surgery : JPRAS, 66(8), 1109–16.
http://doi.org/10.1016/j.bjps.2013.04.007
Liu, Y., Zeng, C., Fan, M., Hu, L., Ma, C., & Tian, W. (2015). Assessment of respiration-
induced vertebral motion in prone-positioned patients during general anaesthesia. The
International Journal of Medical Robotics + Computer Assisted Surgery : MRCAS.
http://doi.org/10.1002/rcs.1676
Lo, S.-F. L., Otake, Y., Puvanesarajah, V., Wang, A. S., Uneri, A., De Silva, T., … Siewerdsen,
J. H. (2015). Automatic localization of target vertebrae in spine surgery: clinical evaluation
of the LevelCheck registration algorithm. Spine, 40(8), E476-83.
http://doi.org/10.1097/BRS.0000000000000814
Lorias-Espinoza, D., Carranza, V. G., de León, F. C.-P., Escamirosa, F. P., & Martinez, A. M.
(2016). A Low-Cost, Passive Navigation Training System for Image-Guided Spinal
Intervention. World Neurosurgery, 95, 322–328. http://doi.org/10.1016/j.wneu.2016.08.006
Luciano, C. J., Banerjee, P. P., Bellotte, B., Oh, G. M., Lemole Jr., M., Charbel, F. T., &
Roitberg, B. (2011). Learning retention of thoracic pedicle screw placement using a high-

234
resolution augmented reality simulator with haptic feedback. Neurosurgery, 69(1 Suppl
Operative), ons14-9; discussion ons19. http://doi.org/10.1227/NEU.0b013e31821954ed
Luther, N., Iorgulescu, J. B., Geannette, C., Gebhard, H., Saleh, T., Tsiouris, A. J., & Ha, R.
(2015). Comparison of Navigated Versus Non-Navigated Pedicle Screw Placement in 260
Patients and 1434 Screws Screw Accuracy , Screw Size , and the Complexity of Surgery,
28(5), 298–303.
Luther, N., Iorgulescu, J. B., Geannette, C., Gebhard, H., Saleh, T., Tsiouris, A. J., & Härtl, R.
(2015). Comparison of navigated versus non-navigated pedicle screw placement in 260
patients and 1434 screws: screw accuracy, screw size, and the complexity of surgery.
Journal of Spinal Disorders & Techniques, 28(5), E298-303.
http://doi.org/10.1097/BSD.0b013e31828af33e
Manbachi, A., Cobbold, R. S., & Ginsberg, H. J. (2014). Guided pedicle screw insertion:
techniques and training. Spine J, 14(1), 165–179.
http://doi.org/10.1016/j.spinee.2013.03.029
Martin, B. I., Turner, J. A., Mirza, S. K., Lee, M. J., Comstock, B. A., & Deyo, R. A. (2009).
Trends in Health Care Expenditures, Utilization, and Health Status Among US Adults With
Spine Problems, 1997–2006. Spine, 34(19), 2077–2084.
http://doi.org/10.1097/BRS.0b013e3181b1fad1
Mascott, C. R., Sol, J. C., Bousquet, P., Lagarrigue, J., Lazorthes, Y., & Lauwers-Cances, V.
(2006). Quantification of true in vivo (application) accuracy in cranial image-guided
surgery: Influence of mode of patient registration. Neurosurgery, 59(1 SUPPL. 1).
http://doi.org/10.1227/01.NEU.0000220089.39533.4E
Mason, A., Paulsen, R., Babuska, J. M., Rajpal, S., Burneikiene, S., Nelson, E. L., &
Villavicencio, A. T. (2014). The accuracy of pedicle screw placement using intraoperative
image guidance systems. J Neurosurg Spine, 20(2), 196–203.
http://doi.org/10.3171/2013.11.spine13413
Mathew, J. E., Mok, K., & Goulet, B. (2013). Pedicle violation and Navigational errors in
pedicle screw insertion using the intraoperative O-arm: A preliminary report. International
Journal of Spine Surgery, 7, e88-94. http://doi.org/10.1016/j.ijsp.2013.06.002
Maurer, Jr., C. R., Aboutanos, G. B., Dawant, B. M., Margolin, R. A., Maciunas, R. J., &
Fitzpatrick, J. M. (1995). Registration of CT and MR brain images using a combination of
points and surfaces. In M. H. Loew (Ed.), Proc. SPIE (pp. 109–123). International Society
for Optics and Photonics. http://doi.org/10.1117/12.208683
Maurer, C. R., Aboutanos, G. B., Dawant, B. M., Maciunas, R. J., & Fitzpatrick, J. M. (1996).
Registration of 3-D images using weighted geometrical features. IEEE Transactions on
Medical Imaging, 15(6), 836–849. http://doi.org/10.1109/42.544501
Maurice, X., Albitar, C., Doignon, C., & de Mathelin, M. (2012). A structured light-based
laparoscope with real-time organs’ surface reconstruction for minimally invasive surgery. In
2012 Annual International Conference of the IEEE Engineering in Medicine and Biology
Society (pp. 5769–5772). IEEE. http://doi.org/10.1109/EMBC.2012.6347305
McAnany, S., Overley, S., Kim, J., Baird, E., Qureshi, S., & Anderson, P. (2015). Open Versus
Minimally Invasive Fixation Techniques for Thoracolumbar Trauma: A Meta-Analysis.
Global Spine Journal, 6(2), 186–194. http://doi.org/10.1055/s-0035-1554777

235
Mendelsohn, D., Strelzow, J., Dea, N., Ford, N. L., Batke, J., Pennington, A., … Street, J.
(2016). Patient and surgeon radiation exposure during spinal instrumentation using
intraoperative computed tomography-based navigation. The Spine Journal, 16(3), 343–354.
http://doi.org/10.1016/j.spinee.2015.11.020
Metz, L. N., & Burch, S. (2008). Computer-assisted surgical planning and image-guided surgical
navigation in refractory adult scoliosis surgery: case report and review of the literature.
Spine, 33(9), E287-92. http://doi.org/10.1097/BRS.0b013e31816d256e
Milne, A. D., Chess, D. G., Johnson, J. A., & King, G. J. W. (1996). Accuracy of an
electromagnetic tracking device: a study of the optimal operating range and metal
interference. Journal of Biomechanics, 29(6), 791–793.
Mínguez, M. F., Buendía, M., Cibrián, R. M., Salvador, R., Laguía, M., Martín, A., & Gomar, F.
(2007). Quantifier variables of the back surface deformity obtained with a noninvasive
structured light method: evaluation of their usefulness in idiopathic scoliosis diagnosis.
European Spine Journal, 16(1), 73–82. http://doi.org/10.1007/s00586-006-0079-y
Mirota, D. J., Ishii, M., & Hager, G. D. (2011). Vision-Based Navigation in Image-Guided
Interventions. Annual Review of Biomedical Engineering, 13(1), 297–319.
http://doi.org/10.1146/annurev-bioeng-071910-124757
Mirza, S. K., Wiggins, G. C., Kuntz, C. th, York, J. E., Bellabarba, C., Knonodi, M. A., …
Shaffrey, C. I. (2003). Accuracy of thoracic vertebral body screw placement using standard
fluoroscopy, fluoroscopic image guidance, and computed tomographic image guidance: a
cadaver study. Spine (Phila Pa 1976), 28(4), 402–413.
http://doi.org/10.1097/01.brs.0000048461.51308.cd
Mody, M. G., Nourbakhsh, A., Stahl, D. L., Gibbs, M., Alfawareh, M., & Garges, K. J. (2008).
The Prevalence of Wrong Level Surgery Among Spine Surgeons. Spine, 33(2), 194–198.
http://doi.org/10.1097/BRS.0b013e31816043d1
Mösges, R., & Schlöndorff, G. (1988). A new imaging method for intraoperative therapy control
in skull-base surgery. Neurosurgical Review, 11(3–4), 245–7.
Mroz, T. E., Abdullah, K. G., Steinmetz, M. P., Klineberg, E. O., & Lieberman, I. H. (2011).
Radiation Exposure to the Surgeon During Percutaneous Pedicle Screw Placement. Journal
of Spinal Disorders & Techniques, 24(4), 264–267.
http://doi.org/10.1097/BSD.0b013e3181eed618
Mulconrey, D. S. (2016). Fluoroscopic Radiation Exposure in Spinal Surgery: In Vivo
Evaluation for Operating Room Personnel. Clinical Spine Surgery, 29(7), E331-5.
http://doi.org/10.1097/BSD.0b013e31828673c1
Murphy, M. A., McKenzie, R. L., Kormos, D. W., & Kalfas, I. H. (1994). Frameless stereotaxis
for the insertion of lumbar pedicle screws. Journal of Clinical Neuroscience : Official
Journal of the Neurosurgical Society of Australasia, 1(4), 257–60.
Nakashima, H., Sato, K., Ando, T., Inoh, H., & Nakamura, H. (2009). Comparison of the
percutaneous screw placement precision of isocentric C-arm 3-dimensional fluoroscopy-
navigated pedicle screw implantation and conventional fluoroscopy method with minimally
invasive surgery. Journal of Spinal Disorders & Techniques, 22(7), 468–72.
http://doi.org/10.1097/BSD.0b013e31819877c8

236
Nasrabadi, N. M. (2007). Pattern Recognition and Machine Learning. Journal of Electronic
Imaging, 16(4), 49901. http://doi.org/10.1117/1.2819119
Nasser, R., Nakhla, J., Echt, M., De la Garza Ramos, R., Kinon, M. D., Sharan, A., & Yassari, R.
(2018). Minimally Invasive Separation Surgery with Intraoperative Stereotactic Guidance:
A Feasibility Study. World Neurosurgery, 109, 68–76.
http://doi.org/10.1016/j.wneu.2017.09.067
NDI. (2018a). Aurora Accuracy Performance - Technical Specifications. Retrieved January 19,
2018, from https://www.ndigital.com/medical/products/aurora/#specifications-planer-field
NDI. (2018b). Polaris Specifications. Retrieved January 19, 2018, from
https://www.ndigital.com/medical/products/polaris-family/#specifications
Nelson, E. M., Monazzam, S. M., Kim, K. D., Seibert, J. A., & Klineberg, E. O. (2014).
Intraoperative fluoroscopy, portable X-ray, and CT: patient and operating room personnel
radiation exposure in spinal surgery. Spine J, 14(12), 2985–2991.
http://doi.org/10.1016/j.spinee.2014.06.003
Neo, M., Sakamoto, T., & Fujibayashi, S. (2005). The Clinical Risk of Vertebral Artery Injury
From Cervical Pedicle Screws Inserted in Degenerative Vertebrae, 30(24), 2800–2805.
Neo, M., Sakamoto, T., Fujibayashi, S., & Nakamura, T. (2005). The clinical risk of vertebral
artery injury from cervical pedicle screws inserted in degenerative vertebrae. Spine, 30(24),
2800–5.
Nolte, L. P., Slomczykowski, M. a, Berlemann, U., Strauss, M. J., Hofstetter, R., Schlenzka, D.,
… Lund, T. (2000). A new approach to computer-aided spine surgery: fluoroscopy-based
surgical navigation. European Spine Journal : Official Publication of the European Spine
Society, the European Spinal Deformity Society, and the European Section of the Cervical
Spine Research Society, 9 Suppl 1, S78--88. http://doi.org/10.1007/PL00010026
Nooh, A., Lubov, Ã. J., Weber, M. H., Aoude, A., Aldebeyan, S., Jarzem, P., & Ouellet, J.
(2017). Differences between Manufacturers of Computed Tomography – Based Computer-
Assisted Surgery Systems Do Exist : A Systematic Literature Review.
Nottmeier, E. W. (2012). A review of image-guided spinal surgery. J Neurosurg Sci, 56(1), 35–
47.
Nottmeier, E. W., & Crosby, T. (2009). Timing of Vertebral Registration in Three-dimensional,
Fluoroscopy-based, Image-guided Spinal Surgery. Journal of Spinal Disorders &
Techniques, 22(5), 358–360. http://doi.org/10.1097/BSD.0b013e31817dfcda
Nottmeier, E. W., Seemer, W., & Young, P. M. (2009). Placement of thoracolumbar pedicle
screws using three-dimensional image guidance: experience in a large patient cohort. J
Neurosurg Spine, 10(1), 33–39. http://doi.org/10.3171/2008.10.spi08383
Nottmeier, E. W., Seemer, W., & Young, P. M. (2009). Placement of thoracolumbar pedicle
screws using three-dimensional image guidance: experience in a large patient cohort.
Journal of Neurosurgery. Spine, 10(1), 33–9. http://doi.org/10.3171/2008.10.SPI08383
O’Brien, M. F., Lenke, L. G., Mardjetko, S., Lowe, T. G., Kong, Y., Eck, K., & Smith, D.
(2000). Pedicle morphology in thoracic adolescent idiopathic scoliosis: is pedicle fixation
an anatomically viable technique? Spine, 25(18), 2285–93.

237
Oertel, M. F., Hobart, J., Stein, M., Schreiber, V., & Scharbrodt, W. (2011). Clinical and
methodological precision of spinal navigation assisted by 3D intraoperative O-arm
radiographic imaging. Journal of Neurosurgery. Spine, 14(4), 532–536.
http://doi.org/10.3171/2010.10.SPINE091032
Ofiram, E., Garvey, T. A., Schwender, J. D., Denis, F., Perra, J. H., Transfeldt, E. E., …
Wroblewski, J. M. (2009). Cervical degenerative index: a new quantitative radiographic
scoring system for cervical spondylosis with interobserver and intraobserver reliability
testing. Journal of Orthopaedics and Traumatology, 10(1), 21–26.
http://doi.org/10.1007/s10195-008-0041-3
Okamoto, T., Onda, S., Yanaga, K., Suzuki, N., & Hattori, A. (2015). Clinical application of
navigation surgery using augmented reality in the abdominal field. Surgery Today, 45(4),
397–406. http://doi.org/10.1007/s00595-014-0946-9
Overley, S. C., Cho, S. K., Mehta, A. I., & Arnold, P. M. (2017). Navigation and Robotics in
Spinal Surgery : Where Are We Now ?, 80(3). http://doi.org/10.1093/neuros/nyw077
Papadopoulos, E. C., Girardi, F. P., Sama, A., Sandhu, H. S., & Cammisa, F. P. Accuracy of
single-time, multilevel registration in image-guided spinal surgery. The Spine Journal :
Official Journal of the North American Spine Society, 5(3), 263–7; discussion 268.
http://doi.org/10.1016/j.spinee.2004.10.048
Papadopoulos, E. C., Girardi, F. P., Sama, A., Sandhu, H. S., & Cammisa Jr., F. P. (2005).
Accuracy of single-time, multilevel registration in image-guided spinal surgery. Spine J,
5(3), 263–7; discussion 268. http://doi.org/10.1016/j.spinee.2004.10.048
Parker, S. L., McGirt, M. J., Farber, S. H., Amin, A. G., Rick, A. M., Suk, I., … Witham, T. F.
(2011). Accuracy of free-hand pedicle screws in the thoracic and lumbar spine: analysis of
6816 consecutive screws. Neurosurgery, 68(1), 170–8; discussion 178.
http://doi.org/10.1227/NEU.0b013e3181fdfaf4
Patil, A. A. (1984). Computed tomography plane of the target approach in computed
tomographic stereotaxis. Neurosurgery, 15(3), 410–4.
Paul, P., Morandi, X., & Jannin, P. (2009). A surface registration method for quantification of
intraoperative brain deformations in image-guided neurosurgery. IEEE Transactions on
Information Technology in Biomedicine, 13(6), 976–983.
http://doi.org/10.1109/TITB.2009.2025373
Pelizzari, C., & Chen, G. (1987). The use of computers in radiation therapy : proceedings of the
Ninth International Conference on the Use of Computers in Radiation Therapy held in
Scheveningen, the Netherlands, June 22-25, 1987. In I. A. D. Bruinvis (Ed.), (p. 590). North
Holland.
Pereira, E. A. C., Green, A. L., Nandi, D., & Aziz, T. Z. (2008). Stereotactic Neurosurgery in the
United Kingdom: The Hundred Years from Horsley to Hariz. Neurosurgery, 63(3), 594–
607. http://doi.org/10.1227/01.NEU.0000316854.29571.40
Pereira, V. M., Smit-Ockeloen, I., Brina, O., Babic, D., Breeuwer, M., Schaller, K., … Ruijters,
D. (2015). Volumetric Measurements of Brain Shift Using Intraoperative Cone-Beam
Computed Tomography: Preliminary Study. Neurosurgery.
http://doi.org/10.1227/NEU.0000000000000999

238
Peterhans, M., vom Berg, A., Dagon, B., Inderbitzin, D., Baur, C., Candinas, D., & Weber, S.
(2011). A navigation system for open liver surgery: design, workflow and first clinical
applications. The International Journal of Medical Robotics + Computer Assisted Surgery :
MRCAS, 7(1), 7–16. http://doi.org/10.1002/rcs.360
Phan, K., Hogan, J., Maharaj, M., & Mobbs, R. J. (2015). Cortical Bone Trajectory for Lumbar
Pedicle Screw Placement: A Review of Published Reports. Orthopaedic Surgery, 7(3), 213–
221. http://doi.org/10.1111/os.12185
Phan, K., & Mobbs, R. J. (2016). Minimally Invasive Versus Open Laminectomy for Lumbar
Stenosis. SPINE, 41(2), E91–E100. http://doi.org/10.1097/BRS.0000000000001161
Pisapia, J. M., Nayak, N. R., Salinas, R. D., Macyszyn, L., Lee, J. Y. K., Lucas, T. H., …
Schuster, J. M. (2017). Navigated odontoid screw placement using the O-arm: technical
note and case series. Journal of Neurosurgery: Spine, 26(1), 10–18.
http://doi.org/10.3171/2016.5.SPINE151412
Podolsky, D. J., Martin, A. R., Whyne, C. M., Massicotte, E. M., Hardisty, M. R., & Ginsberg,
H. J. (2010). Exploring the role of 3-dimensional simulation in surgical training: feedback
from a pilot study. Journal of Spinal Disorders & Techniques, 23(8), e70-4.
http://doi.org/10.1097/BSD.0b013e3181d345cb
Pomerleau, F., Colas, F., Siegwart, R., & Magnenat, S. (2013). Comparing ICP variants on real-
world data sets: Open-source library and experimental protocol. Autonomous Robots, 34(3),
133–148. http://doi.org/10.1007/s10514-013-9327-2
Pottmann, H., & Hofer, M. (2003). Geometry of the Squared Distance Function to Curves and
Surfaces (pp. 221–242). Springer, Berlin, Heidelberg. http://doi.org/10.1007/978-3-662-
05105-4_12
Presciutti, S. M., Karukanda, T., & Lee, M. (2014). Management decisions for adolescent
idiopathic scoliosis significantly affect patient radiation exposure. The Spine Journal :
Official Journal of the North American Spine Society, 14(9), 1984–90.
http://doi.org/10.1016/j.spinee.2013.11.055
Pribanić, T., Džapo, H., & Salvi, J. (2009). Efficient and Low-Cost 3D Structured Light System
Based on a Modified Number-Theoretic Approach. EURASIP Journal on Advances in
Signal Processing, 2010(1), 474389. http://doi.org/10.1155/2010/474389
Quillo-Olvera, J., Lin, G.-X., Suen, T.-K., Jo, H.-J., & Kim, J.-S. (2017). Anterior transcorporeal
tunnel approach for cervical myelopathy guided by CT-based intraoperative spinal
navigation: Technical note. Journal of Clinical Neuroscience.
http://doi.org/10.1016/j.jocn.2017.11.012
Quiñones-Hinojosa, A., Robert Kolen, E., Jun, P., Rosenberg, W. S., & Weinstein, P. R. (2006).
Accuracy over space and time of computer-assisted fluoroscopic navigation in the lumbar
spine in vivo. Journal of Spinal Disorders & Techniques, 19(2), 109–13.
http://doi.org/10.1097/01.bsd.0000168513.68975.8a
Qureshi, S., Lu, Y., McAnany, S., & Baird, E. (2014). Three-dimensional Intraoperative Imaging
Modalities in Orthopaedic Surgery. Journal of the American Academy of Orthopaedic
Surgeons, 22(12), 800–809. http://doi.org/10.5435/JAAOS-22-12-800
Rajaee, S. S., Bae, H. W., Kanim, L. E., & Delamarter, R. B. (2012). Spinal fusion in the United

239
States: analysis of trends from 1998 to 2008. Spine (Phila Pa 1976), 37(1), 67–76.
http://doi.org/10.1097/BRS.0b013e31820cccfb
Rajasekaran, S., Bhushan, M., Aiyer, S., Kanna, R., & Shetty, A. P. (2018). Accuracy of pedicle
screw insertion by AIRO® intraoperative CT in complex spinal deformity assessed by a
new classification based on technical complexity of screw insertion. European Spine
Journal. http://doi.org/10.1007/s00586-017-5453-4
Rajasekaran, S., Vidyadhara, S., Ramesh, P., & Shetty, A. P. (2007). Randomized clinical study
to compare the accuracy of navigated and non-navigated thoracic pedicle screws in
deformity correction surgeries. Spine (Phila Pa 1976), 32(2), E56-64.
http://doi.org/10.1097/01.brs.0000252094.64857.ab
Rambani, R., Ward, J., & Viant, W. (2014). Desktop-based computer-assisted orthopedic
training system for spinal surgery. Journal of Surgical Education, 71(6).
http://doi.org/10.1016/j.jsurg.2014.04.012
Rampersaud, Y. R., Foley, K. T., Shen, A. C., Williams, S., & Solomito, M. (2000). Radiation
exposure to the spine surgeon during fluoroscopically assisted pedicle screw insertion.
Spine, 25(20), 2637–45.
Rampersaud, Y. R., Simon, D. a, & Foley, K. T. (2001). Accuracy requirements for image-
guided spinal pedicle screw placement. Spine, 26(4), 352–359.
http://doi.org/10.1097/00007632-200102150-00010
Ray, W. Z., Ravindra, V. M., Schmidt, M. H., & Dailey, A. T. (2013). Stereotactic navigation
with the O-arm for placement of S-2 alar iliac screws in pelvic lumbar fixation. Journal of
Neurosurgery: Spine, 18(5), 490–495. http://doi.org/10.3171/2013.2.SPINE12813
Reinges, M. H., Spetzger, U., Rohde, V., Adams, L., & Gilsbach, J. M. (1998). Experience with
a new multifunctional articulated instrument holder in minimally invasive navigated
neurosurgery. Minimally Invasive Neurosurgery : MIN, 41(3), 149–51.
http://doi.org/10.1055/s-2008-1052032
Reinhardt, H. F., Horstmann, G. A., & Gratzl, O. (1993). Sonic stereometry in microsurgical
procedures for deep-seated brain tumors and vascular malformations. Neurosurgery, 32(1),
51–7; discussion 57.
Reinhardt, H., Meyer, H., & Amrein, E. (1988). A Computer-Assisted Device for the
Intraoperative CT-Correlated Localization of Brain Tumors. European Surgical Research,
20(1), 51–58. http://doi.org/10.1159/000128741
Ringel, F., Villard, J., Ryang, Y.-M., & Meyer, B. (2014). Navigation, robotics, and
intraoperative imaging in spinal surgery. Advances and Technical Standards in
Neurosurgery, 41, 3–22. http://doi.org/10.1007/978-3-319-01830-0_1
Rivkin, M. A., & Yocom, S. S. (2014). Thoracolumbar instrumentation with CT-guided
navigation (O-arm) in 270 consecutive patients: accuracy rates and lessons learned.
Neurosurgical Focus, 36(3), E7. http://doi.org/10.3171/2014.1.FOCUS13499
Roberts, D. W., Hartov, A., Kennedy, F. E., Miga, M. I., & Paulsen, K. D. (1998). Intraoperative
brain shift and deformation: a quantitative analysis of cortical displacement in 28 cases.
Neurosurgery, 43(4), 749-58-60.
Roberts, D. W., Strohbehn, J. W., Hatch, J. F., Murray, W., & Kettenberger, H. (1986). A

240
frameless stereotaxic integration of computerized tomographic imaging and the operating
microscope. Journal of Neurosurgery, 65(4), 545–549.
http://doi.org/10.3171/jns.1986.65.4.0545
Roberts, T. (1998). The BRW/CRW stereotactic appratus. In P. Tasker & P. Gildenberg (Eds.),
Textbook of Functional and Stereotactic Neurosurgery (pp. 65–71). New York: McGraw-
Hill.
Robertson, P. A., Novotny, J. E., Grobler, L. J., & Agbai, J. U. (1998). Reliability of axial
landmarks for pedicle screw placement in the lower lumbar spine. Spine, 23(1), 60–6.
Robinson, S., Robertson, F. C., Dasenbrock, H. H., O’Brien, C. P., Berde, C., & Padua, H.
(2017). Image-guided intrathecal baclofen pump catheter implantation: a technical note and
case series. Journal of Neurosurgery: Spine, 1–7.
http://doi.org/10.3171/2016.8.SPINE16263
Roessler, K., Ungersboeck, K., Dietrich, W., Aichholzer, M., Hittmeir, K., Matula, C., … Koos,
W. T. (1997). Frameless stereotactic guided neurosurgery: clinical experience with an
infrared based pointer device navigation system. Acta Neurochirurgica, 139(6), 551–9.
Roser, F., Tatagiba, M., & Maier, G. (2013). Spinal robotics: Current applications and future
perspectives. Neurosurgery, 72(SUPPL. 1), 12–18.
http://doi.org/10.1227/NEU.0b013e318270d02c
Ryang, Y.-M., Villard, J., Obermüller, T., Friedrich, B., Wolf, P., Gempt, J., … Meyer, B.
(2015). Learning curve of 3D fluoroscopy image–guided pedicle screw placement in the
thoracolumbar spine. The Spine Journal, 15(3), 467–476.
http://doi.org/10.1016/j.spinee.2014.10.003
Sakai, Y., Matsuyama, Y., Nakamura, H., Katayama, Y., Imagama, S., Ito, Z., & Ishiguro, N.
(2008). Segmental pedicle screwing for idiopathic scoliosis using computer-assisted
surgery. Journal of Spinal Disorders & Techniques, 21(3), 181–6.
http://doi.org/10.1097/BSD.0b013e318074d388
Salvi, J., Fernandez, S., Pribanic, T., & Llado, X. (2010). A state of the art in structured light
patterns for surface profilometry. Pattern Recognition, 43(8), 2666–2680.
http://doi.org/10.1016/j.patcog.2010.03.004
Sanborn, M. R., Thawani, J. P., Whitmore, R. G., Shmulevich, M., Hardy, B., Benedetto, C., …
Stein, S. C. (2012). Cost-effectiveness of confirmatory techniques for the placement of
lumbar pedicle screws. Neurosurg Focus, 33(1), E12.
http://doi.org/10.3171/2012.2.focus121
Sanborn, M. R., Thawani, J. P., Whitmore, R. G., Shmulevich, M., Hardy, B., Benedetto, C., …
Stein, S. C. (2012). Cost-effectiveness of confirmatory techniques for the placement of
lumbar pedicle screws. Neurosurgical Focus, 33(1), E12.
http://doi.org/10.3171/2012.2.FOCUS121
Sasso, R. C., & Garrido, B. J. (2007). Computer-assisted spinal navigation versus serial
radiography and operative time for posterior spinal fusion at L5-S1. Journal of Spinal
Disorders & Techniques, 20(2), 118–22.
http://doi.org/10.1097/01.bsd.0000211263.13250.b1
Schafer, S., Nithiananthan, S., Mirota, D. J., Uneri, A., Stayman, J. W., Zbijewski, W., …

241
Siewerdsen, J. H. (2011). Mobile C-arm cone-beam CT for guidance of spine surgery:
Image quality, radiation dose, and integration with interventional guidance. Medical
Physics, 38(8), 4563–4574. http://doi.org/10.1118/1.3597566
Scheufler, K.-M., Franke, J., Eckardt, A., & Dohmen, H. (2011a). Accuracy of image-guided
pedicle screw placement using intraoperative computed tomography-based navigation with
automated referencing, part I: cervicothoracic spine. Neurosurgery, 69(4), 782–95;
discussion 795. http://doi.org/10.1227/NEU.0b013e318222ae16
Scheufler, K.-M., Franke, J., Eckardt, A., & Dohmen, H. (2011b). Accuracy of image-guided
pedicle screw placement using intraoperative computed tomography-based navigation with
automated referencing. Part II: thoracolumbar spine. Neurosurgery, 69(6), 1307–16.
http://doi.org/10.1227/NEU.0b013e31822ba190
Schizas, C., Thein, E., Kwiatkowski, B., & Kulik, G. (2012). Pedicle screw insertion: robotic
assistance versus conventional C-arm fluoroscopy. Acta Orthopaedica Belgica, 78(2), 240–
5.
Schlaier, J., Warnat, J., & Brawanski, A. (2002). Registration accuracy and practicability of
laser-directed surface matching. Computer Aided Surgery : Official Journal of the
International Society for Computer Aided Surgery, 7(5), 284–90.
http://doi.org/10.1002/igs.10053
Schmalz, C., Forster, F., Schick, A., & Angelopoulou, E. (2012). An endoscopic 3D scanner
based on structured light. Medical Image Analysis, 16(5), 1063–1072.
http://doi.org/10.1016/j.media.2012.04.001
Schmerber, S., Chen, B., Lavallee, S., Chirosel, J., Poyet, A., Colomb, M., & Reyt, E. (1997).
Markerless hybrid registration method for computer assisted endoscopic ENT surgery. In H.
Lemke, M. Vannier, & K. Inamura (Eds.), CAR (pp. 799–806). Elsevier, Amsterdam.
Schröder, J., & Wassmann, H. (2006). Spinal navigation: an accepted standard of care?
Zentralblatt Fur Neurochirurgie, 67(3), 123–8. http://doi.org/10.1055/s-2006-942146
Shimizu, M., Takahashi, J., Ikegami, S., Kuraishi, S., Futatsugi, T., & Kato, H. (2014). Are
pedicle screw perforation rates influenced by registered or unregistered vertebrae in
multilevel registration using a CT-based navigation system in the setting of scoliosis?
European Spine Journal, 23(10), 2211–2217. http://doi.org/10.1007/s00586-014-3512-7
Shimokawa, N., & Takami, T. (2016a). Surgical safety of cervical pedicle screw placement with
computer navigation system. Neurosurgical Review. http://doi.org/10.1007/s10143-016-
0757-0
Shimokawa, N., & Takami, T. (2016b). Surgical safety of cervical pedicle screw placement with
computer navigation system. Neurosurgical Review. http://doi.org/10.1007/s10143-016-
0757-0
Shin, B. J., James, A. R., Njoku, I. U., Hartl, R., & Härtl, R. (2012). Pedicle screw navigation: a
systematic review and meta-analysis of perforation risk for computer-navigated versus
freehand insertion. J Neurosurg Spine, 17(2), 113–122.
http://doi.org/10.3171/2012.5.spine11399
Shin, J. H., Hoh, D. J., & Kalfas, I. H. (2012). Iliac screw fixation using computer-assisted
computer tomographic image guidance: technical note. Neurosurgery, 70(1 Suppl

242
Operative), 16–20; discussion 20. http://doi.org/10.1227/NEU.0b013e318230517a
Shrout, P. E. ., & Fleiss, J. L. (1979). Intraclass correlations: uses in assessing rater reliability.
Psychological Bulletin, 86(2), 420–428.
Smith, H. E., Welsch, M. D., Sasso, R. C., & Vaccaro, A. R. (2008). Comparison of radiation
exposure in lumbar pedicle screw placement with fluoroscopy vs computer-assisted image
guidance with intraoperative three-dimensional imaging. J Spinal Cord Med, 31(5), 532–
537.
Smith, J. D., Jack, M. M., Harn, N. R., Bertsch, J. R., & Arnold, P. M. (2016). Screw Placement
Accuracy and Outcomes following O-Arm-Navigated Atlantoaxial Fusion: A Feasibility
Study. Global Spine Journal, 6(4), 344–349. http://doi.org/10.1055/s-0035-1563723
Smith, Z. A., & Fessler, R. G. (2012). Paradigm changes in spine surgery—evolution of
minimally invasive techniques. Nature Reviews Neurology, 8(8), 443–50.
http://doi.org/10.1038/nrneurol.2012.110
Spiegel, E. A., Wycis, H. T., Marks, M., & Lee, A. J. (1947). Stereotaxic Apparatus for
Operations on the Human Brain. Science (New York, N.Y.), 106(2754), 349–50.
http://doi.org/10.1126/science.106.2754.349
Stefini, R., Peron, S., Mandelli, J., Bianchini, E., & Roccucci, P. (2017). Intraoperative Spinal
Navigation for the Removal of Intradural Tumors: Technical Notes. Operative
Neurosurgery. http://doi.org/10.1093/ons/opx179
Steinmeier, R., Rachinger, J., Kaus, M., Ganslandt, O., Huk, W., & Fahlbusch, R. (2000).
Factors influencing the application accuracy of neuronavigation systems. Stereotactic and
Functional Neurosurgery, 75(4), 188–202. http://doi.org/10.1159/000048404
Sun, H., Lunn, K. E., Farid, H., Wu, Z., Roberts, D. W., Hartov, A., & Paulsen, K. D. (2005).
Stereopsis-guided brain shift compensation. IEEE Transactions on Medical Imaging, 24(8),
1039–1052. http://doi.org/10.1109/TMI.2005.852075
Sundar, S. J., Healy, A. T., Kshettry, V. R., Mroz, T. E., Schlenk, R., & Benzel, E. C. (2016). A
pilot study of the utility of a laboratory-based spinal fixation training program for
neurosurgical residents. Journal of Neurosurgery. Spine, 24(5), 850–6.
http://doi.org/10.3171/2015.8.SPINE15119
Tabaraee, E., Gibson, A. G., Karahalios, D. G., Potts, E. A., Mobasser, J.-P., & Burch, S. (2013).
Intraoperative Cone Beam–Computed Tomography With Navigation (O-ARM) Versus
Conventional Fluoroscopy (C-ARM). Spine, 38(22), 1953–1958.
http://doi.org/10.1097/BRS.0b013e3182a51d1e
Takahashi, J., Hirabayashi, H., Hashidate, H., Ogihara, N., & Kato, H. (2010). Accuracy of
multilevel registration in image-guided pedicle screw insertion for adolescent idiopathic
scoliosis. Spine, 35(3), 347–52. http://doi.org/10.1097/BRS.0b013e3181b77f0a
Tamura, Y., Sugano, N., Sasama, T., Sato, Y., Tamura, S., Yonenobu, K., … Ochi, T. (2005).
Surface-based registration accuracy of CT-based image-guided spine surgery. European
Spine Journal, 14(3), 291–297. http://doi.org/10.1007/s00586-004-0797-y
Tatar, F., Mollinger, J., den Dulk, R., van Duyl, W., Goosen, J., & Bossche, A. (2002).
Measurement position and orientation of surgery tools inside the human body using
ultrasound. In Margineanu (Ed.), International Conference on Optimizatoin of Electrical

243
and Electronic Equipments OPTM (pp. 721–724). Brasov, Romania: Transilvania
University.
Tatsui, C. E., Nascimento, C. N. G., Suki, D., Amini, B., Li, J., Ghia, A. J., … Rao, G. (2017).
Image guidance based on MRI for spinal interstitial laser thermotherapy: technical aspects
and accuracy. Journal of Neurosurgery: Spine, 26(5), 605–612.
http://doi.org/10.3171/2016.9.SPINE16475
Tauchi, R., Imagama, S., Sakai, Y., Ito, Z., Ando, K., Muramoto, A., … Ishiguro, N. (2013). The
correlation between cervical range of motion and misplacement of cervical pedicle screws
during cervical posterior spinal fixation surgery using a CT-based navigation system.
European Spine Journal : Official Publication of the European Spine Society, the European
Spinal Deformity Society, and the European Section of the Cervical Spine Research Society,
22(7), 1504–8. http://doi.org/10.1007/s00586-013-2719-3
Tenhagen, M., Bruse, J. L., Rodriguez-Florez, N., Angullia, F., Borghi, A., Koudstaal, M. J., …
Dunaway, D. (2016). Three-Dimensional Handheld Scanning to Quantify Head-Shape
Changes in Spring-Assisted Surgery for Sagittal Craniosynostosis. Journal of Craniofacial
Surgery, 27(8), 2117–2123. http://doi.org/10.1097/SCS.0000000000003108
Tian, N. F., Huang, Q. S., Zhou, P., Zhou, Y., Wu, R. K., Lou, Y., & Xu, H. Z. (2011). Pedicle
screw insertion accuracy with different assisted methods: a systematic review and meta-
analysis of comparative studies. Eur Spine J, 20(6), 846–859.
http://doi.org/10.1007/s00586-010-1577-5
Tian, W., Weng, C., Liu, B., Li, Q., Sun, Y. Q., Yuan, Q., … He, D. (2013). Intraoperative 3-
dimensional navigation and ultrasonography during posterior decompression with
instrumented fusion for ossification of the posterior longitudinal ligament in the thoracic
spine. Journal of Spinal Disorders & Techniques, 26(6), E227-34.
http://doi.org/10.1097/BSD.0b013e318286ba39
Tjardes, T., Shafizadeh, S., Rixen, D., Paffrath, T., Bouillon, B., Steinhausen, E. S., & Baethis,
H. (2010). Image-guided spine surgery: State of the art and future directions. European
Spine Journal, 19(1), 25–45. http://doi.org/10.1007/s00586-009-1091-9
Uehara, M., Takahashi, J., Ikegami, S., Kuraishi, S., Shimizu, M., Futatsugi, T., … Kato, H.
(2017). Are pedicle screw perforation rates influenced by distance from the reference frame
in multilevel registration using a computed tomography-based navigation system in the
setting of scoliosis? The Spine Journal, 17(4), 499–504.
http://doi.org/10.1016/j.spinee.2016.10.019
Ughwanogho, E., Patel, N. M., Baldwin, K. D., Sampson, N. R., & Flynn, J. M. (2012).
Computed Tomography–Guided Navigation of Thoracic Pedicle Screws for Adolescent
Idiopathic Scoliosis Results in More Accurate Placement and Less Screw Removal. Spine,
37(8), E473–E478. http://doi.org/10.1097/BRS.0b013e318238bbd9
Uneri, A., Stayman, J. W., De Silva, T., Wang, A. S., Kleinszig, G., Vogt, S., … Siewerdsen, J.
H. (2015). Known-Component 3D-2D Registration for Image Guidance and Quality
Assurance in Spine Surgery Pedicle Screw Placement. Proceedings of SPIE--the
International Society for Optical Engineering, 9415. http://doi.org/10.1117/12.2082210
van Herk, M., & Kooy, H. M. (1994). Automatic three-dimensional correlation of CT-CT, CT-
MRI, and CT-SPECT using chamfer matching. Medical Physics, 21(7), 1163–1178.

244
http://doi.org/10.1118/1.597344
Verma, R., Krishan, S., Haendlmayer, K., & Mohsen, A. (2010). Functional outcome of
computer-assisted spinal pedicle screw placement: a systematic review and meta-analysis of
23 studies including 5,992 pedicle screws. Eur Spine J, 19(3), 370–375.
http://doi.org/10.1007/s00586-009-1258-4
Villard, J., Ryang, Y.-M., Demetriades, A. K., Reinke, A., Behr, M., Preuss, A., … Ringel, F.
(2014). Radiation exposure to the surgeon and the patient during posterior lumbar spinal
instrumentation: a prospective randomized comparison of navigated versus non-navigated
freehand techniques. Spine, 39(13). http://doi.org/10.1097/BRS.0000000000000351
Vougioukas, V. I., Hubbe, U., Schipper, J., & Spetzger, U. (2003). Navigated transoral approach
to the cranial base and the craniocervical junction: technical note. Neurosurgery, 52(1),
247–50; discussion 251.
Wagner, S. C., Morrissey, P. B., Kaye, I. D., Sebastian, A., Butler, J. S., & Kepler, C. K. (2017).
Intraoperative pedicle screw navigation does not significantly affect complication rates after
spine surgery. Journal of Clinical Neuroscience, 47, 198–201.
http://doi.org/10.1016/j.jocn.2017.09.024
Wang, M. N., & Song, Z. J. (2011). Classification and Analysis of the Errors in Neuronavigation.
Neurosurgery, 68(4), 1. http://doi.org/10.1227/NEU.0b013e318209cc45
Wang, Y., Xie, J., Yang, Z., Zhao, Z., Zhang, Y., Li, T., & Liu, L. (2013). Computed
tomography assessment of lateral pedicle wall perforation by free-hand subaxial cervical
pedicle screw placement. Arch Orthop Trauma Surg, 133(7), 901–909.
http://doi.org/10.1007/s00402-013-1752-3
Wang, Y., Xie, J., Yang, Z., Zhao, Z., Zhang, Y., Li, T., & Liu, L. (2013). Computed
tomography assessment of lateral pedicle wall perforation by free-hand subaxial cervical
pedicle screw placement. Archives of Orthopaedic and Trauma Surgery, 133(7), 901–9.
http://doi.org/10.1007/s00402-013-1752-3
Waschke, A., Walter, J., Duenisch, P., Reichart, R., Kalff, R., & Ewald, C. (2013). CT-
navigation versus fluoroscopy-guided placement of pedicle screws at the thoracolumbar
spine: single center experience of 4,500 screws. European Spine Journal, 22(3), 654–660.
http://doi.org/10.1007/s00586-012-2509-3
Watanabe, E., Mayanagi, Y., Kosugi, Y., Manaka, S., & Takakura, K. (1991). Open surgery
assisted by the neuronavigator, a stereotactic, articulated, sensitive arm. Neurosurgery,
28(6), 792-9-800.
Watanabe, E., Watanabe, T., Manaka, S., Mayanagi, Y., & Takakura, K. (1987). Three-
dimensional digitizer (neuronavigator): new equipment for computed tomography-guided
stereotaxic surgery. Surgical Neurology, 27(6), 543–7.
Watkins, R. G., Gupta, A., & Watkins, R. G. (2010). Cost-effectiveness of image-guided spine
surgery. Open Orthop J, 4, 228–233. http://doi.org/10.2174/1874325001004010228
Webb, J. E., Regev, G. J., Garfin, S. R., & Kim, C. W. (2010). Navigation-assisted fluoroscopy
in minimally invasive direct lateral interbody fusion: a cadaveric study. SAS Journal, 4(4),
115–121. http://doi.org/10.1016/j.esas.2010.09.002
Wiles, A. D., Thompson, D. G., & Frantz, D. D. (2004). Accuracy assessment and interpretation

245
for optical tracking systems. SPIE Medical Imaging, 421. http://doi.org/10.1117/12.536128
Wong, A. P., Smith, Z. A., Stadler, J. A., Hu, X. Y., Yan, J. Z., Li, X. F., … Khoo, L. T. (2014).
Minimally invasive transforaminal lumbar interbody fusion (MI-TLIF): surgical technique,
long-term 4-year prospective outcomes, and complications compared with an open TLIF
cohort. Neurosurgery Clinics of North America, 25(2), 279–304.
http://doi.org/10.1016/j.nec.2013.12.007
Wood, M. J., & McMillen, J. (2014). The surgical learning curve and accuracy of minimally
invasive lumbar pedicle screw placement using CT based computer-assisted navigation plus
continuous electromyography monitoring - a retrospective review of 627 screws in 150
patients. International Journal of Spine Surgery, 8, 27–27. http://doi.org/10.14444/1027
Wray, S., Mimran, R., Vadapalli, S., Shetye, S. S., McGilvray, K. C., & Puttlitz, C. M. (2015).
Pedicle screw placement in the lumbar spine: effect of trajectory and screw design on acute
biomechanical purchase. Journal of Neurosurgery: Spine, 22(5), 503–510.
http://doi.org/10.3171/2014.10.SPINE14205
Xiao, R., Miller, J. A., Sabharwal, N. C., Lubelski, D., Alentado, V. J., Healy, A. T., … Benzel,
E. C. (2017). Clinical outcomes following spinal fusion using an intraoperative computed
tomographic 3D imaging system. Journal of Neurosurgery: Spine, 1–10.
http://doi.org/10.3171/2016.10.SPINE16373
Xin, W., & Pu, J. (2010). An Improved ICP Algorithm for Point Cloud Registration. 2010
International Conference on Computational and Information Sciences, 565–568.
http://doi.org/10.1109/ICCIS.2010.144
Xu, R.-J., Yan, Y.-Q., Chen, G.-X., Zou, T.-M., Cai, X.-Q., & Wang, D.-L. (2014). A method of
percutaneous vertebroplasty under the guidance of two C-arm fluoroscopes. Pakistan
Journal of Medical Sciences, 30(2), 335–8.
Ying, S., Peng, J., Du, S., & Qiao, H. (2009). A scale stretch method based on ICP for 3D data
registration. IEEE Transactions on Automation Science and Engineering, 6(3), 559–565.
http://doi.org/10.1109/TASE.2009.2021337
Zamorano, L. (1999). The Zamorano-Dujovny multipurpose localizing unit. Advanced
Neurosurgical Navigation, 255–266.
Zamorano, L. J., Nolte, L., Kadi, A. M., & Jiang, Z. (1993). Interactive intraoperative
localization using an infrared-based system. Neurological Research, 15(5), 290–8.
Zeilenhofer, H., Krol, Z., Sader, R., Hoffmann, K., Hogg, M., Schwaiger, M., … Horch, H.
(1997). Multimodal images in diagnostics of head and neck area using efficient registration
and visualization methods. In H. Lemke, M. Vannier, & K. Inamura (Eds.), CAR 97 (pp.
723–728). Amsterdam: Elsevier.
Zhang, W., Takigawa, T., Wu, Y., Sugimoto, Y., Tanaka, M., & Ozaki, T. (2016). Accuracy of
pedicle screw insertion in posterior scoliosis surgery: a comparison between intraoperative
navigation and preoperative navigation techniques. European Spine Journal, 1–9.
http://doi.org/10.1007/s00586-016-4930-5
Zhang, Y.-H., White, I., Potts, E., Mobasser, J.-P., & Chou, D. (2017). Comparison Perioperative
Factors During Minimally Invasive Pre-Psoas Lateral Interbody Fusion of the Lumbar
Spine Using Either Navigation or Conventional Fluoroscopy. Global Spine Journal, 7(7),

246
657–663. http://doi.org/10.1177/2192568217716149