Embed Size (px)
Citation preview

By Adam Hollingworth
6.Circulation through Regions - 1
6.Circulation Through Regions Table of Contents
Organ Supply & Consumption ........................................................................................................................ 2 Summary Highs & Lows .................................................................................................................................................................. 2
Autoregulation .................................................................................................................................................................. 3 Definition & Intro ............................................................................................................................................................................... 3
Cerebral Circulation ........................................................................................................................................... 4 Vessels ..................................................................................................................................................................................................... 4
Cerebral Blood Flow & Regulation ............................................................................................................................. 4 Special Tasks of Cerebral Circulation ........................................................................................................................................ 4
Adaptations to Meet Special Tasks ............................................................................................................................ 5 Structural Adaptations ..................................................................................................................................................................... 5 Functional Adaptations .................................................................................................................................................................... 5 Special Problems Facing Cerebral Circulation .................................................................................................................... 10 Measurement of Cerebral Circulation .................................................................................................................................... 10
Brain Metabolism ......................................................................................................................................................... 10 O2 Consumption .............................................................................................................................................................................. 10 Energy for Brain ............................................................................................................................................................................... 10 Glutamate & Ammonia Removal ............................................................................................................................................... 11
Spinal Cord Circulation .................................................................................................................................... 12 Arterial ................................................................................................................................................................................................. 12 Spinal Cord Perfusion Pressure ................................................................................................................................................ 14 Epidural Content .............................................................................................................................................................................. 15
Coronary Circulation ........................................................................................................................................ 16 Vessels & Valves ............................................................................................................................................................................... 16 Special Tasks ..................................................................................................................................................................................... 16 Structural Adaptations to Meet Tasks Required ................................................................................................................ 17 Functional Adaptation ................................................................................................................................................................... 17 Special Problems ............................................................................................................................................................................. 18 Measurement of Coronary Flow ............................................................................................................................................... 19 O2 Supply vs Demand of the Heart .......................................................................................................................................... 19
Renal Ciculation ................................................................................................................................................. 20
Hepatic Circulation ........................................................................................................................................... 20 Flow Pressures ................................................................................................................................................................................. 21 Hepatic Artery vs Portal Vein ..................................................................................................................................................... 21 Effect of Anaesthesia on Hepatic Blood Flow ...................................................................................................................... 22 Measurement .................................................................................................................................................................................... 23
Cutaneous Circulation ...................................................................................................................................... 24 Special Tasks ..................................................................................................................................................................................... 24 Structural Adaptation .................................................................................................................................................................... 24 Functional Adaptation ................................................................................................................................................................... 24 Special Problems ............................................................................................................................................................................. 25 Measurement of Skin Circulation ............................................................................................................................................. 25 Examples of Skin Reactions ........................................................................................................................................................ 25
Muscle Circulation ............................................................................................................................................. 27 Special tasks ....................................................................................................................................................................................... 27 Functional Adaptation ................................................................................................................................................................... 27 Special Problems ............................................................................................................................................................................. 28 Measurement .................................................................................................................................................................................... 28
Summary Relationship Between CO & Regional Circulations ............................................................ 28

By Adam Hollingworth
6.Circulation through Regions - 2
Organ Supply & Consumption Regional Blood Flows:
• Brain: 50-54 ml/100g/min (whole brain) or ~ 750 ml/min or ~ 15% of CO Note: flow to grey matter ~ 100ml/100g/min ( Note:Regional flows in cortex does change according to activity )
• Coronary:84ml/100g/min or 200-250 ml/min or ~ 5% of CO • Renal: 400ml/100g/min or ~ 1200-1300 ml/min or ~ 25% CO ( 95% cortex , 5% medulla) • Hepatic: Total:57ml/100g/min or 1500 ml/min or ~ 30% CO
→ Hepatic artery: 300-500 ml/min → Portal vein: 1000-1200 ml/min
• Resting skeletal muscle: 2-3 ml/100g/min or ~ 1000 ml/min or ~ 15-20% CO • Skin: ~15ml/100g/min (thermoneutral) ~ 300 ml/min or ~ 6% CO (variable)
Regional O2 consumptions:
• Brain: (1400g) 3-3.5 mlO2/100g/min or ~ 50 mlO2/min = ~ 20% of basal VO2
• Coronary: (300g heart) 6-7 mlO2/100g/min or ~ 21 – 27 mlO2/min = ~ 10% of whole body basal VO2
• Renal: (300g) 6mlO2/100g/min or ~ 18mlO2/min = ~ 7% of basal VO2
• Hepatic: ( 2600g liver) 2mlO2/100g/min or ~ 50 mlO2/min = ~ 20% of basal VO2 • Resting muscle: ( 30kg) 0.2mlO2/100g/min or ~ 50mlO2/min = 20% of basal VO2 • Skin: (2-3kg) 0.3mlO2/100g/min or ~ 12mlO2/min
= ~ 4.3% of basal VO2
Summary Highs & Lows • Blood flow to:
o Max: Liver 1500ml/min o Min: Heart 250
• A/V O2 difference: o Max: heart 114ml/min(65%) ; liver (50%) o Min: Kidneys 14, carotid body
• Resistance: o Max: Skeletal Muscle/kg; skin (absolute)
• Cardiac Output %total: o Max: Liver 27.8 o Min: heart 4.7
• O2 consumption: o Max: liver, mm, brain o Min: skin

By Adam Hollingworth
6.Circulation through Regions - 3
Autoregulation Definition & Intro • The ability of organs to ensure adequate perfusion in the face of changes in perfusion pressure ( ΔP )
or changes in metabolic demand, by means of local mechanisms only. ΔP Ohm’ law: Qorgan = VRorgan ( VR = vascular resistance for the organ in question) ΔP = MAP - venous pressure ( MAP = same through out the body in supine, but venous pressure differ from organ to organ. Also, if a Starling resistor applies, a third pressure comes into play, and ΔP = MAP – (larger of VP and 3rd pressure)
• From Ohm’s law, one can see that, to maintain a constant perfusion (Qorgan), the organ will need to change its vascular resistance (VR) 8ηL Vascular resistance for laminar flow = πr4
• ∴ only way organ can change its Vasc resistance is by changing radius of supplying vessel • & this is powerful mechanism due to r4 effect • 2 types of autoreg:
o pressure aka myogenic o metabolic
• in many organs combo of mechanisms exists ! usually one more predominant than other
• NB in kidneys also a 3rd mechanism = Tubuloglommerular feedback (TGF) which interlinks with pressure autoreg
Pressure Autoregulation • = ensures adequate flow in the face of changing perfusion pressure • if an ↑MAP then ↑vasoC to the organ to normalise flow • myogenic theory states that stretch of vessel causes it to constrict & vice versa • method not understood – may be
o endothelial production of vasoconstrictor (?endothelin) in response to ↑intraluminal pressure OR o stretch ⇒ prolonged depolarisation ⇒ ↑open probability of VOC Ca channels
• organs where pressure autoreg predominant: o total cerebral circ o renal o coronary – metabolic is also impt but it resets pressure autoreg to operate at higher flows
Metabolic • = ensure adequate flow in face changing metabolic demands • eke metabolic hyperaemia, metabolic vasoD • locally produced metabolites as well as ↓O2 & ↑CO2 ⇒ vasoD or supply vessels
! lactic acid, H, ADP, adenosine, K • organs where metabolic predominant:
o coronary – (see above) o skeletal mm o Regional cerebral circ:
! Pressure autoreg determines total cerebral flow unless eg generalised seizures

By Adam Hollingworth
6.Circulation through Regions - 4
Cerebral Circulation Vessels • Inflow to brain:
o 2 carotids o 2 vertebrals ⇒ basilar
• Little crossing over side to side as pressure equal both sides • are precapillary anastomoses between cerebral vessels but flow not enough with sudden occlusion • Outflow:
o Dural sinuses⇒IJV o Ophthalmic & pterygoid venous plexous ⇒ emissary veins ⇒ scalp ⇒ paraverterbral veins in
spinal canal • Endothelial cells of capillary wall –
o Gaps inbetween o Few vesicles in cytoplasm ∴ little vesicular transport
! multiple other transport systems • Choroid epithelial cells on top have tight junctions • Astrocytes:
o Surround brain capillaries o Do not cover entire capillary wall o Gaps in end feet on basal lamina of 20nm
Cerebral Blood Flow & Regulation • Average brain weighs ~ 1400g ( 40% grey and 60% white matter), • Receives an average blood flow of 54ml/100g/min
! grey matter basal flow ~ 100ml/100g/min • critical blood flow awake = 20mls/100g/min • Av brain ∴
o Total flow = ~750ml/min o = ~ 15% of CO
• global flow constant but see regional changes in flow in cortex
ΔP__ QBrain = CVR and thus DO2Brain = QBrain x CaO2 ) CBF = CPP/CVR CPP = MAP – (higher of ICP or CVP) Special Tasks of Cerebral Circulation • Need for totally secure DO2Brain:
o Grey matter: ! highly metabolically active (VO2 ~7mlO2/100g/min) ! accounts for ~20% total basal VO2 ! extremely sensitive to hypoxia:
• seconds of ischaemia ⇒ LOC • minutes ⇒ irreversible damage
o ∴ primary task (of whole cardioresp system) is to ensure uninterrupted DO2Brain
ΔP = MAP (@level of brain) – CVP or ICP (whichever is bigger) CVR = cerebral vascular resistance ! arterioles of cerebral circ are short ∴ arteries account for ~40-50% CVR (unusually high) ! receive rich autonomic supply

By Adam Hollingworth
6.Circulation through Regions - 5
• Adjusting local supply to local demand: o Mental functions are localised to well defined regions eg vision in occipital cortex o Local neuronal activity ⇒ ↑ed local metabolic rate
Adaptations to Meet Special Tasks Structural Adaptations • Circle of Willis
o 2 entry vessels into cranium: ! basilar ! ICA
o Form cicle of willis around optic chiasma o ACA, MCA, PCA all arise from circle o If blockage of 1 ICA should be redundancy from contralateral side
! true in young, less so in elderly o Main cerebral arteries divide into pial arteries o Pial arteries run over surface of brain o Finer arteries arise from pial arteries and penetrate parenchyma to form short arterioles
• High Capillary density:
o Grey matter contains av 3000-4000 capillaries/mm2 ! ie similar ot myocardium
o High density ⇒ ! large exchange area ! minimises extravascular diffusion distance
Functional Adaptations 1. high basal blood flow 2. protection of cerebral flow by reflex control of other circulations 3. cerebral autoregulation 4. Sensitivity to PaCO2 & hypoxia 5. Regional functional hyperaemia in brain 6. Nervous innervation of intra & extracerebral vessels 7. BBB 1. High Basal blood Flow

By Adam Hollingworth
6.Circulation through Regions - 6
• grey matter: o receives ~ 100ml blood/100g/min o ie x 10 the whole body average o extracts ~ 35% of the delivered O2 (~3 – 3,5 mlO2/100g/min).
2. Protection of cerebral flow by reflex control of other circulations • Ohms equation on laminar flow states that blood flow to organ is dependant on balance of pressure &
resistance ie MAP & CVR • This present in brain as well as other organs • BUT brain able to safeguard its own blood supply by:
o controlling CO & o vasc resistance of other organs ! via modulating autonomic output
• ∴ brain can sacrifice other organs perfusion to protect it own ! all except heart
3. Cerebral AutoRegulation • pressure autoregulation v well developed in brain • purely local mechanism • autoreg =allows maintenance of norm cerebral blood flow if arterial pressure 50-175mmHg • function:
o ↓in MAP⇒ cerebral vasoD ⇒ maintain CBF o ↑in MAP ⇒ cerebral vasoC ⇒ limit CBP ! autonomic activity can augment length of plateau via further VC vasodilators eg ACEIs do opposite ie shortern plateau
• mechanism: o myogenic – predominantly pressure autoregulation o metabolic (less) - mostly involved in changes in regional flow
• limits: <50 and >175mmHg see sharp changes in CBP with anymore extremes of MAP ! ie greater pressure increase without incr in blood flow to head
4. Sensitivity to PaCO2 & Hypoxia • ↑PaCO2 ⇒ vaso D of cerebral vessels • ↓PaCO2 ⇒ vasoC • CBF changes linearly with changes in PaCo2 between 20 – 80mmHg
! ~ 4% change / mmHg PaCO2 change
vasoD vasoC

By Adam Hollingworth
6.Circulation through Regions - 7
• The ↓CBF of ↓PaCo2 diminishes after approx. 4-6hrs due to:
o HCO3 equilibriates across BBB o Normalisation of interstitial fluid pH o CBF return to baseline ! after this a sudden return to ‘normal’ PaCo2 ⇒ ↑CBF & ↑ICP
• Outside CBF-PCO2 response curve (<20 and >80): o levels out at low PaCO2s due to:
! VasoC ⇒ hypoxia ⇒ cerebral vasoD o Upper limit of CBF due to vessel maximal vasoD
• Effect of ↑PaCO2 on pressure autoregulation:
• Hypoxia:
o ⇒ causes cerebral vasoD o only see ↑CBF when PaO2 < 50mmHg then steep ↑in CBF as vasoD occurs o this mechanism dictated by OHDC:
! DO2brain only starts to ↓ when PaO2 <60mmHg (ICU point) ! ie steep drop off of O2 content from this point
• The vasoD from hypercarbia and hypoxia likely mediated by NO from endothelial cells

By Adam Hollingworth
6.Circulation through Regions - 8
5. Regional Functional Hyperaemia in Brain • = metabolic autoregulation • Cause for cortical metabolic hyperaemia due to:
o ↑interstitial K – from outward K currents from active neurons o H+ o Adenosine
• This system (metabolic regional autoreg) should not influence total CBF unless: o Generalised seizure ↑CBF o Induced coma with drugs that ↓CMRO2 eg thiopentone ↓CBF
6. Nervous Innervation of Intra & Extra Cerebral Vessels • Intracerbral arteries poorly innervated • Extracerebral arteries well innervated by symp constrictor vessels
! NB brain vessels don’t really participate in art baroreceptor reflex • Control of vasculature:
o Direct SympNS input: ! postganglionic sympathetic neurons:
• cell bodies = sup Cx ganglion • endings ⇒ vasoC
o Noradenaline o Neuropeptide Y
! Poor max cerebral response of only ~37% ↑vascular resistance o Direct Parasymp NS input (vasoD) to cerebral arteries:
! Cholinergic neurons • Originate = sphenopalatine ganglia
! Postganglionic cholinergic neurons: • Endings = Acetylchline & VIP
o Hormonal control - only have few alpha adrenoceptors ∴ respond poorly to circulating NA o Perivascular nerve fibres:
! 5-HT – potent vasoC effect on cerebral arteries ! along with high K implicated in vasospasm following SAH ! 5-HT implicated in migraines
• sensory fibres – see abundance of perivascular sensory fibres – cause pain in vascular headache ie migraine/stroke

By Adam Hollingworth
6.Circulation through Regions - 9
• Role of vasoC innervation is to protect BBB against sudden rises in bp
7. Blood Brain Barrier • BBB function:
o excludes lipid insoluble substances from crossing into brain interstitium ie toxins o conserves neuropeptides (would otherwise wash away after release
• ∴brain neuronal environment is most tightly controlled environment in body ! neurons protected from fluctuating ion & catecholamine levels in blood stream
• BBB can be disrupted by: o Acute severe HTN o Cerebral ischaemia o cerebral infection/meningitis o Head injury
• Formed by o tight junctions in:
! Capillary endothelial cells ! Epithelial cells in Choroid plexus
o Basement membrane o Astrocyte foot processes
• Penetration of BBB: o Active transporter systems to get things in:
! GLUT1 transporter in brain in 2 forms: • GLUT 1 55K
o High conc in capillaries • GLUT 1 45K
! Other transporters: • Thyroid hormones • Organic acids • Choline • Amino acids
o Several drugs & peptides cross cerebral capillaries passively ! transported back by multidrug nonspecific transporter
! ATP dependant P glycoprotein in apical membrane endothelial cells ! movement out of brain is more free than into it
o Easy to penetrate bbb: ! Lipid soluble steroid hormones ! Water ! Co2 ! O2
o Difficult to penetrate: ! Lipid insoluble substances ! Urea – slow penetration ! Protein bound steroid hormones ! Proteins ! Polypepides
• BBB is absent in some areas = o Circumventricular area:
! Neurohypophsysis aka post pituitary ! SCO ! Area postrema –
• Chemoreceptor trigger zone for vomiting based chemical changes in plasma • Angiotensin II ⇒ ↑bp

By Adam Hollingworth
6.Circulation through Regions - 10
! OVLT – supraoptic crest • Osmoreceptor controlling vasopressin secretion • IL1 ⇒ fever
! SFO – subfornical organ • Angiotensin II ⇒ polydipsia
! these areas have fenestrated capillaries ∴seen to be outside bbb • Functions of these areas:
o Neurohormonal organs – secrete polypeptides into circulation o Chemoreceptor zones – sense substances from circulation which don’t penetrate bbb
! Note: pineal gland & anterior pituitary are outside bbb • Development of BBB:
o BBB less developed in infants ! eg jaundiced infants with high free bilirubin ⇒ bilirubin enters brain ± ⇒ kernicterus
(basal ganglia damage) Special Problems Facing Cerebral Circulation Effect of Gravity • Gravity has no direct effect on CBF during orthostatsis as cerebral circulation behaves like inverted U
tube: o Arterial limb – drag o Venous limb & CSF – equivalent drag encouraging movement through U tube
! remember Starling resistor • Does have indirect effect via ↓CVP & ↓SV ⇒ ↓CO when moving into standing
! need quick baroreflex to prevent postural hypotension and syncope Encasement of brain in Rigid Cranium • Monro Kelly doctrine – see below Measurement of Cerebral Circulation • Fick principle –
o Nitrous oxide – most common o Xenon 133
• Ketty Scmidt: o 10% NO2 over 15-20mins o map arterial & venous conc o gap in middle of 2 sigmoid curves = flow
• Carotid angiography • Transcranial dopplerimetry • SPECT imaging • Cerebral Spo2 monitoring
Brain Metabolism O2 Consumption • Cerebral metabolic rate for o2 = 20% total body resting
o2 consumption • Loss of o2 ⇒ LOC in 10secs • Brain stem more resistant to hypoxia ∴ creates
vegetative state with loss of higher reasoning • Most sensisitve =
o basal ganglia – chronic hypoxia ⇒ Parkinsonism o thalamus
Energy for Brain • glucose:

By Adam Hollingworth
6.Circulation through Regions - 11
o provides 90% energy to maintain ion gradients across membranes o GLUT 1 transports it in across capillaries o Other GLUT transporters then redistribute it o Insulin not required to use glucose o Other substances can be used if lack of glucose o In normal conditions: 30% glucose converted to:
! Amino acids/proteins ! lipids
• Respiratory Quotient of cerebral tissue = 0.95-0.99 Glutamate & Ammonia Removal • Glutamate [in] ∝ glutamine [out] • Glutamate [in] + ammonia ⇒ glutamine
! detoxifying mechanism to remove amnonia ! opposite to reaction in kidneys

By Adam Hollingworth
6.Circulation through Regions - 12
Spinal Cord Circulation Arterial • mainly dependant on 3 longitudinal vessels:
o anterior median longitudinal spinal artery (Ant spinal artery)– ! from convergence of vertebral arteries in midline ! runs length of spinal cord in ant media fissure
o pair (x2) of posterolateral trunks (posterior spinal arteries): ! from vertebral arteries ! receive contributions from post radicular arteries ! at some points along cord almost disappear making arteries look discontinuous
• these vessels largest in Cx & Lx regions due to demand grey matter > white matter ! ∴ blood supply to Tx cord is poorest between T4-T9
ASA • sulcal arteries:
o arise from ASA and penetrate ant 2/3 of cord o alternate sides at each level
! occlusion of ASA or sulcal arteries ⇒ ant spinal artery syndrome ! post 2/3 as supplied by pair of posterolateral trunks:
• Ant spinal artery syndrome:
o mid thoracic esp sensitive to hypoperfusion o initial: flaccid paralysis below level – due to spinal shock o later: spastic paralysis & UMN signs due to destruction of corticospinal tracts o diagnosis = below level of:
! loss of pain & temp = lat spinothalamic tract ! preservation of proprioception = dorsal columns
Other Contributing Arteries • other reinforcing vessels supplying some circulation:
o major segmental arteries: ! originate depending on level:
• Cx – vertebral arteries • Tx – posterior intercostal arteries • Lx – subcostal & lumbar arteries • Sx – iliolumbar & sacral arteries
! feed into radicular arteries o radicular or segmental medullary arteries of the cord –
! at every level of spine in pairs ! branch & anastomose profusely at:
• intervertebral foramen
By Adam Hollingworth
6.Circulation through Regions - 13
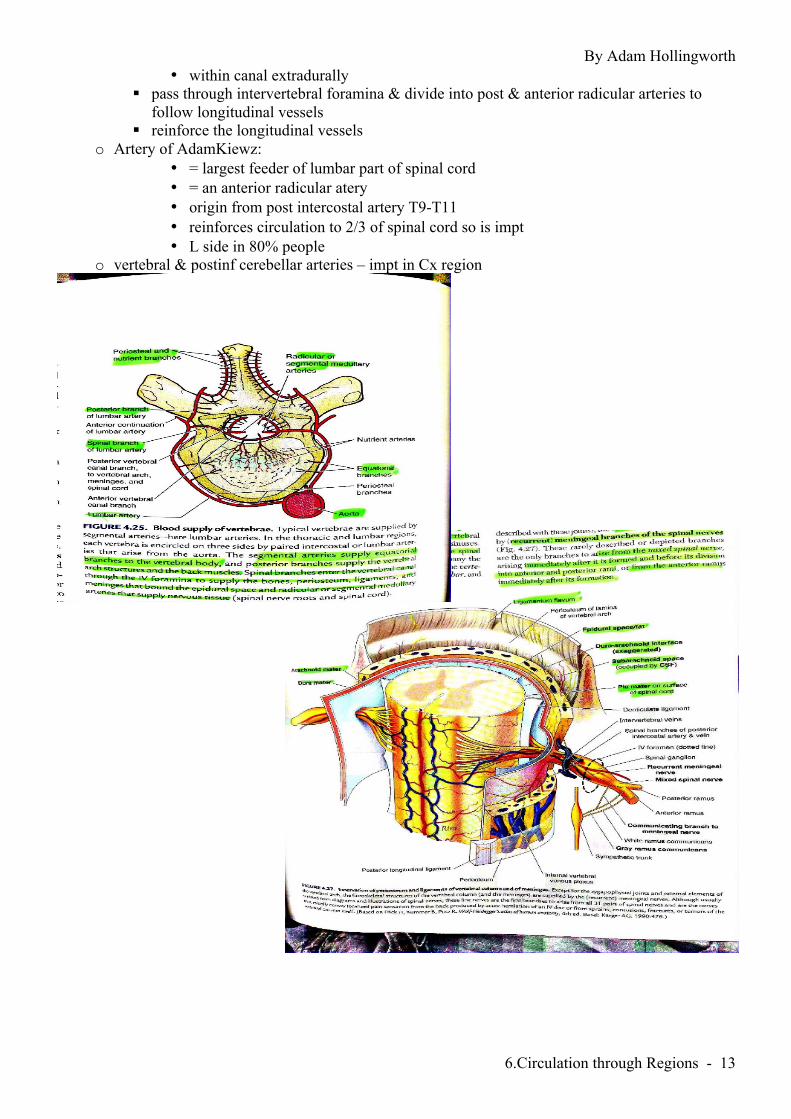
• within canal extradurally ! pass through intervertebral foramina & divide into post & anterior radicular arteries to
follow longitudinal vessels ! reinforce the longitudinal vessels
o Artery of AdamKiewz: • = largest feeder of lumbar part of spinal cord • = an anterior radicular atery • origin from post intercostal artery T9-T11 • reinforces circulation to 2/3 of spinal cord so is impt • L side in 80% people
o vertebral & postinf cerebellar arteries – impt in Cx region

By Adam Hollingworth
6.Circulation through Regions - 14
Venous • not as clearly defined as arterial circulation but tend to follow their distribution • can be highly variable • generally 2 sets of vessels:
o veins of spinal cord: ! 3 ant spinal veins – freely cross communicate
• drained by: o anterior & posterior radicular veins o feed into epidural venous plexus
o venous plexus of Batson: ! large & complex venous channel ! 3 components – all cross communicate:
• epidural venous plexus ⇒ continues through foramen magnum into dural sinuses & skull veins
• extravertebral venous plexus • veins to osseous structures of spine
! from base of skull to coccyx ! communicates directly with IVC & SVC
• no valves in spinous venous network: o high intraabdo pressure ⇒ pelvic blood passes superiorly in epidural (internal) vertebral plexus o jugular veins obstructed ⇒ blood leaves via same internal vertebral plexus
• as prostatic plexus is continuous with vertebral system ⇒ neoplasm prostate ⇒ vertebra, spinal cord, brain, skull
Spinal Cord Perfusion Pressure • perip op risk of spinal cord ischaemia: up to 8% in some cases:
o immediate vs delayed: 37% are delayed ie 13hr – 91days o >50% resolve with Rx
• SCPP = MAP – (CSF + CVP) • theory is a loss of autoregulation due to surgical intervention ∴ perfusion becomes pressure dependant • risk factors:
o prev AAA o L subclavian occlusion o emergency procedure o MAP <70 o renal impairement
• anaesthetic aim is: o MAP >80 o SCPP >60 o maintain DO2
• anaesthetic factors: o maintain SCPP - vasoactives o CSF drainage:
! ↓risk by 80% ! 50% post op deficits can be reveres by spinal drain insertion
o intraop monitoring: ! can do motor evoked potentials (MEPs) ! requires TIVA as is abolished by volatiles & NMBs
o ↓metabolic demand: ! hypothermia – systemic (33C or epidural). no clear evidence ! pharmacological strategies:

By Adam Hollingworth
6.Circulation through Regions - 15
• CSF opiates ↑ spinal cord ischaemia • α2 agonists ↓ischaemia – clonidine/dexmedetomidine • other good options:
o anti-inflam – steroids, o antioxidant – mannitol o antiexcitatory – MgSo4, thiopentone
! preconditioning – needs further trials Epidural Content • venous plexus • spinal nerves • loos areolar tissue & fat • lymph • arteries
By Adam Hollingworth
6.Circulation through Regions - 16
Coronary Circulation • Average heart weight = 300g • Receives
o Basal CO: ~84ml blood/100g/min (=200-250ml/min) = 5% CO o Max cardiac work: 300-400ml/100g/min
• VO2 (consumption): o Basal: 6-7mlO2/100g/min (20-25mlO2/min) or ~10% basal total VO2
• ∴ mismatch of %CO & %VO2 = why O2 extraction must be high ~67% ! ∴ ↑VO2 need must be met by ↑ing coronary flow
ΔP Qcor = CVR Starling Resistor • Starling resistor exists in heart in respect to ΔP
! 3rd pressure = intraventricular pressure (IVP) • ΔP = aortic root pressure – (larger of IVP or RAP)
! simplistic equation as flows for RCA & LCA differ during cardiac cycle
Vessels & Valves • Aortic sinuses kept away from valves by eddy currents • Orifices patent throughout cardiac cycle • RCA & LCA arise immediately above the cusps of AV (aortic root) • LCA supplies:
o LV & septum • RCA supplies – mainly RV
! dominant circulation named after which one supplies AVN: • 70% people R dominant • 20% co-dominant • 10% L dominant
• Venous blood return:
o Coronary sinus ⇒ RA – 95% of blood o Ant coronary vein ⇒ RA o Thesbian veins ⇒ various cardiac chambers
! some drain into LV contribute to physiological shunt ! ie contributing to normal D[A-a]O2
o Others: ! Arteriosinusoidal vessels – connect arterioles to chambers ! Arterioluminal vessels – arteries straight into chambers
Special Tasks • Circulation must deliver O2 at high rate to keep up with demand • @rest VO2 of myocytes is x20 of skeletal mm • @exercise cardiac work rate can ↑x5
CVR = Coronary vasc resistance

By Adam Hollingworth
6.Circulation through Regions - 17
Structural Adaptations to Meet Tasks Required • high myocardial capillary density ~3000-5000 capp/mm2 ie ~1capp/myocyte • facilitates O2 & nutrient delivery:
o ↑endothelial area o ↓ed max diffusion distance
• O2 transport ↑ed by presence of myoglobin in cardiac myocytes (3.4g/L) Functional Adaptation 1. High basal flow & high O2 extraction 2. Autoregulation 3. Coronary vasomotor nerves 1. High basal flow & high O2 extraction • Basal flow/unit weight = ~x10 of whole body average • Myocardium extracts 65-75% O2 from coronary blood
! can ↑to ~90% in severe exercise ! whole body average 25%
• Myocardial fibre has PO2 ~6mmHg • ∴ venous blood returned to RA =
o O2 content ~50-70ml/O2/L o PO2 ~20mmHg
• Energy source - % extraction from blood: o High: fatty acids (40-70%) o Low: Glucose (2-3%) ! = substrate preference
• NO produced continuously to encourage continuous blood supply 2. Autoregulation • Both methods of autoregulation seen in coronary flow BUT metabolic is dominant process Metabolic Auto reg: • Extra O2 required at high work rates met mostly by ↑flow (less by extraction):
o CBF : VO2: ! Light – moderate work: linear ↑in CBF with ↑VO2 ! High work:
• ↑in flow lags • ↑O2 extraction forced
• myocardial metabolism generates vasodilator messages in quantative manner • mechanism for VD:
o interstitial hypoxia – acts directly on vascular smooth mm cells via hyperpolarization o adenosine –
! created from ATP degradation ! evidence that only see ↑release at low PO2s ∴only in ischaemic or flow limited
myocardium o ↑Co2 o ↑H+ o ↑K+ o lactate o prostaglandins
Pressure Auto Reg: • is reset by metabolic auto reg to operate at higher flows • this protects myocardium against under perfusion during periods of ↓bp to around ~50mmHg 3. Coronary Vasomotor Nerves • Coronary arteries & arterioles are well innervated by SNS vasoC fibres
! tonic d/c ⇒ arteriolar tone

By Adam Hollingworth
6.Circulation through Regions - 18
• NB if have total cardiac symp stim to all areas ie pacemaker, myocytes: o Predicted response would see:
! ↑HR ! ↑contractility ! ↑cardiac work
o Overall balance of response actually seen: ! Metabolic vasoD outweighs vasoC effect sof sympathetics
! ∴ CBF ↑s ie metabolic autoreg overrides SNS • Also see endothelial receptors for circulating catecholamines:
o α-adrenergic receptors ⇒ VC o β – adrenergic receptors ⇒ VD
• adrenaline release from adrenals (& iatrogenic NA) effect: o reinforces coronary hyperaemia via B1 (also skeletal mm & liver) o ↑HR o ↑force of cardiac contraction o VC of skin, renal, splachnic vessels o Expected direct effect coronary VC
! but due to metabolite build up actually see overall coronary VD not VC • vagal fibres ⇒ coronary VD • severe cold can induce reflex SNS mediated coronary vasoC in hearts with CAD (coronary art disease)
! not in norm hearts Special Problems 1. Effect of Changes in IVP During Cardiac Cycle on RCA & LCA Flow 2. Acute Coronary Artery Obstruction 3. Gradual Obstruction 1. Effect of Changes in IVP During Cardiac Cycle on RCA & LCA Flow • pressures in heart during cardiac cycle:
o Systole: ! L ventricle = 120 mmHg ! R vent = 25 ! Aorta = 120
o Diastole: ! L vent = 5mmHg ! R vent = 2 ! Aorta = 80
• Pressure higher in L vent during systole ⇒ flow in aorta • But IVP in systole > aortic root pressure ∴ no coronary blood flow

By Adam Hollingworth
6.Circulation through Regions - 19
! same as West zone 1 in lung (PA > Pa >Pv and thus no flow) o ∴ no flow in systole to coronary vessels of subendocardial portion of L vent
! why this portion most susceptible to ischaemic damage ! is some flow to superficial portions of L vent in systole
o pressure in R vent < aorta ∴ do get flow in systole • LCA receives bulk of CBF because of ↑ed LV mm mass • ∴ ΔP is usually measured as aortic diastolic pressure (ADP) less the larger of LVEDP or RAP
• Blood flow to L vent is ↓ed with aortic stenosis because L vent pressure must be much higher than
aorta to achieve outflow • Coronary flow also ↓ed when aortic diastolic is low as ↓effective coronary perfusion pressure
! seen in heart failure ⇒ shunting blood to venous side of circ
2. Acute Coronary Artery Obstruction • Cross connections do exist between branches of coronary arteries BUT few and small • ∴ coronary arts = functional end arteries • clot to art ⇒ residual flow downstream <10% ⇒ acute ischaemia • MI most frequent in subendocardium as wall stress greatest here
! ∴ endocardial flow lowest at low perfusion pressures 3. Gradual Obstruction • Atheroma ⇒ gradual narrowing then anastomoses have time to enlarge & maintain precarious nutrient
flow • BUT cannot supply additional flow needed for exercise/stress ∴⇒angina
Measurement of Coronary Flow • For absolute flow = Coronary sinus thermal dilution method
O2 Supply vs Demand of the Heart • Supply Myocardial DO2: DO2Cor = CaO2 x QCor
• CaO2 = (Hb x1.39 x SpO2) + (PaO2 x 0.03): important = Hb, SpO2 • QCor = ΔP* / CVR : NB = aortic diastolic P, LVEDP (Starling resis), radius4, η • Heart rate: ↑ rate ⇒ decreased diastolic filling time (most impt in LV) Demand • Basal requirements ( ie VO2 of ~ 6-7 mlO2/100g/min) • Heart rate: ↑ HR ⇒ ↑ demand (thus, ↑ HR = double edged sword re O2 balance) • Contractility • Wall stress: (S = P.r/2w):
o ↑ IVP: ↑ Afterload (eg ↑MAP) + ↑ Preload (LVEDP) o ↑ radius (eg dilated heart) o ↑ wall thickness(w) will decrease wall stress

By Adam Hollingworth
6.Circulation through Regions - 20
The Balance • O2 extraction already high ∴ ↑demand (initially) met by ↑ing flow • Metabolic autoreg (↑radius) vital in ↑ing flow
! less effective in atherosclerotic arteries • BBlockers are very good for O2 balance:
o ↓HR o ↓contractility o ↓central SNS output o ↓renal renin production
• clinically used indexs: o supply = diastolic P time index (DPTI)
! = AUC for diastolic part of of an aortic + LV pressure trace o demand = tension time index
! = AUC for the systolic part of the trace ! from these the endocardial viability ratio (EVR) can be calculated (see A-Z anaesthesia)
• EVR = DPTI/TTI (ie supply/demand) • If <0.7 ↑likelihood for ischaemia
Renal Ciculation See renal notes
Hepatic Circulation • Liver = 2400g • Receives 57ml/100g/min or 1500ml/min = 30% CO • Divided flow:
o Hepatic art 300-500ml/min = 40-50% hepatic DO2 o Portal vein – 1000-1200ml/min = 50-60% hepatic DO2
• VO2 = 2mlO2/100g/min or 50mlO2/min = 20% total basal VO2
QHep art = ( MAP – hep venous P ) / Hep vascular resistance = 25% total flow QPort vein = ( Portal venous P – hep venous P ) / HVR = 75% total flow
• As already high blood flow to liver: if ↑O2 demand then ↑oxygen extraction rather than ↑flow

By Adam Hollingworth
6.Circulation through Regions - 21
Flow Pressures • pressures:
o portal venous norm ~10mmHg o hepatic venous norm ~ 5mmHg o hepatic artery branches mean norm ~ 90mmHg
• ∴ hepatic arterioles large ↓adjustment pressure prior to blood entering sinusoids ! drugs which alter presinusoidal pressure have little effect on sinusoidal pressure
• if ↑systemic venous pressure: o passive dilation of portal veins ⟹ ↑flow into liver o eg chronic ↑systemic pressure in heart failure ⟹ hepatic venous congestion
! ie big difference in effect on liver arterial vs venous pressure changes • if ↓systemic arterial bp⟹ ↑NA discharge:
o ⟹ intrahepatic portal veins constrict ⟹ ↑portal pressure ⟹ ↓blood flow into liver ⟹ blood bypasses and stays in systemic circulation
o ⟹ hepatic arterioles constriction ⟹ blood stays in systemic circ o ⟹ mesenteric arterioles constriction ⟹ ↓portal inflow
• inverse relationship between hepatic artery & portal venous blood pressure • reserve sinusoids are recruited during times of ingestion
↳ prevents portal pressures ↑ing linearly with portal flow which would ⟹ ↑fluid loss into ascites eg in hard liver states cirrhosis
• vasoconstriction: o intrahepatic portal vein can vasoC in response to NA vasoC nerve fibres o hepatic artery via fibres from hepatic symp plexus
• large gaps between sinusoidal endothelial cells ⇒ large permeability (reflection coefficient ~0) ⇒ lymph drainage high in protein
Hepatic Artery vs Portal Vein • Autoregulation:
o Intrinsic: ! Portal vein :
• flow related linearly to pressure • if ↓flow through hepatic artery portal vein can not compensate • (can only vasoC via extrinsic mechanism)
! Hepatic artery – has some degree of metabolic autoreg – can adjust 50% of flow via this mechanism

By Adam Hollingworth
6.Circulation through Regions - 22
• Hepatic buffer response: o if ↓portal vein flow ⇒ ↑hepatic art flow and vice versa o = hepatic arterial buffer response o mediated by adenosine (vasoD) not being washed away by low portal flow ⟹
vasoD of hepatic arterioles o if ↑portal vein pressure ⇒ ↓hep artery flow - ?due to myogenic mechanism
! eg in heart failure o Extrinsic:
! SNS activity: • ↑portal vein flow via ↑splachnic venoC • ↓hepatic art flow • liver venoC ⇒ emptying of hepatic blood reservoir into systemic circ
o ! ~ 350-500ml blood ! acute haemorrhage:
• ↓portal venous blood > systemic arterial flow • O2 supply to liver maintained by ↑extraction
! other causes ↑hepatic blood flow: • feeding - ↑s intestinal blood flow ⇒ ↑hepatic blood flow • hypercapnia
! other causes ↓hepatic blood flow: • vasopressin – vasoC hepatic vasculature • heavy exercise: splachnic vasoC • +ve pressure ventilation via ↓CO • hypocapnia: ↓flow by 30% via ↑resistance in portal venous system • hypoxia – initially ↓arterial flow but return to norm in 20mins (no effect on portal)
• if blood supply change to liver ⇒ O2 consumption met by ↑↓ing O2 extraction • delivery of O2 to liver:
o 40-50% hepatic artery = even though 1/3 of flow o 50-60% portal vein
Effect of Anaesthesia on Hepatic Blood Flow • categorise:
o drug effects o effects of ventilation & surgery
Drugs • generally all drugs which ↓CO ⇒ ↓liver blood flow • spinal & epidural ⇒
o depends on level of block eg T4 = ↓20% flow o ↓portal & mean art pressure ⇒ ↓total hep blood flow
• inhalational agents – generally ↓total hep blood flow: o halothane = greatest ↓total hep flow:
! due to ↑ed hep arterial resistance despite ↓ed portal venous flow ! ie ↓↓hepatic arterial buffer response
o enflurane = similar effects to halothane but less severe o isoflurane/des/sevo = minimal or no change
! hep arterial flow unchanged or ↑ed if ↓ed portal flow ! ie hepatic arterial buffer working better
• IV agents (thio, etomidate, propofol) = dose dependant ↓hepatic blood flow caused by: o ↓CO o ↓hepatic arterial buffer mechanism
• ß blockers (propranolol) ⇒ ↓flow

By Adam Hollingworth
6.Circulation through Regions - 23
• induced hypotension eg SNP ⇒ inversion in contribution of hep artery & portal venous supplies • H2 antagonists Effects of Surgery • Upper abdo surgery = ↓ flow 60% • Ventilation:
o IPPV: ↓portal flow due to ↑splachnic resistance o PEEP: further ↓flow due to ↑hepatic venous pressure (via ↑CVP)
Summary • All anaesthesia ⇒ ↓hepatic blood flow • BUT O2 requirements also ↓ so rarely a problem Measurement • via Fick principle • use indocyanine green as indicator • dye is removed from circ only in liver • totally excreted in bile with no enterohepatic recirculation • level in body measured by spectrophotometry • method:
o give dye by constant infusion until steady state ie infusion = hep elim rate o periph artery is measured (as indirect marker of hep artery) o catheter sampling placed in hepatic vein for sampling
rate of uptake of substance = (amount entering tissue) - (amount leaving the tissue)
(time) (time) Or: Vx = Q.ca – Q.cv = Q(ca – cv ) thus: Q = Vx / (ca – cv ) Remember: Indocyanine green is used in the indicator dilution (washout) technique to measure cardiac output.

By Adam Hollingworth
6.Circulation through Regions - 24
Cutaneous Circulation • av weight = 2.5kg • flow ~ 15ml/100g/min (thermoneutral) = ~300ml or 6% CO • min flow = 1ml/100g/min • max flow = 150-200ml/100g/min • VO2 ~ 0.3mlO2/100g/min = 12mlO2/min or 4.3% basal VO2 Special Tasks Thermoregulation • Core temp kept +/- 1deg C of 37 • Done by balancing internal heat loss production with external heat loss • Heat loss occurs by 4 methods:
o Radiation: ! Most significant in theatre patients ! Rate loss proportional to diff between ambient temp vs skin temp ! Skin temp dependant on rate of blood flow to skin
o Conduction & convection: ! Warm skin heats adjacent air, convection moves air away ! Rate of heat loss proportional to skin ambient temp differential
o Evaporation: ! 2.4KJ heat energy consumed/gram water evaporated
! = latent heat of evaporation ! water & heat delivered to skin by blood flow
! ∴ blood flow vital for all mechanisms of loss • skin = poikilothermic ie over short periods can tolerate temp extremes 0-45degs Response to trauma/Defence • vasoD in response to trauma ⇒ healing Structural Adaptation Arteriovenous Anastomosis in the Extremities (AVAs) • aka sacral areas • = exposed areas with high SA/volume ratio eg finger, toe pal, lips, nose, ears • exists direct connections between dermal arterioles & venules • AVAs =
o coiled muscular walled vessels av diameter 35um o no basal tone o activity controlled exclusively by SNS (constrictor fibres)
! have basal tonic d/c o SNS controlled by temp regulation centre in hypothalamus o ↑core temp ⇒ ↓SNS output ⇒ dilation AVAs ⇒ low resistance shunt ⇒ ↑skin flow o converse in cold
Functional Adaptation • SNS control:
o Dominant & regulated by core temp receptors • Direct sensitivity of vessel tone to local temp change:
o Hand immersed in <10deg water: ! Initial cold induced constriction ! ↑ing painful sensation ! 5-10min: vasoD ⇒ reddening of skin & relief of pain
! occurs in AVA rich areas thought due to paralysis of NA transmission prevents skin damage in prolonged exposure to cold ie red nose

By Adam Hollingworth
6.Circulation through Regions - 25
• dependant vasoC by local mechanisms: o eg vasomotor reflexs o 1hand in cold water ⇒ modest vasoC seen in other hand o due to SNS mediated spinal reflex initiated by temp receptors in immersed hand
• role & reg of arterial MAP & CVP o eg reflex vasoC & venoC in response to shock o this 2ndary to neural reflexes & circulatory hormones
• triple response to cutaneous trauma: o creates hyperaemia, ↑cap permeability & ↑delivery defensive elements to injured tissue o see below
Special Problems • compression with weight bearing/bed sores:
o ischaemic damage usually prevented by ! high tolerance of skin to hypoxia ! reactive hyperaemia on removal stress ! behavioural responses eg restlessness
• hot weather problems: o local swelling o venoD & pooling blood ⇒ post hypotension
Measurement of Skin Circulation • digital plethysmograph • Kety’s isotope clearance method • Laser-Doppler flow probe Examples of Skin Reactions White Reaction • = pointed object drawn lightly over skin ⇒ pale stroke line in ~15secs • due to mechanical stimulus ⇒ contraction precapillary spincter ⇒ blood drain out capillary’s Triple Response • more firm stroke of pointed object:
o red reaction ! in ~ 10 sec ! capillary dilation in response to pressure
o wheal: ! = swelling & mottling ! ↑permeability of capillaries & venules ! mediated by substance P
o flare: ! = redness spreading from injury ! arteriolar dilation ! due to axon reflex:
• antidromic conduction ! impulse from sensory nerve doesn’t go to spinal cord but are relayed back down other branch of sensory nerves to arteriole
• reaction persists after sympathectomy Reactive Hyperaemia • blood supply to limb occluded ⇒ arteriole below occlusion dilate 2nd to local hypoxia • circ restablished ⇒ ↑blood into dilated vessels Generalized Responses • cold blue skin =
o arteriole VC; o capillaries VD

By Adam Hollingworth
6.Circulation through Regions - 26
! Warm red skin = both dilated • Norad & adrenaline ⇒ VC of cutaneous vessels • VD caused by:
o ↓constrictor tone 2nd to ↓Norad & ↓adrenaline o ↑local VD metabolites ! there are no VD nerve fibers to skin
• examples of skin reaction: o painful event: ↑Norad d/c ⇒ generalised skin VC & triple response o exercise:
! ↑norad BUT body temp rise overcomes VC ⇒ VD o pyrexial: hypothalamic temp ↑ overcomes other reflex activity ⇒ VD
! why if pyrexial shock is more profound o hypothermic:
! initially VC ! later in severe ↓temp ± superficial VD

By Adam Hollingworth
6.Circulation through Regions - 27
Muscle Circulation • weight ~ 50kg • flow ~2-3ml/100g/min (resting), 1000ml/min = 20% CO • VO2 ~ 0.2mlO2/100g/min = 50mlO2/min = ~20% total basal VO2 Special tasks • Delivery O2 & nutrients & removal of waste products in proportion to requirement • Contribution to homeostasis of MAP:
o Skel mm ! contains ~40% total body water ! large vasc beds which affects ↑↓SVR as required
Functional Adaptation • participation in vascular reflexs:
o mm arterioles richly innervated by SNS (cholinergic fibres) o art baroreflex controls vasoC nerve activity
• dominance of metabolic autoregulation during exercise: o during hard exercise see ↑blood flow to 80-90% of CO o ↑in % CO almost entirely due to fall in local vasc resistance by metabolic vasoD
! rather than due to modest ↑MAP o ↑flow linearly with ↑local metabolic rate o timing:
! 1st few mins: • ↑interstital K ⇒ vasoD • ↑interstital osmolarity ⇒ further vasoD
! later: • inorganic phosphate released from contracting mm ⇒ vasoD • hypoxia augments above factors • ↓diffusion distances by capillary recruitment (resting mm 1/3 capillaries perfused)
o maintainence of ↑ed flow mechanism is unclear – adenosine implicated • variable oxygen extraction & O2 debt
o resting mm 25-30% extraction o exercise 80-90% extraction o in severe exercise intracellular PO2 falls so low ⇒ anaerobic glycolysis predominates ⇒ lactic
acid o lactate & ↑K stim local nociceptors ⇒ pain o amount of lactate = index of deficit O2 supply o O2 debt can reach several litres of lactate o Post exercise:
! Post exercise hypraemia ! Gradually washes out accumulated lactate & other VasoD substances ! Small amount lactate metab locally – the rest moved away by blood stream to:
• liver (majority) ⇒ resynthesis into glycogen • heart – primary substrate for energy
• skeletal mm pump: o massaging effect of isotonic contraction ⇒ ↑VR aided by venous valves
• vasodilator response of skeletal mm arterioles to adrenaline: o in physiological doses circulating adrenaline ⇒ vasoD via B2 receptors in:
! skeletal mm ! Gs linked ⇒ ↑cAMP ! heart ! liver

By Adam Hollingworth
6.Circulation through Regions - 28
Special Problems • mechanical interference during contraction:
o forceful contraction can compress vessels ⇒ ↓flow esp isometric ! not major issue in isotonic contraction
o mm myoglobin O2 store only sufficient for 5-10secs o ∴ fibres rapidly hypoxic ⇒ ↑lactate ⇒ pain & fatigue
• fluid translocation across capillaries ⇒ 10-15% ↓plasma volume Measurement • venous occlusion plethysmography • Doppler velocity meter • Kety’s isotope clearance method
Summary Relationship Between CO & Regional Circulations
• Tissues control the CO to themselves as a consequence of autoregulation: o Pressure o Metabolic
• Sum of all local organ & tissue flows = CO • Heart is a demand pump ie delivers required output as set by the tissues • Autonomic n.s (mainly SNS) maintains a constant MAP in order to allow each tissue to adjust its
blood flow indep of other tissues: o Doen by adjusting local arteriolar resistance
• SNS activity if very high might adversely ↓flow to some tissues but important tissues (brain, heart, kidney) benefit due to o ↓ed level of nervous control o & better developed autoregulation
• both autoreg & SNS achieve effects by changing arteriolar resistance (! also effects CO by means of inotropy, chronotrophy, varied afterload) • SNS changes SVR: MAP = SVR x CO) • Autoreg changes local resistance: Q = MAP/resistance
• ∴ stable MAP vital: o organ manipulates local resistance without effecting systemic MAP