Embed Size (px)
Citation preview
Thrombolytics for Acute Pulmonary Embolism:
Clot bustin’ and myth bustin’… maybe?
©iStockphoto.com/dturnerrx
DeAnna W. Turner, PharmD PGY1 Pharmacy Resident
Department of Pharmacy, University Health System, San Antonio, Texas Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center, University of Texas Health Science Center at San Antonio
January 25, 2013
Learning Objectives:
1. Describe the pathophysiology and etiology of pulmonary embolism 2. Identify thrombolytic agents utilized in the treatment of pulmonary embolism 3. Evaluate the role of thrombolytics in acute pulmonary embolism 4. Indicate where the use of thrombolytics for acute pulmonary embolism may be beneficial
Turner 2
VENOUS THROMBOEMBOLISM I. Definition and Epidemiology1-5
a. Formation of blood clot within a vein b. Venous thromboembolism (VTE) = deep vein thrombosis (DVT) and/or pulmonary embolism (PE) c. Epidemiology
i. Estimated 300,000 to 600,000 people affected yearly in the United States
Increasing incidence with age
a. 1 per 100,000 in childhood; 1 per 100 80 years of age
Incidence slightly higher in men than women
Incidence greater among African Americans and Caucasians d. Approximately two thirds of patients present with DVT and one third with PE
II. Morbidity and mortality1,3
a. Complications associated with VTE include pulmonary hypertension, chronic venous insufficiency, post-thrombotic syndrome, and death
i. Chronic venous insufficiency and post-thrombotic syndrome lifelong conditions characterized by swelling, pain, ulceration, and skin necrosis
b. PE is the primary cause of mortality associated with VTE i. Approximately 10% to 30% of patients die within one month of diagnosis
c. PE is the leading cause of preventable hospital death
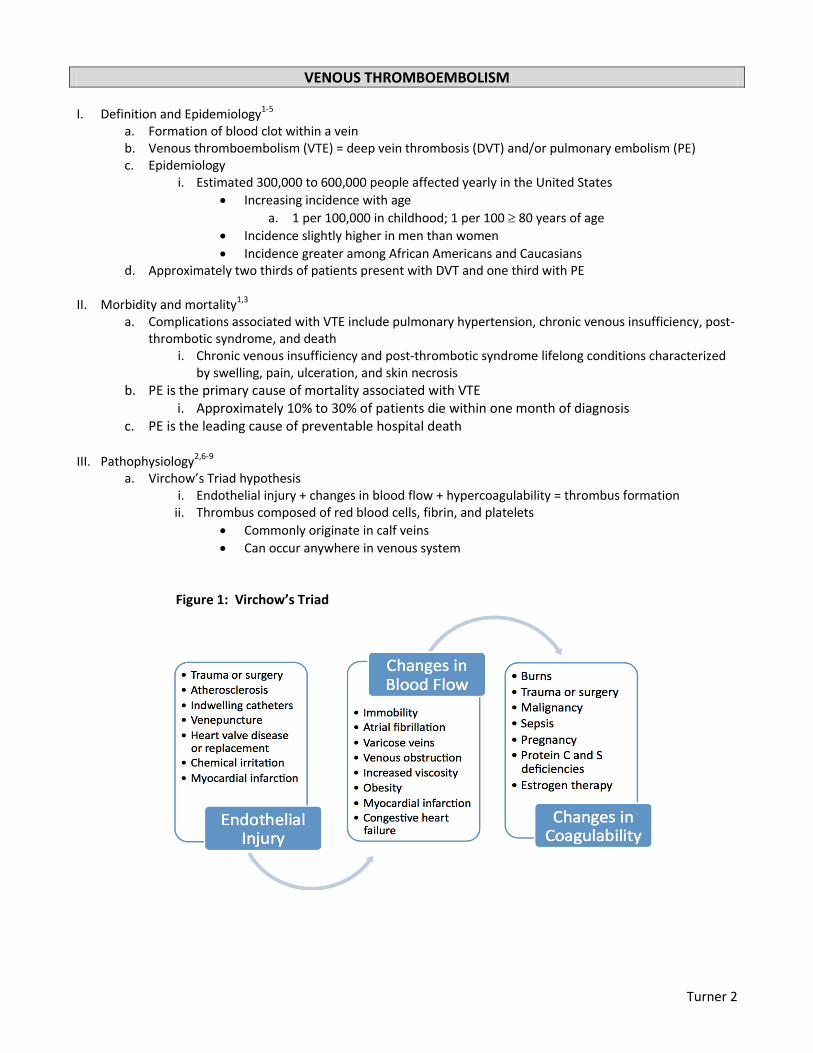
III. Pathophysiology2,6-9 a. Virchow’s Triad hypothesis
i. Endothelial injury + changes in blood flow + hypercoagulability = thrombus formation ii. Thrombus composed of red blood cells, fibrin, and platelets
Commonly originate in calf veins
Can occur anywhere in venous system
Figure 1: Virchow’s Triad

Turner 3
IV. VTE Risk factors1,3,5 a. Lack of identified acquired risk factor in 50% of cases (idiopathic)
Table 1: Risk Factors for VTE
Acquired Transient Acquired Genetic
Advanced age Hormone therapy Family history Malignancy Pregnancy Protein C deficiency
Obesity Immobilization Protein S deficiency Chronic disease Trauma Factor V Leiden Antiphosphlipid
antibodies Surgery Antithrombin
deficiency Hospitalization Sickle cell trait Oral contraceptives Prothrombin G20210A
V. Clinical manifestations3,5,6,10-12
a. DVT i. Up to half of people with DVT asymptomatic
ii. Pain, tenderness, swelling, warmness to touch, and erythema most common signs and symptoms
b. PE i. Arises when a section of clot breaks off and lodges in pulmonary arteries
ii. Symptoms generally appear when 20% to 30% of lung vasculature occluded iii. Cardiac arrest can occur within one to two hours following symptom onset iv. Right ventricular dysfunction (RVD)
Associated with a 66% increase in mortality
Right ventricular (RV) afterload increases as embolic burden increases
RV dilation follows with release of cardiac enzymes
Hypokinesis develops, cardiac output decreases, and cardiac arrest follows v. Sudden death documented as first symptom in approximately 25% of patients
Figure 2: Signs and Symptoms of PE
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Pe
rce
nta
ge
Signs and Symptoms

Turner 4
VI. PE Diagnosis2,7,12,13 a. Clinical assessment
i. Pretest probability assessment
Wells Score and Revised Geneva Score (APPENDIX A and B)
1st step when VTE suspected; based on medical history and physical examination
Risk divided into low, intermediate, or high probability categories b. Laboratory studies
i. D-dimer
Product of fibrin degradation
Level >500 ng/ml considered abnormal
Fast, noninvasive, and inexpensive
95% sensitivity; negative predictive value a. Elevated D-dimer concentrations can also be seen in the presence of
malignancy, inflammation, or surgery b. Predictive value improved when used in combination with pretest probability
assessment c. Imaging techniques
i. Chest computed tomography (CT) with contrast ii. Ventilation-perfusion (V/Q) lung scan
V/Q mismatch = normal ventilation; perfusion defect iii. Pulmonary angiography
Gold standard; most invasive and expensive
Usually reserved for patients with negative noninvasive tests and high clinical probability
d. Assessment of RVD i. Increased biomarkers
Cardiac troponin T >0.07 ng/ml a. Directly correlates with degree of RVD
Brain natriuretic peptide (BNP) 600 pg/ml ii. Electrocardiogram
New right bundle branch block (RBBB)
T-wave inversion in leads V1-V4
S1Q3T3 pattern iii. Echocardiogram
Pulmonary hypertension
Right ventricular dilatation and hypokinesis VII. PE Management and treatment14-18
a. Anticoagulation i. Halts clot propagation and inhibits recurrent thrombus formation
ii. Agents
Unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and fondaparinux
Eventually bridged to warfarin or rivaroxaban for long-term treatment b. Thrombectomy
i. Catheter-directed or surgical ii. Reserved for unstable patients who have:
Contraindication to thrombolysis
Failed thrombolysis
Shock c. Thrombolytics
i. Considered standard of care in MPE

Turner 5
ROLE OF THROMBOLYSIS IN PULMONARY EMBOLISM I. American Heart Association classification of PE14,19
a. Low-risk PE: Acute PE and the absence of the clinical markers or adverse prognosis that define massive or submassive PE
b. Submassive PE: Acute PE without systemic hypotension but with either RVD or myocardial necrosis c. Massive PE (MPE): Acute PE with sustained hypotension, pulselessness, or persistent profound
bradycardia i. Sustained hypotension defined as: Systolic blood pressure <90 mmHg for at least 15 minutes
or requiring inotropic support, not due to a cause other than PE ii. Profound bradycardia defined as: Heart rate <40 bpm with signs and symptoms of shock
II. Thrombolytic agents14,20-26
a. Mechanism of action: Act by converting the pro-enzyme plasminogen to plasmin, leading to degradation of the fibrin matrix within thrombus
b. Selective agents i. Bind preferentially to clot-bound plasminogen
ii. Alteplase most commonly used; approved indication for MPE iii. Tenecteplase and reteplase not approved for use in MPE
c. Nonselective agents i. Activate clot-bound and circulating plasminogen
ii. Streptokinase
Derived from group C -hemolytic streptococci
Use limited due to antigenic potential – exacerbates hypotension
Approved indication for MPE; not available in the United States iii. Urokinase
Use limited due to concentration needed for PE lysis
Approved indication for MPE; not available in the United States d. Superiority of one thrombolytic regimen approved for MPE over another not clearly established
Table 2: Summary of Selective Thrombolytic Agents
Alteplase Tenecteplase Reteplase
Dose 100 mg IV infusion
over 2 hours
Weight-adjusted IV bolus over 5-10 sec (APPENDIX C)
10 units IV bolus x 2 30 mins apart
T ½ <5 mins Initial: 20-24 mins
Terminal: 90-130 mins 13-16 mins
Excretion Hepatic Hepatic Hepatic and renal Fibrin specificity ++ +++ +
FDA approved for MPE? Yes No No
Adverse events Bleeding complications biggest limitation to therapy
Intracranial hemorrhage most devastating Contraindications APPENDIX D
FDA = Food and Drug Administration; IV = intravenous; mins = minutes; sec = seconds
III. 2012 updates to the Antithrombotic Therapy and Prevention of Thrombosis American College of Chest
Physicians Guidelines17 a. Thrombolytics recommended in hemodynamically unstable patients with MPE b. Thrombolytics not recommended for hemodynamically stable patients with submassive PE and RVD c. Patients with low-risk PE should not receive thrombolytic therapy

Turner 6
CLINICAL QUESTIONS I. With weak recommendations and the increased risk of bleeding complications, should thrombolytics be
considered in acute pulmonary embolism, and if so, what dose should be used? II. Factors to consider during evaluation
a. Thrombolytic treatment: Was a bolus dose used? Infusion time? b. Elapsed time between cardiac arrest and initiation of thrombolytic c. Outcomes: Survival to hospital discharge? Recurrent PE? d. Adverse events: Bleeding complications? Neurologic sequelae?
THROMBOLYTICS IN ADVANCED CARDIAC LIFE SUPPORT I. Sudden cardiac arrest27-30
a. Abrupt cessation of spontaneous circulation and ventilation with hemodynamic collapse b. Requires intervention for restoration of spontaneous circulation c. Estimated 300,000 to 500,000 cardiac deaths annually in the United States
i. 43,717 cardiac deaths reported in Texas in 1999
26,004 due to sudden cardiac death d. Approximately 70% of sudden cardiac arrests caused by acute myocardial infarction (AMI) and massive
pulmonary embolism (MPE) e. Major health dilemma with poor prognosis
II. Advanced Cardiac Life Support (ACLS)31
a. Multi-stage algorithms developed b. Divided into two groups based on cardiac arrest rhythms:
i. Shockable = pulseless VT and VF ii. Non-shockable = PEA and asystole
III. Thrombolytics during cardiopulmonary resuscitation (CPR)27,32-34
a. Two proposed mechanisms: i. Local effects at site of pulmonary thrombosis
ii. Prevents “no-reflow” phenomenon
Cardiac arrest and CPR associated with coagulation activation
Inadequate endogenous fibrinolysis
Microthrombi develop throughout circulatory system
Microcirculation impaired, contributing to cardiovascular and cerebral dysfunction
Thrombolytic therapy leads to improved microcirculatory reperfusion and hemodynamic stability
b. Advantages: i. Administered without need for specialty services required of surgery (interventional radiology)
ii. May lyse smaller emboli located in distal pulmonary vasculature not accessible to surgeons c. Disadvantages:
i. PE diagnosis during cardiac arrest may be impossible ii. Indiscriminant use may lead to a higher incidence of bleeding occurrences
IV. Safety of thrombolysis during CPR27,35
a. Ongoing CPR once regarded as a contraindication to thrombolysis i. Chest compressions thought to be potential risk for bleeding complications
ii. No longer considered a contraindication

Turner 7
Langdon RW, et al. Ann Emerg Med. 1989;18(6):678-80.34 Patient Demographics
33 year old female
Medical History One week prior: abdominal hysterectomy
Presentation Unconscious, apneic, pulseless
Experienced brief syncopal episode and sudden extreme dyspnea earlier the same day
Treatment Prior to Thrombolytic
CPR
Endotracheal intubation and ventilation
Epinephrine*
Atropine*
Sodium bicarbonate*
Dopamine*
IV fluids
rt-PA Course
100 mg total dose o 10 mg bolus via central line o 90 mg continuous infusion over two hours
Administration Delay (after CPR initiation)
30 minutes
Response Palpable pulse and sinus rhythm detected within moments of rt-PA administration
Progressed to tachycardia
SBP 121 mmHg
Remained unresponsive
Transported to cardiac catheterization laboratory o Confirmed MPE on pulmonary angiography
Consciousness regained
Outcome Transported to ICU
BP 118/80 mmHg
Heparin infusion initiated; IVC filter placed
Eight day hospitalization
Experienced pelvic bleeding at site of recent hysterectomy o Required surgical intervention
Discharged home on low-dose warfarin Take Home Points
Successful outcomes rare with CPR alone in MPE
rt-PA administration potentially a life-saving alternative in known or suspected MPE refractory to aggressive CPR
No neurologic complications reported
Embolectomy not practical in arresting patients, nor is it available at all facilities, when contraindications to systemic thrombolysis exist
Non-fatal bleeding complication reported BID = twice daily; ICH = intracranial hemorrhage; TEE = transoesophageal echocardiography; VAP = ventilator associated pneumonia *Doses not reported

Turner 8
Ruiz-Bailen M, et al. Resuscitation. 2001;51(1):97-101.36 Objective Assess outcomes of thrombolysis during CPR for cardiac arrest due to MPE
Case 1 Case 2 Case 3 Case 4 Case 5 Case 6
Patient Demographics
Female 45 years old
Male 28 years old
Male 34 years old
Male 73 years old
Male 76 years old
Female 56 years old
Medical History Cardiac valve disease
Neoplasm of pancreas
Fracture of patella
None None Protein S deficiency
History of Present Illness
Presented with signs of DVT 5 days post-valve replacement with cardiac arrest 2 days later
Presented with dyspnea, tachypnea, hypotension, cyanosis with cardiac arrest 72 hours after admission
7 days after fracture presented with chest pain, fever, dyspnea, tachypnea with cardiac arrest the next day
Presented with sudden dyspnea, chest pain, tachypnea with cardiac arrest 12 hours later
Presented with syncope followed by dyspnea and cyanosis with respiratory and cardiac arrest 48 hours later
Presented in respiratory arrest after sudden onset dyspnea with cardiac arrest shortly thereafter
Presenting Rhythm
PEA PEA Asystole PEA Asystole PEA
CPR Initiation Immediate After 5 mins After 10 mins
Immediate Immediate Immediate
rt-PA Course* 50 mg bolus + 50 mg bolus after 30 mins
50 mg bolus + 50 mg bolus after 30 mins
50 mg bolus 50 mg bolus + 50 mg bolus after 30 mins
50 mg bolus + 50 mg bolus after 30 mins
50 mg bolus + 50 mg bolus after 30 mins
Administration Delay (after CPR initiation)
60 minutes 30 minutes 30 minutes 15 minutes Immediate 15 minutes
Total CPR Time 70 minutes 45 minutes 90 minutes 30 minutes 5 minutes 40 minutes
Other Treatments
Heparin, dopamine
Heparin None Heparin, dopamine
Heparin, epinephrine
Heparin dopamine
Evidence of RVD Yes Yes Yes Yes Yes Yes
PE Diagnosis (after rt-PA given)
Scintigraphy Necropsy Necropsy Pulmonary arteriography
Scintigraphy Scintigraphy
Neuro Sequelae None Death Death None None None
Post-CPR Complications
Hemorrhage at injection sites
None None None Hemorrhage at injections sites; upper GI bleed
None
Outcome Alive without sequelae after one year
Death Death Alive without sequelae after one year
Developed stroke after one year
Alive without sequelae after six months
Take Home Points
ROSC and survival to hospital discharge successful in 4/6 cases (66.7%)
2/6 patients with mild hemorrhage – no fatal hemorrhages reported o Case 1: no intervention required; Case 5: transfusion of two units required
Potential benefit during prolonged CPR and/or delayed administration
No reported neurologic sequelae from acute event in survivors
Potential life-saving benefits of rt-PA administered on strong clinical suspicion of MPE during cardiac arrest may outweigh risks associated with therapy
rt-PA dosing consistent in case series; however, dose in cardiac arrest not established *First bolus administered over 2-3 minutes; second bolus over 5 minutes

Turner 9
V. Landmark trials evaluating thrombolytics in ACLS
Abu-Laban RB, et al. NEJM. 2002;246(20):1522-1528.37 Purpose Evaluate effect of rt-PA during CPR in adults with undifferentiated PEA
Design Randomized, double-blind, placebo-controlled study
3 tertiary teaching hospitals and 7 paramedic base stations in Vancouver, Canada
Outcomes Primary:
Survival to hospital discharge Secondary:
ROSC, neurologic outcome, length of stay, hemorrhage
Methods Standard care received by all patients during CPR
Resuscitation efforts continued a minimum of 15 minutes post-infusion
Further treatment at discretion of CPR leader
Administration of aspirin, heparin, or both at discretion of attending physician
Interventions:
Treatment arm o 100 mg rt-PA infused over 15 minutes during CPR
Matching placebo
Results 233 patients enrolled – baseline characteristics similar between groups
36 minutes (median) elapsed from collapse to initiation of rt-PA o Average 32.1 minutes of CPR prior to rt-PA administration
Outcomes
Variable rt-PA (n=117) no. (%)
Placebo (n=116) no. (%)
p-Value
ROSC 25 (21.4) 27 (23.3) 0.85
Died at scene 73 (62.4) 74 (63.8) 0.93
Transported to hospital 39 (33.3) 38 (32.8) 0.96
Enrolled at hospital; died in emergency room
5 (4.3) 4 (3.4) 0.99
Survived to hospital admission 7 (6.0) 6 (5.2) 0.99
Major hemorrhage 2 (1.7) 0 0.50
Minor hemorrhage 1 (0.9) 1 (0.9) 0.99
Length of stay (days) Median Mean
0.4 6.3
0.5 0.5
0.62
Survival to hospital discharge 1 (0.9) 0 0.99
Findings From Autopsy (n=42)
No. of Patients Percent
Cardiovascular Myocardial infarction Hemorrhage
25 9 4
59.5 21.4 9.5
Pulmonary embolism 1 2.4
Miscellaneous 16 38.1
Author’s Conclusions
No evidence of improved survival to hospital discharge with administration of rt-PA during CPR with undifferentiated PEA
96.1% of cardiac arrests occurred out-of-hospital – causes undifferentiated
Earlier administration of rt-PA may yield different outcome (median time = 36 minutes)
Future investigation needed to evaluate earlier administration of thrombolytics

Turner 10
Take Home Points
rt-PA ineffective for undifferentiated PEA
Poor prognosis associated with out-of-hospital cardiac arrest
Results not generalizable to cardiac arrest patients with known or highly suspected PE in the inpatient setting
Only one confirmed PE – ability to detect treatment effect low
Delay in administration may contribute to adverse effects on outcome
Routine use of thrombolytics in undifferentiated cardiac arrest not recommended AED = automated external defibrillator
Bottiger BW, et al. NEJM. 2008;359(25):2651-2662.30 Purpose Determine whether the use of tenecteplase during CPR can improve survival in adults with
witnessed out-of-hospital arrest
Design Prospective, randomized, open-label, double-blind, placebo-controlled study
66 emergency-medical-service systems in 10 European countries
Outcomes Primary:
30-day survival Secondary:
ROSC, hospital admission, 24-hour survival, survival to hospital discharge
Methods CPR continued for a minimum of 30 minutes after administration of tenecteplase when required
Adjunctive anticoagulation and antiplatelet therapy restricted until hospital admission Interventions:
Treatment arm o Tenecteplase dosing = weight based
Matching placebo
Results 1,050 patients enrolled – baseline characteristics similar between groups
Approximately 18 minutes elapsed from collapse to administration
Outcomes
Variable Tenecteplase (n=525) no. (%)
Placebo (n=525) no. (%)
p-Value
30-day survival 77 (14.7) 89 (17.0) 0.36
ROSC 283 (55) 279 (54.6) 0.96
Hospital admission 281 (53.5) 289 (55) 0.67
24-hour survival 158 (30.6) 171 (33.3) 0.39
Survival to hospital admission 78 (15.1) 90 (17.5) 0.33
Safety endpoints Symptomatic ICH Any ICH Major non-ICH Ischemic stroke
4 (0.8)
14 (2.7%) 40 (7.7) 4 (0.8)
0
2 (0.4) 33 (6.4) 3 (0.6)
0.13
0.006 0.48 1.00
Author’s Conclusions
No survival benefit shown in out-of-hospital cardiac arrest
Pre-hospital emergency care difficult setting for research
Findings do not suggest withholding thrombolytic therapy in patients with a pathologic condition known to be responsive to such treatment

Turner 11
Take Home Points
Study terminated early due to futility
Out-of-hospital cardiac arrest associated with poor prognosis
Thirty-seven patients with presumed PE enrolled o Only 2 PE confirmed – number too small to determine treatment effect
Tenecteplase used as study drug
Higher frequency of ICH in treatment group
Results not generalizable to patients with suspected MPE in the inpatient setting ICH = intracranial hemorrhage
IV. 2010 updates to the American Heart Association’s ACLS guidelines:31,38
a. Routine use of thrombolytic therapy not recommended in cardiac arrest b. Thrombolytic therapy may be considered in cases of cardiac arrest due to known or suspected MPE
THROMBOLYSIS IN SUBMASSIVE PULMONARY EMBOLISM Konstantinides S, et al. NEJM.
2002;347(15):1143-1150.39
Sharifi M, et al. Am J Cardiol. 2013;111(2);273-277.40
Study Design Prospective, randomized, double-blind, placebo-controlled
49 centers in Germany
Prospective, randomized, controlled, single-center open study
Arizona Purpose Compare effects of heparin + alteplase vs.
heparin + placebo on outcomes of submassive PE in hemodynamically stable patients
Evaluate the role of “safe dose” thrombolysis in reduction of pulmonary arterial pressure in moderate PE in hemodynamically stable patients
Patient Population
TG: Heparin + rt-PA (n=118)
CG: Heparin + placebo (n=138)
TG: Anticoagulation + rt-PA (n=61)
CG: Anticoagulation alone (n=60) Dosing rt-PA = 100 mg total dose
o 10 mg bolus o 90 mg infused over two hours
All patients received UFH
Oral anticoagulation started on day three after randomization
rt-PA = weight based dosing
≥50 kg: 50 mg total dose o 10 mg bolus IVP over one minute o 40 mg infused within two hours
<50 kg: 0.5 mg/kg o 10 mg bolus o Remainder infused within two
hours
All patients received either UFH or enoxaparin ; warfarin started at admission in all patients
Outcomes Primary:
In-hospital death
Clinical deterioration requiring escalation of treatment
Secondary:
Recurrent PE
Major bleeding
Ischemic stroke
Primary:
Development of pulmonary HTN
Composite endpoints of pulmonary HTN and recurrent PE
Secondary:
Total mortality
Bleeding
Recurrent PE
Duration of hospitalization
Composite endpoints of mortality and recurrent PE

Turner 12
Mortality TG (4/118; 3.4%); CG (3/138; 2.2%) NS
Escalation of treatment significantly higher in CG vs TG (34/138; 24.6% vs. 12/118; 10.2%) p=0.004
Study terminated after interim analysis due to statistically significant difference favoring alteplase treatment
TG (1/61; 1.6%); 3/60; 5%) NS Total mortality plus recurrent PE:
TG (1/61; 1.6%); CG (6/61; 10%) p=0.049
Bleeding Complications
Major bleeding:
TG (1/118;0.8%); CG (5/138;2.9%) NS
Fatal bleeding:
TG (zero); CG (1/138;0.7%) NS Hemorrhagic stroke: zero for both groups
No bleeding complications reported
Recurrent PE TG (4/118; 3.4%); CG (4/138; 2.9%) NS TG (zero); CG (3/60; 5%) p=0.08
Author’s Conclusions
Alteplase in combination with heparin may improve clinical course of submassive PE with low risk of major bleeding complications
Such treatment may prevent further hemodynamic deterioration requiring escalation of treatment
“Safe dose” thrombolysis (≤50% standard alteplase dose) safe and effective for submassive PE
Significant, immediate reduction in pulmonary arterial pressure documented after thrombolysis, which was maintained at 28 month follow-up (p<0.001)
Take Home Points
Thrombolytics not currently recommended for treatment of hemodynamically stable patients with submassive PE; however, these results indicate a potential mortality benefit and a trend towards reduction in PE recurrence
Bleeding complications rare in both studies
Small sample sizes limitation to results
Larger studies needed to evaluate potential benefit in this patient population CG = control group; HTN = hypertension; IVP = intravenous push; NS = non-significant; TG = treatment group;

Turner 13
RECOMMENDATIONS I. Should thrombolytics be considered in acute MPE? Yes… cautiously.
a. Thrombolytics recommended in hemodynamically unstable patients with MPE in the absence of contraindications
i. Must weigh risk vs. benefit when contraindications exist b. Lack of proven mortality benefit with increased bleeding risks c. Case reports and case series may be associated with reporting bias d. Hemodynamically unstable patient with pulse:
i. rt-PA – 100 mg total dose
10 mg bolus over two to three minutes, followed by 90 mg over two hours e. Pulseless patient:
i. rt-PA – 0.6 mg/kg bolus (50 mg max) ii. Standard ACLS protocols should always be followed in cardiac arrest
iii. Use of thrombolytics should be considered in this patient population when MPE confirmed or highly suspected
Potentially life-saving alternative iv. Do NOT delay therapy for PE confirmation in cardiac arrest when clinical suspicion is high v. Minimize time from collapse to thrombolytic administration when treatment indicated
If MPE confirmed prior to cardiac arrest, administer thrombolytic immediately vi. Can be argued that most contraindications become null in a pulseless patient
vii. Resuscitative efforts should be continued until ROSC achieved or until efforts deemed futile; minimum of 15 minutes
II. Should thrombolytics be considered in acute submassive PE? Maybe in the future.
a. Promising data in this population, with two larger randomized trials in recruitment phase b. Select patients displaying signs of impending clinical deterioration (eg, worsening RVD or hypotension),
may benefit from “early” administration of a low-dose thrombolytic when bleeding risk is low c. Potential benefits beyond trend towards reduction of mortality and/or recurrent PE
i. Reduction of pulmonary HTN complication may provide quality of life benefit d. Results from larger trials needed to confirm findings of smaller studies before comprehensive
recommendation for thrombolytic therapy can be extended to submassive PE

Turner 14
APPENDICES
APPENDIX A – Wells Score41 APPENDIX B – Revised Geneva Score41 Variable Points
Predisposing factors Previous DVT or PE Recent surgery or immobilization Cancer
+ 1.5 + 1.5 + 1.0
Symptoms Hemoptysis
+ 1.0
Clinical signs Heart rate >100 beats/min Clinical signs of DVT
+ 1.5 + 3.0
Clinical judgment Alternative diagnosis less likely than PE
+ 3.0
Total
Clinical probability (3 levels) Low Intermediate High
0 – 1 2 – 6
7.0
Clinical probability (2 levels) PE unlikely PE likely
0 – 4 >4.0
APPENDIX C – Tenecteplase Dosing26
Weight (kg) Dose <60 30 mg
≥60 to <70 35 mg
≥70 to <80 40 mg
≥80 to <90 45 mg
≥90 50 mg
APPENDIX D – Contraindications to thrombolytics for PE17,23
Absolute
History of cerebrovascular accident Recent intraspinal or intracranial trauma or surgery Active internal bleeding Severe uncontrolled hypertension Known bleeding diathesis Intracranial neoplasm, aneurysm, or arteriovenous malformation
Relative
Age >75 years Pregnancy Uncontrolled hypertension Recent internal bleeding (non-intracranial) Recent trauma, including traumatic CPR Diabetic retinopathy Recent surgery or invasive procedure Pericarditis Ischemic stroke (>3 months prior) Patients currently receiving oral anticoagulation (eg, warfarin)
Variable Points Predisposing factors Age >65 years Previous DVT or PE Surgery or fracture within 1 month Active malignancy
+ 1.0 + 3.0 + 2.0 + 2.0
Symptoms Unilateral lower limb pain Hemoptysis
+ 3.0 + 2.0
Clinical signs Heart rate 74-95 beats/min
95 beats/min Pain on lower limb deep vein at palpation and unilateral edema
+ 3.0 + 5.0 + 4.0
Total
Clinical probability Low Intermediate High
0 – 3
4 – 10
11.0

Turner 15
REFERENCES
1. Beckman MG, Hooper WC, Critchley SE, Ortel TL. Venous thromboembolism: a public health concern. Am J Prev Med. 2010;38(4):S495-S501.
2. Meyer NJ, Schmidt GA. Chapter 27. Pulmonary Embolic Disorders: Thrombus, Air, and Fat. In: Hall JB, Schmidt GA, Wood LD, eds. Principles of Critical Care. 3rd ed. New York: McGraw-Hill; 2005. http://www.accessmedicine.com.libproxy.uthscsa.edu/content.aspx?aID=2285540. Accessed December 28, 2012.
3. Centers for Disease Control and Prevention. Deep Vein Thrombosis/ Pulmonary Embolism. Data & Statistics. Available at: http://www.cdc.gov/ncbddd/dvt/data.html. Accessed December 28, 2012.
4. Schneider D, Lilienfeld DE, Im W. The epidemiology of pulmonary embolism: racial contrasts in incidence and in-hospital case fatality. J Natl Med Assoc. 2006;98(12):1967-1972.
5. Witt DM, Nutescu EA, Haines ST. Chapter 26. Venous Thromboembolism. In: Talbert RL, DiPiro JT, Matzke GR, Posey LM, Wells BG, Yee GC, eds. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw-Hill; 2011. http://www.accesspharmacy.com/content.aspx?aID7973333. Accessed December 28, 2012.
6. Kline JA. Chapter 60. Thromboembolism. In: Tintinalli JE, Stapczynski JS, Cline DM, Ma OJ, Cydulka RK, Meckler GD, eds. Tintinalli's Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York: McGraw-Hill; 2011. http://www.accessmedicine.com.libproxy.uthscsa.edu/content.aspx?aID=6355989. Accessed December 28, 2012.
7. Kyrle PA, Eichinger S. Deep vein thrombosis. Lancet. 2005;365:1163-1174. 8. Dalen JE. Pulmonary Embolism: What Have We Learned Since Virchow? CHEST. 2002;122(4):1440-1456. 9. Tapson VF. Thrombolytic therapy in acute pulmonary embolism. Curr Opin Cardiol. 2012;27(6):585-591. 10. Kurkciyan I, Meron G, Sterz F, et al. Pulmonary embolism as a cause of cardiac arrest: presentation and outcome.
Arch Intern Med. 2000;160(10):1529-1535. 11. Dalen JE, Alpert JS. Natural history of pulmonary embolism. Prog Cardiovasc Dis. 1975;17(4):259-270. 12. Goldhaber SZ. Chapter 262. Deep Venous Thrombosis and Pulmonary Thromboembolism In: Longo DL, Fauci AS,
Kasper DL, Hauser SL, Jameson JL, Loscaizo J, eds. Harrison's Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012. http://www.accessmedicine.com.libproxy.uthscsa.edu/content.aspx?aID=9128812. Accessed December 29, 2012.
13. Ramzi DW, Leeper KV. DVT and pulmonary embolism: Part I. Diagnosis. Am Fam Physician. 2004;69(12):2829-2836.
14. Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123(16):1788-1830.
15. Zamanian RT, Gould MK. Effectiveness and cost effectiveness of thrombolysis in patients with acute pulmonary embolism. Curr Opin Pulm Med. 2008;14(5):422-426.
16. Fengler BT, Brady WJ. Fibrinolytic therapy in pulmonary embolism: an evidence-based treatment algorithm. Am J Emerg Med. 2009;27(1):84-95.
17. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST. Feb 2012;141(2):419S-494S.
18. Ramzi DW, Leeper KV. DVT and pulmonary embolism: Part II. Treatment and prevention. Am Fam Physician. 2004;69(12):2841-2848.
19. Vyas PA, Donato AA. Thrombolysis in acute pulmonary thromboembolism. South Med J. 2012;105(10):560-570. 20. Genentech, Inc. Activase® Prescribing Information. Available at:
http://www.gene.com/download/pdf/activase_prescribing.pdf. Accessed December 30, 2012. 21. CSL Behring Canada, Inc. Streptase® Prescribing Information. Available at:
http://www.cslbehring.ca/docs/831/938/Streptase_app%2029mar07.pdf. Accessed December 30, 2012. 22. Abbott Laboratories, Inc. Abbokinase® Prescribing Information. Available at:
http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/ucm080776.pdf. Accessed December 30, 2012.
23. Daley MJ, Lat I. Clinical controversies in thrombolytic therapy for the management of acute pulmonary embolism. Pharmacotherapy. 2012;32(2):158-172.
24. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353:1386-1389.

Turner 16
25. Hospira, Inc. Retavase® Prescribing Information. Available at: http://www.retavase.com/pdf/Retavase_PI.pdf. Accessed January 12, 2013.
26. Genetech, Inc. TNKase® Prescribing Information. Available at: http://www.gene.com/download/pdf/tnkase_prescribing.pdf. Accessed January 12, 2013.
27. Papastylianou A, Mentzelopoulos S. Current pharmacological advances in the treatment of cardiac arrest. Emerg Med Int. 2012;2012:815-857.
28. Centers for Disease Control and Prevention. State-Specific Mortality from Sudden Cardiac Death - United States, 1999. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5106a3.htm. Accessed November 25, 2012.
29. Myerburg RJ, Castellanos A. Chapter 273. Cardiovascular Collapse, Cardiac Arrest, and Sudden Cardiac Death In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison's Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012. http://www.accessmedicine.com.libproxy.uthscsa.edu/content.aspx?aID=9106203. Accessed December 29, 2012.
30. Bottiger BW, Arntz HR, Chamberlain DA, et al. Thrombolysis during resuscitation for out-of-hospital cardiac arrest. NEJM. 2008;359(25):2651-2662.
31. Neumar RW, Otto CW, Link MS, et al. Part 8: Adult Advanced Cardiovascular Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18):S729-S767.
32. Bottiger BW, Motsch J, Bohrer H, et al. Activation of blood coagulation after cardiac arrest is not balanced adequately by activation of endogenous fibrinolysis. Circulation. 1995;92(9):2572-2578.
33. Fischer M, Hossmann KA. No-reflow after cardiac arrest. Intensive Care Med. 1995;21(2):132-141. 34. Langdon RW, Swicegood WR, Schwartz DA. Thrombolytic therapy of massive pulmonary embolism during
prolonged cardiac arrest using recombinant tissue-type plasminogen activator. Ann Emerg Med. 1989;18(6):678-680.
35. Spohr F, Bottiger BW. Safety of thrombolysis during cardiopulmonary resuscitation. Drug Saf. 2003;26(6):367-379.
36. Ruiz-Bailen M, Aguayo-de-Hoyos E, Serrano-Corcoles MC, et al. Thrombolysis with recombinant tissue plasminogen activator during cardiopulmonary resuscitation in fulminant pulmonary embolism. A case series. Resuscitation. 2001;51(1):97-101.
37. Abu-Laban RB, Christenson JM, Innes GD, et al. Tissue plasminogen activator in cardiac arrest with pulseless electrical activity. NEJM. 2002;346(20):1522-1528.
38. Vanden Hoek TL, Morrison LJ, Shuster M, et al. Part 12: Cardiac Arrest in Special Situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18):S829-861.
39. Konstantinides S, Geibel A, Heusel G, et al. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. NEJM. 2002;347(15):1143-1150.
40. Sharifi M, Bay C, Skrocki L, al. e. Moderate Pulmonary Embolism Treated With Thrombolysis (from the "MOPETT" Trial). Am J Cardiol. 2013;111(2):273-277.
41. Torbicki A, Perrier A, Konstantinides S, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008;29(18):2276-2315.