Embed Size (px)
Citation preview
Benjamin Walton, MD Faculty Advisor: Vicente Resto, MD, PhD
The University of Texas Medical Branch at Galveston Department of Otolaryngology
Grand Rounds Presentation August 31, 2010
History
Anatomy
Classification
Reconstructive Techniques Available
TMJ reconstruction
XRT and TMJ reconstruction

Airway Stability
Speech
Deglutition
Mastication The mandible must be able to withstand a
significant amount of force during mastication
Maximal Molar Occlussal Forces of 4346N
Shape and Contour of the Lower Face

Before advanced surgical techniques and improved hardware, disappointing results
Vascularized Bone Grafts disappointing as failures reached 50%
Advances in free tissue transfer including osteocutaneous free flaps have revolutionized mandibular reconstruction
Panje and colleagues introduced successful reconstruction in 1976 with free groin transfer opening the door to further advances
Hardware initially composed of Vitallium (alloy containing cobalt, chromium, and molybdenum
Initial combination of well-vascularized soft tissue reconstruction with recon plates significantly improved short-term results

Long term results of soft tissue reconstruction with recon plates disappointing owing to plate extrusion, plate fracture, and screw loosening

Strongest Facial Bone
U-shaped with horizontal section (body) containing the alveolar process with 2 vertical segments (rami) which through the temporomandibular joints articulate with the skull
Dense cortical structure with small core of spongiosa containing nerves, blood vessels, and lymphatic vessels

Mandible Anatomy Flint: Cummings Otolaryngology:
Head & Neck Surgery, 5th ed.
Alveolar Process contains dental sockets to support teeth
Changes to alveolar process occur throughout adult life, especially after dental extractions
Mental foramen found between inferior border and upper edge of alveolar process at the level of the second premolar tooth

Mandible Anatomy Flint: Cummings Otolaryngology:
Head & Neck Surgery, 5th ed.

Rami composed of broad, thin plates of dense bone
Each joins with body to form angle of mandible
Anteriorly ends in the coronoid and condylar processes
Inferior Alveolar Nerve passes through the Mandibular Foramen into the Alveolar Canal

Mandible Anatomy Flint: Cummings Otolaryngology:
Head & Neck Surgery, 5th ed.

Dependent primarily on 2 groups of muscles Depressor-Retractor Group
Geniohyoid
Digastric
Elevator Group
Masseter
Medial Pterygoid
Temporalis

Medial Pterygoid inserts on inner surface at mandible angle while Masseter inserts on outer surface
Angulation of attachment at the angle more favorable for the medial pterygoid
Medial pterygoid overpowers masseter in segmental defects causing typical displacement patterns inward

Lateral Pterygoid and Mylohyoid have minor influences on the movement of the mandible
Lateral Pterygoid- attaches to the neck and pulls anteriorly and medially

Ablative Surgery for Benign or Malignant Neoplastic tumors Often associated with soft-tissue defect
Trauma
Osteoradionecrosis
Bisphosphonate-induced osteonecrosis
Osteomyelitis

Various Classification Schemes HCL (Boyd and colleagues classification)
H defects are lateral defects of any length up to midline including condyle
L defects lateral excluding the condyle C defects involve central segment containing 4
incisors and 2 canines 3 lower case letters describe soft tissue component o – no skin or mucosa
s – skin
m – mucosa
sm – skin and mucosa

Boyd and Colleagues Classification
P. Maurer et al. / British Journal of Oral and Maxillofacial Surgery 48
(2010) 100–104

Urken et al Classification Based on functional considerations caused by
detachment of different muscle groups and difficulties with cosmetic restoration
C – condyle
R – ramus
B – body
S – total symphysis
SH – hemisymphysis

Urken et al Classification Mehta and Deschler
Mandibular reconstruction in 2004 289

Accurate Classification of defect and understanding of functional deficits
Restore Form and Function Restore Bony Contour of native mandible
Restoration of Mastication
Greater then loss of tongue volume, greater negative impact on patient’s prognosis for recovery of oral function
Deglutition
Articulation
Maintenance of adequate airway

Alloplastic implants
Vascularized free tissue transfer
Adjuvants to vascularized osseous free tissue transfer

Most commonly used are bone plates and screws
Indicated in patients with poor performance status or where soft-tissue defects of the oral cavity/oropharynx are more extensive than bony mandibular defect.
Innovation in self-drilling, self-tapping screws and locking miniplates assist in microvascular reconstruction
First reconstruction plate with mechanism for osseointegration at the bone-to-screw interface
Locking mechanism at screw-to-plate interface
Found to be superior to solid screw steel and titanium plates
Recent studies comparing THORP to vascularized bone grafts show significant delayed complications of hardware extrusion

Fibular Free Flap
Scapular Free Flap
Iliac Crest Free Flap
Radial Forearm Free Flap
Double Flap Reconstruction


Workhorse of mandibular reconstruction
Used to reconstruct bony defects as long as 30cm in length
Vascular pedicle may be 6-10 cm in length
Allows placement of osseointegrated dental implants
Only donor site that allows reconstruction of total mandibular defects
Based on the Peroneal Artery and Vein
Harvested with the Flexor Hallucis Longus Muscle
Skin Island can be used both intraoral and Externally
Can harvest up to 27cm of bone
Receives both segmental and intraosseous blood supplies allowing for multiple osteotomies
Position allows for simultaneous dissection
Small Defects (<5cm) can be primarily closed

Limited in amount of soft tissue that can be transferred
Skin island thought to be “unreliable”
Does not recreate alveolar height of native dentate mandible
Donor site generally minimal IF 7-8cm of bone at ankle and 3-4 cm of bone at knee are preserved
Most patients return to full ambulation in 2 months
Evaluation of lower extremity vasculature recommended to assess disease precluding transfer
MR angiography recommended and has replaced conventional angiography

Fibular Free Flap (continued) M. Bak et al. / Oral Oncology 46
(2010) 71–76
Cohort Study involving 30 patients Donor site closure remains somewhat
controversial with most advocating split-thickness skin graft from secondary donor site
STSG site often adds to pain and poses potential for addition morbidity
Purposes of study to examine donor site morbidity in patients undergoing fibula free flap reconstruction where skin graft taken from cutaneous paddle of the fibula

September 1, 2006 to March 30, 2007
30 patients included in study from 2 institutions
15 men and 15 women with mean age of 58 (range 19-88 years)
All underwent fibula free flap harvest with STSG (thickness 0.04cm)

Flap Failure
Hardware complications
Intraoral complications
Need for additional surgery

14 donor sites from the right leg
16 donor sites from the left leg
Average STSG thickness 0.04 cm with area of 16x6cm
26 patients with viable skin grafts at follow up (87%)
4 (13%) with partial loss (range of 15-50% of graft)
0 were completely lost
Primary Tumors composed of 20 squamous cell carcinoma (67%)
6 mucoepidermoid carincoma (20%)
2 osteosarcoma (7%)
1 mandibular osteoradionecrosis (3%)
1 osteomyelitis (3%)

6 major sites of soft tissue defect Floor of mouth (12 tumors, 40%)
Mandibular alveolar ridge (8 tumors, 27%)
Base of tongue (3 tumors, 10%)
Parotid (3 tumors, 10%)
Oral tongue (2 tumors, 7%)
Pharynx (2 tumors, 7%)
Average flap ischemia time 2 hours, 38 minutes (range of 1 hour 45 minutes to 4 hours); did not contribute significantly to outcome measures
One skin paddle necrosis requiring surgical debridement (patient seropositive for HIV with post-operative Streptococcus infection
2 patients with orocutaneous fistulas managed conservatively with dressing changes
1 patient with adhesion formation between base of tongue and tonsil defect requiring adhesion lysis with placement of STSG

Inraoperative and Post-operative pictures
Kim et al, Arch Otolaryngol Head Neck Surg/Vol 134 (No12), Dec 2008

Post-operative minor fistula rate was 7% No major fistulas requiring flap or other
surgical interventions 17 (57%) of patients in study required post-
operative radiation therapy (1 of 2 patients in study with fistula formation)
Complication of procedure involved patient with opposing defects, developing post-operative adhesions requiring additional surgery – authors recommend that in defects involving opposing surfaces, epithelialized tissue should be used
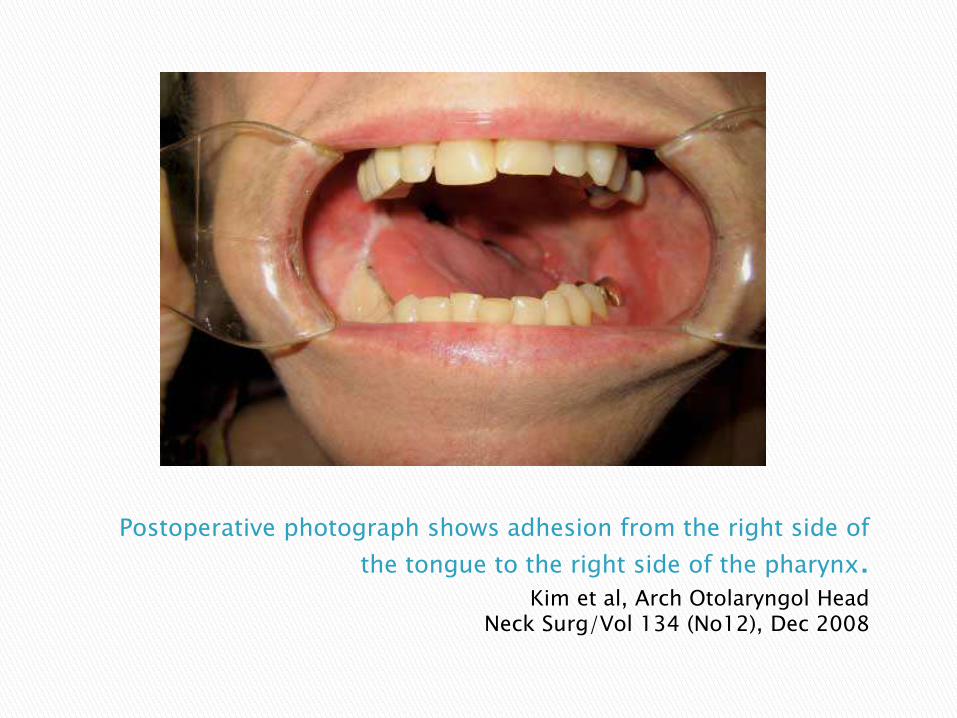
Postoperative photograph shows adhesion from the right side of
the tongue to the right side of the pharynx. Kim et al, Arch Otolaryngol Head
Neck Surg/Vol 134 (No12), Dec 2008

Flap based on Circumflex Scaplular Artery and Vein
Vessels of good length and diameter
Provides up to 14 cm of bone but of poor quality generally
Large, well vascularized skin island with moderate bulk
Can be osteotomized safely
Cannot be performed simultaneously with ablative procedure

Good choice of through and through defects involving facial skin, bone, and mucosa
Many recommend it’s use in recurrent parotid malignancies requiring cheek skin and ascending ramus resection
Can accept osseointegrated dental implants
Especially useful in setting of salvage surgery after Chemo/XRT failure due to ability to include latissmus dorsi muscle used to cover major vasculature in neck
Preferred by some for geriatric patient due to ability to ambulate early after surgical resection

Decreased range of motion of shoulder
Difficult for 2 team approach
Limited in amount of bone harvestable

Scapular Free Flap M. Bak et al. / Oral Oncology 46
(2010) 71–76
One time, workhorse of mandible reconstruction
Blood supply based on Deep Circumflex Iliac Artery
Vessels are generally short and of small diameter
Can harvest large quantity of bicortical bone

Supplies bone with height comparable to native dentate mandible
Contoured to fit most segmental mandibular defects
Can harvest internal oblique muscle by including ascending branch of DCIA

Iliac Crest Free Flap M. Bak et al. / Oral Oncology 46
(2010) 71–76
Bone lacks segmental perforators
Skin Island Unreliable and often provides too much bulk
Donor Site Morbidity Numbness to Anterior Hip Region
Complications include Hernia of the internal oblique muscle

Hidalgo et al completed 10-year follow up study
Found acceptable aesthetic outcomes in 90% of patients
70% of patients were eating regular diet while rest of patients in study remained on soft diet
More than 90% of bone height was preserved
Study often cited most for efficacy of free-flap reconstruction of mandible defects

Temporary Intraoperative External Fixation Aids in maintaining the preoperative three-dimensional
relationships Commonly done with bridging reconstruction bar or use of
arch bars and intermaxillary fixation
Periosteal Free Flaps Fascioperiosteal radial forearm free flap Used to enhance survival of iliac crest corticocancellous
autograft Kelley et al (2003) found osteogenic capacity of periosteal
tissues
Osseointegrated Dental Implants Require bone height of approximately 6 to 7mm Found to work identically to implants on native bone Must delay placement for at least 6 months if receiving
postoperative radiation

Used to reconstruct partial mandibular defects from small segmental resections
Not used when soft tissue defects are present
Advocated only in uses of small, partial or segmental mandibular defects
Often cancellous bone chips Autogenous bone chips often taken from iliac crest
No mucosal or soft-tissue defects
Should never be used in patient’s undergoing radiation therapy as results have been poor with many complications

Reconstruction techniques involving the condyle are controversial
Oral competence, tongue and laryngeal mobility not significantly affected
Reconstruction of TMJ and condyle is usually disappointing

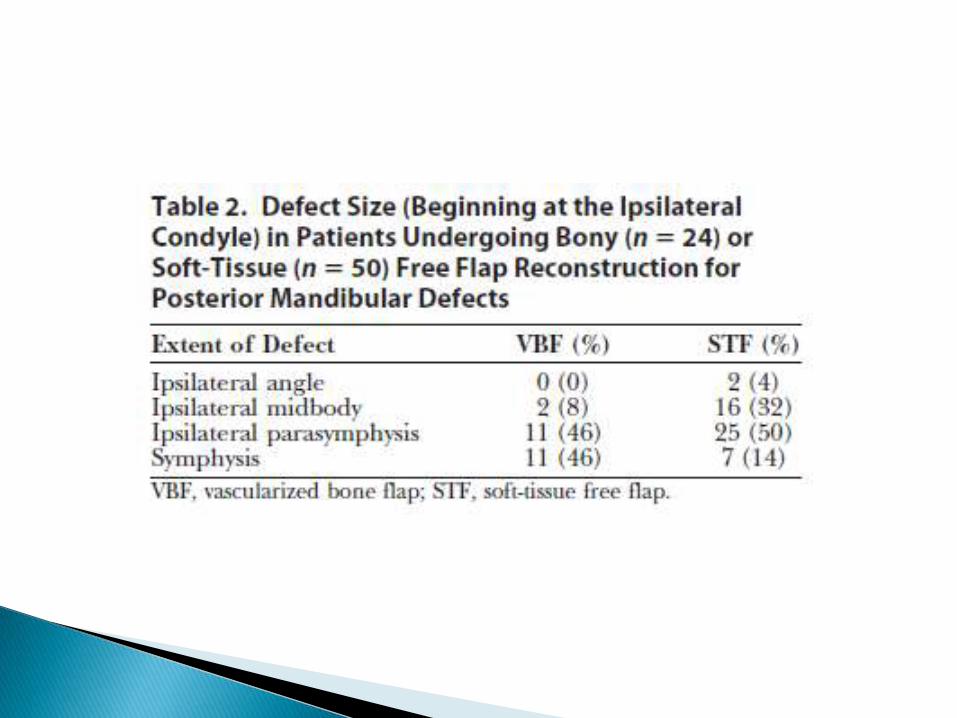
Prospective Trial of 74 patients (45 men and 29 women) undergoing microvascular free flap reconstruction at UT Houston
Compared outcomes between vascularized bone flap and soft tissue free flap reconstruction
Posterior mandible defect defined as one that includes at least the condyle and ramus up to angle

Age
Tobacco Use
Medical comorbities
Dentition
History of Preop or Postop Radiation and chemotherapy
Details of defect and reconstruction
Perioperative complications
Post-operative diet Post-operative mouth
opening ASA class Kaplan-Feinstein
classification Mouth Opening Crossbite





Time to oral intake, postoperative diet and mouth opening similar between 2 groups
Degree of cross-bite sole functional outcome difference (0 to 6mm in vascularized bone flap group and 0 to 16mm in soft-tissue free flap)
Advanced age, higher ASA class, and Kaplan-Feinstein classification biased toward soft-tissue free flap reconstruction
Oncologic prognosis did not affect reconstructive technique
Presence of natural or prosthetic teeth influences ability to have regular mechanical vs. soft or pureed diet


Disarticulation resection results in complex deformity that can affect facial appearance and oral function
Options are limited
Reconstruction plates with attached metallic condylar prostheses
Autogenous rib grafting
Cadaveric mandibles
Vascularized Tissue Transfer
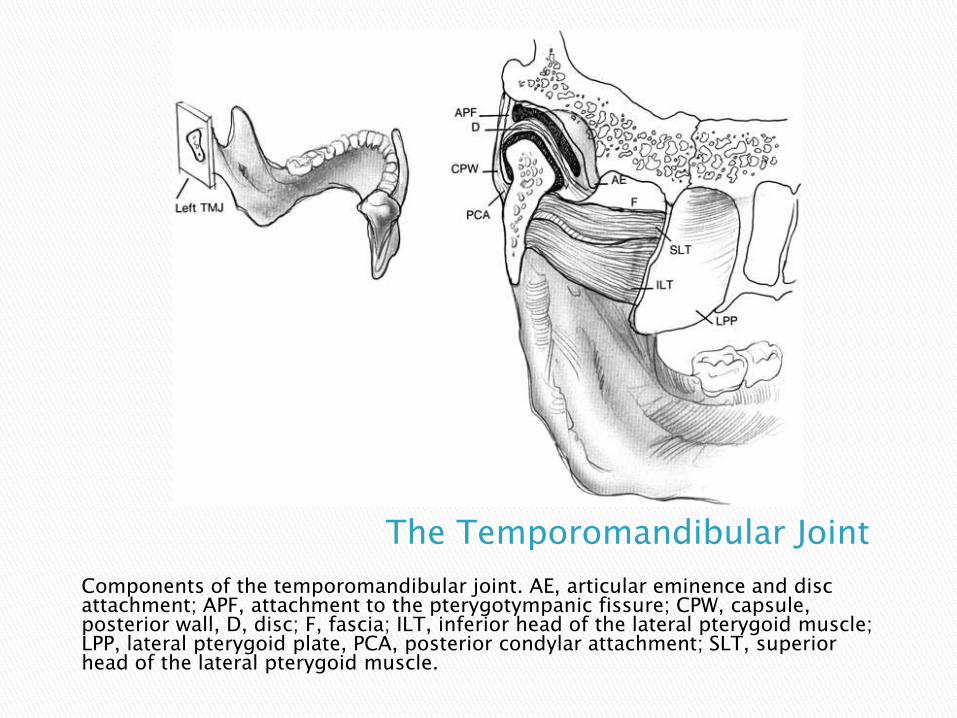
The Temporomandibular Joint
Components of the temporomandibular joint. AE, articular eminence and disc attachment; APF, attachment to the pterygotympanic fissure; CPW, capsule, posterior wall, D, disc; F, fascia; ILT, inferior head of the lateral pterygoid muscle; LPP, lateral pterygoid plate, PCA, posterior condylar attachment; SLT, superior head of the lateral pterygoid muscle.
Alloplastic materials first reported by Gordon in 1955
Rationale was to use implant to maintain functional mandibular ramus height, avoid malocclusion, and prevent hypomobility
Condylectomy without reconstruction would result in facial deformity, pain, and limitation of movement

Case Series and Literature Review
4 patients from September 1989 to April 1995
Underwent condylar reconstruction with metallic condylar prostheses after hemimandibulectomy
Three patients required reconstruction for retromolar trigone squamous cell carcinoma
1 received pre-operative radiation therapy
2 received post-operative radiation therapy
One patient required reconstruction for Ewing’s sarcoma

Post-operative follow-up with special attention toward complications
Mean follow-up of 23.3 months (5-37 months)
Cross-bite deformity and malocclusion (n=1)
Infection (n=2)
Transient Facial Nerve Paralysis (n=1)

An axial computed tomogram of the temporal bones shows
extension of a prosthesis into the epitympanum, abutting the ossicular chain.
Also, bony destruction exists medially from the epitympanum to the cochlea.
1 patient with migration of prosthesis into epitympanum
Caused otorrhea, Profound SNHL due to bony destruction of cochlea, and transient facial nerve paralysis

Patient with exposed bar 5 months after placement.
Exposure or Extrusion of prosthesis in the 3 patients with radiation exposure

Metallic condylar prosthesis in settings of tumor resection and reconstruction involve significant risks and potential complications
Do not offer satisfactory results
Authors suggest vascularized bone grafting when possible

Single Surgeon’s experience retrospectively reviewed
82 patients from January 1987 to December 1990
Mean length of follow-up of 11 years
Mean patient age of 48 years
Examined many aspects including aesthetics, return to diet

Condyle can be resected and fixed to the end of the free-flap bone graft
These grafts can last for over a decade 2 patients where nonvascularized condyle
failed Advocates the use of nonvascularized graft
when specimen transection is planned at the midramus or higher
Superior alternative to no reconstruction, shaping the end of the graft, or using a prosthetic condyle
12 of 20 patients received full radiation therapy following mandible resection and primary reconstruction
Shown to not delay healing of osteotomies or to compromise bone graft viability
Osseointegrated dental implants were not placed in these patients

Metallic Implants Christensen implant Titanium-coated Hollow-screw Reconstruction
Plate (THORP)
Silicone Rubber (Silastic) Proplast Polytef (Teflon) Autogenous Materials
Temporalis muscle/fascia flap Osteochondral rib grafts Vascularized bone grafts
In use for more than 25 years
Comprises metal fossa and metal condyle with articulating dome of polymethylmethacrylate
Has been successful in severe TMJ disorders
Polymethylmethacrylate can cause fibrosis, neo-ossification or heterotrophic bone formation
Can create patient-specific TMJ prosthesis

Christensen implant Courtesy TMJI, INC. accessed on
http://www.tmj.com/products/tmj_total_custom.php
on 8/29/2010
Raveh et al reported successful reconstruction in 2 patients
Major advantages: Stable anchorage of carrier plate to mandible by hollow
screws 3-dimensional adaptability of condylar prosthesis after
fixation to mandible
Allows condyle to articulate with glenoid fossa reproducing normal rotational and translational movement
Advent of osteointegrating screws that lock to plate has reduced risk of loosening hardware

Kim and Donoff used reconstruction plates to reconstruct mandibular condyle and ramus in 13 patients
1 patient required revision or plate removal secondary to infection
Majority of plate losses secondary to patients undergoing irradation which is often necessary in advanced stage cancers requiring mandibulectomy

23 TMJ arthroplasties using metallic condylar prostheses, 9 for malignant tumors
Average follow-up of 25 months
Clinical and Radiographic follow-up study
Reconstruction plate including condyle (AO/ASIF reconstruction plate, Stratec Medical)
Radiographic evaluation included Panorex and Towne view, also used other modalities when clinically relevant
9 patients required reconstruction secondary to malignant tumors
Three plates required removal secondary to infection (two cases) or necrosis of the pectoral flap (one case)
Plate fractured in 1 patient requiring exchange
Three patients died during follow-up (2 patients had functional alloplastic joint)
Condyle displaced in 4 cases
Two cases of bony erosion into the skull base
Heterotrophic new bone formation in four joints


Tumor patients can benefit from condylar prosthesis for reconstruction
Special anatomic and functional conditions in the region of the TMJ articulation indicate using autogenous materials whenever possible

Temporary or Permanent Facial Nerve Weakness Middle Ear infections Temporary or Permanent hearing loss Tinnitus Disequilibrium Malocclusion Infection Extrusion or exposure of the prosthesis Adhesions or ankylosis within the joint space Heterotrophic bone formation Bony erosion of the skull base Foreign body reaction Rejection of the implant

Plate exposure is most common cause of reconstructive failure
Increased incidence in patients requiring extensive soft tissue resection or radiation therapy
Some authors have expressed concern with titanium plates as they potentionally can cause hot spots contributing to overlying skin breakdown
Proplast, polytef (Teflon), and Silastic known to cause severe foreign body giant cell reaction
Can cause soft tissue and bony destruction
Migration of microparticulate debris to other areas
Implants no longer indicated in condylar reconstruction
Free bone grafts, especially the osteochondral rib graft, often susceptible to unpredictable resorption, and often insufficient for reconstruction of ramus and body
Vascularized bone grafts effective Resistant to infection and extrusion
Can survive in poor recipient bed from prior irradiation
Fibular free flap and iliac crest have best functional and aesthetic results
Can restore bony and soft tissue defects in one procedure
3 techniques available Addition of condylar prosthesis to the flap
Addition of resected condyle to the flap
Placement of distal portion of flap directly into glenoid fossa
Condylar prosthesis has many complications involved
Addition of native condyle often not possible

Case report of 33 y/o M with left odontogenic keratocyst
Fibula free flap used to reconstruct condyle
Distal end of the fibula free flap was rounded allowing it to seat passively against TMJ disc in glenoid fossa
Masseter muscle sutured to angle of reconstruction plate to actively seat the “neocondyle” into the fossa

Application of fibula free flap to reconstruct the left mandible as seen on panorex 4 weeks postoperatively
Engroff, OOOOE, December 2005,663
Hidalgo shown that condyle as free graft to flap is a viable alternative
Fibula well-suited for reconstruction of condyle
Tubular in shape and densely cortical
Narrow shape allows fit through the soft tissue tunnel avoiding dissection around the facial nerve
Several studies have shown success in this technique
Guyot et al reported 11 patients followed over 6 years, oral function was preserved with no cases of ankylosis

Mandibular Reconstruction poses a specific challenge in both functionality and aesthetics
There are many options available, each with its own risks and benefits
The fibula free flap has become the workhorse of mandible reconstruction
The condyle and TMJ remain surgical challenges in tumor reconstruction
Free tissue transfer has been proven to be the most beneficial

Radiation, both pre-operatively and post-operatively, increases risks involved with mandibular reconstruction
Limited evidence in radiation and TMJ reconstruction
Metallic prostheses have many complications when involved in tumor reconstruction
Further work remains in developing a standard reconstruction of the condyle and TMJ
Lindqvist C, Soderholm AL, Hallikainen D, Sjovall L. “Erosion and Heterotopic Bone Formation after alloplastic temporomandibular joint reconstruction.” J Oral Maxillofac Surg. 1992;50:942-949
Patel A, Maisel R. “Condylar Prostheses in Head and Neck Cancer Reconstruction.” Arch Otolaryngol Head Neck Surg. 2001;127:842-846
Daniel E, Browne D. “Minimizing Complications in the use of Titanium Condylar Head Reconstruction Prostheses.” Otolaryngolog-Head and Neck Surgery. 2004;130:344-350
Hanasono M, Zevallos J, Skoracki R, Yu P. “A Prospective Analysis of Bony versus Soft-Tissue Reconstruction for Posterior Mandibular Defects.” Plastic and Reconstructive Surgery. 2010;125:1413-1421
Engroff S. “Fibula Flap Reconstruction of the Condyle in Disarticulation Resections of the Mandible: A case report and review of the technique.” Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100:661-665
Hidalgo DA, Pusic AL. “Free-flap Mandibular Reconstruction: a 10-year follow-up study.” Plast Reconstr Surg. 2002;110:438-449
Hundepool AC, Dumans AG, Hofer SOP, Fokken NJW, Rayat SS, van der Meij EH, Schepman KP. “Rehabilitation after Mandibular Reconstruction with the Fibula Free-Flap: Clinical Outcome and Quality of Life Assessment.”Int. J. Oral Maxillofac. Surg. 2008;37:1009-1013

Bak M, Jacobson AS, Buchbinder D, Urken ML. “Contemporary Reconstruction of the Mandible.” Oral Oncology. 2010;46:71-76
Head C, Alam D, Sercarz JA, Lee JT, Rawnsley JD, Berke GS, Blackwell KE. “Microvascular Flap Reconstruction of the Mandible: A Comparison of Bone Grafts and Bridging Plates for Restoration of Mandibular Continuity.” Otolaryngology-Head and Neck Surgery. 2003;129:48-54
Mehta RP, Deschler DG. “Mandibular Reconstruction in 2004: An Analysis of Different Techniques.” Current Opinion in Otolaryngology & Head and Neck Surgery. 2004;12:288-293
Shockley WW, Weissler MC, Pillsbury HC. “Immediate Mandibular Replacement Using Reconstruction Plates.” Arch Otolaryng Head Neck Surg. 1991;117:745-749
Maurer P, Eckert AW, Kriwalsky MS, Schubert J. “Scope and Limitations of Methods of Mandibular Reconstruction: A Long-Term Follow-Up.” British Journal of Oral and Maxillofacial Surgery. 2010;48:100-104
Kim PD, Fleck T, Heffelfinger R, Blackwell KE. “Avoiding Secondary Skin Graft Donor Site Morbidity in the Fibula Free Flap Harvest.” Arch Otolargol Head Neck Surg. 2008;134:1324-1327
Holt GR. “Grafts and Implants in Facial, Head, and Neck Surgery.” Head & Neck Surgery – Otolaryngology. Bailey BJ and Johnson JT, 2006; Philadelphia, PA.
Nussenbaum B, “Reconstruction of the Mandible.” Flint: Cummings Otolaryngology: Head & Neck Surgery, 5th ed. 2010.
Cordeiro PG, Santamaria E, Disa JJ. “Mandible Reconstruction.” Atlas of Head and Neck Cancer. 358-375

















![Current Advances in Mandibular Condyle Reconstruction · The LIPUS is considered the preferred method of mechanical stimulation, also known as “preferred bioreactor” [25]. 5](https://img.dokumen.tips/doc/110x75/5e96a9d67ba2de640562addd/current-advances-in-mandibular-condyle-reconstruction-the-lipus-is-considered-the.jpg)











