Embed Size (px)
Citation preview

Cardiopulmonary Resuscitation During Pregnancy
Spencer Topp, MDDepartment of Emergency Medicine
University of Florida-Jacksonville

Case #1It’s a quiet Tuesday morning in Resus and
Laperouse is peacefully sipping his coffee, updating his procedure log on New Innovations while Al is busy restocking bed #4 and bitching the whole time he’s doing it.
The EMS phone suddenly goes off and someone yells out- “JFR has a 34-week pregnant lady in respiratory distress and they’re requesting a resus bed!”

Case #1Upon arrival, you get a quick story from EMS that the
lady is a 24-year old G1P0 at about 34 weeks. She had acute onset of SOB and chest pain and her husband called 911. She is in obvious respiratory distress, diaphoretic, and not mentating appropriately. She quickly gets hooked up to the monitor and her vitals show-
BP- 85/40, Pulse 144, RR 34, O2 sats 92% Temp 98.7, Accu-check 112

Case #1Physical Exam
Gen- tachypnic, diaphoreticHEENT-no trauma, PERRL, MMM, no JVDCardiac- tachycardic, loud systolic murmur over
pulmonic valve, no S3 or S4Lungs- tachypnic, otherwise CTABAbdomen- consistent with a 34-week gestation, no
obvious TTPExt- 1+ bilateral LE edema, weakly palpable peripheral
pulses Neuro- AOx 1 (person only), one word responses, follows
minimal commands, however moving all extremities Fetus- doppler showed fetal cardiac activity- 150-160
BPM

Case #1-2 IV’s established, 2 L NS hanging, 100% NRB applied, and Life-Pak pads placed
-Labs ordered and sent, EKG and CXR completed
-About 10 minutes after arrival, no significant change – what do you want to do now?
-You’re quickly trying to remember if RSI is safe in pregnancy when suddenly Al says, “guys, I don’t think she has a pulse anymore.”
-Rhythm on monitor shows PEA and color of Laperouse’s pants shows brown.

Objectives-Discuss incidence and causes of maternal cardiac arrest during pregnancy-Discuss pregnancy related physiologic changes-Differences in ACLS algorithms during pregnancy?-What therapy options are available? -What drugs are safe?-Emerging therapies for maternal cardiac arrest?

Cardiopulmonary Arrest in Pregnancy
-Incidence of cardiac arrest is about 1 in 30,000 pregnancies-Because most pregnant women are young and healthy, causes of arrest differ slightly from the general population-Causes include:
1) Pulmonary Embolism2) Pre-ecclamsia/Ecclampsia3) Sepsis4)Maternal hemorrhage
-these account for nearly 70% of all maternal arrests
-amniotic fluid embolism, trauma, peripartum cardiomyopathy, stroke and MI account for the remainder
-iatrogenic causes- hypermagnesmia, anaphylaxis, anesthesia complications

Physiologic Changes During Pregnancy
Airway Changes Upper airway edema and increased
secretions
Most women go from Mallampati class 1 or 2 to a grade 4 airway by term
Progesterone delays gastric emptying, increasing risk of aspiration
Gravid uterus compresses diaphragm making BVM more difficult
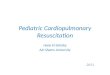
Airway Changes during Labor and Delivery
Kodali B-S, Chandrasekhar S, Bulich LN Anesthesiology vol. 108, 357 - 362, 2008

Physiologic Changes During Pregnancy
Pulmonary Physiology Changes
Progesterone induced increase in minute ventilation through increased tidal volume
-ABG’s during late pregnancy shows a compensated respiratory alkalosis (PCO2 of 28-32)
Decreased functional residual capacity and limited oxygen reserve
-pregnant patients quickly desaturate during both RSI (with proper pre-oxygenation) or apnea caused by arrest
Chest wall compliance is reduced secondary to mechanical effects (enlarged breasts and gravid uterus)

Physiologic Changes During Pregnancy
Cardiovascular Physiologic Changes
Increased cardiac output (30-50% by 32 weeks)
Increased oxygen consumption
Decrease in SVR secondary to uteroplacental blood flow-up to 30% of CO goes to pregnant uterus, compared to 2% in non-gravids
Aortocaval compression by the gravid uterus - in the supine postion, venous blood return may be completely obstructed with all blood return supplied by the azygous, lumbar and paraspinal veins

Differences in Pregnant Resuscitation
-In general, resuscitation algorithms during cardiac arrest are the same for pregnant and non- pregnant patients (with a few exceptions)
• more aggressive airway management
• slight modification in CPR/chest compressions
• early consideration of perimortem
cesarean delivery

CPR Changes During Pregnancy
-Cardiac output during CPR is estimated to be ~30% of normal
-Uteroplacental blood flow is markedly reduced even with optimal chest compressions
-During the second half of pregnancy, when performing CPR, an attempt is made to relieve the aortocaval compression that occurs in the supine position
-However, a true “lateral decubitus” position is not optimal when performing chest compressions

Cardiff WedgeRees and Willis in 1990 -measured the force achieved with chest compressions in the supine, lateral decub, and various intermediary angles as compared to optimal CO
-their work led to the development of the Cardiff wedge
-inclined at 27o to specifically perform CPR on pregnant patients
If no wedge available, rolled up bed sheet under patient’s right hip or knee of resus team member under patient’s right hip
Also can try manual displacement of uterus up and to the left (much like pannus retraction during central line placement)

BLS and ACLS in Pregnancy
No changes in defibrillator pad placement in pregnancy
No changes in defibrillator energy requirements
Nanson et al studied transthoracic impedence
looked at 45 women at term and then again at 6-8 weeks post-partum
no difference in the two groups
No contraindication to external defibrillation in pregnancy
multiple studies have demonstrated no adverse fetal effects
countershocks up to 400 J have been used without adverse fetal effects

BLS and ACLS in Pregnancy
ACLS medications are given in the standard doses and routes
Theoretically, the α-adrenergic agents may cause uteroplacental vasoconstriction
This further compromises already poor uterine blood supply
However, actual clinical effects not known (try posing that one to the IRB)
Sodium Bicarb use controversial May worsen fetal acidosis
The BEST chance for fetal survival is rapid resuscitation of the mother

Bradycardia in PregnancySymptomatic bradycardia rare occurrence during pregnancy
Common causes include: Vasovagal events Hypothyroidism Hypothermia Myocardial ischemia Supine Hypotensive Syndrome of Pregnancy
(bradycardia, hypotension, syncope)
Treatment for symptomatic pregnant patients no different
Atropine still treatment medication of choice Transcutaneous pacing also safe during
pregnancy

SVT in PregnancyMost frequent tachyarrhythmia of pregnancy
Pregnancy increases risk for new onset SVT
Pregnancy also increases frequency and severity of pre-existing SVT
Treatment algorithm same as for non-gravids
Stable vs unstable Again, DC cardioversion safe Adenosine at standard doses also safe

V Tach in PregnancyIn setting of structurally normal hearts, VT in pregnancy is rare
When VT does occur in pregnant patient consider these causes: Severe acid-base disorder Severe electrolyte disorder Abuse of stimulants
Again, cardioversion and defibrillation safe
Lidocaine (class B) and Procainamide (class C) safe for sustained, stable VT
Amiodarone (class D)- use limited by teratogenic profile Use for pharmacologic and shock resistant VT

Cardiac Arrest: VF, PEA, Asystole
As discussed previously, ACLS algorithms basically unchangedRemember left lateral decub position for chest compressionsIntubate sooner than during other code situationsDefibrillate at same energiesEpinephrine, Vasopressin, Atropine should not be withheld because of concern for fetal effects
How long do you resuscitate the mother before you turn your attention to a viable fetus?

Perimortem C-sectionCesarean delivery is one of the oldest surgical procedures, dating back nearly 3000 years
The procedure is believed to have derived it’s name from the Lex Cesare or “Law of Caesar”
Fetuses had to be separated from the mothers who died during child birth for religious purposes
Interestingly, some of the infants survived
Perimortem C-section first began to be described in the medical literature in the late 19th and early 20th centuries

Perimortem C-sectionKatz and colleagues in 1986 reviewed all the reports of perimortem C-sections
Found reports of 188 such precedures 61 of the reports included time of arrest or death of the
mother to time of delivery of infant
Time (in minutes)
# of infants surviving
% surviving neuro intact
0-5 45 98
6-15 18 83
16-25 9 33
26-35 4 25
36+ 1 0

Perimortem C-sectionBased on these findings, Katz and colleagues recommended
“initiation of C-section within 4 minutes of maternal arrest and fetal delivery within 5 minutes.”
These recs have been supported by other studies and consensus panels
Forms the basis of the “4 minute” rule
Case reports of prolonged time (>20) do not make this “4 minute rule “ absolute

Perimortem C-sectionGestational age is an important factor in predicting the prognosis for infants after perimortem cesarean deliveries
What is the gestational age threshold for expected fetal viability?
-Most institutions agree between 24-26 weeks
Because exact gestational age is sometimes unknown during an arrest situation, what are some ways you can estimate GA?
-Ultrasound (also gives info on fetal lie, placental location, or presence of fetal cardiac activity)
-Measure from pubic symphysis to top of uterine fundus

Perimortem C-sectionThe primary goal of perimortem C-section traditionally has been to save the fetus
The procedure may be life saving for both mother and fetus Significant aortocaval compression by >20 week uterus Delivery of fetus may significantly improve maternal cardiac output Numerous case reports to support this (?)
Cardiac arrest in early pregnancy Unknown if C-section is beneficial Much smaller fetal-placental mass, little to no aortocaval
compression Less hemodynamic benefits Not recommended at gestational age of less than 24 weeks Focus on optimizing resuscitation of mother

Perimortem C-section Decision Making
Prepare for emergent c-section as soon as cardiac arrest identified in the pregnant woman
Quickly determine gestational age during initial resuscitation of mother
Once procedure begins, ideally two teams now working independently
CPR is continued on mother
Factors that increase the infant’s chance of survival Short interval between arrest and delivery No sustained prearrest hypoxia of mother Minimal or no signs of fetal distress before arrest Aggressive/effective resuscitation of mother Procedure performed in center with neonatal ICU Emergency C-section within rescuer’s procedural range of experience/skills

Fibrinolytic Therapy During Pregnancy
No randomized controlled trials about thrombolytics in pregnancy have been conducted
pregnant women were excluded from phase-II and phase-III trials for Alteplase (t-PA)
The package insert for t-PA states pregnancy to be a “relative contraindication,” with other sources stating t-PA to be pregnancy category B (presumably safe based on animal studies)
Thrombolytics do not cross the placenta

Fibrinolytic Therapy During Pregnancy
In 2006, Leonhardt et al. published a review article dealing with the question of thrombolytic safety during pregnancy
28 cases in which t-PA had been used during pregnancy
Indications for use were stroke (n=10), thrombosis of cardiac valve prosthesis (n=7), pulmonary embolism (n=7), DVT (n=3), and myocardial infarction (n=1)
The pregnant patients that received thrombolytics did not have any higher complication rates than in the large, randomized trials for thrombolytics in stroke, PE, or MI
6 of the children (24%) died, 3 secondary to abortion for maternal health. In only 2 of the fetal deaths was there a probable, causal relationship between fetal death and the use of t-PA (8%).

Fibrinolytic Therapy During Pregnancy
Alternatives to thrombolytics in massive PE would be surgical embolectomy or catheter-directed thrombolytic therapy
not always available in a time-sensitive fashion, and not without their own risks and complications (10% fetal death reported during surgical embolectomy)
Unfortunately, not enough good evidence exists to propose a set of guidelines for the use of thrombolytics in a pregnant patient
small series of case reports available suggests the use of thrombolytics to be both safe and efficacious in the treatment of massive PE in pregnancy
should be considered on a case by case basis, keeping in mind it may be the quickest, most efficacious treatment
Keep in mind, would definitely complicate an emergent C-section

Therapeutic Hypothermia During Pregnancy
Single case report of a 35 y/o, 13 weeks pregnant
Witnessed, out-of-hospital V-fib arrest
Defibrillated 4 times and Lidocaine given for non-sustained, polymorphic VT
Decision was made, in consult with family, for therapeutic hypothermia for 24 hours
At goal of 33oC, fetal bradycardia (90-100 BPM) was noted
Pt rewarmed and fetal HR normalized
Mother sustained mild neurologic deficits
Infant was “normal” at 2 months

Questions?