Embed Size (px)
Citation preview

British Heart Journal, I972, 34) 392-395.
Atrial flutterA rare manzfestation of digitalis intoxication
B. L. Agarwal, B. V. Agrawal, R. K. Agarwal, and S. C. KansalFrom the Department of Medicine, M.L.N. Medical College, Allahabad, India
Three cases are described of atrial flutter as a result of digitalis intoxication. One of these diedduring the attempt to restore basic rhythm with intravenous propranolol. The possible mechanismof its production and rarity is discussed.
The classical atrial arrhythmia due to digitalistoxicity is paroxysmal atrial tachycardia withAV block. Atrial flutter has been universallydescribed as rare, though Chung and Thomas(i965) have included atrial fibrillation in thesame category. It was reported for the firsttime by Wedd in I924 in digitalis toxicity. Ina critical review of the cases reported till I959,CofEman and Whipple (1959) accepted I5only as truly toxic. They added one of theirown cases to the list. Since then the numberof reported cases has nearly doubled (Aravanisand Michaelides, I959; Brest, Durge, andGoldberg, I960; Soffer, I96I; Delman andStein, I964; Pomerantz and Varriale, I967;Paull and Deshpande, I967; Parameswaran,I968; Chung, I969; Lely and Van Enter,I970).We ourselves encountered 3 examples
which form the basis of this paper in a periodof 2 years during which we were activelyengaged in a prospective study of digitalistoxicity. It seems that atrial flutter as a resultof digitalis intoxication may not after all be sorare.
Case reportsCase i A 17-year-old girl suffering fromrheumatic heart disease with regular sinusrhythm and moderate congestive heart failure hadbeen on maintenance digoxin 025 mg orally perday and hydrochlorothiazide 50 mg twice a weekfor a year. Digoxin was increased to 0-5 mg dailyI5 days before admission.On admission, her pulse was II4 a minute and
regular, and the blood pressure was 120/70mmHg. Jugular venous pressure was raised to4 cm above the sternal angle with bilateral pedaloedema and tender hepatomegaly (5 cm belowthe subcostal margin). There was moderatecardiomegaly with murmurs of mitral stenosisReceived 29 June 1971.
and incompetence. The lungs showed bilateralbasal moist rales.The first electrocardiogram on admission
showed regular sinus rhythm with PR interval ofo i8 second and right ventricular and left atrialhypertrophy. Digoxin was increased to 0o75 mgdaily in addition to 50 mg hydrochlorothiazideper day. Anorexia, nausea, and headache suggest-ive of digitalis intolerance were noted on theeighth day without any cardiac arrhythmia. A daylater, on 24 April i969, pulse became irregularand the patient started vomiting. Electrocardio-gram disclosed atrial fibrillation which was con-sidered to be toxic in view of the symptoms, anddigitalis was ordered to be stopped. Oral potas-sium chloride 4 g daily was added. A tablet ofdigoxin (0o25 mg) was, however, administered tothe patient in error. The repeat electrocardiogramnext day revealed atrial flutter with regularlyplaced atrial complexes at a rate of 315 a minuteand varying AV block (Fig. I). On cessation ofdigitalis, sinus rhythm was restored 24 hourslater, while the patient continued oral potassiumchloride.
Case 2 A 25-year-old woman who had notedeffort intolerance for the past 2 years becameseverely dyspnoeic with cough and mucopurulentexpectoration after an upper respiratory infection.She was admitted with signs of congestive cardiacfailure due to tight mitral stenosis and superaddedacute bronchitis. She had not been taking digitalisbefore admission and was in sinus rhythm.The patient was digitalized orally and after
2-5 mg digoxin in 6o hours developed headache,nausea, and vomiting with irregular pulse.Electrocardiogram revealed atrial fibrillation. Theglycoside was stopped for 3 days and her toxicsymptoms subsided but atrial fibrillation per-sisted. Digoxin was restarted as fibrillation wasinterpreted to be a spontaneous development.After further administration of I 5 mg of the drugin a period of 2 days, rhythm became regular andthe tracing disclosed atrial flutter (230 per minute)with 2: I AV block (Fig. 2). Digitalis and diureticswere stopped and oral potassium chloride 4 g
on April 19, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.4.392 on 1 April 1972. D
ownloaded from

Atrialflutter: digitals induced 393
.AT . .........
FIG. I Atrialflutter (third strip) inadministration, in error, of digoxin oto toxic atrial fibrillation. First an
stnps are of pre- and post-toxic sinit(Case x). All are Vi leads.
FIG. 2 Toxic atrial flutter (atrial ja minute with 2: i AV block, 4th strpreceded by toxicfibrillation. Thereweto sinus rhythm after passing throughalation (fifth strip) and supraventricucardia i: (sixth strip). All are Vi leathat of tachycardia which is lead II
t~*1, 69
24.2.89
X7.£*$9 i 5D5| _I' l ! N t! " | §| t S ! S | g g g g zffi gi g i St: E a
I i @ 0 E :X&.., '.::s' F t+'{daily was started. Repeat electrocardiograms onsubsequent days revealed atrial fibrillation (27January I969), supraventricular tachycardia withi: i response (29 January I969), and finally sinusrhythm on 30 January I969.
Case 3 A 45-year-old man was a known case ofrheumatic mitral stenosis who was in rightventricular failure and atrial fibrillation for atleast 5 years. He had been receiving digoxin andchlorthalidone or chlorothiazide for the sameperiod.
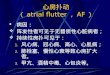
In spite of maintenance therapy with o025 mgdigoxin daily and 50 mg chlorothiazide, signsof right ventricular failure were conspicuous atthe time of admission to the hospital. He alsocomplained of loss of appetite. The possibility ofdigitalis toxicity was considered but he was con-tinued on the same doses of the two drugs as theelectrocardiogram did not reveal any toxicfeatures except for the basic rhythm of fibrillation.Five days later lassitude and nausea developed.Electrocardiogram showed atrial flutter (315 aminute) with a changing AV block (Fig. 3). Afteradministration of I12 mg atropine intravenously,propranolol in two doses of i mg each was slowlyinjected for this toxic arrhythmia. But the patient
duced after developed complete heart block with idio-)'25 mg ventricular rhythm and expired in a few minutesid last as a result of rapidly developing and irreversibles rhythms toxicity to this drug.
Comment All the three examples of atrialflutter are considered to be digitalis induced as thepatients exhibited symptoms of toxicity. Main-tenance doses of digitalis were rather more in the
rate 230 first case and an increment of glycoside wasip) w0s administered in error after development of toxicas reverszon fibrillation. Similarly in the second case toxicitrialfibril- fibrillation was considered as spontaneous rhythmJar tachy- and digitalis continued. Ventricular rates unlikerds except that of ordinary flutter were on the low side, 85 in(Case 2). the first case and 115 in the next two cases. Fatal
outcome of the third case on treatment withpropranolol may be an additional point in favourof toxicity.
DiscussionDigitalis is usually administered to patientsfor treatment of atrial flutter. It may fre-quently be the result of digitalis toxicity andthe failure to recognize it as such may giverise to serious consequences. Criteria for the
-t diagnosis of an arrhythmia stemming fromdigitalis intoxication are well laid down (Lownand Levine, I958; von Capeller, Copeland,and Stem, 1959; CofEnan and Whipple, I959;Agarwal and Agrawal, I972). In mostinstances distinction of toxic flutter from themore common PAT with AV block is easy andis based primarily on electrocardiographicfeatures of atrial rate faster than 200 aminute and the presence of saw-tooth undula-tions of the baseline in at least one lead. Doubt
JIM-
w3:-
on April 19, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.4.392 on 1 April 1972. D
ownloaded from

394 Agarwal, Agrawal, Agarwal, and Kansal
may still be cast that it may be an unrecognizedPAT with AV block (Friedberg and Donoso,I960). If atrial rate is the main criteria indistinguishing the two, authenticity of a largenumber of cases of toxic PAT with blockwhere the reported atrial rates have been ashigh as 400 (Simonson and Berman, i95i)may also be questioned. El-Sherif (1970) hasreferred to the significant overlap betweensupraventricular tachycardia with block andatrial flutter at the high rate levels. For-tunately, from the therapeutic point of view,differentiation between these two arrhythmias- if toxic - is of academic interest only. In caseof doubt it is always safer to withholddigitalis and start an intravenous infusion ofpotassium chloride, as continued use ofdigitalis may be disastrous.Even after application of stringent criteria
for the diagnosis, it may still be argued thatthe arrhythmia may be associated withdigitalis administration, and not necessarilycaused by intoxication. A number of factorsconsidered together will help to establish thetrue nature. They are the clinical set up, con-current symptoms of digitalis overdosage,ventricular premature beats, and, in the finalanalysis, rapid response to potassium in-fusion. Demonstration of ventricular ectopicbeats in the same tracing would have beenvery useful objective evidence of toxicity.However, in a series of 40 patients withspontaneous flutter, 22 per cent had prematurebeats (Lown and Levine, I958) and nearlythe same percentage of records of toxicflutter displayed the ectopics (Coffman andWhipple, I959).
It is essential to take continuous long stripsof at least 5 to 6 seconds' duration for thediagnosis of flutter. Short segments ofimpure flutter (flutter fibrillation) may have Pwaves of such uniform contour and regularitythat they may closely simulate flutter.
Mechanism According to the generallyaccepted view both atrial flutter and paroxys-mal atrial tachycardia are the result of a rapiddischarge from an ectopic focus. It is situatedmostly in the cephalic portion of the atriumnear the sinus node in patients with paroxys-mal atrial tachycardia, while in flutter it iscaudally located. There is no satisfactoryexplanation for the relative rarity of the latter.An inviting hypothesis may be that caudalportions of the atrial muscle - excluding theregion of AV node and coronary sinus - areless prone to develop automaticity and evenwhen it develops it is at a subdued rate.One is on firmer ground in explaining it on
the basis of action of digitalis on atria, which
....1......
1.10.70.3*lQ4.ite.
FIG.3 Basic rhythm - atrialfibrillation (leadVir). Toxic flutter with varying block (secondstrip). 2 mg intravenous propranolol induceda slow atrial rhythm, complete A V block withidioventricular rhythm. The last strip wasrecorded immediately before death (Case 3).
depends on which is predominant: the directmyocardial action or the indirect effectmediated reflexly through vagus. Potassiumdepletion, both as a result of toxic doses ofdigitalis and the use of potassium depletingdiuretics, results in a loss of atrial responsive-ness to the vagal influence. With the diminu-tion or abolition of this vagal effect, directmuscular action of increase in automaticity bydigitals is often exhibited. This is the basis ofthe frequent development of toxic PAT withAV block. Furthermore, digitalis by slowingconduction and lengthening the effectiverefractory period would, as a rule, precludehigh atrial rates beyond 20o a minute (Lownand Levine, I958). The infrequency of atrialflutter where atrial rates are higher than2d50 aminute is, therefore, understandable.
Propranolol, atrial flutter, and digitalistoxicity Propranolol, combined with appro-priate supplements of potassium, has beendescribed by the manufacturers (ImperialChemical Industries Ltd) in their latest manualas the treatment of choice for digitalis inducedarrhythmias. It is recommended that the drugbe given intravenously in a dose Of 3-5 mgbut may be increased up to i0 mg. Watt et al.(I970) succeeded in converting 6 Out Of 7consecutive cases of nontoxic atrial flutter intosinus rhythm by a combination of digoxin andpropranolol and consider it to be more effec-
on April 19, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.4.392 on 1 April 1972. D
ownloaded from

Atrial flutter: digitalis induced 395
tive than existing forms of drug therapy. Thesenior author Watt (I968) had also reportedearlier the hazards of treating 2 cases ofarrhythmia caused by digitalis intoxicationwith small doses of oral propranolol. One oftheir patients expired in a few hours and theother was rescued just in time by administra-tion of atropine sulphate. Our third case diedin spite of pretreatment with atropine. Thesolitary example of this series gives support tothe recommendations of Watt (I968) thattreatnent of toxic arrhythmias should beinitiated with a small test dose of 5 mg oreven less of oral propranolol.
ReferencesAgarwal, B. L., and Agrawal, B. V. (1972). Digitalis
induced paroxysmal atrial tachycardia with A-Vblock. British Heart_Journal.
Aravanis, C., and Michaelides, G. (1959). Paroxysmalauricular flutter and right bundle-branch blockfollowing digitalis therapy. American Journal ofCardiology, 4, I24.
Brest, A. N., Durge, N. G., and Goldberg, H. (I960).Conversion of atrial fibrillation to atrial flutter as amanifestation of digitalis toxicity. AmericanJrournal of Cardiology, 6, 682.
Chung, E. K. (I969). Digitalis Intoxication. ExcerptaMedica, Amsterdam.
Chung, E. K., and Thomas, J. (i965). Arrhythmiascaused by digitalis toxicity. Geriatrics, 2o, I006.
Coffman, J. D., and Whipple, G. H. (I959). Atrialflutter as a manifestation of digitalis toxicity.Circulation, i9, I88.
Delman, A. J., and Stein, E. (I964). Atrial fluttersecondary to digitalis toxicity: report of 3 casesand review of the literature. Circulation, 29, 593.
El-Sherif, N. (I970). Supraventricular tachycardiawith AV block. British Heart Journal, 32, 46.
Friedberg, C. K., and Donoso, E. (I960). Arrhythmiasand conduction disturbances due to digitalis. Pro-gress in Cardiovascular Diseases, 2, 408.
Lely, A. H., and Van Enter, C. H. J. (1970). Largescale digitoxin intoxication. British MedicalJournal,3, 737.
Lown, B., and Levine, H. D. (I958). Atrial Arrhyth-mias, Digitalis and Potassium. Landsberger MedicalBooks, New York.
Parameswaran, R. (I968). Atrial flutter due to digitalistoxicity. Cardiologia, 53, 57.
Paull, A. M., and Deshpande, S. Y. (i967). Atrialflutter with complete AV heart block due todigitalis toxicity. Report of a case. Unique case iscontrolled by withholding digitalis. Rhode IslandMedical,Journal, 50, 258.
Pomerantz, B., and Varriale, P. (I967). Atrial flutter asmanifestation of digitalis toxicity. New York StateJournal of Medicine, 67, 713.
Simonson, E., and Berman, R. (ig5i). Differentiationbetween paroxysmal auricular tachycardia withpartial AV block and auricular flutter. AmericanHeart_Journal, 42, 387.
Soffer, A. (I96I). The changing clinical picture ofdigitalis intoxication. Archives of Internal Medicine,107, 68I.
Somlyo, A. P. (I960). The toxicology of digitalis.American Journal of Cardiology, 5, 523.
von Capeller, D., Copeland, G. D., and Stem, T. N.(I959). Digitalis intoxication: a clinical report of148 cases. Annals of Internal Medicine, 50, 869.
Watt, D. A. L. (I968). Sensitivity to propranolol afterdigoxin intoxication. British MedicalJournal, 3, 4I3.
Watt, D. A. L., Livingstone, W. R., MacKay, R. K. S.,and Obineche, E. N. (1970). Use of propranolol inatrial flutter. British Heart,Journal, 32, 453.
Wedd, A. M. (1924). Clinical auricular flutter. Annalsof Clinical Medicine, 3, 69.
Requests for reprints to Professor B. L. Agarwal,4 Professor's Bungalow, Medical College Enclave,Allahabad, India.
on April 19, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.4.392 on 1 April 1972. D
ownloaded from