Embed Size (px)
Citation preview

Managerial EpidemiologyPart II
Ty Borders, Ph.D.
Assistant Professor
Department of Health Services Research & Management
School of Medicine

Objectives
• Identify groups at higher risk for poor health and need for health service– Calculate Relative Risk, Attributable Risk, & Odds Ratio
• Discuss strengths and weaknesses of designs to identify at risk groups– Case control studies
– Prospective and retrospective cohort studies
Epidemiology and Levels of Disease Prevention
• Primary– Risk factor reduction– Decreases incidence and mortality
• Secondary– Screening (early detection and medical
treatment)– Decreases mortality and sometimes incidence
• Tertiary– Alleviation of disability– Decreases mortality
Identifying High Risk Groups: Observational Studies
• Cross - sectional– Provides estimate of the strength of association
between a factor and outcomes or event– Can not determine timing of exposure– e.g., A telephone survey of rural residents
conducted at one point in time
Observational Studies (cont.)
• Prospective and retrospective (historical) cohort studies– Compare risk of disease or other outcome
among 2 or more groups (i.e., exposed and unexposed)
• Case - control study– Compare odds of exposure between 2 or more
groups with disease (i.e., cases and controls)
Risk Factors
• Risk factor– Associated with increased risk
• Exposure– Contact with a risk factor– Dose and duration dependent– Direct or indirect

Cohort Studies
Onset of study
Time
Exposed
Unexposed
Eligible subjects Disease
No Disease
Disease
No Disease
Direction of inquiry
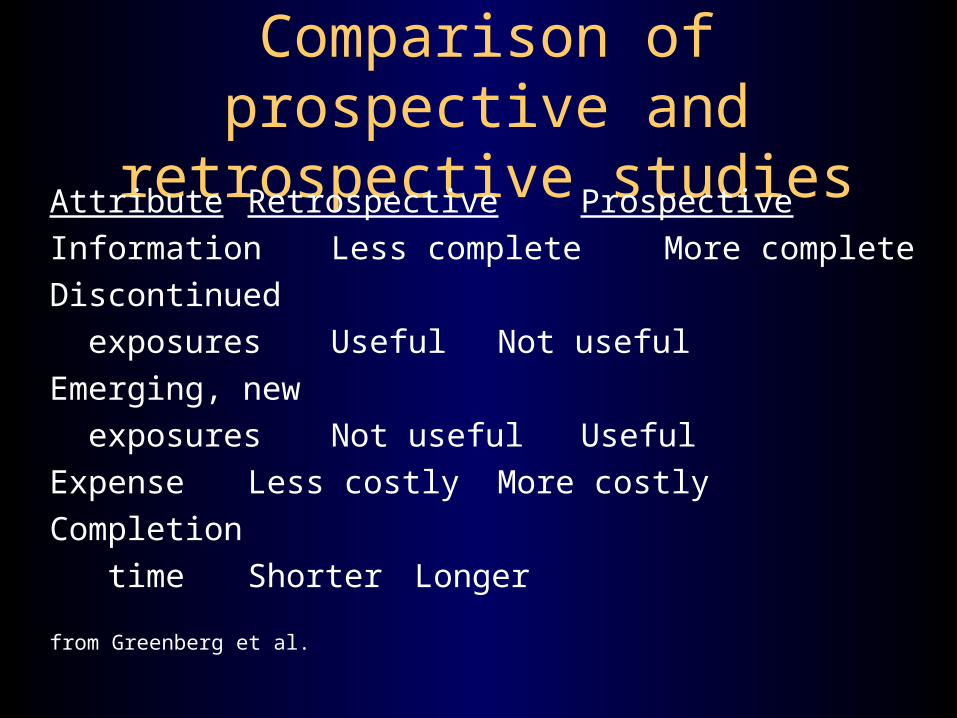
Comparison of prospective and retrospective studies
Attribute Retrospective Prospective
Information Less complete More complete
Discontinued
exposures Useful Not useful
Emerging, new
exposures Not useful Useful
Expense Less costly More costly
Completion
time Shorter Longer
from Greenberg et al.

Adv./Disadv. of cohort studiesAdvantages Disadvantages
Direct calculation Time consuming
of relative risk
May yield info. on incidence Require large sample sizes
Clear temporal relationship Expensive
Can yield info. on multiple Not efficient for study of
exposures rare events
Minimizes bias Losses to follow-up
Strongest observational design
for establishing cause-effect
from Greenberg et al.
Relative and Attributable Risk
Relative risk (risk ratio) = ratio of incidence in exposed to incidence in unexposed
RR = incidence rate among exposed
incidence rate among unexposed
Attributable risk (risk difference) = additional risk of disease following exposue above that of the unexposed
AR = incidence rate among exposed - incidence rate among unexposed
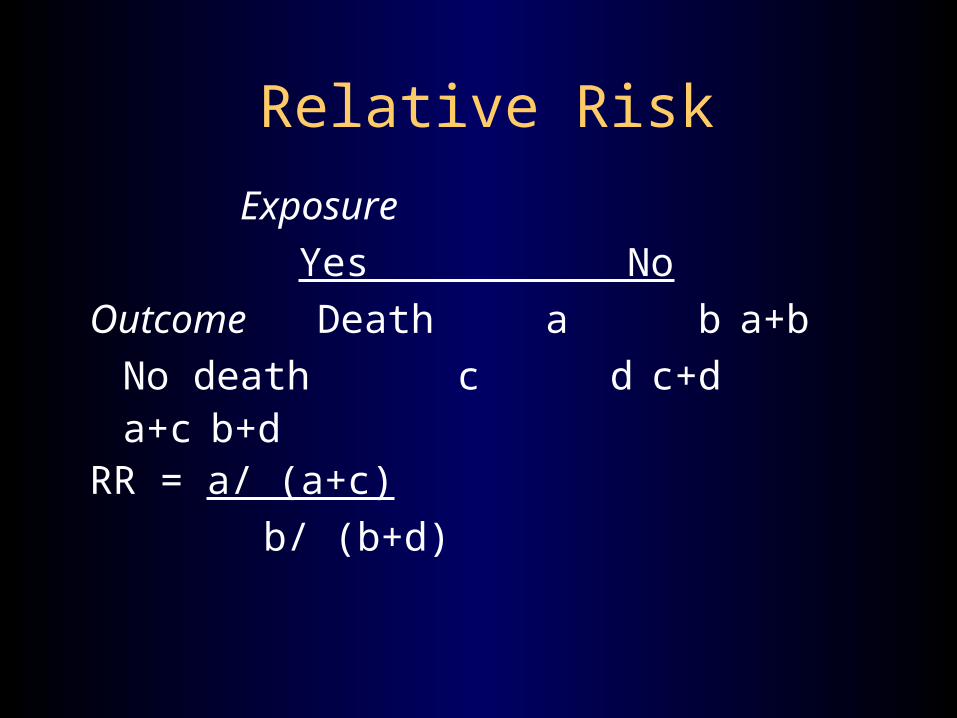
Relative Risk
Exposure
Yes No
Outcome Death a b a+b
No death c d c+da+c b+d
RR = a/ (a+c)
b/ (b+d)

Example of Relative Risk
Apgar score 0-3 4-6
Outcome Death 42 43 85No death 80 302 382
122 345 467
Risk among exposed = 42 / 122 = 34.4%Risk among unexposed = 43 / 345 = 12.5%RR = 34.4 / 12.5 = 2.8
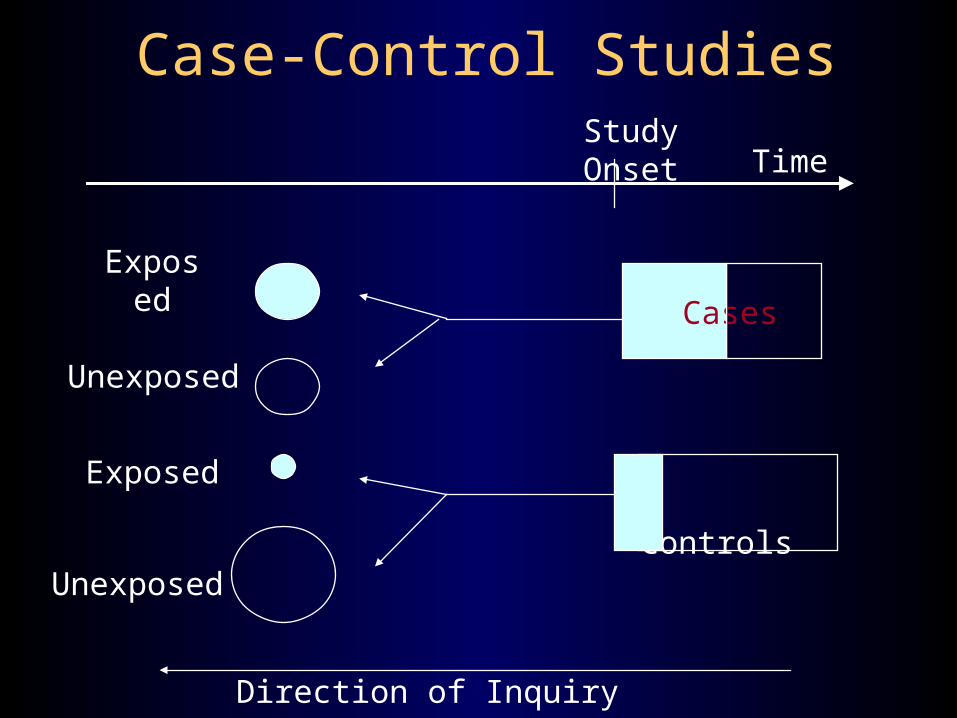
Case-Control Studies
Time
Controls
Direction of Inquiry
CasesExposed
Unexposed
Unexposed
Exposed
Study Onset

Cases and controls
• Cases– Identified and selected from a defined source
population (e.g., all patients from a clinic, hospital, HMO, state, or nation)
– Likelihood of a case being included in study must not depend on exposure to risk factor
– Criteria for defining cases should be sensitive and specific
Cases and controls
• Controls– Identified and selected from a defined source
population (e.g., all patients from a clinic, hospital, HMO, state, or nation)
– Chosen at random from source population– An exposed member of the population should have
the same chance of becoming a control as an unexposed member

Exposure status
• Interviews and questionnaires typically used
• Objective measures preferred– e.g., biological markers, such as a measure of an
agent in the blood– Not always feasible, especially if test is invasive– Many exposures don’t have biological markers– Biological marker may not be present when test is
taken (e.g., aspirin quickly metabolized)
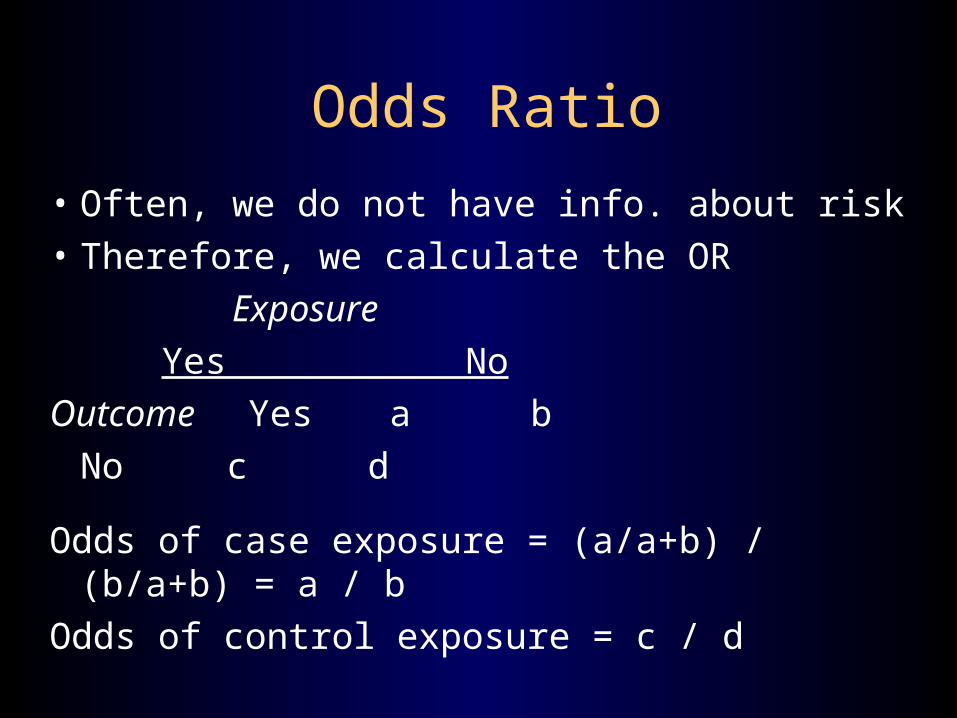
Odds Ratio
• Often, we do not have info. about risk
• Therefore, we calculate the OR
Exposure
Yes No
Outcome Yes a b
No c d
Odds of case exposure = (a/a+b) / (b/a+b) = a / b
Odds of control exposure = c / d

Example of Odds Ratio
Exposure
Yes No
Cases 50 15
Controls 30 20
OR = (a/b) / (c/d)
= ad / bc = 50*20 / 30*15 = 2.22
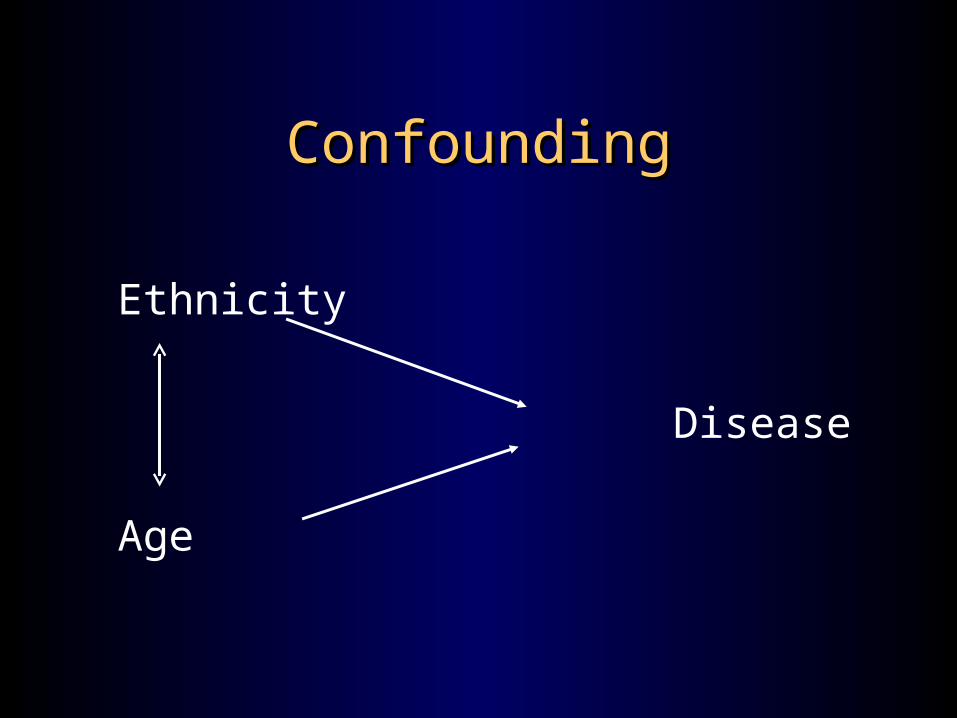
ConfoundingConfounding
Ethnicity
Disease
Age

ConfoundingConfoundingAge distribution (%)
44.0
51.6
36.1
38.0
38.3
38.2
24.6
26.7
25.7
27.0
24.1
25.7
16.8
16.2
19.6
19.1
19.3
19.2
14.7
5.6
18.6
15.9
18.4
16.9
Other Races
Hispanics
Non-Hispanic Whites
Urban residents
Rural residents
Overall
81+
76-80
71-75
65-70

ConfoundingConfoundingAge distribution (%)
44.0
51.6
36.1
38.0
38.3
38.2
24.6
26.7
25.7
27.0
24.1
25.7
16.8
16.2
19.6
19.1
19.3
19.2
14.7
5.6
18.6
15.9
18.4
16.9
Other Races
Hispanics
Non-Hispanic Whites
Urban residents
Rural residents
Overall
81+
76-80
71-75
65-70

1.39
0.91
0.74
0.72
0.68
0.71
2.18
0.61
0.53
0.57
0.59
0.83
-0.5 0.5 1.5 2.5
Hypertension
CHD
Lung disease
Stroke
Arthritis
Diabetes
OR
Adj. OR
Odds of DiseaseHispanics Relative to Non-Hispanic Whites
Adjusted and unadjusted
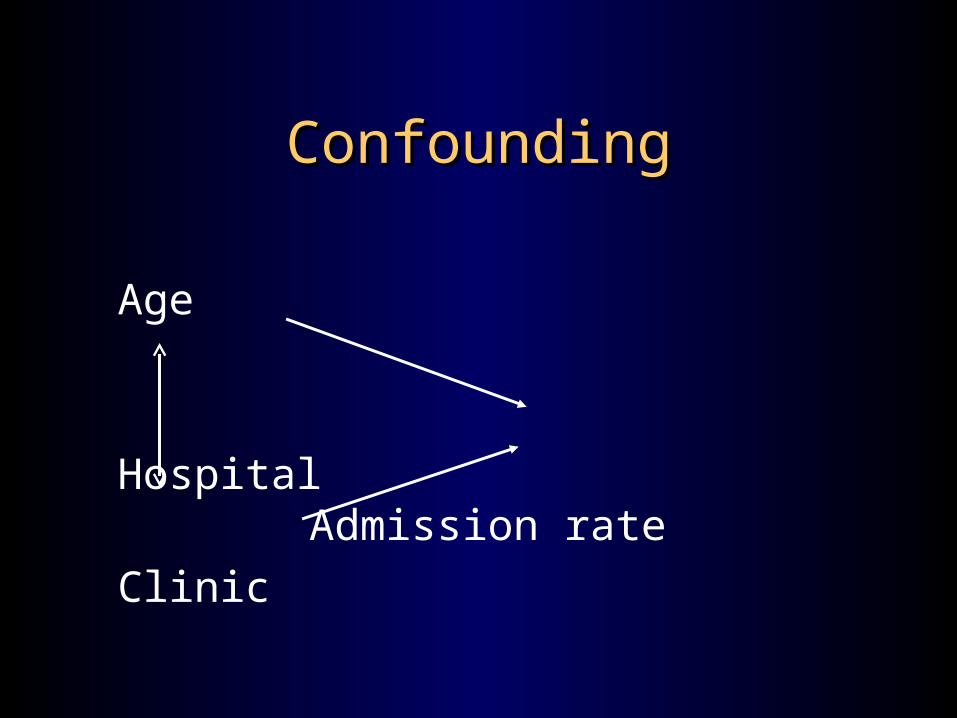
ConfoundingConfounding
Age
Hospital
Admission rate
Clinic

StandardizationStandardization
• Direct– Derived by applying category-specific rates
observed in each study population to a standard population
– Choice of study population• One of the populations to be compared
• Study populations combined
• An outside standard of interests (e.g., 1960 U.S. population)
StandardizationStandardization
• Indirect– Derived by applying the category-specific rates in the
standard population by the number of person-years or individuals in the study population
Indirect rate = crude rate of * observed events
study pop. expected events
• Both methods involve taking a weighted average of category-specific rates
Risk adjustmentRisk adjustment
• Direct and indirect standardization
• Case-mix adjustment– Uses billing data to classify patients into groups
that have similar costs
• Demographics (age, gender, etc.)
• Psychosocial factors
• Severity of disease

Survey Research Example
• Purpose– To determine who migrates or travels for physician care
– To determine why they migrate or travel for physician care
• Dependent variable– Whether the physician was located in the individual’s
home county (local market area) or another county (external market area)

Research MethodologyResearch Methodology
• Cross-sectional, population-based survey of– Perceived health status (e.g. SF-12)
– Health behaviors
– Realized health care utilization
– Accessibility of local providers
– Satisfaction with care
– Demographic factors
– Economic factors, including health insurance coverage
– Health services use

Independent Variables Independent Variables Health system factorsHealth system factors
• Perceived shortage of local family physicians – note: dummy variables created for most independent
variables
• Perceived shortage of local specialty physicians
• Rating of local delivery system– (excellent/very good versus good/fair/poor)
Predisposing - Predisposing - Demographic/Social Structural variablesDemographic/Social Structural variables
• Age category Gender• Education Employment status • Race Ancestry• Religion Live in-town• Live on farm• High number of individuals in household• Social support for health-related problems
Predisposing - Predisposing - Health belief variablesHealth belief variables
• Believe family physicians care beneficial
• Believe family physician care cost-beneficial
• Believe specialty physician care beneficial
• Believe specialty physician care cost-beneficial
Enabling variablesEnabling variables• Residence located in a fringe county• Location of specialty physician • Location of family physician• Household income level• Type of insurance coverage• Prepaid or FFS financing• Adequacy of insurance coverage• Bureaucracy of insurance coverage• Overall rating of health insurance coverage

Need variablesNeed variables
• Modified SF-12 Physical Component Score
• Modified SF-12 Mental Component Score
• High, moderate, or low user of physician services

Family Physician Migration -Significant Odds Ratios
0.306
2.278
0.47 0.489
2.919
0.375
0
0.5
1
1.5
2
2.5
3P
os
.ra
tin
g
Fa
m.
sh
ort
ag
e
Lu
the
ran
Liv
e in
-to
wn
Sp
ec
. o
ut
of
co
un
ty
Pri
va
tein
s.
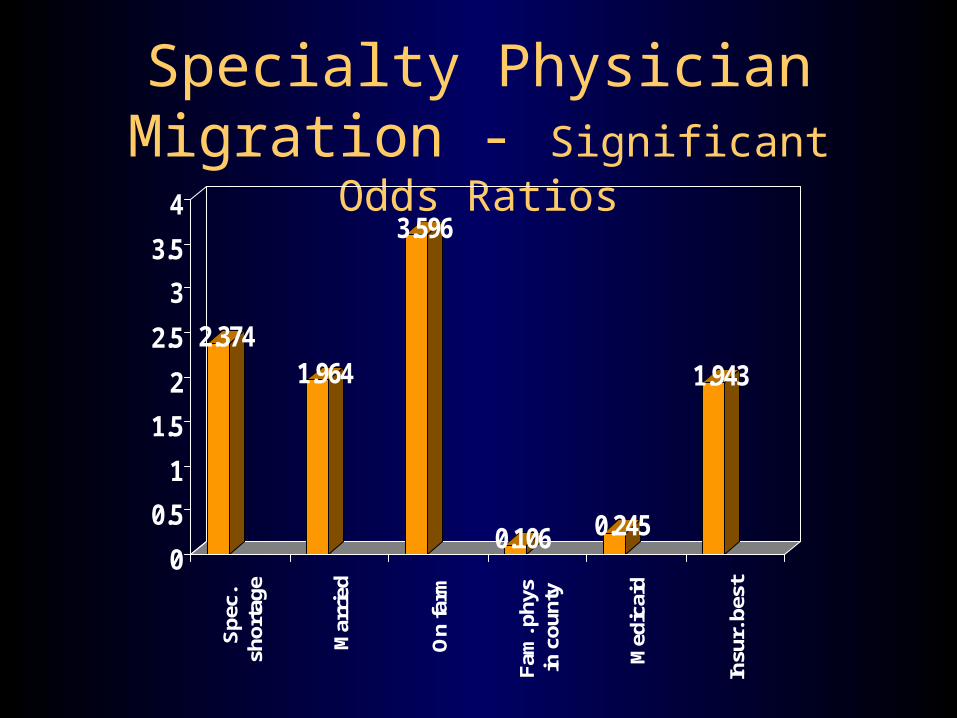
Specialty Physician Migration - Significant Odds Ratios
2.3741.964
3.596
0.106 0.245
1.943
0
0.5
1
1.5
2
2.5
3
3.5
4S
pec.
shor
tage
Mar
ried
On
farm
Fam
. phy
sin
cou
nty
Med
icai
d
Insu
r. b
est

Market Research ImplicationsMarket Research Implications
• Supply of rural physicians and health system quality– Health systems linkages– Hospital/health system ownership– Telemedicine
• Physicians needs among market segments– Target groups of migrators
(e.g. farmers, married people)
Another example: Another example: Underservice among malesUnderservice among males
• Cross-sectional survey conducted in a rural Iowa county
• Separate analyses for males and females
• Identified risk factors associated with service use to segment the market

Segmented by marital statusSegmented by marital status
0.992 0.941
2.31
1.268 1.29
3.544
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Adjusted Log Log No. of visits
Single Married

Segmented by employmentSegmented by employment
1.405 1.469
4.588
1.068 1.033
2.413
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Adjusted Log Log No. of visits
Unemployed
Employed
Strategies to attract malesStrategies to attract males
• Price (not too important in health care)
• Distribution (e.g. extended office hours)
• Product (e.g. lower office waiting times)
• Promotion