Embed Size (px)
Citation preview

Managerial EpidemiologyPart I: Descriptive Epidemiology for
Strategic Planning and Marketing
Ty Borders, Ph.D.
Assistant Professor
Department of Health Services Research & Management
Texas Tech School of Medicine

Learning objectives
– Define epidemiology– Explain the role of epidemiology in health care
management– Explain characteristics of disease transmission
and the development of disease– Calculate descriptive epidemiologic indicators– Identify health-related indicators for strategic
marketing and planning
– Identify sources of health-related indicators

Some basics: What is epidemiology?
• Study of the distribution and determinants of disease in humans
• The doctrine of what is among or happening to people
• Concerned with person, place, and time

History of epidemiology
• 1662, John Graunt – a petty merchandiser in London, publishes a report on births and deaths
in London. First to quantify disease patterns.
• 1839, William Farr– a physician, establishes system for routine compilation of no. and
causes of death in England and Wales
• 1855, John Snow
a physician, studied whether drinking water in Southwark and Vauxhall increased risk of cholera

Some subfields of epidemiology
• Social epidemiology (populations)
• Clinical epidemiology (patients)
• Genetic epidemiology (patients/populations)
• Health services epidemiology (populations/patients)
Health services epidemiology
• Study of the distribution and determinants of health-related events and states
– Utilization of health services
– Health-related quality of life
– Satisfaction with care

Managerial Epidemiology
Epidemiological methods applied to the...
– Assessment of community health for strategic purposes
– Study of the determinants of risk of poor health and overutilization of services strategic purpose
– Assessment and monitoring of health outcomes for quality improvement

Organizational mission and epi
• Children’s Hospital of Wisconsin mission statement
– Provide comprehensive health care services to children appropriate for their special needs
– Provide leadership, experience, and expertise as a community and state resources to advocate for the health and welfare of children……..

Organizational mission and epi
• Mount Sinai, Chicago
– Mount Sinai Hospital Medical Center is committed to the health and well-being of all those we serve. We accomplish this through: (1) Efficient and compassionate delivery of quality health care to our patients, regardless of their ability to pay; (2) Continuous improvement in the quality of the care and service we provide; (3) Leadership that involves and empowers our local communities in the development, advocacy, and implementation of innovative solutions to problems that affect social, economic, and individual health and well-being……...

Why apply epidemiology to strategic planning and
marketing?• Marketing orientation assumes that customer wants
and needs must be met for organizational survival (Ginter, Duncan, & Swayne, Strategic Management of Health Care Org.)
• Market share a key health care organization performance indicator (Griffith, Well Managed Community Hospital)
• But, only about 20% of hospitals are market-oriented (Journal of Health Care Marketing)

Market definition and analysis• Define market
– Geographic (counties, city, city block, zip codes)– Demographic (age, gender)– Scope of services offered (open heart surgery, hernia repairs, primary
care)– Scope of disease treated (diabetes, cancer, depression)
• Determine population size
• Estimate rate of growth – Secondary data sources– Demographic and social indicators
Customer analysis
• Forecast demand from current and new customers– Health status and demographic indicators
– Admission, discharge, and visit data
• Determine unmet health care needs– Rates of preventable diseases
– YPLL
– Social indicator analysis (median family income, % of families in poverty, % unemployed, % teenagers not in school)
– Treatment rate analysis
– Community-based surveys

Strategic Implementation
• Expansion/market development– New service areas, new delivery sites
• Expansion/product development– New products or service lines
• Contraction/decrease scope– Reduce product lines, reduce product variations
– Contraction/decrease service area– Close entire facilities, close unites, limit services to smaller
market areas.

Review: Biologic Concepts
• Agent-Host Environment– An agent interacts with a host in a particular
environment to produce disease (the epidemiologic triangle)
Host
Vector
Agent Environment

Biologic Concepts
• Agent– Infectious, pharmacological, toxicological, injury
• Environment– Biologic (reservoirs, vectors, nutrition)– Social (culture, economics)– Physical (heat, light, personal contact, crowding)
• Host– Behavior, age, genetics, physical status, immunity

Incubation or Induction Period
• The period of time between exposure to a causative agent and the appearance of first clinical manifestations
Infection
Incubation/induction/ latent period
Disease
FatalInapparen
t Mild Moderate Severe
Likely to be seen by doctorLikely to be hospitalized

Disease outbreaks
• Development and maintenance of outbreak depends upon
– Presence of pathogen in sufficient quantities
– Appropriate mode of transmission of pathogen to susceptible persons
– Adequate pool of susceptible persons exposed to pathogen

Characteristics of infectious agents• Pathogenecity
– Ability to cause detectable diseasetotal # of individuals with disease
total # of infected individuals
• Infectivity– Ability to invade and multiply in host
• Virulence– Proportion of cases of disease that result in severe
disease or death
• Immunogenicity– Ability of infection to produce immunity

Mode and source of transmission• Modes
– Person-to-person spread (direct transmission)• e.g., coughing, sexual intercourse, etc.
– Indirect transmission• vehicle born (e.g., contaminated food, water)• vector born (e.g., mosquito)• airborne
• Sources– Common source (e.g., shared water, food)
– Uncommon source (e.g., multiple persons)

Examples of routes of transmission
Agent Disease
Respiratory Cigarette smoke Lung cancer
Influenza virus Flu
Gastrointestinal Vibrio cholera Cholera
Lead Lead poison.
Sexual transm. HIV AIDS
Perinatal exposure Rubella virus Cong. Defects
Blood stream exp. Clostridium tetani Tetanus
& skin breakage
Investigation
• Calculate attack rates among different groups
• Then compare attack rates to identify those at higher risk
• Obtain more detailed information, possibly through surveys, but be aware of potential bias

Termination of disease outbreak
• Usually depends upon
– Removal or elimination of pathogen source
– Blockage of transmission process
– Elimination of susceptibility (e.g., through vaccination or medication)

Assessment of health care needs:Measures of disease occurrence
• 3 measures used to assess the frequency of disease or other health events
– Risk, also referred to as cumulative incidence
– Prevalence
– Incidence density, also called incidence rate

Risk or Cumulative Incidence
Proportion of unaffected individuals who, on average, will contract disease of interest over a specified period of time
Risk or CI = New cases
Persons at risk
R = 0 if no new occurrences arise
R = 1 if the entire population becomes infected

Risk, continued
• Risk factor– Associated with increased risk– Dose, latency, frequency, susceptibility,
multiplicity (multiple causal factors)
• Exposure– Contact with a risk factor– Dose and duration dependent– Direct or indirect
Calculation example
We are interested in the risk of acquiring a nosocomial infection. A study was conducted on 5031 patients5031 patients.
596 patients developed infection within 48 hours after admission.
R = 596 / 5031 = 0.12 = 12%

Prevalence
• Prevalence is a measure of the number of existing cases in a population
• Specifically, the proportion of a population that has a disease at a particular point in time
P = Number of cases
Number of persons in population
Prevalence, like risk, ranges between 0 and 1

Incidence rate or incidence density
• Reflects the occurrence of new cases (like risk), but also measures the rapidity with which event occurs
IR = New cases
Person time

ExamplePatient A develops a disease 2 years after entry into
study. Thus, the person-time for Patient A is 2 years.
Patients B,C,D,E an F contribute 2,3,7,2 and 6 years, respectively. Thus, the number of person-years is 2+2+3+7+2+6 = 22.
IR = new cases/ PT = 1 / 22

Summary
Characteristic Risk Prev. IR
What is Prob. % of pop. Rapiditymeasured of disease with dis. of dis.
Occurrence
Units None None Cases/person-
time
Time of disease Newly Existing Newlydiagnosis diagnosed diagnosed
Synonyms Cumulative - IncidenceIncidence Density

Survival
• Probability of remaining alive for a specific length of time
• For chronic disease, like cancer, 1-year and 5-year survival are important indicators of prognosis and severity.

Calculation of survival
Survival = A - D
A
D = number of deaths observed over a defined period of time
A = number of newly diagnosed patients under observation

Types of data
• Continuous (interval, ratio)
• Categorical (dichotomous, nominal, ordinal)– Frequency distribution– Proportion– Rate– Ratio

Types of descriptive rates
• Crude rates– Rates presented for entire population– e.g. Cancer mortality rate in 1980
(416,481 cancer deaths / midyear U.S. population)
• Category specific rates– Rates presented for individuals in specific
categories– e.g. Cancer deaths among persons 45-54

Adjusted rates
• If we are interested in the magnitude of the health problem, we don’t need adjusted rates
• If we are interested in comparing populations, we need to adjust for differences

Adjustment methods
• Take a weighted average of category-specific rates
• Direct method
• Indirect method

Pros/cons of crude, specific, and adjusted rates
Type Strengths LimitationsCrude Actual summary Difficult to interpret
rates b/c populations may
vary in composition
Specific Homogeneous Cumbersome to compare
subgroups many subgroups of 2
or more populations
Adjusted Summary statistics Fictional rates
Differences in Absolute magnitude
composition removed depends on standard
population chosen

Standardized mortality rate (SMR)
• SMR = observed deaths / expected deaths= indirect adjusted rate / crude rate of
standard pop.
• Usually expressed as a percent

Types of Incidence and Prevalence Measures
Rate Type Numer. Denom.
Morbidity rate Incidence # new nonfatal Total pop.
cases at risk
Mortality rate Incidence # deaths from Total pop.
a disease(s)
Case-fatality rate Incidence # deaths from # of cases
a disease of that disease
Period Prevalence # existing cases Total pop.
plus new cases
diagnosed during
given time period

Age-adjusted cancer morbidity and mortality rates
• All cancers Prostatic• Cervical Lung and bronchial• Colorectal Female breast• Laryngeal Pancreatic• Non-Hodgkin’s lymphoma• Skin melanoma Urinary bladder• Brain Kidney/renal• Ovarian

Age-adjusted mortality rates for other diseases
• Stroke
• Arteriosclerosis
• Diabetes
• Diseases of arteries
• Chronic obstructive pulmonary disease (COPD)
• Pneumonia and influenza rate
• Chronic liver disease and cirrhosis

Age-adjusted injury morbidity and mortality rates
• Stroke
• Arteriosclerosis
• Diabetes
• Diseases of arteries
• Chronic obstructive pulmonary disease (COPD)
• Pneumonia and influenza rate
• Chronic liver disease and cirrhosis
Crude infectious disease rates
• Syphilis incidence rate
• Chlamydia incidence rate
• Gonorrhea incidence rate
• Tuberculosis incidence rate

Youth health data
• % of live births to teens
• Fetal mortality rate
• Infant mortality rate
• Homicide mortality rate ages 15-19
• Suicide mortality rate ages 15-19
• % of extramarital live births to teens
• Founded cases of child birth

Socioeconomic data
• Per capita income
• Unemployment rate
• % of population below 200% of poverty level
• % of population with at least a baccalaureate degree
• % of population Medicaid eligible
• Population density
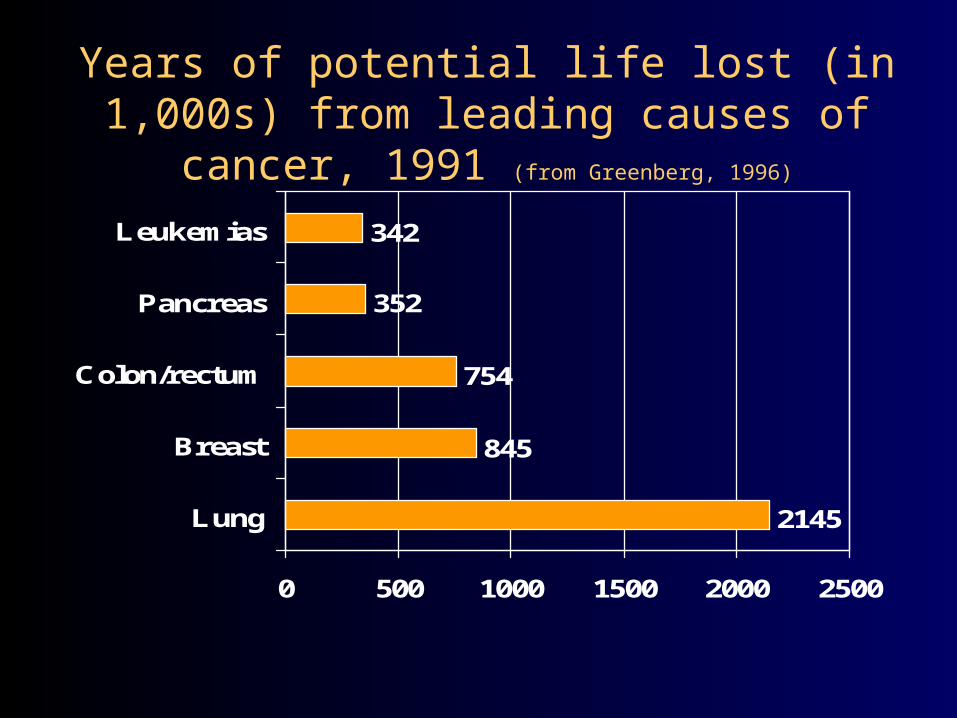
Years of potential life lost (in 1,000s) from leading causes of cancer, 1991 (from Greenberg, 1996)
2145
845
754
352
342
0 500 1000 1500 2000 2500
Lung
Breast
Colon/rectum
Pancreas
Leukemias

Years of Potential Life Lost before age 65 by cause of death (per 100,000 person years) (from Greenberg,
1996)
935
843
628
395
347
0 200 400 600 800 1000
Injuries
Cancer
Heart disease
Homicide
HIV infection

Health-Related Data Sources
• Texas Department of Health
• U.S. Census Bureau
• Centers for Disease Control
• Health Resources and Services Administration
• Surveys

Health-Related Data Sources
• Group records
– Centers for Medicare and Medicaid Services (CMS)
• DRGs
– BCBS, insurance companies, HMOs
• ICD-9 codes, CPT-codes



![MALARIA [Descriptive Epidemiology of Malaria] Dr …wp.cune.org/.../11/MALARIA-descriptive-epidemiology-of-malaria.pdfMALARIA [Descriptive Epidemiology of Malaria] Dr Adeniyi Mofoluwake](https://img.dokumen.tips/doc/110x75/5ac17de07f8b9ad73f8cf6b2/malaria-descriptive-epidemiology-of-malaria-dr-wpcuneorg11malaria-descriptive-epidemiology-of-.jpg)