Embed Size (px)
Citation preview

:-----
IBRITI ---II ______-- --
Anatomical studies and five years clinical experience with the distally based medial fasciocutaneous flap of the lower leg
__ _..~ _-.. _~__ _.-...
.\‘I .\l,\l.-i I( )’ Anatomical dissections, dve studies and clinical experience with the highly versatile inferiorly based medial lower leg fasciocutaneous flap, oiiginally described by Amarante et al.,’ have been described.
Clinicall uses include cover of the lower half of the tibia, foot and tendo achilles. Variations of the flap are described. The flap has been used in 42 clinical cases with only 2 failures and 2 partial failures. The dissection of the flap is quick and simple and the perforators reliable. The flap has obviated the need for a free flap in many of the cases, thus increasing, the turnover in a busy unit.
Dye injection studies and clinical experience have alerted us to the random nature of the flap in the proximal
segment as described by Amarante.’ In high risk patients we modify the design. __c___ ___~~
tlap cover for the lower half of the leg IS ;1 prohletn for the plastic surgeon. There are four possible types of tlap available: ( 1 ) A proximally based flap: (3) A distally based Ilap: (3) A cross leg flap; (3) Free tissue Iransfer.
.A pros~tnall~ based fap is often not possible. Ta\lor (‘I ~rl.‘- described ;t system of designing
t,,scijcut~i.nec,us f,lps marking out perforators with ;I Doppler. Thts opened up new avenues of flap design and enabled them to he designed safely. Amarante c’t (;/.’ in I Y8h designed ;I flap based on perforators from the postet ior tibia1 artery which are reliably constant. ?‘hc 11ap Ilax :I narrow pedicle and ;I long arc oi rlltation: Ihi pi\es Ihe flap versatility for cover over the distal t~txa or Ihe foot. Following some promising clinical ca\t’s MC decided to perform further anatomical \Ludiez and explore further clinical uses for the Hap.
‘rhc medial cc~mparrment of 5 fresh cadaver legs was dissected from distal to proximal. Three large fascio- cutaneous prrthrutorh were consistently found within I 0 cm of the medial malleolus, emergtng within the beptum bctwren the flexor digitorum longus and >oleus. The mean distances of the perforators frotn the mallcolu~ were 3.0 cm, 6.5 cm and X.0 cm. The width of the pcrfot-sting arteries ~vas 0.8--l .J tnm (mean 1 ,O mm) c\tcrnal diameter.
The postcrlor ttbial arter>’ was ligated above the second lonest perrotxtor and cannulated at the lex,el of the ankle joint. -&I) ml of Indian ink was injected slowlq into the postertor tibia1 artery in a proxitnal direction. Staining 3.)f’ Indian ink was evident over most of the
medial cc~tiipartment (Fig. I 1.
Reduced staining was evident O\IJI- the mc~dial bell! of the gastrocnrmius muscle.
Whilst dissecting distally based tlap:, LI line t)l‘ pet-fat-- alors was also noted on the posterior Ghial bc~rder. The perforator vessels are approximately 15 mm long a they cross the loose areolar tissue. Thus ma! JIOIV LI longer arc’ of rotation if the flap is islanded. One f;lirl) constant perforator LVX located IO cm ;t hove the tncdial malleolus. Another smaller one was MX~ 6 cm above this. The lower one at IO cm was uai together with the perforator at 8 cm for the island tlap mcn- tionrd below and in the faps with an extended pediclc.
Clinical experience
Afdiirlg rlw f/ti[J
Wherel,er possible. and always I+ hen the blood suppI! was in doubt. the site of perforators w’;i\ confirtned

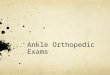
Fig. 2
Figure Z-Skin markinga of the fap
with a Doppler. The course of the posterior tibia1 artery was plotted on the skin. An 8 cm arc was drawn from the medial malleolus as the lowest point of the flap and 10 cm below the medial tibia1 plateau as the upper limit of the flap. The posterior border of the tibia was drawn as the most anterior limit of the flap. Other markings of the flap were often predetermined by existing scars. However. the width of the pedicle could be narrowed to 4 cm based on the surface markings of the posterior tibia1 vessel (Fig. 3).
Dissection of the flap starts proximally. incising down to and through the deep fascia (Fig. 3).
Occasionally the long saphenous vein and nerve may need to be sacrificed and are included in the flap. The skin edges from around the flap donor site are bevelled and sutured to the muscle with an absorbable suture and a large skin graft stapled into the flap donor site. The total operating time is approximately one and a quarter hours (Fig. 4).
Clittictrl iticiicutiott,v
We have used this flap for the following clinical conditions :
1. Primary cover of exposed shaft of tibia. medial and
7 -.
3.
lateral malleoli. tendo achilles and medial border and dorsum of foot. Chronic instability of skin over a malleolua or Ihe anterior tibia (Fig. 5). Chronic superficial osleitis of the tibia.
Modifications
This was used in three cases. Patients wcrc aped 36. 36 and 49 years. All were incorrigible smokers and one a diabetic. Ipsilateral flaps were not available. One patient had already had a failed free flap. The advantage of the distally based cross leg Hap was that normal hip and knee movements were possible, thus preventing stiffness of the leF,during the period before the flap was divided. In addition it ~vas easy to cover a larger area with less of the flap wasted as a pedicle because the distance between the two legs. by this technique, was shorter (Fig. 6).
’ Twttorw,flu/l, _.
This was used in three cases. One case \vas to cover the medial border of the foot. The flap was deepithelialised and the fascial side was skin grafted. The foot was saved and eventually healed but skin graft take on the back of the flap was poor initially and needed supplementing and it is not recommended in future for

T’his wxs used in one case. PreLious scars limited the length o;‘ the llap which was required to cover the iinterior I ibis. Extra length was gained by islanding the Ilap on t’r\o perforators at 8 cm and IO cm above the medial malleolus. This flap proved very robust and hurvived despite poor patient compliance. The perfor- ,ltors are approsima~ely I5 mm long in the subfascial layer and :illo~ ;i lot of movement.
Where the viability of the flap has been in an! way in doubt th: base of the pedicle has been broadened to include the perforator located on the posterior tibia1 horder IO cm above the medial malleolus. This can be done cas~ly if only a small arc of rotation is required. rhis \v;is done in 5 cases.
The adipnfascial modification described by Lees and Townsend” was used in one case in our series to cover .~n exposed fracture of the medial malleolus and an exposed screw. This was a late referral with much scarring .lnd tight skin. Tunnelling the pedicle of the Ilap doun to the ankle was not feasible due to its bulk. ho the tight part of the tunnel was laid open and skin crraftcd. A second adipofascial flap was tunnelled to z proGde padding where painful bony spurs resulting I’rom an old fractured tibia had been flattened.
Results
rhis tlap has heen used in 31 cases to date. bv the senior authors or in cases under our direct supervision 111 7 hospitals in Durban. with encouraging results r Table 1)
Table 1 Result5
Table 2 (.‘ompl~cat~ons
Complete loss occurred in orx cross leg Ilap III ;i
diabetic patient on the 7th da> due to in(L,t!on. The other case was the result of a damaged posterior tlbial artery. The Doppler studies prcoperati\cly had demonstrated the perforators but anpiography after the flap had failed demonstrated arterial division : blood had entered perforators distally through rctro- vade flow. c
Tip loss occurred in one flap that \IYI~ r;iihed too posteriorly ocer the belly ofthe medial gustrocnemius. The other case of tip loss was in a diabetic smoker who had previously had two unsuccessful attempt\ ;II reconstruction in another unit. After he had given up smoking the remaining pedicle was tubed and sue- cessfully waltzed into place in the traditional wa!.
Cellulitis of the flap occurred in 5 paiients with bridging pedicles but was successfull> treated \vith antibiotics in 4 and caused loss of the t1;1p in the cross leg flap.
In one case the skin of the flap necroscd but the underlying fasciu survived to support ;I skin graft.
Discussion
Our dissections confirmed the findings of Amarante r’l II/.’ that the perforators were reluti\,ell; consistent, emerging at 4.0 cm and 6.5 cm abo\c the medial malleolus. Although Amarantc did not mention the perforator at 8.0 cm he based his flaps Iron1 this spot.

642 British Journal of Plastic Surgcrq
We found a perforator at 10.0 cm on the posterior It has also been noted here that if a flap transgresses tibia1 border which was also reliably constant and the limits delineated by Amarante et d.’ e.g. is wider or useful for raising a wide flap to be transposed onto the longer, there is a high incidence of necrosis of the edge adjacent tibia. or the tip.
The perforating vessels in 2 young children emerged a correspondingly shorter distance above the malleolus but were of good calibre, nearly as large as an adult’s, The perforating vessels run a course of approximately IS mm in the loose areolar tissue between the muscle and the deep fascia. If they are carefully mobilised, the flap can be made to reach a correspondingly further distance.
Our dye studies showed dye in most of the medial compartment of the leg after injecting via the lower perforators. The faint staining over the medial belly of the gastrocnemius muscle was thought to be because it is the vascular territory of musculocutaneous perfor- ators from the medial sural artery. a branch of the popliteal artery that perforates from the medial gastro- cnemius muscle. Any flap raised in this area is ” random”.
Many of our patients are incorrigible smokers. and 10% of patients in South Africa are diabetics, all unsuitable candidates for free flap surgery. Our work- load is so great in Durban that we have been forced to rationalise our free flap surgery to limited cases. Most of our cases were salvage surgery: late referrals often after other surgeons elsewhere had had several un- successful attempts to obtain healing. The relatively high complication rate should be viewed against this background. Where blood supply is compromised we try to include perforators from the posterior border of the tibia to improve vascularity. Many of the flaps are oedematous for some weeks postoperatively. Pressure garments have helped to control the oedema in these cases.
Our most exciting development was the cross leg flap. The advantage of having the pedicle originating at the same level of the limb as the recipient site has enabled the patient to have considerable mobiliLy in bed. flexing and extending the knees and turning in bed and even standing (Fig. 7).
In our experience this flap has made a major con- tribution in distal lower leg skin cover, especially with tibia1 trauma. The lower half of the tibia cannot easily be covered except with a distally based soleus flap (which has an unreliable blood supply). a cross leg flap or a free flap. This flap is easy and quick to raise. reliable in its vasculature, and should cause minimal donor site morbidity.
The most serious problem encountered has been ol cellulitis in flaps with bridging pedicles, even though the back of the pedicle was skin grafted (Fig. 8). All of these patients were smokers and the patient who lost his cross leg flap was also a diabetic. We have learned to administer a prophylactic antibiotic in all cases with a bridging pedicle because the flap is not a highly
Fig. 7
Figure 7 --Used 3s a cross leg Rap the technique allowa rasy knee and

1. acul;lri<cd tlap and is unable to tolerate infecCon ~x~nilxired to the rt’\:erse posterior tibia1 arter!’ flap. ilrscribcd b> Hong.’
Hong’s tlap relics on an intact anterior tibia1 artery .ind in our experience the anterior tibia1 vessels arc I’requcntl!, damaged and the blood supply to the leg alread> cc~mpromised. This Hap is therefore often Ilnsuitablc for ipsilateral ~1st. For the cross leg flap the posterior tiblal flap which has subsequently been described h\; Shurma md Kola’ provides ;I safer. more i ascular tlap it‘ there 1s ;t bridging pedicle.
The latc\t Jmelopment in this flap is the adipotascial Ilap and zkin graft :I> described by Lees and Towns- cmi:’ The fascd Hap provides more length. less dog- cxjr and IW donor site morbididy. It also obviates the need for ;I bridging pedicle as the pedicle could be runnrlled under the skin. This is an improvement on I~LII’ turncl\ttr demo-fascial flap and could eliminate I hc clangcar 01‘ lnt’ection in bridging pedicles. However. II_ ;I 1‘att\ padding ib required the quality of padding ;~nd ski{; gral‘~ (v.‘:. o\‘er the tendo achill&) might not he w gocxl. A dijtally based posterior Gbial arterial ;idipot’xcial flap has also been described.”
One arc’;t I+ here the flap could be dc\,eloped with greater tinehsc ix the island Hap. The flap could be Ik~ndccl over any perforator that is locutccl by ;I Doppler proht‘ and transposed without dog-ear to ;I trrealer djstance as an island. In our case we used two - .tdj;icent perforators. The vessels appeared lung and narrow but the tlap survived well despite the patient \valking and mohing imrnedialely. The surgeon needs IO be confident in the perforating blood vessels and to ~ahc time for- A careful dissection.
Grcatcr libel-t? can safeI> be taken in children. All but the uppmn~~s~ pt‘rt’ora~or was damaged by ;I blunshot injure Ih;it shattered the tibia of a Sytxr-old : c.hild ,just above the medial malleolus. but 21 large ffap P,lpct- rrcelved 7 .Aprll IYY.:.