-
8/17/2019 CKD Dengan Dislipidemia
1/9
Clinical Therapeutics/Volume 36, Number 8, 2014
Comparison of the Ef cacy and Safety Prole of
MorningAdministration of Controlled-release Simvastatin
VersusEvening Administration of Immediate-release Simvastatin
in Chronic Kidney Disease Patients With Dyslipidemia Yong
Jin Yi, MD1; Hyo Jin Kim, MD1; Sang Kyung Jo, MD2; Sung Gyun Kim,
MD3; Young Rim Song, MD3; Wookyung Chung, MD4; Kum Hyun Han,
MD5;Chang Hwa Lee, MD6; Young-Hwan Hwang, MD7; and Kook-Hwan Oh,
MD, PhD1
1Department of Internal Medicine, Seoul National University
Hospital, Seoul, Republic of Korea; 2Department of Internal
Medicine, Korea University Medical College, Seoul, Republic of
Korea; 3Divisionof Nephrology, Department of Internal
Medicine, Hallym University Sacred Heart Hospital, Anyang,Republic
of Korea; 4Department of Internal Medicine, Gachon
University of Medicine and Science,
Incheon, Republic of Korea;
5
Department of Internal Medicine, Inje University Ilsan Paik
Hospital, Ilsan,Republic of Korea; 6Department of Internal
Medicine, Hanyang University, Seoul, Republic of Korea;
and 7 Department of Internal Medicine, Eulji General
Hospital, Eulji University, Seoul, Republic of Korea
ABSTRACT
Purpose: Evening administration of the conven-
tional immediate-release (IR) formulation of simvas-
tatin is recommended because of its short half-life (1.9
hours). In a healthy population, morning administra-
tion of a controlled-release (CR) formulation of
simvastatin was shown to have equivalent lipid-
lowering ef cacy and a safety prole similar to thatof
evening doses of IR simvastatin. The present study
aimed to verify noninferiority and to compare the
safety of morning administration of CR simvastatin
with that of evening administration of IR simvastatin
in patients with chronic kidney disease (CKD) who
have dyslipidemia.
Methods: The present study was a prospective,
multicenter, double-blind, Phase IV trial with an
active comparator. We randomly assigned 122 pa-
tients with CKD and dyslipidemia to 1 of 2 drug
administration groups: morning administration of CRsimvastatin
20 mg (test group) and evening admin-
istration of IR simvastatin 20 mg (control group).
After 8 weeks, the treatment outcomes and adverse
effects of the 2 treatments were compared.
Findings: The mean (SD) percentage of change in
serum LDL-C at the end of treatment was –35.1%
(15.7%) for the test group and –35.6% (14.6%) for
the control group. The difference between the 2
groups was not signicant (P ¼ 0.858). The 95% CI
of the difference in the percentage of change of LDL-C
between the test and control groups was –6.0 to 5.0.
There was no difference in the percentage of change of
total cholesterol (–24.3% [12.5%] vs –26.5%
[12.0%], P ¼ 0.317), triglyceride (–10.6%
[35.1%]
vs –12.4% [33.2%], P ¼ 0.575) and
HDL-C (10.2%
[20.7%] vs 4.5% [11.4%], P ¼ 0.064).
Treatment-
related adverse events were similar in both groups (10events in
the test group vs 8 events in the control
group, P ¼ 0.691).
Implications: The ef cacy of morning administra-
tion of CR simvastatin was noninferior to evening
administration of IR simvastatin in patients with
CKD. Furthermore, the safety prole analysis showed
no signicant difference between the 2 treatments.
Morning administration of CR simvastatin is expected
to increase patient compliance and therefore better
control of dyslipidemia in CKD patients. (Clin Ther.
2014;36:1182–
1190) & 2014 The Authors. Publishedby Elsevier
HS Journals, Inc.
Accepted for publication June 2, 2014.
http://dx.doi.org/10.1016/j.clinthera.2014.06.005
0149-2918/$ - see front matter
& 2014 The Authors. Published by Elsevier HS Journals,
Inc. This is an
open access article under the CC BY-NC-ND license
(http://creativecommons.org/licenses/by-nc-nd/3.0/).
1182 Volume 36 Number 8
Downloaded from ClinicalKey.com at ClinicalKey Global Guest
Users May 09, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
http://localhost/var/www/apps/conversion/tmp/scratch_1/dx.doi.org/10.1016/j.clinthera.2014.06.005http://localhost/var/www/apps/conversion/tmp/scratch_1/dx.doi.org/10.1016/j.clinthera.2014.06.005http://localhost/var/www/apps/conversion/tmp/scratch_1/dx.doi.org/10.1016/j.clinthera.2014.06.005http://localhost/var/www/apps/conversion/tmp/scratch_1/dx.doi.org/10.1016/j.clinthera.2014.06.005
-
8/17/2019 CKD Dengan Dislipidemia
2/9
Key words: chronic kidney disease, controlled-
release preparations, drug administration schedule,
dyslipidemia, simvastatin.
INTRODUCTION3-Hydroxy 3-methylglutaryl coenzyme A (HMG-CoA)
reductase inhibitors, also known as statins, are
a highly potent group of agents that reduce serum
LDL-C levels. Previous clinical trials have reported
that statin therapy is benecial for the primary1 and
secondary2–4 prevention of cardiovascular disease,
such as coronary atherosclerosis. Statin therapy is of
particular benet to dyslipidemia patients with
chronic kidney disease (CKD), which is associated
with a high incidence and increased severity of
cardiovascular disease.5 The Kidney Disease Out-
come Quality Initiative guidelines for dyslipidemia6
recommend that lipid-lowering therapy, along with
therapeutic lifestyle modication, should be initiated
for CKD patients with LDL-C levels above 100 mg/
dL. According to the latest meta-analysis of statin
therapy in CKD, all-cause and cardiovascular mortal-
ity was signicantly decreased without increasing
treatment-related adverse effects.7,8
Despite the benecial effects of statin therapy,
patients with chronic diseases who are taking medi-
cations in multiple doses are frequently noncompliant
in taking their medication.9–11 There is a diurnal
variation of plasma LDL-C levels, with the lowest
levels detected in the morning and the highest levels
peaked in the evening.12 Simvastatin is an established
HMG-CoA reductase inhibitor that has been clinically
evaluated in thousands of cases.2,13 In some trials
comparing the ef cacy of morning and evening ad-
ministration of simvastatin, there was signicantly
lower reduction in LDL-C levels when simvastatin
was given in the morning.14 However, taking simvas-
tatin in the evening may increase the complexity of the
dosing regimen, in turn, reducing patient compliance.9
Recently, a controlled-release (CR) simvastatin
formulation was released (Simvast CR tablet*); it
has a longer half-life (11.4 hours) than that of the
conventional immediate-release (IR) formulation (1.9
hours). In a Phase III trial of CR simvastatin, the
formulation was reported to have equivalent ef cacy
and a similar safety prole within the study popula-
tion as those of IR simvastatin.15 We designed a Phase
IV, postmarketing trial of CR simvastatin in CKD
patients. The purposes of the present study were
twofold: (1) to verify in CKD patients whether the
ef cacy of CR simvastatin administered in the
morning was noninferior to that of IR simvastatinadministered in
the evening and (2) to assess whether
a regular dose regimen of CR simvastatin was safe
compared with that of IR simvastatin in CKD
patients.
METHODSThe present study was a prospective, randomized,
double-dummy, double-blind,, multicenter Phase IV
trial that evaluated the ef cacy and safety prole
of
morning administration of CR simvastatin tablets
compared with evening administration of IR simvas-
tatin tablets (Zocor tablet†) in CKD patients. The
participants were recruited from the following
hospitals in South Korea: Seoul National University
Hospital, Gachon University Gil Medical Center,
Seoul Eulji General Hospital, Hallym University
Sacred Heart Hospital, Inje University Ilsan Paik
Hospital, Hanyang University Seoul Hospital, and
Korea University Anam Hospital. Before entering the
study, all patients provided written informed consent.
The institutional review boards of each hospital
approved the study design, and the study wasperformed in
accordance with the Declaration of
Helsinki and its amendments.
PatientsThe study was conducted from December 2010 to
May 2012. Patients, 20 to 75 years of age, with CKD
stage 3, 4, or 5 (predialysis) were enrolled if their
serum LDL-C levels were between 100 and 220 mg/dL
and their serum triglyceride (TG) levels were o400
mg/dL. The reasons for exclusion of patients were as
follows: previous hypersensitivity to components of
any HMG-CoA reductase inhibitor, drug abuse and
alcohol consumption of least 14 standard units per
week,16,17 impaired liver function (serum aspartate
aminotransferase or alanine aminotransferase level of
42 times the upper limit of normal), uncontrolled
diabetes (HgA1c level of 49.0%),
uncontrolled
* Trademark: Simvast CR tablet s, Hanmi Pharmaceutical
Co,Ltd, Seoul, Republic of Korea.
† Trademark: Zocor s tablet, Merck & Co,
Inc, WhitehouseStation, New Jersey.
Y.J. Yi et al.
August 2014 1183
Downloaded from ClinicalKey.com at ClinicalKey Global Guest
Users May 09, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
http://-/?-http://-/?-http://-/?-http://-/?-
-
8/17/2019 CKD Dengan Dislipidemia
3/9
hypertension (systolic blood pressure 4160 mm Hg
or diastolic 4100 mm Hg at screening), congestive
heart failure with symptoms of New York Heart
Association Functional Class III or IV symptoms,
unstable angina, myocardial infarction, history of
percutaneous coronary intervention or bypass surgery,
cerebral infarction or transient ischemic accident anddeep
venous thrombosis in the past 6 months, active
peptic ulcer disease, gastrointestinal disease that might
inuence the absorption of the test drug, current
therapy with an immunosuppressant, and malignancy.
The following drugs were prohibited during the entire
study period: other
HMG-CoA reductase inhibitors, nicotinic acid de-
rivatives, omega-3 fatty acid
formulations, bric acids, peroxisome proliferator-
activated receptor γ agents, and bile acid
sequestrants.
Screening and Treatment PeriodAt visit 1, all screened patients
were instructed to
discontinue lipid-lowering medication during the
screening period and to initiate therapeutic lifestyle
changes (TLCs), including diet modication, for 4
weeks. Participants’ serum lipid levels were reassessed
after 4 weeks of TLCs (visit 2). At visit 2, patients who
met the above LDL-C and TG criteria were randomly
assigned to 2 drug administration groups: CR simvas-
tatin (test group) and IR simvastatin (control group).
We used a xed-allocation (1:1) block-randomizationmethod.
The size of each block was 4 patients. The
study referral institutions completed the random
assignment of patients. All clinicians and patients
remained blinded until the end of the study.
During 8 weeks of treatment, patients in the test
group took a CR formulation of simvastatin as a 20-
mg tablet in the morning and a placebo of IR
simvastatin in the evening. Conversely, patients in the
control group took a placebo of CR simvastatin in
the morning and an IR simvastatin 20-mg tablet in the
evening. Each placebo was prepared in the same colorand shape as
the corresponding drugs so that patients
and physicians could not differentiate them (double-
blinding). Four weeks after randomization (visit 3), the
participants were contacted by telephone to check for
any adverse events or concomitant medications. If any
adverse events were reported, the participants were
asked to return to the outpatient clinic for an evalua-
tion. At 8 weeks (visit 4), the patients were evaluated
for drug compliance, ef cacy, and safety prole
pertaining to the treatment. Patients who dropped out
after randomization (1 subject in the test group and 2
in the control group) were also encouraged to visit for
the nal (ef cacy) laboratory tests at visit 4.
Efficacy and Safety Profile Assessment LDL-C, HDL-C, total
cholesterol (TC), and TGlevels in 12-hour fasting blood samples
were deter-
mined at week 0 (baseline) and week 8 (Wako Pure
Chemical Industries Ltd, Osaka, Japan). The primary
end point of the study was the percentage of change in
LDL-C levels over the 8 weeks of treatment. The
secondary end points were the percentage of change in
TC, HDL-C, and TG levels. For the safety prole
assessment, vital signs and laboratory parameters
were monitored, including hemoglobin level; hema-
tocrit, white blood cell, and platelet counts; trans-aminase,
γ-glutamyl transferase, serum creatinine,
blood glucose, and creatine kinase levels; urinalysis;
and ECG.
Statistical AnalysisThe aim of the study was to conduct a
noninfer-
iority comparison between a morning dose of CR
simvastatin and an evening dose of IR simvastatin.18
The margin of difference for noninferiority was
regarded as o–6.5%, according to previous
studies.19,20
When setting the statistical power at80% and the α
value at 0.05, the calculated number
of enrolled patients required was 52 in each group. An
assumed a dropout rate of 15% gave a nal sample
size of 61 patients in each group. The equation for
sample size determination was as follows:
n ¼ 2ðZα þ Z β Þ2σ 2
ðð μT μC Þ d Þ2
Zα = the limit value of α error
(0.05) in normal
distribution, Zβ = the limit value of β
error (0.20) in
normal distribution, d = noninferiority
margin (6.5%),and σ ¼ SD.
The primary and secondary end-point analyses
were based on the intention-to-treat (ITT) population,
which included any enrolled patients who took at least
1 dose of the medication and underwent ef cacy
testing at week 8. The safety prole analysis was
based on the safety set, which was dened as the
group of patients who had taken at least 1 tablet of
the study drug.
Clinical Therapeutics
1184 Volume 36 Number 8
Downloaded from ClinicalKey.com at ClinicalKey Global Guest
Users May 09, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/17/2019 CKD Dengan Dislipidemia
4/9
To compare the percentage of change in LDL-C
levels, the primary end point, the Student t
test was
performed to calculate the 95% CI of the percentage
of difference between the test and control groups. If
the 95% CI did not exceed the set point of the
noninferiority margin (–6.5%), the ef cacy of CR
simvastatin was considered to be noninferior. Toassess the
signicance of the change in LDL-C, TC,
HDL-C, and TG levels before and after treatment, the
paired t test (to compare within groups) and
Student t
test (to compare between groups) were used. In an
analysis of participant demography, continuous vari-
ables that followed a normal distribution were pre-
sented as mean (SD) and were analyzed using the
Student t test; categorical values were
represented by
number and percentage and were analyzed by the χ2
or Fisher exact test. P o 0.05 was dened as
statisti-
cally signicant. All statistical analyses were performedusing
SPSS 19.0 (SPSS Inc, an IBM company, Chicago,
Illinois).
RESULTSA total of 122 patients were randomly assigned to
either the test (n = 62) or control (n
= 60) group. On
completion, 118 patients (59 for each group) were
included in the ITT population, after exclusion of 1
subject in the control group who refused to participate
immediately after enrollment without taking the study
drug and 3 in the test group who failed to undergo the
ef cacy evaluation blood test after 8 weeks of medi-
cation. Forty-ve patients in the test group and 47 inthe control
group completed the study (Figure 1).
Baseline CharacteristicsOf the 118 patients assigned to
treatment, 92
completed the 8-week trial. With regard to age, sex,
weight, CKD stage, alcohol consumption, underlying
disease, previous medication (including statins, aspirin,
angiotensin-converting enzyme inhibitors/angiotensin re-
ceptor blockers, β-blockers, calcium channel
blockers,
and loop and thiazide diuretics), and baseline laboratory
test results (TC, TG, LDL-C, HDL-C, and creatininelevels), there
were no statistically signicant differences
between the test and control groups (Table I).
Changes in the Lipid ProfileBoth the morning dose of CR
simvastatin and
evening dose of IR simvastatin signicantly lowered
Screening : Patients with dyslipidemia and CKD (n = 168)
12 rejected TLC
122 subjects randomized
118 patients at week 0 : ITT population
Discontinued administration : 1
Drug compliance < 75% : 4 Violate prohibited drug :
7
Others : 2
Discontinued administration : 2
Drug compliance < 75% : 4 Violate prohibited drug :
5
Others : 1
At week 8
PP popualtion (N=92)
45 completed study 47 completed study
59 received morning administration
of CR simvastatin
59 received evening administration
of IR simvastatin
1 refused after randomization
3 failed to perform efficacy test
34 were in exclusion criteria
Figure 1. Flow chart of the study. CKD ¼ chronic
kidney disease; CR ¼ controlled-release;
IR ¼ immediate-release; ITT ¼
intention-to-treat; PP ¼ per-protocol; TLC ¼
therapeutic lifestyle change.
Y.J. Yi et al.
August 2014 1185
Downloaded from ClinicalKey.com at ClinicalKey Global Guest
Users May 09, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/17/2019 CKD Dengan Dislipidemia
5/9
blood levels of LDL-C, TC, and TG. Levels of HDL-Csignicantly
increased in both groups. A between-
group analysis of HDL-C level after treatment re-
vealed a signicantly higher HDL-C level in the test
group than in the control group (P ¼ 0.012).
There
were no between-group differences in LDL-C, TC, or
TG level after treatment (Table II).
Patient LDL-C levels decreased by 35.1% (SD
15.7%) in the test group and by 35.6% (SD 14.6%)
in the control group (P ¼ 0.858). The 95% CI of
the
difference in the percentage of change in LDL-C levelbetween the
test and control groups was (–6.0% to
5.0%), which did not meet the predened noninferiority
margin (–6.5%) in a 1-tailed signicance test (Figure 2).
Adverse EventsOne patient in the test group discontinued the
study
because of a side effect (dizziness) of the test drug. The
medication was well tolerated by all other participants.
The number and incidence of total adverse events were
Table I. Baseline characteristics of the
intention-to-treatment population in the trial.
Characteristic
Test Group
(n ¼ 59)
Control Group
(n ¼ 59)
Total
(N ¼ 118) P
Age, y, mean (SD) 56.9 (10.5) 57.0 (12.1) 57.0 (11.3) 0.978
Sex, male, no. (%) 28 (47.5) 29 (55.1) 57 (48.3)
0.853 Weight, kg, mean (SD) 64.3 (11.1) 63.7 (10.4) 64.0
(10.8) 0.764
CKD stage, no. (%) 0.827
3 43 (72.9) 40 (67.8) 83 (70.3)
4 15 (25.4) 18 (30.5) 33 (28.0)
5 1 (1.7) 1 (1.7) 2 (1.7)
Alcohol consumption, no. (%) 0.387
None 47 (80.7) 43 (72.9) 90 (76.3)
Present 12 (20.3) 16 (27.1) 28 (23.7)
Underlying disease, no. (%)
Hypertension 52 (88.1) 54 (91.5) 106 (89.8) 0.542
Diabetes mellitus 24 (40.7) 18 (30.5) 42 (35.6) 0.249Ischemic
heart disease 3 (5.1) 1 (1.7) 4 (3.4) 0.618
Stroke 4 (6.8) 2 (3.4) 6 (5.0) 0.579
Previous statin use, no. (%) 9 (15.2) 9 (15.2) 18 (15.2)
1.000
Medication, no. (%)
Aspirin 20 (33.9) 16 (27.1) 36 (30.5) 0.424
ACEi/ARB 52 (88.1) 52 (88.1) 104 (88.1) 1.000
β-Blocker 18 (30.5) 15 (25.4) 33 (28.0) 0.538
Calcium channel blocker 33 (59.9) 24 (40.7) 57 (48.3) 0.097
Loop diuretics 10 (16.9) 9 (15.3) 19 (16.1) 0.802
Thiazide 10 (16.9) 6 (10.1) 16 (13.5) 0.282
Baseline laboratory tests, mg/dL, mean (SD) Total
cholesterol 228.7 (36.8) 220.0 (36.4) 224.4 (36.8) 0.199
LDL-C 143.9 (28.1) 137.0 (28.4) 140.5 (28.3) 0.186
HDL-C 46.9 (14.5) 48.8 (13.5) 47.8 (14.0) 0.464
Triglycerides 190.3 (73.0) 167.6 (70.7) 178.9 (72.5)
0.090
Creatinine 2.0 (0.9) 2.0 (0.8) 2.0 (0.8) 0.816
ACEi ¼ angiotensin-converting enzyme inhibitor; ARB
¼ angiotensin receptor blocker; CKD ¼
chronic kidney disease.
Clinical Therapeutics
1186 Volume 36 Number 8
Downloaded from ClinicalKey.com at ClinicalKey Global Guest
Users May 09, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
-
8/17/2019 CKD Dengan Dislipidemia
6/9
similar in both groups. In terms of a causal relation-
ship, the adverse events were classied into 5 catego-
ries: denitely related, probably related, possibly
related, uncertainly related, and not related to treat-
ment. Each category was further dened according to
the chronological order of administration, a response
of discontinuation or redosing, and other signicant
causes of the adverse events.
Treatment-related adverse events are shown in Table
III. In total, 10 patients in the test group and 8 in the
control group reported treatment-related adverse events.
In 1 patient in the control group both edema andnausea developed
during the trial. There was no differ-
ence between the 2 groups in the incidence of treatment-
related adverse events (P ¼ 0.691, by the χ2
test).
DISCUSSIONThe present study was designed as a double-blind,
prospective, randomized clinical trial with an active
comparator. It compared the ef cacy and safety
prole of morning administration of a CR simvastatin
formulation with those of IR simvastatin in patients
with underlying CKD. The difference in the percent-age of change
in LDL-C level did not meet the
predened noninferiority margin. This nding sug-
gests that CR simvastatin has an ef cacy similar to
that of IR simvastatin. In the Scandinavian Simvasta-
tin Survival Study (4S),2 simvastatin doses of 20 to 40
mg/d lowered the LDL-C level by 35%, which was
similar to results seen in the present study of IR
simvastatin ef cacy. There were also no signicant
differences in the incidence of treatment-related ad-
verse events.
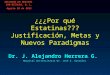
LDL-C40
20
0
–20 % c
h a n g e
–40
–60
Test group
–35.1 ±15.7%
–35.6 ±14.6%
Control group
TC TG HDL-C
–24.3 ±12.5%
–26.5 ±12.0%
–10.6 ±35.1%
–12.4 ±33.2%
–10.2 ±20.7%
–4.5 ±11.4%
Figure 2. Percentage of change in lipid para-meters after
treatment. TC ¼ totalcholesterol; TG ¼
triglycerides.
Table II. Profiles and differences of fasting lipids at
baseline and 8 weeks after treatment.
Test Group (n ¼ 59) Control Group (n ¼
59)P (Between
Groups After
Treatment)Baseline
8 Weeks After
Treatment
P (Within
Group) Baseline
8 Weeks After
Treatment
P (Within
Group)
Total cholesterol,
mg/dL
228.7 (36.8) 172.3 (35.1) o0.001 220.0 (36.4) 160.6
(31.9) o0.001 0.587
Change, %* −24.3 (12.5) o0.001 −26.5 (12.0)
o0.001 0.317
Triglycerides,mg/dL
190.3 (73.0) 159.8 (65.9) o0.001 167.6 (70.7) 136.6
(61.6) o0.001 0.963
Change, %* −10.6 (35.1) 0.023 −12.4 (33.2) 0.001
0.575LDL-C, mg/dL 143.9 (28.1) 92.8 (25.7)
o0.001 137.0 (28.4) 87.5 (23.2) o0.001 0.722
Change, %* −35.1 (15.7) o0.001 −35.6 (14.6)
o0.001 0.858HDL-C, mg/dL 46.9 (14.5) 51.0 (15.6) 0.001 48.8 (13.5)
50.7 (14.3) 0.011 0.012
Change, %* 10.2 (20.7) o0.001 4.5 (11.4) 0.003 0.064
Values shown are mean (SD).*Percentage of change from
baseline to end of treatment phase.
Y.J. Yi et al.
August 2014 1187
Downloaded from ClinicalKey.com at ClinicalKey Global Guest
Users May 09, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/17/2019 CKD Dengan Dislipidemia
7/9
With regard to the secondary end points, the HDL-
C level after treatment was higher in the test group
than in the control group. However, the increment of HDL-C
after treatment was only marginally greater in
the test group. It remains to be investigated in a future
study whether slow controlled release of simvastatin is
more benecial in terms of HDL-C than its immediate
release.
Dyslipidemia is one of the most important manage-
ment issues for patients with CKD. It is known that an
abnormality of plasma lipoprotein metabolism in
kidney disease causes dyslipidemia,21,22 and it is also
suggested that lipid toxicity causes glomerular and
tubulointerstitial injury, thereby generating a
viciouscycle.23,24 A meta-analysis of randomized, controlled
trials reported that lipid lowering preserved the
glomerular ltration rate and reduced proteinuria in
patients with renal disease.25
Although 2 large-scale clinical trials in patients
with CKD have reported conicting results for the
effects of statin therapy on cardiovascular outcomes
and all-cause mortality,26,27 1 recent meta-analysis
reported that statin therapy reduces the risk of major
cardiovascular events in patients with CKD.8 Such
evidence suggests that statin treatment could be
justied for predialysis in patients with CKD.Simvastatin is an
established HMG-CoA reductase
inhibitor that has been studied in 2 large-scale out-
come trials, the Heart Protection Study and the 4S.2,13
These 2 landmark studies showed that simvastatin
treatment reduced coronary heart disease and all-
cause mortality as their primary outcome, and con-
rmed the long-term safety prole.
The half-life of the active metabolite of conven-
tional IR simvastatin is 1.9 hours.28 A few studies on
the administration time of IR simvastatin have
reported that lowering of serum LDL-C levels is morepronounced
with evening versus morning administra-
tion.14,29,30 According to these results, it is recom-
mended to take IR simvastatin in the evening.31
However, given that CKD patients are likely to take
multiple medications such as aspirin, antihypertensive
drugs, diuretics, and phosphate binders, evening
administration could render the medication sche-
dule more complex and might compromise patient
compliance.10,11 The present study showed that the
Table III. Treatment-related adverse events among the
study participants.
Test Group
(n ¼ 62*)
Control Group
(n ¼ 59)
Total
(N ¼ 121*) P
Gastrointestinal disorders
Nausea 2 (3.2) 2 (3.4) 4 (3.3)Abdominal pain 0 (0) 3 (5.1) 3
(2.5)
Diarrhea 1 (1.6) 0 (0) 1 (0.8)
Musculoskeletal disorders
Myalgia 1 (1.6) 2 (3.4) 3 (2.5)
Central nervous system disorders
Headache 2 (3.2) 0 (0) 2 (1.7)
Dizziness 1 (1.6) 0 (0) 1 (0.8)
Urinary system disorders
Albuminuria 2 (3.2) 0 (0) 2 (1.7)
Other disorders
Edema 1 (1.6) 1 (1.7) 2 (1.7) Total events 10 (16.1) 8
(13.6)† 18 (14.9)† 0.691
Values shown are number (%).* Three patients who took
the test drug at least once but did not undergo ef cacy
laboratory tests were also included in thesafety analysis.†One
patient in the control group experienced both edema and nausea
during medication.
Clinical Therapeutics
1188 Volume 36 Number 8
Downloaded from ClinicalKey.com at ClinicalKey Global Guest
Users May 09, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/17/2019 CKD Dengan Dislipidemia
8/9
therapeutic ef cacy of morning administration of CR
simvastatin is equivalent to that of evening adminis-
tration of IR simvastatin in terms of lowering LDL-C,
TC, and TG levels. Therefore, morning administration
of CR simvastatin could simplify the dosing schedule
and improve the compliance of patients with CKD
who are taking multiple medications.According to a previous
study,32 common adverse
effects of simvastatin include gastrointestinal symptoms
such as constipation, abdominal pain, and atulence. In
the present study, there was no difference in the
frequency of gastrointestinal side effects between the
test and control groups. Myopathy is a common
adverse effect of HMG-CoA reductase inhibitors. The
denition of myopathy in the literature is broad,
ranging from mild muscular pain to severe rhabdo-
myolysis. In a previous study,32 myopathy leading to
the discontinuation of simvastatin developed in 0.08%of
patients. It is also known that the frequency of severe
biochemical abnormalities (serum creatine kinase level
410 times the upper normal level) is very low.33 In this
study, overall, there were 3 cases of myalgia (2.5%)
related to statin administration, and no difference was
reported in the frequency of myalgia between the 2
groups. Only 1 patient (0.8%) in the test group
exhibited an increase in creatine kinase 410 times the
upper limit of normal at the end of treatment, which
returned to a normal level after completing treatment.
The present study has the following limitations: (1)The ITT
population was smaller than we expected.
This was due to a higher dropout rate and several
patients who failed to undergo the ef cacy test at the
end of treatment. (2) Dietary compliance of both
groups was assumed to be equivalent because both
groups were equally given TLC during the screening
and follow-up periods.
CONCLUSIONSFor patients with CKD, morning administration of
CR
simvastatin and evening administration of IR simvas-tatin didn't
show statistically signicant differences in
safety prole or ef cacy. Morning administration
of
CR simvastatin may simplify the administration sched-
ule and improve the compliance of patients with CKD
who are taking multiple medications.
ACKNOWLEDGMENTSThis study was funded by Hanmi Pharmaceutical
Company Ltd., Seoul, Republic of Korea.
Dr. Yi participated in the implementation of the
study, data collection and analysis and manuscript
preparation. Dr. H.J. Kim contributed to the data
collection and analysis. Dr. Oh had a substantial
contribution to the design of the study, data analysis
and manuscript preparation and overviewing. Drs. Jo,
S.G. Kim, Song, Chung, Han, Lee and Hwangparticipated in the
patient recruitment, implementa-
tion of the study, safety monitoring and manuscript
overviewing.
CONFLICTS OF INTEREST The authors have indicated that they
have no conicts
of interest regarding the content of this article.
REFERENCES1. Shepherd J, Cobbe SM, Ford I, et al.
Prevention of
coronary heart disease with pravastatin in men with
hypercholesterolemia. West of Scotland Coronary Preven-
tion Study Group. N Engl J Med .
1995;333:1301–1307.
2. Randomised trial of cholesterol lowering in 4444
patients
with coronary heart disease: the Scandinavian Simvastatin
Survival Study (4S). Lancet . 1994;344:1383–1389.
3. Sacks FM, Pfeffer MA, Moye LA, et al. The effect
of
pravastatin on coronary events after myocardial infarction
in patients with average cholesterol levels. Cholesterol and
Recurrent Events Trial investigators. N Engl J Med .
1996;
335:1001–
1009.4. Prevention of cardiovascular events and death
with
pravastatin in patients with coronary heart disease and
a broad range of initial cholesterol levels. The Long-Term
Intervention with Pravastatin in Ischaemic Disease (LIPID)
Study Group. N Engl J Med . 1998;339:1349–1357.
5. Levey AS, Beto JA, Coronado BE, et al. Controlling
the
epidemic of cardiovascular disease in chronic renal
disease: what do we know? What do we need to learn?
Where do we go from here? National Kidney Foundation
Task Force on Cardiovascular Disease. Am J Kidney
Dis.
1998;32:853–906.
6. Kasiske B, Cosio F, Beto J, et al. Clinical practice
guide-lines for managing dyslipidemias in kidney
transplant
patients: a report from the Managing Dyslipidemias in
Chronic Kidney Disease Work Group of the National
Kidney Foundation Kidney Disease Outcomes Quality
Initiative. Am J Transplant . 2004;4:13–53.
7. Barylski M, Nikfar S, Mikhailidis DP, et al.
Statins
decrease all-cause mortality only in CKD patients not
requiring dialysis therapy –a meta-analysis of 11
random-
ized controlled trials involving 21,295 participants.
Phar-
macol Res. 2013;72:35–44.
Y.J. Yi et al.
August 2014 1189
Downloaded from ClinicalKey.com at ClinicalKey Global Guest
Users May 09, 2016.For personal use only. No other uses without
permission. Copyright ©2016. Elsevier Inc. All rights reserved.
http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref7http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref6http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref5http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref4http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref3http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref2http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref1
-
8/17/2019 CKD Dengan Dislipidemia
9/9
8. Hou W, Lv J, Perkovic V, et al.
Effect of statin therapy on cardio-
vascular and renal outcomes in
patients with chronic kidney dis-
ease: a systematic review and
meta-analysis. Eur Heart J.
2013;34:1807–
1817.9. Sung JC, Nichol MB, Venturini F,
Bailey KL, McCombs JS, Cody M.
Factors affecting patient compli-
ance with antihyperlipidemic medi-
cations in an HMO population. Am
J Manag Care. 1998;4:1421–1430.
10. Osterberg L, Blaschke T. Adherence
to medication. N Engl J Med .
2005;353:487–497.
11. Claxton AJ, Cramer J, Pierce C. A
systematic review of the associa-
tions between dose regimens andmedication compliance.
Clin Ther .
2001;23:1296–1310.
12. Miettinen T. Diurnal variation of
LDL and HDL cholesterol. Ann Clin
Res. 1980;12:295–298.
13. Heart Protection Study Collaborative
Group. MRC/BHF Heart Protection
Study of cholesterol lowering with
simvastatin in 20,536 high-risk indi-
viduals: a randomised placebo-
controlled trial. Lancet . 2002;360:
7–
22.14. Saito Y, Yoshida S, Nakaya N, Hata
Y, Goto Y. Comparison between
morning and evening doses of sim-
vastatin in hyperlipidemic subjects.
A double-blind comparative study.
Arterioscler Thromb Vasc Biol . 1991;11:
816–826.
15. Kim SH, Kim MK, Seo HS, et al.
Ef cacy and safety of morning
versus evening dose of controlled-
release simvastatin tablets in pa-
tients with hyperlipidemia: a rando-mized, double-blind,
multicenter
phase III trial. Clin Ther . 2013;35:
1350–1360. e1.
16. Bush K, Kivlahan DR, McDonell MB,
Fihn SD, Bradley KA. The AUDIT
alcohol consumption questions
(AUDIT-C): an effective brief screen-
ing test for problem drinking. Am-
bulatory Care Quality Improvement
Project (ACQUIP). Alcohol Use
Disorders Identication Test. Arch
Intern Med . 1998;158:1789–1795.
17. Bradley KA, Bush KR, McDonell MB,
Malone T, Fihn SD, Project ACQI.
Screening for problem drinking. J Gen
Intern Med . 1998;13:379–389. doi:
10.1046/j.1525-1497.1998.00118.x .18. Products CfPM.
Guideline on the
choice of the non-inferiority mar-
gin. London (UK): European Med-
icines Agency (EMEA); 2005.
19. Sbarouni E, Flevari P, Kroupis C,
Kyriakides ZS, Koniavitou K, Kre-
mastinos DT. The effects of ralox-
ifene and simvastatin on plasma
lipids and endothelium. Cardiovasc
Drugs Ther . 2003;17:319–323.
20. Jang SB, Lee YJ, Lim LA, et al.
Pharmacokinetic comparison of controlled-release and
immediate-
release oral formulations of simvas-
tatin in healthy Korean subjects:
A randomized, open-label, paral-
lel-group, single-and multiple-dose
study. Clin Ther . 2010;32:206–216.
21. Kaysen GA. Lipid and lipoprotein
metabolism in chronic kidney dis-
ease. J Ren Nutr . 2009;19:73–77.
22. Tsimihodimos V, Dounousi E,
Siamopoulos KC. Dyslipidemia in
chronic kidney disease: an approachto pathogenesis and
treatment. Am
J Nephrol . 2008;28:958–973.
23. Moorhead JF, Chan MK, El-Nahas
M, Varghese Z. Lipid nephrotoxicity
in chronic progressive glomerular
and tubulo-interstitial disease.
Lancet . 1982;2:1309–1311.
24. Gyebi L, Soltani Z, Reisin E. Lipid
nephrotoxicity: new concept for an
old disease. Curr Hypertens Rep. 2012;
14:177–181.
25. Fried LF, Orchard TJ, Kasiske BL.
Effect of lipid reduction on the pro-
gression of renal disease: a meta-
analysis. Kidney Int . 2001;59:260–269.
26. Baigent C, Landray MJ, Reith C, et al.
The effects of lowering LDL cholesterol
with simvastatin plus ezetimibe inpatients with chronic kidney
disease
(Study of Heart and Renal Protection):
a randomised placebo-controlled
trial. Lancet . 2011;377:2181–2192.
27. Fellström BC, Jardine AG, Schmieder
RE, et al. Rosuvastatin and cardio-
vascular events in patients under-
going hemodialysis. N Engl J Med .
2009;360:1395–1407.
28. Vickers S, Duncan C, Chen I-W,
Rosegay A, Duggan D. Metabolic
disposition studies on simvastatin, acholesterol-lowering
prodrug. Drug
Metab Dispos. 1990;18:138–145.
29. Lund TM, Torsvik H, Falch D,
Christophersen B, Skardal R, Gul-
lestad L. Effect of morning versus
evening intake of simvastatin on the
serum cholesterol level in patients
with coronary artery disease. Am J
Cardiol . 2002;90:784–786.
30. Wallace A, Chinn D, Rubin G. Taking
simvastatin in the morning compared
with in the evening: randomisedcontrolled trial. BMJ.
2003;327:788.
31. Zocor [package insert]. Whitehouse
Station, NJ: Merck & Co, Inc. (1993).
32. Boccuzzi SJ, Bocanegra TS, Walker
JF, et al. Long-term safety and
ef cacy prole of simvastatin. Am
J Cardiol . 1991;68:1127–1131.
33. Silva MA, Swanson AC, Gandhi PJ,
Tataronis GR. Statin-related adverse
events: a meta-analysis. Clin Ther .
2006;28:26–35.
Address correspondence to: Kook-Hwan Oh, MD, PhD,
Department of
Internal Medicine, Seoul National University Hospital, 101
Daehakro,
Chongno-Gu, Seoul, 110-744, Seoul, Republic of Korea. E-mail:
khoh@
snu.ac.kr
Clinical Therapeutics
1190 Volume 36 Number 8
http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://localhost/var/www/apps/conversion/tmp/scratch_1/dx.doi.org/10.1046/j.1525-1497.1998.00118.xhttp://refhub.elsevier.com/S0149-2918(14)00361-0/sbref18http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref18http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref18http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref18http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32mailto:[email protected]:[email protected]:[email protected]:[email protected]://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref32http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref31http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref30http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref29http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref28http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref27http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref26http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref25http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref24http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref23http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref22http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref21http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref20http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref19http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref18http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref18http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref18http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref18http://localhost/var/www/apps/conversion/tmp/scratch_1/dx.doi.org/10.1046/j.1525-1497.1998.00118.xhttp://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref16http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref15http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref14http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref13http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref12http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref11http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref10http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref9http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8http://refhub.elsevier.com/S0149-2918(14)00361-0/sbref8