Embed Size (px)
Citation preview

Cardiopulmonary Cerebral Resuscitation (CPCR)
Danielle Berube DVM, DACVECCUpstate Veterinary Specialties
September 17, 2016

Outline
• Introduction– Definitions– Outcome– Who is at risk
• Basic Life Support• Advanced Life Support• RECOVER Initiative• Summary and updates

Definitions
• Respiratory arrest– Cessation of breathing
• Cardiopulmonary arrest– Cessation of effective and spontaneous perfusion and
breathing (no palpable pulse, no heart sounds)• CPR vs CPCR– Cardiopulmonary resuscitation– Cardiopulmonary cerebral resuscitation

Outcomes
• Overall poor prognosis– Survival to discharge 6-7%
• Re-arrest rates– 68% dogs and 37% cats Survival to discharge

• Large prospective observational study that investigated many aspects of CPR
• Survival to discharge: 6% dogs and 3% cats• Simple anesthetic arrest (only 3 cases)– 33% survived to discharge

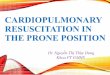
Dogs WithCPA
ROSC58%
No ROSC23%
ROSC < 20 min: 23% Euth: 10% Repeat CPA:13%
ROSC > 20 min: 35%
No longer alive at 24 hr. Euth: 21% Repeat CPA: 4%
Alive at 24 hr.10% Euth: 4%
Repeat CPA:
0Survive to Discharge6%

Outcome• We often cannot change what happened to the
patient prior to arrest• We can change staff and equipment variables that
affect outcome• Successful outcomes are dependent on– Staff preparedness– Stocked crash area– Working and available equipment– TEAM WORK

Outcome: Staff Preparedness
• Recognize patients at risk• Didactic training and hands on practice– Refresher every 6 months
• Centrally located crash cart– Routinely checked
• Algorithm and dosing charts

Outcome: Staff Preparedness
• Standardized CPR guidelines in human medicine improved outcome after in hospital CPA:– 2000: 13.7%– 2009: 22.3%

Who is at risk?• Trauma• Respiratory system disease• Septicemia• Prolonged seizures• Cardiac disease• Vagal stimulation• Anesthetic agents• Severe metabolic disease

Goals of CPCR
• Provide artificial respiration and cardiovascular support until Return of Spontaneous Circulation (ROSC) – Coronary perfusion pressure– Cerebral perfusion pressure
• Identify cause and treat immediately

Goals: Coronary Perfusion Pressure
• = Aortic diastolic pressure – right atrial pressure

Goals: Cerebral Perfusion Pressure
• = mean arterial pressure – intracranial pressure

CPR/CPCR
• Be prepared– Determine if a pet is breathing or if it has a
heartbeat– Training, supplies, cognitive aids
• Don’t panic!– Try to remain calm but efficient
• Call for help– CPCR is labor intensive and is more likely to be
successful with a team rather than an individual

CPR/CPCR
• First, follow your ABC’s (basic life support)– Airway– Breathing – Circulation/chest compressions
• Then, think about your DEF’s (advanced life support)– Drugs– Electrical defibrillation/ECG/End tidal CO2– Fluid therapy

CPR/CPCR
• First, follow your ABC’s (basic life support)– Circulation/chest compressions– Airway– Breathing
• Then, think about your DEF’s (advanced life support)– Drugs– Electrical defibrillation/ECG/End tidal CO2– Fluid therapy

Recover: JVECC 22 (S1) 2012, S102-S131

Basic Life Support
Recover: JVECC 22 (S1) 2012, S102-S131

Basic Life Support
• CIRCULATION– Check for heart beat/pulse– Do not assume there is no heart beat or pulse just
because they are not breathing– Place patient in lateral recumbancy • Preferably right
– If no heart beat or pulse begin chest compressions

Basic Life Support
• CIRCULATION/CHEST COMPRESSIONS– Goal• Maximize blood to the heart and brain• Restore pulmonary CO2 elimination and O2 uptake by
providing pulmonary blood flow– Small patients• One hand thumb and forefingers
Cardiac pump theory
Recover: JVECC 22 (S1) 2012, S102-S131

Basic Life Support
• CIRCULATION/CHEST COMPRESSIONS– Large patients• Hands on top of one another at a 90 angle• Widest part of chest• Elbows straight• Bend at the waist
Thoracic pump theory
Recover: JVECC 22 (S1) 2012, S102-S131

Basic Life Support
• CIRCULATION– Chest compressions – where• Cardiac Pump - patients <15kg (<33 pounds)
– Compress directly over the heart– Point of the elbow
• Thoracic Pump- patients >15 kg or barrel chested breeds– Compress at the widest part of thorax (usually further
back/caudal)

Basic Life Support• CIRCULATION/CHEST COMPRESSIONS• Minimize interruptions to <10 seconds and switch out
every 2 minutes or upon checking vitals• Including for intubation, blood draws, drug
administration

Basic Life Support
• Circulation/Chest compressions– How hard• Compress thoracic wall by ~1/3-1/2
– What rate• At least 100 compressions/minutes• “Stayin’ Alive” vs. “Another One Bites the Dust”
– What rhythm• 1:1 cycle (equal time spent compressing as allowing
chest to expand)

Basic Life Support
• AIRWAY – If agonal or not breathing obtain airway– Check airway for any obstruction to flow• Tilt head slightly back and extend the neck• Carefully, pull tongue forward and down to better
visualize • Use suction if needed• Use manual palpation if needed

Basic Life Support
• AIRWAY– Ensure proper tube placement• Visualize placement• Auscult for breath sounds• Observe for chest excursions• ETCO2
– Esophageal intubation-zero

Basic Life Support
• BREATHING– Connect to a resuscitation/ambu bag– Provide positive pressure ventilation up to 20 cm
H20– 100% oxygen, 8-10 breaths/minute– Inspiratory time 1 sec– Tidal volume 10 ml/kg– Avoid hyperventilation

Basic Life Support
• BREATHING– Trouble shooting• High pressure needed to generate breath
– Pleural space disease– Pulmonary disease– Tube obstruction
• No chest excursion– Inappropriate endotracheal tube placement– Cuff leaking– See above

Recover: JVECC 22 (S1) 2012, S102-S131

Advanced Life Support
Recover: JVECC 22 (S1) 2012, S102-S131

Advanced Life Support: Monitoring
• Monitoring– ECG• Asystole (22.8 – 72%)• Pulseless electrical activity (11 - 23.3%)• Sinus bradycardia (19 - 23% )• Ventricular fibrillation (2 – 19.8%)
– ETCO2• Proportional to pulmonary blood flow• Low: poor prognosis

Advanced Life Support: Monitoring
• Attach ECG– White lead – Right front– Black lead – Left front– Green lead – Right hind– Red lead – Left hind
• Minimal alcohol or use conducting gel• Rhythm diagnosis– Administer appropriate drugs

Asystole• No rhythm on ECG• Survival rate in people nearly 0%• Treatment options– Atropine– Epinephrine– Vasopressin

Pulseless Electrical Activity (PEA)• Aka electromechanical dissociation• Human survival 1-4%• Treatment options:– Epineprhine– Atropine– Vasopressin– Treat underlying cause

Sinus Bradycardia
• Sinus rate < 60 dog/ <160 cat with palpable pulses• Treatment– Atropine– Reverse offending sedatives– Treat suspected underlying cause

Ventricular Fibrillation• Course V Fib
– 30% response rate– SVT or sinus rhythm common when converted
• Fine V Fib– 5% conversion rate– Asystole converted rhythm
• Predisposing causes– Hypokalemia– Hypomagenesemia
www.mauvila.com
www.resuscitationcentral.com

Advanced Life Support
• DRUG ADMINISTRATION– Intravenous• Ideal mode• Central large bore catheter best• Peripheral typically easier during arrest• Consider venous cutdown early• If peripheral catheter, flush with 5-50 ml flush to reach
the heart

Jugular Cut Down• Quickly clip and prep area over jugular vein• 1-2 cm incision made through skin (#10 or #11 blade) parallel
to the vessel• Vessel dissected free from tissue• Hemostats to lift/isolate vessel• Catheter placed directly into vessel• Secure in place by suturing
Advanced Monitoring and Procedures for Small Animal Emergency and Critical Care Fig 4.5

Intraosseous Catheter• DRUG ADMINISTRATION– Intraosseus
• For small patients and exotics• All medications can be given
– Equipment• Jamshidi bone marrow needle• 18-30g hypodermic needles• Spinal needle
– IO catheter sites• Trochanteric fossa of femur• Wing of the ilium• Greater tubercle of the humerus

Advanced Life Support• DRUG ADMINISTRATION
– Intratracheal• Double dose• Dilute with saline to 5-6 ml• Flush to carina with red rubber catheter• Give two deep breaths• DO NOT GIVE SODIUM BICARBONATE via this route
– NAVEL• Naloxone• Atropine• Vasopressin• Epinephrine• Lidocaine

Advanced Life Support
• Common drugs – Epinephrine– Atropine– Vasopressin– Dextrose– Sodium bicarbonate
– Calcium gluconate, insulin
– Reversal agents• Naloxone, flumazenil,
antisedan

Vasopressors
• Increased vascular resistance to redirect blood flow to core– Epinephrine• Low dose (0.01 mg/kg) recommended every 4-5 min
– Vasopressin• 0.8 U/kg• Can be used interchangeably or in combination with
epinephrine

Parasympatholytics
• Atropine– Extensively studied in CPR– 0.04 mg/kg every 4-5 minutes

Antiarrhythmic drugs
• Ventricular tachycardia– Lidocaine 2mg/kg IV
• Ventricular fibrillation– Electrical defibrillation– If no response: amiodarone 2.5-5 mg/kg IV or IO• Risk of allergic reaction

Reversal Angents
• Naloxone (Reverses opioids)– 0.04 mg/kg IV
• Flumazenil (Reverses Benzodiazepines)– 0.01 mg/kg IV
• Atepamazole (Reverses alpha2 agonists)– 0.05 mg/kg IV

Advanced Life Support: Alkalinizing Agents
• Sodium bicarbonate• Indications– Prolonged CPA ( >10-15 min) with severe
metabolic acidosis ( pH <7)• 1mEq/kg dilute IV

Available at VECCS.org

Advanced Life Support
• Tricks or “short cuts” to remember doses– Epinephrine: 0.1ml per 20 lbs– Atropine: 1.0 ml per 20 lbs – Naloxone: 1.0ml per 20 lbs– Flumazenil: 1.0 ml per 20 lbs

Advanced Life Support
• ELECTRICAL DEFIBRILLATION– Reserved for ventricular fibrillation
– 4-6 J/kg (40 J per 20 lbs)

Electrical Defibrillation
• ELECTRICAL DEFIBRILLATION– Conducting gel for the paddles– Rinse off alcohol if present– Put patient in dorsal recumbancy– Place paddles on either side of chest– Charge paddles– Yell “Clear” and make sure staff is clear– Immediately resume CPR for 2 minutes before
assessing rhythm

Advanced Life Support: IV Fluids
• Fluid therapy– Shock fluid therapy reserved for hypovolemic
patients only– IVF contraindicated in euvolemic patients• IVF therapy can decrease coronary perfusion
Coronary perfusion pressure = aortic diastolic pressure – right atrial pressure

Advanced Life Support
• Ideal additional monitoring– ETCO2
• With ROSC see a steady increase in value• Humans with ETCO2 not reaching above 12mmHg
during arrest did not have ROSC– Obtain blood for stat labs• PCV/TS, BG, electrolytes and pH
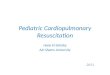
Fig 9: Capnography in dogs: Compendium October 2004

• ETCO2 </= 10 mmHg after 20 minutes of CPCR accurately predicts death
• “Cardiopulmonary resuscitation may reasonably be terminated in such patients”

Additionally…
• Things to anticipate– Large dogs or patients with intrathoracic disease may
require open chest CPR– If no venous access
• Get red rubber ready for intratracheal administration • Be prepared for cut down

Open Chest CPR
• Indications– Pleural space disease– Pericardial effusion– Penetrating chest wounds/chest wall trauma– Heavy patient/large breeds/incompressible thorax– Intra –operative arrests– No ROSC after 2-5 minutes of closed chest CPR– Post cardiothoracic surgery, chest/abdomen is already
open

RECOVER Initiative
• Reassessment Campaign on Veterinary Resuscitation• VECCS and ACVECC worked together to evaluate
resuscitation and how it is applied clinically• Adapted the approach taken by the American Heart
Association (AHA) and the International Liaison Committee on Resuscitation (ILCOR)
• Results published in JVECC as supplemental volume in June 2012

RECOVER Initiative
• Divided into 7 parts focusing on evidence and knowledge gap analysis– Part I: Evidence analysis and consensus process:
collaborative path toward small animal CPR guidelines– Part II: Preparedness and prevention– Part III: Basic Live support– Part IV: Advanced life support– Part V: Monitoring– Part VI: Post cardiac arrest care– Part VII: Clinical guidelines

RECOVER Initiative
• Divided into 7 parts focusing on evidence and knowledge gap analysis– Part I: Evidence analysis and consensus process:
collaborative path toward small animal CPR guidelines– Part II: Preparedness and prevention– Part III: Basic Live support– Part IV: Advanced life support– Part V: Monitoring– Part VI: Post cardiac arrest care– Part VII: Clinical guidelines

RECOVER Initiative
• Preparedness and Prevention– Equipment and supply delays or failure resulted in
delay of CPCR in 18% of cases– Routine training and review– Use of flow charts/dosing charts– Team leader during arrest– De-brief following successful or unsuccessful CPCR

RECOVER Initiative
• Basic Life Support– Chest compressions
• Large dogs: hands over widest part of chest• Small dogs: hands directly over heart• Very small dogs/cats: circumferential• 100-120 compressions per minute
– Ventilation• Continuous compression and ventilation• 10 breaths per minute
– Cycles• Rotate compressors every 2 minutes

RECOVER Initiative
• Advanced Life Support– Epinephrine: low dose every 3-5 minutes– Atropine– Vasopressin: 0.8 units/kg as a substitute or in
combination with epinephrine– Defibrillation: in cases of V-fib– 100% O2
– IVF: not recommended if euvolemic

RECOVER Initiative
• Monitoring– ETCO2: use for monitoring of ROSC– Additional monitoring can be considered but
should NOT interrupt compressions• ECG• Doppler• Electrolytes
– Use along with auscultation of heart and lungs (do not use as sole device)

RECOVER Initiative
• Post Cardiac Arrest Care

Updates Since RECOVER INITIATIVE
• Metabolic acidosis and hyperlactatemia (100%)
• Respiratory acidosis:– 88% during CPR – 61% following ROSC
• Hyperkalemia 65%
• Decreased iCa 18%• Hypoglycemia 21%• Hyperglycemia 62%
Take away message: Point of care testing may be important during CPR

Updates Since RECOVER INITIATIVE
• Since RECOVER initiative this hospital showed:– Increased use of capnography– Increased use of suction to aid in intubation
• RECOVER guidelines altered CPR teaching

Updates Since RECOVER INITIATIVE
• To provide recommendations for reviewing and reporting CPR events in dogs and cats
• Template for standardized reporting• Will allow high quality veterinary CPR
research, improve data comparison and serve as the foundation for veterinary CPR registries

Summary
• Be Prepared– All staff know what to look for– All staff know where supplies are
• Check for breathing and pulses • Follow your ABC’s (or BACs) and then the
DEF’s• Record what was done and when.• Remember, this is a TEAM effort.

Questions
• Thank You!• References available upon request