Embed Size (px)
Citation preview

REFERENCES
1. Reich P, Muller-Schunk S, Liebetrau M, Scheuerer W, Bruckmann H, HamannGF. Combined cerebellar and bilateral cervical posterior spinal artery strokedemonstrated on MRI. Cerebrovasc Dis 2003; 15: 143–147.
2. Sandson TA, Freidman JH. Spinal cord infarction. Report of 8 cases and reviewof the literature. Medicine 1989; 68: 282–292.
3. Salvador de la Barrera S, Barca-Buyo A, Montoto-Marques A, Ferreiro-VelascoM, Cidoncha-Dans M, Rodriguez-Sotillo A. Spinal cord infarction: prognosisand recovery in a series of 36 patients. Spinal Cord 2001; 39: 520–525.
4. Mawad ME, Rivera V, Crawford S, Ramirez A, Breitbach W. Spinal cordischemia after resection of thoracoabdominal aortic aneurysms: MR findings in24 patients. Am J Neuroradiol 1990; 11: 987–991.
5. Weidauer S, Nichtweiss M, Lanfermamm H, Zanella FE. Spinal cordinfarction: MR imaging and clinical features in 16 cases. Neuroradiology 2002;44: 851–857.
6. Bammer R, Fazekas F, Augustin M, et al. Diffusion-weighted MR imaging ofthe spinal cord. AJNR Am J Neuroradiol 2000; 21: 587–591.
7. Fujikawa A, Tsuchiya K, Koppera P, Aoki C, Hachiya J. Case report: spinalcord infarction demonstrated on diffusion-weighted MR imaging with asingle-shot fast spin-echo sequence. J Comput Assist Tomogr 2003; 27: 415–419.
8. Stepper F, Lovblad KO. Anterior spinal artery stroke demonstrated by echo-planar DWI. Eur Radiol 2001; 11: 2607–2610.
9. Weidauer S, Dettmann E, Krakow K, Lanfermamm H. Diffusion-weighted MRIof spinal cord infarction. Description of two cases and review of the literature.Nervenarzt 2002; 73: 999–1003.
10. Gudbjartsson H, Maier SE, Mulkern RV, Moocz IA, Patz S, Jolesz FA. Linescan diffusion imaging. Magn Reson Med 1996; 36: 509–519.
11. Robertoson RL, Maier SE, Mulkern RV, Vajapayam S, Robson CD, Barnes PD.MR line-scan diffusion imaging of the spinal cord in children. ANJR Am JNeuroradiol 2000; 21: 1344–1348.
Massive cerebral airembolism aftercardiopulmonaryresuscitation
Shiuh-Lin Hwang1MD PHDMD PHD, Ann-Shung Lieu1
MDMD,
Chih-Lung Lin1MDMD, Gin-Chung Liu2
MDMD,
Shen-Long Howng1MD PHDMD PHD, Tai-Hung Kuo3
MDMD
1Division of Neurosurgery, 2Department of Radiology, Kaohsiung Medical
University Hospital, Kaohsiung; 3Department of Neurosurgery, Armed Forces
Tso Ying Hospital, Kaohsiung; Taiwan
Summary We report a case of massive intracerebral air embolism
after cardiopulmonary resuscitation in a patient with a fatal head
injury. There was no pneumothorax or extravascular pneumo-
cephalus, however, air was found in the internal carotid artery.
Massive cerebral air embolism may occur after entrance of air into
the circulatory system via ruptured pulmonary vessels during
cardiopulmonary resuscitation.
ª 2005 Elsevier Ltd. All rights reserved.
Journal of Clinical Neuroscience (2005) 12(4), 468–469
0967-5868/$ - see front matter ª 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jocn.2004.03.041
Keywords: cerebral air embolism, cardiopulmonary resuscitation
Received 11 February 2004
Accepted 24 March 2004
Correspondence to: Tai-Hung Kuo MD, Department of Neurosurgery, Armed
Forces Tso Ying Hospital, 553 Chun Chiao Rd, Tsoying, Kaohsiung, Taiwan.
Tel.: +886 7 3215049; Fax: +886 7 3215039;
E-mail: [email protected]
INTRODUCTION
Intracerebral air embolism is not uncommon. However, massiveair embolism into the intracranial vessels demonstrated on CTscan is rare, with only three cases reported (Table 1).1–3 All re-ported cases occurred in the setting of cardiopulmonary resuscita-tion (CPR) with pneumothorax or extravascular pneumocephalus.We report a case of massive cerebral air embolism after CPR in apatient with a fatal head injury, but without pneumocephalus orpneumothorax.
CASE REPORT
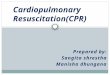
A 32-year-old man sustained a severe head injury after a trafficaccident. He arrived in the emergency room by ambulance incardiopulmonary arrest. His pupils were dilated. He was intu-bated immediately and CPR was performed. There was noapparent chest trauma. A chest X-ray revealed no haemothoraxor pneumothorax. A brain CT scan obtained after CPR revealedwidespread low density areas with serpentine distribution in thebasal cisterns and bilateral subarachnoid spaces, which werehighly suggestive of intra-arterial air embolism (Fig. 1). Therewas no skull fracture or extravascular pneumocephalus. Therewas air in the internal carotid artery but no cervical trauma.Although systemic circulation was restored, the patient died2 h after admission.
DISCUSSION
Embolismof air into the cerebral vessels is not rare. Itmay occur as acomplication of angiography or via a peripheral or central venousline.4–8 It may also occur in thoracic, cardiovascular and neurosur-gical surgeries, thoracic or cranial trauma and during haemodialy-sis.9–15 The volume of intravascular air embolised in these casesis usually small. Massive air embolism to the major cerebral vesselsis extremely rare. Only three cases with diffuse intra-arterial airembolism in the brain have been reported.1–3 All of them had re-quired cardiopulmonary resuscitation and massive cerebral airembolism was attributed to tension pneumothorax1 or pulmonarybarotrauma due to CPR or positive pressure ventilation.1,2,16,17
In the reported case, we suggest that a large amount of air en-tered the pulmonary veins via ruptured pulmonary vessels duringCPR and thereby reached the systemic circulation.1 Alternately,positive pressure ventilation can produce pulmonary barotrauma
Table 1 Summary of the literature reports of massive cerebral air embolism demonstrated by brain CT
Authors (year) Primary condition CPR Other clinical findings
Yamaki et al. (1989)1 Myocardial infarction + Pneumothorax, mediastinal emphysema
Iwama et al. (1994)2 Head injury + Skull fracture, pneumocephalus
Akaishi et al. (2000)3 Head injury + Tension pneumothorax
Present case Head injury + Nil
CPR, cardiopulmonary resuscitation.
Journal of Clinical Neuroscience (2005) 12(4) ª 2005 Elsevier Ltd. All rights reserved.
468 Hwang et al.

and cerebral air embolism.16,17 Experimental rat studies demon-strate that high alveolar pressure can result in cerebral air embo-lism.18 If rupture of pulmonary vessels occurs in associationwith parenchymal damage, air can enter the pulmonary vein andreach the systemic circulation. In the present case, primary CPRwas successful and the cerebral circulation temporarily preserved.Accordingly, the air from the pulmonary vessels could diffuselyenter the major cerebral arteries and peripheral cerebral vessels.Massive cerebral air embolism and air in the internal carotid arterywere demonstrated on brain CT.Intracerebral air embolism may be observed with increasing fre-
quency with the widespread use of ventilatory assistance andCPR. Massive cerebral air embolism is fatal and there is no effec-tive therapy.
REFERENCES
1. Yamaki T, Ando S, Ohta K, Kubota T, Kawasaki K, Hirama M. CTdemonstration of massive cerebral air embolism from pulmonary barotraumadue to cardiopulmonary resuscitation. J Comput Assist Tomogr 1989; 13:313–315.
2. Iwama T, Andoh H, Murase S, Miwa Y, Ohkuma A. Diffuse cerebral airembolism following trauma: striking postmortem CT findings. Neuroradiology1994; 36: 33–34.
3. Akaishi K, Hongo K, Obinata C, Kobayashi S. Pneumoangiogram in a patientwith severe head injury. J Neurosurg 2000; 92: 502.
4. Ordway CB. Air embolus via CVP catheter without positive pressure:presentation of a case and review. Ann Surg 1974; 179: 479–481.
5. Price DB, Nardi P, Teitcher J. Venous air embolization as a complication ofpressure injection of contrast media: CT findings. J Comput Assist Tomogr1987; 11: 294–295.
6. Rubinstein D, Symonds D. Gas in the cavernous sinus. AJNR Am J Neuroradiol1994; 15: 561–566.
7. Takahashi W, Yoshii F, Ohsuga S, Izumi Y, Shinohara Y. Two patients withparadoxical cerebral air embolism due to accidental disconnection of asubclavian intravenous catheter. Jpn J Stroke 1995; 17: 89–94.
8. Woodring JH, Fried AM. Nonfatal venous air embolism after contrast-enhancedCT. Radiology 1988; 167: 405–407.
9. Hwang TL, Fremaux R, Sears ES, et al. Confirmation of cerebral airembolism with computerized tomography. Ann Neurol 1993; 13:214–215.
10. Jansen ME, Lipper MH. CT in iatrogenic cerebral air embolism. AJNR Am JNeuroradiol 1986; 7: 823–827.
11. Kearns PJ, Haulk AA, McDonald TW. Homonymous hemianopia due tocerebral air embolism from central venous catheters. Western J Med 1984; 140:615–617.
12. Menkin M, Schwartzman RJ. Cerebral air embolism: report of five cases andreview of the literature. Arch Neurol 1977; 34: 168–170.
13. Nakao N, Moriwaki H, Oiwa Y. Barotraumatic cerebral air embolism followingscuba diving. Brain Nerve 1990; 42: 1097–1100.
14. Temple AP, Katz J. Air embolism: a potentially lethal surgical complication.AORN J 1987; 45: 387–402.
15. Tsuiki H, Sano S, Yamamoto T, Miyamoto S. Cerebral air embolism on CTscan after chest injury. J Acute Med 1994; 18: 1893–1896.
16. Banagale RC. Massive intracranial air embolism: complication of mechanicalventilation. Am J Dis Child 1980; 134: 799–800.
17. Brown ZA, Clark JM, Jung AL. Systemic gas embolus: a discussion of itspathogenesis in the neonate, with a review of the literature. Am J Dis Child1977; 131: 984–985.
18. Kao DK, Tierney DF. Air embolism with positive-pressure ventilation of rats. JAppl Physiol 1977; 42: 368–371.
Motor cortex excitabilityafter thalamic infarction
TS Miles1 DSCDSC, MC Ridding1PHDPHD, D McKay1 PHDPHD,
PD Thompson2,3PHD FRACPPHD FRACP
1Department of Physiology, The University of Adelaide, Royal Adelaide
Hospital, Adelaide SA 5000, Australia, 2University Department of Medicine,
The University of Adelaide, Royal Adelaide Hospital, Adelaide SA 5000,
Australia, 3Department of Neurology, Royal Adelaide Hospital, Adelaide SA
5000, Australia
Summary Transcranial magnetic stimulation was used to map hand
muscle representations in the motor cortex of a patient in whom
infarction of the sensory thalamus deprived the sensorimotor cortex
of sensory input. The threshold for activation of the motor cortex on
the affected side was higher and the cortical representational maps of
individual muscles were less well defined than those on the normal
side. It is concluded that electrophysiological changes in cortical
organisation can be demonstrated following withdrawal of, or imbal-
ance in sensory afferent activity to the cerebral cortex in humans.
ª 2005 Elsevier Ltd. All rights reserved.
Journal of Clinical Neuroscience (2005) 12(4), 469–472
0967-5868/$ - see front matter ª 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jocn.2005.01.002
Keywords: plasticity, thalamic stroke, sensorimotor cortex
Correspondence to: P.D. Thompson, University Department of Medicine,
Royal Adelaide Hospital, Adelaide, SA 5000, Australia. Tel.: +618 8222 5502;
Fax: +618 8223 3870;
E-mail: [email protected]
Fig. 1 (a, b) CT scan showing massive intracerebral air embolism. Low density areas with a serpentine distribution were observed in the basal cisterns and
subarachnoid spaces. The air distribution pattern is highly suggestive of an intra arterial location.
ª 2005 Elsevier Ltd. All rights reserved. Journal of Clinical Neuroscience (2005) 12(4)
469Cortical organisation