Embed Size (px)
Citation preview
Endovascular Neurointervention
in Cerebral Ischemia
Beyond Thrombolytics
Curtis A. Given II, MD
Co-Director, Neurointerventional Services
Baptist Physician Lexington
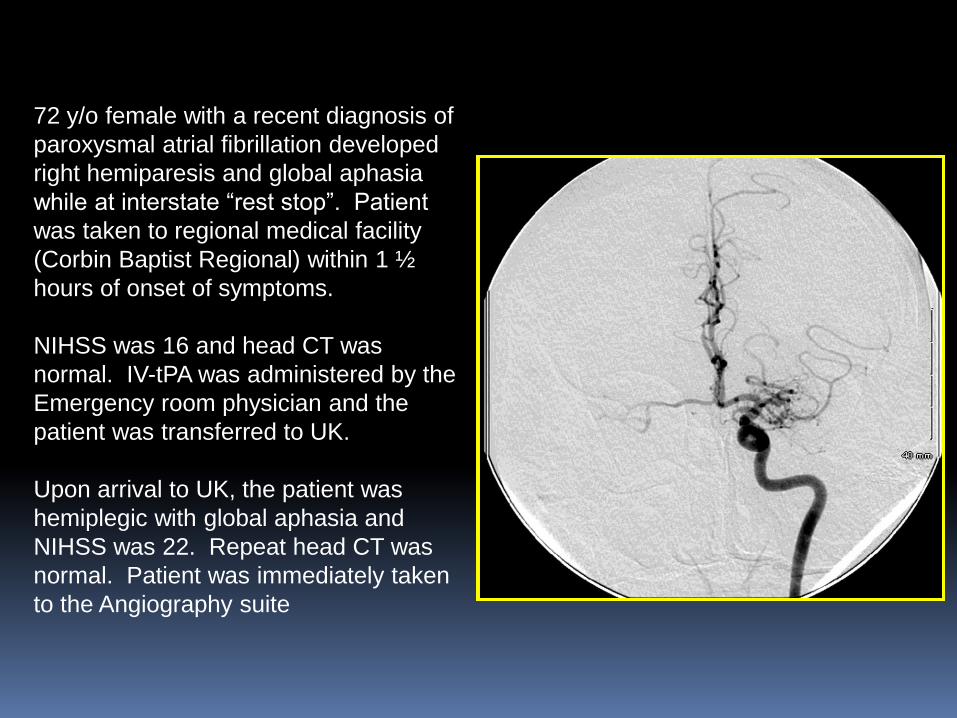
72 y/o female with a recent diagnosis of
paroxysmal atrial fibrillation developed
right hemiparesis and global aphasia
while at interstate “rest stop”. Patient
was taken to regional medical facility
(Corbin Baptist Regional) within 1 ½
hours of onset of symptoms.
NIHSS was 16 and head CT was
normal. IV-tPA was administered by the
Emergency room physician and the
patient was transferred to UK.
Upon arrival to UK, the patient was
hemiplegic with global aphasia and
NIHSS was 22. Repeat head CT was
normal. Patient was immediately taken
to the Angiography suite
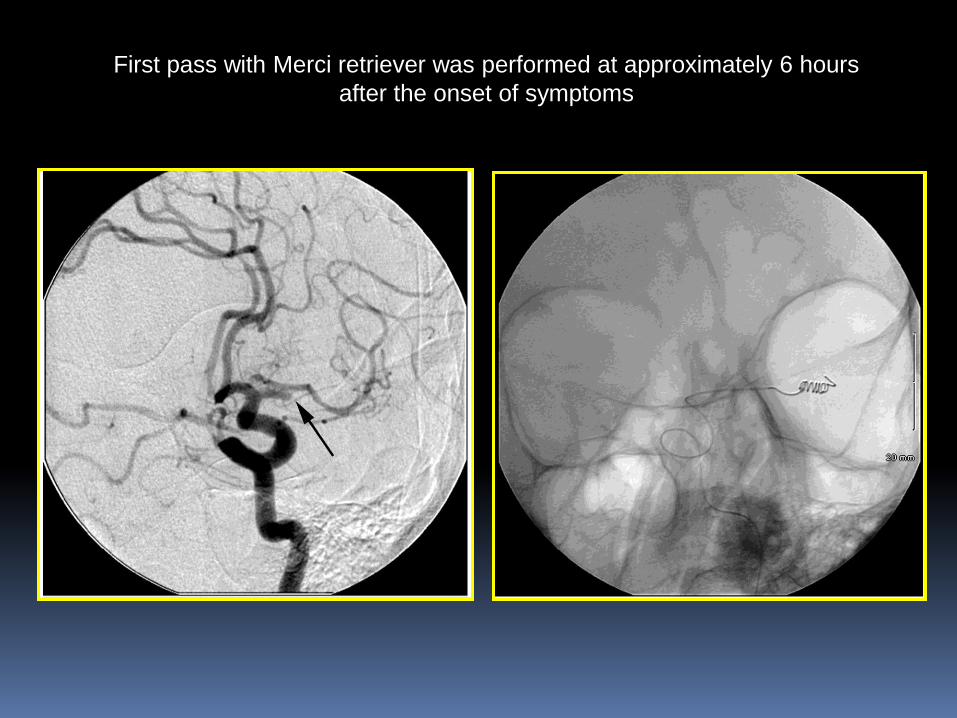
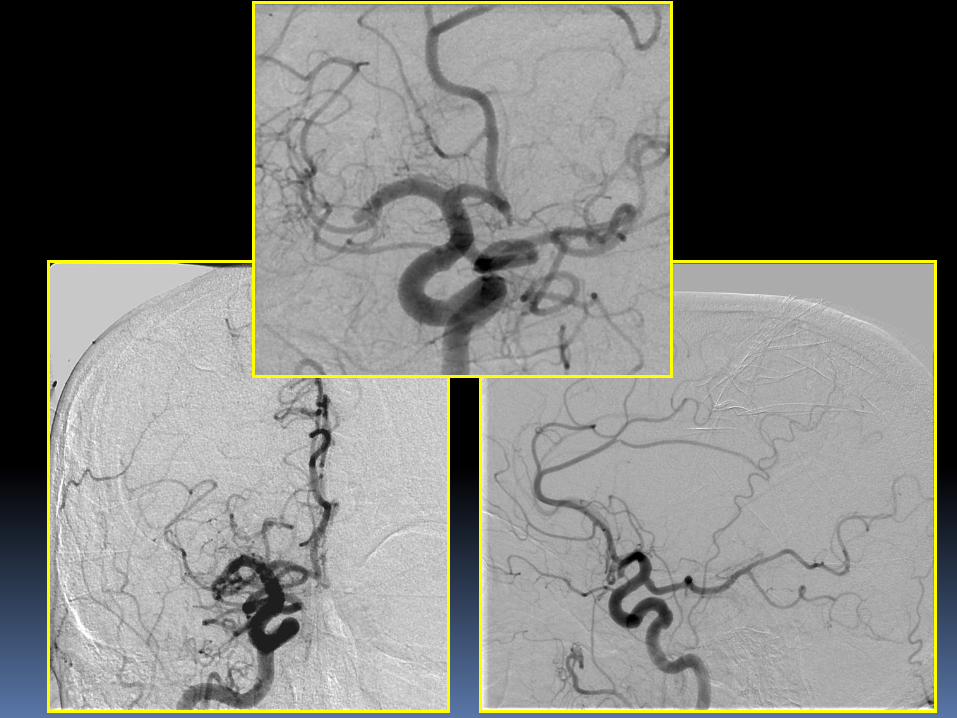
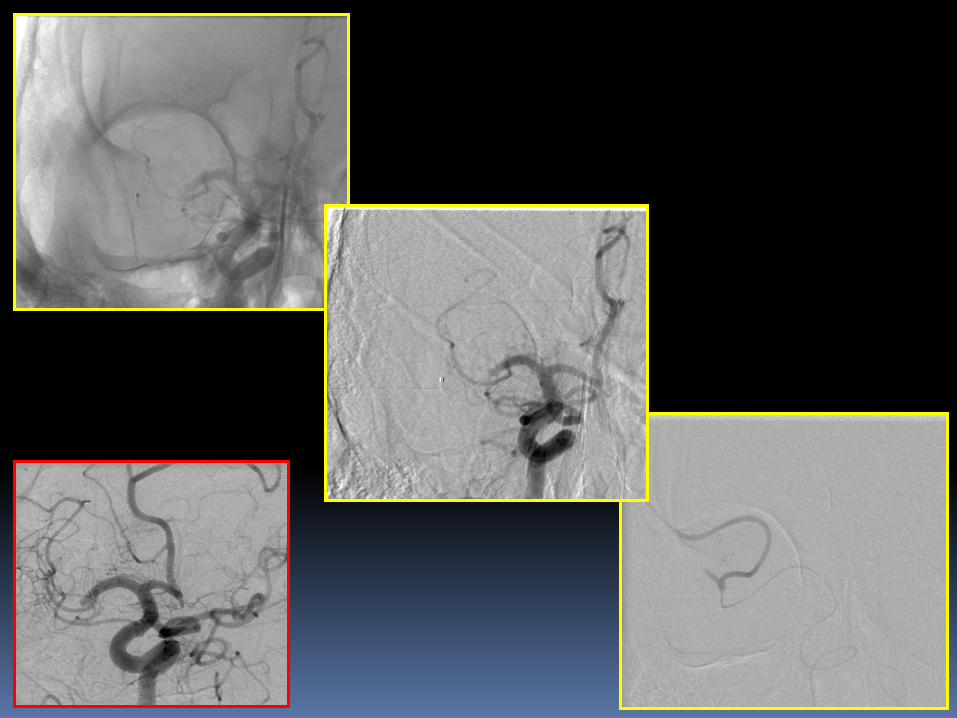
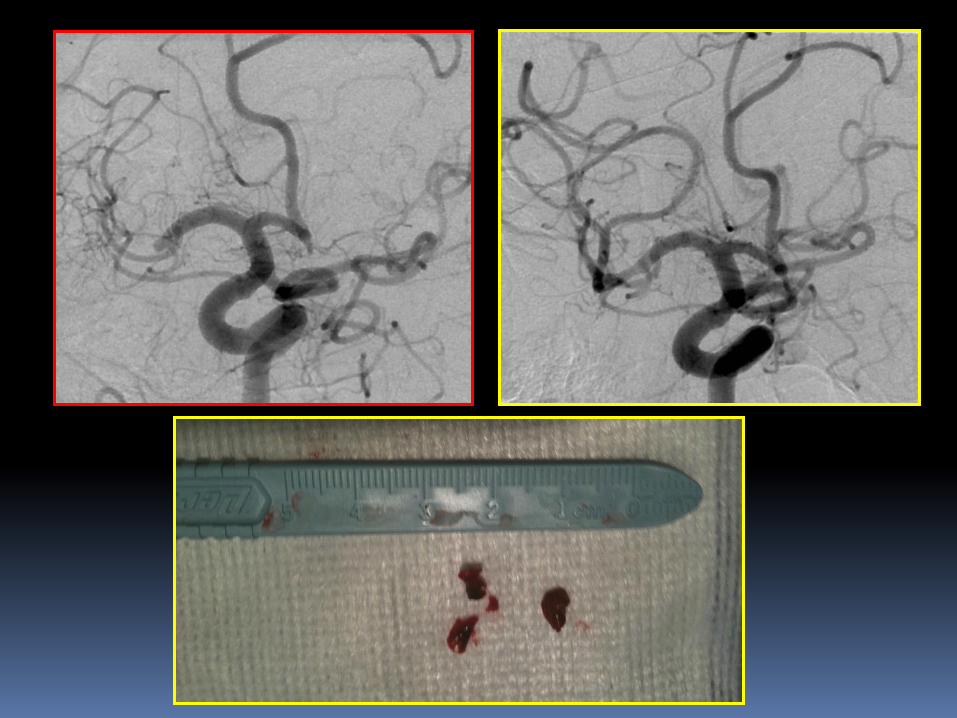
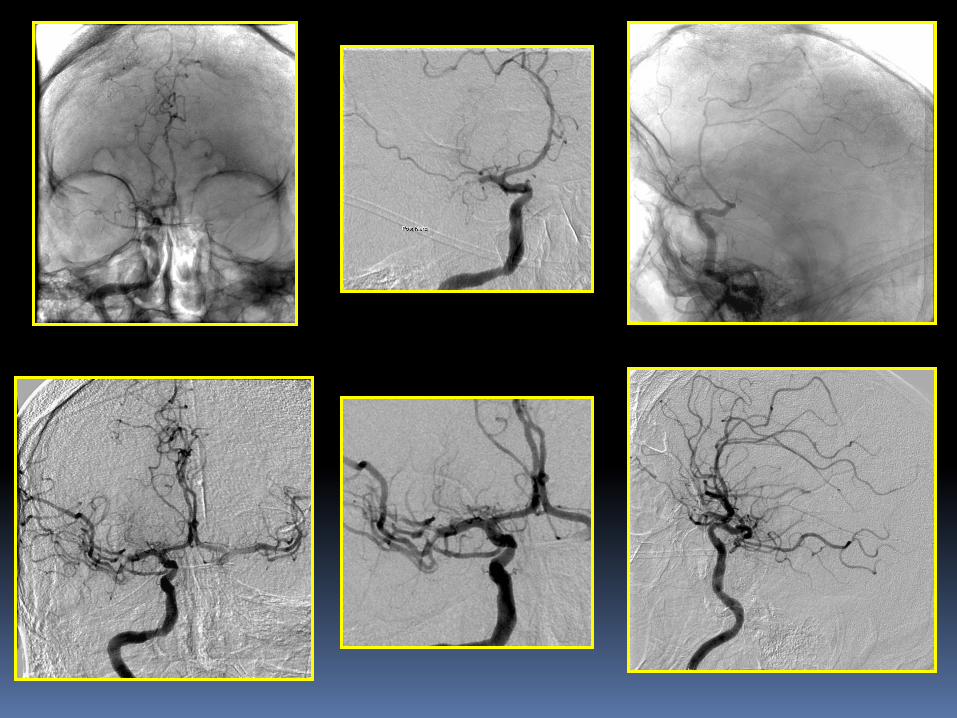
First pass with Merci retriever was performed at approximately 6 hours
after the onset of symptoms
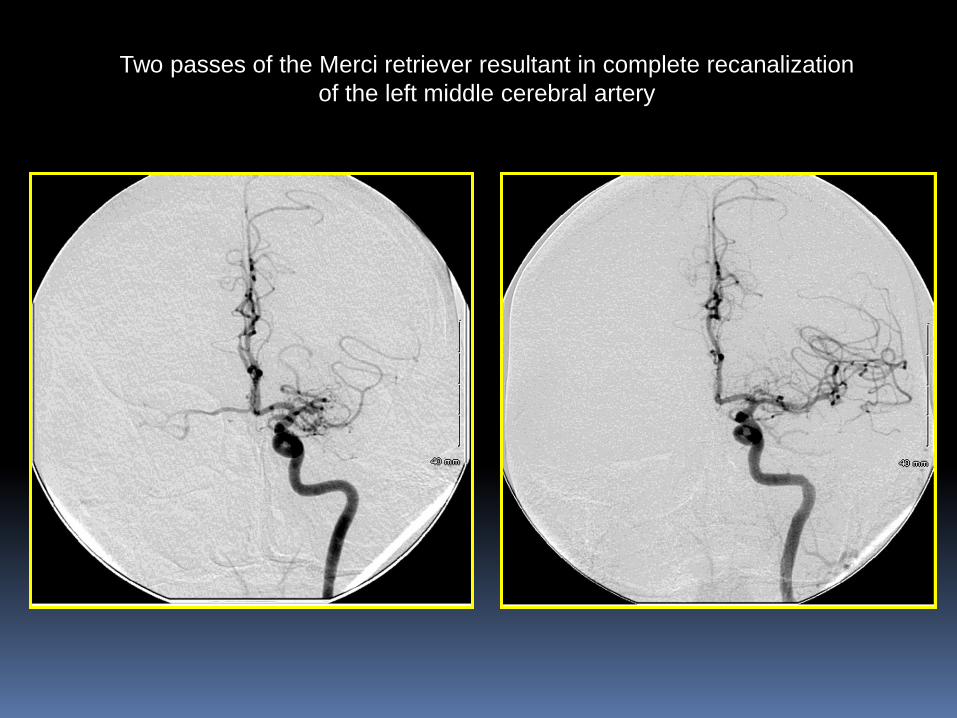
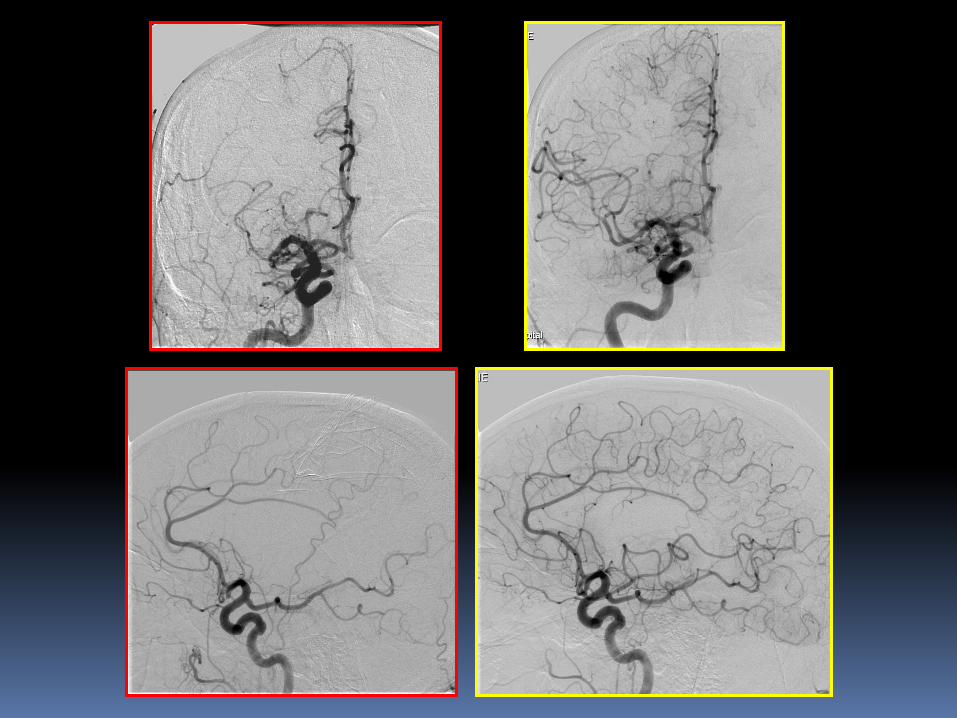
Two passes of the Merci retriever resultant in complete recanalization
of the left middle cerebral artery
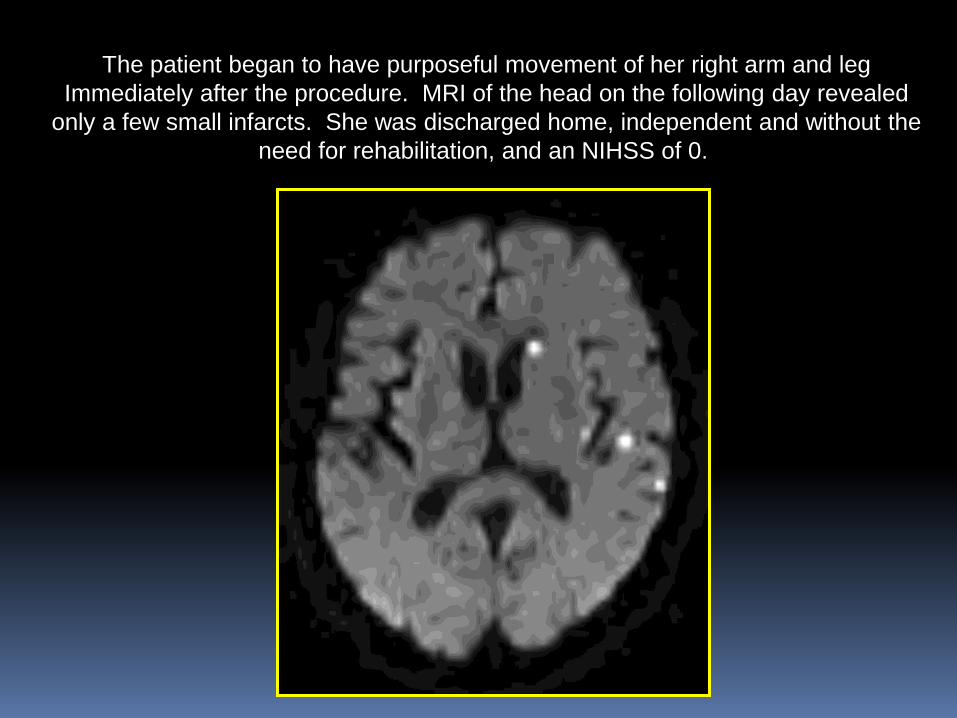
The patient began to have purposeful movement of her right arm and leg
Immediately after the procedure. MRI of the head on the following day revealed
only a few small infarcts. She was discharged home, independent and without the
need for rehabilitation, and an NIHSS of 0.
Stroke • Impact
– Every 45 seconds someone in the U.S. has a stroke
– Stroke is #3 cause of death
– Stroke is #1 cause of adult disability
– Approximately 87% ischemic
• Limited treatment options
– Intravenous lytic
• Limitation: must be administered within 3 hours of stroke
onset
• Estimated <5% of stroke patients receive IV lytic
– Mechanical revascularization with Merci® and Penumbra ®
Retrieval Systems
• Option beyond 3 hour window, and for patients who are
ineligible for or who fail IV t-PA therapy
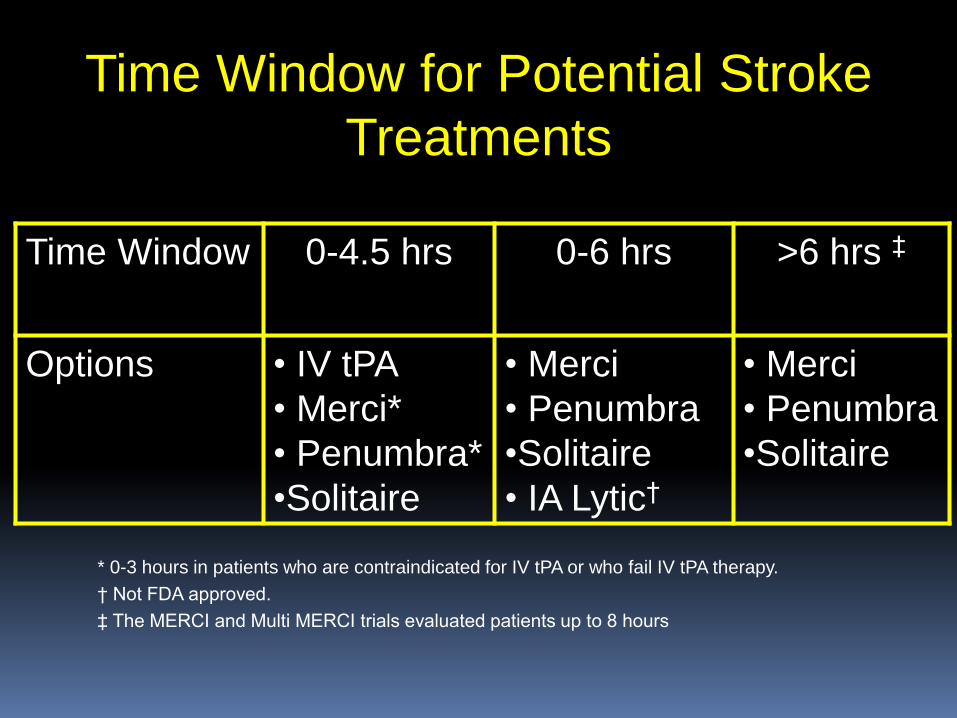
Time Window for Potential Stroke
Treatments
Time Window 0-4.5 hrs 0-6 hrs >6 hrs ‡
Options • IV tPA
• Merci*
• Penumbra*
•Solitaire
• Merci
• Penumbra
•Solitaire
• IA Lytic†
• Merci
• Penumbra
•Solitaire
* 0-3 hours in patients who are contraindicated for IV tPA or who fail IV tPA therapy.
† Not FDA approved.
‡ The MERCI and Multi MERCI trials evaluated patients up to 8 hours

Patient Selection for Intra-arterial Therapy
Generally patients with symptoms of large
vessel occlusion (NIHSS > 8)
No changes of large infarct (less than 1/3 of vascular territory) on CT or DWI
No hemorrhage on CT
< 8 hours since “last seen normal” OR significant tissue “at-risk/penumbra” on Perfusion imaging
Any patient with basilar occlusion
Large vessel occlusion on CTA/MRA
Contraindications to IA Thrombolysis
• CT-documented hemorrhage or significant mass effect
• Fibrinogen < 120 mg*
• Platelet count < 80,000*
• Active internal bleeding or recent surgery (<10 days)*
• Prior allergic reaction to r-tPA*
• BP > 200 systolic or >120 diastolic despite medical therapy
• No clot on angiography
* Not contraindication to mechanical thrombectomy
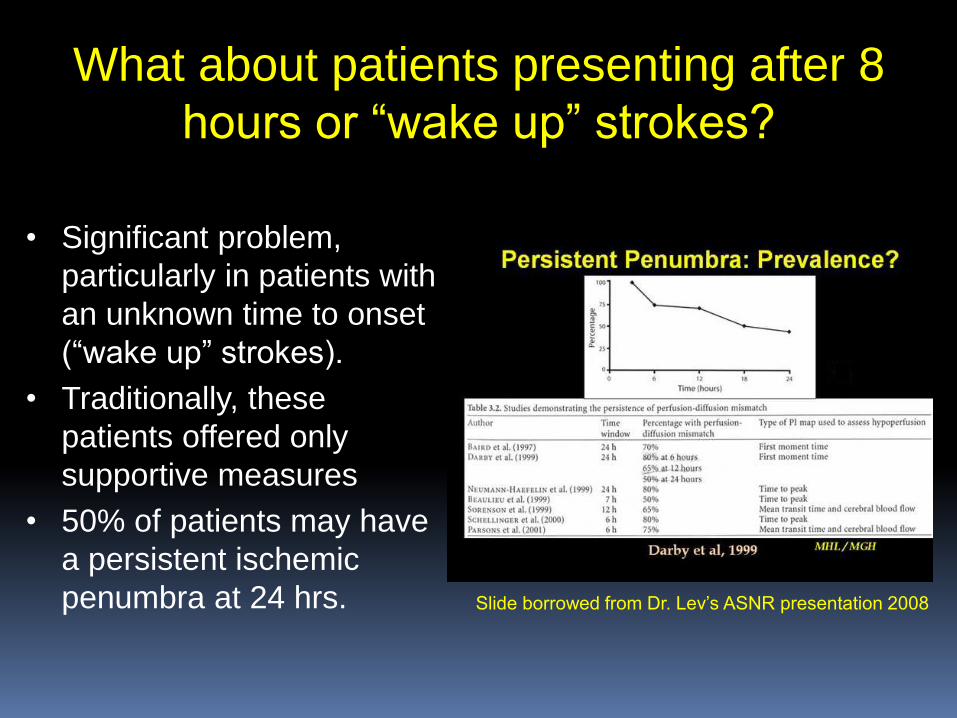
What about patients presenting after 8
hours or “wake up” strokes?
• Significant problem,
particularly in patients with
an unknown time to onset
(“wake up” strokes).
• Traditionally, these
patients offered only
supportive measures
• 50% of patients may have
a persistent ischemic
penumbra at 24 hrs.
Slide borrowed from Dr. Lev’s ASNR presentation 2008
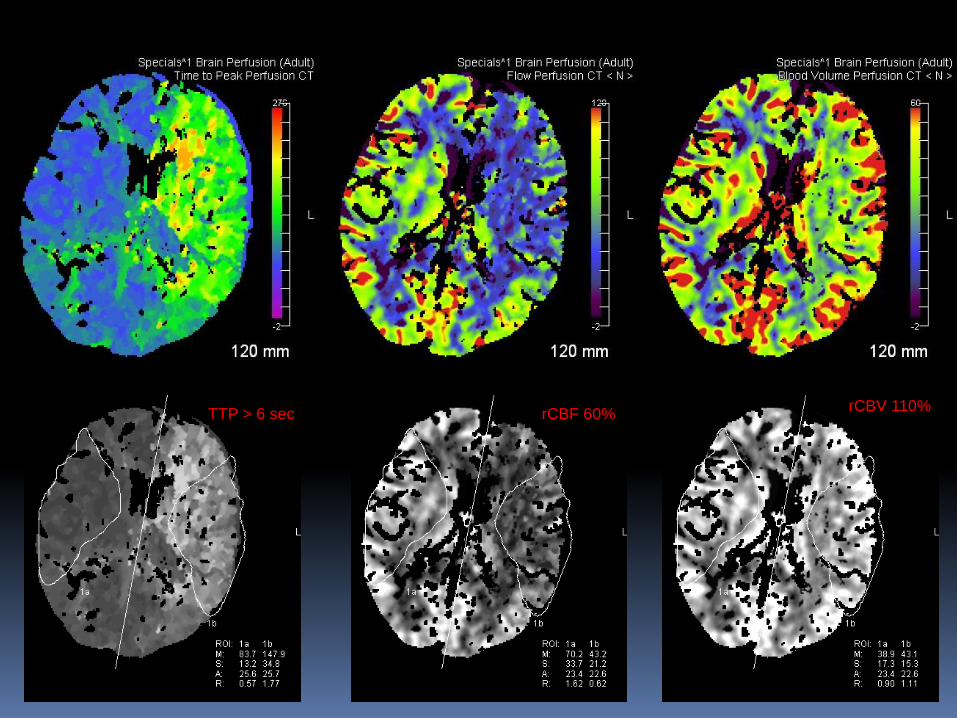
rCBF 60% rCBV 110%
TTP > 6 sec
Trials of Intra-arterial Thrombolytic Agents
PROACT II Furlan A. et al. JAMA 282:2003, 1999
• Randomized open-label trial of prourokinase (r-pro-UK) 9 mg
with heparin vs systemic heparin in patients with middle
cerebral artery occlusions within 6 hours of onset.
• Pro-urokinase delivered over 2 hours by microcatheter into
the middle cerebral artery at the face of the clot.
• Mechanical clot disruption was not permitted.
• Final angiogram at 2 hours in both groups.
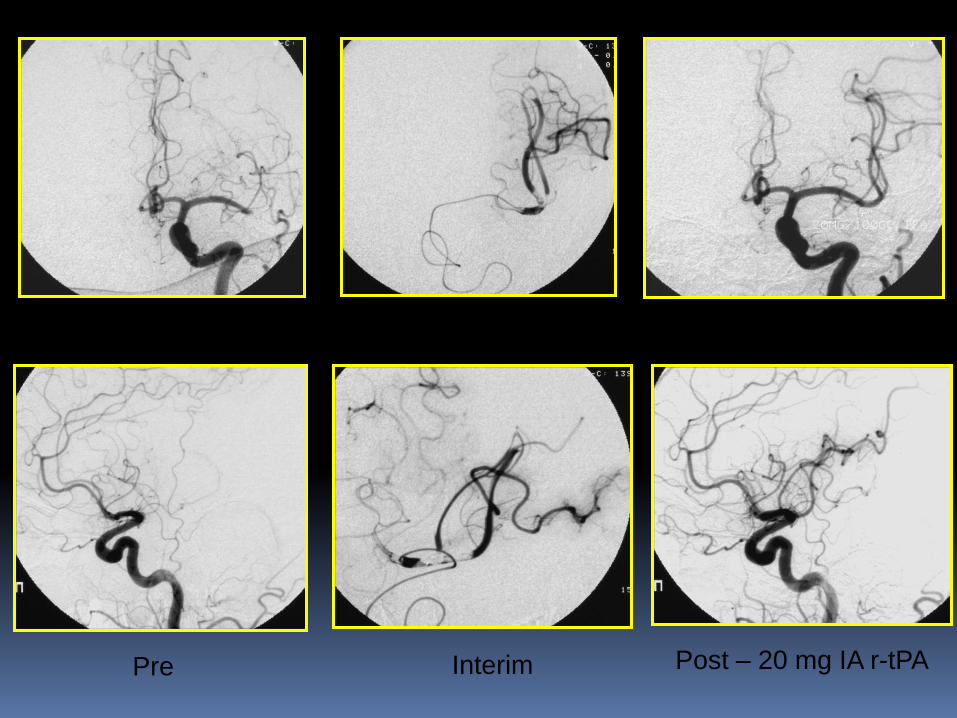
Pre Post – 20 mg IA r-tPA Interim
Endovascular Thrombectomy of Cerebral Vessels
• Merci Retriever
• First surgical device
cleared by the FDA for acute
ischemic stroke patients
• Restores blood flow to the
brain by physically removing
thrombus from the occluded
precerebral or cerebral
vessel
Candidates for Merci Therapy
• Patients who are ineligible for treatment with intravenous tPA :
– outside 3-4.5 hour window
– other clinical factors, eg. recent surgery,
long-term current use of anticoagulants for atrial
fibrillation, allergy to t-PA
• Patients who have failed (or not responding to) prior
intravenous t-PA therapy
Only used for patients with ischemic stroke, not hemorrhagic stroke
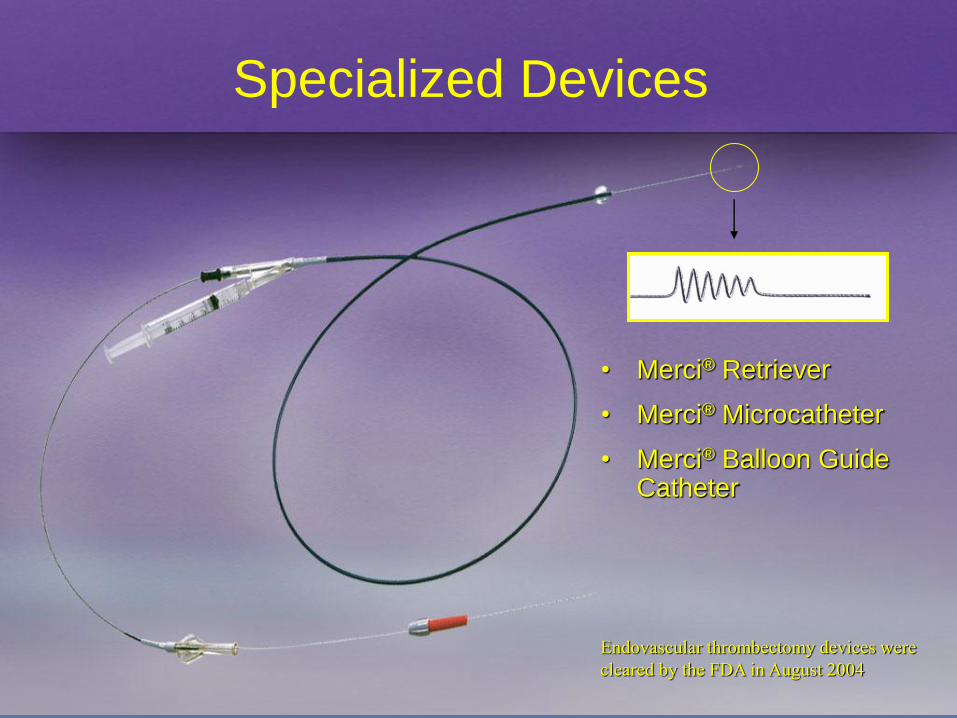
Specialized Devices
• Merci® Retriever
• Merci® Microcatheter
• Merci® Balloon Guide Catheter
Endovascular thrombectomy devices were
cleared by the FDA in August 2004


Merci Registry Background
The Merci Registry is a Post-Market study
designed to capture “real-world”
interventional treatment of acute stroke with
the Merci Retriever system, unconstrained
from the “trial” environment
The Largest, Prospective Multi-Center Study of
Mechanical Embolectomy for AIS
• Prospective, multi-center study (36 centers)
• 1,000 patients enrolled in 3 years
– Interim results presented at ISC 2010 analyzed 625 patients
• Inclusion criteria: procedure must have included a Merci
Retriever and patient informed consent
• No exclusion criteria
• Interim results validated MERCI and Multi MERCI results
in a much larger unconstrained cohort
Merci Registry
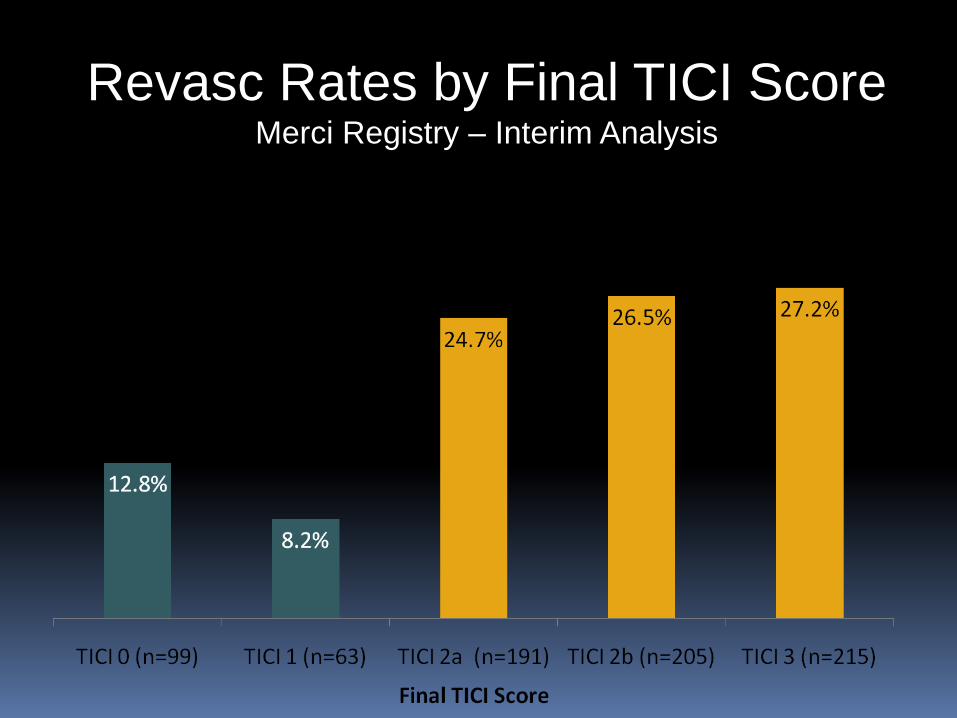
Revasc Rates by Final TICI Score Merci Registry – Interim Analysis
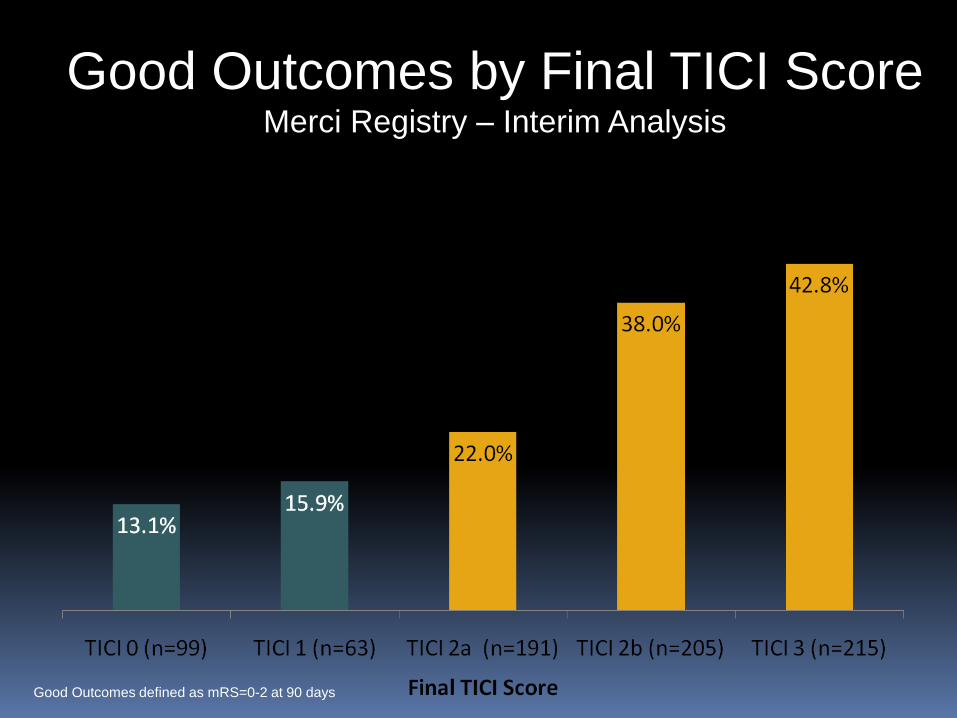
Good Outcomes by Final TICI Score Merci Registry – Interim Analysis
Good Outcomes defined as mRS=0-2 at 90 days
The Penumbra System is designed to revascularize
large vessel occlusions in the intracranial circulation. The
Penumbra System uses a unique microcatheter and
SeparatorTM based thrombus debulking approach to
intracranial vessel revascularization.
The Penumbra advantages are:
•Proximal working position
•Continuous Aspiration
•Variable sizing for variable anatomy
Penumbra Thrombectomy System
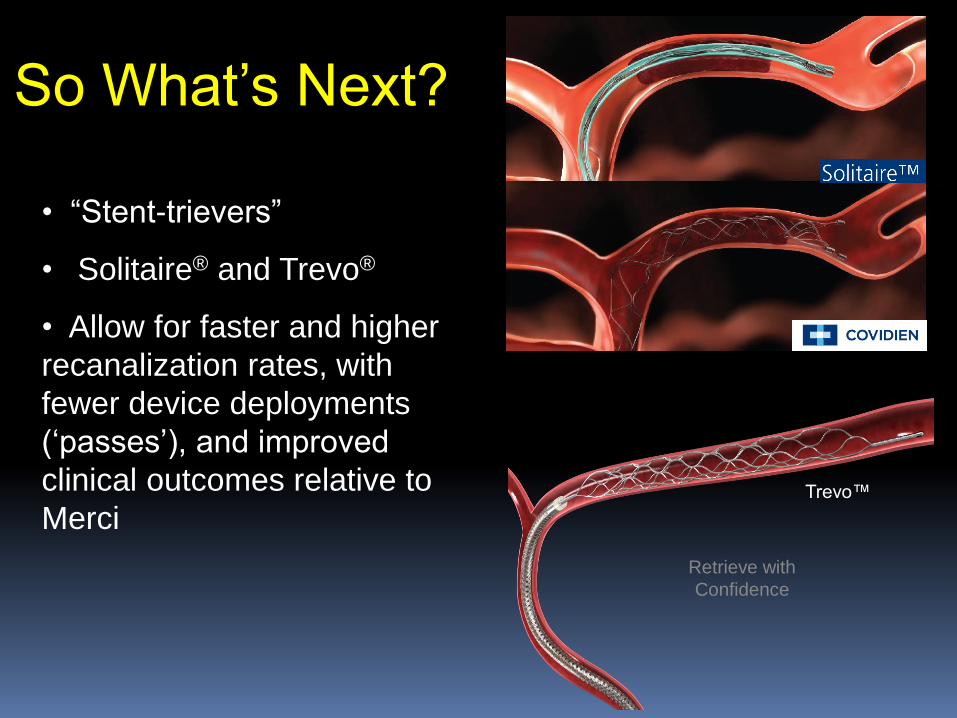
So What’s Next?
• “Stent-trievers”
• Solitaire® and Trevo®
• Allow for faster and higher
recanalization rates, with
fewer device deployments
(‘passes’), and improved
clinical outcomes relative to
Merci Trevo™
Retrieve with
Confidence
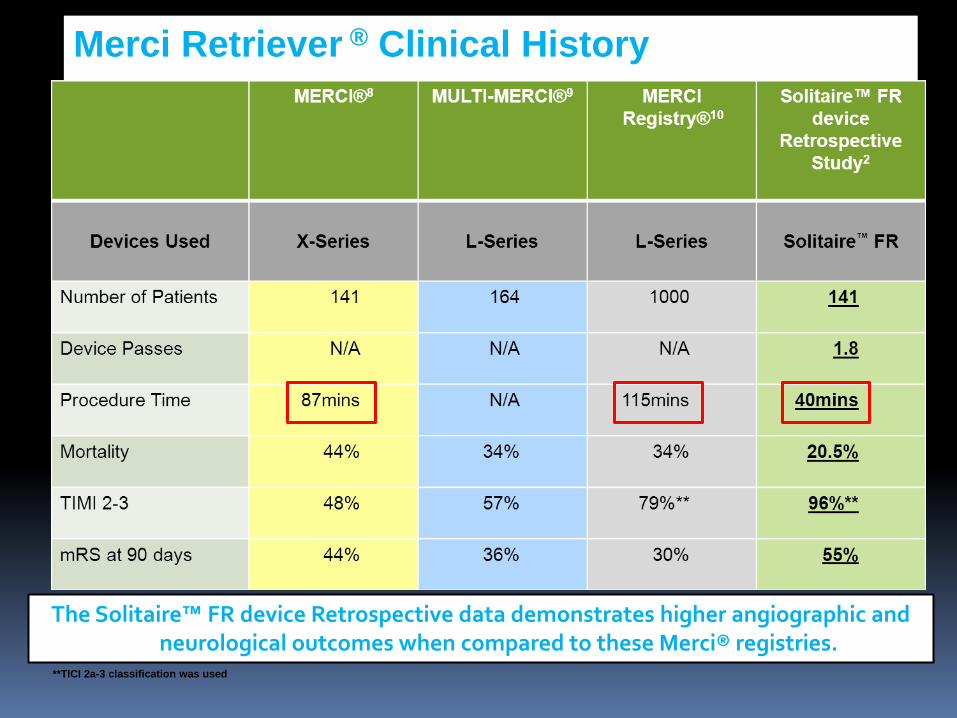
Merci Retriever ® Clinical History
The Solitaire™ FR device Retrospective data demonstrates higher angiographic and neurological outcomes when compared to these Merci® registries.
**TICI 2a-3 classification was used
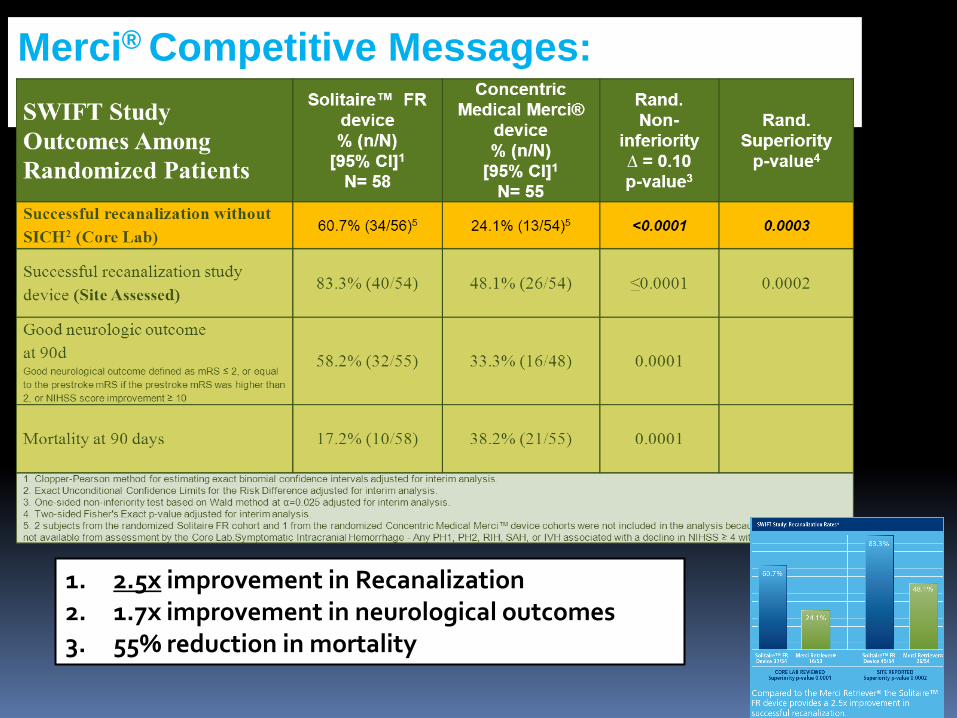
Merci® Competitive Messages:
1. 2.5x improvement in Recanalization 2. 1.7x improvement in neurological outcomes 3. 55% reduction in mortality
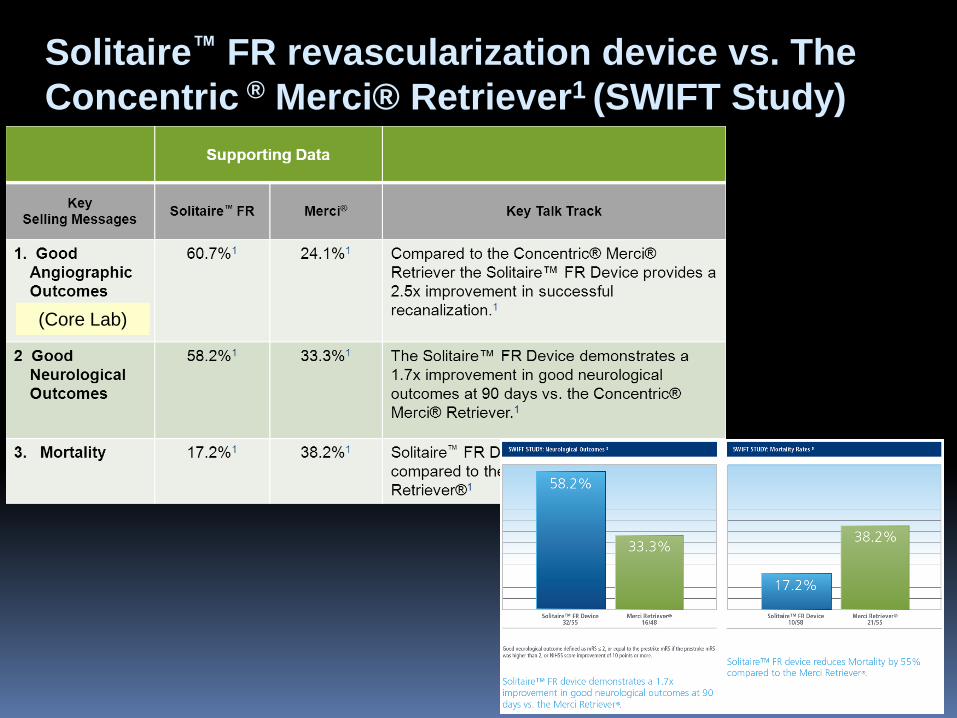
Solitaire™ FR revascularization device vs. The
Concentric ® Merci® Retriever1 (SWIFT Study)
(Core Lab)
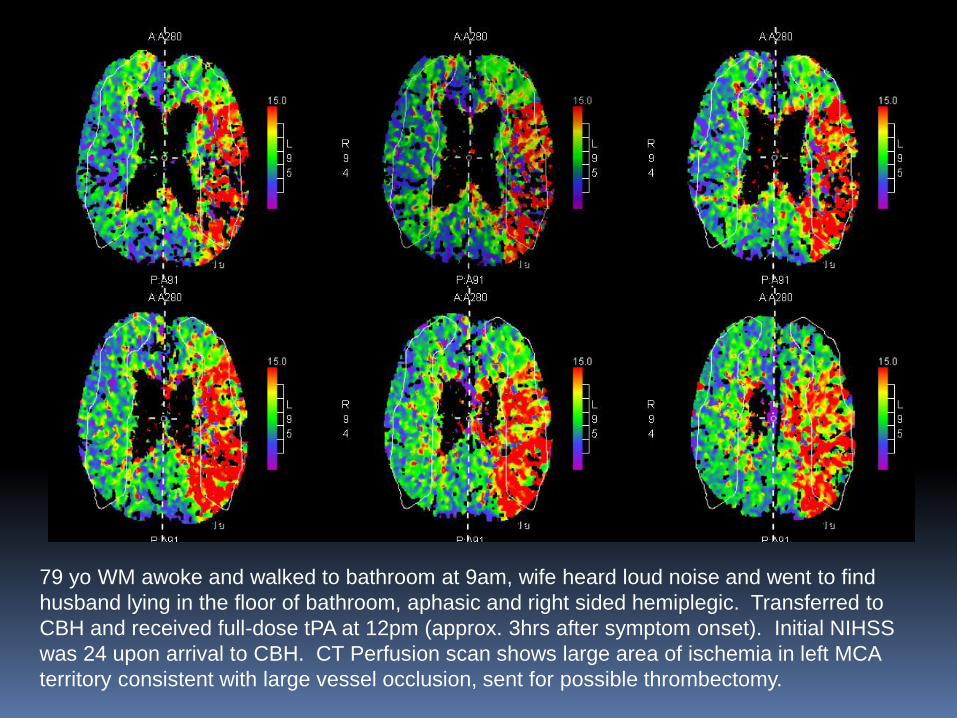
79 yo WM awoke and walked to bathroom at 9am, wife heard loud noise and went to find
husband lying in the floor of bathroom, aphasic and right sided hemiplegic. Transferred to
CBH and received full-dose tPA at 12pm (approx. 3hrs after symptom onset). Initial NIHSS
was 24 upon arrival to CBH. CT Perfusion scan shows large area of ischemia in left MCA
territory consistent with large vessel occlusion, sent for possible thrombectomy.
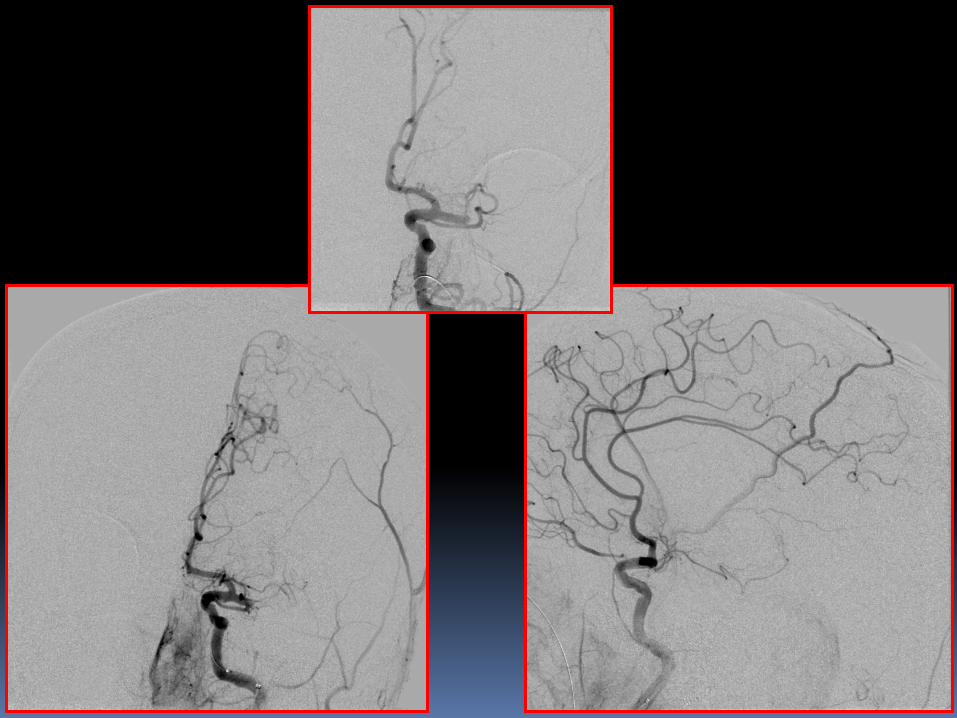
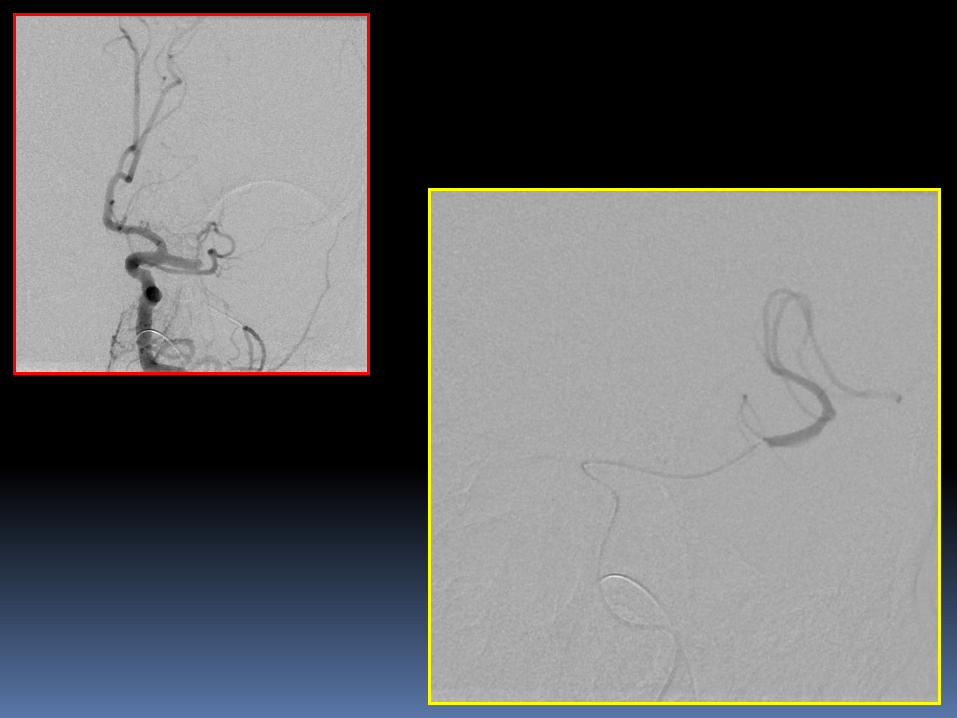

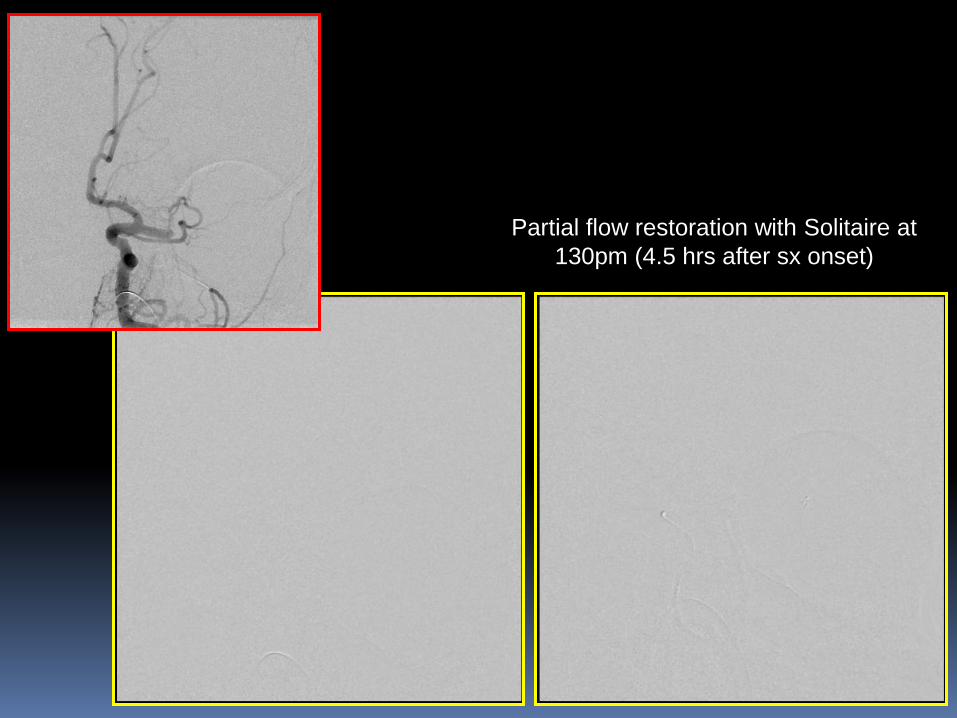
Partial flow restoration with Solitaire at
130pm (4.5 hrs after sx onset)

Two passes with 4x20mm Solitaire
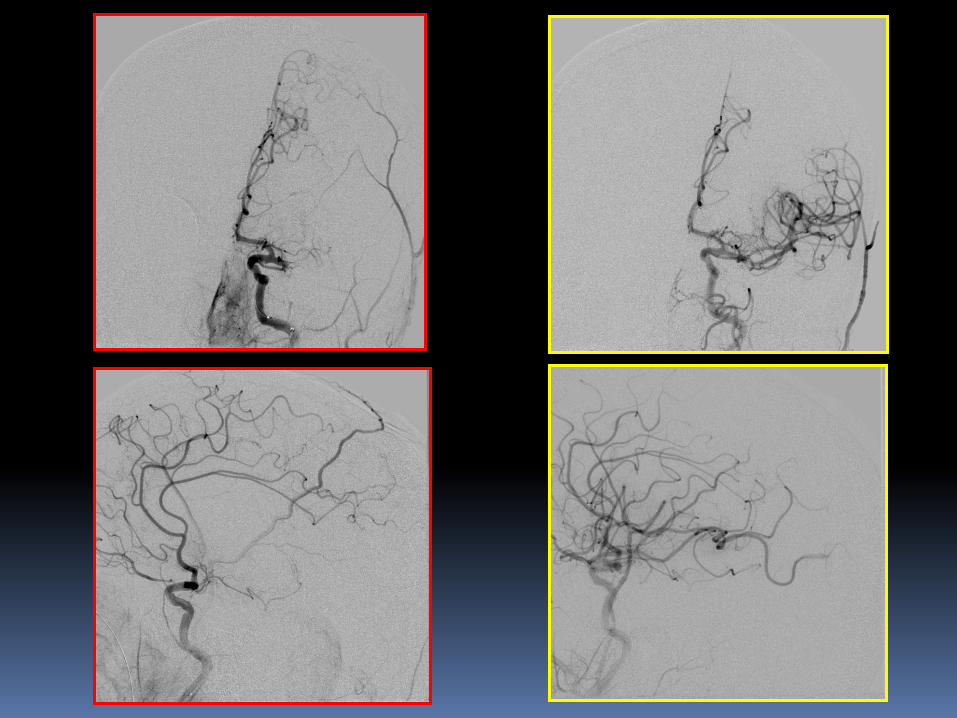

The next day, the patient had regained anti-gravity strength in the right upper and
lower extremities and significant improvement in speech (mild-moderate residual
expressive aphasia). 24 hr NIHSS had improved to 6 (initial was 24).
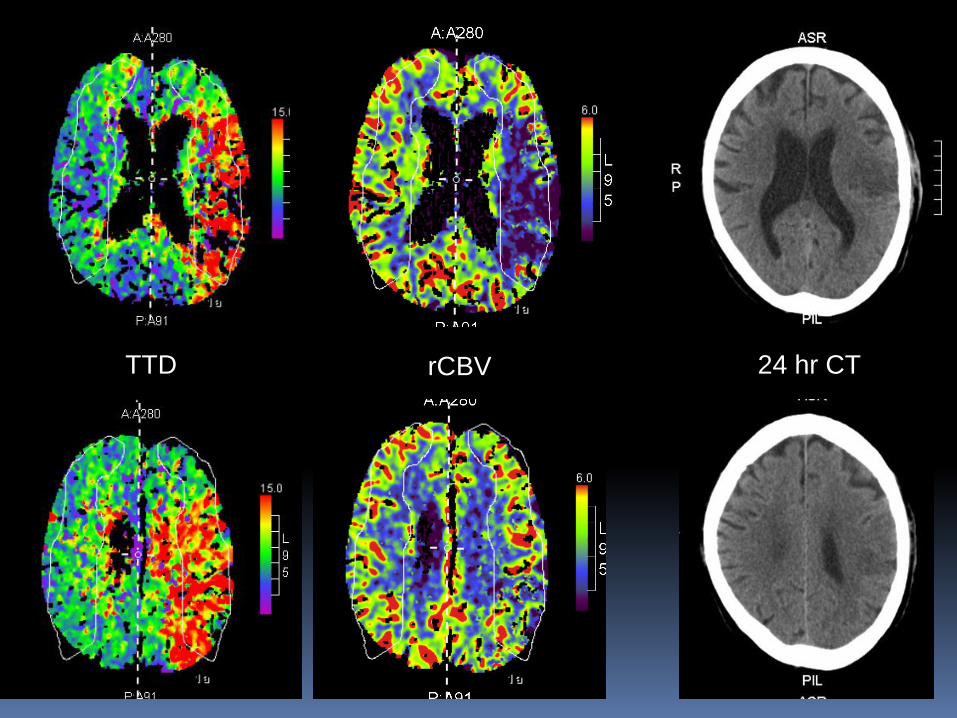
TTD rCBV 24 hr CT
TREVO 2 Thrombectomy REvascularization of large Vessel Occlusions
in acute ischemic stroke
Randomized, prospectively controlled, multi-center, non-inferiority IDE study of arterial revascularization in acute ischemic stroke patients
Up to 25 sites (at least 20 sites in North America) – 1st and only site in Kentucky
178 patients, with a planned interim analysis at 120
Randomized 1:1, with test arm using the Trevo device, the control arm using the Merci device

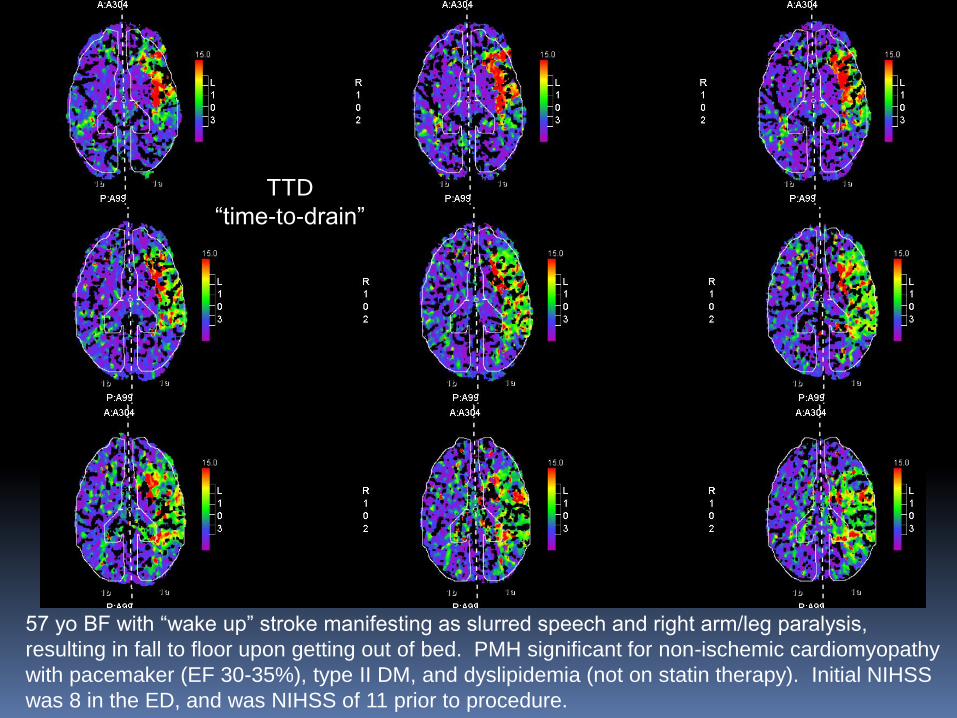
TTD
“time-to-drain”
TTD
“time-to-drain” TTD
“time-to-drain”
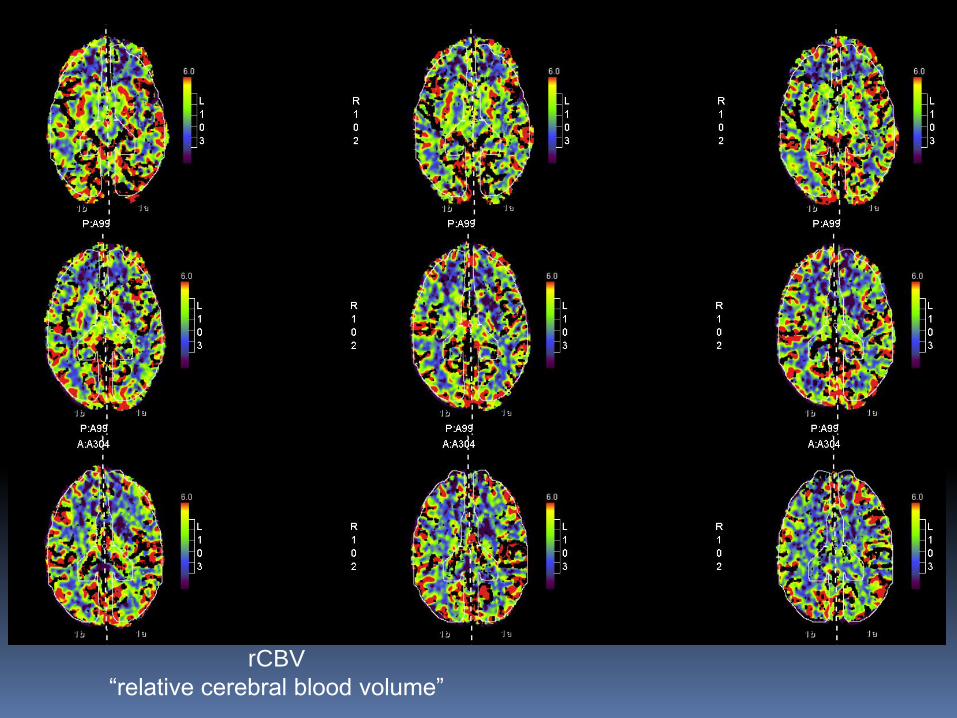
rCBV
“relative cerebral
blood volume”
rCBV
“relative cerebral
blood volume”
rCBV
“relative cerebral
blood volume”
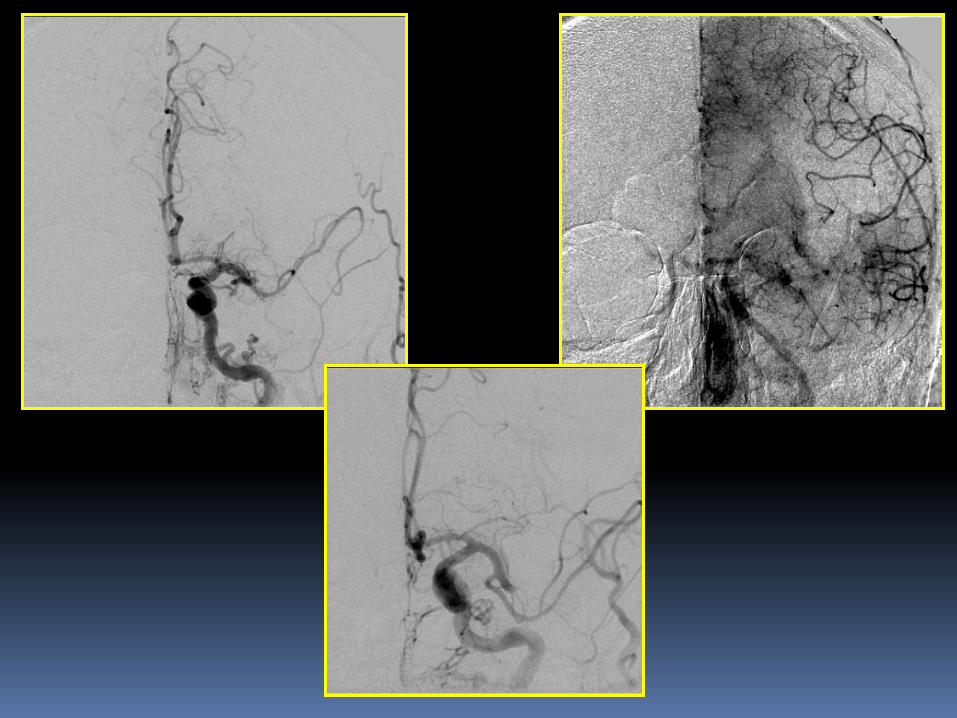
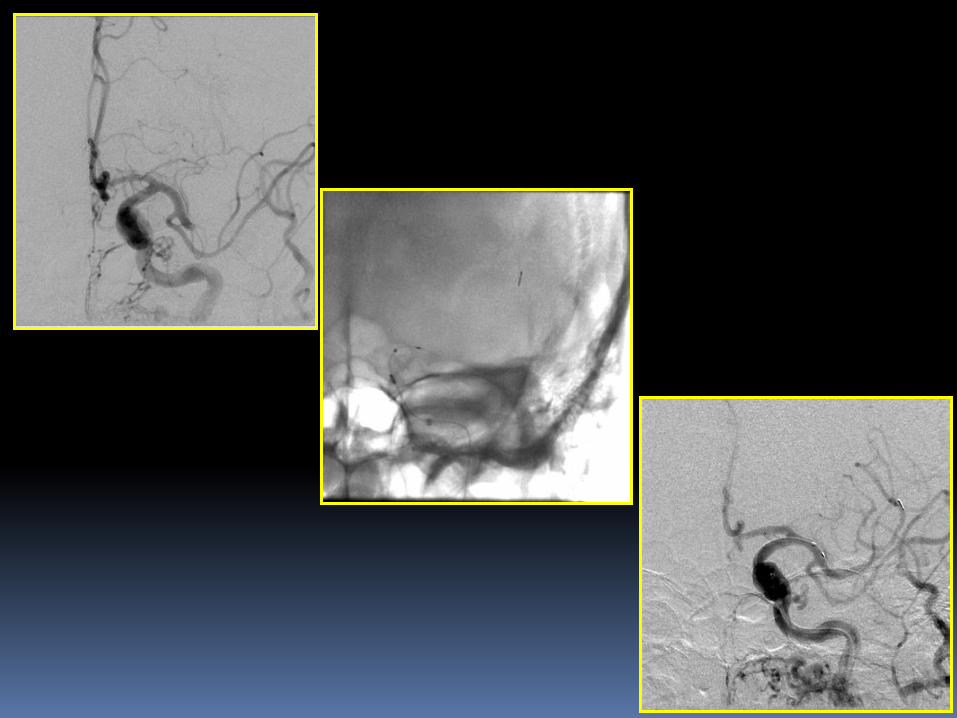
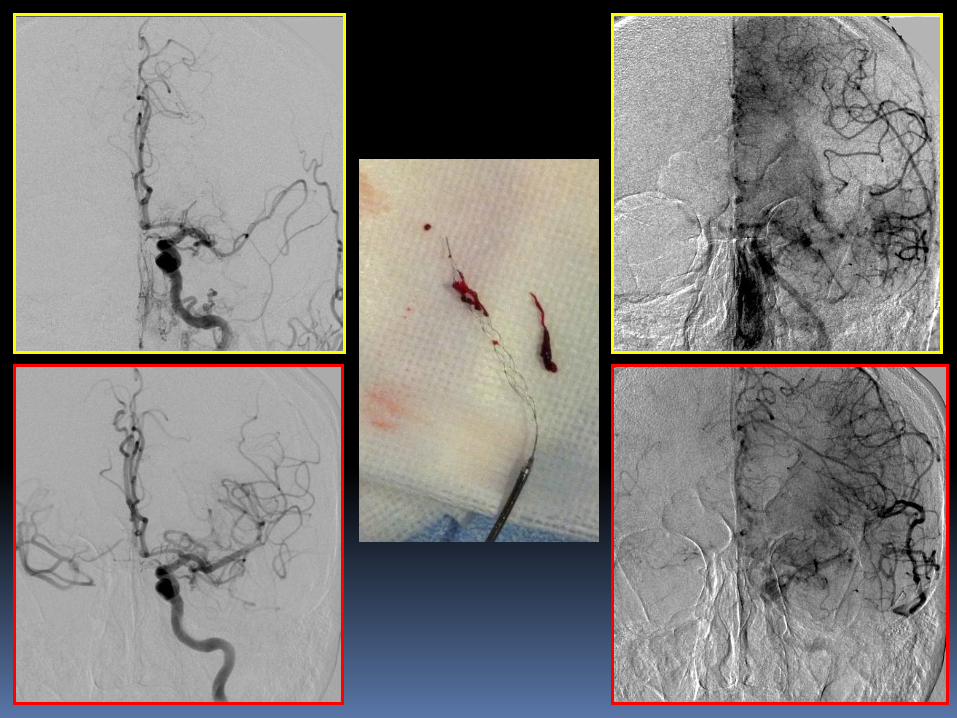
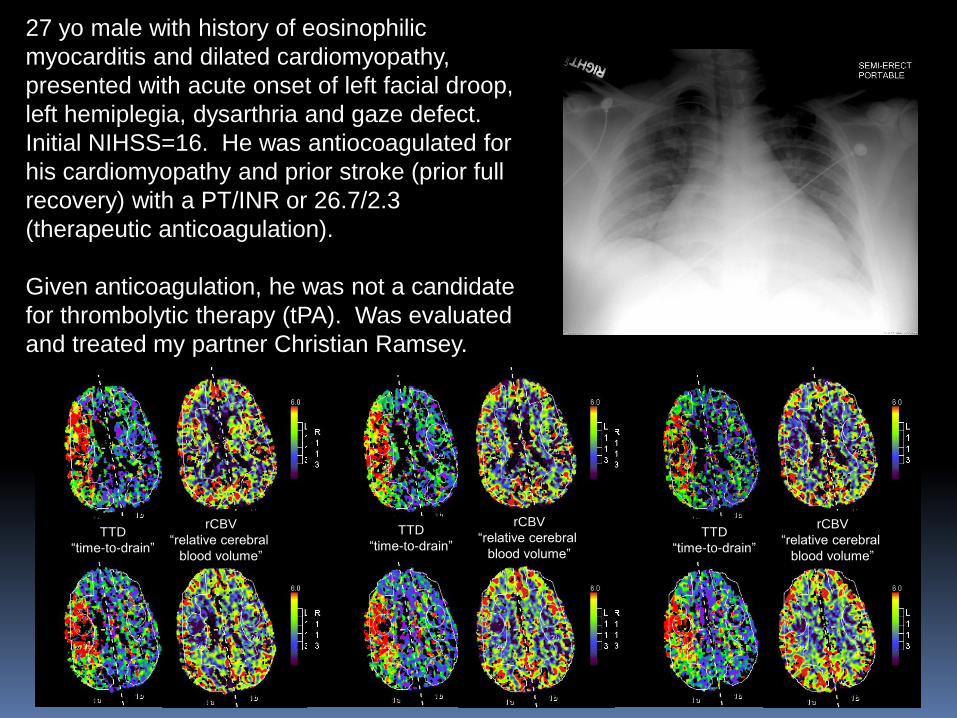
27 yo male with history of eosinophilic
myocarditis and dilated cardiomyopathy,
presented with acute onset of left facial droop,
left hemiplegia, dysarthria and gaze defect.
Initial NIHSS=16. He was antiocoagulated for
his cardiomyopathy and prior stroke (prior full
recovery) with a PT/INR or 26.7/2.3
(therapeutic anticoagulation).
Given anticoagulation, he was not a candidate
for thrombolytic therapy (tPA). Was evaluated
and treated my partner Christian Ramsey.
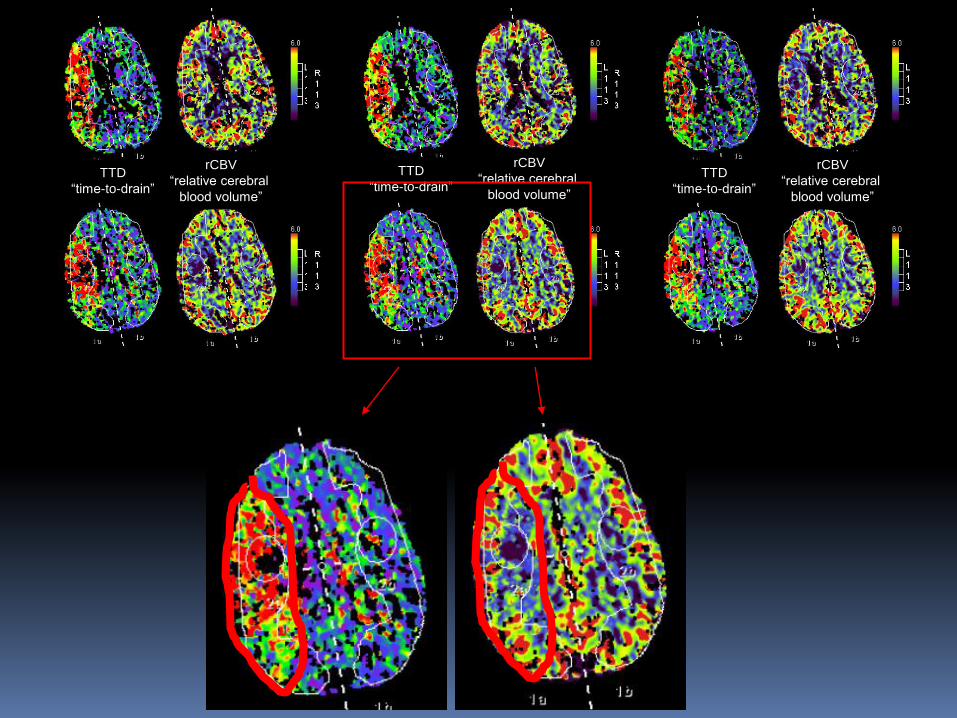
TTD
“time-to-drain”
TTD
“time-to-drain” TTD
“time-to-drain”
rCBV
“relative cerebral
blood volume”
rCBV
“relative cerebral
blood volume”
rCBV
“relative cerebral
blood volume”

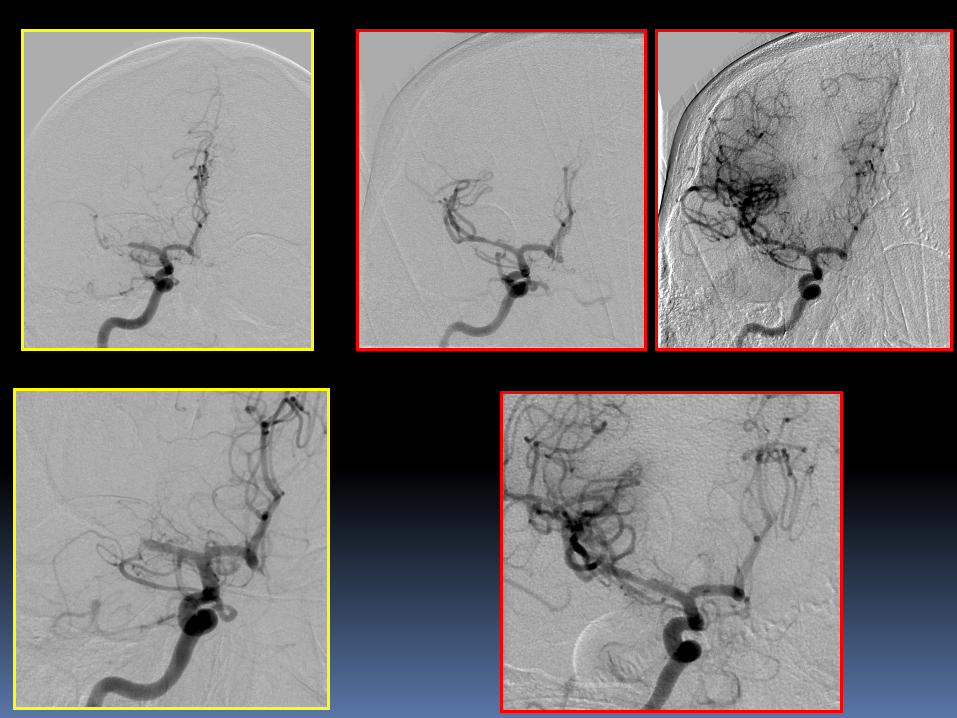
4x20mm Solitaire
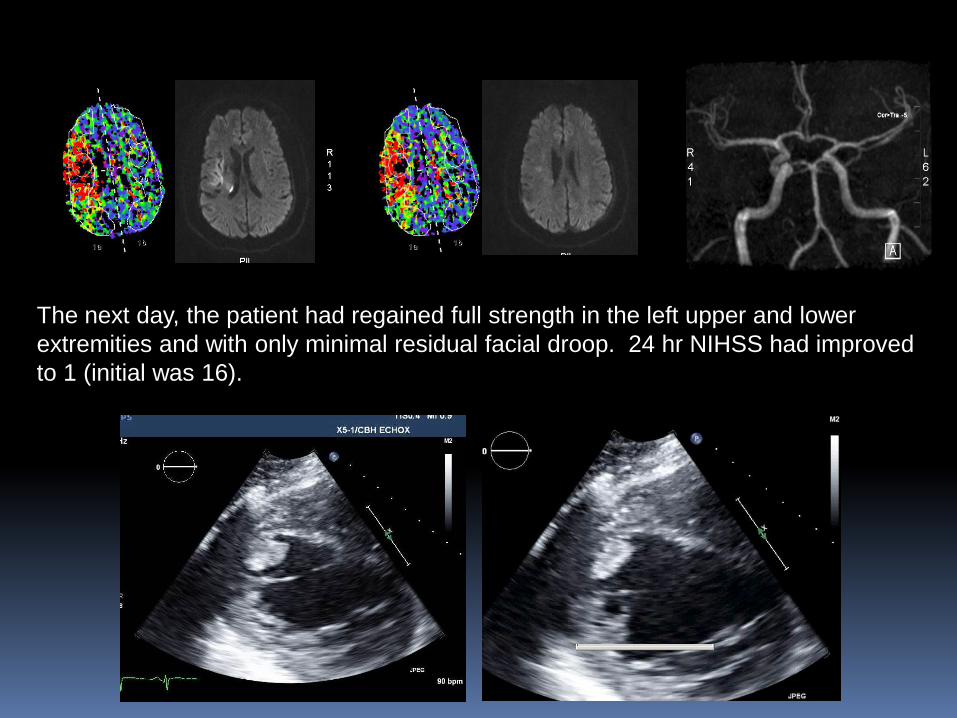
The next day, the patient had regained full strength in the left upper and lower
extremities and with only minimal residual facial droop. 24 hr NIHSS had improved
to 1 (initial was 16).

TTD
“time-to-drain”
57 yo BF with “wake up” stroke manifesting as slurred speech and right arm/leg paralysis,
resulting in fall to floor upon getting out of bed. PMH significant for non-ischemic cardiomyopathy
with pacemaker (EF 30-35%), type II DM, and dyslipidemia (not on statin therapy). Initial NIHSS
was 8 in the ED, and was NIHSS of 11 prior to procedure.
rCBV
“relative cerebral blood volume”
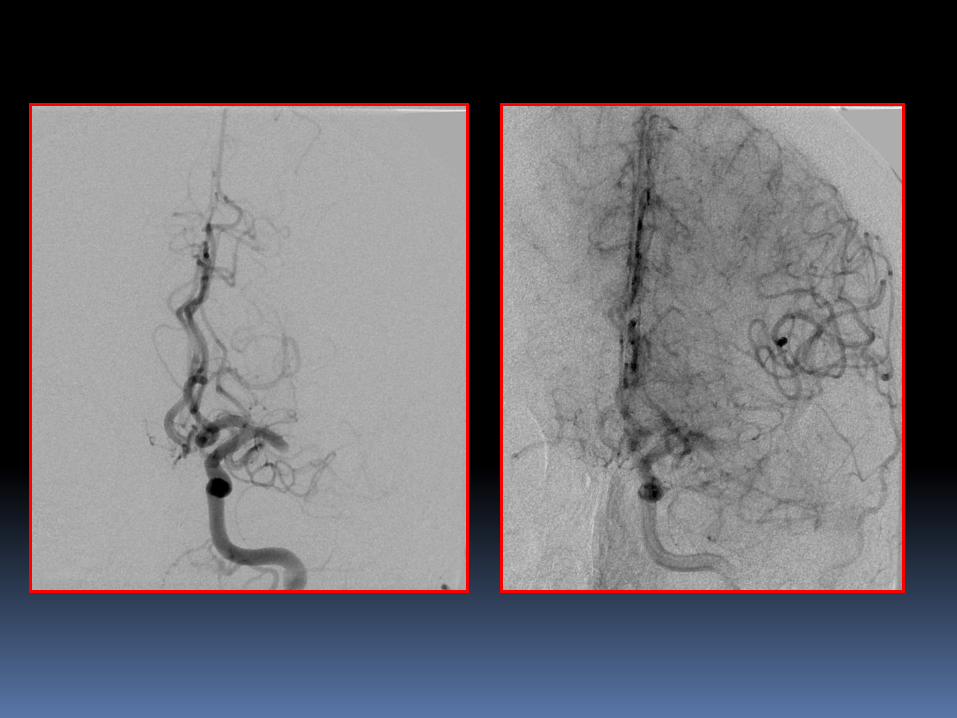

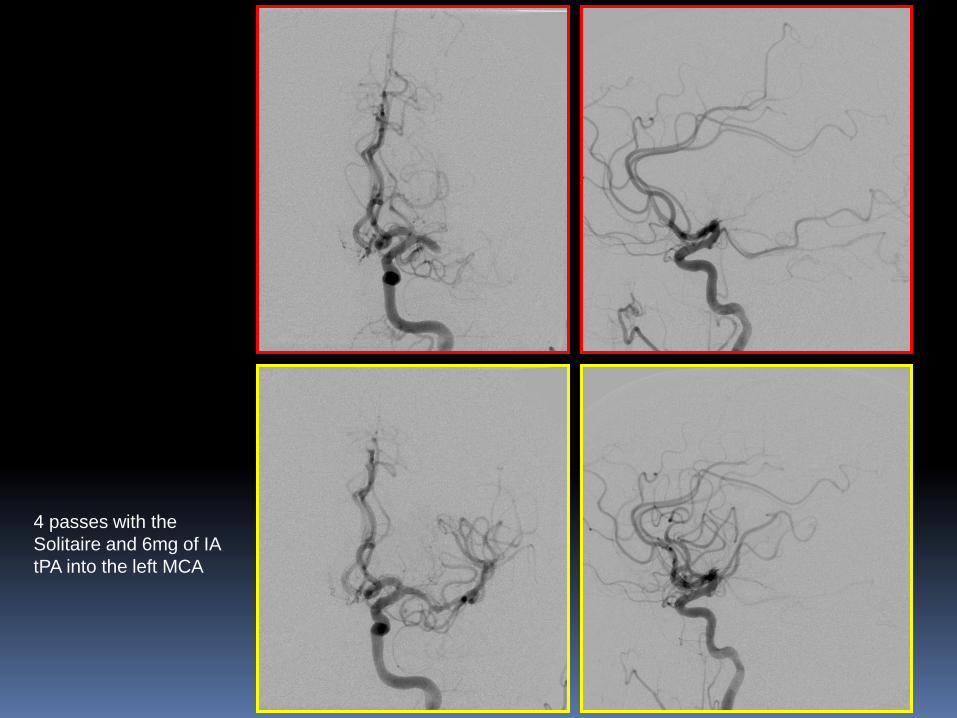
4 passes with the
Solitaire and 6mg of IA
tPA into the left MCA
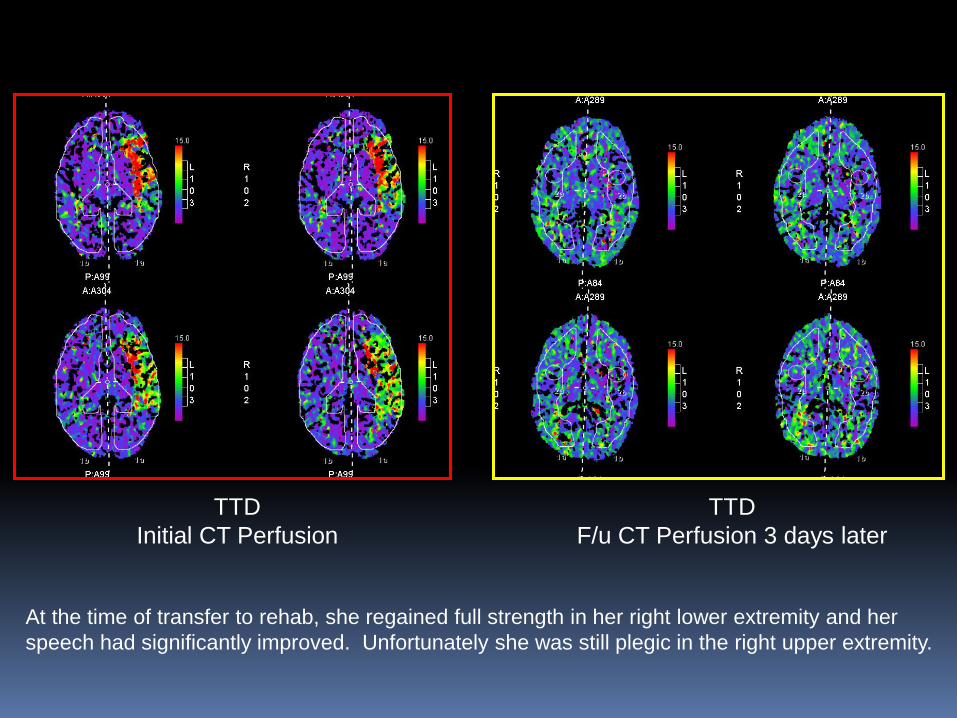
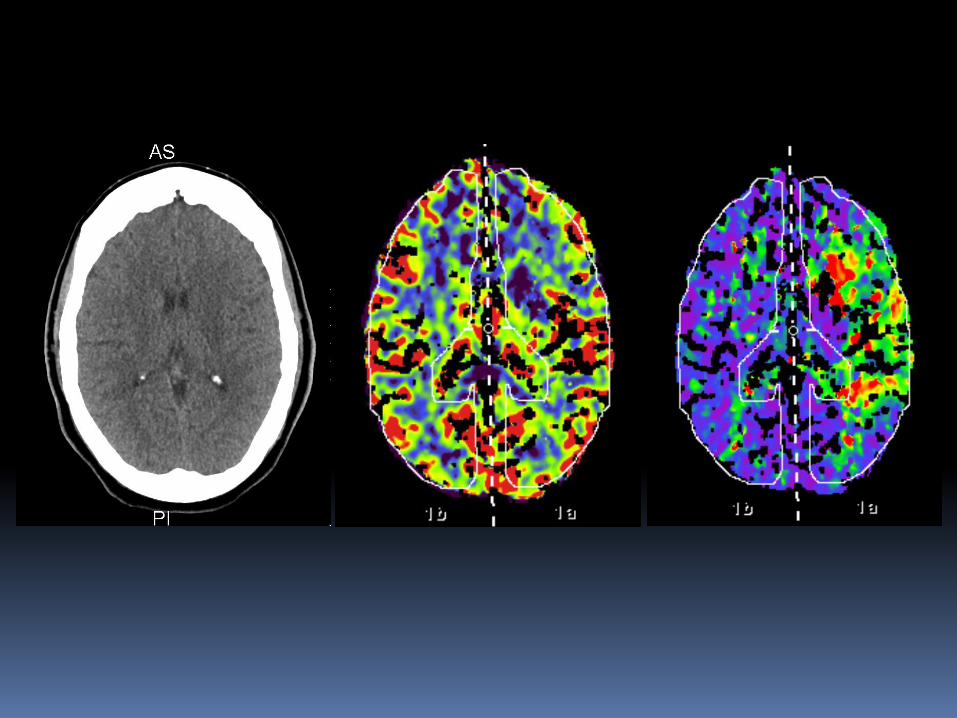
TTD
Initial CT Perfusion
TTD
F/u CT Perfusion 3 days later
At the time of transfer to rehab, she regained full strength in her right lower extremity and her
speech had significantly improved. Unfortunately she was still plegic in the right upper extremity.
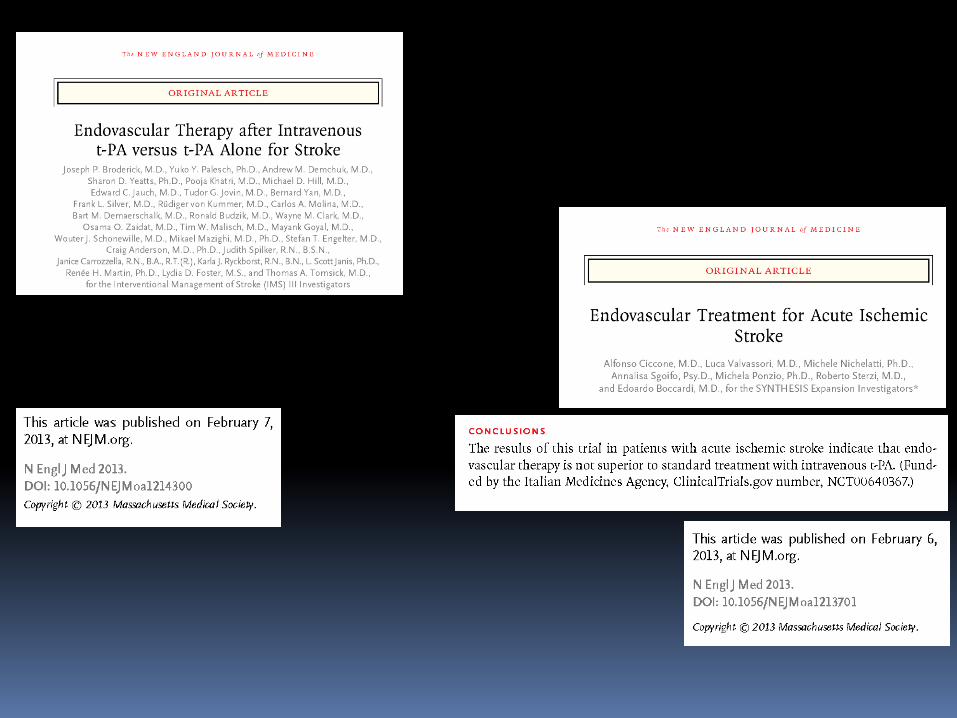
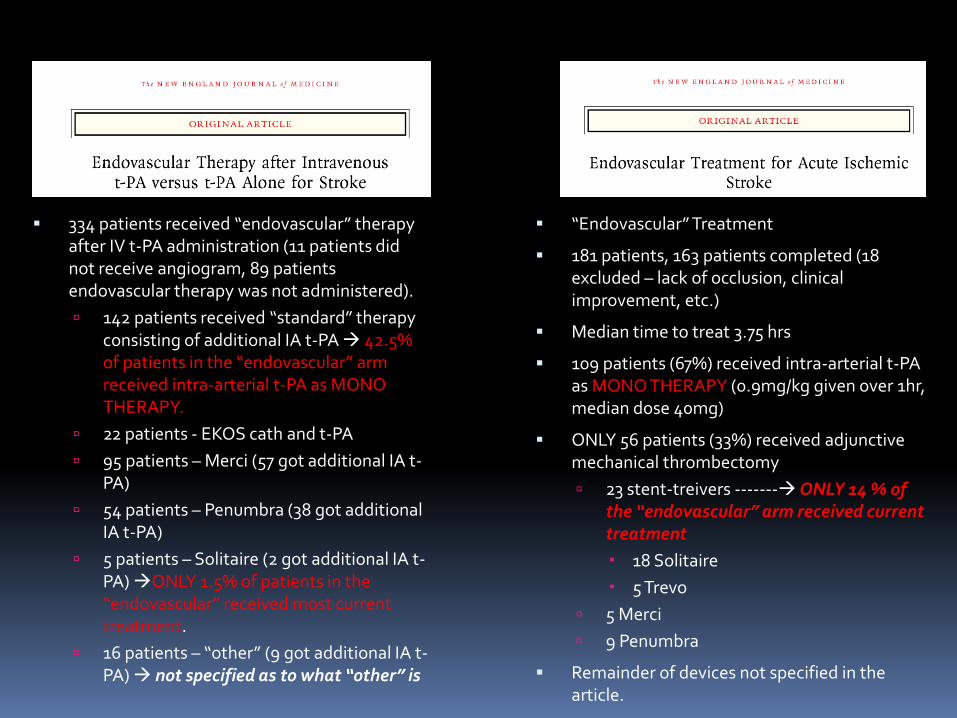
334 patients received “endovascular” therapy after IV t-PA administration (11 patients did not receive angiogram, 89 patients endovascular therapy was not administered).
142 patients received “standard” therapy consisting of additional IA t-PA 42.5% of patients in the “endovascular” arm received intra-arterial t-PA as MONO THERAPY.
22 patients - EKOS cath and t-PA
95 patients – Merci (57 got additional IA t-PA)
54 patients – Penumbra (38 got additional IA t-PA)
5 patients – Solitaire (2 got additional IA t-PA) ONLY 1.5% of patients in the “endovascular” received most current treatment.
16 patients – “other” (9 got additional IA t-PA) not specified as to what “other” is
“Endovascular” Treatment
181 patients, 163 patients completed (18 excluded – lack of occlusion, clinical improvement, etc.)
Median time to treat 3.75 hrs
109 patients (67%) received intra-arterial t-PA as MONO THERAPY (0.9mg/kg given over 1hr, median dose 40mg)
ONLY 56 patients (33%) received adjunctive mechanical thrombectomy
23 stent-treivers ------- ONLY 14 % of the “endovascular” arm received current treatment
18 Solitaire
5 Trevo
5 Merci
9 Penumbra
Remainder of devices not specified in the article.
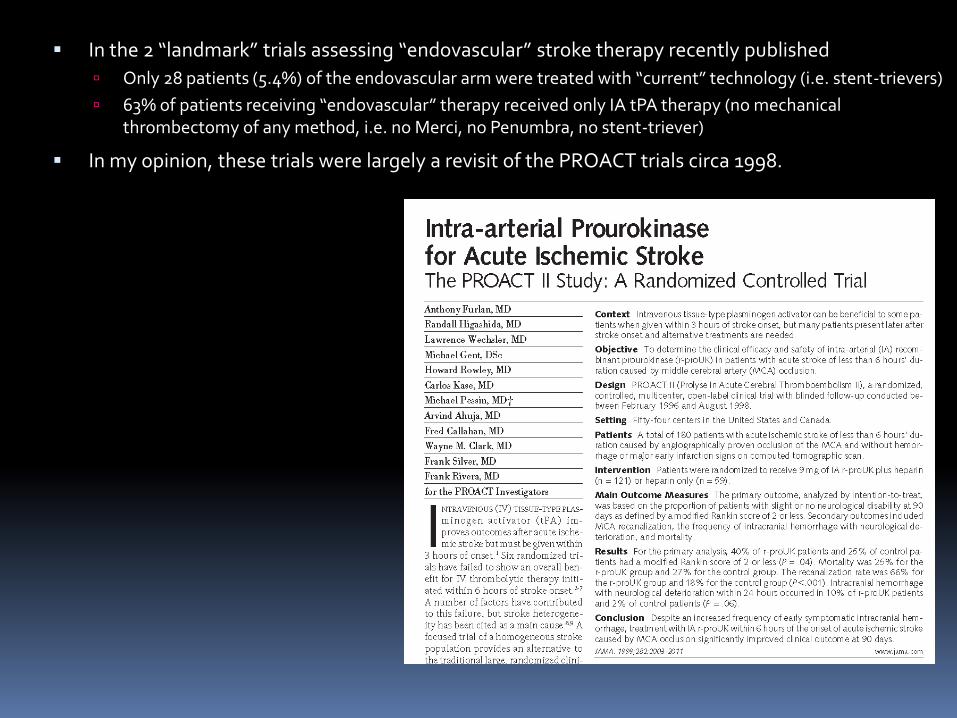
In the 2 “landmark” trials assessing “endovascular” stroke therapy recently published
Only 28 patients (5.4%) of the endovascular arm were treated with “current” technology (i.e. stent-trievers)
63% of patients receiving “endovascular” therapy received only IA tPA therapy (no mechanical thrombectomy of any method, i.e. no Merci, no Penumbra, no stent-triever)
In my opinion, these trials were largely a revisit of the PROACT trials circa 1998.
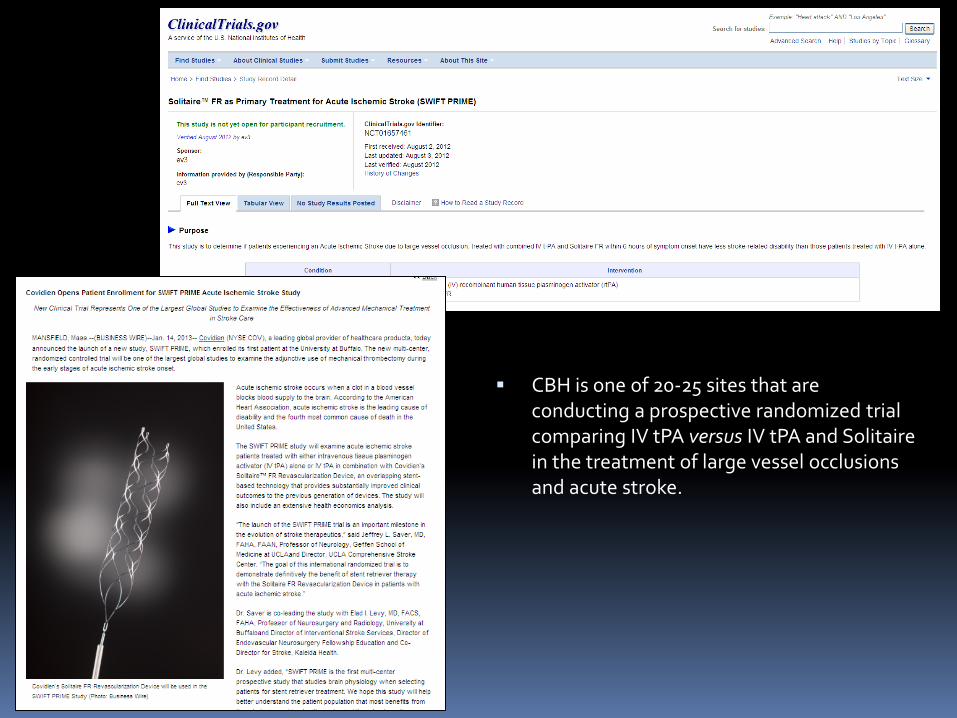
CBH is one of 20-25 sites that are conducting a prospective randomized trial comparing IV tPA versus IV tPA and Solitaire in the treatment of large vessel occlusions and acute stroke.
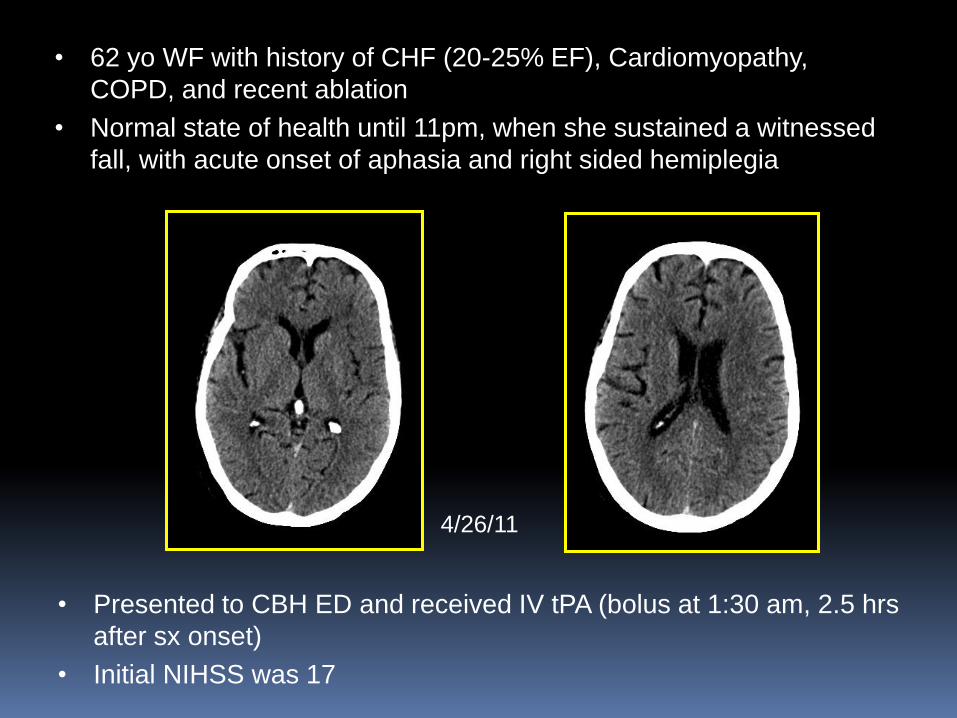
• Presented to CBH ED and received IV tPA (bolus at 1:30 am, 2.5 hrs
after sx onset)
• Initial NIHSS was 17
4/26/11
• 62 yo WF with history of CHF (20-25% EF), Cardiomyopathy,
COPD, and recent ablation
• Normal state of health until 11pm, when she sustained a witnessed
fall, with acute onset of aphasia and right sided hemiplegia

Right CCA Left CCA
Only mild clinical improvement (NIHSS 15),
brought to cath lab, initial angios at 2:30am
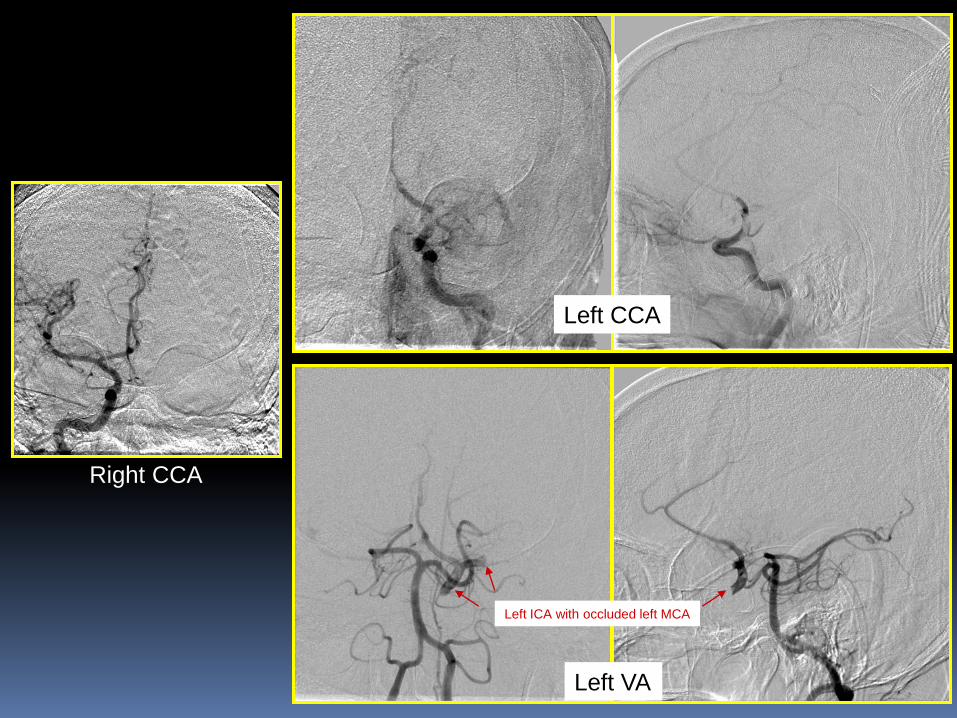
Right CCA
Left CCA
Left VA
Left ICA with occluded left MCA
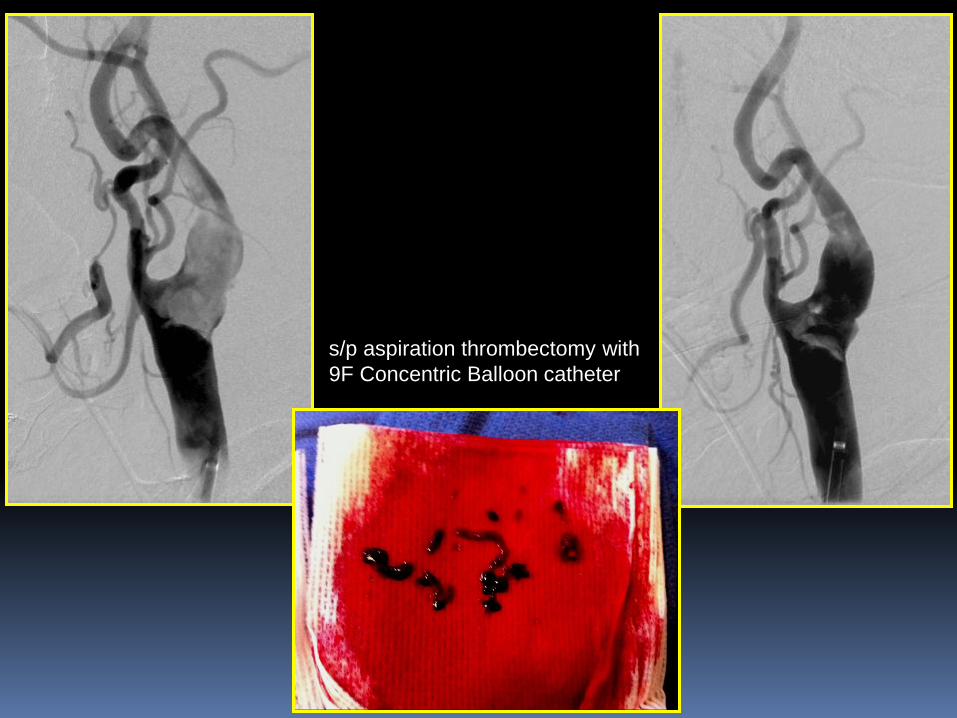
s/p aspiration thrombectomy with
9F Concentric Balloon catheter

Carotid Wallstent, effectively
(luckily) trapped residual clot
against ECA origin, protecting the
CCA/ICA
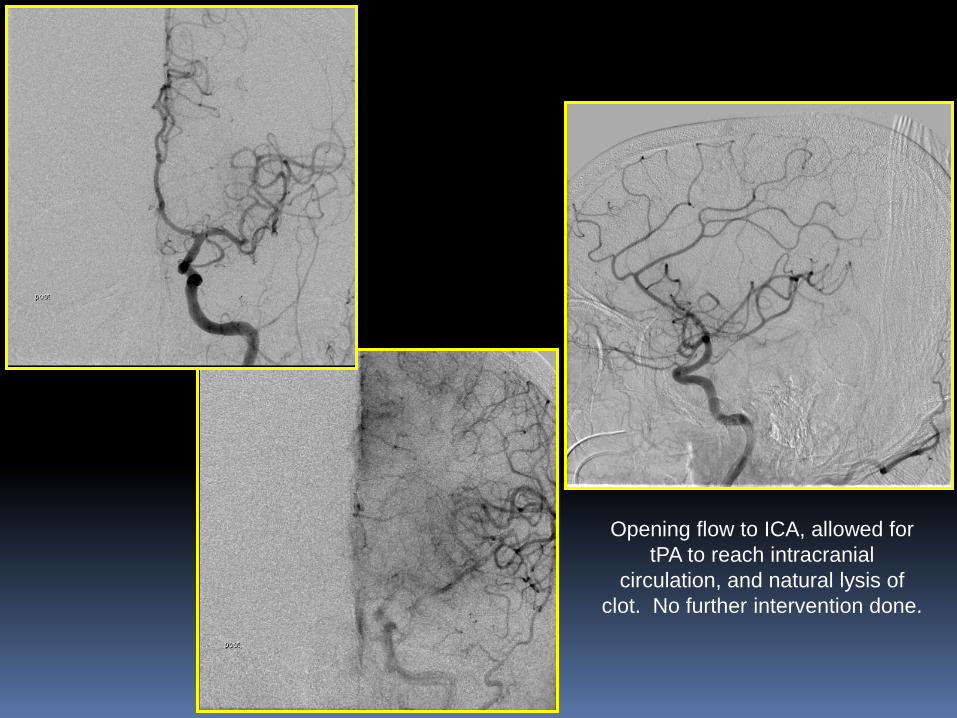
Opening flow to ICA, allowed for
tPA to reach intracranial
circulation, and natural lysis of
clot. No further intervention done.
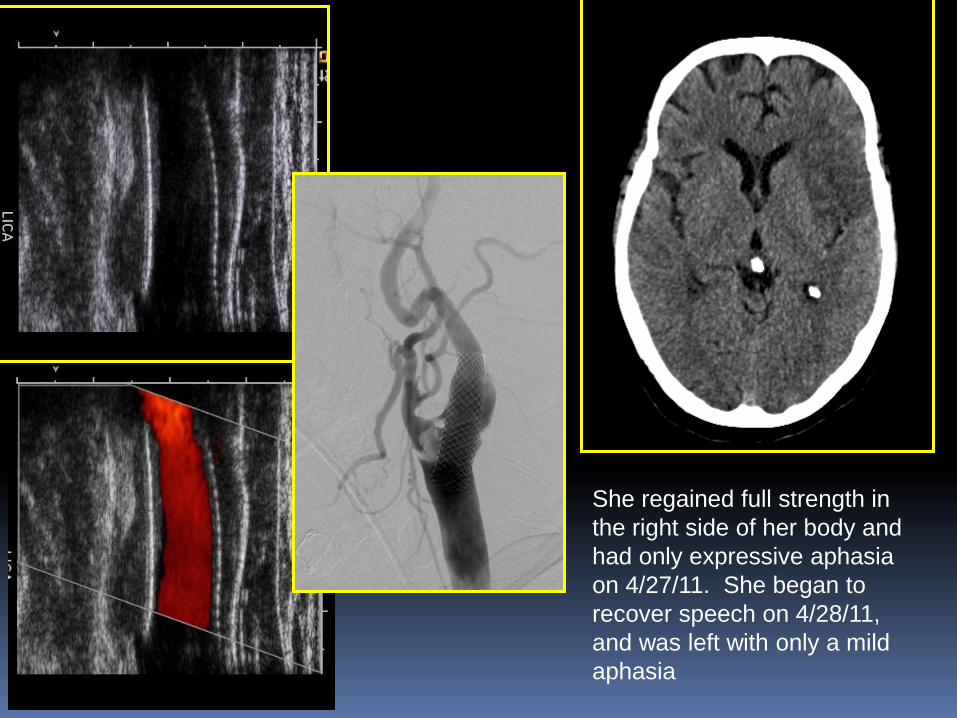
She regained full strength in
the right side of her body and
had only expressive aphasia
on 4/27/11. She began to
recover speech on 4/28/11,
and was left with only a mild
aphasia
4/27/11
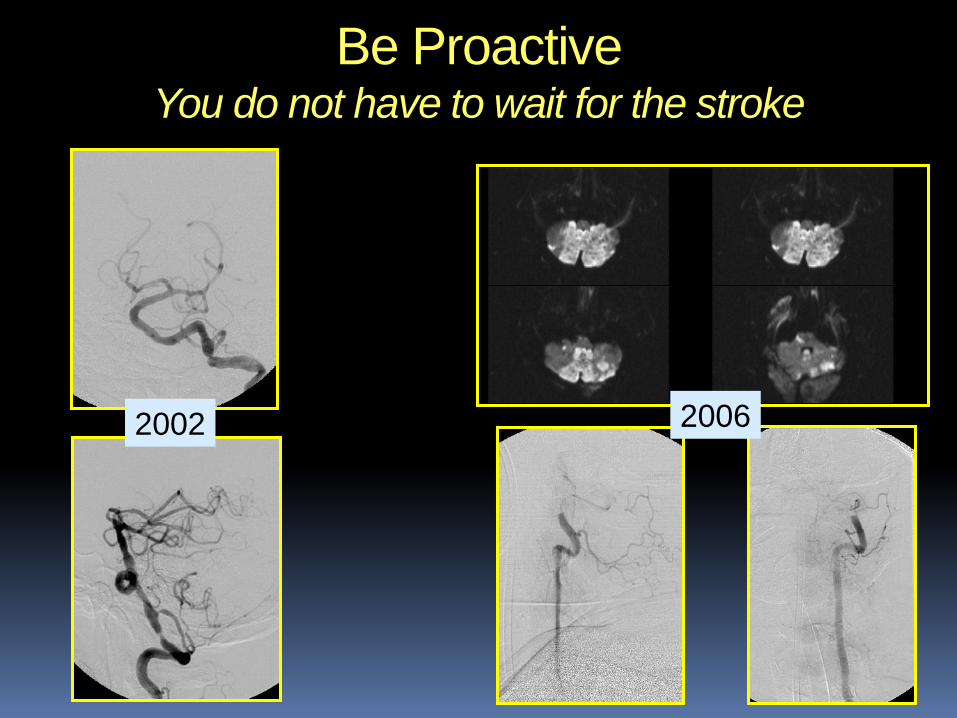
2002 2006
Be Proactive You do not have to wait for the stroke
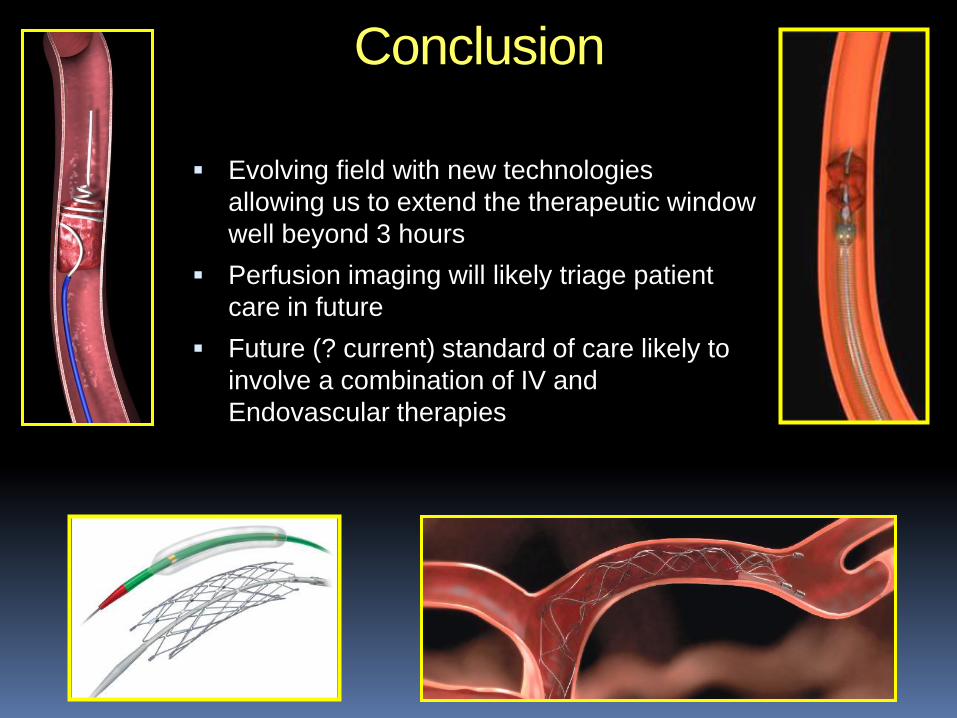
Conclusion
Evolving field with new technologies
allowing us to extend the therapeutic window
well beyond 3 hours
Perfusion imaging will likely triage patient
care in future
Future (? current) standard of care likely to
involve a combination of IV and
Endovascular therapies