Embed Size (px)
Citation preview

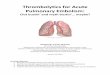
Table 2. Summary of 8 items composing pre/post training self efficacy of emergency disaster preparedness (n¼20).
Items
Pretraining PosttrainingMean
Difference1 P Value2Mean SD Mean SD
I can quickly assess and triage patients according to severity 4.05 .945 4.55 .686 .500 .029*I can manage multiple critical patients independently 3.35 1.040 4.00 1.124 .650 .004*I can prioritize procedures based on patients needs and
potential outcomes4.00 .918 4.60 .883 .600 .004*
I can prioritize and reorder access to testing/studies based onpatient critical needs
3.95 .999 4.50 .761 .550 .012*
I understand when to contact hospital administrationfor additional resources
3.55 1.234 4.35 1.182 .800 .032*
I understand hospital incident command system 2.55 1.276 3.15 1.565 .600 .019*I can effectively be a member of a disaster team 3.85 1.089 4.70 .657 .850 .002*I can effectively lead a disaster team 2.90 1.021 3.90 1.119 1.000 <.001*
1Mean difference¼posttest mean pretest mean.2Statistical significance level at .05.*Statistically significant at .05. (Paired sample t test.)
CORD Abstracts
for Teamwork Effectiveness and Patient Safety (STEPS) training questionnaires andtrainee satisfaction with the training model.
Results: Our residents demonstrated statistically significant improvement in 11 of14 competencies and reported high levels of satisfaction on 5 qualitative assessmentquestions (Table 1).
Conclusion: We evaluated using high-fidelity simulators in a simulatedmulticasualty disaster drill as a training experience for EM residents (Table 2). Allresidents indicated that exposure to a simulated disaster was a valuable educationalexercise and made significant improvement in their understanding of disaster medicineconcepts and team dynamics. The residents indicated increased confidence in theirability to manage a multiple casualty situation. They perceived that they had achievedbetter understanding of the challenge of managing a multicasualty disaster than theywould have from a lecture format. Simulated disaster training provides a realism thatcannot be achieved in other formats and may be the ideal educational method fordisaster education.
The “Bird’s Eye View”: A Novel Use of Video Assisted
33 Debriefing in Medical SimulationParry T, Stahmer C, Josephson E/Lincoln Medical & Mental Health Center, Bronx, NYIntroduction/Background: Simulation (SIM) is an important learning aid toevaluate medical knowledge, team skills, and decisionmaking. Debriefing participants isa crucial aspect of this process. Video-assisted debriefing (VAD), a common tool forthis purpose, often provides a global view as opposed to focusing on the team leader’sexperience.
Educational Objectives: The “bird’s-eye view” VAD is intended to assess theleader’s proficiency while directing a team through a simulated case and further usingthat information for didactic purposes.
Curricular Design: Cases obtained from various sources were programmed on aLaerdal SimMan 3G. A resident team chosen (cross-section of training levels) wasprovided with a pre-SIM survey. A team leader selected to supervise the resuscitationwore a forehead-mounted GoPro video camera used to record the SIM. The teamdiscussed details of the session before being given a post-SIM survey. The team leaderthen developed a brief interactive presentation describing their case. The GoPro videoand the presentation were then shown during a weekly didactic conference, allowingresidents who were not involved to learn from the team’s experience. After theconference, the same team completed a final postconference survey.
Impact/Effectiveness: The initial acceptance for this training tool was very high(rated 4 on a 4-point scale). Residents experienced an increase of 13% (2.38 to 2.68) intheir subjective comfort level in caring for critically ill patients, with the greatestimprovement noted in the intern class (1.5 to 2.5). In addition, residents thought thisallowed a worthwhile teaching experience in conference (rated 4), portraying them asan expert rather than being judged by their peers (3.5).
The bird’s-eye view model presents a novel and valuable tool for VAD whileproviding an opportunity to use these experiences for resident education on a largerscale rather than the traditional team-specific approach.
Volume 62, no. 5 : November 2013
Ability of Emergency Medicine Residents to Appropriately
34 Administer Thrombolytics for ST Elevation MyocardialInfarction During Small Team Based SimulationKoboldt T, Wagner J, Sampson C/University in St. Louis School of Medicine,St. Louis, MO
Background: Acute ST-elevation myocardial infarction (STEMI) is a time-criticaldiagnosis requiring efficient diagnosis and treatment. Roughly 1.5 million people haveacute myocardial infarction every year in the United States. A more favorable outcomehas been shown in those patients who receive appropriate, timely administration ofthrombolytics.
Annals of Emergency Medicine S177

CORD Abstracts
Objectives: To assess the ability of resident physicians to appropriately administerthrombolytics (door to lytic time of 30 minutes) for STEMI during a small team–basedsimulated patient encounter without making a critical error.
Methods: This was a pilot study involving EM residents at an academic residencyprogram. Twenty-seven residents participated in separate small group simulationsbetween November 2010 and November 2011. Each team consisted of 1 resident with2 ED RNs. The scenario was a patient presenting with STEMI and no availablecatheterization laboratory, requiring administration of thrombolytics within30 minutes. This challenged the residents because at this institution there is continuouscatheterization laboratory availability so thrombolytics are rarely (4 times/year) givenfor STEMI. Encounters were video recorded and then later reviewed and scored byresearch assistants. A critical error was failure to administer thrombolytics within the30-minute time frame of the case, lack of adequate laboratory workup, not reviewingradiograph, or failure to assess contraindications before thrombolytic administration.
Results: In this study, 93% (25/27) of residents gave thrombolytics, but only 37%(10/27) did so without making a critical error. Of those who gave thrombolytics, 60%(15/25) did so after making a critical error.
Conclusion: During small-group simulation, only 38% of residents were able toappropriately give thrombolytics for STEMI. In training institutions wherethrombolytics are rarely given because of readily available catheterization laboratories,there appears to be a knowledge gap on the appropriate administration ofthrombolytics for STEMI.
Comparison of Sealants’ Ease of Use for Dental Fractures in
35 the Emergency DepartmentHealy K, Peterson T, Rogers J, Edwards A/University of Alabama at Birmingham,Birmingham, ALBackground: Radio-opaque calcium hydroxide and zinc oxide/eugenol are 2 dentalsealants commonly used in the ED. Research addressing perceived complexity applyingthese sealants for fracture repair is limited.
Objectives: To compare the level of difficulty involved with mixing and preparingradio-opaque calcium hydroxide and zinc oxide/eugenol for application.
Methods: Twenty residents filled out a 5-question pretest survey measuringprevious dental fractures repaired, as well as comfort level managing fractures,knowledge of dental sealants, and ability to prepare and apply dental sealant. The last4 questions used a scale from 1 to 10, with 1 being very uncomfortable. Residentsattended a dental fracture lecture and then practiced applying 2 types of sealants,calcium hydroxide (Dycal) and zinc oxide/eugenol (Temrex), to models. Afterwards,residents completed a posttest survey with the 5 pretest survey questions, as well as aquestion comparing the complexity of preparing Dycal and Temrex, using the same 1to 10 scale.
Results: Aggregate scores of the pre- and posttest surveys were compiled and meanscores calculated. The mean pretest knowledge of dental sealants was 4 (IQR 2 to 6.5),with a mean posttest knowledge of 8 (IQR 7.5-9), P<.001. The mean pretest score forability to prepare dental sealant was 3.5 (IQR 2 to 7), whereas the posttest mean was9 (IQR 8 to 9), P<.001. The ability to apply dental sealant had a mean pretest score of4.5 (IQR 3 to 7) and posttest score of 9 (IQR 8 to 9), P<.001. The mean perceivedlevel of complexity of preparing radio-opaque calcium hydroxide was 2.3, whereas themean for zinc oxide/eugenol was 3.7.
Conclusions: Although future research should increase sample size, this researchshowed improved resident confidence preparing and applying dental sealants after abrief educational workshop. There was no statistically significant difference incomplexity preparing and applying calcium hydroxide versus zinc oxide/eugenol.
Teaching Common Clinical Procedures to Emergency
36 Medicine Residents: Efficacy of Simulation Task TrainersVersus Fresh Tissue CadaversJhun P, Levine M, Shoenberger J/Los Angeles County, University of Southern CaliforniaMedical Center, Los Angeles, CA; University of Southern California Medical Center,Los Angeles, CA
Background: Simulation task trainers are the most commonly used educationalmodality in emergency medicine (EM) residency programs for hands-on teaching andpracticing procedures prior to clinical exposure. Cadavers in fresh tissue dissectionlaboratories (FTDL) have been used with great success in training postgraduate
S178 Annals of Emergency Medicine
physicians in various surgical subspecialties but have been underused in EMresidencies.
Objective: This study compares the efficacy of simulation task trainers to freshtissue cadavers in improving the self-assessed confidence of EM residents whenperforming common clinical procedures.
Methods: Setting: The Department of Emergency Medicine at the Los AngelesCounty+USC Medical Center has access to a simulation center with task trainers and aFTDL supplied with fresh cadavers.
Subjects: Seventeen PGY-1 EM residents participated in this study duringresidency orientation.
Design: Prior to instruction, residents completed a self-assessment survey using a10-point Likert scale, which was designed to assess clinical confidence in performingthese procedures: intubation, central line placement, and chest tube insertion.Residents then received a 30-minute didactic lecture on each procedure and practicedeach procedure on simulation task trainers. Two weeks later, residents practiced thesame procedures on fresh cadavers. Residents completed the same survey assessingclinical confidence, after having completed the simulation task trainers and the FTDL.
Results: All 17 residents completed the pre- and postsurveys. Prior to instruction,the overall mean baseline confidence level of all residents on a 10-point scale was 4.7.Postsimulation task trainers, the mean confidence level was 5.1. Post-FTDL, the meanconfidence level was 6.8 (Tables 1 and 2).
Conclusions: The use of fresh tissue cadavers appears to have a greater effect thansimulation task trainers on the confidence of PGY-1 EM residents in performingcommon clinical procedures in EM.
Table 1. PGY 1 Mean Confidence Scores.
BASELINE POST TASK TRAINER POST FTDL
Volume 62, no. 5 : Nove
4.7
5.1 6.8Table 2. Confidence Scores By Procedure.
BASELINE POST FTDL
Endotracheal Intubation
4.9 6.9 Central Line Placement 4.9 6.8 Chest Tube Insertion 4.2 6.7FAST Wars: Assessing Competency and Speed in a
37 Simulated Trauma PatientDuran Gehring P, Jacobson L, Saldana N/University of Florida Jacksonville,Jacksonville, FLBackground: The Focused Assessment with Sonography in Trauma (FAST)examination has long been used for the assessment of trauma patients and is aprocedural competency in emergency medicine residency training. Skills laboratories,written examinations, and standardized patients have previously been used to assessFAST examination skills; however, we wanted to assess the ability of our residents toperform this examination in a real-world scenario. Execution of the FAST examinationduring a trauma assessment can expedite diagnosis and treatment, but distracters canimpede examination performance. We assessed resident FAST performance during asimulated trauma scenario in which they had to work around the trauma teamperforming the assessment, deal with a difficult patient, and finish in a timely manner.
Methods: Residents were timed individually performing a FAST examination,using standardized views, on a simulated trauma patient who decompensates during the5-minute scenario. Obstacles were created at specific intervals, increasing in frequencyafter the 2-minute goal for examination completion. Examinations were timed fromthe input of patient identifying data into the ultrasonographic machine until either thetime had expired or the examination was completed. Residents were not forewarnedabout the simulation to assess baseline abilities.
Results: Although checked off on the FAST during their US rotation, only 10% ofresidents completed the examination within 2 minutes and 38% were unable tocomplete it within 5 minutes. We found 4 common errors in residents unable toperform the FAST examination rapidly: the inability to work with the trauma team,
mber 2013