Embed Size (px)
Citation preview


INTRODUCTION
Cardiovascular risk management decisions are
totally based on the profile of cardiovascular risk
factors (CVRF).
They lead to determining total cardiovascular
risk as being the risk of fatal cardiovascular
events in a predefined period.
It is important to know not only the CVRF
number got by a person but also the magnitude of
each factor, both of which are proportional to
cardiovascular risk (CVR).

CVRF CLASSIFICATION
Major risk factors
(whose association with the risk of cardiovascular disease was highly significant)
WHO defined the major risk factors using 3 criteria:
1. high prevalence among population;
2. independent impact on the risk of coronary heart disease or stroke;
3. their treatment or supervision decrease risk.
• Contributing risk
factors (that increase
CV risk at a less
significant level).

CRF CLASSIFICATION
modifiable risk factors
(factors that can be
controlled by diet or
treatment, for example:
smoking, obesity,
dyslipidemia, diabetes,
hypertension)
• non-modifiable risk
factors (for example: age,
sex, height, heredity).

CRF CLASSIFICATION
classical risk factors
(proved by many social
studies to be correlated
with CV risk).
• new risk factors (there are
more recent studies for
them and they may be
involved in different parts
of physiopathogenic cycle,
for example: lipoprotein,
homocysteine ,
proinflammatory and
thrombotic factors).


AGE
Over 83% of the population affected by coronary
heart disease is over 65 years old.
For both sexes, the risk of CAD increases with
age.
It is considered that the age limit for the risk of
CVD is over 45 years for men and over 55 years
for women. With age, the female advantage of
low CVR before menopause is lost.
At older age, women with myocardial have a
lower survival than men.
One explanation is the fact that most CVRF have
a higher age rate (e.g.: hypertension,
dyslipidemia, obesity, diabetes).

SEX incidence is significantly lower at women than at men
before the age of 50, for middle-age people the risk is 2-5 times higher at men than at women.
A INTERHEART research showed that women usually have their first AMI 9 years later than men.
The men AMI at a younger age may be explained by higher levels of plasma lipids and smoking before 60. Especially that in most countries smoking is more common in males.
In the past estrogen was considered as protective factor for atherosclerosis at women, but random studies regarding the hormone replacement therapy led to reconsideration of relationship between estrogen and the risk of AMI. It is proved that estrogen has a positive effect on lipid profile and improves vascular function at women, but social studies have brought controversial results on vascular protection offered by hormone replacement therapy .

HEREDITY
Family backgroung is considered as CVRF
in case of premature CVD, (e.g. IMA) at
first degree relatives: males <55 years old,
females <65 years old.
Racial factor plays a great role along with
heredity. For example, African Americans
with more severe hypertension than
Caucasians have higher CVR.
These differences must be taken into
account in determining overall risk as
well.

OBESITY
Obesity is a major CVRF with increasing
prevalence in developed countries mainly
due to:
environmental and social factors,
peculiarities of diet,
sedentary way of life.
Obesity is more common among people
with low socioeconomic level, thus linking
to this psychosocial risk factors.

INDEXES OF OBESITY Index Definition Limită obezitate
Body mass index (BMI)
(kg / sq m)
Ratio of weight (in kg) and
square height (m) (G/ h
square)
IMC=25-29,9 kg/sq m -
overweight
IMC>30 kg/sq m - obesity
IMC>40 kg/sq m – lethal
obesity
Abdominal circumference
(cm)
Circumference measured
at the umbilicus and
halfway between costal
margin and iliac crest
NCEP: > 102 cm at men
and > 88 cm at women
IDF: >94 cm at men and >
80 cm at women
Waist circumference to hip
circumference ratio (waist
to hip ratio, WHR)
Ratio of the 2
circumferences reflects the
type of obesity
> 0.95 (M) and> 0.81 (W)
- CVR associated
moderately high
IDF - International Diabetes Federation; NCEP- National Cholesterol Education Program

OBESITY Several recent studies have shown obesity (measured by
BMI) as an independent predictor of CVR, especially for high values of BMI;
BMI limiting parameter explained by the fact that it does not reflect the distribution of body fat nor does it differentiate between muscle and fat.
As a result, other parameters such as waist circumference and hip circumference ratio in waist circumference were proposed (waist to hip ratio, WHRM).
Waist to hip circumference ratio is a derived parameter that reflects the abdominal fat in report to the general body size.
In the INTERHEART study, this ratio was correlated significantly and progressively with the risk of AMI.

"OBESITY PARADOX" described recently in several social studies
defined as a better short- and long-term
prognosis at overweight or obese patients.
There were launched some possible
explanations (better metabolic reserve,
protective effects of some cytokines
secreted by adipose tissue, lower renin
activity, etc.), but so far there is no unique
satisfactory physiopathological
explanation.
At present it is considered that efforts
related to maintaining normal body mass
index should be kept at population level.

NORMAL WEIGHT OBESITY defined by normal body mass index (BMI <25 kg / sqm)
and excess body fat.
Threshold value above which it is considered that body
adiposity is increased at these patients has not been
established, but the largest study published up to date
defines excess fat as follows:
fat over 23.1% of body weight at men
fat over 33.3% of body weight at women
Normal weight obesity is associated with:
cardiometabolic abnormalities such as
metabolic syndrome and its components,
proinflammatory status,
increased oxidative stress,
increased cardiovascular mortality in women.

SEDENTARISM Sedentarism is a growing problem in the developed world:
Over 60% of population does not meet the minimum requirement of 30 minutes of daily physical activity
quarter of population does not perform any physical activity during the week.
Inactivity is associated with an increase 1.5-2 of CVR in comparison with active people.
The INTERHEART study showed that exercise was a protective factor with an OR of 0.86 for AMI occurrence (95% confidence interval 0.76 to 0.97M).
The mechanisms by which physical activity plays a CV protective role are multiple:
maintaining an appropriate body weight
increase in HDL-cholesterol
lowering triglycerides
increase of insulin sensitivity
reducing blood pressure
improve the uptake of oxygen by the myocardium
Increase of coronary artery diameter.

SMOKING Smoking is a major risk factor for atherosclerotic disease
(coronary, carotid, peripheral), including passive smoking,
showing to increase RCV.
Risk stratification should be based on total consumption of
cigarettes (expressed for example as parcel number per
year)
Calculation method number of packets per year:
Number of packet/year = (packets smoked per day)
x (years as a smoker)
Number of packets/year = (number of cigarettes
smoked per day) × (years as a smoker) / 20
(1 packet- 20 cigarettes)
Example: a patient smoking 15 cigarettes / day for 40 years
has consumpted (15 times 40) / 20 = 30-year packets.
CV risk is even greater as smoking onset occurs before the
age of 15 years.

SMOKING
The mechanisms by which smoking increases the CVR are:
Increase of total cholesterol and decrease of HDL cholesterol
platelet and leukocyte activation
Increase of circular fybronogen
endothelial dysfunction as well as promoting crack
vulnerable plaques
Increase of heart rate and blood pressure
Arterial vesselconstruction (including coronary spasm)
effects of worsening myocardial ischemia due to carbon
monoxide.
Stopping smoking is an effective method to reduce the CVR.
CV risk of former smokers decreases rapidly, reaching in
about 3 years after stopping to the level of similar non-
smokers.

SMOKING
Quitting smoking is the most effective of all
preventive measures, the effect being
pronounced at patients with coronary artery
disease.
There is no age limit for the benefits of
quitting smoking.
Clear and strong urge for smoking cessation
is often decisive, especially when it happens
during an event procedure or during an
coronorian intervention, the patient being
very motivated when deciding to quit
smoking.

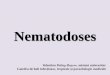
ALGORITHM FOR SMOKING CESSATION
ASSISTANCE
patient consumes tobacco
want to quit smoking now?
create motivation to quit
Yes
Yes
start your
therapy
No
No
No
prevent
relapse Maintain Abstinence
Ever smoked?
Yes

SMOKING
Drug therapy includes nicotine replacement therapy,
available in different forms (gum, patch, nasal spray
or inhalators, pills), being considered that they would
increase 50-70% withdrawal rate.
Some European countries have adopted legislative
measures banning smoking in public places,
estimating that more than 200 million European
citizens would benefit from this legislation.
After banning smoking in public places, several
countries have reported reduction of acute coronary
events (in Italy, 11.2% in people between 35-64 years
and 7.9% for those between 65 and 74 years) .

ALCOHOL
Link between alcohol and CVR is more complex.
CVR is high for intensive consumers
CVR is lower for moderate drinkers compared to
abstainers.
Thus it is known that excessive alcohol consumption
(> 90g per day for at least 5 years) is a risk factor for
the development of dilated cardiomyopathy (DCM),
the cause of over a quarter of cases of CMD.
Also, excessive alcohol consumption increases the risk
of hypertension and, in parallel, the risk of
hemorrhagic stroke or subarachnoid hemorrhage.
Drinking large amounts of alcohol can lead to
particularly supraventricular arrhythmias (e.g. atrial
fibrillation in the so-called ,,Haliday-heart
syndrome,,).

ALCOHOL
On the other hand, all recent epidemiological
studies agree that moderate alcohol
consumption appears to have a protective CV
effect with evidence collected especially for red
wine.
In this kind of alcohol,the effects of
polyphenols contained in wine are more
beneficial than the effects of ethanol contained
in it.
However, it is proved that considering the
absence (and ethical difficulties) of average
studies, patients can not be advised to use
moderate amount of alcohol in order to reduce
CVR.

HIGH BLOOD PRESSURE
High blood pressure defined as values of blood pressure
over 140/90 mmHg, is one of the most important preventive
causes of cardiovascular death, contributing to about half of
the global CV mortality.
Cardiovascular mortality doubles for every 10 mmHg
increase in diastolic blood pressure and with 20 mmHg
systolic blood pressure.
Not only the absolute values of blood pressure are
cardiovascular risk factors, but the pulse pressure (the
difference between systolic blood pressure and diastolic
blood pressure), whose increase reflects the presence of a
predominant systolic high blood pressure, represents an
independent factory of risk for the cardiovascular mortality
(in particular coronary and for cardiovascular accidents )
especially after 55 years.

HIGH BLOOD PRESSURE
In consequence, the decrease in blood pressure values through measures of lifestyle modification and pharmacological treatment has a very important impact on reducing cardiovascular mortality in primary prevention.
Of lifestyle measures remain essential :
hyposalted diet
dropping weight
moderating alcohol consumption for consumers of ethanol
At these it should be added pharmacological measures for obtaining the normal values of blood pressure.
And in secondary prevention, it is proven that an optimal control of the blood pressure values significantly decreases the risk of relapse of ischemic cardiovascular accident, cardiovascular mortality after coronary accident.

DYSLIPIDEMIA
Dyslipidemia is one of the factors with high
prevalence and susceptibility to be modified.
It includes a series of disorders of lipid
metabolism with the potential of inducing and
maintenance of aterosclerotic phenomenon:
Classic anomalies ( increase of total cholesterol,
LDL cholesterol and decrease of HDL cholesterol)
Items recently described of the lipid imbalance
(apolipoproteins changes, the increasing number
of small dense LDL particles, of lipoproteins (a),
triglyceride-rich lipoproteins and their
fragments)

TOTAL CHOLESTEROL
Epidemiological studies ( Framingham studies,
Multiple Risk Factor Intervention Trial - MRFIT,
Atherosclerosis Risk In Communities - ARIC etc.)
have proved to be a direct relationship between
the serum levels of total cholesterol and
cardiovascular mortality and morbidity.
Cardiovascular risk increases by 2-3% for each
percentage point of total cholesterol
concentration.
Clinical trials that have used hypolipomiant
therapies have shown that reduction of colesterol
values joins morbidity and mortality reduction in
cardiovascular diseases in patients with or
without established cardiovascular disease.

LDL-CHOLESTEROL
Numerous clinical studies have shown that lowering
serum values of LDL cholesterol is associated with
decreased cardiovascular risk.
It has been proven that in order to reduce to 30 mg/dl
in plasmatic LDL cholesterol register a 30%
reduction of cardiovascular risk.
As a result, the reduction in serum concentration of
LDL cholesterol is the next target of therapy in people
with dyslipidemia, causing marked reduction in the
risk of coronary death, nonfatal myocardial infarction,
revascularization procedures and strokes.
The national guide Cholesterol Education Program
(NCEP) established in patients with cardiovascular
disease targets of LDL cholesterol concentration <
100 mg/dl or even < 70 mg/dl.

HDL CHOLESTEROL
Unlike LDL, increased HDL cholesterol level is a
cardiovascular protective factor.
This inverse relationship between HDL levels and
cardiovascular risk is explained by the role of HDL
cholesterol reverse transport that is mobilized from the
periphery to be catabolized in the liver, and involvement
in other antiaterogenic mechanisms.
antioxidant function
improvement of the inflammatory cascade
protection against procoagulant activity
The value of serum HDL cholesterol less than 40 mg/dl is
a predictive factor for cardiovascular disease.
Low HDL levels along with trygleceridemia are the
elements of the metabolic syndrome.

DIABETES MELLITUS
Insulin resistance, hyperinsulin and hyperglycemia are associated pathophysiological with atherosclerotic cardiovascular disease.
The diabetes have a higher risk of myocardial infarction or cardiovascular accident of 2-3 times, independent of other cardiovascular risk factors .
NCEP included in 2002 as a equivalent of BCI with a high risk.
Control of risk factors as well as glycemic values must be aggressive in patients with diabetes mellitus (LDl cholesterol values < 100 mg/dl and the optimal values of blood pressure of <130/80 mmHg ).
Optimal control of diabetes leads to lowering the rate of cardiovascular complications.

PSYCHOSOCIAL FACTORS
Includes:
Professional or personal stress
financial stress
stressful life events
depression
the perception of skill to control the situations of life
lack of social support
results of the study have shown that psychosocial factors can contribute in a significant proportion to lower risk of myocardial infarction.
their overall effect was smaller than the smoking, but comparable with hypertension or abdominal obesity.
the effect of stress on the risk of myocardial infarction was similar in men and women, age boundary and in all regions.


HOMOCYSTEINE
The first Association of increased serum homocysteine
concentration (Hcys) and atherosclerosis was based on necroptic studies in patients with the homozygot deficiency of enzymes necessary in homocysteine metabolism ( CBS, metilentetrahidrofolat reductase, MTHFR).
In patients with these defects, severe atherosclerosis develops from childhood and many of them shows a first myocardial infarction before the age of 20 years.
Homocysteine has toxic effects on the endothelium, is protrombotic, increases the synthesis of collagen and decreases nitric oxide availability.
Depending on the lab, hyperhomocystein is defined by a level of Hcys over 12-16 mmol/l. a level of 15-100 mmol/l is considered to be moderately increased, and more than 100 mmol/l is severely increased.

HOMOCYSTEINE
The main cause of hyperhomocysteinemia
remains the genetic one.
Main mutations found in the population are
mutations of the MTHFR gene, type C677T
and A1298C type.
These patients have an increased
atherosclerotic risk to the coronary artery,
peripheral and cerebral.
Blood concentration can be reduced to normal
through treatment with folic acid, but are
still needed studies to determine if this
treatment prevents the progression and
eventually the regression of atherosclerotic
lesions.

LIPOPROTEIN (A)
The lipoprotein (a) is a particle containing an ester of
cholesterol and apolipoprotein B100, differing of LDl
cholesterol by the presence of glycoprotein apo (a), a
plasminogen analog.
Studies in vitro and in vivo have shown that favors
atherogenesis and thrombogenesis, representing a
cardiovascular risk factor independently moderated.
A metaanalyse including 31 prospective studies reported a
relative risk of 1.5 times in patients with values of Lp (a)
in the upper third in comparation with lower distribution
Lp (a) (according to the averages in those categories of 50
versus 5 mg/dl)
The coexistence of an increased level of LDL, decreased of
HDL or the high blood pressure increases secondary the
cardiovascular risk in the patients with a high level of Lp
(a).

PROTHROMBOTIC FACTORS
Thrombosis plays a central role in the pathogenesis of acute coronary syndromes, through processes that involve both platelets and clotting factors.
An important haemostatic factor associated with the risk of major coronary ischemic is Fibrinogen. Thus, the high level of fibrinogen is associated with cardiovascular risk independent of lipid profile.
Other haemostatic factors correlated with increased cardiovascular risk are :
activated factor VII
Plasminogen activator inhibitor-1
Plasminogen Activator Tissue
Von Willebrand (that is a marker of endothelial dysfunction )
Relatively common genetic defects in population leading to a procoagulant potential are known as thrombophilias (factor V Leiden mutation, prothrombin -factor II mutation, deficits of protein C, S or antithrombin III)
Indications for setting completely thrombophilic profile :
in case of the disease at young age (below 45)
of his family agregation

CARDIOVASCULAR RISK SCORES
Estimation of the effect of combined
cardiovascular risk factors on
cardiovascular morbidity require the
use of risk scores, in which the major
risk factors to be included on the
basis of their weighted prognostics.

FRAMINGHAM SCORE
Framingham score is calculated on the basis of
equations that take into account gender, age, total
cholesterol, HDL cholesterol, smoking and systolic blood
pressure, assigning a number of points depending on
the presence and magnitude of each factor.
A form easier to use in actual practice is derived from
this score as a coronary risk map (Coronary Risk
Chart).
In order to evaluate the risk of cardiovascular morbidity
and mortality, the score set arbitrary limits :
<10% for low risk
10-20% for intermediate risk
>20% for high risk, that requires pharmacological
intervention.

THE SCORE SCORE
Unlike Framingham score:
report on cardiovascular mortality and not on
total cardiovascular events.
are taken into account and the deaths by
atherosclerosis in non-coronary territories
(AVC)
the score is adjusted average ages, changing
risk with age is more steep
there are separate scores for European
countries with high risk and low risk, where
there was complete data about mortality.

THE SCORE SCORE
The score is available in two
versions, one for the regions with low
risk (Belgium, France, Greece, Italy,
Spain, Luxemberg, Switzerland and
Portugal) and another for those at
high risk, where fit and our country,
along with other European countries
which were not mentioned in the list
above.


THE SCORE SCORE
It should be noted that the SCORE will be aimed at individuals without cardiovascular disease, aged up to 65 years. The subjects with the disease manifest ATS are considered already high risk and should be treated as such.
The SCORE has a few functions:
highlights the risk of CVD fatal event in the next 10 years in the table, without additional calculations
estimated relative risk, comparing a cell (square of the grid) with any other, in the same category of age,
assess the impact of the improvement of the risk factor (the move from one category to another risk by stopping smoking, lowering total cholesterol, etc.)
highlight the effect of the action of a risk factor in time (increased risk with aging)


THE IMPORTANCE OF THE PROBLEM Cardiovascular disease is the cause of the 48% of deaths (43%
in men and 55% women) in Europe and 42% in the countries of
the European Union, produce more than 4.3 million deaths in
European countries and over 2 million in the 27 countries of
the EU.
A notable proportion of these deaths occurs in relatively young
individuals under 65, and more than 800,000 according to
Europe and over 230,000 in EU countries.
Coronary heart disease (CHD) is the most common cause of
death in Europe, being responsible for 1 in 5 deaths in Europe.
Most epidemiological models used suggest that improvement
and control of risk factors, have had a more marked than in
the control treatment of CVD (here being included major
changes in the treatment of acute coronary syndromes,
hypertension and heart failure, secondary prevention
measures).

PREVENTION STRATEGIES
The work of prevention of CVD has as targets the reduction of mortality and morbidity and increasing hope of life while maintaining or improving quality of life.
There's clear scientific records whitch show that the change in style of life and the control of risk factors in reducing their action, can influence the development and progression of the disease, both before and after producing a clinical event manifest.

PREVENTION STRATEGIES
The World Health Organization (WHO) considers that
a comprehensive action for prevention must include
three components:
Populational strategy - referring to the change in
lifestyle and the environment and addressing social
and economic factors, cultural, determinants of CVD,
is accomplished through the formulation of strategies
and interventions in the community.
Strategy for high-risk population - pressure identified
individuals to high risk and the reduction of risk
factors.
Secondary prevention - prevention of recurrence and
progression of the disease in patients with CVD
clinically manifest.
These three strategies are complementary.

POPULATION STRATEGY
Population Strategy is crucial in
reducing the overall incidence of
cardiovascular disease ,proposing to
reduce the influence of risk factors at
the population level through changes
in lifestyle and social environment,
without the need for individual
medical examination.
Measures of influence on lifestyle
refer to:
• Reducing the number of smokers,
• Encouragement of physical
activity,
• Promotion of healthy eating
habits.

POPULATION STRATEGY
In 2005 the EU adopted a declaration defining characteristics associated with cardiovascular state of health: • No smoking, • Regular physical activity (at least 30 minutes daily) • healthy eating habits, • avoidance of overweight, • blood pressure below 140/90mmHg in patients without diabetes or target organ damage or with multiple risk factors, • Total cholesterol below the threshold of 5 mmol / L (about 200mg/dl). • These characteristics can be summarized as a number: 0-3-5-140-5-3-0
0 - no smoking
3 - 3km or 30 minutes of physical activity daily
5 - fruit and vegetable servings daily
140 - systolic blood pressure less than 140mmHg,
5 - total cholesterol below 5 mmol / l,
3 - LDL cholesterol less than 3 mmol / l,
0 - no overweight or diabetes).

TOTAL RISK ESTIMATION
• Total risk is the probability of a person developing
a fatal cardiovascular event in a defined period of
time.
• Assessment is done by taking into account all risk
factors, not just one.
• The example shown in the table below shows how
a female of 60 years, with a high cholesterol level of
310mg/dl has a 9-fold lower risk for cardiovascular
mortality than a male of the same age, but who
smokes and is hypertensive.

Gender Age Cholester
ol
mmol/l
AP (mm
Hg)
Smoker Risc (%)
F 60 8 120 No 2
F 60 7 140 Yes 5
M 60 6 160 No 8
M 60 5 180 yes 19

STRATEGY FOR HIGH-RISK
POPULATION
• preventive measures for persons at high risk, but otherwise in good health, must become part of clinical practice. Total cardiovascular risk estimation is the first step in prevention measures. • People at high risk are those with: - Multiple risk factors, giving a risk score of ≥ 5% - Significantly increased level of a single risk factor, e.g. BP ≥ 180/110 mmHg or persistent BP ≥ 160/110mmHg, these values should be treated, regardless of the presence of other risk factors, - Total cholesterol ≥ 8 mmol / L (320mg/dL) - LDL-cholesterol ≥ 6 mmol / L (240mg/dL) - Diabetes mellitus (relative risk is 5 for women and 3 for men).

SECONDARY PREVENTION
• Targets patients who have had a cardiovascular event and is considered to be the best cost-effective strategy. • Secondary prevention initially addressed patients with coronary artery disease, particularly those with myocardial infarction or those who were revascularized, both categories being included in rehabilitation program. • Cardiovascular Rehabilitation, with a mainstay at physical activity has been shown to reduce both cardiac mortality, as well as mortality overall. • Patients are relatively few (compared to the population level), easily identifiable and more motivated than those who are asymptomatic. • Secondary prevention suggests counseling regarding lifestyle and pharmacological therapy as the integral part of patient care after a cardiovascular or neurological event.

OBJECTIVES OF SECONDARY PREVENTION:
Smoking cessation
Healthy nutrition
Physical activity: at least 30 minutes of moderate
physical activity daily
Total cholesterol<4,5 mmol/L (175mg/dL) with
option of <4mmol/L (155mg/dL), where feasible
Total LDL-cholesterol <2,5mmol/L (100mg/dL)
with option of < 2 mmol/L (80mg/dL), where
feasible
BP<130/80mmHg.

PHYSICAL ACTIVITY • Lack of physical activity is a major lifestyle problem since childhood. Nowadays, few children practice sports, and most of them become sedentary reaching adulthood. Also, few patients with cardiovascular disease participate in programs with physical exercise, especially when in presence of heart failure. • It is estimated that at least 60% of the world population does not meet the recommended minimum of 30 minutes of moderate physical activity daily • proportion of people who do not perform any kind of physical movement in a week is 25%.
• The risk of developing a cardiovascular disease is at least 1.5 times higher in the inactive people with major impact on the young people, where currently has been registered a marked decrease in physical activity levels at the age group from 12 to 21 years, with a tendency for stabilization at average age (30-64 years) and even improvement at more advanced age.

The combination of excessive caloric intake and insufficient exercise is a contributing factor to the development of metabolic syndrome, with registered epidemic growth in recent years.
The latest report published by the AHA in December 2009 on coronary heart disease and stroke, shows that almost one third (31.9%) of children aged between 2 and 9 years old are overweight or obese.
The study on primary prevention from 2008, which included 513,472 individuals, shows that people who exercise during their free time lower the risk of development of coronary disease or cardiovascular mortality with 27% (for intense physical activity) and with 12% (for moderate activity) in comparison with those with low physical activity, or none at all.
In secondary prevention, reduction of total mortality due to only practicing of physical exercise was assessed at 27% and 31% for cardiac mortality.

PHYSICAL ACTIVITY Weight maintenance or even weight loss for the
overweight,
Has effect on lipid profile by means of increasing, mostly, HDL-cholesterol and lowering the level of triglycerides
Increases insulin sensitivity
Reduces blood pressure
Increases compliance to the measures of influence on other risk factors, thus lowering the incidence of cardiovascular disease and cardiac mortality
Any kind of increase, low to moderate, of the level of effort has positive effects (e.g. usage of stairs instead of elevator).
Everyone can choose the modality of physical activity which seems to be more attractive ( walking, cycling, gardening).

RECOMMENDATIONS
ON PHYSICAL
ACTIVITY
Physical activity may not add
too many years of life,
but more importantly,
adds more life to years remaining

CHILDREN AND ADOLESCENTS
• Each child should be encouraged to perform at least 60,
preferably 90 minutes of physical activity daily, which
significantly increases heart rate , under aerobic
conditions (vigorous intensity at least 3 days a week) ,as
well as muscle and bone strengthening exercises.
• The proposed activities must be adjusted to age, be
pleasant and appealing.

HEALTHY ADULTS
• The European guide on prevention shows that 30 minutes of
moderately vigorous exercise on most days of the week will reduce risk
and increase tonus (physical).
• In practice, this recommendation can be accomplished by performing
at least 30 minutes of moderate physical activity 5 days a week or at
least 20 minutes of vigorous activity three days a week or a
combination of these 2 regimens.
• To the aerobic activity (brisk walk, jogging, dancing, swimming,
games such as basketball), muscle toning exercises should be added at
least 2 days per week (jumping, pushups, squats, lifting weights, elastic
bands, 8 -12 reps per set).
• Additional benefits are obtained by moderate activity of 300 minutes
(5 hours) per week or 150 minutes of vigorous activity or combination
of these two modalities.

ADULT WITH CARDIOVASCULAR DISEASE
• Recommendations on physical training are based on
information obtained from effort tests , whether it is a standard
ECG, or preferably the measurement of gas changes and direct
assesment of oxygen consumption.
• One of the most important components of secondary prevention
is cardiac rehabilitation(rehab).
• The term “Cardiac Rehabilitation” refers to the coordinated,
comprehensive intervention which has as a goal optimization of
physical, psychological and social status of a cardiac patient
with slowing down, stabilization and even regression of
atherosclerotic process, thus reducing morbidity and mortality.

NUTRITION
The relationship between dietary habits and cardiovascular
risk is well established, as demonstrated in several clinical and
epidemiological studies.
General recomandations for subjects with high cardiovascular
risc
nutrients % of energetic
comsumption
Total fats
Saturated fats
Trans acids
Polyunsaturated
N-3
Cholesterol
Fruits and vegetables
Salt
30
10
<2
>10
1g/day
<300g/day
>5 portions/day
<6g/day

LIPIDS
have a major role in the formation of atheromatous plaque.
• The relationship between fat intake and the development of
cardiovascular disease is related to the content of saturated fatty acids,
which increase LDL cholesterol concentration. The main sources are
animal products, processed food industry and certain fats used in
cooking.
• Monounsaturated fatty acid intake is associated with decreased risk of
cardiovascular disease.
• Fatty acids with trans configuration are produced by industrial
hydrogenation of vegetable fats and oils. There is a positive association
between trans acids and cardiovascular morbidity and mortality, which
led to banning of their presence in food in many European countries.
• polyunsaturated acids n-6 and n-3, the main representative of which
is linoleic acid, are derived mainly from vegetable oils and were found
to lower LDL cholesterol and cardiovascular risk compared with intake
of saturated or trans fatty acids.

FRUIT AND VEGETABLES
• are sources of vitamins and fibers, regular intake of which reduces systolic and diastolic blood pressure. • The risk of coronary events is reduced by 7% and stroke by 5% for one serving of fruit and vegetables per day. • In EU countries is recommended consumption of at least 400g/day (leading to prevention of 135,000 cardiovascular disease deaths annually), consumption of 600g daily reduces the risk of cardiovascular disease by 18% and stroke by 11%. • Note that approximately 90% of children in European countries consume fruit and vegetables on daily basis below the recommended amount.

SALT INTAKE
• Approximately 75% of the amount of salt we eat is already in the
food.
• The amount of salt can vary widely within the same product (bread,
for example, can contain from 0.7 to 3 g/100 g of product).
• Reduction of salt intake from food products to 3g (equivalent to
1200mg of sodium) reduces the annual number of new cases of heart
disease by 60,000 to 120,000, of stroke by 32000-66000 and
myocardial infarction with 54000-99000, number of deaths from any
cause being reduced from 44,000 to 92,000.
• The effect is similar to that obtained by reduction of tobacco
consumption by 50%, reduction by 5% of body mass index in obese or
usage of statins in people with low or intermediate risk. Reducing
dietary salt up to 3g/day correlates with lowering of health costs with
10-24 billion annually.
• Currently guidelines for hypertension management based on data
from WHO, recommend daily consumption of only 5g of salt (one
teaspoon).