Embed Size (px)
Citation preview
Update on Novel (and well-worn) Anticoagulants and Thrombolytics
Melinda T. Ryan, RN, BSN, MSN, CNP
Department of Vascular Medicine
Cleveland Clinic

Disclosures
• None

New options!

Acronyms for new oral anticoagulants
• NOACs: new oral anti-coagulants,
novel oral anti-coagulants, non-monitored oral anti-coagulants, non-warfarin oral anti-coagulants, non Vitamin K antagonist oral anti-coagulants
• DOACs: direct oral anti-coagulants
• TSOCs: target specific oral anticoagulants
• ODIs oral direct inhibitors

Factor Xa inhibitors
Apixaban (Eliquis)
Rivaroxaban (Xarelto)

Coagulation pathway

Apixaban
• FDA approved indications for treatment
• Nonvalvular a-fib
• Treatment of DVT/PE
• Reduction in the risk of recurrent DVT/PE following initial therapy
• Prophylaxis for DVT after orthopedic surgery
• Trials
• Non-valvular afib : ARISTOTLE
• DVT/PE: AMPLIFY,
• Reduction in the risk of recurrent DVT/PE: AMPLIFY-EXT
• Prophylaxis for orthopedic surgery: ADVANCE 1-3

Apixaban Dosing
• Non-valvular afib
5 mg twice daily
Dose adjustment for NVAF pts w/following criteria
- Age > 79 years
- Body weight <60 kg
- Serum creatinine >1.5 mg/dl
2.5 mg twice daily
• DVT/PE
10 mg twice daily for the first 7 days
Then 5 mg twice daily

Apixaban dosing
• Reduction in the risk of recurrent DVT/PE following initial therapy
• 2.5 mg twice daily after at least 6 months of treatment for DVT/PE
• DVT/PE prophylaxis after orthopedic surgery–
• 2.5 mg twice daily x35 days starting 12-24 hours after hip replacement surgery
• 2.5 mg twice daily for 12 days after 12-24 hours after knee replacement surgery

Apixaban Pharmacologic profile
• Onset of action: 3-4 hours
• Protein Binding ~87%
• Metabolism: predominantly via CYP3A4/5
• Bioavailability ~50%
• Time to peak 3-4 hours
• ½ life: ~ 12 hours
• Excretion: Urine ~27% as parent drug, feces

Contraindications to Apixaban
• Acute bleeding
• Severe reaction to ELIQUIS (anaphylactic reactions)
• Use w/caution
ASA, anti-platelets , NSAIDs, thrombolytics, SSRI, SNRIs
NOT approved for prosthetic heart valves
Recommends against use in acute PE in a hemodynamically unstable pt or pts who require thrombolysis or pulmonary embolectomy
• Coadministration with strong dual inhibitors of CYP3A4 and P-gp should be avoided
Examples: - Ketoconazole - Itraconazole - Ritonavir - Clarithromycin - Rifampin - Carbamazepine - St. John’s wort

Apixaban
• Use caution w/ pts who underwent spinal and epidural anesthesia
• Per package insert
• Catheters should not be removed earlier than 24 hours after last administration of apixaban
• The next dose of apixaban should not be administered earlier than 5 hours after the removal of the catheter
• If traumatic puncture delay the administration of apixaban x48 hours
Rivaroxaban
• FDA approved indications for treatment
• nonvalvular a-fib
• PE/DVT
• reduce the risk of recurrence of DVT and/PE
• prophylaxis for orthopedic surgery
• Trials
• A-fib: ROCKET AF
• DVT/PE EINSTEIN DVT and PE
• Reduce the risk of recurrent DVT/PE: EINSTEIN-EXT
• Prophylaxis for orthopedic surgery RECORD 1-4

Rivaroxaban Dosing
• Nonvalvular Afib:
• 20 mg daily w/evening meal: Pts with CrCl>50 mL/min
• 15 mg daily w/evening meal Patients CrCl 15-50 mL/min
• DVT/PE
• 15 mg TWICE daily x21 days
• Then 20 mg once daily w/food

Rivaroxaban dosing
• Extended Treatment:
• 20 mg once daily with food
• Orthopedic surgery Prophylaxis
• Knee: 10 mg once daily x 12 days
• Hip: 10 mg once daily x35 days
• Initial dose should be taken at least 6-10 hours after surgery once hemostasis established

Rivaroxaban Pharmacologic Profile
• Absorption: Rapid
• Protein Binding: ~92-95% primarily to albumin
• Metabolism: Hepatic via CYP3A4/5 and CYP2J2
• Bioavailability: Absolute bioavailability: 10 mg dose: ~80% to 100%; 20 mg dose: ~66% (fasting; increased with food)
• ½ life: 5-9 hours for healthy subjects 20-45 years 11-13 hours in the elderly
• Time to peak: 2-4 hours
• Excretion: Urine (66% primarily via active tubular secretion, feces
Contraindications to Rivaroxaban
• Acute pathological bleeding
• Severe hypersensitivity to rivaroxaban
• Use w/caution: ASA, anti-platelets , NSAIDs, thrombolytics
• NOT approved for prosthetic heart valve
• Avoid concomitant administration of rivaroxaban w/CYP3A4 and drug transport systems
• Ex: Rifampin, phenytoin, carbamazepine, St. John’s wort
Rivaroxaban
• Pts w/renal impairment receiving full dose rivaroxaban in combination w/drugs classified as combined P-gp and weak or moderate CYP3A4 inhibitors may have increase in exposure
• EX: amiodarone, diltiazem, verapamil, quinidine, ranolazine, dronedarone, felodipine, erythromycin, and azithromycin

Rivaroxaban
• Use w/caution in pt undergoing spinal/Epidural Anesthesia
• An epidural catheter should not be removed earlier than 18 hours after last administration of Rivaroxaban.
• The next Rivaroxaban dose should not be administered earlier than 6 hours after the removal of catheter
• If traumatic puncture hold x24 hours

Factor Xa Inhibitors things to consider
• Both Apixaban and rivaroxaban can effect INR (i.e. elevate INR) w/out direct correlation to level of anticoagulation
• Currently there is no therapeutic assay, to check levels of drug
• No antidote or reversal agent in life threatening bleeding
• Increased risk of stroke after discontinuation in nonvalvular atrial fib
Converting to Factor Xa
• DC warfarin Begin apixaban or rivaroxaban once INR <3
• Note onset of action is rapid
• if converting from LMWH or parental agent, begin Factor Xa when next dose of injection is due, or stop heparin gtt begin Factor Xa inhibitor
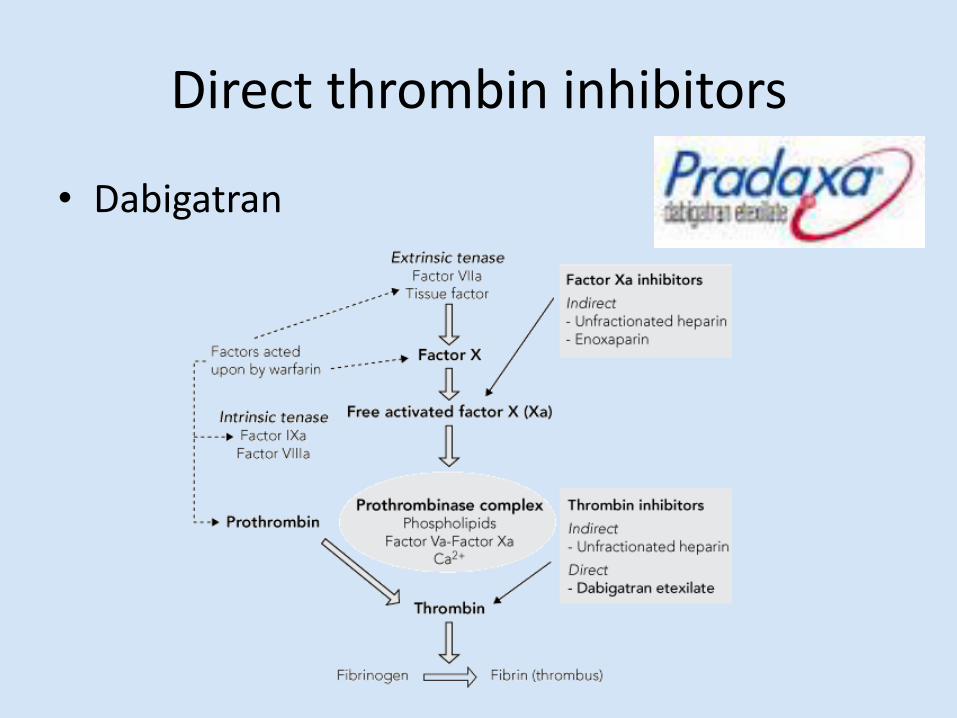
Direct thrombin inhibitors
• Dabigatran
Dabigatran
• FDA approved:
• Nonvalvular afib
• DVT/PE (w/bridging)
• To reduce the risk of recurrence of DVT/PE in pts who have been previously treated
• Trials
• Nonvalvular afib: RE-LY
• DVT/PE: RECOVER I, II
• To reduce the risk of recurrence of DVT/PE in pts who have been treated: RE-MEDY
Dabigatran Dosing
• Nonvalvular afib:
• 150 mg twice daily CrCl>30 mL/min
• 75 mg twice daily CrCl 15-30 mL/min
• DVT/PE
• 5-10 days of parental anticoagulant (LMWH, Fondaparinux, IV unfractionated heparin
• Then:
• 150 mg twice daily

Dabigatran Pearls
• Take w/w/out food but should be taken with a full glass of water
• Caution in pts w/GI bleeding or ulcer or dyspepsia, gastritis
• Dabigatran capsules light sensitive, come in blister packs or bottles but should not be placed in pill containers

Dabigatran Pharmacologic Profile
• Absorption: Rapid, initially slow post-operatively
• Protein Binding 35% • Metabolism: Hepatic;
dabigatran etexilate is rapidly and completely hydrolyzed to dabigatran (active form) by plasma and hepatic esterases
• Bioavailability 3-7% • ½ life: 12-17 hours;
Elderly: 14-17 hours; Mild-to-moderate renal impairment: 15-18 hours; Severe renal impairment: 28 hours
• Time to Peak: plasma: Dabigatran: 1 hour; delayed 2 hours by food (no effect on bioavailability)
• Excreted: Urine (80%)

Contraindication to Dabigatran
• Life threatening bleeding
• Sensitivity to dabigatran
• Prosthetic heart valves (trial ended early due to more thromboembolic events and bleeding
• Use w/caution:
• Age >75 years of age
• Have kidney problems
• Have hx of GI bleeding
• Concomitant use of dabigatran and P-gp Inducers and inhibitors
• (dronedarone, ketoconazole)

Dabigatran
• Use w/caution in spinal/epidural anesthesia or puncture
• Drug profile does not give specific recommendations for dosing

Dabigatran
• No monitoring for compliance
• Can effect aptt, may use aptt to predict excretion of drug (not directly reliable)
• Also can use ECT or thrombin time
• No reversal agent
• Dialysis has been used in life threatening cases
• Activated charcoal if recent ingestion

Low molecular weight heparin
• Dalteparin
• Enoxaparin

Low molecular weight heparin

Dalteparin
• FDA indications: DVT prophylaxis in patients undergoing abdominal surgery, orthopedic surgery, medical pts
• prevention of ischemic complications in patients with unstable angina or non-Q-wave myocardial infarction on concurrent aspirin therapy
• in patients with cancer, extended treatment (6 months) of acute symptomatic venous thromboembolism (DVT and/or PE) to reduce the recurrence of venous thromboembolism
• Unlabeled use: (US) treatment of acute DVT/PE

Dalteparin dosage
• prophylactic dose: 5,000 IU SC daily
• DVT/PE dose:
• 200 IU/kg SC injection daily x 30 days
• Followed by
• 150 IU/kg for maintenance therapy
• Be aware of weight restrictions in obese pts
• Syringe sizes:
• 5,000 IU
• 7,500 IU
• 10,000 IU
• 12,500 IU
• 15,000 IU
• 18,000 IU
Dalteparin Pharmacologic Profile
• Onset of action: 1-2 hours
• Protein binding: Low affinity for plasma proteins
• Bioavailability: SubQ: 81% to 93%
• ½ life elimination 3-5 h; 6-7h renal impairment
• Time to peak, serum: ~4 hours
• Excretion: Primarily renal

Contraindications to Dalteparin
• Active bleeding • Hypersensitivity reaction
to Dalteparin • Active HIT or history of
HIT • Kidney Dysfunction CrCl
<30
• Use w/caution: extremes in weigh (high or low)
• Max dose of Dalteparin 18,000 IU syringe
• Monitor closely if impaired renal function
Examine for safe SC injection sites in low body weight pts •Use w/caution in concomitant: NSAID, ASA, anti-platelet agents

Enoxaparin
• FDA approved:
• ACS (acute coronary syndrome)
• Acute STEMI/NSTEMI
• DVT prophylaxis in orthopedic, abdominal surgery and medical pts
• DVT/PT treatment

Enoxaparin Dosing
• ACS: different protocols but used IV in PCI then:
• 1 mg/kg q 12
• 1.5 mg/kg q 24
• DVT/PE
• 1 mg/kg q 12 or
• 1.5 mg/kg q 24
• DVT prophylaxis medical/surgical pts
• Lovenox 40 mg daily
• Except:
• Total knee replacement
• Lovenox 30 mg q 12
• Bariatric surgery
• 40 mg q 12 or
• 60 mg q 12

Enoxaparin Pharmacologic profile
• Onset of action:3-5 hours
• Protein binding: does not bind to heparin binding proteins
• Metabolism: Hepatic, to lower molecular weight fragments (little activity)
• ½ life; 4.5 to 7 hours
• Excretion: Urine (40% of dose; 10% as active fragments)

Contraindications to Enoxaparin
• Life threatening bleeding
• Anaphlyactic reaction to injections
• Kidney dysfunction CrCl <30
• Pt w/active heparin induced thrombocytopenia or history of HIT
• Use w/caution:
Extremes of weight Low and high
Max dose is 150 mg
Examine for safe SC injection sites in low body weight pts
•Use w/caution in concomitant: NSAID, ASA, anti-platelet agents
•Use w/caution in impaired renal function

LMWH pearls
• At times very expensive out of pocket cost, ensure pt can afford co-pay prior to leaving hospital or clinic
• Can check LMWH assay to ensure compliance or in extremes of weight (low or high) or pregnant patients
• LMWH assay should be drawn 4 hours after 3rd dose of enoxaparin or dalteparin
• Target LMWH assay 0.5-1.0
• Use w/caution in spinal/epidural anesthesia
• LMWH is partially reversible w/protamine in life threatening bleeding
• unlabeled use: IV: Note: Anti-Xa activity is never completely neutralized (maximum: ~60% to 75%).

Protamine dosage for LMWH
• Enoxaparin • Last dose administered in ≤8
hours: Dose of protamine should equal the dose of enoxaparin administered. Therefore, 1 mg of protamine sulfate neutralizes 1 mg of enoxaparin.
• Enoxaparin administered in > 8 hours or if it has been determined that a second dose of protamine is required (eg, if aPTT measured 2-4 hours after the first dose remains prolonged or if bleeding continues): 0.5 mg of protamine sulfate for every 1 mg of enoxaparin administered
• Dalteparin • 1 mg protamine for each 100
anti-Xa units of dalteparin if PTT prolonged 2-4 hours after first dose (or if bleeding continues), consider additional dose of 0.5 mg for each 100 anti-Xa units of dalteparin or tinzaparin.
• Note check allergies, fish allergy Protamine contraindicated
• Use caution in male pts w/surgical history of vasectomy

CLOT trial
• 2003 NEJM
• Compared Dalteparin vs. warfarin in malignancy pts
• The incidence of recurrent thromboembolism in the dalteparin only group was significantly less than the oral anticoagulation group.
• There was no significant difference in bleeding or mortality detected between the two groups.
• This trial is why LMWH injections are preferred over warfarin in malignancy patients
Injectable factor Xa
• Fondaparinux • FDA indications: DVT prophylaxis in patients undergoing surgery for orthopedic surgery, abdominal surgery. Treatment of acute PE/DVT Unlabeled Use: Prophylaxis in pts w/history of HIT, treatment of acute thrombosis (unrelated to HIT) in patients with a past history of HIT; acute symptomatic superficial vein thrombosis (≥5 cm in length) of the legs

Fondaparinux Pharmacologic Profile
• Absorption: Rapid and Complete
• Protein Binding: ≥94% to antithrombin III
• Bioavailability: SubQ: 100%
• ½ life 17-21 hours, prolonged in renal dysfunction
• Time to Peak: Time to peak: SubQ: 2 to 3 hours
• Excretion: Urine (~77%, unchanged drug)

Fondaparinux Dosing
• Prophylactic Dose: in adults pts > 50 kg 2.5 mg SC daily
• Acute DVT/PE: < 50 kg: 5 mg SC injection daily
50-100 kg: 7.5 mg SC injection daily
>100 kg: 10 mg SC injection daily
• May be a better option for morbidly obese pts (trials included pts up to 180 kg)
• Case reports of Fondaparinux induced “HIT”

Contraindications to Fondaparinux
• Active Bleeding
• Hypersensitivity reaction to injections
• CrCl <30
• Use w/caution in spinal/epidural anesthesia pts
•Use w/caution in concomitant: NSAID, ASA, anti-platelet agents
•Use w/caution in impaired renal function

Vitamin K Antagonist
• Warfarin
• Extrinsic Pathway
• Suppresses Protein C/S, Factors II, VII, IX, X

Warfarin

Warfarin
• FDA indications:
• Prophylaxis and treatment of thromboembolic disorders (eg, venous, pulmonary) and embolic complications arising from atrial fibrillation or cardiac valve replacement
• Adjunct to reduce risk of systemic embolism (eg, recurrent MI, stroke) after myocardial infarction

Warfarin Pros and Cons
• Pros • Tried and true medication • Well studied and understood • Fully reversible w/life
threatening bleeding (Vitamin K)
• Only anticoagulant available for pts w/CrCl <30
• Only approved anticoagulant for long-term AC for mechanical valves
• Lab testing that has therapeutic level (INR)
• Cons • Need for monitoring/frequent
lab draws • Multiple med interactions • Diet interactions • Even in clinical trials INRs
within target range 36%-68% of time
• In acute VTE must bridge w/parental agent IV UF heparin, LMWH, Fondaparinux for minimum 5 days and INR>2 for 24 hours

2012 CHEST guidelines
• 3.3.1 In patients with DVT of the leg and no cancer, we suggest VKA therapy over LMWH for long-term therapy (Grade 2C)
• For patients with DVT and no cancer who are not treated with VKA therapy, we suggest LMWH over dabigatran or rivaroxaban for long-term therapy (Grade 2C) .
• 3.3.2. In patients with DVT of the leg and cancer, we suggest LMWH over VKA therapy (Grade 2B) .
• In patients with DVT and cancer who are not treated with LMWH, we suggest VKA over dabigatran or rivaroxaban for long-term therapy (Grade 2B) .

2012 CHEST Guidelines
• Remarks (3.3.1-3.3.2): Choice of treatment in patients with and without cancer is sensitive to the individual patient’s tolerance for daily injections, need for laboratory monitoring, and treatment costs.
• Treatment of VTE with dabigatran or rivaroxaban, in addition to being less burdensome to patients, may prove to be associated with better clinical outcomes than VKA and LMWH therapy.
• When these guidelines were being prepared (October 2011), post marketing studies of safety were not available. Given the paucity of currently available data and that new data are rapidly emerging, we give a weak recommendation in favor of VKA and LMWH therapy over dabigatran and rivaroxaban, and we have not made any recommendations in favor of one of the new agents over the other.

NOACs the unknown..
• Effective in malignancy patients?
• Hypercoaguable states (i.e. lupus anticoagulant) ?
• Arterial thrombosis?
• Mechanical valves?
• Heparin induced thrombocytopenia?
• Pregnant patients?
• Still w/short term clinical experience in NOACs
• FDA approval for VTE:
• Rivaroxaban approved in 11/2012
• Dabigatran 4/2014
• Apixaban 8/2014
Warfarin is not going away
• Only option:
• Dialysis patients
• Mechanical valves
• borderline renal functions
• High risk bleeding pts (fully reversible)

Case Study 1.
• 35 y/o female presents to internal medicine clinic w/left calf pain and tightness. Has recent history of ankle fracture 4 weeks ago and in a cast. No plans for surgery
• Duplex US positive for L popliteal/gastroc DVT
• Hgb 11.9
• Platelets 216,000
• Creatinine 0.70
• PT/INR 0.9

What would you do? #1
• 1. LMWH to warfarin
• 2. Fondaparinux to warfarin
• 3. LMWH/Fondaparinux x5-10 days then Dabigatran
• 4. Apixaban
• 5. Rivaroxaban
• Note female reproductive years must counsel on birth control methods

Case Study 2
• 56 y/o male w/Crohn’s disease s/p colectomy and end ileostomy. Post-op w/ shortness of breath and tachycardia and found to have R lobar PE and B/L subsegmental PE
• Duplex positive for L femoral DVT
• Consulted in the hospital for AC management
• Hgb 9.0
• Platelets 180,000
• Creatinine 1.2

What would you do? #2
• 1. Heparin to warfarin
• 2. LMWH/Fondaparinux to warfarin
• 3. LMWH/Fondaparinux x5-10 days then Dabigatran
• 4. Apixaban
• 5. Rivaroxaban

Case Study 3
• 55 y/o female history of DVT in the past x3. First after pregnancy, received 6 months of warfarin. 2nd after knee replacement surgery 10 years later, received 3 months of warfarin. 3rd after gallbladder surgery (overnight hospital stay) and told she should be on “life long Coumadin”
• Seen in Vascular Medicine Clinic.
• Inquiring about “these new medications I keep seeing on TV instead of warfarin”
• Hgb 10.9
• Platelets 175,000
• Creatinine 0.89

What would you do? #3
• 1. Continue warfarin
• 2. LMWH/Fondaparinux monotherapy
• 3. LMWH/Fondaparinux x5-10 days then Dabigatran
• 4. Apixaban
• 5. Rivaroxaban

Case Study 4
• 65 y/o male presents to the ER w/swollen left leg and duplex US reveals L external iliac/common femoral/femoral/popliteal DVT R gastroc/PT DVT.
• Pt recently diagnosed w/non-small cell lung adenocarcinoma and is undergoing chemotherapy
• Admitted to hospital for further work-up.
• Vascular medicine consulted
• Hgb 8.7
• Platelets 156,000
• Creatinine 1.0

What would you do? #4
• 1. LMWH monotherapy
• LMWH to warfarin
• 2. Fondaparinux to warfarin
• 3. LMWH/Fondaparinux x5-10 days then Dabigatran
• 4. Apixaban
• 5. Rivaroxaban

Alteplase
• Thrombolytic
• FDA approved: STEMI, massive PE, acute stroke, CVC catheter clearance (low dose),
• Unlabeled use: peripheral arterial occlusion, Complicated parapneumonic effusion, prosthetic valve thrombosis

Alteplase Pharmacologic Profile
• Duration: >50% present in plasma cleared ~5 minutes after infusion terminated, ~80% cleared within 10 minutes; fibrinolytic activity persists for up to 1 hour after infusion terminated (Semba, 2000)
• Excretion: Clearance (in patients with acute MI receiving accelerated regimen): Rapidly from circulating plasma (572 ± 132 mL/minute) (Tanswell, 1992), primarily hepatic; >50% present in plasma is cleared within 5 minutes after the infusion is terminated, ~80% cleared within 10 minutes (Semba, 2000)

TPA in massive PE
• 100 mg over 2 hours; may be administered as a 10 mg bolus followed by 90 mg over 2 hours
• Heparin gtt to be started post thrombolysis as per orders by medical team and pharmacy

What constitutes high risk or massive PE?
• PE leading to cardiogenic shock: SBP <90 for at least 15 minutes and or need for vasopressors PLUS end-organ dysfunction or
• PE that causes cardio-respiratory arrest or
• PE that causes respiratory failure requiring mechanical ventilation or
• A pressure drop of >40 mmHg for greater than 15 minutes not due to sepsis or hypovolemia

2012 CHEST Guidelines for TPA in PE
• 5.6.1.1. In patients with acute PE associated with hypotension (eg, systolic BP , 90 mm Hg)who do not have a high bleeding risk, we suggest systemically administered thrombolytic therapy over no such therapy (Grade 2C) .
• 5.6.1.2. In most patients with acute PE not associated with hypotension, we recommend against systemically administered thrombolytic therapy (Grade 1C) .

Contraindications to thrombolytic therapy for DVT/PE
• Absolute contraindications:
• Prior intracranial hemorrhage
• Known structural cerebral vascular lesions
• Known malignant intracranial neoplasm
• Ischemic stroke within 3 months (excluding stroke with 3 hours)
• Suspected aortic dissection
• Active bleeding or bleeding diathesis (excluding menses)
• Significant closed-head trauma or facial trauma within 3 months

Relative contraindications to thrombolytic therapy
• Hx of chronic, severe, poorly controlled HTN
• Severe uncontrolled HTN on presentation (SBP >180 mmHg or DBP >110 mmHg)
• Hx of ischemic stroke more than 3 months prior
• Traumatic or prolonged (>10 minutes) CPR
• Major surgery <3 weeks • Recent (within 2-4 weeks)
internal bleeding • Recent LP puncture within 1
week
• Non compressible vascular punctures
• Recent invasive procedure • Pregnancy • Active peptic ulcer • Pericarditis or pericardial fluid • Current use of anticoagulant • Recent GI or GU bleed • Age >75 years • Diabetic retinopathy

What are we allowed to prescribe?

OHIO APN prescribing

Ohio APN formulary continued

Happy APN week!!!
Cure sometimes, treat often, comfort always.
--------- Hippocrates

Questions???