Embed Size (px)
Citation preview

Intracerebral Hemorrhage: Update on Management
Douglas W. Laske, MD
Chief, Division of Neurosurgery, Abington Memorial Hospital
Adjunct Professor of Neurosurgery, Temple University School of Medicine
Howard Eisenbrock, DO
Robert Lynagh, DO

Disclosures
• No financial disclosures or conflict of interest.
Epidemiology • For a patient who presents with the abrupt
onset of a new focal neurological deficit : • 5% are seizure, tumor or psychogenic • 95% are vascular
– 15% hemorrhagic • ICH, SAH, SDH
– 85% ischemic infarct • Lacunar, cardiogenic embolus, large artery
cerebrovascular lesion, atherosclerotic plaques in the aortic arch, unknown

Epidemiology • Incidence 12-15/100,000/yr • Intracerebral hemorrhage (ICH) is more than
twice as common as subarachnoid hemorrhage (SAH)
• Much more likely to result in death or major disability than cerebral infarction or SAH
• 35% to 50% can be expected to die within the first month after bleeding
• Only 10% of patients are living independently 1 month after the hemorrhage
• 20% are independent at 6 months

Epidemiology • Risk factors
– Advancing age and hypertension are the most important risk factors
– Age : after 55 doubles with each decade until 80 – Gender : more common in men – Ethnic : More common among young and middle-age blacks than whites of similar ages – More common in Asians (Japanese) compared to whites – Previous CVA increases risk by 23:1 – High alcohol intake – Drug abuse – Liver dysfunction

Epidemiology • Locations of hemorrhage
– Putamen, lenticular nucleus, internal capsule, globus pallidus 50%
– Thalamus 15% – Pons 10-15% – Cerebellum 10% – Cerebral white matter 10% – Brain stem 6%
• Common arterial feeders of ICH – Lenticulostriates – putaminal – Thalamoperforators – Paramedian branches of the basilar artery

Epidemiology • Lobar hemorrhage vs deep hemorrhage
– Hemorrhage into the occipital, temporal, frontal and parietal lobes as opposed to deep structures – BG, thalamus, infratentorial structures
– More likely associated with structural abnormalities – More common in patients with high alcohol consumption – More benign outcome – Causes
• Extension of deep hemorrhage • Cerebral amyloid angiopathy • Trauma • Hemorrhagic transformation • Tumor • AVM/aneurysm

Rebleeding
• Early rebleeding – Usually with deterioration – 33-38% in 1-3 hours, 16% in 3-6, 14% at 24hrs – Pts with enlarging hematomas assoc. with larger
size and/or coagulopathy – Those more likely to rebleed have
• Hx cva,liver dz,DM,sbp>195, ETOH abuse,coagulopathy,hematoma >25cm3 ,irregular shape to hematoma, high WBC, elevated temp

Etiologies • Classified as either primary or secondary
hemorrhage – Primary: spontaneous rupture of small vessels
damaged by chronic HTN or amyloid angiopathy – Secondary: vascular lesions (AVM, aneurysm,
AVDF, cavernoma), tumors, previous CVA, impaired coagulation, CNS infection, sinus thrombosis, post-traumatic, drugs, pregnancy related, following craniotomy

Etiologies • Primary
– HTN: causes degenerative changes in walls of small penetrating arteries
– Decreases vessel compliance-increasing chance of rupture
• Annual risk ICH with chronic HTN: 2%
– 1868 Charcot and Bouchard • Attributed to rupture to points of dilation in walls of
small arterioles= microaneurysms • Later found to be subadventitial hemorrhages from
endothelial damage by hematoma

Etiologies
• Primary – Amyloid angiopathy
• Beta-amyloid protein deposits within media of small and medium size arteries
• ICH in white matter of the cerebral lobes • Usually >70yo (50% of pts over 70 have amyloid) • 10.5% per year risk of hemorrhage

Etiologies • Amyloid angiopathy Dx
1.Definite CAA Post mortem analysis: shows lobar,cortical or subcortical
hemorrhage, severe CAA,and absence or another diagnosis 2.Probable with path evidence same as above with difference being some amyloid deposition 3.Probable CAA Clinical + MRI findings: Age> 60,multiple hemorrhage in
cortical,subcortical,lobar. Absence of other cause 4. Possible CAA age>60. single lobar,cortical,subcortical hemorrhage without
another cause, or if multiple bleeds with unclear cause

Etiologies • Secondary ICH
– Metastases • Present in 3-14% of mets • Most common mets to bleed RCC(60-70%), melanoma(40%),
choriocarcinoma(50%),thyroid(25%) • Bronchogenic Ca (9%) most common due to prevelance
– Vascular malformations • Usually AVM’s: 81% when bleed has sig. intraparenchymal component • Cavernous malformations • Aneurysm

Etiologies • Secondary ICH cont.
– Oral anticoagulant use • Relative risk increases x10 for>50 yo • Warfarin for a-fib associated with 1-2% per year risk of ICH
with 65% mortality – TPA
• Incidence of symptomatic ICH within 36 hours is 6.4% – Coagulopathies – Leukemia – Prior CVA – Recent surgery (carotid or craniotomy)

Etiologies
• Secondary ICH cont – CNS infections
• Fungal,herpes
– Venous sinus thrombosis – Substance abuse
• >3 drinks/day inc. risk x7
– Pregnancy • 1 in 9500 births • Assoc. with eclampsia or pre-eclampsia

Primary ICH Outcomes
• ICH score (system of Hemphill et al.) – GCS Score - 2 points if 3-4, 1 point if 5-12 – ICH volume - 1 point if at least 30cc – IVH - 1 point if IVH – Infratentorial - 1 point if infratentorial origin – Age - 1 point if at least 80 years old

Primary ICH Outcomes
• 30 Day Mortalities for Total ICH Scores: – 0 = 0% – 1 = 13% – 2 = 26% – 3 = 72% – 4 = 97% – 5 = 100% – 6 - estimated to be 100%, no patients in the study
fell under this category Hemphill J C et al.: The ICH Score. Stroke. 2001;
32:891-897.

Management

Management

Management • Imaging
– Rapid neuroimaging with CT or MRI is recommended to distinguish ischemic stroke from ICH (Class I; Level of Evidence: A). (Unchanged from the previous guideline)
– CT angiography and contrast-enhanced CT may be considered to help identify patients at risk for hematoma expansion (Class IIb; Level of Evidence: B), and CT angiography, CT venography, contrast-enhanced CT, contrast-enhanced MRI, magnetic resonance angiography, and magnetic resonance venography can be useful to evaluate for underlying structural lesions, including vascular malformations and tumors when there is clinical or radiological suspicion (Class IIa; Level of Evidence: B). (New recommendation)

Value of CTA/DSA • From a prospective study of 206 ICH cases evaluated w CT
and angiography – Angiographic yield
• Lobar ICH in patients >45y w preexisting HTN = 10% • Putaminal, thalamic, and posterior fossa hemorrhages in patients of
all ages with preexisting HTN = 0% • Lobar ICH in patients <45y = 65% • Putaminal, thalamic, and posterior fossa hemorrhages in
normotensive patients <45y = 48% • Putaminal, thalamic, and posterior fossa hemorrhages in
normotensive patients >45y = 7% • CTA warranted in all patients <45 years and those >45 years
without history of preexisting HTN in areas of bleed other than putaminal, thalamic, pons or cerebellum
Medical treatment
• BP control • Correct anticoagulation • ICP monitoring • Mannitol, Hypertonic saline • Ventricular drainage • Antiseizure medication • Aggressive treatment of fever • Treat hyperglycemia

Management
Based on INTERACT and ATACH trials

INTERACT 1 and 2 (Intensive BP Reduction in Acute Cerebral Hemorrhage Trials)
• Wanted to look at whether aggressive BP control (SBP goal < 140 mmHg) was safe and subsequently more beneficial when compared to standard care of treating SBP >180 mmHg
• Interact 1 found a 36% lower risk of hematoma growth in the intensively treated group
• Interact 1 also found that the risk of adverse advents was not statistically significant when compared to standard treatment
• Interact 2 was planned to assess outcomes between the two groups

INTERACT2

Design • Multicenter, prospective, randomized, open-treatment,
blinded end point trial • Compared effect of targeting a lower blood pressure within
1 hour for those with SBP between 150-220 mmHg • Intensive treatment group: SBP was to be maintained <140
mmHg for 7 days • Standard treatment group: SBP > 180 mmHg was treated as
needed without a goal identified • Patients were excluded if they had a clear contraindication
to BP lowering, if they had GCS < 6, massive hematoma with poor prognosis, or were planned for early surgery

Results
• No statistical difference in death or major disability
• Improved functional outcome in aggressive BP control group
• No significant difference in treatment related complications

Management • Seizures and Antiepileptic Drugs
– Clinical seizures should be treated with antiepileptic drugs (Class I; Level of Evidence: A). (Revised from the previous guideline)
– Continuous EEG monitoring is probably indicated in ICH patients with depressed mental status out of proportion to the degree of brain injury (Class IIa; Level of Evidence: B).
– Patients with a change in mental status who are found to have electrographic seizures on EEG should be treated with antiepileptic drugs (Class I; Level of Evidence: C).
– Prophylactic anticonvulsant medication should not be used (Class III; Level of Evidence: B). (New recommendation)

Management • Hemostasis/Antiplatelets/Deep Vein Thrombosis Prophylaxis
– Patients with a severe coagulation factor deficiency or severe thrombocytopenia should receive appropriate factor replacement therapy or platelets, respectively (Class I; Level of Evidence: C). (New recommendation)
– Patients with ICH whose INR is elevated due to OACs should have their warfarin withheld, receive therapy to replace vitamin K–dependent factors and correct the INR, and receive intravenous vitamin K (Class I; Level of Evidence: C). PCCs have not shown improved outcome compared with FFP but may have fewer complications compared with FFP and are reasonable to consider as an alternative to FFP (Class IIa; Level of Evidence: B). rFVIIa does not replace all clotting factors, and although the INR may be lowered, clotting may not be restored in vivo; therefore, rFVIIa is not routinely recommended as a sole agent for OAC reversal in ICH (Class III; Level of Evidence: C). (Revised from the previous guideline).

Treatment • FAST trial (randomized to 20 or 80 ug/kg rFVIIa for ICH within 4
hours) – Treatment with 80 μg significant reduction in growth in volume of the
hemorrhage. – The mean increase in volume of the ICH at 24 hours was 26% in the
placebo group, 18% in the group receiving 20 μg (P=0.09) and 11% in the group receiving 80 μg (P<0.001).
– The growth in volume of ICH was reduced by 2.6 ml (95% confidence interval [CI], −0.3 to 5.5; P=0.08) in the group receiving 20 μg and by 3.8 ml (95% CI, 0.9 to 6.7; P=0.009) in the group receiving 80 μg
– no significant difference among the three groups in the proportion of patients with poor clinical outcome (24% in the placebo group, 26% in the group receiving 20 μg, and 29% in the group receiving 80 μg
– frequency of thromboembolic serious adverse events was similar in the three groups; arterial events were more frequent in the group receiving 80 μg (9% vs. 4%, P=0.04).

Management
• Hemostasis/Antiplatelets/Deep Vein Thrombosis Prophylaxis – Although rFVIIa can limit the extent of hematoma
expansion in noncoagulopathic ICH patients, there is an increase in thromboembolic risk with rFVIIa and no clear clinical benefit in unselected patients. Thus rFVIIa is not recommended in unselected patients. (Class III; Level of Evidence: A). (New recommendation) Further research to determine whether any selected group of patients may benefit from this therapy is needed before any recommendation for its use can be made

Management • The usefulness of platelet transfusions in ICH patients
with a history of antiplatelet use is unclear and is considered investigational (Class IIb; Level of Evidence: B). (New recommendation)
• Patients with ICH should have intermittent pneumatic compression for prevention of venous thromboembolism in addition to elastic stockings (Class I; Level of Evidence: B). (Unchanged from the previous guideline)
• After documentation of cessation of bleeding, lowdose subcutaneous low-molecular-weight heparin or unfractionated heparin may be considered for prevention of venous thromboembolism in patients with lack of mobility after 1 to 4 days from onset (Class IIb; Level of Evidence: B). (Revised from the previous guideline)

Treatment • Guidelines for Surgery(AHA/ASA) • 1. For most patients with ICH, the usefulness of
surgery is uncertain (Class IIb; Level of Evidence: C). (New recommendation) Specific exceptions to this recommendation follow
• 2. Patients with cerebellar hemorrhage who are deteriorating neurologically or who have brainstem compression and/or hydrocephalus from ventricular obstruction should undergo surgical removal of the hemorrhage as soon as possible (Class I; Level of Evidence: B). (Revised from the previous guideline) Initial treatment of these patients with ventricular drainage alone rather than surgical evacuation is not recommended (Class III; Level of Evidence: C). (New recommendation)
Treatment • Guidelines cont. • 3. For patients presenting with lobar clots >30 mL and within 1 cm
of the surface, evacuation of supratentorial ICH by standard craniotomy might be considered (Class IIb; Level of Evidence: B). (Revised from the previous guideline)
• 4. The effectiveness of minimally invasive clot evacuation utilizing either stereotactic or endoscopic aspiration with or without thrombolytic usage is uncertain and is considered investigational (Class IIb; Level of Evidence: B). (New recommendation)
• 5. Although theoretically attractive, no clear evidence at present indicates that ultra-early removal of supratentorial ICH improves functional outcome or mortality rate. Very early craniotomy may be harmful due to increased risk of recurrent bleeding (Class III; Level of Evidence: B). (Revised from the previous guideline)

Craniotomy • The most widely used surgical intervention in ICH is craniotomy and
evacuation of the gross clot. • In 1903, Cushing first removed an intracerebral hematoma by
craniotomy • This is a relatively invasive procedure associated with additional
risks by subjecting patients to surgery with brain manipulation, and anesthesia
• Position head so that trajectory to clot is near vertical • Bipolar cautery and small suction tips can be used to dissect down
to the hematoma under magnification • Once clot is evacuated, hemostatic agents such as FloSeal,
hydrogen-peroxide soaked cotton balls, thrombin-soaked Gelfoam, Avitene or surgicel may be used to obtain hemostasis of the cavity
• Option of craniectomy

Craniotomy • Corticotomies are placed near the epicenter of the ICH
, their length is minimized, eloquent tissue is avoided • Avoid usage of self-retaining retractors as steady
retraction is deleterious to brain parenchymal. • The center of hematoma is removed first with the
remaining marginal clot then collapses and can likewise be evacuated.
• Particular attention to bleeding points and possible subtle pathologic findings such as small tumors, cryptic AVMs and cavernous angiomas .
• All tissue is sent for histologic analysis .
Youmans Neurological Surgery Fifth Edition Volume 2 : Chapter 105 pages 1733-1768

Surgery • Timing of Surgery
– In the case of spontaneous ICH, earlier interventions would intuitively appear superior
– Early evacuation of hematoma improves CBF, brain edema, ischemia, and outcome.
– It is supported by the following • 50% death of patient with ICH occur within 48 hours of
hemorrhage • Radiographic expansion or rebleeding occurs maximally
within 3-4 hours • Exacerbation occurs suddenly and most often within 4 to 6
hours of bleeding • Secondary changes such as edema occur 7 to 8 hours after a
hemorrhage

Surgery • Timing:
– Kaneko and colleagues[1983] also demonstrated superior outcomes (relative to epidemiological data) when they reported a 6-month 7% mortality rate in a series of patients with 100 putaminal ICHs treated surgically within 7 hours of ictus
– Zuccarello M, Brott T, Derex, et al [1999] and Morgenstern LB, Frankowski RF, Shedden P, Pasteur W, Grotta JC; Surgical treatment for intracerebral hemorrhage [1998] are 2 pilot studies suggested a benefit with early surgery (<12 hours) but were limited by small numbers.
– Morgenstern and colleagues[2001] showed that ultra-early surgery (4 hours after ICH) is associated with increased re-hemorrhage and mortality rates
Neurosurg Focus 15 (4):Article 2, 2003, Update on management of intracerebral hemorrhage, NADER POURATIAN, M.D., PH.D., NEAL F. KASSELL, M.D., AND AARON S. DUMONT, M.D.

Surgery
• Patient selection learned from case series – Patients with relatively normal consciousness (GCS
Scores 13–15 ) rarely require surgery, whereas deeply comatose patients (GCS Scores 3–5 ) rarely benefit from surgery
– Surgery is therefore usually considered to have the most potential benefit for the group of patients with GCS scores between 6 and 12 or in patients with deteriorating status Neurosurg Focus 15 (4):Article 1, 2003, Spontaneous intracerebral hemorrhage: a review MATTHEW E. FEWEL, M.D., B.
GREGORY THOMPSON, JR., M.D., AND JULIAN T. HOFF, M.D

Treatment • Volume
– Volpin et al, Neurosurgery (1984) retrospective reviewed of 132 patients with supratentorial ICH,
• Those with hematoma volume >85cm3 have 100% mortality irrespective of treatment
• Those with hematoma volume <26cm3, all survived without surgery
– Large-volume thalamic hematoma are more devastating than similar sized subcortical or putaminal hematomas
– For infratentorial hematomas, all cerebellar hematomas greater than 3 cm in diameter are recommended for surgery

Surgery
• High level evidence from prospective, randomized clinical trials of surgery for ICH was needed to inform clinical practice – STICH 1 – STICH2 – MISTIE 3

STICH I

Method • 1033 patients were recruited from 107 centers • Patients must have spontaneous supratentorial ICH
that arose within 72hours of randomization and the neurosurgeon was uncertain to benefits of either treatment
• Minimal hematoma diameter of 2cm • Must have GCS of 5+ • Primary outcome measure: extended Glasgow
outcome score at 6 months • Secondary outcomes measured were mortality and the
modified Rankin scale

Outcome measurement • Patients were given an initial prognostic score based on an
equation – Prognostic score = (10 x admission GCS)-age (years) – (0.64 x
volume mL) • Patients were placed in either good or poor prognostic
groups based on the median prognostic score • For the poor prognostic group:
– Favorable outcome included good recovery, moderate disability, and upper severe disability categories of the extended GOS
• For the good prognosis group: – Favorable outcome included good recovery and moderate
disability


Hematoma characteristics


Surgical details

6 month outcome

Survival
STICH I Outcomes • No significant difference in the primary outcome between
those treated with early surgery and those who underwent initial conservative management
• The only significant finding was that patients with hematomas 1cm or less from the cortical surface were more likely to have a favorable outcome (29% relative benefit)
• In those with initial GCS or 8 or less there was near uniform poor outcomes
• In terms of cost analysis, those who underwent early surgery tended to have shorter stays and require less services at discharge – As a result the early surgery group had lower overall costs

STICH II

STICH II • To analyze the benefit of early surgical intervention for
hematoma evacuation in those with ICH of significant volume and that is reasonably accessible without traversing eloquent cortex
• Based on the subgroup analysis results from STICH I that showed better outcomes in those who had early craniotomy and clot evacuation with a hematoma within 1cm of the cortical surface
• Hypothesis: early surgery would improve outcomes in conscious patients with a superficial ICH of 10-100mL without any IVH

Methods • Multicenter, prospective, randomized, parallel group
trial • 129 neurosurgical units in 39 countries • Must have spontaneous lobar ICH within 1cm of the
cortical surface • Volume between 10-100 mL • Presentation within 48h of ictus • Best GCS motor score of 5 or 6 • Best GCS eye score of 2+ • Excluded if includes the BG, thalami,
cerebellum, brain stem or if there is IVH

Methods
• Hematoma must be evacuated within 12 hours
• Delayed evacuation was permitted in the conservative group if deemed appropriate
• Primary outcome: prognosis based favorable or unfavorable outcome based on extended GOS survey at 6 months – 10 × GCS – age – 0・64 × volume


Patient characteristics

Characteristics

Hematoma characteristics

Surgical patient characteristics
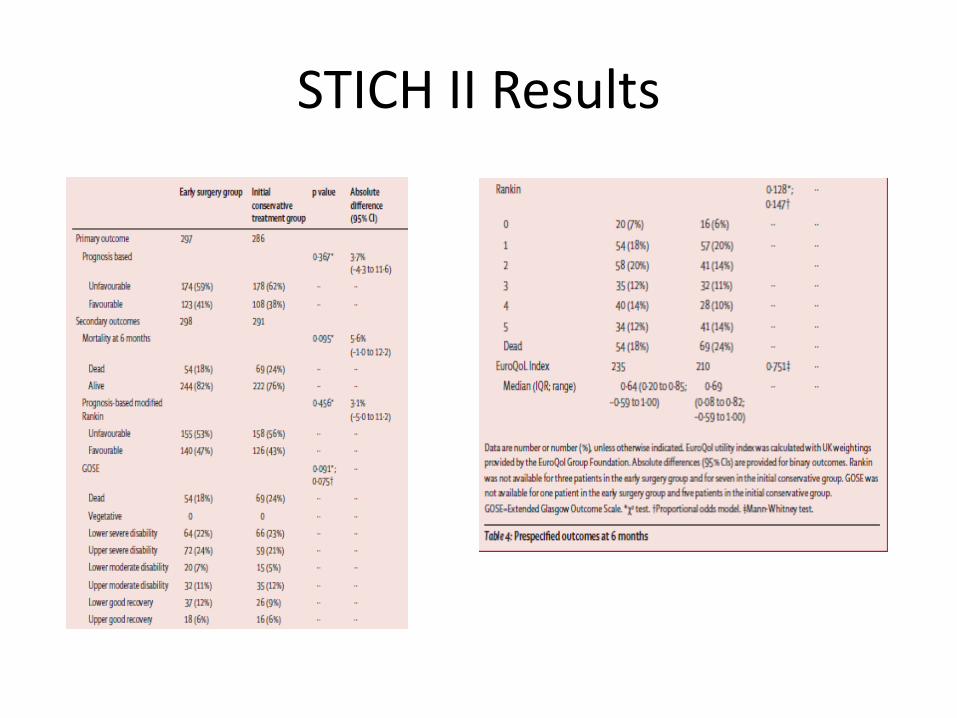
STICH II Results

STICH II Results

STICH II summary • No significant evidence to support early surgery in
general
• Patients with poor prognosis had significantly better outcomes in the early surgical group vs the initial conservative treatment group
• Patients with GCS of 9-12 benefit from early surgery
• 21% of the initial conservative management group crossed over to surgery due to depressed mental status
• These patients may have died without surgery

Surgery for ICH • Surgery provides benefit to subgroups of patients with ICH. •Would minimally invasive hematoma removal cause less brain trauma than open surgery and prove more efficacious, particularly with deep hematomas?

Stereotactic aspiration • First used by Benes and coworkers in 1965 with
limited success and only in 1978, Backlund and Von Holst performed first successful stereotactic aspiration of an acute hemorrhage.
• Some of these early series suggested a more favorable outcome than craniotomy in deep-seated hemorrhages.
• However, lack of direct visualization and the risk of rebleeding may limit this technique’s utility especially during the hyper acute phase of hemorrhage.

Endoscopy • Minimally invasive technique • One study used a 6 mm diameter
neuroendoscope which was placed through a burr hole and guided by intraoperative ultrasonography
• Associated with good outcome in about 50% of the patients with more than 70% clot evacuated
• There were no differences in outcome for putaminal or thalamic hemorrhages
Youmans Neurological Surgery Fifth Edition Volume 2 : Chapter 105 pages 1733-1768

Stereotactic aspiration • In 1985, Niizuma et al reported a CT-guided technique of
hematoma aspiration and lysis using urokinase . • Fibrinolysis is used to facilitate clot dissolution by activating
plasminogen, which dissolves fibrin. • Localization by direct-image projection on CT scanner with a
radiopaque marker has approximately 5mm error compared to stereotaxy.
• After localization, 3-4mm silicone tube is passed into the clot and hematoma is aspirated with a syringe repeatedly until no more clot is removed.
• Then a Dandy ventricular catheter is placed into the hematoma bed, and urokinase ( 6000 U in 3 ml ) is infused, repeated two to four times a day in 1 to 6 days until CT documents clot resolution.

Stereotactic aspiration
• Naff et al . [Neurosurgery, 2004, Class I] randomized 48 patients with spontaneous IVH to receive placebo or 3 mg TPA injected every 12 hours into the ventricle. Clot resolution was faster in the TPA group , and there was a trend toward lower mortality , although bleeding complications were greater in patients receiving TPA
• Lee et al . [ Hong Kong Med J 2003 , Class III] reported on 29 patients with IVH treated with intraventricular streptokinase or urokinase, and found that blood could be removed safely (infection rate 3%, no bleeding) and effectively

Multicenter, International Phase III
randomized trial
PI: Daniel F. Hanley, MD
Minimally Invasive Surgery +
rt-PA for ICH Evacuation


+20 Hr. +42 Hr. +52 Hrs. Pre-surgery
Surgical Intervention Post-Surgery
3D post-op & post rt-PA

MISTIE II
Exclusion
Infratentorial ICH
Vascular malformation or brain tumor
Irreversibly impaired brainstem function
Inclusion Age 18-75
GCS < 13 or NIHSS > 6
Spontaneous supratentorial ICH > 20cc
Stable clot at second CT scan performed > 6 hours after diagnosis

Outcome measure: Modified Rankin Scale

14%

MISTIE II – Benefits summary
What’s next?
Test in a larger population in MISTIE III
-14% improvement in mRS 0-2 -38 fewer days in hospital -$44,000 savings per subject -14% fewer 365-day subjects in long-term care
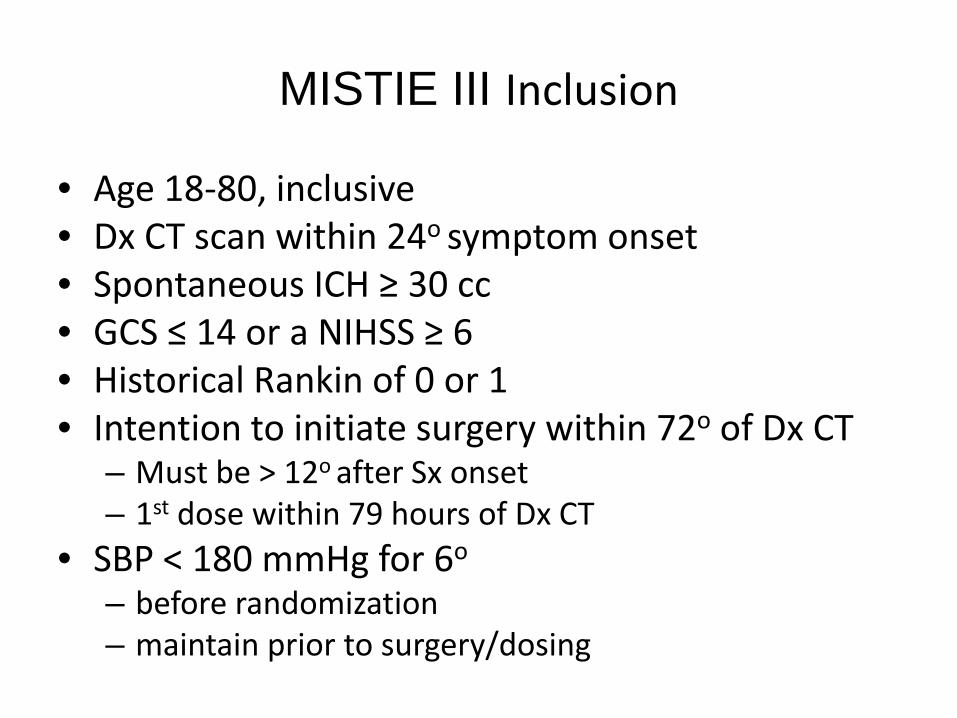
MISTIE III Inclusion
• Age 18-80, inclusive • Dx CT scan within 24o symptom onset • Spontaneous ICH ≥ 30 cc • GCS ≤ 14 or a NIHSS ≥ 6 • Historical Rankin of 0 or 1 • Intention to initiate surgery within 72o of Dx CT
– Must be > 12o after Sx onset – 1st dose within 79 hours of Dx CT
• SBP < 180 mmHg for 6o – before randomization – maintain prior to surgery/dosing

Hemorrhage Volume
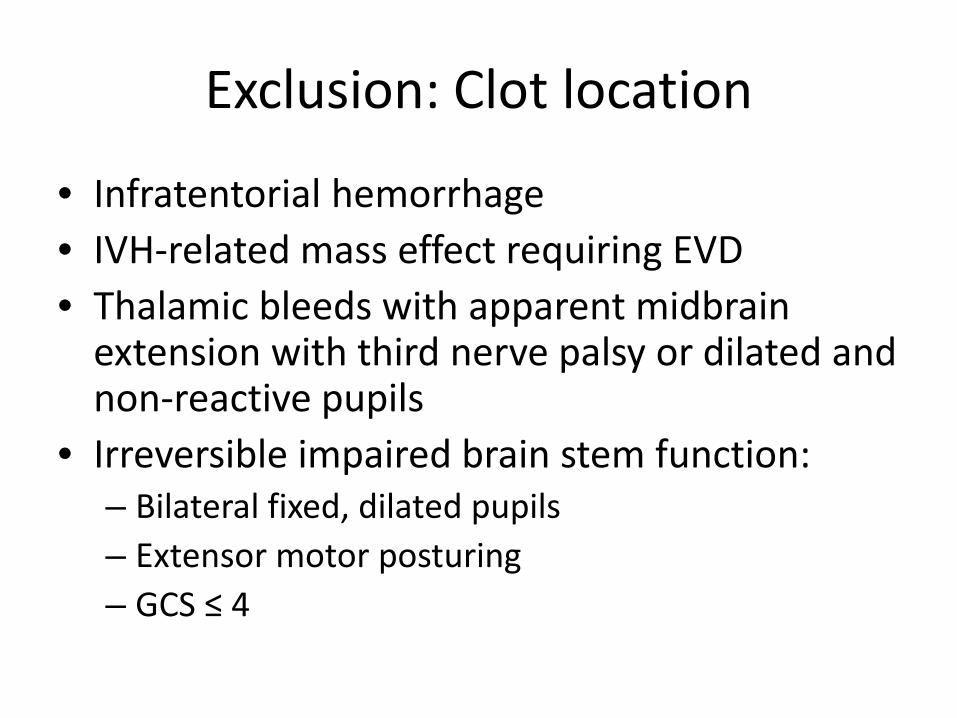
Exclusion: Clot location
• Infratentorial hemorrhage • IVH-related mass effect requiring EVD • Thalamic bleeds with apparent midbrain
extension with third nerve palsy or dilated and non-reactive pupils
• Irreversible impaired brain stem function: – Bilateral fixed, dilated pupils – Extensor motor posturing – GCS ≤ 4

Exclusion: Underlying Pathology
• Untreated ruptured cerebral aneurysm • Ruptured intracranial AVM • Vascular anomaly, such as
– Treated aneurysm or AVM within 90 days – Tumor – Choroid plexus vascular malformation
• Moyamoya disease • Unstable mass or evolving intracranial
compartment syndrome

Protocol At-A-Glance
ICH
BP control MRI/MRA or CTA to rule out underlying
pathology
CT to Demonstrate ICH Stability & acquire images for Surgical Planning and Image Guidance
Consent & Randomization
Surgical Management: Initiate surgery and give 1.0 mg rt-PA Q8hr for up
to 9 doses
6+ hrs
MISTIE III
Dosing
Day: 1 2 3 4 5 6 7 30 90 180 270 365
= CT scan = MRI = Dose
Diagnostic Stability
MIS Surgery
Post-Surgery
*green indicates surgical patients only
24hr post-removal
Catheter Removal
Follow-up
Randomization

Cerebellar ICH • No evidence from randomized trials of benefits of surgical
evacuation in ICH • Evidence mostly in the form of case series • Kobayaski S, Miyata A, Serizawa T, et al. Treatment of
cerebellar hemorrhage—surgical or conservative. Stroke. 1990; 21(8) Suppl: I-62. – Design: Non-randomized Prospective – Patients: 75 patients with cerebellar hemorrhage
• 45 treated medically • 30 treated with decompressive surgery
– Patients with GCS < 13, and hematoma > 40 mm – Good outcome occurred 58% with surgery while only 18% with
conservative medical therapy

On the Horizon • SLEUTH
Safety of Lysis with EKOS Ultrasound in the Treatment of Intracerebral and Intraventricular Hemorrhage
• SHRINC Safety of Pioglitazone for Hematoma Resolution In Intracerebral Hemorrhage [SPORTIAS]
• Simvastatin For Intracerebral Hemorrhage Study • STOP-IT
The Spot Sign for Predicting and Treating ICH Growth Study
• PATCH Platelet Transfusion in Cerebral Hemorrhage

Thank you