Embed Size (px)
Citation preview

Jeffrey J. Popma, MD
Director, Innovations in Interventional Cardiology
Senior Attending Physician
Beth Israel Deaconess Medical Center
Associate Professor of Medicine
Harvard Medical School
Boston, MA
Medtronic CoreValve
US Pivotal Trial:Design Considerations and Perspectives:

Nitinol: Selected for its shape recovery after
percutaneous delivery chronic outward force for
stabilization and conformability to anatomy
Nitinol Characterization:
Specifications and Testing
• Radial Force, Fatigue
Physiology: Understanding the in-vivo
Environment
• Aortic compliance
• In-vivo pressures
FEA Modeling And Device Design:
Functional and Safety Verification
• Operational Stresses
• Fatigue and Durability
Frame Durability Proof Test

CoreValve Global Clinical Experience
18 Fr. CVSS&E Study
CE Marking
EER
(Post-CE
Mark)
Australia
New Zealand
Trial
Published Single-
Center Experience
Munich
(Lange)1
Siegburg
(Grube)2
Dates 5/06 – 6/07 4/08 – 11/08 4/07 – 12/08 8/08 - Ongoing 6/07 – 8/08 5/06 – 3/08
Patients (n) 112 14[a] 1,424 Up to 150 137 102
Logistic
EuroSCORE23.1 13.4 25.7 17.1 22.6 13.9 17.6 13.3 24.3 14.9 24.5 15.4
STS Score Not collected 17.7 12.3 Not collected Being collected 23.4 10.1 8.6 4.7
Adjudicated Yes Yes No Yes No No
1. Bleiziffer, et al. Eur J Cardiothorac Surg 2009 Apr;35(4):615-20
2. Grube, et al. Circ Cardiovas Intervent. 2008;1:167-175
Is percutaneous AVR comparable to surgical AVR in
“high-risk” patients Requires RCTs

18F Safety/Efficacy: Long-Term Survival
28.2% 12 Mo Mortality
15.2% 30 Day Mortality
Serruys TCT 2009
What is the mortality risk for
surgical outcome in comparable
“high-risk” patients?

No.
Pts
Included
CABG
30 Day
Mortality MI Stroke
Reop for
Bleeding PPM
Pulm
Compls
Renal
Failure LOS, d
Prior CABG
Akins , 2004 89 Yes 6.7% 1.1% 4.5% 5.6% 4.5% 9% 11.2% 8
Byrne , 2002 94 Yes 6.4% 7% 11% 3% 7% 7% 2% NR
Fighali , 1995 104 Yes 14% 13% 11% 28% NR NR 11% NR
Elderly (≥ 80 years)
Chiappini , 2004 115 Yes 8.5% 3.8% 1% NR 3.4% NR NR NR
Collart , 2005 215 Yes 8.8% NR NR 6% 6.0% 10.7% 8.8% 14
De Vincentiis ,2008 345 Yes 8.5% NR NR 2% NR 2.7% 4% NR
Gilbert , 1999 103 Yes 18.4% NR 17% 4% 11% NR 12% NR
Kolh , 2007 220 Yes 13% 4% 2% 4% 5% 21% 5% 17.6
Melby , 2007 245 Yes 9% 1% 3% 9% NR 22% 12% 9
Sundt , 2000 133 Yes 11.1% < 1% 3.8% 10.5% NR 26.3% 11.3% 14.7
Thourani , 2008 88 No 5.7% 0 3.4% 6.8% 2.3% NR 4.6% 9.8
“High-Risk” Surgical AVR OutcomesCoreValve
US Pivotal

No.
Pts
Include
CABG
30 Day
Death MI Stroke
Reop for
Bleeding PPM
Pulm
Compls
Renal
Failure LOS, d
Elderly ≥ 70 yr
Tseng, 1997 247 No 6.1% < 1% 2.0% 3.2% NR NR 2.0% 15.1
Bloomstein,2001 180 No 16.7% NR NR NR NR NR NR NR
Euroscore >7
Grossi, 2008 731 No 7.8% 0 3.7 3.6 NR 10.8% 4.2% NR
Reduced LVEF
Powell, 2000† 55 Yes 18% NR NR NR NR NR NR NR
Connolly, 2000†† 52 Yes 21% NR NR NR NR NR NR NR
Tarantini, 2003†† 52 Yes 8% NR NR NR NR NR NR NR
Clavel 2008†††† 44 Yes 18% NR NR NR NR NR NR NR
“High-Risk” Surgical Outcomes
† LVEF < 30% †† LVEF < 35% †††† LVEF <% 40
CoreValveUS Pivotal

sAVR Outcomes in High Risk Patients
30-Day
MortMI Stroke
Bleeding
Re-opPPI
Pulm
Comp.
Renal
FailureLOS, d
Mean 11.3% 5.0% 5.7% 7.1% 5.6% 13.7% 7.3% 12.6
High 5.7 1.0 2.0 2.0 2.3 2.7 2.0 8.0
Low 21.0 13.0 11.0 28.0 11.0 26.3 12.0 17.6
sAVR in high risk patients:Prior CABG, > 80 yrs, > 70 yrs, high-risk, and LEVF < 40%.

Mortality # 6 mo 12 mo 18 mo 24 mo 36 mo 60 mo To, 2008 26 22% 36% 62%* 69%
Sack, 2008 75 30% 40%
Shareghi, 2007 80 25%* 44% 66% 63%* 71%
Klein, 2006 78 62% 69% 69% 80% 86%
Agarwal, 2005 212 36% 48% 53% 72% 86%
Lieberman, 1995 165 39% 45% 59% 75%
Otto, 1993 674 45% 65% 77%
Kuntz, 1992 219 16%* 25% 33%* 40% 43%*
O'Neill, 1991 492 44%* 36%
Kuntz, 1991 205 17%* 25% 34%* 40% 47%*
Ferguson, 1990 68 17% 30%** 33%* 37%*
Brady, 1989 26 32%
Berland, 1989 55 30% 40% 45%
Sherman, 1989 36 28% 55%
Safian, 1988 170 29% 36%
Block, 1988 90 28%
Meta-analytic
mortality rate2671 21.1% 37.4% 42.9% 56.1% 69.6% 86%
Inoperable: Mortality Following BAVCoreValve
US Pivotal
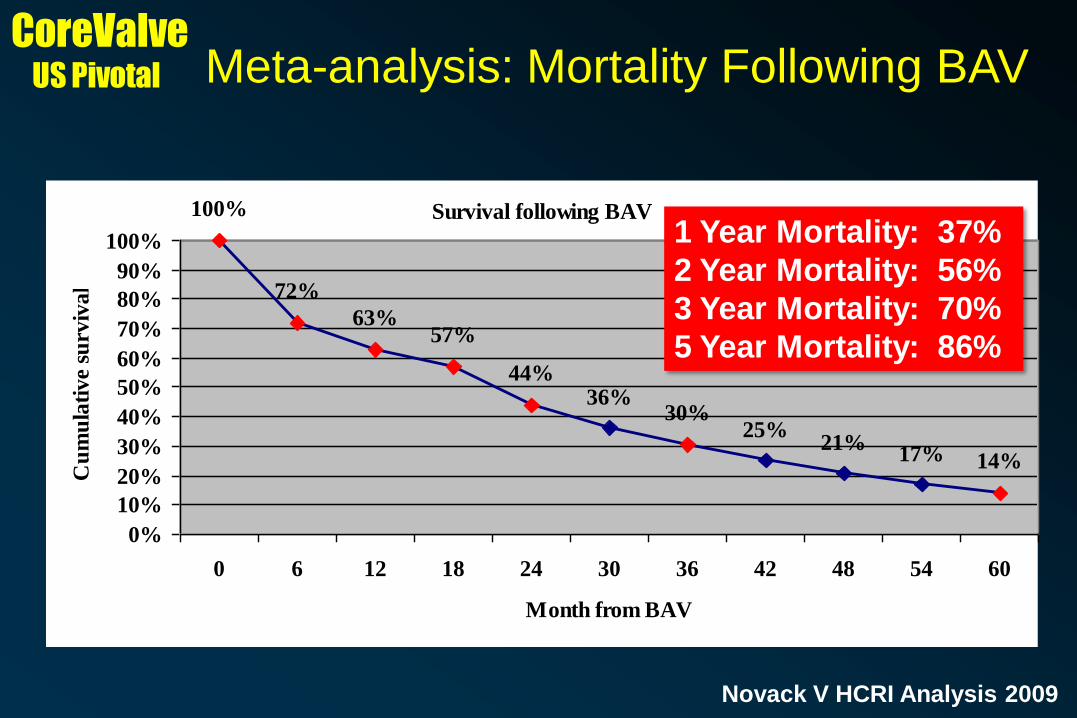
Survival following BAV100%
72%
63%57%
44%36%
30%25%
21%17% 14%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 6 12 18 24 30 36 42 48 54 60
Month from BAV
Cu
mu
lati
ve
surv
iva
lMeta-analysis: Mortality Following BAV
Novack V HCRI Analysis 2009
CoreValveUS Pivotal
1 Year Mortality: 37%
2 Year Mortality: 56%
3 Year Mortality: 70%
5 Year Mortality: 86%

Ongoing Design Discussions
Disclaimer: Discussions are ongoing with the
FDA relating to the final trial CoreValve US
Pivotal trial design.
The purpose of this presentation is to outline the
ongoing considerations for evaluation of the
Medtronic CoreValve device in patients with
severe aortic stenosis who are at “high-risk” or
inoperable for conventional aortic valve
replacement surgery
CoreValveUS Pivotal

DEVICE
DESCRIPTION
The CoreValve ReValvingTM System is an 18F percutaneous
aortic valve consisting of a porcine pericardial valve constructed
on a self-expanding Nitinol frame housed within a percutaneous
delivery catheter.
SPONSOR Medtronic CardioVascular, , Mounds View, MN
STUDY DESIGN Subjects will be randomized to either percutaneous aortic valve
replacement (PAVR) with the study device or to surgical aortic
valve replacement (SAVR).
STUDY
PURPOSE
To evaluate the safety and efficacy of the CoreValve ReValving
System in the treatment of severe symptomatic aortic stenosis
in subjects who have a predicted high risk for heart surgery.
INDICATIONS
FOR USE
The CoreValve ReValving™ System is indicated for use in
subjects with Aortic Stenosis (AS) necessitating valve
replacement who are considered poor surgical candidates with
high surgical risk (STS score ≥ 8 and/or elevated perioperative
mortality risk of ≥15%).
Study ObjectivesCoreValve
US Pivotal

CoreValve sAVR
PI: Jeffrey J. Popma, MD; David Adams, MD
~30-50 sites
United States
Primary Endpoint: 12 month all cause mortality
30d 6mo 4yr3yr2yr9mo 12mo8mo 5yr
All Cause Mortality
Symptomatic patients with severe aortic
stenosis deemed “high risk” for sAVR
Proposed “High-Risk” Randomized ArmCoreValve
US Pivotal

• Subject has senile symptomatic (NYHA Functional Class ≥ II)
degenerative aortic valve stenosis with mean gradient > 40 mmHg
and/or jet velocity greater than 4.0 m/s, or an initial aortic valve
area of ≤ 0.8 cm2 (or AVA index ≤ 0.5 cm2/M2) by echocardiogram
• Subject must have co-morbidities such his/her predicted high risk
for surgery as determined by an STS score ≥ 8%, or have
predicted peri-operative mortality risk of ≥ 15% determined by two
independent cardiac surgeons
• The subject or the subject's legal representative has been
informed of the nature of the study, agrees to its provisions and
has provided written informed consent
“High Surgical Risk”: Inclusion CriteriaCoreValve
US Pivotal

• Evidence of an acute myocardial infarction ≤ 30 days before the
intended treatment.
• Any percutaneous coronary interventional procedure performed
within 30 days prior to the index procedure with bare metal stents
and 6 months with drug eluting stents.
• Blood dyscrasias as defined: leukopenia (WBC < 1000mm3),
thrombocytopenia (platelet count <50,000 cells/mm3), history of
bleeding diathesis or coagulopathy, or hypercoagulable states.
• Untreated clinically significant coronary artery disease requiring
revascularization.
• Cardiogenic shock manifest by low cardiac output, pressure
dependent, or mechanical hemodynamic support.
“High-Risk” Clinical Exclusion CriteriaCoreValve
US Pivotal

• Need for emergency surgery for any reason.
• Severe ventricular dysfunction with LVEF < 20%.
• Subject has been offered surgery but declined.
• Recent (within 6 months) cerebrovascular accident (CVA) or
transient ischemic attack (TIA).
• End stage renal disease requiring chronic dialysis or creatinine
clearance < 15 cc/min.
• Active peptic ulcer or GI bleeding within the past 3 months.
• A known hypersensitivity or contraindication to aspirin, heparin,
nitinol (titanium and nickel alloy), both ticlopidine and clopidogrel,
or sensitivity to contrast media, which cannot be adequately pre-
medicated.
“High-Risk” Clinical Exclusion CriteriaCoreValve
US Pivotal

• Subject refuses a blood transfusion.
• Life expectancy < 12 months due to associated non-cardiac co-
morbid conditions.
• Other medical, social, or psychological conditions that in the
opinion of an Investigator precludes the subject from appropriate
consent.
• Currently participating in an investigational drug or another
device study.
“High-Risk” Clinical Exclusion CriteriaCoreValve
US Pivotal

• Access Site– Artery diameter– Tortuosity– Lesions– Calcification
• Abdominal and thoracic aorta
• Native valve anatomy– Annulus diameter – Valve/Aorta angulation– Valve Calcifications – Sinus dimensions– Sino-tubular junction– Ascending aorta
“High Risk” Anatomic Exclusion CriteriaCoreValve
US Pivotal

• Native aortic annulus size ≤ 20 mm or > 27 mm
• Pre-existing prosthetic mitral/aortic mechanical heart valve
• Mixed aortic valve disease (aortic stenosis and aortic regurgitation
with predominant aortic regurgitation > 3+).
• Moderate-or severe mitral or severe tricuspid insufficiency.
• Hypertrophic obstructive cardiomyopathy.
• Evidence of intracardiac mass, thrombus or vegetation.
• Severe LV hypertrophy (wall thickness > 1.7cm)
• Coronary ostia (from native leaflet) < 14 mm with severe Ca+< 13;
mm with moderate Ca+; < 10 mm without Ca+
• Annulus-to-aorta (angle) > 70
• Ascending aorta diameter > 43 mm.
“High Risk” Anatomic Exclusion CriteriaCoreValve
US Pivotal

• Severe aortic or severe iliofemoral disease with iliac and
femoral vessels (diameter) < 6 mm.
• Significant aortic disease, including abdominal aortic or
thoracic aneurysm defined as maximal luminal diameter 5 cm
or greater; marked tortuosity (hyperacute, bend), severe
unfolding and tortuosity of the thoracic aorta.
• Subjects with either:
“High Risk” Vascular Exclusion Criteria
1. Bi-lateral femoral or aortic vascular conditions (e.g.,
stenosis, tortuousity), that make insertion and
endovascular access to the aortic valve impossible.
2. Symptomatic carotid or vertebral artery disease.
CoreValveUS Pivotal
• Subject must have co-morbidities such that a cardiologist and
two cardiac surgeons agree that medical factors preclude
operation, based on a conclusion that the probability of death or
serious morbidity exceeds the probability of meaningful
improvement. Specifically, the probability of death or serious,
irreversible morbidity should exceed 50% at 12 months.
• Subject has senile degenerative aortic valve stenosis with mean
gradient > 40 mmHg and/or jet velocity greater than 4.0 m/s, or
an initial aortic valve area of < 0.8 cm2 by echocardiogram.
“Inoperable” Inclusion Criteria
Study Design Pending Discussion with FDA
CoreValveUS Pivotal

Study
Endpoints
CoreValve
US Pivotal

• High Risk Surgical
– Freedom from all cause mortality
compared to sAVR at 12 months
• High Risk Inoperable Study
– Freedom from all cause mortality
Primary Trial EndpointsCoreValve
US Pivotal

• Time: 24 hours, 30 days (or in-hospital), 12+ months
• Place: OR, in Hospital, Post-discharge
• Type: Cardiac, vascular, non cardiovascular, valve
related
All Cause Mortality preferred but
Our study population is by definition “high-risk” with
severe co-morbidities that predispose to non-cardiac
mortality at one year – there are challenges in identifying
the specific effect of the valve treatment vs the “noise” of
the co-morbidities in these high risk populations
CoreValveUS Pivotal

• Evidence of prosthetic valve dysfunction (hemolysis, infection,
thrombosis, or migration) at 30 days, 6 months and 12 months.
• Device success (successful delivery and deployment of the device
and retrieval of the delivery catheter resulting in AVA greater than
0.9cm2 and <3+ aortic regurgitation (AR).
• Procedural success, defined as device success and absence of in-
hospital MACCE.
• Major adverse cardiovascular and cerebrovascular events
(MACCE), including all cause death, MI, stroke, or re-intervention
at 30 days, 6 months and 12 months.
• Improvement in NYHA class at 30 days, 6 months and 12 months.
• in distance walked during 6-minute walk test (6MWT) from
baseline to 12 months.
Secondary Endpoints-ICoreValve
US Pivotal

• Quality of Life (QOL) change from baseline at 30 days, 6 months
and 12 months.
• Length of index hospital stay and repeat hospitalization.
• Discharge, 30 day, 6 month and 12 month echocardiographic
assessment of aortic valve function by using the following
measures:
- Transvalvular peak and mean gradient transvalvular gradient
- Effective orifice area
- AV performance index
- Cardiac output
- Aortic or mitral regurgitation, or mitral regurgitation.
Secondary Endpoints-IICoreValve
US Pivotal

5 Year+ Long-Term Durability Studies
Absence of Fracture Absence of Migration
CoreValveUS Pivotal

Unique Design of CoreValve Frame
18Fr SE Feasibility Study Re-Adjudication
CoreValve US Pivotal Study
“High Risk” Study Cohort
Non Operable Cohort
Clinical Endpoints (VARC Study Group)
Next Steps (Soon)
Closing CommentsCoreValve
US Pivotal