Embed Size (px)
Citation preview

Introduc)ontoClinicalHematopoie)cCell
Transplanta)on(HCT)
GeorgeChen,MDFriday,May12,17

GoalsforToday
• WhatisHCT?• HowisHCTdoneandhowisittailoredtofitthepa)ent’sdiseaseandcircumstances?
• WhataresomeoftheclinicalproblemsinHCT?

ImportantConcepts
• AutologousvsallogeneicHCT• Myeloabla)vevsreducedintensitycondi3oningregimens
• Autologous,syngeneic,matchedrelated,matchedunrelated,mismatchedandhaploiden)caldonors
• Acutevs.chronicgra5versushostdisease• Donorchimerism

WhatisHCT?
• Bonemarrowtransplant• Hematopoie)cstemcelltransplant
• Hematopoie)cprogenitorcelltransplant
• Peripheralbloodstemcelltransplant
Thetransferofhematopoie)cprogenitorandstemcellsfortherapeu)cpurposes


ImportantConcepts
• AutologousvsallogeneicHCT• Myeloabla)vevsreducedintensitycondi)oningregimens
• Autologous,syngeneic,matchedrelated,matchedunrelated,mismatchedandhaploiden)caldonors
• Acutevs.chronicgraNversushostdisease• Donorchimerism

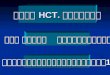
BasicDefini)ons• AutologousHCT–Atransplantusingapa)ent’sowncellsforthegraN.
• AllogeneicHCT–Atransplantusinganotherperson’scellsforthegraN.
Pa)ent AutologousHCT
HighdoseChemo±XRT
RegularChemo±XRT
Freezer
8-14days

Cytotoxicity
ChemotherapydoseCytotoxicityChemotherapydose

Indica)onsforautoHCT
• Diseasesinwhichcytoreduc)on(bychemotherapy)iseffec)veanddosedependent– Germcelltumors(tes)cular)– Largecelllymphoma– Mantlecelllymphoma(usually)– Myeloma
• Replacementofhematopoiesis(rescuetherapy)

Pa)ent
AllogeneicHCT
RegularChemo±XRT
HighdoseChemo±
XRT
14-21days
Time
Donor

Indica)onsforalloHCT• Replacementofhematopoiesis– Aplas)canemia
• Immunemediatedeffectagainsttheunderlyingmalignancy
• Preven)onofrelapse– Acuteandchronicleukemia– Myelodysplas)csyndrome– Indolentlymphomas
Somethingtothinkabout
• Whattumorcharacteris3csareamenabletoautologousversusallogeneictransplanta3on?
• Forlater:Whattumorcharacteris3cslendthemselvestomyeloabla3veversusreducedintensitycondi3oning?

AcuteGvHD(15%)
Infec)on(10%)
Other(5%)
ChronicGvHD,dead(15%)
Diseaserelapse(20%)
ChronicGvHD,alive(15%)
Aliveandwell(20%)
AllogeneicBMTSurvivalOutcomes(AML)
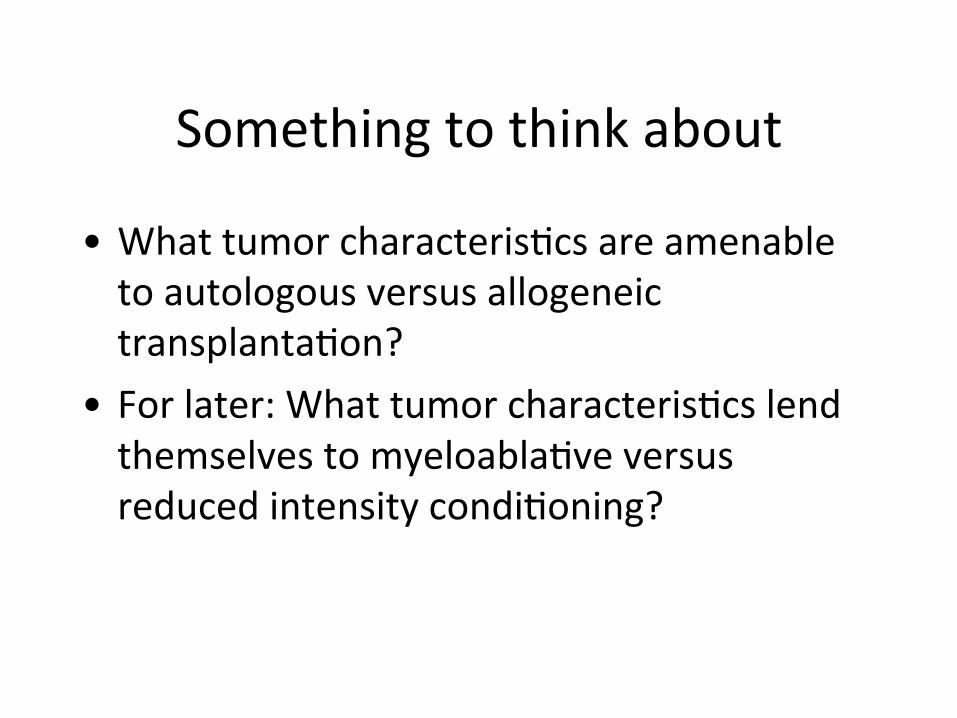
Atransplantisabetagainstthefuture
HighdoseChemo±
XRT
LeukemiaTherapy
95%
5%
65%
35%

Gene)cSubgroupAnalysis:RFS
time (months)
Rel
apse
-free
Sur
viva
l (%
)
0 12 24 36 48 60 72 84 96
0
20
40
60
80
100
NPM1+/FLT3 ITD-
time (months)
Rel
apse
-free
Sur
viva
l (%
)
0 12 24 36 48 60 72 84 96
0
20
40
60
80
100
p=0.71
donor n=35
no donor n=92 donor n=45
no donor n=125
p=0.02
Others
CourtesyofSchlenkRetal,NEJM2008

MUD Transplantation in Relapsed Patients with Unfavorable Genotype
other strategy n=67
MUD n=37
p<0.0001
time (months)
Surv
ival
afte
r rel
apse
(%)
0 12 24 36 48 60
0
20
40
60
80
100

Prognos3ccategoriesforAML• Good
– t(8:21),t(9:22),inv16,t(15:17)– NPM1– CEPB
• Medium– Normalkaryotype
• Poor– Mul3plekaryotypicabnormali3es– Flt3ITDorTDK
• Clinicalfactorsindica3ngapoorprognosis– Induc3onfailure– Priorhematologicdisorder

ImportantConcepts
• AutologousvsallogeneicHCT• Myeloabla)vevsreducedintensitycondi)oningregimens
• Autologous,syngeneic,matchedrelated,matchedunrelated,mismatchedandhaploiden)caldonors
• Acutevs.chronicgraNversushostdisease• Donorchimerism

Pa)ent
AllogeneicBMT
RegularChemo±XRT
HighdoseChemo±
XRT
14-21days
Time
Donor

ImmunologicEffectsofAllogeneicGraNs
• GraN-versus-TumorEffects–Reac)onofthedonorimmunesystemagainsttherecipient’smalignancy
• GraN-versus-HostEffects–Reac)onofthedonorimmunesystemagainsttherecipient’sbody)ssues.
• Differentsidesofthesamecoin.

ProbabilityofRelapseA5er2,254HLA-iden3calSiblingTransplantsfor
EarlyLeukemia
Mln06_1.ppt
0 2 4 61 3 50
20
40
60
80
100
Prob
abilityofR
elap
se,%
Years
TCellDeple3on(n=401)
Twins(N=70)
NoGVHD(n=433)
AGVHDOnly(n=738)
AGVHD+CGVHD(N=485)CGVHDOnly(N=127)
IncreasingGVT
IncreasingGVH

CellKilling
Chemotherapydose Chemotherapydose
CellKilling
Pa3e
ntToxicity
Chemotherapydose

CellKilling
Chemotherapydose Chemotherapydose
CellKilling
Pa3e
ntToxicity
Chemotherapydose
Pa3e
ntToxicity
Chemotherapydose

Pa)ent
ReducedIntensityAlloBMT
RegularTherapy
±Chemo±XRT
14-21days
Time
Donor
Immunosuppression

Pa)ent
AllogeneicBMT
RegularChemo±XRT
HighdoseChemo±
XRT
14-21days
Time
Donor

Transplantregimens
Myelosuppression
Flu-CyFlu-Cy-ATGFlu-lowdoseTBIFluATGTLI/ATGFLU/CY/TBI200cGy
Cy-TBI1200cGYBu-CyMel200
Flu-MelFlu-BuFlu-Mel-TBI400cGy
RegimenRelatedToxicity
LaterGra5-versusDiseaseEffect EarlierAn3-DiseaseEffect
AlloNon-myeloabla3ve
AlloReducedIntensity
AutoandAlloMyeloabla3ve
Relapse
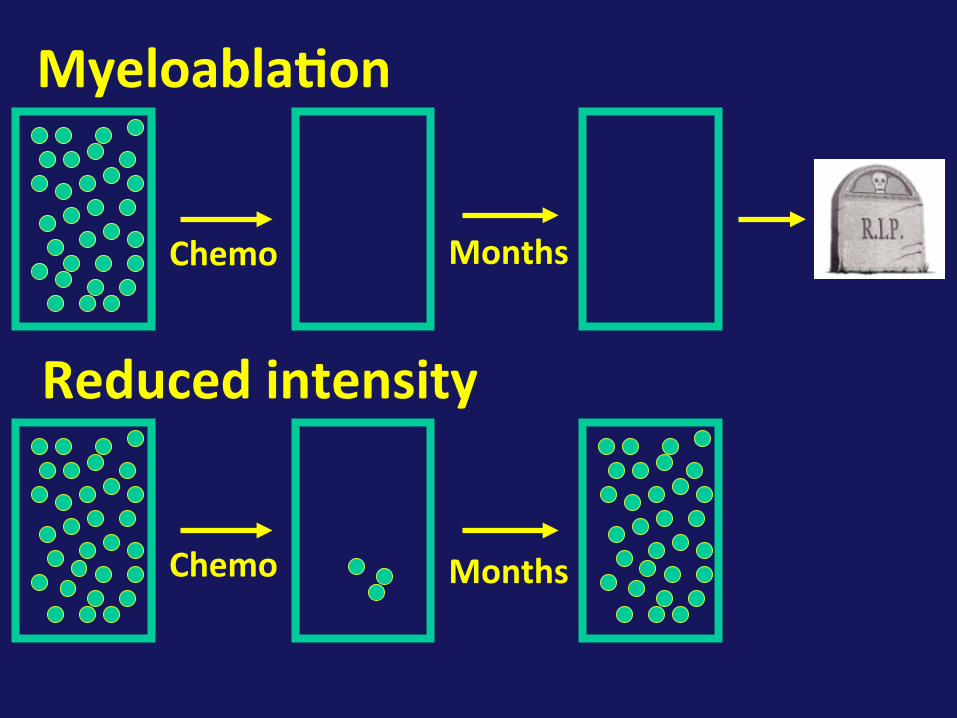
Reducedintensity
Myeloabla)on
MonthsChemo
Chemo Months

Bu, Mel, full dose TBI

Fludarabine Bu, Mel, full dose TBI

Cyclophosphamide
Fludarabine Bu, Mel, full dose TBI

Cyclophosphamide
4-hydroxy-cyclophosphamide
CytochromeP450
Aldophosphamide
Phosphoramidemustard(ac3ve)
Acrolein(ac3ve)
Aldehydedehydrogenase Carboxy
phosphamide(inac3ve)
Tautomer-iza3on

Cyclophosphamide
4-hydroxy-cyclophosphamide
CytochromeP450
Aldophosphamide
Phosphoramidemustard(ac3ve)
Acrolein(ac3ve)
Aldehydedehydrogenase Carboxy
phosphamide(inac3ve)
Tautomer-iza3on
ElevatedinstemcellsHigherinresAnglymphocytesversusacAvatedlymphocytes

Bornhauser,eta
l.LancetOncologyOct2012
1stCRMRD9/10MUD

Bornhauser,eta
l.LancetOncologyOct2012
Allpa3ents
41-60y/o
18-40y/o

Somethingtothinkabout
• Whattumorcharacteris3csareamenabletomyeloabla3veversusreducedintensitycondi3oningallogeneictransplanta3on?

ImportantConcepts• AutologousvsallogeneicHCT• Myeloabla)vevsreducedintensitycondi)oningregimens
• Autologous,syngeneic,matchedrelated,matchedunrelated,mismatchedandhaploiden)caldonors
• Acutevs.chronicgraNversushostdisease• Donorchimerism

Donorsourcereflectspurpose
Rescuehematopoiesis
Immunetherapy
Autologous XXX ?Allogeneic XXX XXX

Adjusted probabilities of leukemia-free survival rates after identical twin bone marrow transplantations with high
(more than 3 × 108 cells/kg) versus low (less than or equal to 3 × 108 cells/kg) cell doses.
Barrett A J et al. Blood 2000;95:3323-3327
©2000 by American Society of Hematology

HumanLeukocyteAn3gen(HLA)• Proteinswhichpresentan3genicpep3destoTcells
• Onsurfaceofmostbodycells• Themostimportantproteinsintransplant• Responsibleforgra5rejec3onandGvHD

HLA
• ClassI–A,B,C• ClassII–DR,DQ,DP


HLAInheritance
Chanceofamatchedsibling=1–0.75#ofsiblings
A2B7
DR01
A23B51DR04
A11B15DR11
A30B35DR13
A2B7
DR01
A11B15DR11
A23B51DR04
A11B15DR11
A2B7
DR01
A30B35DR13
A23B51DR04
A30B35DR13

HLA
• (>1*1012haplotypes)2=>1*1024combina3ons
• Frequenciesarenotequaldistributed• Notallalleleshavebeeniden3fied
HLA DRB1 A B C DQB1Alleles 400 370 660 190 62

HLAExpressionLevel
• Highexpressionlevel(HEL)an3gens–DRB1,A,B,C
• Lowexpressionlevel(LEL)an3gens–DQ,DP,DRB3-5

Rela3veMismatchBetweenDonorSourcesParent1 Parent2
Donor DRB1
B A C DQ DP DRB1
B A C DQ DP
Related = = = = = =Unrelated = = = = = = = = = = = =LEL-MM = = = = ≠ = = = = = ≠ ≠HEL-MM ≠ = = = = = = = = = = =Haplo = = = ≠ ≠ ≠
Pidala,etal.Blood2015
DonorSelec)on
• Humanleukocytean)gen(HLA)matching• Relatedness• Cytomegalovirusstatus• Age• Gender(parity)• NotbloodABOtype(sofar)

ImportantConcepts• AutologousvsallogeneicHCT• Myeloabla)vevsreducedintensitycondi)oningregimens
• Autologous,syngeneic,matchedrelated,matchedunrelated,mismatchedandhaploiden)caldonors
• Acutevs.chronicgraNversushostdisease• Donorchimerism
BMT

BillinghamCriteria(1966)• ThegraNmustcontainimmunologicallycompetentcells
• Thehostmustpossessimportanttransplanta)onalloan)gensthatarelackinginthedonorgraN,sothatthehostappearsforeigntothegraN,andis,therefore,capableofs)mula)ngitan)genically
• Thehostitselfmustbeincapableofmoun)nganeffec)veimmunologicalreac)onagainstthegraN,atleastforsufficient)meforthelamertomanifestitsimmunologicalcapabili)es;thatis,it(thegraN)musthavethesecurityoftenure

AcuteGvHD
• Reac)onofdonor’simmunesystemagainsttherecipient’sbody)ssues
• Manifestsasdiarrhea,skinrash,livertestabnormali)esusuallywithinthefirst100days.
• ~20-50%ofallogeneictransplantswilldevelopsomeaGvHD
• Associatedwitha15-20%mortality

AcuteGvHD 100DaySurvivalGradeI 78-90%GradeII 66-92%GradeIII 29-62%GradeIV 23-25%
Preven3on/ControlofaGvHDIsImportant
(Przepiorkaetal,1995)

• Prophylaxis–Preven3onofaGvHD• Treatment–TherapyofaGvHD

Pa)ent
AllogeneicBMT
RegularChemo±XRT
HighdoseChemo±
XRT
14-21days
Time
Donor

AcuteGvHDProphylaxis
• Micromethotrexate• Posttransplantcyclophosphamide• AlphabetaTcelldeple3onandCD34selec3on

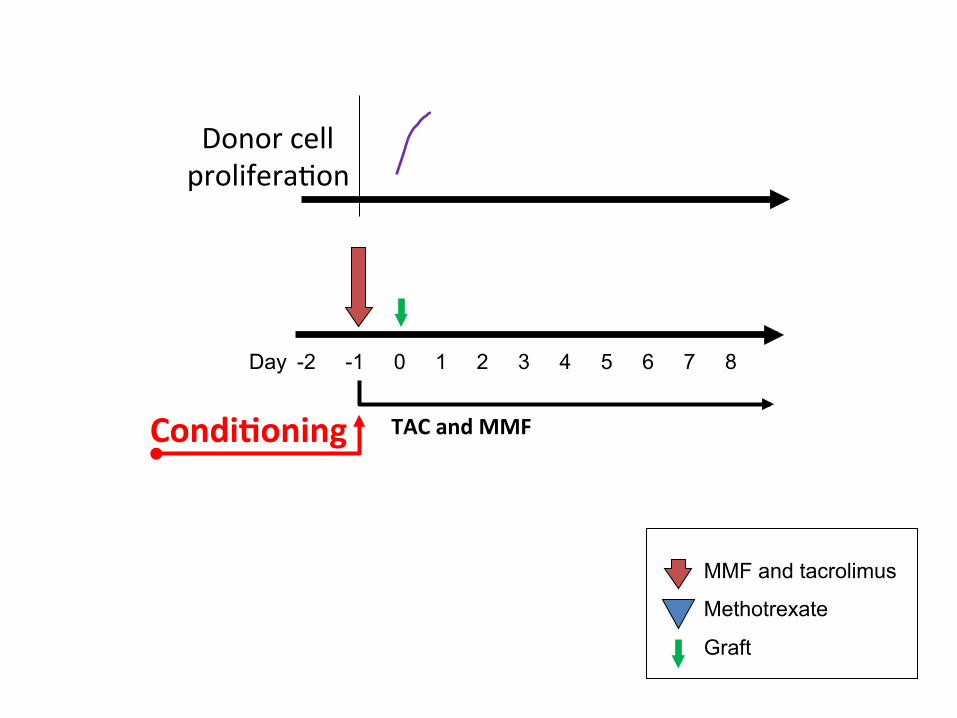
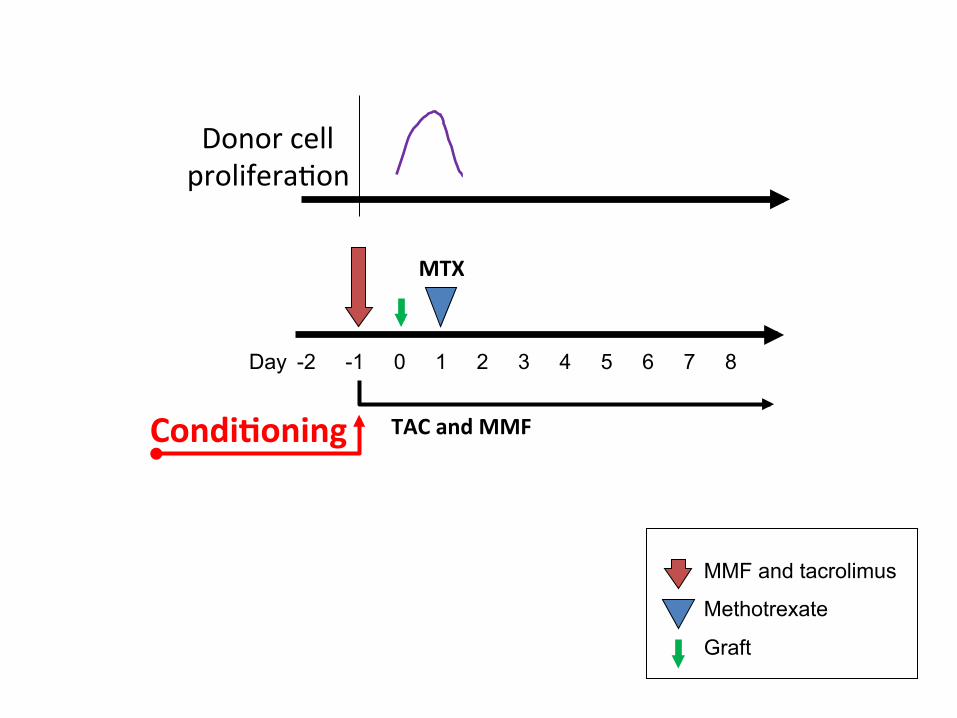
AcuteGvHDProphylaxis–µMTX
• Prophylaxiswithtacrolimus(TAC),mycophe-nolatemofe3l(MMF),andmethotrexate
• Methotrexate(2.5mg/m2isgivenondays1,3,6• MMFisgivenfromday-1un3lday60• TACisgivenfromday-1un3lday100.Atday100taperingbeginsun3lday180whenitisstopped.
• 21%ofpa3entsdevelopaGvHDdespiteprophylaxis

MMF and tacrolimus
Methotrexate
Graft
-2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMFCondi)oning

MMF and tacrolimus
Methotrexate
Graft
-2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMFCondi)oning
MMF and tacrolimus
Methotrexate
Graft
-2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMFCondi)oning
Donorcellprolifera3on
MMF and tacrolimus
Methotrexate
Graft
-2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
MTX
Condi)oning
Donorcellprolifera3on

MMF and tacrolimus
Methotrexate
Graft
-2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
MTX
Condi)oning
Donorcellprolifera3on

MMF and tacrolimus
Methotrexate
Graft
-2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
MTX MTX
Condi)oning
Donorcellprolifera3on

MMF and tacrolimus
Methotrexate
Graft
-2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
MTX MTX MTX
Condi)oning
Tcellprolifera3on

AcuteGvHDProphylaxis
• Micromethotrexate• Posttransplantcyclophosphamide
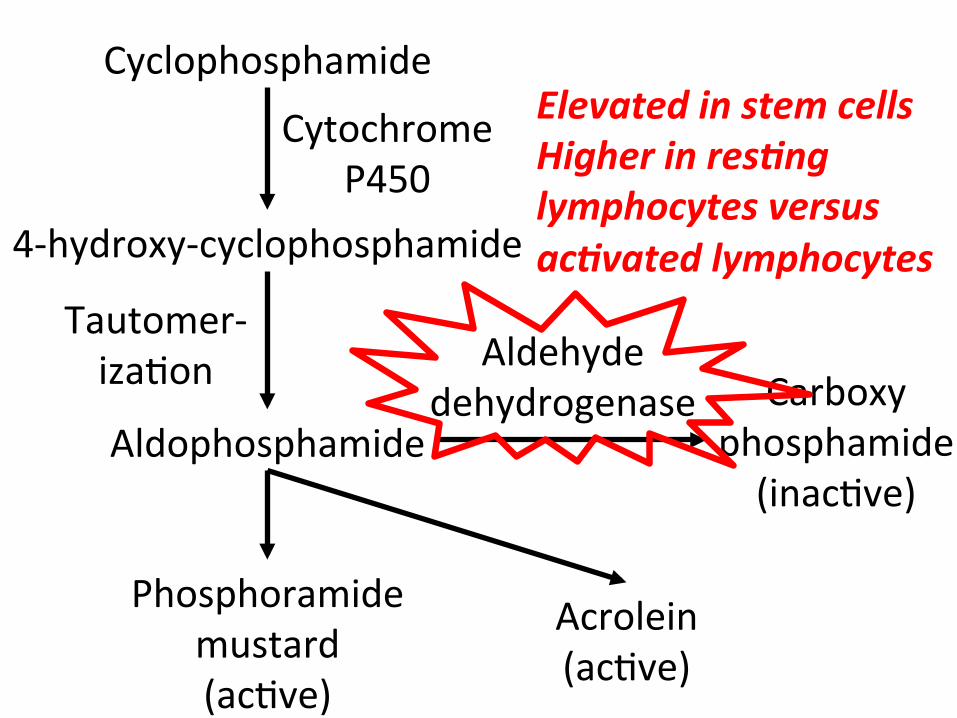
Cyclophosphamide
4-hydroxy-cyclophosphamide
CytochromeP450
Aldophosphamide
Phosphoramidemustard(ac3ve)
Acrolein(ac3ve)
Aldehydedehydrogenase Carboxy
phosphamide(inac3ve)
Tautomer-iza3on
ElevatedinstemcellsHigherinresAnglymphocytesversusacAvatedlymphocytes

MMF and tacrolimus
High dose CY
Graft
-6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
FLU-CY-TBI

MMF and tacrolimus
High dose CY
Graft
-6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
FLU-CY-TBI

MMF and tacrolimus
High dose CY
Graft
-6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
FLU-CY-TBI
Tcellprolifera3on

MMF and tacrolimus
High dose CY
Graft
-6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
CY
FLU-CY-TBI
Tcellprolifera3on

MMF and tacrolimus
High dose CY
Graft
-6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 Day
TACandMMF
CY
FLU-CY-TBI
Tcellprolifera3on
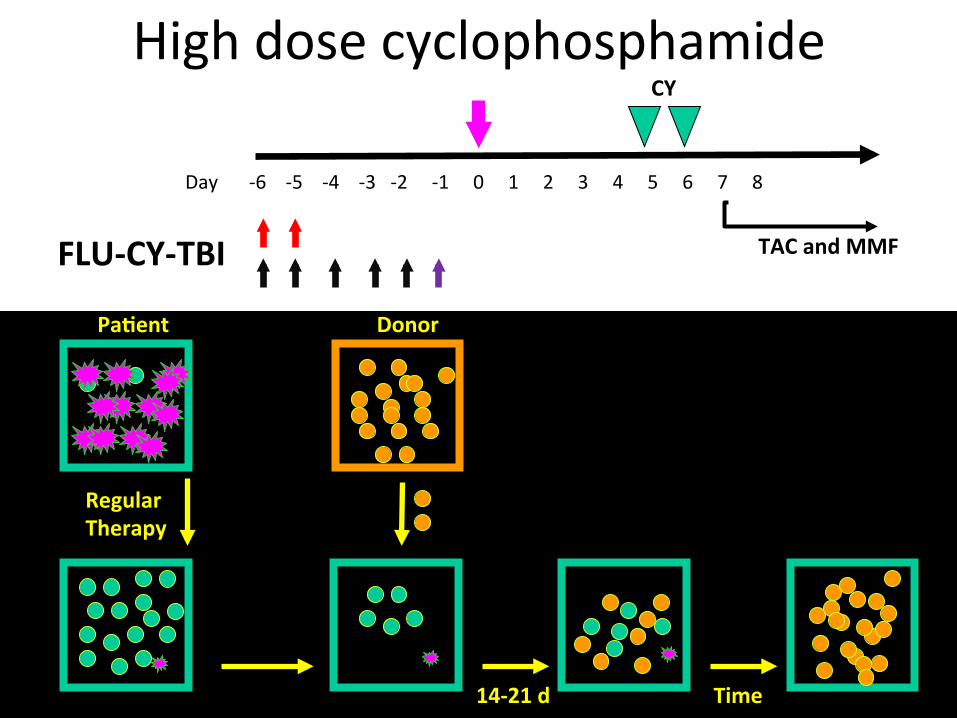
Highdosecyclophosphamide
-6-5-4-3-2-1012345678 Day
TACandMMF
CY
FLU-CY-TBI
RegularTherapy
14-21d
Pa)ent
Time
Donor

Highdosecyclophosphamide
-6-5-4-3-2-1012345678 Day
TACandMMF
CY
FLU-CY-TBI
RegularTherapy
14-21d
Pa)ent
Time
Donor

Highdosecyclophosphamide
-6-5-4-3-2-1012345678 Day
TACandMMF
CY
FLU-CY-TBI
RegularTherapy
14-21d
Pa)ent
Time
Donor

Highdosecyclophosphamide
-6-5-4-3-2-1012345678 Day
TACandMMF
CY
FLU-CY-TBI
RegularTherapy
14-21d
Pa)ent
Time
Donor

PostHCTcyclophosphamide(Cy)forGvHDDay0
76

PostHCTcyclophosphamide(Cy)forGvHD
77

PostHCTcyclophosphamide(Cy)forGvHD
78

PostHCTcyclophosphamide(Cy)forGvHDCy Cy
79

PostHCTcyclophosphamide(Cy)forGvHDCy Cy
XX 80

PostHCTcyclophosphamide(Cy)forGvHD
81

PostHCTcyclophosphamide(Cy)forGvHD
J
J
82

AcuteGvHDProphylaxis
• Micromethotrexate• Posttransplantcyclophosphamide• AlphabetaTcelldeple3onandCD34selec3on

RPCIProphylaxisRegimensPt-Cy uMTX
Ac)veagent Cyclophosphamide Methotrexate
Target Prolifera)ngTcells Prolifera)ngTcellsPlaceofac)on Invivo Invivo
Tcell Deple)on Deple)on
Other TacroCellcept
TacroCellcept
84

HCTforhematologicmalignancyHaplo* Standard#
Condi)oning Flu/Cy/TBI Flu/Mel/TBI
aGvHDprophylaxis Cy/Tac/MMF uMTX/Tac/MMF
GraNfailure 6% 0%
aGvHDGr.III-IV 3%(day180) 27%(day100)
Progressionfreesurvival 37%(3years) 44%(2years)
Overallsurvival 46%(3years) 47%(2years)*Kasamon,etal.JCO2015,#RPCIunpublisheddata 85

Somethingtothinkabout
• HowdoesBillingham’shypothesisexplainhowpost-transplantcyclophosphamidepreventsacutegraN-versus-hostdisease?
• WhatpropertydoescyclophosphamidehavethatenablesitsuseaNertransplantwithoutendangeringthegraN?
ChronicGraN-versus-HostDisease• Posttransplantcomplica)onusuallyoccurring>100dayscharacterizedby– Fibro)cskindisease– Dryandgrimymoutheyesduetoglandulardestruc)on
– Gastrointes)nalfibrosiswithmalnutri)on
• 50%oflongtermsurvivorswilldevelopsomeformofcGvHD
• ChronicGvHDisthemajorcauseoflongtermmortalityotherthanrelapseaNertransplant

C
B
C
D
D

ImportantConcepts• AutologousvsallogeneicHCT• Myeloabla)vevsreducedintensitycondi)oningregimens
• Autologous,syngeneic,matchedrelated,matchedunrelated,mismatchedandhaploiden)caldonors
• Acutevs.chronicgraNversushostdisease• Donorchimerism

Chimera
htp://www.theoi.com/Tartaros/Khimaira.html
KHIMAIRA(Greek)wasathreeheaded,fire-breathingcreaturewiththefore-partsofalion,thehindquartersofagoat,andthetailofaserpent.TheChimerawasslainbyBellerophonastridePegasus.
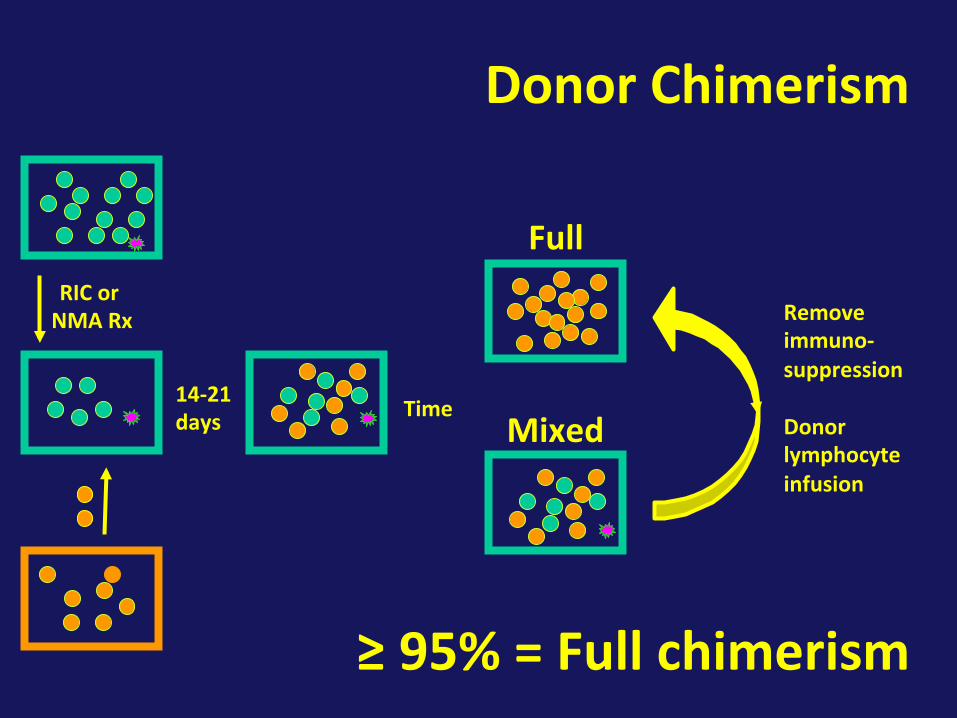
DonorChimerism
RICorNMARx
14-21days Time
Removeimmuno-suppressionDonorlymphocyteinfusion
Mixed
Full
≥95%=Fullchimerism