Embed Size (px)
Citation preview

6.34 Thrombolytics
A E El-Gengaihy, S I Abdelhadi, J F Kirmani, and A I Qureshi, University of Medicine andDentistry of New Jersey, Newark, NJ, USA
& 2007 Published by Elsevier Ltd.
6.34.1 Introduction
7636.34.2 Pathophysiology of Thrombus Formation
7646.34.2.1 Factors Affecting Thrombus Formation
7656.34.2.2 Mechanism of Thrombolysis
7656.34.3 Animal Models and Preclinical Studies
7666.34.4 Current Thrombolytics
7676.34.4.1 Thrombolytic Agents used in Trials and Clinical Practice
767 6.34.4.1.1 First-generation thrombolytic agents 767 6.34.4.1.2 Second-generation thrombolytic agents 769 6.34.4.1.3 Third-generation thrombolytic agents 770 6.34.4.1.4 Fourth-generation thrombolytic agents 7716.34.5 Major Cardiovascular Clinical Trials
7726.34.5.1 Streptokinase
7726.34.5.2 Alteplase
7726.34.5.3 Reteplase
7736.34.5.4 Tenecteplase (TNK-t-PA)
7736.34.5.5 Lanoteplase (nPA)
7746.34.5.6 Saruplase
7746.34.6 Medical Management with Thrombolysis
7746.34.7 New Approaches and Adjuvant Therapy
7756.34.7.1 Aspirin
7756.34.7.2 Dipyridamole
7756.34.7.3 Warfarin, Heparin, and Low-Molecular-Weight Heparins
7756.34.7.4 Glycoprotein IIb/IIIa Receptor Antagonists
7756.34.7.5 P2Y12 Antagonists
7776.34.8 Future Directions
777References
7776.34.1 Introduction
Thrombus formation is a vital part of the hemostatic mechanism. Under normal circumstances formation of the
thrombus is limited to the site of vessel injury and is regulated by different mechanisms to prevent further progression.
Under pathological conditions, a thrombus can propagate into otherwise normal vessels, where it can lead to
obstruction of blood flow and impair normal hemodynamic functions. Heart disease, ischemic stroke, pulmonary
embolism, peripheral vascular disease, and many others all share a common pathophysiological process of thrombus
formation.1 The applications and use of thrombolytic therapy with reperfusion of occluded vessels has a major impact
on the outcome of the above diseases. Thrombolysis is a standard treatment option for acute ST-segment elevation
myocardial infarction (STEMI), stroke, pulmonary embolism, and other thromboembolic diseases. In this chapter the
mechanisms of thrombus formation are reviewed; the various types, mechanism of action, and the use of different
thrombolytic agents as well as major cardiovascular clinical trials are highlighted.
763

764 Thrombolytics
6.34.2 Pathophysiology of Thrombus Formation
Thrombosis is a pathologic event that results in the obstruction of coronary, cerebral, or peripheral blood flow.2 A
thrombus is formed by the two major components of the coagulation system: platelets and coagulation factors.
Normally, the endothelial cell lining of the vessels maintain an antithrombotic status by several mechanisms that
prevent platelet adhesion to the vessel wall, including: maintaining a transmural negative electrical charge; releasing
prostacyclin (PGI2), which prevents platelet aggregation; and activating the fibrinolytic pathway and protein C, which
degrades the coagulation factors.3
In case of vascular injury, platelets and plasma clotting factors become exposed to the subendothelial collagen and
the endothelial basement membrane, which releases adenosine diphosphate (ADP), a potent platelet aggregator, and
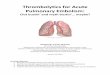
tissue factor, which launches the clotting cascade (Figures 1 and 2). Platelets adhere to the vessel wall and undergo
conformational changes, which enhances more platelet aggregation. Moreover, glycoprotein (GP) IIb/IIIa receptors are
upregulated and subsequently fibrinogen and von Willebrand’s factor bind to activated platelets via GP IIb/IIIa
receptors forming the platelet plug.4
Activated platelets acquire an enhanced capacity to catalyze the interaction between activated coagulation factors.
These factors are generally circulating in the blood in an inactive form (zymogens). The clotting cascade consists of two
separate initial pathways (intrinsic and extrinsic) that converge into a final common pathway, which ends by activation
of factor X to Xa and conversion of fibrinogen to fibrin (Figure 2). The extrinsic pathway is important for the initiation
of fibrin formation while the intrinsic pathway is involved in fibrin growth and maintenance.4
The extrinsic pathway is triggered by tissue factor, also called thromboplastin (a lipid-rich protein material released
after vascular injury). Thromboplastin combines with activated factor VIIa to convert factor IX to activated factor IXa in
the intrinsic pathway and factor X to activated factor Xa in the extrinsic pathway. Factor VII is activated by IXa or XIIa
of the contact system. This process takes 15 s.
The intrinsic pathway is initiated by activation of factor XII by the high-molecular-weight kininogen (the precursor
of vasoactive peptide, bradykinin) and kallikrein in the presence of collagen. Factor XIIa converts factor XI to XIa,
which in turn activates factor IX to factor IXa, and subsequently factor X to Xa. Activated factor Xa then binds with
factor Va, Ca2þ , and phospholipids (PLs) from the platelet membrane to form Xa–Va–PL complex (prothrombinase),
which converts prothrombin to thrombin. Thrombin finally cleaves fibrinogen to release isolated fibrin monomers,
which polymerize with each other to form complex fibrin. Factor XIII, which is also activated by thrombin, stabilizes
fibrin complexes and hence thrombus formation.
There is tight control over the coagulation system; once factor Xa is formed, it binds to tissue factor pathway
inhibitor (TFPI), which inhibits further activation of factor Xa and factor Va. Other control mechanisms include
Tissue injury
Exposure of subendothelial collagen
ADP Release of tissue factor
Platelet aggregation
Activation of factor XII
Activation of extrinsic pathway Activation of intrinsic pathway
Common pathwayPL
Figure 1 Triggering of coagulation cascade

VII
VIIa
TF+VIIa
XIIa
XIXIa
IXXIa
X Xa
Xa+Va+Ca+PL(prothrombinase)
Prothrombin thrombin
Fibrinogen
Fibrin monomers
XIIa
Fibrin polymer
Intrinsic pathway
Extrinsic pathway
Common pathway
Figure 2 Diagram showing the coagulation cascade. PL, phospholipids.
Thrombolytics 765
activation of the fibrinolytic pathway and the presence of antithrombin III, which prevents clotting factor activation,
protein C, which inactivates factor Va, and protein S, which acts as a cofactor for protein C where they form a complex
to inactivate factor VIIIa.3
6.34.2.1 Factors Affecting Thrombus Formation
According to Virchow’s triad,5 there are three possible contributors to the formation of an abnormal clot (thrombus):
vessel wall injury or inflammation, changes in the intrinsic properties of blood, and decrease in blood flow velocity
(Figure 1).5–9 Atherosclerotic plaques, which are found in most major arteries, are the main substrate for thrombus
formation.10 The atherosclerotic process can start even before birth11 with approximately 65% of children between 12
and 14 years of age having intimal alteration.12–14 The lipid core of the atherosclerotic lesion is rich in tissue factor,
which initiates the clotting cascade upon plaque rupture.15 Other factors that affect thrombus formation include the
degree of plaque disruption and the content of tissue factor in the plaque.16 Stenotic arteries and blood velocity also
affect the platelet disposition and thrombus formation as they change the shear rate of flowing blood.17 Certain
systemic risk factors are also associated with thrombus formation, for example, lipoprotein(a) has a similar structure to
plasminogen, which may impair thrombolysis.18 Increased blood thrombogenicity is also associated with increased low-
density lipoprotein (LDL).19 Poorly controlled diabetes mellitus results in glycosylation of collagen and protein,
increasing the levels of plasma fibrinogen. Furthermore, smoking has been found to increase tissue factor levels in
thrombotic plaques.10
6.34.2.2 Mechanism of Thrombolysis
Under normal circumstances there is no plasminogen activation occurring in plasma, the action of the fibrinolytic
system is confined to fibrin. When fibrin is formed, a small amount of plasminogen activator and plasminogen adsorb to
it and plasmin is created in situ to catalyze the degradation of fibrin (Figure 3).20 Naturally occurring plasminogen

Plasminogen Plasmin
t-PAScu-PA
PAI-1
+
Fibrin clot
SolubleD-dimers
− α2-antiplasmin
Binds with
Inert complex
Figure 3 Schematic diagram showing the process of fibrinolysis and its control. D-dimers, breakdown product of fibrin.
766 Thrombolytics
activators are either tissue-type plasminogen activator (t-PA) or single chain urokinase-type plasminogen activator
(scu-PA), both of which are synthesized by the endothelial wall.
The fibrinolytic system is tightly controlled and is normally restricted in the thrombus (Figure 3). Endothelial cells
secrete plasminogen activator inhibitor-1 (PAI-1), which inactivates t-PA in the plasma but not that in the thrombus; in
addition, the plasma t-PA has a short half-life (5–8 min). Also, a2-antiplasmin, a physiological bound serine protease
inhibitor, forms an inert complex with the circulating plasmin but does not act on fibrin-bound plasmin in the
thrombus.4 Any disturbance in this system can cause either excessive thrombus formation, if there is insufficient
activation of the thrombolytic system or if there are excessive inhibitors,21 or bleeding tendency, if there is
overstimulation of the thrombolytic system and deficiency in the release of inhibitors.20
6.34.3 Animal Models and Preclinical Studies
The novel antithrombotic agents were discovered, validated, and characterized through animal studies. Animal models
provide a great deal of information regarding the mechanism, doses, and treatment options, as well as interaction among
different thrombolytic agents. As there are many animal models only a few selected ones are discussed here.
Infused intravenous (i.v.)/intracoronary t-PA in the left anterior descending (LAD) coronary artery in an animal
model induced a thrombus within 1–2 h. Coronary reperfusion, intermediary metabolism, and nutritional myocardial
blood flow were restored within 10 min without inducing a systemic fibrinolytic state.22 Another study compared the
thrombolytic effect of recombinant t-PA (rt-PA) with that of urokinase in dogs undergoing coronary occlusion for 1 h.
Both agents were infused at the same rate. rt-PA elicited a faster reperfusion with less distal coronary embolization and
systemic fibrinolysis as compared to urokinase.23
Dose and rate of infusion of rt-PA directly correlate to the degree of reperfusion of the coronary vessels. This was
shown in open-chested, anesthetized dogs with induced thrombus in the LAD. Two hours after induction of the
thrombus rt-PA was infused intravenously at different rates and doses. Lower rates of infusion and lower doses took
longer to achieve coronary reperfusion when compared with higher doses, e.g., at 5 mg kg� 1 min� 1 time-to-reperfusion
was greater than 40 min, while at 25 mg kg� 1 min� 1 lysis occurred within 13 min. Epicardial electrographic
measurements showed a significant reduction in ST elevation in all reperfused hearts.24
Another important factor is the time of administration of the thrombolytic agent. Administration of rt-PA after
30–80 min in open-chested baboons showed a mean duration of reperfusion at 77 min and a decrease in infarct size by
38%. However, myocardial blood flow in the perfusion area of the LAD was only 70% of normal after 4 h in spite of
perfect angiographic refilling.25 From the above mentioned studies, it is concluded that t-PA i.v. may recanalize
thrombosed coronary vessels without inducing a systemic fibrinolytic state. Timely reperfusion results in infarct sparing
and restoration of nutritional blood flow.
Another comparative study was done using a canine model of coronary thrombosis; the aim of the study was to
compare tissue plasminogen activator and urokinase. Urokinase was given in two doses, 15 000 (UK15) and
30 000 U kg� 1 (UK30), and rt-PA was given in two doses, 0.25 (rtPA.25) and 0.75 mg kg� 1 (rtPA.75). rtPA.75 showed a
higher rate and extent of coronary thrombolysis; rtPA.25 was superior to UK15 but achieved the same results as UK30.
Again, this study indicates that rt-PA is superior to urokinase.26

Thrombolytics 767
Platelet-rich coronary clot is resistant to thrombolytic therapy In order to investigate and overcome such a problem,
investigators developed an animal model (dog) with platelet-rich coronary clot and investigated the effect of
thrombolytic therapy combined with antiplatelet GP IIb/IIIa antibody. The use of a reduced dose thrombolytic therapy
with antiplatelet GP IIa/IIIa can overcome the resistant clot and restore perfusion. This study concluded that platelet-
rich clot can be treated pharmacologically without the need for mechanical thrombolysis.27
A canine model of combined coronary arterial and femoral venous thrombosis was induced to compare intravenous
bolus injection versus infusion of recombinant unglycosylated full-length single chain urokinase-type plasminogen
activator (rscu-PA, saruplase). Coronary artery thrombosis and femoral vein clots were produced in five randomized
blinded groups, each consisting of five dogs. rscu-PA was infused over 60 min at 1 mg kg� 1 and 0.5 mg kg� 1 (group I
and III, respectively), and was given as a bolus at 1 mg kg� 1 and 0.5 mg kg� 1 (group II and IV, respectively). Group V
was the control group. Four out of five dogs showed coronary recanalization in groups I and IV, group I showed the
highest percentage of clot lysis, while both groups I and II showed no coronary reocclusion Globally, this study proved
that in both coronary and venous thrombolysis, intravenous bolus injection of rscu-PA is equipotent to an infusion
over 60 min.28
Recent animal studies are now targeting inhibitors of PAI-1 or PAI-039. As noted above, PAI-1 functions to suppress
t-PA and urokinase-type plasminogen activator (u-PA), so its inhibition should help in thrombolysis. Dogs were given
PAI-039 orally and then subjected to coronary occlusion. Dogs treated with PAI-039 had more time for coronary
reocclusion and thrombus weight was reduced compared to controls. Also the incidence of spontaneous reperfusion of
the coronary artery was greater in dogs that received PAI-039 as compared to controls. Accordingly PAI-1 may be used as
adjunctive therapy to lower the dose of thrombolytics and to increase their efficiency in clot lysis with fewer side
effects such as cerebral hemorrhage and bleeding.29
6.34.4 Current Thrombolytics
Streptokinase entered clinical use in the mid-1940s.30 The first use of a fibrinolytic drug in the treatment of acute
myocardial infarction was reported in 1958, when intravenous infusion of streptokinase was used.31 Shortly after that, in
1960, streptokinase and human plasmid were injected into the aortic root of a man following myocardial infarction.32
However, the revolution of thrombolytic therapy started in 1976 in Russia, with direct intracoronary injection of
fibrinolysin.33 Several trials followed and it was soon recognized that early restoration of the blood flow preserved left
ventricular function and yielded significant mortality benefit. However, the use of intracoronary therapy was limited,
because it was time consuming and needed specially equipped hospitals and well-trained personnel.
t-PA and high-dose intravenous streptokinase became established as a life-saving treatment for acute myocardial
infarction (MI),34 and were approved for use by the US Food and Drug Administration (FDA) in the mid-1980s.35 Trials
to establish the efficacy of streptokinase for acute ischemic stroke were stopped because of a high rate of early death
due to intracerebral hemorrhage. In 1996, the FDA approved intravenous thrombolysis with rt-PA as the ‘first-ever’
effective treatment for ischemic stroke during the first 3 h of onset of symptoms.36 Reteplase was the first of the third-
generation thrombolytics to be approved for use in acute MI.35
6.34.4.1 Thrombolytic Agents used in Trials and Clinical Practice
Thrombolytic drugs lyze preexisting thrombus in both arteries and veins and re-establish tissue perfusion.4 They exert
their action through conversion of plasminogen to plasmin, which then degrades fibrin, a major structural component of
the thrombus.37 The action of thrombolytic drugs is achieved by either potentiating endogenous fibrinolytic pathways
or mimicking natural thrombolytic molecules.1 Currently available thrombolytic agents are derived from bacterial
products or manufactured using recombinant DNA technology. They differ in their efficiency, fibrin selectivity, and
side-effect profile. Even for the same thrombolytic agent, different doses, different administration regimens, and
concomitant use of adjunctive agents can modify its patency rates. However, these differences are only marginal.1 Many
limitations exist among the available generations of thrombolytic agents, raising the need for continued research for
better agents. The indications of fibrinolytic therapy are summarized in Table 1 and contraindications in Table 2.
6.34.4.1.1 First-generation thrombolytic agentsThere are three agents belonging to this group: streptokinase, urokinase, and anisoylated purified streptokinase activator
complex (APSAC). They are not fibrin specific or site specific, and they act anywhere in the blood, converting circulating
plasminogen to plasmin. Eventually, this causes depletion of body plasminogen, disturbing the equilibrium between
circulating plasminogen and plasminogen in the thrombus (plasminogen steal) and reducing clot lysis.

Table 2 Contraindications to fibrinolytic therapy (ACC guidelines)
Absolute contraindications
1. Any prior ICH
2. Known structural cerebral vascular lesion (e.g., AVM/aneurysm)
3. Known malignant intracranial neoplasm
4. Ischemic stroke within 3 months EXCEPT acute ischemic stroke within 3 h
5. Suspected aortic dissection
6. Active bleeding or bleeding diathesis (excluding menses)
7. Significant closed-headi or facial trauma within 3 months
Relative contraindications
1. History of chronic, severe, poorly controlled hypertension
2. Severe uncontrolled hypertension on presentation (SBP greater than 180 mmHg or DBP greater that 110 mmHg)
3. History of prior ischemic stroke greater than 3 months, dementia, or known intracranial pathology not covered in
contraindications
4. Traumatic or prolonged (greater than 10 min) CPR or major surgery (within the last 3 weeks)
5. Recent (within 2–4 weeks) internal bleeding
6. Noncompressible vascular punctures
7. For streptokinase/anistreplase: prior exposure (more than 5 days ago) or prior allergic reaction to these agents
8. Pregnancy
9. Active peptic ulcer disease
10. Current use of anticoagulants: the higher the INR, the higher the risk of bleeding
CPR, cardiopulmonary resuscitation; AVM, arteriovenous malformation; SBP, systolic blood pressure; DBP, diastolic blood
pressure; INR, international normalized ratio.
Table 1 Indications of fibrinolytic therapy (ACC guidelines)
Class I
1. In the absence of contraindications, fibrinolytic therapy should be administered to STEMI patients with symptom onset
within the prior 12 h and ST elevation greater than 0.1 mV in at least 2 contiguous precordial leads or at least 2 adjacent limb
leads (Level of Evidence: A)
2. In the absence of contraindications, fibrinolytic therapy should be administered to STEMI patients with symptom onset
within the prior 12 h and new or presumably new LBBB (Level of Evidence: A)
Class IIa
1. In the absence of contraindications, it is reasonable to administer fibrinolytic therapy to STEMI patients with symptom onset
within the prior 12 h and 12-lead ECG findings consistent with a true posterior MI (Level of Evidence: C)
2. In the absence of contraindications, it is reasonable to administer fibrinolytic therapy to patients with symptoms of STEMI
beginning within the prior 12–24 h who have continuing ischemic symptoms and ST elevation greater than 0.1 mV in at least 2
contiguous precordial leads or at least 2 adjacent limb leads (Level of Evidence: B)
Class III
1. Fibrinolytic therapy should not be administered to asymptomatic patients whose initial symptoms of STEMI began more than
24 h earlier (Level of Evidence: C)
2. Fibrinolytic therapy should not be administered to patients whose 12-lead ECG shows only ST-segment depression except if a
true posterior MI is suspected (Level of Evidence: A)
768 Thrombolytics
6.34.4.1.1.1 Streptokinase
Streptokinase is approved for use in myocardial infarction, pulmonary embolism, deep venous thrombosis,
arteriovenous-cannula occlusions, and peripheral arterial occlusions.30 Streptokinase is an enzyme with a molecular
weight of 47 000 Da35 derived from the culture filtrate of Lancefield group C5 b-hemolytic streptococci.1,35
Streptokinase lyses thrombus by potentiating the body’s own fibrinolytic pathways.1 It acts indirectly2,37 through

Thrombolytics 769
binding with free circulating plasminogen to form a 1:1 complex, resulting in a conformational change and exposure of
an active site that can convert additional plasminogen into plasmin, the main thrombolytic enzyme in the body.4 The
resultant plasmin is of two types: fibrin-bound and unbound. Fibrin-bound plasmin causes direct fibrinolysis of
the thrombus,2 while unbound circulating plasmin leads to systemic fibrinolysis and a hypocoagulable state due to the
depletion of fibrinogen, plasminogen, and factors V and VIII.1,35,37 In addition, streptokinase increases levels of
activated protein C, which enhances clot lysis.35 The greatest benefit of streptokinase appears to be achieved by early
i.v. administration.4
Streptokinase has no metabolites. The complex is inactivated, in part, by antistreptococcal antibodies, resulting
from prior infection,38 and eliminated through the liver.35 It has two half-lives: a fast one (11–13 min) due to inhibition
by the circulating antibodies; and a slow one (23–29 min) due to loss of the enzyme activity.4 The unbound fraction,
which constitutes about 15%, has a serum half-life of 80 min.30 On the other hand, fibrin degradation products can be
detected in the serum for up to 24 h, which means that the patient remains somewhat ‘anticoagulated’ even without
the use of heparin.35,37
6.34.4.1.1.2 Urokinase
Urokinase is the most familiar thrombolytic agent among interventional radiologists and it is often used for peripheral
vascular thrombosis.37 It is approved for pulmonary embolism and for lysis of coronary thrombi, but not for mortality
reduction in acute myocardial infarction.4,35
Urokinase is a trypsin-like1 enzyme that is produced endogenously by renal parenchymal cells30 and found in urine.
Approximately 1500 L of urine are needed to yield enough urokinase to treat a single patient.30 There are two forms of
urokinase, which differ in molecular weight but have similar clinical effect.39 Commercially available urokinase, the
low-molecular-weight form (32 400 Da), is produced from cultured human neonatal kidney cells. It is a two-polypeptide
chain serine protease, containing 411 amino acid residues4,35: an A chain of 2000 Da is linked by a sulfhydryl bond to a B
chain of 30 400 Da. Recombinant techniques are used to produce urokinase in Escherichia coli.30 Unlike streptokinase,
urokinase directly cleaves plasminogen to produce plasmin.1 Although this process is slightly increased in the presence
of fibrin, urokinase produces circulating unbound plasmin, which means that it not only degrades fibrin clots but also
fibrinogen and other plasma proteins leading to systemic fibrinolysis.40
In plasma, urokinase has a half-life of approximately 15 min30 (7–20 min).4,38 It is rapidly metabolized and cleared by
the liver38 with small fractions being excreted in bile and urine. Plasma levels can be elevated two- to fourfold1 and
clearance is reduced in patients with hepatic impairment. Moreover, due to its short half-life, re-thrombosis may occur
within 15–30 min of therapy cessation. Heparin is commonly used during and after urokinase adminstration to
minimize this risk.40
6.34.4.1.1.3 Anisoylated purified streptokinase activator complex (APSAC, anistreplase)
APSAC was the third thrombolytic agent to be developed. It has a molecular weight of 131 000 Da35 and consists of
streptokinase in a noncovalent 1:1 complex with plasminogen.4 It does not require free circulating plasminogen to be
effective. APSAC is catalytically inert because of the acylation of the catalytic site of plasminogen (having the catalytic
site temporarily blocked by a p-anisoyl group), which protects the catalytic center of the complex from premature
neutralization.35 However, the affinity of plasminogen binding to fibrin is maintained.4 APSAC acts as an indirect
plasminogen activator35 and is nonfibrin selective, and so activates both circulating and clot-bound plasminogen, but is
most active within the thrombus.2
Inside the circulation, anistreplase undergoes spontaneous deacylation to form the active complex of plasminogen–
streptokinase. This conversion occurs with a half-life of 90–100 min,2,37 which lengthens its thrombolytic effect after
i.v. injection.4 The active complex is metabolized in the liver35 and has the longest half-life among all thrombolytic
agents, ranging from 90 min4 to 100 min.35
6.34.4.1.2 Second-generation thrombolytic agentsThese agents include t-PA and scu-PA (prourokinase). The second-generation agents are more fibrin selective and
although they were developed to avoid systemic thrombolytic state, they can still cause a mild to moderate decrease in
the levels of circulating fibrinogen and plasminogen.35
6.34.4.1.2.1 Tissue-type plasminogen activator (alteplase)
Alteplase was the first recombinant t-PA to be produced. It is the most familiar fibrinolytic agent in emergency
departments and the most often used agent for treatment of coronary artery thrombosis, pulmonary embolism, and

770 Thrombolytics
acute stroke.30 Alteplase is expensive, costing approximately 8–10 times more than streptokinase per dose.35,37 In vivo,
t-PA is synthesized by the vascular endothelial cells and is considered the physiologic thrombolytic agent that is
responsible for most of the body’s natural efforts to prevent thrombus propagation. Based on the results of Stroke Trials
sponsored by the National Institute of Neurological Disorders and Stroke (NINDS), intravenous thrombolysis with
rt-PA was approved as the ‘first-ever’ effective treatment for ischemic stroke during the first 3 h of symptom onset.36
rt-PA is a sterile purified glycoprotein molecule consisting of 527 amino acids35 that is structurally identical to
endogenous t-PA.1,41 It has a molecular weight of 70 000 Da35 and is produced by recombinant technology1,4,35 from a
human melanoma cell line.35 The molecule contains five domains: finger, epidermal growth factor, kringle 1, kringle 2,
and serum protease.2 There are two different forms of t-PA based on the number of chains: t-PA (the two-chain form
duteplase and alteplase by recombinant technology) and rt-PA (one chain form).2,35 It consists predominantly of the
single-chain form (rt-PA), but upon exposure to fibrin, rt-PA is converted to the two-chain dimer.4
t-PA is a naturally occurring enzyme (serine protease).42 It is the principal physiological activator of plasminogen in
the blood and has a high binding affinity for fibrin4 at the site of a thrombus, directly2,35,37 activating clot-bound
plasminogen only.42 While this might seem an advantage, this selectivity is not absolute; circulating plasminogen may
also be activated by large thrombolytic doses or lengthy treatment.4 Moreover, its action is fibrin-enhanced; that is, in
the absence of fibrin, t-PA is a weak plasminogen activator.42 It is rapidly cleared from plasma with an initial half-life
of approximately 5 min (4–10 min)5,35; however, its effect at the clot persists for over an hour35 (72 min), but
the concentration of circulating t-PA would be expected to return to endogenous circulating levels of 510 ng mL� 1
within 30 min.42 Having a short plasma half-life necessitates its administration as a bolus injection, followed by a
short continuous infusion.2 Heparin is usually coadministered to avoid reocclusion.2,35 The plasma clearance is
380–570 mL min� 1,35 and is primarily mediated by the liver.2,35,43
t-PA is not associated with hypotension35 and is not antigenic; it can be readministered as necessary1 and may be
considered for use in patients who have high antibody titer against streptokinase.35 The activity of t-PA is enhanced in
the presence of fibrin, resulting in thrombus-specific fibrinolysis.1 In practice, however, t-PA causes a milder form of
systemic fibrinogenolysis4,35 than streptokinase at equi-effective doses, but the incidence of bleeding is similar with
both agents.4 Moreover, t-PA is considered more efficacious than streptokinase in establishing coronary reperfusion4
and has a slight mortality advantage over streptokinase due to its accelerated administration because of the shorter half-
life. Unfortunately, this occurs at the cost of a marginal increase in stroke rate.1
The risk of intracranial hemorrhage is higher with t-PA than streptokinase (0.7% versus 0.5%).35 Having a shorter
plasma half-life, the rate of re-thrombosis after t-PA is greater than streptokinase,4 which raises the need for continuous
infusion in order to achieve its greatest efficacy,1 and since t-PA is more expensive and toxic than streptokinase, the
latter is the agent of choice for coronary thrombolysis.35
6.34.4.1.2.2 SPB (scu-PA, prourokinase)
Prourokinase is a new fibrinolytic agent that is currently undergoing clinical trials for a variety of indications. It is a
single chain urokinase35 and has been produced both in glycosylated (ABT-74187) and nonglycosylated (saruplase)
forms.2,35 It is a relatively inactive precursor that must be converted to urokinase before it becomes active in vivo.
However, it displays selectivity for clots by binding to fibrin before activation.37 The mechanism of action of the
nonglycosylated form is unclear, but it is known to be nonfibrin specific.35 Its advantage over other plasminogen
activators is that it is inactive in plasma and so does not consume circulating inhibitors. Also, it is somehow clot specific,
where it needs fibrin to be converted by an unknown mechanism into active urokinase.30 It is usually administered as a
bolus followed by intravenous infusion, but single-bolus regimens are now being developed.35
6.34.4.1.3 Third-generation thrombolytic agentsThese groups of agents have been developed through modifications of the basic t-PA structure. They are either:
conjugates of plasminogen activators with monoclonal antibodies against fibrin, platelets, or thrombomodulin; mutants,
variants, and hybrids of t-PA and prourokinase (amediplase); or new molecules of animal (vampire bat) or bacterial
(Staphylococcus aureus) origin.35 These molecular variations have yielded agents with better pharmacological properties
than t-PA, a longer half-life, resistance to plasma protease inhibitors, and more selective fibrin binding.4,35 Several of
these agents are being developed including reteplase (r-PA, retevase), lanoteplase (nPA), tenecteplase (TNKase),
pamiteplase (YM866; Solinase), staphylokinase, and novel modified tissue plasminogen activator (E6010).
6.34.4.1.3.1 Reteplase (rt-PA, r-PA, retevase)
Reteplase is the first third-generation thrombolytic agent to be approved for use in acute MI to improve postinfarct
ventricular function, lessen the incidence of congestive heart failure, and reduce mortality.35 It is a synthetic

Thrombolytics 771
nonglycosylated deletion mutein of t-PA containing 355 of the 527 amino acids of the native tissue plasminogen
activator; it lacks the finger, epidermal growth factor, and kringle 1 domains2,44 as well as carbohydrate side chains.2
This results in a prolonged half-life and less fibrin specificity than t-PA.37,44 It has a molecular weight of 39 500 Da and
is produced in E. coli by recombinant DNA technology.1 The gene for a fragment of t-PA is inserted into E. coli, and the
protein is then extracted from the bacteria and processed to convert it into an active thrombolytic.30,37
Patients receiving reteplase have faster clot resolution than those receiving t-PA, owing to the fact that reteplase
binds less tightly to fibrin, allowing for more free diffusion through the clot rather than only binding to the surface as
t-PA does. In a controlled trial, 64% of patients who received a double bolus of reteplase showed a decrease in
fibrinogen levels to below 100 mg dL� 1 within 2 h. However, the mean fibrinogen levels returned to baseline within
48 h.45 Moreover, at high concentrations, it does not compete with plasminogen for fibrin-binding sites, allowing
plasminogen at the site of the clot to be transformed into clot-dissolving plasmin.30
The above-mentioned structural modifications result in a fivefold decrease in fibrin binding and an extended half-
life (11–19 min).35,37,44 The longer half-life allows for administration of reteplase by double-bolus infusion rather than a
prolonged infusion.35,37,44 It undergoes renal (and some hepatic) clearance30 at a rate of 250–450 mL min� 1.
6.34.4.1.3.2 Lanoteplase (nPA, novel plasminogen activator)
Lanoteplase is a deletion mutant of t-PA lacking the finger, epidermal growth factor, and one amino acid substitution in
the kringle 1 domain, leading to deletion of a glycosylation site.2,35
6.34.4.1.3.3 Tenecteplase (TNK-t-PA, TNKase)
Tenecteplase is a tissue plasminogen activator with a molecular weight of 70 000 Da,35 produced by genetic
engineering.37 To create tenecteplase, a 527 amino acid glycoprotein molecule, the human gene for t-PA was modified
using 3 amino acid substitutions:37 a substitution of threonine 103 with asparagine and asparagine 117 with glutamine
within the kringle 1 domain, and a tetra-alanine substitution at amino acids 296–299 in the protease domain.2,35 These
mutations resulted in a decrease of plasma clearance, prolonged half-life, higher degree of fibrin specificity, and
increased resistance to PAI-1 as compared to t-PA.2,35,37,46 The FDA has approved the use of tenecteplase in acute MI.37
Tenecteplase is a modified form of human t-PA that binds more avidly to fibrin,4 and directly converts plasminogen
to plasmin.35 This process relatively increases in the presence of fibrin, giving tenecteplase the advantage of being
more specific with minimal systemic effect. However, this specificity is not absolute; a 4–15% decrease in circulating
fibrinogen and 11–24% decrease in plasminogen has been reported following administration. Moreover, its clinical
significance with regard to safety or efficacy has not been established.
A single bolus of tenecteplase administered to patients with acute myocardial infarction exhibits biphasic
disposition from the plasma. The initial half-life is 20 min (15–24 min),35 about four times that of t-PA,4 and is
considered to be the longest elimination half-life among t-PA derivatives.4,35,37 The terminal phase half-life of
tenecteplase is 90–130 min. The initial volume of distribution is weight related and approximates plasma volume. The
main route of elimination is liver, at a clearance rate of 99–119 mL min� 1.37
6.34.4.1.3.4 Staphylokinase
Staphylokinase was known to possess profibrinolytic properties more than four decades ago.35 It is produced by certain
strains of S. aureus. It acts on the surface of the clot to form a plasmin–staphylokinase complex,2 which has high fibrin
specificity, only activating plasminogen trapped in the thrombus.35 After administration, staphylokinase-related antigen
disappears from plasma in a biphasic manner, with an initial half-life of 6.3 min and a terminal half-life of 37 min.35
As compared to t-PA, studies suggest that staphylokinase may have less procoagulant effects. Furthermore, it is
highly antigenic; patients develop neutralizing antibodies in about 1–2 weeks and the titer remains elevated for several
months after therapy cessation.35 This limits the use of a second dose until safer, more effective new variants that have
less immunogenicity are developed.2
6.34.4.1.4 Fourth-generation thrombolytic agents6.34.4.1.4.1 Recombinant desmodus salivary plasminogen activator-1 (r DSPA-1, desmoteplase)
A naturally occurring enzyme in the saliva of the blood-feeding vampire bat (Desmodus rotundus) is genetically related to
t-PA.47 It consists of four different proteases � D. rotundus salivary plasminogen activators (DSPAs). DSPA-1 is the full-
length variant with a greater than 72% sequence homology to human t-PA.48 Unlike t-PA, it exists as single-chain
molecules48 and it is critically dependent on fibrin.47,49,50 DSPA-1 targets and destroys fibrin;47 it is more fibrin

772 Thrombolytics
dependent and fibrin specific than t-PA.47 Its catalytic efficiency is enhanced 13 000-fold47 in the presence of fibrin,
while that of t-PA increases only by 72-fold.49
It has high fibrin specificity and selectivity, and a longer half-life compared to other thrombolytic agents.48,51
Compared to t-PA, it is non-neurotoxic, causes less fibrinogenolysis,50 less antiplasmin consumption, and results in
faster and more sustained reperfusion as demonstrated by animal studies.52 Furthermore, it can be given to acute
ischemic stroke patients within 3–9 h of onset of symptoms.51 DSPA is safe and results in improved perfusion and low
mortality rates without associated symptomatic intracerebral hemorrhage.51
6.34.5 Major Cardiovascular Clinical Trials
Numerous clinical trials with thrombolytic therapy have been performed to determine their clinical efficacy in
cardiovascular settings, namely acute myocardial infarction. Only trials of major significance for each thrombolytic agent
will be discussed in this chapter.
6.34.5.1 Streptokinase
The first large-scale thrombolytic trial was the GISSI-1 (Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto
Miocardico), which evaluated the efficacy of a thrombolytic treatment with streptokinase on in-hospital mortality of
patients with acute myocardial infarction (AMI). The GISSI demonstrated that overall in-hospital mortality was
reduced in those who received streptokinase (10.7%) compared to controls (13%). The degree of benefit, which was
sustained up to 1 year after the AMI episode, was related to the time between onset of symptoms and streptokinase
treatment; the sooner thrombolytics were administered the greater the reduction in mortality. When thrombolytics
were administered more than 6 h after AMI no difference was appreciated.53
Similar benefits were noted in the ISIS-2 trial (Second International Study of Infarct Survival), in which patients
presenting to hospitals within 24 h (mean of 5 h) of onset of suspected AMI were randomly assigned to either: (1) 1 h
i.v. infusion of streptokinase; (2) 1 month of 160 mg day� 1 of enteric coated aspirin (with the first tablet crushed for a
rapid antiplatelet effect); (3) both treatments; or (4) neither treatment Streptokinase alone and aspirin alone each
produced a significant reduction in 5-week vascular mortality. A combination of streptokinase and aspirin was
significantly better than either agent alone and displayed a synergistic effect in the reduction of mortality from 13.2%
(placebo) to 8.0% (streptokinaseþ aspirin).54 As in the GISSI trial, the ISIS-2 demonstrated that early therapy (within
6–24 h) is essential if mortality benefit and long-term benefit is to be achieved.55
6.34.5.2 Alteplase
Two initial trials, the GISSI-2 and ISIS-3 (Third International Study of Infarct Survival), compared the efficacy of
altepase with that of streptokinase. In the GISSI-2 and its International Study Group extension no significant difference
emerged regarding mortality in acute myocardial infarction between alteplase and streptokinase (9.6% versus 9.2%) and
whether heparin was or was not administered (9.3% versus 9.4%). Also, no significant differences were observed
regarding major cardiac complications. However, a small, albeit significant, increase in the incidence of stroke was found
among patients treated with alteplase compared to those treated with streptokinase (1.3% versus 0.9%).56,57 Long-term
follow-up also showed no significant differences between these two thrombolytics in these main clinical findings.58
The ISIS-3 trial, another randomized trial, compared streptokinase and t-PA, but also included APSAC. In this
study, there were no appreciable differences in mortality rates among thrombolytic agents. Moreover, rates for major
in-hospital clinical events, including cardiogenic shock, heart failure requiring treatment, ventricular fibrillation, and
cardiac rupture, were also similar. There was a small but significant deficit of in-hospital re-infarctions in the t-PA
group. Also of note were higher rates of allergy and hypotension requiring treatment in those that received the
bacterially derived proteins streptokinase and APSAC.
Altogether, these trials found no difference in efficacy between alteplase and streptokinase given with or without
subcutaneous heparin.56,59 Such data influenced the design of further studies, including GUSTO-1 (Global Utilization
of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries), which established accelerated
rt-PA combined with i.v. heparin as the optimal thrombolytic strategy for patients with AMI, and found that successful
reperfusion and myocardial salvage produced significant mortality benefits (1% absolute reduction in 30-day mortality)
in the alteplaseþ heparin group when compared to the streptokinaseþ heparin group. This benefit persisted at 1-year
follow-up.60 As with all thrombolytic therapy, bleeding and stroke are of greatest concern. Combinations of
streptokinase plus i.v. heparin and streptokinase plus t-PA were associated with a higher incidence of bleeding than the
use of single agents.

Thrombolytics 773
The Continuous Infusion Versus Double-Bolus Administration of Alteplase (COBALT) study tested therapeutic
equivalence between two alteplase dosing strategies in patients with acute myocardial infarction: a double bolus of
alteplase versus accelerated infusion. The trial was stopped on January 5, 1996 because of higher rates of death, stroke,
and cardiogenic shock in the double-bolus group than in the accelerated infusion group.61
A meta-analysis from the Fibrinolytic Therapy Trialists’ (FTT) collaborative group sought to determine the
indications and contraindications for fibrinolytic therapy and found a reduction in mortality in fibrinolytic-treated
patients (9.6%) compared to controls (11.5%). Mortality was reduced among patients presenting with ST segment
elevation (21%) or left bundle branch block (LBBB) (25%). Not surprisingly, absolute mortality reductions were
greatest in patients treated earlier after symptom onset,62 and FTT was beneficial in reducing mortality among various
types of patients (all ages except those greater than 75 years, patients with or without prior MI, and diabetic and
nondiabetic patients), but not in those without ST elevation or LBBB.62
6.34.5.3 Reteplase
The Recombinant Plasminogen Activator Angiographic Phase II International Dose-Finding Study (RAPID-1) was an
angiographic study that compared reteplase (r-PA) with alteplase (t-PA).45 Patients were randomized to: (1) t-Pa
100 mg i.v. over 3 h; (2) r-PA as a 15 MU single bolus; (3) r-PA as a 10 MU bolus followed by 5 MU 30 min later; or
(4) r-PA as a 10 MU bolus followed by another 10 MU 30 min later. Coronary angiography was then performed at 30, 60,
and 90 min after treatment and then again at discharge. Reteplase given as a double bolus (10þ 10 MU) achieved more
rapid, complete, and sustained thrombolysis of the infarct-related artery than standard dose t-PA, without an apparent
increased risk of complications.
The RAPID-II trial compared the double bolus of r-PA (10þ 10 MU) to a front-loaded regimen of alteplase (100 mg
over 90 min). Again, reteplase proved to be superior to alteplase in achieving recanalization of coronary artery, better
blood flow, and fewer acute (within 6 h) coronary interventions. However, there was no significant difference between
groups for 35-day mortality, bleeding requiring transfusion, or hemorrhagic stroke.63
In both RAPID trials, mortality and other outcomes were more favorable in those who received reteplase. These
hypotheses were further tested in the larger GUSTO-3 trial, which compared the efficacy and safety of alteplase and
reteplase.64 No difference was observed between the two thrombolytics regarding mortality at 30 days and incidence of
stroke. Also, no difference in mortality was appreciated between the two thrombolytics at 1 year (11.2% versus 11.1%).
This lack of significance, according to the GUSTO investigators, could reflect insufficient study size to detect such a
difference.64
Before being compared to alteplase, double-dose reteplase (10 MUþ 10 MU at 30 min) was compared to standard
dose streptokinase (1.5 MU over 1 ) in the INJECT (International Joint Efficacy Comparison of Thrombolyics) trial to
determine whether the effect of both thrombolytics on survival was equivalent.65 At 35 days, mortality, recurrent
myocardial infarction, in hospital stroke, and major bleeding events for the reteplase group and the streptokinase group
were equivalent. Reteplase, however, proved to have significant benefits compared to streptokinase, including fewer
cases of atrial fibrillation, asystole, heart failure, and hypotension. Therefore, the INJECT trial indicated that reteplase
was therapeutically comparable to streptokinase in terms of safety and efficacy.
In 2001, the GUSTO-5 trial compared reperfusion therapy for acute myocardial infarction with standard dose
reteplase versus half-dose reteplase (two boli of 5 U, 30 min apart) plus full-dose abciximab within the first 6 h of
STEMI. The investigators concluded that for patients with STEMI, the combined reteplase and abciximab was
noninferior (although not superior) to standard reteplase for decreasing the 30-day mortality.
6.34.5.4 Tenecteplase (TNK-t-PA)
Tenecteplase, a genetically engineered t-PA, was assessed for pharmokinetics, safety, and efficacy in humans in the
Thrombolysis in Myocardial Infarction 10A (TIMI 10A) trial.66 It was administered over 5–10 s as a single bolus of
5–50 mg and had a half-life of 17 min, nearly five times longer than t-PA.
Subsequently, the TIMI 10B trial, a phase II dosing trial,67 was carried out to identify a specific bolus dosing
regimen of TNK-t-PA that would achieve similar rates of TIMI-3 flow on 90-min angiography as t-PA, with a similar
safety profile. Patients were randomized after 12 h of symptom onset and given either a bolus dose of 30 or 50 mg of
TNK or a front-loaded regimen of t-PA. The 50 mg arm was changed to 40 mg due to a high incidence of intracranial
hemorrhage. The results showed 50 and 40 mg of TNK had a similar rate of TIMI-3 flow when compared to t-PA. No
differences in mortality and reinfarction were observed.

774 Thrombolytics
The Assessment of the Safety of a New Thrombolytic: TNK-t-PA (ASSENT-1) trial, a phase II dose-ranging trial,
was conducted in conjunction with the TIMI 10B trial to test the clinical safety of three doses of tenecteplase-tissue
plasminogen activator (TNK-t-PA) in ST-elevation myocardial infarction.68 Doses of 30, 40, and 50 mg of TNK-t-PA i.v.
bolus were selected. As discussed above, the 50 mg arm was discontinued. Overall, the safety profile of TNK-t-PA was
similar to that of alteplase and no difference in incidence of total stroke, intracranial hemorrhage, severe bleeding, or
death was observed among treatment groups.
Findings from the TIMI 10B and ASSENT-1 trials served as the basis for comparing TNK versus accelerated t-PA in
the ASSENT-2 trial. In the ASSENT-2 trial patients were randomized to weight-adjusted single doses of TNK-t-PA or
accelerated t-PA.69 No difference in mortality was noted at 30 days nor was there a difference in the rate of stroke and
intracerebral hemorrhage. Thus, TNK-t-PA was equivalent to t-PA in terms of its 30-day mortality benefit. Mortality at
1 year remained unchanged between the two agents.70 However, for those treated with TNK-t-PA 4 h after the onset of
symptoms, mortality at 30 days and 1 year was lower compared to t-PA.
In 2001, tenecteplase’s efficacy was assessed with a GP IIb/IIIa inhibitor in the ASSENT-3 trial, a randomized
trial that compared the efficacy and safety of tenecteplase plus enoxaparin or abciximab with that of tenecteplase plus
weight-adjusted unfractionated heparin (UFH) in patients with AMI.71 The tenecteplase plus enoxaparin or abciximab
regimens reduced the frequency of ischemic complications in AMI patients. The combination of tenecteplase with
enoxaparin was more efficacious than tenecteplase with heparin, and there was no increase in the risk of bleeding
or intracranial hemorrhage, even in patients over the age of 75. In contrast, while efficacy was improved with the
combination of tenecteplase plus abciximab, this was offset by a doubling in the rate of major hemorrhage and a higher
event rate in patients over the age of 75 and in diabetic patients. Therefore, it was concluded that tenecteplase plus
enoxaparin was a viable alternative regimen to tenecteplase plus UFH for the treatment of ST-elevation AMI.
6.34.5.5 Lanoteplase (nPA)
The Intravenous nPA for Treatment of Infarcting Myocardium Early (InTIME)-1 study compared a single bolus dose of
lanoteplase (15–120 kU kg� 1) with an accelerated regimen of alteplase in patients and found that coronary patency at
90 min (83% versus 71%) and frequency of TIMI grade III flow were greater with the highest doses of lanoteplase
compared to alteplase.71
The InTIME-1 study was followed by InTIME-2, which assessed mortality at 30 days in patients with acute
myocardial infarction randomized to either nPA or t-PA.72 The 30-day and 6-month mortality was similar between the
two groups. Intracranial hemorrhage was more frequent in those treated with nPA. Overall bleeding complications were
equal in the two treatment groups, however, mild complications occurred more frequently in nPA-treated individuals
(19.6% versus 14.7%).
6.34.5.6 Saruplase
Saruplase has been evaluated in several trials in patients with acute MI or unstable angina. The Comparison Trial of
Saruplase and Streptokinase (COMPASS), the largest of saruplase trials, attempted to demonstrate the equivalence of
saruplase to streptokinase in the treatment of patients with ST-segment elevation myocardial infarction (STEMI).
Patients were randomly assigned to receive heparin and saruplase (20 mg i.v. bolus followed by 60 mg i.v. over the next
60 min) or streptokinase without heparin. Saruplase was associated with a reduction in mortality compared to
streptokinase. Patients treated with saruplase were also less likely to develop hypotension, but more likely to develop
hemorrhagic stroke than those treated with streptokinase (0.9% versus 0.3%). The overall bleeding rates between the
two treatment groups were similar (10.4% versus 10.9%). These findings suggested that saruplase is as effective as
streptokinase in the treatment of acute STEMI, with a similar safety profile.73
6.34.6 Medical Management with Thrombolysis
Numerous studies have been performed and enough evidence accumulated showing an unequivocal benefit, in terms of
mortality and morbidity, in regards to thrombolytic treatment of patients presenting with AMI. As discussed above, the
FTT collaborative group found patients who presented within a ‘therapeutic window’ (less than 1 h) of symptom onset
and found to have either LBBB or STEMI benefited most from thrombolytic therapy, most benefit being seen in those
treated soonest after onset of symptoms. Patients presenting after 12 h should not receive fibrinolytics, unless there is
evidence of ongoing ischemia, as no significant benefit has been shown. Unless clearly contraindicated (see Table 2),

Thrombolytics 775
patients with infarction, particularly, STEMI (ST elevation greater than 0.1 mV in 2 contiguous leads) or new LBBB,
should receive prompt treatment with fibrinolytic therapy and aspirin without delay. Patients with LBBB or anterior ST
elevation are at greater inherent risk from MI and achieve greater benefit with fibrinolytic therapy. If possible,
fibrinolysis should be started within 90 min of the patient calling for medical treatment (‘call-to-needle’ time) or within
30 min of arrival at the hospital (‘door-to-needle’ time).74 As per the American College of Cardiology (ACC) guidelines,
attainment of additional ECG leads (right sided and/or posterior) or an echocardiogram may help clarify the location
and extent of infarction and anticipated risk of complications, but it is important that acquisition of such ancillary
information does not interfere with the strategy of providing timely reperfusion in patients with STEMI.
6.34.7 New Approaches and Adjuvant Therapy
6.34.7.1 Aspirin
Aspirin (Figure 4) is a nonselective cyclooxygenase inhibitor that has antithrombotic effects mediated by inhibition of
blood platelets. Inhibition of cyclooxygenase blocks production of thromboxane A2, which activates platelets leading to
aggregation, an early step in thrombosis. Aspirin is more effective in preventing arterial thrombosis (myocardial
infarction, stroke) than venous thrombosis (deep venous thrombosis, pulmonary embolism).
6.34.7.2 Dipyridamole
Dipyridamole (Figure 4) is an inhibitor of nucleoside transport (hENTs) acting to block platelet aggretion by increasing
adeonsine levels. Dipyridamole can also reduce plasma von Willebrand factor levels and serum C-reactive protein.75
6.34.7.3 Warfarin, Heparin, and Low-Molecular-Weight Heparins
Warfarin (Figure 4) inhibits vitamin K, which is essential for effective production of clotting factors II, VII, IX, X, and
anticoagulant proteins C and S. Heparin inhibits thrombin (factor IIa), and factors Xa and IXa. Heparin is used to treat
unstable angina and to prevent and treat venous thromboembolism. Low-molecular-weight heparins (LMWHs) are
fragments of the heparin molecule that inhibit clotting factor Xa more than factor IIa. Dalteparin, enoxaparin, and
tinzaparin are three such LMWHs.
6.34.7.4 Glycoprotein IIb/IIIa Receptor Antagonists
Activation of platelets by several agonists results in the expression of specific functional receptors for fibrinogen on the
platelet surface, referred to as GP IIb/IIIa receptors. The GP IIb/IIIa receptor is a member of the integrin family of
receptors.76 When platelets are activated by a variety of stimuli including thrombin, collagen, ADP, and epinephrine,
the GP IIb/IIIa receptor changes its conformation to be receptive to one end of a fibrinogen dimer. Occupancy of a GP
IIb/IIIa receptor by the other end of the dimer provides the basis for platelet aggregation. Thus, the GP IIb/IIIa
receptor is considered the final common pathway of platelet aggregation.77
Abciximab (c7E3) is a chimeric mouse� human monoclonal antibody directed against the GP IIb/IIIa receptor. Its
mechanism of action appears to be steric hindrance of the receptor as opposed to direct binding to the RGD binding
site of the receptor. Abciximab also inhibits the vitronectin (av b3)receptor, which mediates both platelet coagulation in
addition to endothelial and vascular smooth muscle cell proliferation. The significance of vitronectin-receptor blockade
is unknown. It produces a direct antithrombotic effect by inhibiting the binding of fibrinogen to the receptor and
consequently inhibiting platelet aggregation.78 Because abciximab is a more potent inhibitor of platelet function than
aspirin, it potentially produces a greater degree of thrombolysis and prevents rethrombosis in short-term management
of patients with STEMI.78,79
Eptifibatide (Figure 4) is another GP IIb/IIIa antagonist. It dose-dependently inhibits platelet aggregation and in a
baboon model refractory to aspirin and heparin, inhibited aggregation, preventing acute thrombosis with only a modest
prolongation (two- to threefold) of the bleeding time.
Tirofiban (Figure 4) is a nonpeptide inhibitor of the GP IIb/IIIa receptor. It reduces ischemic events at 48 h
following infusion when compared to standard heparin therapy and is extensively used in percutaneous transluminal
coronary angioplasty (PTCA) and acute coronary syndromes (ACS).
Platelet GP IIb/IIIa receptor antagonists have been shown to be effective and safe in reducing death and cardiac
ischemic events among patients presenting with acute coronary syndromes without ST-segment elevation.80

CO2H
OCOCH3
Aspirin
CH2
N
SCl
Ticlopidine
N
N
NN
N N
C2H4OH
C2H4OH
N
HOC2H4
HOC2H4
Dipyridamole
O
OH
O
CH2COCH3
Warfarin
H2N NH
NH
HN
OO
HN
S
H2N
O
HN
O N
O
NH
CH2CO2HO
HN
NH
SO
EptifibatideS N
H
OOCH3
Cl
Clopidogrel
HN (CH2)4O
H2C
H
CO2H
NHSO2(CH2)3CH3
Tirofiban(a)
(b)
NS
SN
C2H5O
O
O
OH
S
O OO
HN
S
N
OC2H5
CT-50547
N
N N
N
O
OO
NH
O
NH
C2H5
OP
ONaO
NaO
H
H
H
INS-50589
N
Figure 4 Thrombolytics.
776 Thrombolytics
Angiographic observations suggest that abciximab facilitates dissolution of intracoronary thrombi without a significant
risk of distal embolization.81 Moreover, abciximab administered in conjunction with low-dose thrombolytic agents, e.g.,
reteplase, produces a sustained fibrinolytic effect and enhanced early reperfusion in patients with AMI with a favorable
hemorrhagic profile as compared to full-dose thrombolytic therapy.82 However, larger mortality trials need to be
performed to provide definitive evidence as to whether such combination therapies improve mortality without
increasing the risk of intracranial hemorrhage to an unacceptable level.37

Thrombolytics 777
6.34.7.5 P2Y12 Antagonists
Ticlopidine and clopidogrel (Figure 4) are prototypic antagonists of the platelet P2Y12 receptor that is involved in the
inhibition of platelet function by selectively blocking ADP-induced platelet aggregation. These compounds were in
clinical use long before the P2Y12 receptor was identified and cloned. In patients with unstable angina, ticlopidine
reduced endpoints that included nonfatal and fatal myocardial infarction and any cause of cardiovascular death in
events at 6 months (13.6% placebo, 7.3% ticlopidine) with a noted trend toward mortality benefit as well. Clopidogrel
produces platelet inhibition in a shorter period than ticlopidine, has fewer severe adverse effects, requires only once
per day dosing, and is cheaper than a twice per day regimen of ticlopidine. Newer P2Y12 receptor antagonists include
CT-50547 and INS-50589 (Figure 4) both of which are in the preclinical stage.
6.34.8 Future Directions
Older agents, though effective, still have limitations such as risks of intracranial hemorrhage and 5–15% reocclusion
rate. Ongoing efforts to develop newer thrombolytics that overcome the limitations seen with older agents are
underway. Ideally, new thrombolytic agents should: (1) be fibrin specific; (2) be directed to newly formed fibrin
without affecting normal hemostasis; (3) be nonantigenic; (4) be cost effective; and (5) have rapid onset. One such
agent is BB-10153, an engineered variant of human plasminogen that is modified to be activated to plasmin by
thrombin (a.k.a thrombin-activatable plasminogen). It was designed to act as a prodrug, persisting in the blood and
activating only plasmin in fresh or forming thrombi. In essence, it should only act on clot-bound thrombin.
Consequently, thrombus dissolution may be achieved without systemic destruction of hemostatic proteins, thus
potentially reducing the risk of haemorrhage. The plasma half-life of BB-10153 was found to be 3–4 h and it also had no
effect on plasma a2-antiplasmin or fibrinogen levels, coagulation assays, or bleeding time. The long half-life and
thrombus-selective thrombolytic activity of BB-10153 are promising and might allow it to overcome the bleeding and
reocclusion shortfalls in the performance of current thrombolytics.83,84
Essentially, development of newer agents and an approach using a combination of pharmacological and mechanical
strategies would increase the rates of recannalization, enhance the reversal of acute coronary syndromes, and improve
patient outcomes.
References
1. Blann, A. D.; Landray, M. J.; Lip, G. Y. Br. Med. J. 2002, 325, 762–765.
2. Bizjak, E. D.; Mauro, V. F. Ann. Pharmacother. 1998, 32, 769–784.
3. Davoren, J. B. Blood Disorders. In Pathophysiology of Disease: An Introduction to Clinical Medicine; McPhee, S. J., Lingappa, V. R., Ganong, W. F.,
Eds.; The McGraw-Hill Companies, Inc.: New York, 2003, pp 113–142.
4. Fedan, J. S. Anticoagulant, Antiplatelet, and Fibrinolytic (Thrombolytic) Drugs. In Modern Pharmacology with Clinical Applications; Craig, C. R.,
Stitzel, R. E., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, 2004, pp 256–267.
5. Virchow, R. A M von Meidinger Sohn. 1856, 520–525.
6. Fuster, V.; Badimon, L.; Badimon, J. J.; Chesebro, J. H. N. Engl. J. Med. 1992, 326, 242–250.
7. Fuster, V.; Badimon, L.; Badimon, J. J.; Chesebro, J. H. N. Engl. J. Med. 1992, 326, 310–318.
8. Fuster, V.; Fayad, Z. A.; Badimon, J. J. Lancet 1999, 353, SII5–SII9.
9. Fuster, V.; Gotto, A. M.; Libby, P.; Loscalzo, J.; McGill, H. C. J. Am. Coll. Cardiol. 1996, 27, 964–976.
10. Rauch, U.; Osende, J. I.; Fuster, V.; Badimon, J. J.; Fayad, Z.; Chesebro, J. H. Ann. Intern. Med. 2001, 134, 224–238.
11. Davies, M. J. Thromb. Res. 1996, 82, 1–32.
12. Stary, H. C. Arteriosclerosis 1989, 9, I19–I32.
13. Stary, H. C.; Blankenhorn, D. H.; Chandler, A. B.; Glagov, S.; Insull, W., Jr.; Richardson, M.; Rosenfeld, M. E.; Schaffer, S. A.; Schwartz, C. J.;
Wagner, W. D. et al. Circulation 1992, 85, 391–405.
14. Wissler, R. W. Ann. NY Acad. Sci. 1991, 623, 26–39.
15. Toschi, V.; Gallo, R.; Lettino, M.; Fallon, J. T.; Gertz, S. D.; Fernandez-Ortiz, A.; Chesebro, J. H.; Badimon, L.; Nemerson, Y.; Fuster, V. et al.
Circulation 1997, 95, 594–599.
16. Mallat, Z.; Hugel, B.; Ohan, J.; Leseche, G.; Freyssinet, J. M.; Tedgui, A. Circulation 1999, 26, 348–353.
17. Turitto, V. T.; Hall, C. L. Thromb. Res. 1998, 92, S25–S31.
18. Loscalzo, J. Arteriosclerosis 1990, 10, 672–679.
19. Brook, J. G.; Aviram, M. Semin. Thromb. Hemost. 1988, 14, 258–265.
20. Collen, D.; Lijnen, H. R. Crit. Rev. Oncol. Hematol. 1986, 4, 249–301.
21. Christ, G.; Hufnagl, P.; Kaun, C.; Mundigler, G.; Laufer, G.; Huber, K.; Wojta, J.; Binder, B. R. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 723–730.
22. Bergmann, S. R.; Fox, K. A.; Ter-Pogossian, M. M.; Sobel, B. E.; Collen, D. Science 1983, 220, 1181–1183.
23. Van de Werf, F.; Bergmann, S. R.; Fox, K. A.; de Geest, H.; Hoyng, C. F.; Sobel, B. E.; Collen, D. Circulation 1984, 69, 605–610.
24. Gold, H. K.; Fallon, J. T.; Yasuda, T.; Leinbach, R. C.; Khaw, B. A.; Newell, J. B.; Guerrero, J. L.; Vislosky, F. M.; Hoyng, C. F.; Grossbard, E.
et al. Circulation 1984, 70, 700–707.
25. Flameng, W.; Van de Werf, F.; Vanhaecke, J.; Verstraete, M.; Collen, D. J. Clin. Invest. 1985, 75, 84–90.

778 Thrombolytics
26. Gu, S.; Ducas, J.; Patton, J. N.; Greenberg, D.; Prewitt, R. M. Chest 1992, 101, 1684–1690.
27. Yasuda, T.; Gold, H. K.; Leinbach, R. C.; Saito, T.; Guerrero, J. L.; Jang, I. K.; Holt, R.; Fallon, J. T.; Collen, D. J. Am. Coll. Cardiol. 1990, 16,
1728–1735.
28. Rapold, H. J.; Wu, Z. M.; Stassen, T.; Van de Werf, F.; Collen, D. Blood 1990, 76, 1558–1563.
29. Hennan, J. K.; Elokdah, H.; Leal, M.; Ji, A.; Friedrichs, G. S.; Morgan, G. A.; Swillo, R. E.; Antrilli, T. M.; Hreha, A.; Crandall, D. L.
J. Pharmacol. Exp. Ther. 2005, 314, 710–716.
30. Feied, C.; Handler, J. A. Thromboytic Therapy. Emergency Medicine, September 7, 2004
31. Fletcher, A. P.; Alkjaersig, N.; Smyrniotis, F. E.; Sherry, S. Trans. Assoc. Am. Physicians 1958, 71, 287–296.
32. Boucek, R. J.; Murphy, W. P., Jr. Am. J. Cardiol. 1960, 6, 525–533.
33. Chazov, E. I.; Matveeva, L. S.; Mazaev, A. V.; Sargin, K. E.; Sadovskaia, G. V.; Ruda, M. I. Ter Arkh 1976, 48, 8–19.
34. Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto Miocardico (gissi). Lancet 1986, 1, 397–402.
35. Khan, I. A.; Gowda, R. M. Int. J. Cardiol. 2003, 91, 115–127.
36. Alexandrov, A. V.; Masdeu, J. C.; Devous, M. D., Sr.; Black, S. E.; Grotta, J. C. Stroke 1997, 28, 1830–1834.
37. Ohman, E. M.; Harrington, R. A.; Cannon, C. P.; Agnelli, G.; Cairns, J. A.; Kennedy, J. W. Chest 2001, 119, 253S–277S.
38. Majerus, P. W.; Tollefsen, D. M. Anticoagulant, Thrombolytic, and Antiplatelet Drugs. In Goodman & Gilman’s the Pharmacological Basis of
Therapeutics; McGraw-Hill: New York, 2001, pp 1519–1538.
39. Gulba, D. C.; Bode, C.; Runge, M. S.; Huber, K. Ann. Hematol. 1996, 73, S9–S27.
40. Maizel, A. S.; Bookstein, J. J. Cardiovasc. Intervent. Radiol. 1986, 9, 236–244.
41. Wagstaff, A. J.; Gillis, J. C.; Goa, K. L. Drugs 1995, 50, 289–316.
42. Collen, D.; Lijnen, H. R. Fibrinolysis and the Control of Hemostasis. In The Molecular Basis of Blood Diseases; Stamatoyannopoulos, G., Nienhui,
A. W., Majerus, P. W., Varmus, H., Eds.; Saunders: Philadelphia, PA, 1994, pp 662–688.
43. Tanswell, P.; Tebbe, U.; Neuhaus, K. L.; Glasle-Schwarz, L.; Wojcik, J.; Seifried, E. J. Am. Coll. Cardiol. 1992, 19, 1071–1075.
44. Wooster, M. B.; Luzier, A. B. Ann. Pharmacother. 1999, 33, 318–324.
45. Smalling, R. W.; Bode, C.; Kalbfleisch, J.; Sen, S.; Limbourg, P.; Forycki, F.; Habib, G.; Feldman, R.; Hohnloser, S.; Seals, A. Circulation 1995,
91, 2725–2732.
46. Davydov, L.; Cheng, J. W. Clin. Ther. 2001, 23, 982–997, discussion 981.
47. Liberatore, G. T.; Samson, A.; Bladin, C.; Schleuning, W. D.; Medcalf, R. L. Stroke 2003, 34, 537–543.
48. Kratzschmar, J.; Haendler, B.; Langer, G.; Boidol, W.; Bringmann, P.; Alagon, A.; Donner, P.; Schleuning, W. D. Gene 1991, 105, 229–237.
49. Bringmann, P.; Gruber, D.; Liese, A.; Toschi, L.; Kratzchmar, J.; Schleuning, W. D.; Donner, P. J. Biol. Chem. 1995, 270, 25596–25603.
50. Toschi, L.; Bringmann, P.; Petri, T.; Donner, P.; Schleuning, W. D. Eur. J. Biochem. 1998, 252, 108–112.
51. Hacke, W.; Albers, G.; Al-Rawi, Y.; Bogousslavsky, J.; Davalos, A.; Eliasziw, M.; Fischer, M.; Furlan, A.; Kaste, M.; Lees, K. R. et al. Stroke 2005,
36, 66–73.
52. Mellott, M. J.; Stabilito, I. I.; Holahan, M. A.; Cuca, G. C.; Wang, S.; Li, P.; Barrett, J. S.; Lynch, J. J.; Gardell, S. J. Arterioscler Thromb. 1992, 12,
212–221.
53. Franzosi, M. G.; Santoro, E.; De Vita, C.; Geraci, E.; Lotto, A.; Maggioni, A. P.; Mauri, F.; Rovelli, F.; Santoro, L.; Tavazzi, L. et al. Circulation
1998, 98, 2659–2665.
54. Isis-2 (Second International Study of Infarct Survival) Collaborative Group. Lancet 1988, 2, 349–360.
55. Baigent, C.; Collins, R.; Appleby, P.; Parish, S.; Sleight, P.; Peto, R. Br. Med. J. 1998, 316, 1337–1343.
56. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico. Lancet 1990, 336, 65–71.
57. The International Study Group. Lancet 1990, 336, 71–75.
58. Gissi-2 and International Study Group: Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto. Eur. Heart J. 1992, 13, 1692–1697.
59. Isis-3 (Third International Study of Infarct Survival) Collaborative Group. Lancet 1992, 339, 753–770.
60. Califf, R. M.; White, H. D.; Van de Werf, F.; Sadowski, Z.; Armstrong, P. W.; Vahanian, A.; Simoons, M. L.; Simes, R. J.; Lee, K. L.; Topol, E. J.
Circulation 1996, 94, 1233–1238.
61. The Continuous Infusion versus Double-Bolus Administration of Alteplase (Cobalt) Investigators. N. Engl. J. Med. 1997, 337, 1124–1130.
62. Fibrinolytic Therapy Trialists’ (ftt) Collaborative Group. Lancet 1994, 343, 311–322.
63. Bode, C.; Smalling, R. W.; Berg, G.; Burnett, C.; Lorch, G.; Kalbfleisch, J. M.; Chernoff, R.; Christie, L. G.; Feldman, R. L.; Seals, A. A. et al.
Circulation 1996, 94, 891–898.
64. The Global Use of Strategies to Open Occluded Coronary Arteries (Gusto iii) Investigators. N. Engl. J. Med. 1997, 337, 1118–1123.
65. International Joint Efficacy Comparison of Thrombolytics. Lancet 1995, 346, 329–336.
66. Cannon, G. P.; McCabe, C. H.; Gibson, M.; The TIMI 10 Investigators. Proc. Natl. Acad. Sci. USA 1994, 95, 351.
67. Cannon, C. P.; Gibson, C. M.; McCabe, C. H.; Adgey, A. A.; Schweiger, M. J.; Sequeira, R. F.; Grollier, G.; Giugliano, R. P.; Frey, M.; Mueller,
H. S. et al. Circulation 1998, 98, 2805–2814.
68. Van de Werf, F.; Cannon, C. P.; Luyten, A.; Houbracken, K.; McCabe, C. H.; Berioli, S.; Bluhmki, E.; Sarelin, H.; Wang-Clow, F.; Fox, N. L.
et al. Am. Heart J. 1999, 137, 786–791.
69. Assessment of the Safety and Efficacy of a new Thrombolytic Investigators. Lancet 1999, 354, 716–722.
70. The 22nd Congress of the European Society of Cardiology, Amsterdam, September 2000.
71. The Assent-3 Randomised Trial in Acute Myocardial Infarction. Lancet 2001, 358, 605–613.
72. den Heijer, P.; Vermeer, F.; Ambrosioni, E.; Sadowski, Z.; Lopez-Sendon, J. L.; von Essen, R.; Beaufils, P.; Thadani, U.; Adgey, J.; Pierard, L.
et al. Circulation 1998, 98, 2117–2125.
73. Tebbe, U.; Michels, R.; Adgey, J.; Boland, J.; Caspi, A.; Charbonnier, B.; Windeler, J.; Barth, H.; Groves, R.; Hopkins, G. R. et al. J. Am. Coll.
Cardiol. 1998, 31, 487–493.
74. Van de Werf, F.; Ardissino, D.; Betriu, A.; Cokkinos, D. V.; Falk, E.; Fox, K. A.; Julian, D.; Lengyel, M.; Neumann, F. J.; Ruzyllo, W. et al. Eur.
Heart J. 2003, 24, 28–66.
75. Zhao, L.; Gray, L.; Leonardi-Bee, J.; Weaver, C. S.; Heptinstall, S.; Bath, P. M. Platelets 2006, 17, 100–104.
76. Coller, B. S.; Folts, J. D.; Smith, S. R.; Scudder, L. E.; Jordan, R. Circulation 1989, 80, 1766–1774.
77. Lefkovits, J.; Plow, E. F.; Topol, E. J. N. Engl. J. Med. 1995, 332, 1553–1559.
78. Coller, B. S. Thromb. Haemost. 1997, 78, 730–735.
79. Davies, C. H.; Ormerod, O. J. Lancet 1998, 351, 1191–1196.

Thrombolytics 779
80. Kong, D. F.; Califf, R. M.; Miller, D. P.; Moliterno, D. J.; White, H. D.; Harrington, R. A.; Tcheng, J. E.; Lincoff, A. M.; Hasselblad, V.; Topol, E.
J. Circulation 1998, 98, 2829–2835.
81. Antman, E. M.; Giugliano, R. P.; Gibson, C. M.; McCabe, C. H.; Coussement, P.; Kleiman, N. S.; Vahanian, A.; Adgey, A. A.; Menown, I.;
Rupprecht, H. J. et al. Circulation 1999, 99, 2720–2732.
82. Califf, R. M. Am. Heart J. 2000, 139, S33–S37.
83. Comer, M. B.; Cackett, K. S.; Gladwell, S.; Wood, L. M.; Dawson, K. M. J. Thromb. Haemost. 2005, 3, 146–153.
84. Curtis, L. D.; Brown, A.; Comer, M. B.; Senior, J. M.; Warrington, S.; Dawson, K. M. P. J. Thromb. Haemost. 2005, 3, 1180–1186.
Biographies
Ahmed E El-Gengaihy, MD, MSc is currently a Chief Neurology Resident at the University of Medicine and
Dentistry of New Jersey (UMDNJ). He has completed his Neuropsychiatry residency at Ain Shams University, Cairo,
Egypt. He subsequently joined Baylor College of Medicine for 1 year as a research fellow followed by his current
residency training at UMDNJ. His research interests include neuroimaging of cerebrovascular diseases, neurocritical
care, and basic and clinical aspects of interventional cerebrovascular diseases.
Samir I Abdelhadi, DO, is currently a second year resident of the Internal Medicine Program at the University of
Medicine and Dentistry of New Jersey (UMDNJ). He hopes to obtain a Cardiology fellowship at the end of his
residency training and is currently doing research within the Cardiology program at UMDNJ.

780 Thrombolytics
Jawad F Kirmani, MD, is currently an assistant professor with the stroke interventional team at the University of
Medicine and Dentistry of New Jersey (UMDNJ). He completed his Neurology residency at the Ohio State University.
He subsequently joined the State University of New York at Buffalo for a 2-year fellowship in neurocritical care and
cerebrovascular diseases followed by two further years of training in interventional neurology at UMDNJ. His research
interests include neuroimaging of cerebrovascular diseases, neurocritical care, neurocardiology, and basic and clinical
aspects of interventional cerebrovascular diseases.
Adnan I Qureshi is Professor of Neurology and Neurosciences and Director of the Cerebrovascular Program at the
University of Medicine and Dentistry of New Jersey (UMDNJ). Dr Qureshi is recognized as an international leader in
stroke research and acute stroke management by physicians from multiple disciplines. He has written over 160
scientific publications in prestigious journals including the New England Journal of Medicine, Lancet, Archives of Internal
Medicine, Critical Care Medicine, Neurology, Stroke, and Circulation. In addition, he has made over 500 presentations in
various national and international meetings. He has served as an invited speaker at numerous national and international
forums. He has also been invited as visiting professor to universities in the United States and abroad. He serves on
editorial boards for several peer-review journals and guideline committees for American Heart Association and
American Society of Neuroimaging. He is the present chair of the interventional section of the American Academy of
Neurology and a Fellow of the American Heart Association. He is also the chair of the research committee of the
American Society of Interventional and Therapeutic Neuroradiology. He was one of the founders of the subspecialty of
interventional neurology.
Dr Qureshi’s work has led to the development of new concepts for therapies and research pertaining to prevention of
stroke. The work has importance for the general population and has appeared in numerous public information sources
such as ABC, NBC, American Heart Association News, American Medical Association News, Web MD, Men’s Health,
and USA Today. His work has impacted upon the management of stroke by other physicians and incorporation into
practice guidelines. Dr Qureshi has received several prestigious awards at the national level including the AMA
Foundation Leadership award, the AAN-AB Baker Teacher Recognition award, NAPH Safety Net Community and
Patient Service Award, Excellence in Care Award, the AHA/NCQA Achievement of Recognition for Delivery of Quality
Stroke Care, and AMA Community Service award. He has been selected by his peers as one of The Best Doctors in America
and was selected by the Consumer Research Council of America as one of America’s Top Physicians.

Thrombolytics 781
Most recently, he laid the foundation of the Zeenat Qureshi Stroke Research Center at University of Medicine and
Dentistry of New Jersey. Since its inauguration, the center has led the way in cutting edge research in epidemiology,
clinical trials, and basic research pertaining to cerebrovascular diseases. Several investigators in the center receive
funding through National Institutes of Health, American Heart Association, and Armed Forces Research Initiatives.
Dr Qureshi has mentored several fellows and medical students. He has trained several clinical fellows in cerebro-
vascular diseases and endovascular procedures and is presently the program director for ACGME accredited vascular
neurology program at UMDNJ. Several of his students and fellows have won national awards for research performed
under his direct supervision. He continues to serve as course director for various educational seminars at a regional and
national level. He is married to Aasma Qureshi who is presently completing her fellowship in Gastroenterology at
Emory University in Atlanta.
& 2007 Elsevier Ltd. All Rights Reserved Comprehensive Medicinal Chemistry II
No part of this publication may be reproduced, stored in any retrieval system or transmittedin any form by any means electronic, electrostatic, magnetic tape, mechanical, photocopying,
recording or otherwise, without permission in writing from the publishers
ISBN (set): 0-08-044513-6
ISBN (Volume 6) 0-08-044519-5; pp. 763–781