Embed Size (px)
Citation preview

CASE REPORT
Hibernoma of the antero-lateral thigh
C. Della Volpe, B. Salazard*, D. Casanova, H. Vacheret,J.F. Bartoli, G. Magalon
Department of Plastic and Reconstructive Surgery, Hopital de la Conception, 147 Boulevard Baille, 13385Marseille Cedex 05, France
Received 25 May 2004; accepted 14 January 2005
S0do
etco
KEYWORDSHibernoma;Sarcoma;Fatty tumour;Brown fat
007-1226/$ - see front matter q 20i:10.1016/j.bjps.2005.01.020
* Corresponding author. Address: Serreparatrice du Professeur Guy
nception, 13005 Marseille, France. TE-mail address: bruno.salazard@wa
Summary Hibernoma is a rare benign tumour of brown fat. In most cases itpresents as a voluminous slow-growing mass in the regions where remnants of brownfat can remain in adults. We report a case of a hibernoma on the thigh and presentthe diagnostic and therapeutic elements of this type of tumour, whose differentialdiagnosis of liposarcoma.q 2005 The British Association of Plastic Surgeons. Published by Elsevier Ltd. Allrights reserved.
Hibernoma is a rare and benign tumour of the softtissue that was first described by Merckel in 1906.Less than 200 cases have been reported in theliterature.1,2 It is a tumour developed from foetalbrown fat tissue, vestigial remnants of the evol-ution of the species.2 In adults, it is usually found inthe regions where islets of brown fat remain in thescapular3 and posterior cervical regions and morerarely, in the folds of the buttocks or the thigh.4–6
Diagnosis is difficult and there is often confusionwith a liposarcoma or intramuscular lipoma. Treat-ment is surgical since only excision can provide adiagnosis and eliminate differential diagnoses. Wepresent a case of hibernoma of the lateral thigh.
05 The British Association of Pl
vice de chirurgie plastiqueMagalon, Hopital de lael.: C33 610 310 380.nadoo.fr (B. Salazard).
Case report
A 28-year-old woman presented with a voluminousmass that had been enlarging for 2 years on theexternal side of the right thigh. She presented nochronic pathology and had no surgical history.
The clinical examination revealed a well definedsolid tumour, adherent to surrounding muscle butwhich caused no pain on palpation.
Recent ultrasonography showed an increase inthe diameter of the right thigh with a fibrousstructure, hyperechoic and well delineated,measuring 2 cm in thickness, over 12 cm in heightand over 10 cm in width, corresponding to anintramuscular lesion of the anterior side of thethigh.
An associated Doppler examination revealedrich vascularisation of this structure. CT scanshowed a hypodense, rather vascular mass, withcentral necrosis (Fig. 1). The lesion essentiallyoccupied the rectus femoralis muscle and its
British Journal of Plastic Surgery (2005) 58, 859–861
astic Surgeons. Published by Elsevier Ltd. All rights reserved.

Figure 1 CT scan of the thigh.
C. Della Volpe et al.860
inferior two-thirds encompassed and was attachedto the entire vastus lateralis. The latter wascompressed, but the tumour appeared had clearlydefined margins. There was no identifiable associ-ated bone lesion. The chest X-ray was normal. Nodiagnosis was made at that time.
Figure 2 MR imaging, T1-weighted image, sagittalview.
MR imaging demonstrated on T1W a superficialmass on the antero-lateral side of the thigh onmixed spontaneoushyperenhancement (Figs. 2 and3).It showed infiltration with compression on theforward part of the rectus femoralis, flatteningwith its posterior part of the vastus lateralis muscleand the femoral pedicle by pushing them againstthe femoral bone. T2W made it possible to deletethe fatty structure of the lesion in order to observesome blood flow phenomena such as suffusion.Injection of gadolinium clearly enhanced the lesion.MR imaging concluded this was a lesion in the softtissue with a fatty matrix because of the relativelywell-defined, but mixed T1-weighted signal. Thepossible diagnosis of liposarcoma dictated surgicalexcision.
Surgical excision was performed under generalanaesthesia. A deep-seated tumour was foundcompressing the muscles in their compartment.Dissection began with the distal part where it wasnot adherent, then proximal where the tumour wasattached to the deep muscles and the cruralpedicle. The surgical specimen was sent to thehistology laboratory. Biopsy samples were alsotaken near the lesion.
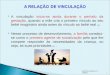
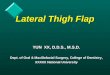
The histological results reported a proliferationwith lobular architecture (Fig. 4) composed ofround or oval monomorphic micro-vacuolatedcells that contained eosinophilic granules (Fig. 5),with no mitotic cells or nuclear atypia, character-istic of a brown fat benign tumour or hibernoma. Notumoural infiltrate was detected in biopsies fromsurrounding tissues.
Figure 3 MR imaging, T1-weighted image, axial view.
Figure 4 Histologic image with lobular proliferation.Figure 5 Histologic image with micro-vacuolated cellsthat contained eosinophilic granules.
Hibernoma of the antero-lateral thigh 861
Discussion
Brown fat is a remnant from the evolution ofspecies—it participates in the thermogenesis ofhibernating mammals. In man, it is found physio-logically in newborns in the axillary and thesubpleural regions but is said to disappear after 8weeks of life.3
Slight quantities can remain in adults in thescapular region and more rarely, in the axillary,3
mediastinal, cervical, gluteus regions, the thigh,4–6
or the popliteal cavity which are the favouredregions for hibernomas.7 No malignant transform-ations have ever been reported in the 100 or socases in the literature.
Today, it is generally agreed that this benigntumour can be diagnosed by MRI with the followingcharacteristics: T1- and T2-weighted images, evo-cative of a fatty signal. In T1, the signal of theentire tumour was not exactly similar but wasdiscretely lower than that of the subcutaneous fat.This signal was evocative of a hibernoma.8,9 In T1inside the tumour, there were areas of intermedi-ate signals between that of the muscle and thesubcutaneous fat. Contrast enhancement was sig-nificant after injection of gadolinium, particularlyin low-signal areas. In T2, the mass signal was oftenvery near that of the subcutaneous fat.8,9
Surgical excision is indispensable because of thediscomfort that is often associated with the tumourand more especially, for histologic confirmation.
Indeed, hibernoma resembles liposarcoma diagnos-tically at a local stage. The rate of development andthe metastatic potential of these lateral tumoursrequire rapid surgical treatment confusion betweenhibernoma and liposarcoma is increased since bothshow onset in the third or fourth decade with apredominance in women (58% of the cases).8,9
References
1. Furlong MA, Fanburg-Smith JC, Miettinen M. The morphologicspectrum of hibernoma: a clinicopathologic study of 170cases. Am J Surg Pathol 2001;25(6):809–14.
2. Chen DY, Wang CM, Chan HL. Hibernoma: case report andliterature review. Dermatol Surg 1998;24(3):393–5.
3. Kunin N, Henno S, Verhoye J-P, Moreau L, Mambrini A.Hibernome de la region axillaire. J Chir 1997;134(3):119–21.
4. Mugel T, Ghossain MA, Guinet C, Buy J, Bethoux J, Texier P,et al. MR and CT findings in a case of hibernoma of the thighextending into the pelvis. Eur Radiol 1998;8(3):476–8.
5. Lewandowski PJ, Weiner SD. Hibernoma of the medial thigh.Clin Orthop 1996;330:198–201.
6. Seynaeve P, Montelmans L, Kockx M, Van Hoye M, Mathijs R.Case report 813: hibernoma of the left thigh. Skeletal Radiol1994;23(2):137–9.
7. Deseran MW, Seeger LL, Doberneck SA, Ecckardt JJ. Hiber-noma of the right gracilis muscles. Skeletal Radiol 1994;23(4):301–2.
8. Atilla S, Eilenberg SS, Brown JJ. Hibernoma: MRI apparance ofrare tumor. Magn Reson Imaging 1995;13(2):335–7.
9. Alvine G, Rosenthal H, Murphey M, Huntrakoon M. Hibernoma.Skeletal Radiol 1996;25(5):493–6.