-
British Heart Journal, 1972, 34, 12I5-I224.
Electrical conversion of atrial flutter to
atrialfibrillationFlutter mechanism in man
,Timothy E. Guiney,2 and Bernard LownFrom the Cardiovascular
Research Laboratories, Department of Nutrition, Harvard Schoolof
Public Health; and the Levine Cardiac Unit, Cardiovascular
Division, Department ofMedicine, Peter Bent Brigham Hospital,
Boston, Mass., U.S.A.
b0.
If human atrial flutter is due to re-entrant excitation,
depolarization as well as repolarizationmust continue throughout
the entire atrial cycle. It follows that the atrial vulnerable
period forinducing atrial fibrillation is also continuous rather
than discrete. This hypothesis was examinedduring cardioversion of
I33 patients with atrial flutter who received 280 low-energy
shocks. Acomposite analysis of these patients demonstrated that all
intervals of the flutter cycle wereequally susceptible to
shock-induced atrial fibrillation. The optimal energy was found to
be ioWsec. The development of atrialfibrillation was independent of
the state of digitalization and wasnot prevented by pretreatment
with atropine or propranolol. These findings are consistent
withre-entry as the basic mechanism of human atrial flutter.
Attempts to clarify the mechanism of atrialflutter have engaged
the energies of numerousphysiologists and clinical investigators
overmore than half a century. Polemics have ragedas to whether the
arrhythmia is sustained by a
e single discharging focus or by a circulatingwave front of
depolarization. In the experi-mental animal there is persuasive
evidencethat a flutter-like arrhythmia can result fromeither of
these mechanisms. When protoplas-mic irritants such as aconitine
(Hayden, Hur-ley, and Rytand, I967; Ishikawa, I967;Prinzmetal et
al., I952; Scherf, I947; Scherfand Terranova, 1949; Scherf, Romano,
and
i Terranova, I948) or delphinine (Scherf et al.,I960; Scherf,
Blumenfeld, and Yildiz, I963)are applied to the atria, the ensuing
flutter-like disorder emanates from the site of drug%pplication.
The extensive investigation ofThomas Lewis (1925) adduced evidence
thatAutter might also result from a circus move-,.ment. Decisive
corroboration was providedby the experiments of Rosenblueth and
GarciaRamos (i947). They were able to initiate and
Oteceived 24 April 1972.1 Supported in part by grants from the
National Insti-tutes of Health, U.S. Public Health Service; and
theFund for Research and Teaching, Harvard School of.iublic Health,
Department of Nutrition.2 Present address: Cardiac Catheterization
Laboratory,Massachusetts General Hospital, Boston, Mass. U.S.A.
maintain a circulating wave front around anobstacle in the right
atrium produced by acrush between the vena cavae. The relevanceof
these animal models to the disorder en-countered in man remains
uncertain.The hypothesis in current favour is that
clinical flutter is due to a re-entrant mechan-ism. As
classically formulated by Lewis(I925), an advancing front of
depolarization isseparated from its tail of refractoriness byfully
recovered tissue, the so-called excitablegap. Some portions of the
atria are, therefore,undergoing depolarization at all times,
whileother portions are either in a state of refrac-toriness or
completely repolarized. It wouldbe inferred that if flutter is the
result of re-entry, vulnerability to fibrillation should alsobe
present throughout the cardiac cycle. Bycontrast, in the presence
of sinus or singlefocus ectopic tachycardia, the vulnerableperiod
is located in a discrete part of the car-diac cycle and is of brief
duration (Lown,Kleiger, and Williams, I965).The opportunity to test
the extent of the
vulnerable period in patients with atrial flutterpresents itself
during cardioversion of thisdisorder to sinus rhythm. Low energy
elec-trical discharges may convert flutter to atrialfibrillation
(Lown, I967). The vulnerableperiod is generaly activated by a
narrowrange of low discharge energies. If the trans-
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
I2I6 Guiney and Lown
TABLE I Underlying heart disease in 144patients with atrial
flutter subjected tocardioversion
Disease No. ofpatients
Rheumatic heart disease 53Coronary artery disease 32Lone flutter
23Pulmonary disease I2Congenital heart disease 9Hypertensive heart
disease 4Pericarditis 4Other 7
formation in atrial rhythm from flutter tofibrillation is
dependent upon the stimulusexciting the atria during their
vulnerableperiod, only a limited range of energies shouldbe shown
to be effective. If the mechanism ofatrial flutter is due to
re-entry, it should bepossible to produce atrial fibrillation by
asingle electric shock from any part of thecardiac cycle. The
present clinical study pro-vides information relating to each of
thesequestions.
MethodsThis study involved cardioversion of i44 con-secutive
patients with atrial flutter admitted to thePeter Bent Brigham
Hospital between AugustI962 and July I970. There were 96 men and
48women. The patients ranged in age from I9 to 89years. Table I
lists the cardiovascular diseasesencountered.The technique for
cardioversion has been
described previously (Lown, Amarasingham, andNeuman, i962a;
Lown, Kleiger, and Wolff, I964).A DC cardioverter was employed, and
the elec-trode paddles were positioned anteroposteriorly.All
patients were pretreated with IOO mg pento-barbitone sodium given
orally one to two hours
TABLE 2 Energy content of initialtransthoracic cardioversion
shock administeredto 133 atrial flutter patients
Energy (Wsec) Shocks (No.) Per cent
I 45 24.85 35 I9.3
I0 20 II225 28 I5.550 44 24-3iooand > 9 4-9
Total I8I* 100
* Some patients were subjected to cardioversion morethan once,
thus accounting for the additional 48 initialshocks.
before the procedure. Anaesthetics included thio-pentone sodium,
methohexitone sodium, com-binations of pethidine hydrochloride and
pento-barbitone sodium or pethidine hydrochloride andpromethazine
hydrochloride. Over the past fouryears diazepam was used almost
exclusively. In6I patients, the doses ranged from 2-5 mg to 40mg,
with a mean dose of I3-5 mg. An initial doseof 2-5 mg to 50o mg
intravenously was followedby 2-5 mg increments every two minutes
untillight sleep was induced. Blood pressure waschecked between
successive doses.A complete i2-lead electrocardiographic
tracing
was recorded before the cardioversion procedure.The standard
limb lead with the most distinctflutter waves was selected for
monitoring through-out the procedure. In the majority of cases,
leadII was employed. A special damping circuit pro-tected the
electrocardiographic recorder and re-sulted in an isoelectric
artefact lasting an averageof i-8 seconds. After each shock, the
cardiacmechanism was identified in lead II; the rhythmwas then
confirmed in lead Vi. This was gener-ally accomplished within 5 to
IO seconds afterthe emergence of the first post-shock complex.One
of four types of response was identified:(i) persisting atrial
flutter, (2) atrial fibrillation,(3) normal sinus rhythm, (4)
junctional or othermechanisms. Of the 299 cardioversion
shocksemployed, I9 shocks in ii patients were excludedfrom analysis
because of the presence of electricalartefacts or uncertainty as to
the underlyingrhythm. Thus, the analysis to be described wascarried
out on the response to 280 shocks in 133patients.At the beginning
of this study all cardioversions
were carried out with an initial setting of IOOWsec. As it
became evident that atrial fluttercould be reverted with lesser
energies, the initialdischarge energy was progressively reduced.
Dis-tribution of energies of the first shock adminis-tered to the
I33 patients in this study is shown inTable 2. In 55.3 per cent,
the initial shock was IOWsec or less. If sinus rhythm did not
result, theenergy content of successive shocks was in-creased. The
following sequence was usually em-ployed: i Wsec, 5 Wsec, IO Wsec,
25 Wsec, 50Wsec, 200 Wsec, 300 Wsec, 400 Wsec. If noreversion to
sinus rhythm occurred with a 400Wsec discharge, the procedure was
stopped. In 5patients, the clinical objective of cardioversionwas
to change the rhythm to atrial fibrillation:this was accomplished
with low energy shock.The location of the cardioversion discharge
in
the flutter cycle varied in different patients. Twofactors
determined where the shock fell in relationto the flutter wave,
namely the degree ofAV blockand the voltage rise time of
ventricular depolariza-tion which triggered release of the electric
dis-charge. Analysis of the location of the electricaldischarge in
relation to the flutter wave was car-ried out on records of I59
shocks delivered to 79patients. These were selected because the
flutterwave, designated as P', could be precisely defined.The
interval between the nadirs of successiveflutter waves in lead II
(P'P') was measured in
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
Atrial flutter 1217
milliseconds. The point of interception of thisinterval by the
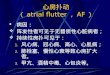
shock, designated as S, providedthe P'S interval. The ratio of
these two intervals,P'S/P'P', defined the position of the
electricaldischarge in the flutter cycle. P'S/P'P' ratios
weredivided into quartiles. Thus, if the shock felli6o milliseconds
after the nadir of the P' waveand the P'P' interval was 200 msec,
the resultingratio was I60/200, or o8o. This was grouped withall
ratios occurring in the quartile of 0-75 too099 (Fig. i).To
determine whether the emergence of atrial
fibrillation was related to shock-induced releaseof neurohumoral
agents (Amory and West, I962;Blinks, I966; Cobb, Wallace, and
Wagner, I968;Nelemans, I95I; Ten Eick et al., I967; Vincenziand
West, I963; Whalen, Fishman, and Erickson,1958), selected patients
were pretreated witheither atropine or propranolol. Twelve
patientsreceived atropine intravenously, in doses of o-6tO 2-2 mg,
five minutes before administering thecardioversion discharge. Ten
patients were givenoral propranolol, in doses ranging from 30 mg
to200 mg daily, for two days preceding cardiover-sion, as well as
on the day of the reversion. Onepatient, subjected to cardioversion
on two differentoccasions, received both atropine and
propranolol.Necessarily, these patients were receiving otherdrugs
that may have influenced the result ofcardioversion. Of the 133
patients, ii6 were onmaintenance digitalis therapy, ii had not
receivedcardiac glycoside at any time, and in 6, digitalishad been
discontinued five or more days beforecardioversion. Seventy-eight
patients were pre-treated with quinidine, in a dose of o-8 to I-2
g,for the 24- to 48-hour period preceding thereversion
procedure.
Results
The 133 patients with atrial flutter received280 transthoracic
shocks. Of this number, 82resulted in atrial fibrillation and 96
wererestored to sinus rhythm; the flutter mechan-ism persisted
after 87 shocks and in I5 thereensued a junctional or an
unidentifiablerhythm. An example of induction of atrialfibrillation
is illustrated in Fig. 2. The medianshock energy which resulted in
atrial fibrilla-tion was io Wsec (Table 3). A high incidenceof
atrial fibrillation was also observed afterdischarges of 5 Wsec.
When results of shocksat these two energies are combined, out of
Ioidischarges 49, or 48 5 per cent, resulted inatrial fibrillation.
Provocation of atrial fibrilla-tion diminished as the energy
content of theshock was increased.
After many of the shocks sinus rhythm,junctional rhythm, or some
other mechanismdeveloped precluding the emergence of
atrialfibrillation. The data were therefore analysedto exclude
those who had these rhythmalterations. Only those shocks that were
fol-
P'-S/P'-P' RATIO
P'-s 160
~0.80
CardioversionShock (S)
l.
P 160 msec
i200msec
i200msec i 200msec i 200msec i
FIG. i The P'S/P'P' ratio was calculated asindicated in this
figure.
lowed by either atrial fibrillation or persistingatrial flutter
were included. The energy mosteffective for inducing atrial
fibrillation wasIO Wsec, with 66-7 per cent of subjects whoreceived
this energy developing atrial fibrilla-tion. There was a stepwise
reduction in occur-rence of atrial fibrillation at lower and
highershock energies (Fig. 3). There was an increasein incidence of
atrial fibrillation at energies ofIOO Wsec or greater; however,
only IO shockswere available for the analysis. The existenceof a
specific effective energy was shown strik-ingly in one patient.
After i and 5 Wsec dis-charges, the atrial flutter remained
unaltered.After IO Wsec the mechanism persisted, how-
FIG. 2 Patient with chronic atrialflutter ata rate of 300 a
minute. After a 5 Wsecshock synchronized to discharge in the
QRS,atrial fibrillation ensued and is clearly seen inlead Vi. (In
this and subsequent figuresnotation for watt seconds is WS.)
A. Flutter5WS Shock
I Atriial Fibrillation444W K44.:. .-4-X :1--J4 &--2~2I.;4-l
:I|- -LJJ; I -LII-
Atriol Rate 300d .
!tz!f b±L-FH:!-IT- LU
V-1.-Li-.--T
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
I2i8 Guiney and Lown
ever, the wave form was changed and theatrial rate increased
slightly. When the energyof the next shock was reduced to 2-5
Wsec,atrial fibrillation resulted (Fig. 4). The factthat atrial
fibrillation was produced at aspecific low energy suggested that
this phe-nomenon was related to the atrial vulnerableperiod.The
next question examined was whether
the vulnerable period was discrete or con-tinuous. The point at
which the electricaldischarge intercepted the flutter
cycle(P'-S/P'-P' ratio) was examined after I09shocks which either
resulted in atrial fibrilla-tion or continued as atrial flutter
(Table 4).When the cycle was divided into quartiles,it became
evident that no part of the fluttercycle was impervious to the
development ofatrial fibrillation. In fact there was no
statistic-ally significant difference between quartiles(X2
analysis, P = os5). Similar results were ob-tained for shocks of I0
Wsec or less. Thesefindings indicated that there was no
distinctpart of the flutter cycle that was exclusivelysusceptible
to the provocation of atrial fibrilla-tion by electrical
discharge.
It is possible that the occurrence of atrialfibrillation was
related to release of neuro-transmitter by the cardioversion
discharge.This question was, therefore, examined in asmall group of
patients.
Atropine Twelve patients were given atro-pine in doses of o6 to
2-2 mg intravenouslywithin five minutes before cardioversion.
Atotal of 25 shocks was delivered. Of these, iishocks resulted in
atrial fibrillation, 5 in sinusrhythm, and 9 remained in atrial
flutter. Thus,in 55 per cent of patients given atropine
atrialfibrillation followed a transthoracic discharge.The median
effective energy in this group wasalso io Wsec (Fig. 5).
Propranolol Ten patients received a totalof 20 shocks at a time
when they were receiv-ing propranolol hydrochloride in doses
rang-ing from 30 mg to 200mg daily. Atrial fibrilla-tion followed
atter five shocks, sinus rhythmafter seven, and the rhythm remained
un-altered after eight. One patient was twice sub-jected to
cardioversion while pretreated withboth atropine and propranolol.
On each occa-sion i Wsec was without effect; 5 Wsec duringthe first
cardioversion and I0 Wsec duringthe second resulted in atrial
fibrillation(Fig. 6).
Since it has been shown that cardioversionenhances the
arrhythmogenic action of digi-talis (Lown et al., I965; Kleiger and
Lown,i966), the possible role of digitalis glycosides
TABLE 3 Result of 280 shocks delivered to133 patients with
atrial flutter as function ofenergy of electrical discharge
Energy of Number of Responseshock (Wsec) shocks at
each energy Atrial Sinus Persisting Otherfibrillation rhythm
flutter rhythms
I 48 I3 3 32 05 56 27 5 24 0I0 45 22 9 I I 325 50 13 25 8 450 59
3 43 6 7iooand > ioo 22 4 II 6 I
Total 280 82 96 87 15
in the emergence of electrically induced atrialfibrillation was
examined. Only patients onmaintenance digitalis therapy but not
receiv-ing quinidine were examined. This groupincluded 55 patients
who were subjected to 83cardioversion shocks. In 28, or 34 per
cent,atrial fibrillation resulted. A nearly identicalresult was
observed in I0 patients whoreceived neither digitalis nor
quinidine; atrialfibrillation followed 37 per cent of the
shocks.
DiscussionThe mechanism of human atrial flutter re-mains
undefined. Two major and opposingtheories have long held sway,
namely, thatthe underlying basis is a rapid firing of anectopic
focus or, that it results from circusmovement or re-entry of an
entrapped wave.The arguments in favour of each of thesehypotheses
have been extensively reviewed(Hecht et al., I953; Katz and Pick,
I960;Rytand, I966; Scherf, Schaffer, and Blumen-feld, I953).
TABLE 4 Distribution of cardioversion shocksin quartiles
offlutter cycle expressed as ratioin P'S/P'P'
Quartiles of P'P' cycle
0 00-0 24 0o25-049 0o50-074 0 75-0 99
A. Total no. of shocks i8 I7 39 35No. with atrial fibrillation 7
I0 22 I7% Atrial fibrillation 39 59 57 49
B. Total no. of shocks I3 I3 27 25No. with atrial fibrillation 4
8 12 II% Atrial fibrillation 3I 62 44-5 44
Data based upon an analysis of I09 shocks in 79 patients, of
which 56 resulted inatrial fibrillation. (A) represents all
energies employed, while (B) only energies ofI0 Wsec or less. (The
differences are not statistically significant.)
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
Atrial flutter 1219
At the turn of this century, the Americanmarine biologist, A. G.
Mayer, induced a con-tinuous recirculating wave of excitation in
aring of tissue cut from the bell of the largemedusa, Cassiopea
(Mayer, I906). In onespecimen the pulsation persisted for ii
days'Mayer, I9I6). Some years later, Mines (I9I3)Lnduced a similar
circulating wave of contrac-tion in the tortoise heart from which
the sinusvenosus had been excised. He noted that, 'the:ontractions
are easily upset by the occurrenceDf an extrasystole'. The term
'circus contrac-tion' was introduced by Garrey (I914), whoroted
that a critical mass of heart muscle wasrequired and who also
recognized the import-mnce of a localized depression in
conductionas a condition favouring such arrhythmia.
It was Thomas Lewis (1925) who providedthe essential theoretical
frame of modem:hinking on re-entrant rhythms. He amassedi wealth of
data derived from galvanic stimu-[ation of dog atria and from
analysis of-lectrocardiographic records of patients withriutter. In
animals having atrial flutter, as thebrief after-effect of rapid
electrical stimula-tion, Lewis, Feil, and Stroud (1920) exploredthe
arrival of the depolarization wave at vari-)us atrial sites. They
concluded that some newpart of atrial muscle was activated
throughoutthe entire atrial cycle and that the propagatedexcitation
traversed a fixed pathway aroundthe orifices of the vena cavae. A
limitation ofthese studies was the failure to define themntire
pathway of excitation in the left atrium.Modern techniques have
permitted Kimura?t al. (I954) to remedy this deficiency inmethod
and confirm Lewis's conclusions.
Investigation of the arrhythmia in man wasmore indirect and
consisted of mapping thetime course of the flutter wave by
determiningthe change in atrial electrical axis during the-ardiac
cycle (Lewis, Drury, and Iliescu,[92I). As studied by vectorial
analysis, themanifest atrial potential appeared to rotate3600. This
circulation was believed to accountFor the continuous undulation of
the electro--ardiographic baseline seen in cases of purelutter
(Lewis et al., 1920). Prinzmetal et al.:195i) later challenged this
interpretation.rhey ascribed baseline motion not to circusnovement,
but to the sequence of depolariza-ion and repolarization which
altered direction)f the atrial vector.Attempts to define the
flutter mechanism
n man have since been largely directed tonapping the time course
of arrival of the-xcitation wave described by Lewis to travel.pward
in the left atrial wall and downwardn the taenia terminalis of the
right atrium*Lewis, I925). Since vectorial analyses have
Trotal Shocks8 L.A.J
8R *Effective Shocks
6060
40is. k 111 I t1 [email protected] 5 10 25 50
ENERGY OF DISCHARGE (w/S
FIG. 3 Incidence of atrialfibrillation afterdifferent energy
shocks tabulated both aspercentages of total shock and of
effectiveshocks, i.e. those shocks that were followed byeither
persistent atrial flutter or developmentof atrial fibrillation (see
also Table 3).
yielded conflicting results (Cabrera and SodiPallares, 1947;
Duchosal and Sulzer, 1949),many studies aimed to achieve greater
prox-imity by means of oesophageal and right intra-atrial
electrodes (Duchosal and Sulzer, I949;Enselberg, I95I; Giraud,
Latour, and Puech,1955; Grishman et al., 1950; Groedel andMiller,
I950; Kato et al., I956, I957; Koss-mann and Berger, I941;
Prinzmetal et al.,1953; Rosenblueth, I953; Rytand, I966;Wenger and
Hofmann-Credner, I952). Oeso-phageal electrocardiography confirmed,
in
FIG. 4 Shocks of Io Wsec (5 Wsec and IWsec not shown) failed to
induce atrial fibrilla-tion though there occurred a slight
accelerationin atrial rate and change in atrial morphology.After
2-5 Wsec atrial fibrillation resulted.
Atnral Rate236
lOws Atrial Rate244
i I I Iil1. /--J ..Q ..AV.. V4: 1, . I-J.-vlol-.
230 2.5ws atrial fibrillation
2.~~~~~~~~.o
................
......
...............
........
........
100+
VI
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
1220 Guiney and Lown
most cases, a caudocephalic direction of thedepolarization wave
in the left atrial wall,though the opposite direction was
occasionallynoted (Cabrera and Sodi Pallares, I947; Du-chosal and
Sulzer, I949; Enselberg, I95I;Grishman et al., I950; Kossmann and
Berger,I94I; Prinzmetal et al., I952). Direct mappingof the path of
the excitation wave was onlyrarely attempted and the results have
beeninconclusive (Groedel and Miller, I9so;Prinzmetal et al.,
1953).
Recently Kishon and Smith (I969) haveaddressed themselves to
this question. In I0patients with flutter, they timed arrival of
theintrinsic deflection by recording simultane-ously from
oesophageal and right atrial elec-trodes at different levels. In 4
patients, atrialactivation progressed cephalad in the leftatrium
and caudad in the right atrium.Though exploration of the excitatory
pathwaywas incomplete, almost two-thirds of the atrialcycle could
be defined. They judged thesefindings to be consistent with a
circus move-ment. In the 6 other patients no such sequencewas
recorded, the excitation wave occupiedonly one-third of the atrial
cycle and spreadcephalad simultaneously in both atria.
Theyconcluded that two mechanisms operated inhuman flutter. Kishon
and Smith (I969)acknowledged that if the circus pathway waslocated
low in the atrium, it would not havebeen detected by the techniques
employed intheir investigation.The present study of the flutter
mechanism
is also indirect but is based upon an entirelydifferent
approach. The ability to convertflutter to fibrillation at a
discrete low energysuggests excitation of an atrial
vulnerableperiod. The observation that vulnerabilityis present
throughout the entire atrial cyclesuggests that this is also true
for the atrialdepolarization-repolarization sequence. An-drus,
Carter, and Wheeler (1930) first showedthat the dog's atrium
possessed a sharply de-marcated vulnerable period. Single
electrical
E£ er gy5ws
lmg Atropine L.V.
FIG. 5 After i mg atropine intravenously 5Wsec shock did not
alter flutter mechanism;however, a IO Wsec discharge induced
atrialfibrillation.
pulses when discharged during this time inter-val of the cardiac
cycle produce atrial fibrilla-tion. Electrophysiologists (Brooks et
al., I95I)have confirmed the existence of such a discretezone in
the atrium, which coincides with thedip in the atrial excitability
curve. Lown (un-published data) looked for the atrial vulner-able
period in the intact dog with transthor-acic shocks and found it to
have a duration ofI0 to 20 msec, with i Wsec being the
optimalenergy. The vulnerable period was locatedconsistently during
inscription of the terminalportion of the QRS complex.There has
been no systematic exploration
for an atrial vulnerable period in man. Atrialfibrillation at
times has been noted to occurduring right atrial pacing (Ross,
Linhart, andBraunwald, I965). In a retrospective analysis,Haft and
coworkers (I968) found 26 episodesof atrial fibrillation or
flutter-fibrillation in 3normal subjects during single or paired
pacingof the right atrium. The interstimulus intervalor the
P-stimulus interval for initiatingarrhythmia was the same and
ranged fromi8o to 280 msec. In over 2oo other patients,atrial
fibrillation was never seen during right
FIG. 6 In a patient pretreated with both atropine and
propranolol, atrial fibrillation was notprevented after a 5 Wsec
cardioversion discharge.
5WS
L I
Lead ]3:
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
Atrial flutter 1221
atrial pacing outside this time period. Addi-tional support for
an atrial vulnerable periodderives from the findings of Killip and
Gault(I965) that atrial premature beats which occurearly in the
cycle are associated with a highincidence of atrial
fibrillation.
Is a vulnerable period present when sinusrhythm is replaced by
an ectopic tachycardia ?No data are available for atrial
tachyarrhyth-mias. However, the vulnerable period appearsunaltered
when the mechanism is ventriculartachycardia. Lown et al. (I965)
explored thecardiac cycle with low energy cardioversionpulses
during ventricular tachycardia inducedby digitalis overdose. They
found a singlesharply demarcated vulnerable period for pro-ducing
ventricular fibrillation which was ofthe same duration and energy
threshold asdetermined during sinus rhythm. It thereforeappears
that when a tachycardia emanatesfrom a single ectopic site, it is
associated witha discrete rather than a continuous
vulnerableperiod. If repetitive discharge from a singleectopic
focus accounted for atrial flutter inman, a similarly circumscribed
period of atrialvulnerability should have been observed.
Thecontrary findings of the present investigation,that fibrillation
could be induced equally wellthroughout the atrial cycle, is thus
consistentwith the circus movement hypothesis.A limitation of the
present study needs to
be emphasized. The presence of a continuousvulnerable period in
atrial flutter was deducedfrom a composite view derived from
manydiscrete observations, where each patient pro-vided but a
single point of datum. It was notbased on a systematic exploration
of the entireflutter cycle in a single individual. Even ifthis were
ethically permissible, it would havebeen difficult to accomplish.
Since there wasfrequently but one chance to test for
vulner-ability, once atrial fibrillation was induced, themechanism
usually persisted or reverted tosinus rhythm. There is, however,
additionalevidence to support the concept that thechange from
flutter to fibrillation was due tostimulation of an atrial
vulnerable period. Ifthis rhythm alteration was simply a
shock-induced disorganization in heart rhythm, itwould have varied
directly with the energyof discharge. This is the case when long
ACpulses are administered transthoracically(Lown et al., i962b).
While at 75 volts theincidence of atrial fibrillation is 40 per
cent, itprogressively increases reaching ioo per centwith a shock
level of 450 volts. On the otherhand, when single short DC pulses
are de-livered to the heart during the atrial or ven-tricular
vulnerable period a narrow range oflow energies exists which is
optimal for induc-
2
Atrial rate236
-tF4-- - ia, *: -*~~~~~~~~~~~~~~~~~~~~~~~~~ ' I -
+s..-.jM'-:=::-':11=.n'-Ls;;_.
240
FIG. 7 Low energy cardioversion dischargechanged direction
offlutter wave withoutsignificantly altering atrial rate.
ing fibrillation. In the present study, the peakincidence of
atrial fibrillation occurred at IOWsec, with less effectiveness
resulting fromeither lower or higher energies.A phenomenon
encountered in 5 of the
patients lends additional support to the circusmovement
hypothesis. After a low energyshock the flutter mechanism
persisted, butcloser inspection of the electrocardiographicrecord
revealed a change in morphology of theatrial complex. In fact the
flutter waves werea mirror image oftheir former contour (Fig. 7).An
additional shock at a higher energyresulted in atrial fibrillation.
It is difficult toexplain this occurrence if the arrhythmia
re-sulted from discharge of an ectopic pace-maker. One would have
to entertain a numberof assumptions, namely, the existence of
twoectopic sites, one held in abeyance by theother and both
discharging at nearly identicalrates, furthermore, that they were
situated atopposite atrial poles to permit a precise mirrorimaging
in wave form. If one holds to thecircus movement hypothesis, such
compound-ing ofimprobable assumptions is unnecessary.A reversal of
direction of the entrapped wavefrom counterclockwise to clockwise,
whenviewed sagittally from the left, would accountfor the
observation.A significant question is the frequency with
which a circus movement operates as themechanism of atrial
flutter in man. The pre-sent study provides some information. At
themost effective energy of IO Wsec, 22 out of33 episodes, or 66f7
per cent resulted in atrialfibrillation. It is possible that IO
Wsec wasnot the optimal energy in the ii patients inwhom failure
was encountered at this energysetting. Indeed, in 6 of the iI,
atrial fibrilla-tion was produced at either higher or lower
L II:T I ; ji.-.1.....-.:. : : -: --
.-.1 . I. .... ..... - il - , 1;-; ItA,ki -.1.I-T' -t I4
-4 .... .... ... ....
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
1222 Guiney and Lown
energy settings, while in the remaining 5sinus rhythm occurred
in a succeeding shock.Thus, 28 of 33, or 85 per cent of the
group,developed atrial fibrillation after a single lowenergy shock.
It is not unreasonable to sur-mise that if the initial choice of
energies werecorrect, the 5 who reverted to sinus rhythmwould also
have developed atrial fibrillation.Thus, it may be that, in I00 per
cent of pa-tients with flutter, it is possible to transformthe
rhythm to fibrillation by stimulating thevulnerable period randomly
in the atrial cycle.The data suggest that human flutter is
theresult of but a single mechanism, namely, thecirculation of an
entrapped wave, as conceivedby Lewis.An alternative explanation for
our data
should be considered. It has been shown thatelectrical discharge
releases acetylcholine andnorepinephrine from nerve endings in
theheart (Amory and West, I962; Blinks, I966;Cobb et al., I968;
Nelemans, i95i; Ten Eicket al., I967; Vincenzi and West, I963;
Whalenet al., I958). It is conceivable that the changein rhythm
resulted from neurotransmitterliberation. In the experimental
animal it hasbeen shown that cholinergic stimuli favourthe
emergence, as well as sustenance, of atrialfibrillation (Scherf and
Schott, 1953). In man,carotid sinus pressure, which causes
reflexvagus stimulation of the heart and acetyl-choline release,
may convert atrial flutter toatrial fibrillation (Anbe, Rubenfire,
and Drake,I969;Bussan, Reid,and Scherf, I957;LownandLevine, I96I;
Rytand, I967; Scherf, Cohen,and Rafailzadeh, I966). Cobb et al.
(1968)found that, in dogs, direct current trans-thoracic shock,
even at a low setting of IWsec, provoked vagal-like effects
manifestedby sinus slowing or sinus arrest. These couldbe prevented
by administering atropine. Itis unlikely that shock-induced
acetylcholinerelease was responsible for the change fromatrial
flutter to fibrillation in man. If neuro-transmitter liberation
were the basis, onewould anticipate the following: (I) A
greaterincidence of atrial fibrillation both at higherenergy
discharge as well as in patients ondigitalis who are more
sensitized to cholinergicstimuli; and (2) prevention of emergence
ofatrial fibrillation by atropine. None of thesewas observed. The
fact that pretreatment withpropranolol did not prevent induction of
atrialfibrillation argues also against a role for cate-cholamine
release.
Several recent reports (Haft et al., I967;Zeft et al., I969)
indicate that atrial fluttermay be reverted to sinus rhythm by
rapidright atrial electrical pacing. The pacing ratesemployed have
ranged from I80 to 600 a
minute. Atrial fibrillation was an intermediaterhythm in I2 of
I3 patients. A similar methodhas been used to convert a disabling
and fre-quently recurring atrial tachycardia, for abrief period, to
atrial fibrillation (Wiener andDwyer, I968). Haft and coworkers
(I967)postulated that frequent atrial stimulationallowed an impulse
to fall within the atrialvulnerable period, thereby initiating
unstableatrial fibrillation. They also suggested over-drive capture
of an ectopic focus as the pos-sible mechanism of conversion in one
of theirpatients. Of interest is the observation ofZeft et al.
(I969) that it was possible to restoresinus rhythm in one patient
without inter-vening atrial fibrillation. This was accom-plished by
pacing at a rate of i8o a minutesignificantly slower than the
atrial flutter rateof 330 a minute. It was suggested that
anappropriately timed atrial stimulus inter-rupted a re-entry
pathway of excitation,extinguishing the arrhythmia and
permittingthe sinus node to establish pacing hegemony.The ability
to terminate a number of
arrhythmias with serial right atrial pacing(Massumi, Kistin, and
Tawakkol, I967; Dur-rer et al., I967), single pulses carefully
timedin the excitation cycle of the tachycardia(Bigger and
Goldreyer, I970; Hunt et al.,I968), low energy cardioversion
shocks, andthump version (Lown and Taylor, 1970;Pennington, Taylor,
and Lown, I970) allpoint to the prevalence of re-entry as
thefundamental mechanism in many diversehuman rhythm disorders.
The authors acknowledge the critical and helpfulcomments of Dr.
John Temte.
ReferencesAmory, D. W., and West, T. C. (I962). Chronotropic
response following direct electrical stimulation ofthe isolated
sinoatrial node: a pharmacologicevaluation. Journal of Pharmacology
and Experi-mental Therapeutics, 137, 14.
Anbe, D. T., Rubenfire, M., and Drake, E. H. (1969).Conversion
of atrial flutter to atrial fibrillation withcarotid sinus
pressure. Journal of Electrocardiology,2, 377.
Andrus, E. C., Carter, E. P., and Wheeler, H. A.(1930). The
refractory period of the normally-beating dog's auricle; with a
note on the occurrenceof auricular fibrillation following a single
stimulus.Journal of Experimental Medicine, St, 357.
Bigger, J. T., and Goldreyer, B. N. (1970). Themechanism of
supraventricular tachycardia. Circu-lation, 42, 673.
Blinks, J. R. (I966). Field stimulation as a means ofeffecting
the graded release of autonomic trans-mitters in isolated heart
muscle.Journal ofPharma-cology and Experimental Therapeutics, 151,
22I.
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
Atrial flutter 1223
Brooks, C. McC., Orias, O., Gilbert, J. L., Siebens,A. A.,
Hoffman, B. F., and Suckling, E. E. (I95I).Auricular fibrillation:
relationship of the 'vulner-able period' to 'dip' phenomenon of
auricularexcitability curve. American Journal of Physiology,I64,
301.
Bussan, R., Reid, E. R., and Scherf, D. (I957). Con-version of
atrial flutter into atrial fibrillation bycarotid pressure. Annals
of Internal Medicine, 46,814.
Cabrera, C. E., and Sodi Pallares, D. (I947). Discus-ion del
movimiento circulary prueba directa desu existencia en el flutter
auricular cinico. Archivosdel Instituto de Cardiolog{a de Mixico,
17, 850.
Cobb, F. R., Wallace, A. G., and Wagner, G. S.(I968). Cardiac
inotropic and coronary vascularresponses to countershock.
Circulation Research,23, 73I1
Duchosal, P. W., and Sulzer, R. (I949). La vecto-cardiographie.
Bibliotheca Cardiologica, 3, I.
Durrer, D., Schoo, L., Schuilenburg, R. M., and Wel-lens, H. J.
J. (I967). The role of premature beatsin the initiation and the
termination of supra-ventricular tachycardia in the
Wolff-Parkinson-White syndrome. Circulation, 36, 644.
Enselberg, C. D. (I95i). The esophageal electrocardio-gram in
the study of atrial activity and cardiacarrhythmias. American Heart
Journal, 41, 382.
Garrey, W. E. (I9I4). The nature of fibrillary contrac-tion of
the heart. American Journal of Physiology,33, 397.
Giraud, G., Latour, H., and Puech, P. (1955). Le flut-ter
humain: etude de l'activation auriculair par lesderivations
oesophagiennes et endocavitaires.Archives des Maladies du Coeur et
des Vaisseaux, 48,8I7.
Grishman, A., Kroop, I. G., Jaffe, H. L., and Stein-berg, F. F.
(I950). Application of intracardiac eso-phageal
(electrocardiography) and vectorcardio-graphy to the problem of the
circus movement inman (abstract). American J'ournal of Medicine,
8,395-
Groedel, F. M., and Miller, M. (I950). Auricular flut-ter
studied in direct leads from the human heart.J7ournal of Applied
Physiology, 3, I83.
Haft, J. I., Kosowsky, B. D., Lau, S. H., Stein, E., andDamato,
A. N. (I967). Termination of atrial flutterby rapid electrical
pacing of the atrium. AmericanJ7ournal of Cardiology, 20, 239.
Haft, J. I., Lau, S. H., Stein, E., Kosowsky, B. D., andDamato,
A. N. (I968). Atrial fibrillation producedby atrial stimulation.
Circulation, 37, 70.
Hayden, W. G., Hurley, E. J., and Rytand, D. A.(I967). The
mechanism of canine atrial flutter.Circulation Research, 20,
496.
Hecht, H., Katz, L. N., Pick, A., Prinzmetal, M.,
andRosenblueth, A. (I953). The nature of auricularfibrillation and
flutter. A symposium. Circulation,7, 591.
Hunt, N. C., Cobb, F. R., Waxman, M. B., Zeft, H. J.,Peter, R.
H., and Morris, J. J. (I968). Conversionof supraventricular
tachycardias with atrial stimu-lation. Evidence for re-entry
mechanisms. Circula-tion, 38, I060.
Ishikawa, K. (I967). An experimental study on themechanism of
atrial flutter and fibrillation by meansof the microelectrode
method. J7apanese CirculationJ7ournal, 31, 1403.
Kato, K., Sato, M., Harumi, K., Salxamato, T., Ko-yama, S., and
Murao, S. (I957). Studies on auricularflutter. Observations upon F
wave. (in Japanese).Respiration and Circulation (Tokyo), 5,
837.
Kato, K., Sato, M., Harumi, K., Murao, S., Kana-zawa, T.,
Hauzawa, S., and Kimura, E. (I956).
Clinical studies on the nature of the auricular flut-ter. Tohoku
Journal of Experimental Medicine, 64,SuppI. 4, 377.
Katz, L. N., and Pick, A. (I960). Current status oftheories of
mechanisms of atrial tachycardias,flutter and fibrillation.
Progress in CardiovascularDiseases, 2, 650.
Killip, T., and Gault, J. H. (I965). Mode of onsetof atrial
fibrillation in man. American Heart3Journal,70, 172.
Kimura, E., Kato, K., Murao, S., Ajisaka, H., Koy-ama, S., and
Omiya, Z. (1954). Experimentalstudies on the mechanism of the
auricular flutter.Tohoku Journal of Experimental Medicine, 60,
I97.
Kishon, Y., and Smith, R. E. (I969). Studies in humanatrial
flutter with the use of proximity electrodes.Circulation, 40,
5I3.
Kleiger, R., and Lown, B. (I966). Cardioversion anddigitalis.
II. Clinical studies. Circulation, 33, 878.
Kossmann, C. E., and Berger, A. R. (I94i). Auricularflutter of
eleven years' duration with observationson esophageal
electrocardiograms. Annals ofInternalMedicine, I5, I28.
Lewis, T. (1925). Mechanism and Graphic Registrationof Heart
Beat, 3rd ed. Shaw & Son, London.
Lewis, T., Drury, A. N., and Iliescu, C. C. (i921).A
demonstration of circus movement in clinicalflutter of the
auricles. Heart, 8, 341.
Lewis, T., Feil, H. S., and Stroud, W. D. (ig20).Observations
upon flutter and fibrillation. Part II -The nature of auricular
flutter. Heart, 7, I9I.
Lown, B. (I967). Electrical reversion of cardiacarrhythmias.
British HeartJournal, 29, 469.
Lown, B., Amarasingham, R., and Neuman, J.(x962a). New method
for terminating cardiacarrhythmias: use of synchronized capacitor
dis-charge.Journal of the American Medical Association,i82,
548.
Lown, B., Kleiger, R., and Williams, J. (I965). Cardio-version
and digitalis drugs: changed threshold toelectric shock in
digitalized animals. CirculationResearch, 17, 519.
Lown, B., Kleiger, R., and Wolff, G. (I964). Thetechnique of
cardioversion. American Heart Jour-nal, 67, 282.
Lown, B., and Levine, S. A. (I96I). The carotid sinus;clinical
value of its stimulation. Circulation, 23, 766.
Lown, B., Neuman, J., Amarasingham, R., and Berko-vits, B. V.
(i962b). Comparison of alternating cur-rent with direct current
electroshock across theclosed chest. American Journal of
Cardiology, io,223.
Lown, B., and Taylor, J. (I970). Editorial. 'Thump -version.'
New England Journal of Medicine, 283,I223.
Massumi, R. A., Kistin, A. D., and Tawakkol, A. A.(I967).
Termination of reciprocating tachycardiaby atrial stimulation.
Circulation, 36, 637.
Mayer, A. G. (I9o6). Rhythmical pulsation in scypho-medusae.
Carnegie Institution Publication No. 47, I.Carnegie Institution,
Washington.
Mayer, A. G. (I9I6). Nerve conduction, and otherreactions in
Cassiopea. American Journal of Physi-ology, 39, 375-
Mines, G. R. (1913). On dynamic equilibrium in theheart. Journal
of Physiology, 46, 349.
Nelemans, F. A. (i9Si). Liberation of sympathin andacetylcholine
by faradic stimulation of the frog'sheart. Acta Physiologica et
Pharmacologica Neer-landica, 2, 5I.
Pennington, J. E., Taylor, J., and Lown, B. (I970).Chest thump
for reverting ventricular tachycardia.New England Journal of
Medicine, 283, II92.
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/
-
1224 Guiney and Lown
Prinzmetal, M., Corday, E., Brill, I. C., Oblath, R. W.,and
Kruger, H. E. (1952). The Auricular Arrhyth-mias, p. 387. Charles
C. Thomas, Springfield,Illinois.
Prinzmetal, M., Corday, E., Oblath, R. W., Kruger,H. E., Brill,
I. C., Fields, J., Kennamer, S. R.,Osborne, J. A., Smith, L. A.,
Sellers, A. L.,Flieg, W., and Finston, E. (I95i). Auricular
flutter.American,Journal of Medicine, II, 410.
Prinzmetal, M., Goldman, A., Gerlach, E., and Ken-namer, R.
(I953). Nature of spontaneous auricularflutter in man. Report of a
case observed directlyduring cardiac surgery. J'ournal of the
AmericanMedical Association, 153, 553.
Rosenblueth, A. (1953). The mechanism of auricularflutter and
auricular fibrillation. Circulation, 7, 6I2.
Rosenblueth, A., and Garcia Ramos, J. (1947). Estu-dios sobre el
flutter y la fibrilacion: II. La influenciade los obstaculos
artificiales en el flutter auricularexperimental. Archivos del
Instituto de Cardiologiade Mixico, 17, I.
Ross, J., Jr., Linhart, J. W., and Braunwald, E. (I965).Effects
of changing heart rate in man by electricalstimulation of the right
atrium. Circulation, 32, 549.
Rytand, D. A. (I966). The circus movement (entrappedcircuit
wave) hypothesis and atrial flutter. Annals ofInternal Medicine,
65, I25.
Rytand, D. A. (I967). Electrocardiographic patternsat the
termination of atrial flutter. American HeartJournal, 74, 741.
Scherf, D. (I947). Studies on auricular tachycardiacaused by
aconitine administration. Proceedings ofthe Society for
Experimental Biology and Medicine,64, 233.
Scherf, D., Blumenfeld, S., Taner, D., and Yildiz, M.(I960). The
effect of diphenylhydantoin (Dilantin)sodium on atrial flutter and
fibrillation provokedby focal application of aconitine or
delphinine.American Heart Journal, 60, 936.
Scherf, D., Blumenfeld, S., and Yildiz, M. (I963).Experimental
study of ectopic impulse formationin the left atrium. Cardiologia,
43, 133.
Scherf, D., Cohen, J., and Rafailzadeh, M. (I966).Excitatory
effects of carotid sinus pressure: en-hancement of ectopic impulse
formation and of
impulse conduction. American Journal of Cardi-ology, 173
240.
Scherf, D., Romano, F. J., and Terranova, R. (1948).Experimental
studies on auricular flutter andauricular fibrillation. American
Heart Journal, 36,241.
Scherf, D., Schaffer, A. I., and Blumenfeld, S. (I953).Mechanism
of flutter and fibrillation. Archives ofInternal Medicine, 91,
333.
Scherf, D., and Schott, A. (1953). Extrasystoles andAllied
Arrhythmias. William Heinemann MedicalBooks, London.
Scherf, D., and Terranova, R. (I949). Mechanism offlutter and
fibrillation. American J'ournal of Physi-ology, 159, 137-
Ten Eick, R. E., Wyte, S. R., Ross, S. M., and Hoff-man, B. F.
(I967). Postcountershock arrhythmias inuntreated and digitalized
dogs. Circulation Research,21, 375.
Vincenzi, F. F., and West, T. C. (I963). Release ofautonomic
mediators in cardiac tissue by directsubthreshold electrical
stimulation. J7ournal ofPharmacology and Experimental Therapeutics,
141,i85.
Wenger, R., and Hofmann-Credner, D. (1952). Obser-vations on the
atria ofthe human heart by direct andsemidirect
electrocardiography. Circulation, 5, 870.
Whalen, W. J., Fishman, N., and Erickson, R. (1958).Nature of
the potentiating substance in cardiacmuscle. American J7ournal of
Physiology, 194, 573.
Wiener, L., and Dwyer, E. M., Jr. (I968). Electricalinduction of
atrial fibrillation: an approach tointractable atrial tachycardia.
American Journal ofCardiology, 21, 731.
Zeft, H. J., Cobb, F. R., Waxman, M. B., Hunt, N. C.,and Morris,
J. J. (I969). Right atrial stimulation inthe treatment of atrial
flutter. Annals of InternalMedicine, 70, 447.
Requests for reprints to Dr. Bernard Lown, De-partment of
Nutrition, Harvard University Schoolof Public Health, 665
Huntington Avenue, Boston,Massachusetts 02II5, U.S.A.
on April 4, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.34.12.1215 on 1 Decem
ber 1972. Dow
nloaded from
http://heart.bmj.com/