Embed Size (px)
Citation preview

4/10/2018
1
What recollections in tranquility do to a promised topic
Talk about the probable best treatment packages for AoS and aphasia
Turns out that the condition-specific methods are limited ◦ Will discuss one for AOS and one for aphasia
Most of the aphasia programs function as potential retention activities for AoS
The Pittsburgh group has structured a number of traditional steps into a useful program
Name has come to be Sound Production Treatment (SPT)
This program can be used with a variety of severities by simply selecting appropriate stimuli
It is conceptually sound And the developers have done (and continue
to do) the hard work of research
Wambaugh et al JSHR, 41, 1998 (20 years old)
Five step program, from less to more cueing Built on minimal contrast pairs in words For example, p vs b (pad vs bad) In one experiment one sound was the target
◦ Logical because of frequent AoS error pattern of : Place, voicing, and plosion for frication errors
Data based on only fifteen treatment sessions
Modeling
Repetition
Minimal pair contrasts
Integral stimulation
Articulatory placement cueing
Feedback ◦ All sounds pretty familiar and it should
◦ We’ve known about txing speech problems for decades
Clinician produces both in pair and pt says both
If error, then each one of pair presented and produced separately
If both correct, repeat and on to next pair
Provide knowledge of results (good, okay, etc)
If not, step is repeated
If still not, went to next step
4/10/2018
2
Cl showed printed versions of the target
Says this is the sound you are working on
Then repeat step one
If BOTH okay go on to next pair
If not, go to next step
If only target was wrong earlier or if both were then only target was subjected to integral stimulation
Watch me, listen and say what I say If correct try to get two to four more
repetitions If correct go on to next pair If target is incorrect go to next step
Cl produced the target using silent juncture after the target and before the rest of word
If correct, went to next pair
If not, went to next step
Cl provided verbal description of sound and produced it in isolation
Correct or incorrect Cl then went on to next pair
Or in another version, simplify the context
Usually use 8 to 10 stimuli
In substitutions use sound that most frequently substitutes for the target (one of several emerging rules)
Try to work at word or phrase level
Try to use all stimuli in each session
Try to get through all at least 4 to 8 times per session
Trained and untrained items improved
Generalization was limited
As was maintenance
Subjects had aphasia and apraxia
Another problem was overgeneralization of the sound treated ◦ Started showing up where it was not appropriate
4/10/2018
3
This program uses all the traditional approaches
It is the time honored task continuum
The study itself is controlled in the traditional ways with generalization probes, baseline line and maintenance probes
Can do the treatment based on it ◦ So excellent for students and new clinicians
Some of our very first convincing data
Acquired Apraxia of Speech: Evidence-Based Intervention. ASHA Professional Development ASHA products sales 10801 Rockville Pike Rockville MD 20852-3279
Wambaugh et al (2006). Treatment guidelines for acquired apraxia of speech…JMS-LP, 2, xv-xxxiii
Overgeneralization is a huge problem for all of us in AoS tx sessions and with this program in original form ◦ Sound we emphasize comes to dominate others
Limited generalization to other sounds, environments and across time is also frequent
How the authors address these limitations Wambaugh et al (2012) Treatment of acquired apraxia of
speech: examination of treatment intensity and practice schedule. Epub
Wambaugh & Mauszycki (2010). Sound production treatment with severe apraxia of speech. Aphasiology, 24 (6-8), 814-825
Wambaugh & Nessler (2004). Modifications of SPT…Aphasiology, 18, 407-427
Wider variety of stimuli across manner, place and voicing, presented in unpredictable order, and including at least one “hard” one
Other cognitive, learning components ◦ Plan before you speak
◦ Pt self-evaluation and attempted self-correction
◦ Less frequent feedback
◦ Distractions
◦ Fewer, wider spaced responses
Step one: modeling/imitation ◦ Clinician produces both (for example, ban and pan) ◦ (could become ban, pan, Dan, ran {usually a hard
stimulus} in variable order)
◦ in pair ◦ (now four stimuli, or what ever number you and pt agree
on)
◦ and pt says both ◦ (or whatever number you have chosen) (and only after
active silence)
◦ In original clinician then provides feedback ◦ (instead patient evaluates each, clinician and patient
evaluate the adequacy of that evaluation and then patient tries to self-correct)
4/10/2018
4
Need some activity/participation steps
Way to approximate communication
Contrastive stress drill is a Q-A drill
Could be used even with single words
Idea is for cl to ask a variety of Qs about components of sentences already worked on in other ways
Stimulus: I got pie on my tie
Drill ◦ Cl: Did you get tooth paste on your tie?
◦ Pt: No, I got PIE on my tie
◦ Cl: Did you get pie on your shoe?
◦ Pt: No, I got pie on my TIE
◦ And so on
Many, many more treatment packages for aphasia
Want to highlight one that seems particularly promising for aphasia of the Broca’s type
One of the newest and most intriguing (to me) therapies is
◦ VERB NETWORK STRENGTHENING TREATMENT
Edmonds, Nadeau, Kiran (2009). Aphasiology, 23, 402-424
Edmonds & Babb (2011). Effect of verb network strengthening treatment in moderate to severe aphasia. AJSLP, 131-145
Going to do rationale and method first, data second
Focus on “the predictive components of the distributed semantic representation of concepts, which are expressed linguistically as verbs” (p. 404).
These components can be called agents (old name subjects) and patients (old name objects)
4/10/2018
5
Cut as a verb
Agents (those who cut) include butcher, builder, budget controller
Patients (what is cut) meat, board, budget
Thus retrieval is for a wider range of concepts than in the usual naming therapy with emphasis on “What is this?”
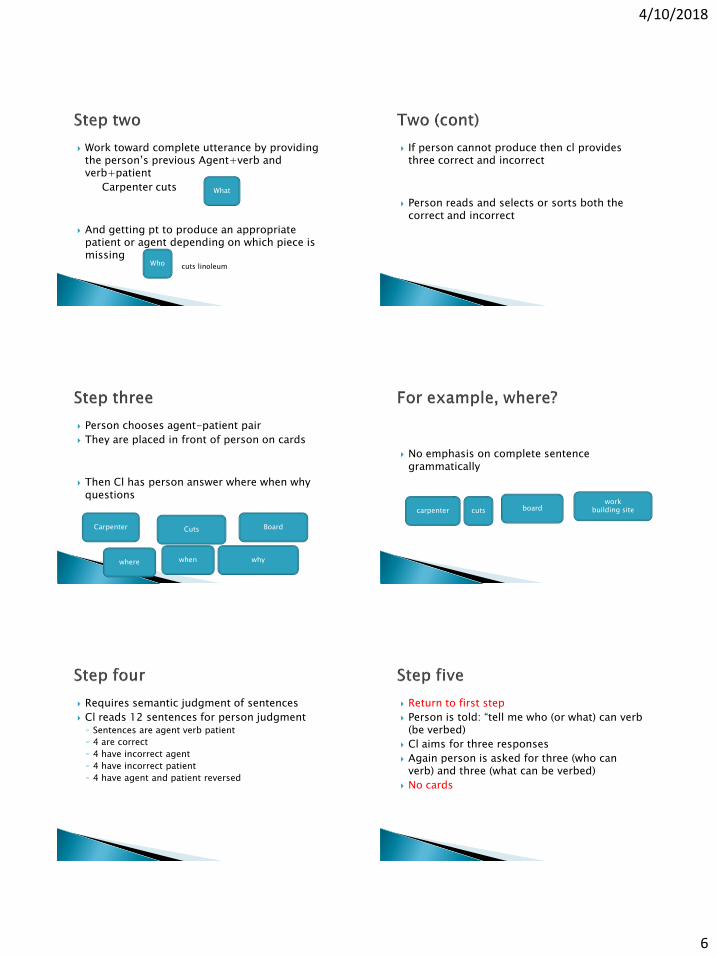
Verb cards with one verb on each card
Prepare a bunch of agent and patients for each verb
Prepare five cards with one of these following words: who, what, where, when, why
Cuts Agent Patient
Who What Where When Why
12 sentences for semantic judgment ◦ Three correct
Carpenter cuts linoleum
◦ Inappropriate agent
Barber cuts linoleum
◦ Inappropriate patient
Carpenter cuts hair
◦ Thematic reversal
Linoleum cuts the carpenter
Cl says “tell me who or what can (verb) be verbed?) Puts out the who or what card and the card with a verb written on it
Each word generated is then written on a card and placed under the who/what
Minimum of three required before going on
Who cuts cuts what or
Carpenter
Seamstress
Barber
If pt can’t get three then cl provides several appropriate and inappropriate and pt chooses
Beanie
Barber
Spinach
The who and what are to be rotated so that both agents and patients are elicited ◦ The carpenter cuts what?
◦ Who cuts the linoleum?
May take some considerable cueing even with appropriate and inappropriate foils for some pts to get three of each
4/10/2018
6
Work toward complete utterance by providing the person’s previous Agent+verb and verb+patient
Carpenter cuts
And getting pt to produce an appropriate patient or agent depending on which piece is missing
What
Who cuts linoleum
If person cannot produce then cl provides three correct and incorrect
Person reads and selects or sorts both the correct and incorrect
Person chooses agent-patient pair
They are placed in front of person on cards
Then Cl has person answer where when why questions
Carpenter Cuts Board
where when why
No emphasis on complete sentence grammatically
carpenter cuts board work
building site
Requires semantic judgment of sentences
Cl reads 12 sentences for person judgment ◦ Sentences are agent verb patient
◦ 4 are correct
◦ 4 have incorrect agent
◦ 4 have incorrect patient
◦ 4 have agent and patient reversed
Return to first step
Person is told: “tell me who (or what) can verb (be verbed)
Cl aims for three responses
Again person is asked for three (who can verb) and three (what can be verbed)
No cards
4/10/2018
7
This is, of course, merely the bare bones of the tx
May have to do much more cueing and repetition
N=2, Nonfluent
Two, two hour sessions per week
Pt 1 got 45 hours-Pt 2 got 37.5
Outcomes: ◦ WAB
◦ Sentence production
◦ Discourse
◦ Proxy/pt report of functional outcome
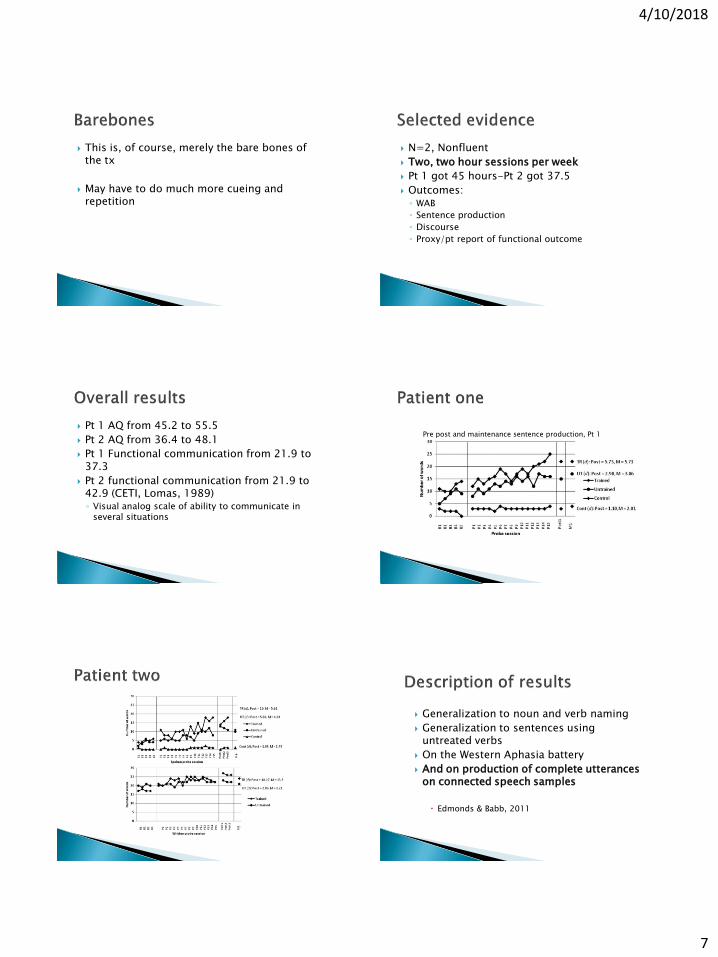
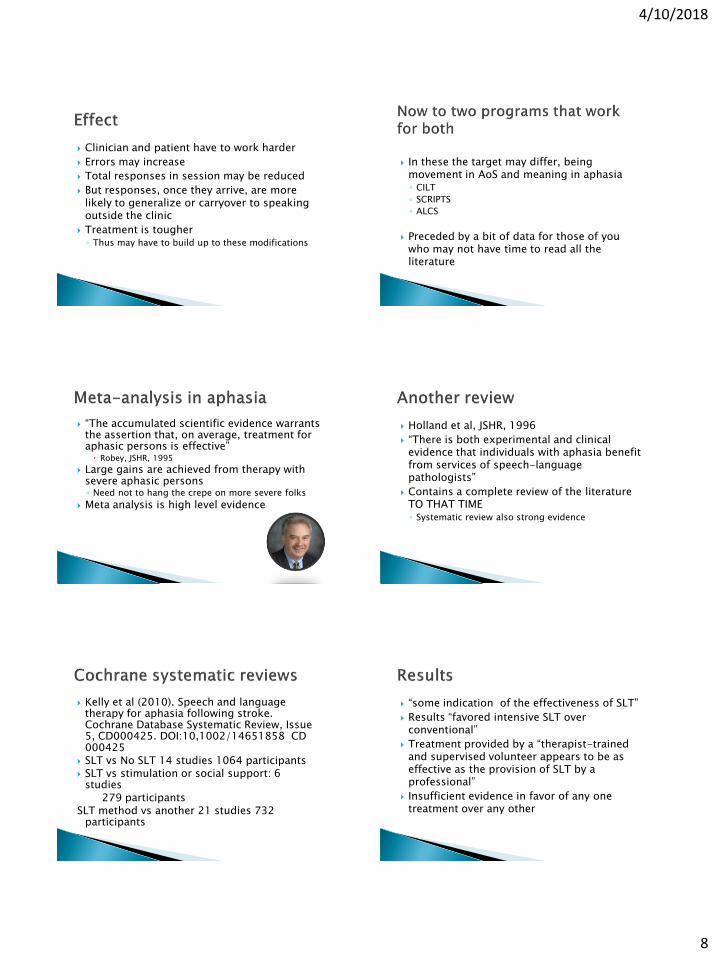
Pt 1 AQ from 45.2 to 55.5
Pt 2 AQ from 36.4 to 48.1
Pt 1 Functional communication from 21.9 to 37.3
Pt 2 functional communication from 21.9 to 42.9 (CETI, Lomas, 1989) ◦ Visual analog scale of ability to communicate in
several situations
Pre post and maintenance sentence production, Pt 1
Generalization to noun and verb naming
Generalization to sentences using untreated verbs
On the Western Aphasia battery
And on production of complete utterances on connected speech samples
Edmonds & Babb, 2011
4/10/2018
8
Clinician and patient have to work harder
Errors may increase
Total responses in session may be reduced
But responses, once they arrive, are more likely to generalize or carryover to speaking outside the clinic
Treatment is tougher ◦ Thus may have to build up to these modifications
In these the target may differ, being movement in AoS and meaning in aphasia ◦ CILT
◦ SCRIPTS
◦ ALCS
Preceded by a bit of data for those of you who may not have time to read all the literature
“The accumulated scientific evidence warrants the assertion that, on average, treatment for aphasic persons is effective” Robey, JSHR, 1995
Large gains are achieved from therapy with severe aphasic persons ◦ Need not to hang the crepe on more severe folks
Meta analysis is high level evidence
Holland et al, JSHR, 1996
“There is both experimental and clinical evidence that individuals with aphasia benefit from services of speech-language pathologists”
Contains a complete review of the literature TO THAT TIME ◦ Systematic review also strong evidence
Kelly et al (2010). Speech and language therapy for aphasia following stroke. Cochrane Database Systematic Review, Issue 5, CD000425. DOI:10,1002/14651858 CD 000425
SLT vs No SLT 14 studies 1064 participants SLT vs stimulation or social support: 6
studies 279 participants SLT method vs another 21 studies 732
participants
“some indication of the effectiveness of SLT”
Results “favored intensive SLT over conventional”
Treatment provided by a “therapist-trained and supervised volunteer appears to be as effective as the provision of SLT by a professional”
Insufficient evidence in favor of any one treatment over any other
4/10/2018
9
Brady et al. Speech and language therapy for aphasia following stroke. Cochrane Database Syst Rev. 2012. CD 000425
Identified 39 RCTs with 2418 participants ◦ 19 with 1414 compared SLT (all treatment
procedures combined) with no SLT
Results: SLT producing significant benefits on expressive and receptive language
7 RCTs comparing SLT and social support ◦ Result: No differences in functional communication
25 “randomized comparisons” (they had trouble with many of the designs) of SLTs of two different types ◦ Results: No indications of superiority of any
individual approach
“Some evidence of the effectiveness of SLT for people with aphasia following stroke in terms of improved functional communication, receptive and expressive language”
“Insufficient evidence to draw any conclusions regarding the effectiveness of any one specific SLT approach over another”
Greener et al. Speech and language therapy for aphasia following stroke. Cochrane Database Syst Rev. 2000(2). CD 000425 ◦ N=12 RCTs
◦ “Speech and language treatment on people with aphasia after stroke has not been shown either to be clearly effective or clearly ineffective within an RCT”
Suggest using other forms of evidence
• Single subject and small group data GENERALLY are accumulating showing treatment effects even in severe, several years post
• Case study • Kendall showed functional change in a person with
aphasia 40+ years post
• MRI on pt shows large chronic lesion
• Used LiPS or the phonetically based program initially developed to teach reading to children
4/10/2018
10
These were all developed for aphasia
But by changing stimuli can put them in a continuum of functional steps for AoS
Several levels of task difficulty
Stimuli are manipulated to increase or decrease difficulty:
Characteristics of items (e.g. word+color) Good “vegetable” Yellow, red or green?
Requirements of the response during the therapy games (longer or shorter)
Cueing provided if necessary to reduce error responses
Card matching task
First pt and then cl asked (without showing as barrier between) for a matching card
When pt turn cl cued with phonemic, description and other traditional cues
Goal was for the listener to produce the appropriate card ◦ And for patient to produce the right word or
approximation to allow clinician to select and hand over the correct card
Up to three patients and one clinician seated with barriers
Pairs of cards distributed so that no one has both copies of a card
Cards can be ◦ Objects, written words, drawings or photos of
complex daily activities
Also called Language Action Therapy
Turn taking with one person asking in whatever way possible who has a card similar to the one he/she has selected from individual stack
Person who has the other copy turns it over and takes a turn
Another clinician can provide cueing and encouragement
Some clinicians require only talking
Others allow gesturing ◦ And other turn it into a supported communication
task and allow/encourage any form of communication
Object is to progressively make the stimuli more difficult conceptually and linguistically
4/10/2018
11
LEVEL MATERIAL DESCRIPTION EXPECTED REQUEST
EXPECTED RESPONSE
1 Pairs of cards Single wd naming using Q inflection
Naming with Q –Bread?
Yes/no +naming
2 Pairs of cards Address player by name and us Q naming
Persons’ name-do you have (name)
Yes/no (name) I do/don’t have Name
3 Pairs displayed in 2 versions
As above but add modifier to distinguish among the two
(Name) do you have a (descriptor, eg toasted) name (bread)
Yes/no I don’t have a (descriptor) name
4 Pairs in two versions and two amounts
Add amount Name do you have amount of descriptor object
Yes/no and etc
Effect of the method continues to be demonstrated in many studies
However, ◦ Read Rose (2014) Am JSLP ◦ Loose the restraints and get same or even broader
effects
Or Wilssens et al (2015) Am JSLP showing its intensity and not program ◦ Doesn’t matter (within limits of course) what we do
as long as we do a lot of it
This program is an approximation of a functional program
And it seems few people are using the rigid constraint these days
Holland (2002). Scripts in the management of aphasia. Paper presented to the world Federation of Neurology. Villefranche, FR
Holland et al (2010). Tell me your story: analysis of script topics selected by persons with aphasia. AJSLP, 19, 198-203
More recent pubs folded into upcoming slides
Notion is simply that pt (when possible) and pt and cl when necessary create discussions of an appropriate length and difficulty ◦ Can even be for the patient single words: salmon, Kiwi, smelt ◦ Need to be relevant to pt’s life and passions ◦ Written out ◦ Parts for both Cl and Pt are typical ◦ But may be a short script for pt only to tell of an interest or
happening or wish
Then practice begins with written script in front of both persons ◦ And Cl and Pt take turns ◦ In the beginning the Cl can do the asking and cl the answering
Can be practiced first with clinician then with communication partner
Cl: Lets go eat
Pt: OK CL: Where do you want to go Panera or Satchel’s?
Pt: Satchel’s
Cl: What time shall we go?
Pt: 5:30
CL: You going to eat your usual pizza? Pt: No
Cl: So what are you going to have?
Pt: Pasta
And etc
4/10/2018
12
Clinician can do lots of cueing ◦ Highlighting key words
◦ Choral reading of pt’s part
◦ With visual and auditory cues
◦ Or delayed reading with v-a cues
Then begin fading cues
And with questions clinician can help the pt move beyond the script to related content
This is a formal way to move toward more functional communication
N=2
Script training done via videoconferencing
3 weeks of three times per week tx
Results: ◦ Both improved in scripts and functional
conversation
Accuracy
Grammatical productivity
Rate of speech
Articulatory fluency
Goldberg et al (2012). AJSLP, on line
N=3, 1 Broca, 1 Wernicke, 1 anomic
9 weeks of home treatment via computer
All improved on ◦ Content
◦ Grammatical productivity
◦ Rate of production
◦ On every script
Increased verbal communication
Increased performance in other modalities
Changes recognized by others
Increased confidence
Satisfaction with software
Cherney et al (2008). Am J SLP, 17, 19-34
Especially if they are somewhat more complex
The hard work has been done for us ◦ Kaye & Cherney (2016). Script templates: A practical
approach to Script training in aphasia. Top Lang Disord, 36, 136=153
BTW this article reviews all the articles and data until 2016.
Templates at five levels of difficulty for ◦ Ordering pizza
◦ Planning to buy groceries
Written to include 10 turns of communicator
Five levels of difficulty ◦ Give criteria for choosing as reading ability
◦ Difficulty determined by data based decisions on
Readability, grammatical and semantic complexity
Go to original article-templates are available on line
4/10/2018
13
Cherney and colleagues (2014) experimented with more and less cueing Cherney et al (2014). Acquisition and maintenance of
scripts in aphasia…AJSLP, 23, S343-S360
◦ Cues in high
Highlighting key words or even sentence
Careful modeling of mouth movements
Visual and auditory cueing and choral reading
◦ The more severe the more cueing necessary
◦ This was done via computer BTW
Aphasiascripts is trademarked computer program
A crisp little program worked out by
Dr. Yvonne Rogalski For mild moderate aphasia-usually more
posterior or fluent
Pubs: Rogalski & Edmonds (2008). Attentive Reading and Constrained Summarisation (ARCS) treatment in primary progressive aphasia: a case study. Aphasiology, 22, 763-775
Rogalski et al (2012) CAC annual convention
AR piece ◦ Read appropriately long and interesting text aloud
◦ With understanding that summarization will be the goal
◦ Can be short and easy or longer and more difficult depending on pt ability and interest
◦ Cl helps with errors in the aloud reading and does all the other traditional cueing
CS PIECE ◦ Summary is constrained by pt specific laws
◦ Laws or restraints are written down and reviewed
◦ Exs:
No general words such as stuff or thing
No extraneous info (a big one for most aphasic people)
Sometimes no pronouns so that person is required to provide names
Can cue
Can get repetition of the summary
Shape language at discourse level
The aphasic brain loses some degree of ability to select and order-in other words impaired attention
This little program structures the shaping
Seems especially useful for those with more fluent aphasias
Single patient with PPA
18 treatments of one hour in 17 weeks
Stimuli: current news of interest to pt from http://www.the week daily.com
Tested pre-post and after 2 months
Measured a number of variables including ◦ Coherence: coherent organization of main ideas
and details
◦ Cohesion: appropriate relationships of words and sentences
4/10/2018
14
No opinions
No pronouns
No non-specific words such as stuff
Written out and presented to him any time one was violated
Increased coherence
Increased cohesion
Increased words per minute and correct information units=number of information units/total number of words
Results maintained
Increased lexical retrieval
Decreased number of reading errors
In one of two patients with moderate-severe Wernicke’s aphasia
That’s all right
Evidence-based practice also gives equal status to clinical intuition
And the data will arrive




![WELCOME [ct1.medstarhealth.org] · 2016-05-05 · •Cancer is a complex disease •Some risk factors we cannot change •Many risk factors can be reduced •The more you know about](https://img.dokumen.tips/doc/110x75/5f0ea7bc7e708231d4404937/welcome-ct1-2016-05-05-acancer-is-a-complex-disease-asome-risk-factors.jpg)







![Apraxia Tt[1]](https://img.dokumen.tips/doc/110x75/557202a74979599169a3e543/apraxia-tt1.jpg)