Embed Size (px)
Citation preview

ECG of the week
-Dr. Prof Mageshkumar’s Unit
Devendra Patil

Daniel , 50 / M came with chief complains of
Palpitations since 2 hrs
chest pain since 2 hrs
ECG was taken:


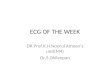
• ECG:Atrial rate 300Heart rate 75/minRegular rhythm4:1 constant blockNo iso electric baselineSaw tooth appearance in inferior leadsRsr’ in v1
Impression:Atrial flutter with incomplete RBBB

Atrial Flutter
• Mechanism:
macro re-entrant tract in the atria
• Types:
- right / left re-entrant tract
- counterclockwise / clockwise tract
- typical /reverse typical / atypical
- regular / irregular rhythm
- isthumus dependent / non dependent (recent)
Typical atrial flutter
• Pathway:
in the typical form the re-entrant wavefront moves from up in the interatrial septum and then down the free right atrial wall. i.e. counterclockwise
• Tract location :
cavo – tricuspid isthumus


• ECG Findings:
Atrial complexes of constant morphology polarity and cycle length
Presence of Flutter ( F ) wavesPicket fence appearance of F wavesSaw toothed appearance of F wavesNo iso-electric base lineUsually the atrial rate is 300 / min and there is a 2:1
block , so heart rate is 150 / minTypically leads II III and avF show negative F wavesLead V1 shows positive F waves and this may be
confused with sinus tachycardia

• ECG findings:
Very rapid Venticular rates makes ECG diagnosis difficult
The F waves may superimpose on the terminal QRS and the T waves and make the diagnosis difficult
Use of vagal manuovers or Inj. Adenosine to transiently increase the AV delay may unmask the flutter waves
Clockwise Atrial flutter:positive waves in inferior leads and V1 shows
a biphasic or sometimes negative F waves

Few more ECGs





Etiology
• First week after open heart surgery
• COPD
• Mitral or tricuspid valve lesions
• Thyrotoxicosis
• Surgical correction of congenital heart disease
• Right atrial enlergement

Treatment
• Acute:cardioversion
• Longtermanti-coagulation ( similar to AF )anti-arrhythmics Catheter ablation of tractpacemaker insertion

Cardioversion
• External trans thoracic syncronised DC shock is highly effective
• Intravenous Ibulitide or procainamide can also be used
• Care should be taken during use of class 1 esp 1C agents because they may slow the atrial rate and an inadequately suppressed AV node may give way to 1:1 conduction leading to high rates and circulatory collapse.


Long term treatment