Embed Size (px)
DESCRIPTION
Â
Citation preview

JULY/AUGUST 2014VOLUME 20 | NUMBER 4
Page 3 Inside: MCMS Past President
Kelly O’Keefe, MD, Passes the Gavel to Incoming President Jeffrey Keating, MD
SCCMA Past President
Sameer Awsare, MD,
Passes the Gavel to
Incoming President James
Crotty, MD

2 | THE BULLETIN | JULY/AUGUST 2014
65606, Santa Clara/Monterey, (7/14)Full Size: 8.5” x 11” Bleed: 8.75” x 11.25” Live: 7.5” x 10”Folds to: N/A Perf: N/AColors: 4c=(Process) Stock: N/A Postage: N/A Misc: N/AM
ERCE
R
A former employee sued me for wrongful termination.
For more information on these important benefits, and the special SCCMA/MCMS First-Time Buyers Program, please contact Mercer at:
800-842-3761
or email us at [email protected]
Sponsored by:
65606 (7/14) Copyright 2014 Mercer LLC. All rights reserved. • 777 S. Figueroa St., Los Angeles, CA 90017 www.CountyCMAMemberInsurance.com • [email protected]
Mercer Health & Benefits Insurance Services LLC • CA Ins. Lic. #0G39709 • 800-842-3761
You are not alone. Employment-related lawsuits are more common. What many physicians don’t realize is that help is literally a phone call away. SCCMA/MCMS members have access to a unique blend of risk management services and insurance specifically designed to assist physician groups in addressing these important employment issues. Among the features of the sponsored Employment Practices Liability program are:
A Helpline staffed by experienced employment defense attorneys. Any manager, officer or principal of your practice has access to the Helpline for obtaining advice on handling workplace issues, including internal sexual harassment complaints, discipline and employee terminations.
If a member seeks and follows Helpline advice on an employee termination or demotion which later results in a claim, there is a 50% reduction of the member’s EPLI deductible for that claim.
Free, comprehensive criminal background checks for newly hired and promoted managers/supervisors.
EEO compliance training for managers/supervisors. An internet-based training program, compliant with California law, provides supervisors with sexual harassment training.
Optional Wage and Hour Defense Coverage. (Subject to additional premium.)
Ask about our First-Time Buyers Program.

JULY/AUGUST 2014 | THE BULLETIN | 3
MCMS Past President Kelly O’Keefe, MD, Passes the Gavel to
Incoming President Jeffrey Keating, MD

4 | THE BULLETIN | JULY/AUGUST 2014
OFFICERSPresident
James Crotty, MDPresident-Elect
Eleanor Martinez, MDPast President
Sameer Awsare, MDVP-Community Health
Cindy Russell, MDVP-External Affairs
Kenneth Blumenfeld, MDVP-Member Services
Peter Cassini, MDVP-Professional Conduct
Seema Sidhu, MDSecretary
Seham El-Diwany, MDTreasurer
Scott Benninghoven, MD
CHIEF EXECUTIVE OFFICERWilliam C. Parrish, Jr.
AMA TRUSTEE - SCCMAJames G. Hinsdale, MD
CMA TRUSTEES - SCCMA Thomas M. Dailey, MD
(District VII)Martin L. Fishman, MD
(District VII)Randal Pham, MD
(Ethnic Member Organization Societies)Tanya Spirtos, MD
(District VII)
COUNCILORSEl Camino Hospital of Los Gatos:
Arthur Basham, MDEl Camino Hospital:
Laura Cook, MDGood Samaritan Hospital:
David Feldman, MDKaiser Foundation Hospital - San Jose:
Hemali Sudhalkar, MDKaiser Permanente Hospital:
Anh Nguyen, MDO’Connor Hospital:
Michael Charney, MDRegional Med. Center of San Jose:
Erica Timiraos, MDSaint Louise Regional Hospital:
Diane Sanchez, MDStanford Hospital & Clinics:
Vanila Singh, MDSanta Clara Valley Medical Center:
Richard Kramer, MD
Printed in U.S.A.
EditorJoseph S. Andresen, MD
Managing EditorPam Jensen
Opinions expressed by authors are their own, and not necessarily those of The Bulletin, SCCMA, or MCMS. The Bulletin reserves the right to edit all contributions for clarity and length, as well as to reject any material submitted in whole or in part. Acceptance of advertising in The Bulletin in no way constitutes approval or endorsement by SCCMA/MCMS of products or services advertised. The Bulletin and SCCMA/MCMS reserve the right to reject any advertising.
Address all editorial communication, reprint requests, and advertising to:
Pam Jensen, Managing Editor 700 Empey Way San Jose, CA 95128 408/998-8850, ext. 3012 Fax: 408/289-1064 [email protected]
© Copyright 2014 by the Santa Clara County Medical Association.
THE SANTA CLARA COUNTY MEDICAL ASSOCIATION
THE MONTEREY COUNTY MEDICAL SOCIETYBULLETIN
THE
Official magazine of the Santa Clara County Medical Association and the Monterey County Medical Society
OFFICERSPresident
Jeffrey Keating, MDPresident-Elect
James Hlavacek, MDPast President
Kelly O'Keefe, MDSecretary
Patricia Ruckle, MDTreasurer
Steven Vetter, MD
CHIEF EXECUTIVE OFFICERWilliam C. Parrish, Jr.
DIRECTORSPaul Anderson, MD Valerie Barnes, MD
Ronald Fuerstner, MD Gary Gray, DO
Steven Harrison, MD David Holley, MD John Jameson, MD
William Khieu, MD Eliot Light, MD
Edward Moreno, MD Marc Tunzi, MD Craig Walls, MD
Cary Yeh, MD
AMA TRUSTEE - MCMSDavid Holley, MD

JULY/AUGUST 2014 | THE BULLETIN | 5
Feature Articles 14 MCMS’s Annual Awards Banquet and Installation
18 SCCMA Award Presentations and Installation
26 SCCMA Awards Banquet Photos
38 Food Addiction Program for Food Addicts of All Ages
40 Patient Behavior: The Key to Improving Patient Outcomes
44 Managing the Risks of Treating Chronic Pain With Opioids
46 Three Things Every Physician Should Know About Covered California
Departments 6 From the Editor’s Desk
7 Message From the SCCMA President
8 Final Message From the Outgoing SCCMA President
10 Message From the MCMS President
12 Message From the CEO
35 SCCMA Alliance Foundation
36 Choosing Wisely
48 Medical Times From the Past
50 Classified Ads
52 Member Spotlight: Joseph Andresen, MD
53 SCU Students Give Their Talents
BULLETINTHE
Official magazine of the Santa Clara County Medical Association and the Monterey County Medical Society
MEMBER BENEFITS
Billing/Collections
CME Tracking
Discounted Insurance
Financial Services
Health Information Technology
Resources
House of Delegates
Representation
Human Resources Services
Legal Services/On-Call Library
Legislative Advocacy/MICRA
Membership Directory iAPP for
the iPhone
Physicians’ Confidential Line
Practice Management
Resources and Education
Professional Development
Publications
Referral Services With
Membership Directory/Website
Reimbursement Advocacy/
Coding Services
Verizon Discount
700 Empey Way • San Jose, CA 95128 • 408/998-8850 • www.sccma-mcms.org

6 | THE BULLETIN | JULY/AUGUST 2014
By Joseph S. Andresen, MDEditor, The Bulletin
Leadership is a quality of character that has many facets. A visionary, a good communicator, having tireless energy, willingness to make person-al sacrifices for the common good, and the ability to inspire others are all traits that come to mind.
There is no easy or simple path to becoming a great leader. Some may have many of these qualities that are never realized. For most, it is often an unexpected opportunity to step forward with a willingness to serve oth-ers. And it is not until this occurs, do we begin to understand who we are, our strengths and weaknesses and ability to grow with the greater respon-sibilities bestowed upon us. What kind of leader could you be? Are you willing to step forward and find out?
Dr. Sameer Awsare, a board cer-tified internist, leaves office as our 2013-2014 outgoing President of the Santa Clara County Medical Associa-tion. Over this past year, Dr. Awsare has given us all a much clearer under-standing of the many challenges facing our medical community during his tenure. As so well stated in his incom-ing remarks entitled, “Your Voice is the Key to Our Success,” we all know the importance of involvement with our medical organization. His high-lighting advanced care planning with a glimpse of the success in La Crosse, Wisconsin, sets a new high bar for us to emulate. Health Insurance Exchanges and Covered California oppor-tunities and pitfalls are now more well understood, thanks to Dr. Awsare’s attention to this important topic. The MICRA challenge and prescription drug overdoses are equally important areas that must garner our contin-ued attention.
Dr. Kelly R. O’Keefe, a board certified pathologist, leaves office as this past year’s President of the Monterey County Medical Society. From all accounts, he will be missed for his wit and, by his own admission, brev-ity in his initial incoming remarks. As CEO of Adaptive Clinical Solu-
tions, physician members have also benefited from Dr. O’Keefe’s analyti-cal mind and abilities as a problem solver. I had forgotten how valuable a resource Index Medicus was back in the day, and have since learned that its last 2004 publication weighed over 150 pounds, making it a difficult resource to use on rounds. Dr. O’Keefe offered some helpful advice on our attempts to keep up with this information over-load. I am now reading the medical literature with a bit more skepticism after his highlighting a recent article by Dr. John Joannidis’s article, “Why Most Published Research Findings Are False.” Perhaps with PubMed’s almost two-thirds of a million new cita-tions each year, we may find that we need the big data talents of the Na-tional Security Agency to help us find the absolute truths!
From my medical school days, it was said that internists know every-thing, but do nothing. Pathologists know everything, do everything, but when it’s too late. I have to say that Drs. Awsare and O’Keefe completely dispel these self-deprecating adages. Both leaders have shared their wis-dom and insight with clear vision and, in doing so, inspired us all to con-tinue to promote the vitality of our medical community for the betterment of our patients. Now that’s great leadership! Thank you Drs. Awsare and O’Keefe for your service!
FROM THE EDITOR’S DESK
Thank You Past Presidents
JOSEPH S. ANDRESEN, MDEditor, The Bulletin
Joseph S. Andresen, MD, is the editor of The Bulletin. He is board certified in anesthesiology and is currently practicing in the Santa Clara Valley area.

JULY/AUGUST 2014 | THE BULLETIN | 7
By James R. Crotty, MD, MBAPresident, Santa Clara County Medical Association
I am excited and honored to hold the highest office in the Santa Clara County Medical Association. My first responsibility was to accept the offi-cial passing of the gavel, with photo ops, at the annual awards ceremony at the Fairmont hotel on June 17, 2014. At this energetic gathering, I also had the pleasure to hear the comments from the people selected by our Awards Committee to be awarded and recognized for contributions to the medical association, the medical community, and public health. I wish to thank Lisa Krieger for helping us understand how the treatment of her father, at the end of life, triggered a must-read award winner series of articles in the San Jose Mercury News. I wish to thank Gay Crawford for helping us understand how her early battles, fighting and surviving cancer, inspired her to help hundreds of other cancer patients. I wish to thank Jonathan Blum, MD, for injecting his humor and enthusiasm that has character-ized his dedication to teaching medical students, interns and residents. I wish to thank Keith Fabisiak, MD, for explaining how his simple love of gardening inspired him to become involved in the community, teaching sustainable food systems. I wish to thank Gary Hartman, MD, for helping us see a great man whose humility gave credit to his team for the success in treating surgical pediatric disease. I wish to thank David Campen, MD, for his courage and contributions to organized medicine. I especially wish to thank Marty Fishman, MD, who gave us inspiration to continue to con-tribute to patient care in addition to seeing patients in the office.
The Santa Clara County Medical Association needs to continue its mission of promoting the medical profession, continuing our dedication to public health, and contributing to the satisfaction of physicians in Santa Clara County who are engaged in the challenging, rewarding, privileged, but also very stressful occupation of being a physician.
Just as how I know that all bicyclists are judged by how I ride, and how I signal, as I ride my bicycle home from work, I know that all physicians are judged by the actions of other physicians. Unfortunately, what grabs the headlines is about the negative. We want people to think of physicians as competent, well-trained, empathetic, considerate, and caring. We must act this way and also state this is what people should expect.
At the awards dinner, I did take the opportunity as president to speak about the threatening ballot initiative that can only increase costs, leading to decreases in access to care. This initiative was submitted to the attorney general as the “Troy and Alana Pack Patient Safety Act of 2014.” Troy and Alana Pack were tragically killed by a reckless driver in 2003. The father, Robert Pack, has been active trying to have stricter laws for prescription pain medications. He has been an advocate for the Controlled Substance Utilization Review and Evaluation System (CURES) established in 2008 by the California Department of Justice. He has also joined forces with
Consumer Watchdog, a non-profit organization that advocates for con-sumer interests. This year, the trial lawyers have joined with Consumer Watchdog and Robert Pack to launch a campaign to change the Medi-cal Injury Compensation Reform Act (1975). This ballot initiative has three main requirements: 1) Doctors will need to check the CURES data-base prior to prescribing pain medications; 2) Doctors must submit to be drug tested; and 3) The current cap on non-economic damages would be changed from the current $250,000 to $1.4 million or more.
We know that the CURES database is not robust enough at this time to support the millions of requests needed. There are also significant data privacy issues and concerns about how the information will be used. We also know that the drug testing, as outlined in this initiative, is completely impractical. There is no evidence that this would improve patient safety. It would also be prohibitively expensive.
The increase in the cap for non-economic damages would certainly lead to higher malpractice premiums. About half the states in the United States have caps. The malpractice rates are currently 4-5 times more ex-pensive in comparable examples. There would be an increase in the num-ber of allegations and suits. The cost of this initiative is being underwritten to a large extent by trial lawyer organizations. These changes to MICRA would primarily benefit the income of trial lawyers.
Many have said this, but at this time there is intense pressure to con-trol costs. The Affordable Care Act has created another incentive for health insurance companies to pay less. There is now a large coalition of business, labor, and professionals who have denounced this ballot initiative (Propo-sition 46). We can expect underhanded and “guerrilla” tactics from Con-sumer Watchdog. The medical profession will be examined and be in the spotlight. Fortunately, our membership dues have created an experienced and hard-working organization led by CMA CEO Dustin Corcoran. There has been a large amount of donations to fight this misleading and costly proposition that will decrease access to health care, just at a time when we are trying to increase access and decrease the millions of people who are uninsured in California.
We must work together. Encourage any physicians who are not mem-bers of CMA to join. Talk to family and friends. Inform patients. Contrib-ute money to the campaign. Do everything that you can to defeat Propo-sition 46. Approval of Proposition 46 by the voters in November would severely damage our efforts to increase access and control costs for medi-cal care delivery in California. Please join the fight to defeat this proposi-tion!
MESSAGE FROM THE SCCMA PRESIDENT
Inaugural Address
JAMES R. CROTTY, MD, MBAPresident, Santa Clara County Medical Association
James R. Crotty, MD, MBA, is the 2014-2015 president of the Santa Clara County Medical Association. He is a urologist and is currently practicing with The Permanente Medical Group/Kaiser in San Jose.

8 | THE BULLETIN | JULY/AUGUST 2014
By Sameer V. Awsare, MD, FACPPast-President, Santa Clara County Medical Association
The following speech was presented at SCCMA’s Annual Awards Ban-quet and Installation Dinner on June 17, 2014.
Good evening, fellow physician members of the Santa Clara County Medical Association, family members, distinguished guests, and spon-sors. It is my honor and privilege, and my final opportunity, to address you as the 78th President of the Santa Clara County Medical Association (SCCMA). I would like to begin by thanking Bill Parrish, our CEO, and his team – Mark, Jean, Sandie, Pam, Shannon, Maureen, and Molly for the incredible job that they have done over the last 12 months. They have not only supported me personally in my role as President, but have always been available to assist our Executive Committee, Council, Officers, mem-bers, patients, and community. Their work has not only allowed the SC-CMA to fulfill its mission, but has also made our medical association the largest, in terms of membership, in the entire state of California. This has brought us recognition and given us significant influence in the legislature and within the house of medicine. Over the last 12 months, the SCCMA and our Bureau of Medical Economics have done well. They exceeded their financial expectations, and the SCCMA surpassed its membership recruitment and retention goals. So lets have a big round of applause for Bill and the SCCMA team!
The last 12 months have been a turbulent and disruptive time in health care. The Affordable Care Act was actually implemented and, in our state, we now have our own health insurance exchange called Cov-ered California. For the first time in history, millions of people now have health insurance. Depending on which plan they purchased, people still have a significant deductible. For instance, the Covered California Bronze plan has a $5,000 deductible before any insurance kicks in. For the most vulnerable of our citizens, this is a tough decision about whether to spend money on seeing the doctor, putting gas in their car, paying for clothing, or feeding their children. The delivery system is challenged as well, with a shortage of physicians to see these patients, and with California’s Medi-Cal reimbursements being 47th out of 50 in the nation, the task becomes even more difficult. Then, there is a shortage of residency slots in our state due to which our well trained University of California medical students have to look for positions outside our state. Many then end up living and practicing outside California. Needless to say, our health care system has begun to change and, like Medicare, it will need years of amending to get even better. However, it is imperative that physicians and their patients have a major voice in this process.
Critical issues that affect physicians in our state are being decided by
our legislature. At CMA’s 40th Annual Legislative Leadership Day, we lob-bied our legislators about restoring the 10% cut in Medi-Cal rates, trans-parency in health insurers’ contracts with physicians, scope of practice issues, reimbursement for telephone/electronic management of patients, and increasing residency training slots in California. We also asked our legislators for their commitment to protect MICRA, which the trial law-yers are attempting to repeal in an effort to increase their own incomes. I was happy to see that medical students, residents, and physicians from solo, small group, large group, county, and academia were united and speaking with the one voice of the house of medicine. I am disappointed that our colleagues from Stanford have still not joined the SCCMA to show their support and to ensure that their voice is also heard, and I chal-lenge them to do so.
As SCCMA President, I had the opportunity to hear stories from my colleagues. A surgeon complained about his Blue Shield contract that in-cluded a 70% reduction in reimbursement for Covered California patients. They were trying to force him to sign the contract by telling him that he would not get to see Blue Shield PPO patients if he did not sign. Another colleague, who is an OB/GYN in Campbell/Los Gatos, told me that she needed to earn $250 an hour just to keep her office open. Anything she made above that she could take home. With the new rate reductions she had received, she was not sure she could keep her doors open. Another col-league told me that he was listed as a Covered California provider by Blue Cross, but he did not ever remember signing a contract with them. Every day, he gets patients that he was not sure were covered by his usual Blue Cross Plan, since often the membership card does not have the Covered California logo. It usually took his staff 45 minutes to figure out if the pa-tient even had coverage, and he was turning away over three patients a day. Finally, another ophthalmology colleague discussed Medi-Cal reimburse-ment, which had decreased so much that he had to stop taking Medi-Cal patients this April, after taking them for over 20 years. He felt really guilty about this since he had been a Medi-Cal patient as a child. He said the $24 he got for a patient visit was about the price for a delivery of a large pizza to his home, and at that rate, he was losing money on every Medi-Cal patient he saw. These are stories that I will not forget and they highlight the chal-lenges that physicians are facing and why it is important for physicians to speak with one voice.
The tidal wave of change in health care has created significant stress on physicians. So why continue to practice? Recently, I reflected on why I
MESSAGE FROM THE SCCMA PAST-PRESIDENT
Outgoing President’s Speech
SAMEER V. AWSARE, MD, FACPPast-President, SCCMA
Sameer V. Awsare, MD, FACP, was the 2013-2014 president of the Santa Clara County Medical Association. He is a board certified internist and is currently practicing with The Permanente Medical Group in Campbell.

JULY/AUGUST 2014 | THE BULLETIN | 9
became a physician. I really enjoy helping people and feel that, as a physi-cian, I have a unique opportunity to change my patients’ lives for the bet-ter. My role models were my grandparents, who were both physicians. My grandfather was a family physician who often made several home visits, starting at 6:00 a.m., before he started clinic at 9:00 a.m. He saw patients until about 12:30 p.m., and then came home for lunch and a siesta. He would then take a break and spend time reading, writing, composing mu-sic, painting, or hanging out with his artist friends. He would then start clinic again, at 5:00 p.m., and keep going until every patient was seen. Sometimes this was 8:00 p.m., but often it was 9:30 p.m. My grandmother was an OB/GYN and she would get up early to make hospital rounds, after which she was either in clinic or in surgery. She was on-call every day and night for her deliveries and she had a lot of them since there were not many women OB/GYNs in 1928. She often took us on her “social service” mis-sions that could include teaching kids, working at a camp, or even clean-ing sewers. Nothing was beneath us (although sometimes the stench was unbearable) and she frequently reminded us that Mahatma Gandhi had cleaned the toilets of the untouchables. I remember when I was in medi-cal school, HIV was a new disease, and we were scared to touch patients without wearing a mask, gown, glasses, and gloves. I remember my grand-
mother telling me that these patients were human, just like the rest of us, and that I should not be afraid to touch them and take care of them. She reminded me that when she was in training, they had a disease called tu-berculosis, and that she had cared for many patients with TB when her colleagues were afraid to do so. The profession of medicine is one of the noblest and I don’t see myself doing anything else. We have a shortage of primary care physicians that is only going to grow, so I encourage you to ask your kids and grandkids to become physicians.
I cannot leave without taking a few minutes to talk about advance care planning, which is a topic that is important to me. Although a major-ity of Americans state that they want to die at home, today 80% of Ameri-cans die in hospitals or nursing homes. Unfortunately, all of us know a story of a patient who declines faster than expected, and loses the ability to speak for him or herself, leaving loved ones to make decisions on their behalf. Generally, the patient has never had a conversation with his or her loved ones about their wishes, hence, family members are left to guess. According to the Centers for Disease Control and Prevention (CDC), only
30% of patients prepare Advance Directives so that their wishes can be known during periods of incapacity or at the end of life. The SUPPORT trail showed that even when a patient had an advance directive, about 50% of the time their wishes were not respected by health care professionals. The good news is that it doesn’t have to be this way and there are places in the country where they are doing better. A glimpse of this can be found in La Crosse, Wisconsin, where Gundersen Health System pioneered a pro-gram called Respecting Choices, which is a systematic approach to advance care planning that includes detailed conversations with patients and their health care agents by highly trained facilitators.
A recent review of the deaths that occurred in La Crosse showed that an astounding number of the patients (96%) had either a written advance directive or a Physician Orders for Life-Sustaining Treatment (POLST) that were readily available to the patient’s family and health care profes-sionals, hence, there was a 99% consistency between decisions made on behalf of patients and their expressed wishes. If any geography is capable of developing a more integrated approach to advance care planning, you’d think it would be right here in Silicon Valley! I believe that our Santa Clara County Medical Association has a critical role in making communi-ty-based advance care planning a reality, and seated in the room today are
fellow physicians, the chiefs-of-staffs of the various hospitals in our com-munity, insurance executives, and Lisa Krieger from the San Jose Mercury News. Lisa was courageous to share the story of her dad’s final days with all of us in Silicon Valley and I have particularly enjoyed her series on the “Cost of Dying.” I want to challenge all of you in this room to commit to working together in our county to match the performance of La Crosse, so that the wishes of all of our patients are honored when they are no longer able to speak for themselves.
In closing, I have some advice for our new President, Jim Crotty, MD (Jim, I hope you don’t mind). The first is to be prepared and read every-thing you are sent. Always keep thinking about topics for your next Bul-letin article. Consult with Bill and his team since they know a lot, if not ev-erything! Manage your meetings well. Don’t meet just to meet, and finish on time, or even early. Be available by phone, text, or email. Finally, let Bill and his staff do their job. I look forward to your year as President, and let me know how I can be of help.

10 | THE BULLETIN | JULY/AUGUST 2014
MESSAGE FROM THE MCMS PRESIDENT
Inaugural Address
JEFFREY KEATING, MDPresident, Monterey County Medical Society
By Jeffrey Keating, MDPresident, Monterey County Medical Society
The following speech was presented at MCMS’s Annual Awards Ban-quet and Installation Dinner on June 5, 2014.
I am deeply honored to have been chosen as President of the Mon-terey County Medical Society. I would like to recognize the fine job Kelly O’Keefe, MD, has done as the preceding president. Special thanks go to Dr. James Ramseur, who encouraged my participation in the society and who served as a role model on how to be an effective president.
Monterey is an exciting place to practice medicine, and with such excellent institutions and staff from places such as Salinas Valley Medi-cal Center, Natividad Medical Center, Community Hospital of the Mon-terey Peninsula, Mee Memorial, Clinicas de Salud, and numerous well run multidisciplinary and group practices, as well as private offices, there is a wealth of physician expertise and experience, and I look forward to repre-senting them all.
The major emphasis of my term will be the MICRA ballot initiative, a battle from which we cannot walk away from as a medical community. I will not address the specifics of the battle, as that will have been done/has been done by our keynote speaker, Francisco Silva. Rather, I will address the specific steps we need to take to win this battle. The main approach is by increasing membership in the society. The increased numbers and, yes, money will go a long way to giving us a louder voice. To that end, I chal-lenge every current member of the society to bring up the issue of MICRA with at least one colleague and personally invite them to join the fight by becoming members of the society. The next is to educate non-physician members of the community, be it friends, coworkers, or neighbors about the potential negative consequences of a successful ballot initiative in No-vember 2014. At times, it seems that there is too much division within our ranks, be it primary care versus specialist, or one hospital system versus another. Beyond the MICRA fight, the increased membership and phy-sician participation will pay dividends as there are many other forces at play against us, and I feel that our best chance of success in advocating for ourselves and our patients is by working together.
Before I wrap up, I would like to thank Congressman Sam Farr for his ultimate success in his greater than 15-year tireless effort to fix the Geo-graphic Practice Cost Index (GPCI) problem. Briefly, this was the formula in use since 1966 by which physician payment for Medicare services was
based on a “rural” versus “urban” classification. His bill resulted in a per-manent fix to underpayment to such “rural” locales with low cost of liv-ing as Monterey, Santa Cruz, and San Diego counties. This bill, which has been signed into law, corrects underpayment of up to 10%, which caused physicians in the affected counties to forgo up to $54 million per year. I was able to talk to Congressman Farr at a congratulatory event in his honor at Moss Landing in mid-May, organized by the California Medical Association, and I can say he is an advocate for our medical community.
Lastly, I would like to recognize my wife, Gina, without whom I could not do all that I do, and to recognize all of the other spouses of our mem-bers for the same.
Once again, I am deeply honored to be your president.
Jeffrey Keating, MD, is the 2014-2015 president of the Monterey County Medical Society. He is a pathologist and is currently practicing with Community Hospital of Monterey Peninsula in Monterey.

JULY/AUGUST 2014 | THE BULLETIN | 11
Legacy Wealth Advisors
Managing the reserve investment accounts of the Santa Clara
County Medical Association (SCCMA) and the Bureau of Medical Economics (BME) since 2000
1900 The Alameda Suite 510 San Jose, CA 95126
P: (408) 452-7700 F: (408) 452-7470 Email: [email protected]
www.lwallc.com
Wealth Management Legacy offers a broad range of wealth management services to SCCMA and MCMS physician members and their families. Such services include:
• Financial Planning, Risk Management, Educational & Retirement Planning Projections
• Liquidity Management and Cash Flow Analyses • Estate Tax and Charitable Planning • Existing Portfolio Analysis • Design and Implementation of Investment Strategies
Member Savings!
Legacy offers a one-hour complimentary financial planning check-up to Association members (this is a $500 savings). For more information, please call Lawrence Pizzella at (408) 452-7700 or email [email protected]
HONESTFAIR
ACCOUNTABLE
ACCURATECONSISTENT
KNOWLEDGEABLE
BILLING COLLECTIONS CONSULTING
Call (408) 998-5811 x 3034 • 1 (888) 543-7497Email [email protected] • www.bmesc.org
THE BUREAU OF MEDICAL ECONOMICS
Competitive pricing and superior service for your billing, collection, and consulting needs.
Committed to providing superior billing and collection services to physicians and other
professional providers of health services while upholding the professional integrity of those we
represent since 1947.
A rate of recovery over twice the national average.

12 | THE BULLETIN | JULY/AUGUST 2014
MESSAGE FROM THE CEO
Vote No on Prop. 46
WILLIAM PARRISH, MBACEO, Santa Clara County Medical Association &
Monterey County Medical Society
By William Parrish, CEOSanta Clara County Medical Association
Monterey County Medical SocietyOn November 4, 2014, voters will be asked to weigh in on the MICRA
(Medical Injury Compensation Reform Act) health care lawsuit measure, which will hugely jeopardize the privacy of patients’ personal prescription medical information.
The initiative will force doctors and pharmacists to use a massive statewide database known as the Controlled Substance Utilization Re-view Evaluation System (CURES), which is filled with patients’ personal prescription drug information. Though the database already exists, it is underfunded, understaffed, and technologically incapable of handling the massively increased demands that this ballot measure will place on it.
While many of you and your colleagues may find the general concept of the CURES database helpful, this ballot measure will force the program to respond to tens of millions of inquiries each year – something it simply isn’t set up to do in its current form or functionality. A system unequipped to handle these requirements will put physicians and pharmacists in the untenable position of having to break the law to treat their patients, or break their oath by refusing some patients much needed medications.
Most concerning, the massive ramp-up of this database will signifi-cantly put patients’ private medical information at risk and the ballot mea-sure doesn’t contain any provisions or funding to help upgrade the system or increase the database’s security standards.
As many of you know, the CURES database contains highly sensi-tive patient information including personal and potentially stigmatizing details about their health. Prescription information including medication used to treat obesity, narcolepsy, conditions related to cancer and AIDS, asthma, and other sensitive information are all contained within the CURES database. The ballot measure’s massive ramp-up of the CURES database comes with no funding for technological improvements and will lead to unintended problems.
SCCMA-MCMS and CMA have joined a campaign coalition to op-pose this initiative. In recent weeks and months, the coalition to oppose the MICRA health care lawsuit initiative continues to grow. Teachers, health care workers, local community groups, and hundreds of others have pledged to vote “NO” on Proposition 46, in November, because they, too, understand the implications this measure would have on patients, taxpayers, and consumers across the state.
We know that if this measure passes, it won’t just be putting patients’ personal medical information at risk, but malpractice lawsuits and pay-outs will also skyrocket, adding “hundreds of millions of dollars” in new costs to state and local governments, according to an impartial analysis
conducted by the state’s Legislative Analyst. State and local governments face higher costs in two ways:
• They provide health care for current and retired employees; • They provide health care for low income residents through Medi-
Cal and other locally run health care programs like community clinics and hospitals.
Someone will have to pay for these increased costs, and that someone is providers, taxpayers, and consumers.
The campaign opposed to the initiative – “Patients and Providers to Protect Access and Contain Health Costs” – is a diverse and growing coalition of trusted doctors, community health clinics, hospitals, family-planning organizations, local leaders, public safety officials, businesses, and working men and women formed to oppose this costly, dangerous ballot proposition that would make it easier and more profitable for law-yers to sue doctors and hospitals. A full and updated list of groups oppos-ing the campaign can be found at www.NoOn46.com.
SCCMA-MCMS is asking each of you to join the effort to oppose the costly MICRA health care lawsuit initiative. So how can you get engaged?
Have you signed up to be a hospital coordinator in your area? We’re always looking for informed and engaged physicians to help
educate about the dangers of this initiative. Visit CMA’s MICRA resource page, www.cmanet.org/micra, to sign up today.
Is your name on the growing list of individuals and groups opposed to the MICRA health care lawsuit initiative?
If not, add it today at www.NoOn46.com.
Need more information? Check out the campaign website, www.NoOn46.com, to learn more
about the impacts this ballot measure would have on health care and your patients.
United as one voice, advocating for patients across the state, we can defeat this ballot measure in November, but we need everyone to commit and become engaged along the way. Thank you in advance for all that you do and all that you’ll continue to do.

JULY/AUGUST 2014 | THE BULLETIN | 13
The Medical Injury Compensation Reform Act (MICRA) is California’s hard-fought law to provide for injured patients and stable medical liability rates. But this year California’s Trial Lawyers have launched an attack to
undermine MICRA and its protections and we need your help. Membership has never been so valuable!
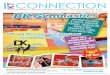
savings of over $86,000
wAys sCCMA/MCMs/CMA Is woRkIng foR you!
Are you a sCCMA/MCMs/CMA member?Physicians in santa Clara & Monterey Counties are saving an average of $86,818 this year.
2013 sCCMA/MCMs MICRA sAvIngs ChART
sCCMA/MCMs700 Empey way, san Jose, CA 95128sCCMA Phone: (408) 998-8850 fax: (408) 289-1064MCMs Phone: (831) 455-1008 fax: (408) 289-1064
* Medical Liability Monitor - Annual Rate Survey Issue, Vol. 38, No. 10, October 2013. Annual rates with limits of $1 million/$3 million.
general surgery Internal Medicine oB/gyn Average (non-Invasive)
santa Clara & Monterey Counties $22,286 $6,315 $29,188 $19,263 Connecticut $92,782 $34,700 $170,389 $99,290 District of Columbia $73,018 $24,010 $147,595 $81,541 new york $148,454 $35,883 $227,899 $137,412 CT-DC-ny Average $104,751 $31,531 $181,961 $106,081
MICRA Savings $82,465 $25,216 $152,773 $86,818

14 | THE BULLETIN | JULY/AUGUST 2014
The Monterey County Medical Society held its annual Awards Banquet and Installation Dinner on Thursday evening, June 5, 2014, at the Nicklaus Club Monterey.
Approximately 90 members and special guests attended, including Keynote Speaker Francisco Silva, Esq. (CMA) and Congressman Sam Farr, Assemblymembers Luis Alejo and Mark Stone, and County Supervisors Simón Salinas and Luis Calcagno.
Kelly O’Keefe, MD, 2013-2014 MCMS president, was hon-ored as the outgoing president, and Jeffrey Keating, MD, was welcomed as MCMS’s incoming president for 2014-2015. Serving in the current fiscal year with Dr. Keating are: James Hlavacek,
MD, as president-elect; Kelly O’Keefe, MD, as past president; Patricia Ruckle, MD, as secretary; and Steven Vetter, MD, as treasurer. The MCMS board of directors are Paul Anderson, MD; Val-erie Barnes, MD; Ron-ald Fuerstner, MD; Gary Gray, DO; Steven Har-rison, MD; David Holley, MD; John Jameson, MD; William Khieu, MD; El-iot Light, MD; Edward Moreno, MD; Marc Tun-zi, MD; Craig Walls, MD; and Cary Yeh, MD.
Award honoree Alex Di Stante, MD, received an award for “Physi-cian of the Year” for his extraordinary commitment to the community and his personal leadership in helping to bring Monterey County’s prospective trauma center to Natividad Medical Center. In honoring Dr. Di Stante, MCMS recognized his enthusiasm and vision. The center at Natividad will be the only Level II trauma center in the state that is fully staffed with trauma-trained surgeons.
Dr. Di Stante joined the medical staff at Natividad Medical Center in 2006. He is now the chief of surgery and trauma director. In addition, Dr. Di Stante started the bariatric surgery program, in 2011, as an alternative means of helping patients lose weight. He is also a former chief of staff at Natividad Medical Center. He received his medical degree from Ponce School of Medicine in Puerto Rico, his surgical residency was at the Poly-clinic in Harrisburg, Pennsylvania, and his fellowship in trauma/critical care was at University of California, Irvine. He is board certified in general surgery and a member of the American College of Surgeons.
The annual banquet was a great success and a lot of fun! MCMS mem-bers, their families, and special guests enjoyed a fantastic meal, camarade-rie, and a great program to wrap-up the evening.
MEMBER NEWS AND HAPPENINGS
MONTEREY COUNTY MEDICAL SOCIETY’S ANNUAL AWARDS BANQUET AND INSTALLATION DINNER
Dr. Alex Di Stante - Physician of the Year

JULY/AUGUST 2014 | THE BULLETIN | 15
1 Kelly O’Keefe, MD (2013-2014 President), celebrates his special
honor with his wife, Patricia.
2 Paul Anderson, MD (MCMS Director), and his wife enjoy the
wonderful dinner.
Monterey County Medical Society
2014 Annual Awards Banquet and Installation
June 5, 2014
1
2

1 James Hlavacek, MD (MCMS President-Elect), and Harry Weiss
(CEO, Natividad Medical Center).
2 Dr. James Hlavacek and Congressman Sam Farr.
3 Award honoree, Alex Di Stante, MD, delivers his acceptance
speech.
4 Dr. Keating and his wife, Gina, celebrate his special evening and
installation as new MCMS President.
16 | THE BULLETIN | JULY/AUGUST 2014
1
3
4
2

B R O N Z EB R O N Z E
S I LV E RS I LV E R
P L AT I N U MP L AT I N U M
G O L DG O L D
JULY/AUGUST 2014 | THE BULLETIN | 17

18 | THE BULLETIN | JULY/AUGUST 2014
MEMBER NEWS AND HAPPENINGS
Santa Clara County Medical Association Award Presentations and Installation
The Fairmont Hotel’s Club Regent, in San Jose, provided the setting this year for Santa Clara County Medical Association’s Annual Awards Banquet.
Sameer Awsare, MD, 2013-2014 SCCMA Presi-dent, following his outgoing president’s speech, pre-sented James Crotty, MD, with the presidential gavel for 2014-2015. Serving in the current fiscal year with Dr. Crotty are: Eleanor Martinez, MD, as President-Elect; Cindy Russell, MD, as Vice President of Community Health; Kenneth Blumenfeld, MD, as Vice President of External Affairs; Peter Cassini, MD, as Vice President of Member Services; Seema Sidhu, MD, as Vice Presi-dent of Professional Conduct; Sameer Awsare, MD, as Past President; Scott Benninghoven, MD, as Treasurer; and Seham El-Diwany, MD, as Secretary. The SCCMA Councilors are: Arthur Basham, MD (El Camino Hos-pital Los Gatos); Laura Cook, MD (El Camino Hospi-tal); David Feldman, MD (Good Samaritan Hospital); Hemali Sudhalkar, MD (Kaiser Foundation Hospital – San Jose); Anh Nguyen, MD (Kaiser Permanente Hos-pital Santa Clara); Michael Charney, MD (O’Connor Hospital); Erica Timiraos, MD (Regional Medical Cen-ter); Diane Sanchez, MD (Saint Louise Regional Hospi-tal); Vanila Singh, MD (Stanford Hospital & Clinics); and Richard Kramer, MD (Santa Clara Valley Medical Center).

JULY/AUGUST 2014 | THE BULLETIN | 19
The evening’s festivities culminated with the recognition of those who have dedicated their lives to furthering the high quality of medical care.
Dr. Crotty made the following presentations:
LISA KRIEGERSPECIAL RECOGNITION AWARD
This award is given in recognition and appreciation for many years of dedication and service to the physicians of Santa Clara County, their pa-tients, and our community.
Lisa Krieger received her BA in Biology at Duke University in 1977. She then worked for three years at The Coastland Times, Manteo, N.C., as a general reporter and photographer. She worked for Reporter, Medical World News, and JAMA in Washington, D.C., and then moved to San Francisco to work for the San Francisco Examiner in 1986. She reported on public health issues for 12 years. She came to the San Jose Mercury News in 1998 and has reported on science, higher education, and medicine.
Ms. Krieger is author of the award-winning series “The Cost of Dy-ing,” that sought to shed light on topics of ICU care, palliative care, ad-vance directives, and caregiving at the end of life. She is also a contribu-tor to Bay Nature magazine. Lisa has been actively participating in public forums discussing end-of-life care and palliative care. Her efforts to bring this issue to the fore and help stimulate public discussion have contributed to the improvement of health care to thousands of patients. So tonight, in acknowledgment and appreciation of her invaluable contributions, the Santa Clara County Medical Association wishes to honor Lisa Krieger with its Special Recognition Award.
GAY CRAWFORDCITIZEN’S AWARD
With the Citizen’s Award, the Medical Association recog-nizes a non-member who has achieved public recognition for
a significant contribution in the health field. Tonight, we recognize Gay Crawford for this award.
Gay Crawford has spent almost 40 years in the cancer field. There are few people who have affected the landscape of Santa Clara County health more than Gay, who has been involved at the local, state, and national levels, fighting for better cancer care, research, advo-cacy, and services since 1974.
Gay is the past president and a founder of Cancer CAREpoint, helping design a patient service program for cancer patients in Silicon Valley. She is a founder of Hospice of the Valley, the founder of Courageous Kids – an American Cancer Society program for children with cancer, cofounder for the Colon Cancer-Free Zone, a founder and first president of the California Cancer In-
cidence Registry, and an honorary life member of the American Cancer Soci-ety. She served as a reviewer on the national research program of the American Cancer Society, where more than $100 million is distributed nation-ally. She has numer-ous awards to her credit, including the American Can-cer Society’s high-est volunteer honor, the St. George Medal, and a Life-time Achievement Award. Gay’s con-tributions are not merely significant, they are truly life changing. It is, therefore, a great honor to present the Santa Clara County Medical As-sociation’s Citizen’s Award to Ms. Gay Crawford.
Continued on page 20

20 | THE BULLETIN | JULY/AUGUST 2014
MARTIN FISHMAN, MDBENJAMIN J. CORY, MD AWARD
This award is given to a phy-sician member of the Asso-ciation who has displayed forward-look-ing, pioneer-ing ideas, e n t e r p r i s e ,
enthu sia sm , and prolonged
professional stature and ability.
Dr. Martin Fishman was raised in California, and
finished his pre-medical studies at the University of California, Berkeley, graduating cum laude in Medical Sciences. He has a Masters Degree in Public Administration in Health Care. He graduated in the top 10% of his medical school class at the University of Califor-nia, San Francisco Medical Center, and fin-ished a medical internship at Harbor Gen-eral Hospital in Torrance, California. He completed a residency in ophthalmology at Washington University Medical Center in St. Louis, Missouri. He then spent two years at the National Institute of Health in Bethesda, Maryland, as a Clinical Fellow at the National Eye Institute, where he performed clinical and laboratory research.
Since beginning practice in Los Gatos in 1976, Dr. Fishman has served in a teaching position at Stanford University. He is now an adjunct clinical professor of Oph-thalmology there, Director of the Pa-thology Section of the Stanford Basic Science Course in Ophthalmology, and has been recognized as an Outstanding Clinical Faculty Teacher.
Dr. Fishman has been active in many
leadership roles, and has served as chief of the medical staff at Community Hospital of Los Gatos, president of the California Association of Ophthal-mology, and, of course, president of our own Santa Clara County Medical Association. He is currently in his ninth year as a trustee of the California Medical Association. His other leadership positions with the Santa Clara County Medical Association include president elect and vice president for External Affairs. He has also been a strong advocate in keeping MICRA intact.
Dr. Fishman joined the Board of Trustees of The Health Trust in 2005, and has been addressing approaches to community health. The Health Trust is responsible for AIDS services, Meals on Wheels, senior programs, community resource centers, a wonderful set of dental clinics for children with Medicaid whose dental care was previously neglected, the drive to fluoridate our water, community gardens in schools and parks, green carts for underserved neighborhoods, and many other programs designed to bring the promise of good health for everyone.
Dr. Fishman also has developed an interest in health care in under-served indigenous populations. He has volunteered, since 2005, for an ongoing program to bring medical and surgical eye care to a population in Guatemala. They have provided care for over 5,000 patients and per-formed over 1,000 operations, primarily cataract surgeries, usually in pa-tients who were blind and had to be led in to the center by their families. He especially enjoys the opportunity to teach the Guatemalan ophthal-mology residents, and to bring Stanford residents on the trips, which will hopefully motivate them to give back to others.
It is a pleasure and a privilege for us all to have Dr. Fishman in our county…and
a distinct honor to present this distin-guished award to Dr. Martin Fishman — our 2014 Benjamin J. Cory, MD Award recipient.
GARY HARTMAN, MDOUTSTANDING
ACHIEVEMENT IN MEDICINE AWARD
The Outstanding Achievement in Medicine Award is given to a physi-cian who, during his/her medical career, has made unique contributions to
the betterment of patient care, for which he/she has
achieved widespread recogni-tion. It is, in a sense, bestowed
SCCMA Award Presentations and Installation, from page 19

JULY/AUGUST 2014 | THE BULLETIN | 21
upon a physician’s physician. Dr. Gary Hartman has his BA in Psychology from Uni-
versity of Wisconsin, and completed his Doctor of Medicine there in 1974. He came to California and completed a Gener-al Surgery residency at Highland General Hospital in 1980. He went on to complete a Pediatric Surgery fellowship at Stanford and further training at the University of Oklahoma. He was vice president of Medical Staff at Lucile Packard Children’s Hospital from 2006-2007, and president of the Medical Staff from 2007-2010. He is currently Division Chief, Pediatric Surgery, Stanford Univer-sity School of Medicine.
Dr. Hartman has published extensively on subjects ranging from pediatric lung trans-plantation to esophageal atresia. His world-famous achievements in separating Siamese twins have been nothing short of spectacular and have brought deserving admiration for his team and Stanford University. The TV coverage was mesmerizing of the wonderful outcome he had for two twins joined at the chest and abdomen, several years ago.
Additionally, Dr Hartman’s legacy is increased yearly by virtue of the many residents and fellows he teaches at Stanford. He is an active sup-porter of our community and provides valuable pediatric surgical cover-age for hospitals in our area, including Good Samaritan. Therefore, it is with great esteem and admiration that we, the Santa Clara County Medi-cal Association, award Dr. Gary Hartman the Outstanding Achievement in Medicine.
JONATHAN BLUM, MDOUTSTANDING CONTRIBUTION IN MEDICAL EDUCATION
This award is given to a physician member of the Association who has exhibited sustained interest and participation in one or more medical edu-cation activities over and above that expected of the membership at-large.
Dr. Blum grew up in New Jersey and did his undergraduate education at Yale University. He completed his Doctorate in Medicine at University of California, San Francisco. He traveled to Beth Israel for internship and residency, followed by fellowship in Infectious Disease at Harvard Medi-cal School in 1996. He did research and teaching at Harvard, and then joined The Permanente Medical Group in 2002. He has been active teach-ing residents and medical students since then, and has received numer-ous teaching awards. He has written papers on immunology, infectious disease, and bacterial genetics, and formerly edited the antibiotic section of the Tarascon Pocket Pharmacopoeia. He is a member of the Infectious Diseases Society of America, the American Society for Microbiology, and
the American Association for the Advancement of Science.
What sets Dr. Blum apart from the herd is his possession
of incredible insight and knowledge, which he is able to tailor to his audience, target-ing them with unerring accu-racy and never failing to deliver the right mes-sage. He engag-es his audience, whether an in-
dividual, a class-room, or a com-munity of Bay Area local news-cast viewers, with his razor-sharp
wit, holding their interest through what can be some rather dry subject matter. For example, to reinforce his hand hygiene message to other physi-cians, Dr. Blum has worn a “sandwich board” sign on his back emblazoned with: “Warning: I Make Frequent Stops to Gel.” His lectures to physician colleagues are always engrossing and full of memorable clinical pearls.
Dr. Blum has influenced and educated a community of physicians. He is passionate about learning, about teaching, about discovering new and better ways of taking care of and preserving the health of patients. He is without peer in the selflessness, generosity, brilliance, and wit with which he shares his abundant knowledge, and thus, it is with great admiration and pleasure that we award Dr. Blum with Santa Clara County Medical Association’s award for Outstanding Contribution in Medical Education.
DAVID CAMPEN, MD OUTSTANDING CONTRIBUTION TO THE MEDICAL ASSOCIATION
This award is given to a physician member of the Association who has exhibited sustained interest and participation in one or more activities of the Association over and beyond that expected of the membership at-large.
David Campen, MD, grew up in San Jose and went from Lincoln High School to University of California, Berkeley, receiving a BA in Physi-ology in 1979. He then went to Tulane Medical Center in New Orleans, completing his MD in 1983. Following this, he completed his residency in Internal Medicine and fellowship in Rheumatology at Los Angeles County University of Southern California Medical Center. He joined The Perma-
Continued on page 22

22 | THE BULLETIN | JULY/AUGUST 2014
nente Medical Group in 1989. He has been active in administrative duties, acting as medical director of the Pharmaceutical Operations Division of the Northern California Kaiser Permanente Medical Program.
David Campen, MD, has been an SCCMA and CMA member since 1989. His support for SCCMA and CMA is greatly admired and appreci-ated. He has served on SCCMA’s Nominating, Membership, and Hospital Chiefs of Staff Committees. His SCCMA positions have included Council-or from 1993 to 1996, and he has been a CMA Delegate from 1997 to 2014.
Dr. Campen’s contributions have been significant to our associa-tion and the CMA. We want to recognize his time, input, and service by awarding him the Outstanding Contribution to the Medical Association Award.
KEITH FABISIAK, MDOUTSTANDING CONTRIBUTION IN COMMUNITY SERVICE
This award is given to a physician member of the Association who has exhibited sustained interest and participation in one or more activi-ties of the community over and above that expected of the membership at-large.
Dr. Keith Fabisiak grew up in central Wisconsin. He attended Marquette University in Milwaukee, Wisconsin, and graduated mag-na cum laude with a BS degree in Biology. He received his Medical De-gree from the Medical College of Wisconsin in 1987, and went on to the
University of Michigan to complete both an internship and residency in the Department of Pediatrics. He joined The Permanente Medical Group in 1991.
Since 2009, Dr. Fabisiak has been working with a non-profit organi-zation in Sunnyvale called Full Circle Farms, a functioning educational
farm in the heart of Silicon Valley. This program is a project of Sus-tainable Community Gardens (SCG), a community-based 501(c)
(3) nonprofit corporation dedicated to the renewal of local, sustainable food systems. As a board member, he has been able to participate in the organizational structure of Full Circle Farms and help with development of their curriculum for students, vision for the future, and programs that help with combating the current epidemic of childhood obesity. Dr. Fabisiak has also been influential in the development of
Kaiser Permanente’s childhood obesity programs, as well as a key contributor to the Kaiser Permanente “Live Well, Be Well”
campaign, which has encouraged Kaiser’s 70,000 employees in 23 medical centers across northern California to adopt healthy habits in nutrition and exercise. His service to our community is both laudable and inspirational. Thus, the Santa Clara County Medical Association, with deep admiration and boundless re-spect, presents the Outstanding Contribution in Community Ser-vice Award to Dr. Keith Fabisiak.
SCCMA Award Presentations and Installation, from page 21
O u r s p e c i a l t h a n k s t o t h e f o l l o w i n g s p o n s o r sf o r c o n t r i b u t i n g t o t h e s u c c e s s o f t h i s e v e n t :
Lisa KriegerSpecial Recognition Award
Gay CrawfordCitizen’s Award
Keith A. Fabisiak, MDOutstanding Contribution
in Community Service
David H. Campen, MDOutstanding Contribution
to the Medical Association
Jonathan H. Blum, MDOutstanding Contribution
in Medical Education
Gary E. Hartman, MDOutstanding Achievement
in Medicine
Martin L. Fishman, MDBenjamin J. Cory,
MD Award
Law Offices of
BRONZE LEVEL SPONSORS
GOLD LEVEL SPONSOR
SILVER LEVEL SPONSORS
PLATINUM LEVEL SPONSOR
James R. Crotty, MD, MBASCCMA President-Elect
Sameer V. Awsare, MD, FACPSCCMA President
2014
2014
~ Honoring ~
~ Award Honorees ~
Tuesday, June 17, 2014 • 6:15 pmThe Fairmont Hotel, San Jose
T H A N K Y O U ! S C C M A’s AWA R D S B A N Q U E T

JULY/AUGUST 2014 | THE BULLETIN | 23
O u r s p e c i a l t h a n k s t o t h e f o l l o w i n g s p o n s o r sf o r c o n t r i b u t i n g t o t h e s u c c e s s o f t h i s e v e n t :
Lisa KriegerSpecial Recognition Award
Gay CrawfordCitizen’s Award
Keith A. Fabisiak, MDOutstanding Contribution
in Community Service
David H. Campen, MDOutstanding Contribution
to the Medical Association
Jonathan H. Blum, MDOutstanding Contribution
in Medical Education
Gary E. Hartman, MDOutstanding Achievement
in Medicine
Martin L. Fishman, MDBenjamin J. Cory,
MD Award
Law Offices of
BRONZE LEVEL SPONSORS
GOLD LEVEL SPONSOR
SILVER LEVEL SPONSORS
PLATINUM LEVEL SPONSOR
James R. Crotty, MD, MBASCCMA President-Elect
Sameer V. Awsare, MD, FACPSCCMA President
2014
2014
~ Honoring ~
~ Award Honorees ~
Tuesday, June 17, 2014 • 6:15 pmThe Fairmont Hotel, San Jose
T H A N K Y O U ! S C C M A’s AWA R D S B A N Q U E T

690 Saratoga Ave | Suite 200 | San Jose, CA 95129 (408) 217-6000 T | (408) 457-8803 F | Lic. 01902032 | www.healthmedrealty.com
1,974 SF AVAILABLE 900 SF AVAILABLE 1,160-1,480 SF AVAILABLE 1,320 SF AVAILABLE
14911 National Ave, Campbell 3425 S. Bascom Ave, Campbell 10430 S. De Anza Blvd, Cupertino 881 Fremont Ave, Los Altos
2nd floor suite with new interiors. Elevator, ADA restroom. Close to Good Samaritan Hospital & Mission Oaks Hospital. TI’s available.
Excellent corridor for medical/dental or office. Elevator, on-site parking and newly renovated restrooms. Close to Hwys 17 & 85.
Medical & plumbed (dental) suites available in 2-story building. Close to Civic Center, City Hall, Apple HQ. Easy access to Hwy 280.
Ground floor space in a 2-story building available. Located in close proximity to the Loyola Corners District of Los Altos.
1,175-9,546 SF AVAILABLE 3,318 SF AVAILABLE BUILT TO SUIT OPPORTUNITY 2,600-8,452 SF AVAILABLE
14830 Los Gatos Blvd, Los Gatos 825 Pollard Rd, Los Gatos 14910 Los Gatos Blvd, Los Gatos 2930 Aborn Square Rd, San Jose
Brand new medical office building. Built with the highest quality materials and finishes. TI’s available. Adjacent to Good Samaritan Hospital.
Great medical building, steps away from El Camino Hospital. Ground floor unit, TI dollars available.
Parcel: 21,400 SF. This is BTS opportunity. Call for more info. Please do not disturb tenant.
Neighborhood shopping center with wide array of retail tenants with Ross Dress For Less anchor.
1,050 SF AVAILABLE 4,336 SF AVAILABLE 600 SF AVAILABLE 2,090 SF AVAILABLE
743 S. Winchester, San Jose 521 Parrott Street, San Jose 10601 S. De Anza Blvd, San Jose 189 N. Bascom Ave, San Jose
Medical office available in newer medical/retail center near Santana Row & freeways. New building, must see! TI’s available.
Excellent for medical/dental or pro-fessional offices. On-site parking. Great steet frontage. Ample power. Turn-key TI’s available.
Medical space facing S. De Anza Blvd. Close to Apple HQ and down-town Cupertino. Great access to Hwys 85 & 280.
Fully plumbed dental suite available for lease. Easy access to Hwys 280 & 880. Space is divisible.
710-1,557 SF AVAILABLE 645-2,511 SF AVAILABLE 980-1,305 SF AVAILABLE 725-2,680 SF AVAILABLE
5150 Graves Ave, San Jose 393 Blossom Hill Rd, San Jose 4155 Moorpark Ave, San Jose 2242 Camden Ave, San Jose
Located in the West Valley Professional Center. Small suite availble NOW. Single-story building.
Modern Class A medical building. Easy access to 85 and 101, and great promotional rate!
Great medical/dental location at Saratoga & Moorpark Ave. Con-venient freeway access, excellent price!
BRAND NEW exteriors, lobby & full ADA upgrades! Located close to Willow Glen, Cambrian & Los Gatos. Easy access to Hwys 880 & 17.
2,136 SF FOR LEASE OR SALE 5,060 SF FOR SALE 5,872 SF FOR SALE 3,128 SF FOR LEASE OR SALE
15055 Los Gatos Blvd, Los Gatos 3229 S. Bascom, San Jose 200 N. Bascom Ave, San Jose 20465 Saratoga Los Gatos Rd, Saratoga
Medical, dental, or retail uses allowed. Great Los Gatos Blvd location. Easy freeway access to Hwys 85 & 17.
Price: $1,589,000. Great corner location near Good Samaritan Hospital. Zoned Pedestrian Commercial. Financing available.
Freestanding medical/retail building in shell condition. Great visibility and freeway access.
Unique owner-user opportunity in the heart of downtown Saratoga. Multi-tenant professional building.
5,000 SF AVAILABLE 1,806-1,927 SF AVAILABLE 1,080 SF AVAILABLE 1,557-4,332 SF AVAILABLE
123 Di Salvo Ave, San Jose 2081 Forest Ave, San Jose 2011 Forest Ave, San Jose 877 W. Fremont Ave, Sunnyvale
California Mission style building. Space is divisible. Waking distance from O’Connor Hospital. Great access to Hwys 280 & 880.
Medical office building with established tenants located directly adjacent to O’Connor Hospital. Flexible terms.
Medical dental suite available. Close to O’Connor Hospital. Great freeway access. Available NOW. TI’s available.
Foothill Medical-Dental Center is a 6 plus acre medical project in the heart of Sunnyvale. Various medical & plumbed (dental) suites available.
HealthMed Realty is a Full-Service Commercial Real Estate Firm specializing in Medical & Dental Real Estate. Put our experience on your side and we will save you time and money.
Call us today! (408) 217-6000
scan me to see our latest availabilities
Do you have an office EMERGENCY?
(408) 217-6000

690 Saratoga Ave | Suite 200 | San Jose, CA 95129 (408) 217-6000 T | (408) 457-8803 F | Lic. 01902032 | www.healthmedrealty.com
1,974 SF AVAILABLE 900 SF AVAILABLE 1,160-1,480 SF AVAILABLE 1,320 SF AVAILABLE
14911 National Ave, Campbell 3425 S. Bascom Ave, Campbell 10430 S. De Anza Blvd, Cupertino 881 Fremont Ave, Los Altos
2nd floor suite with new interiors. Elevator, ADA restroom. Close to Good Samaritan Hospital & Mission Oaks Hospital. TI’s available.
Excellent corridor for medical/dental or office. Elevator, on-site parking and newly renovated restrooms. Close to Hwys 17 & 85.
Medical & plumbed (dental) suites available in 2-story building. Close to Civic Center, City Hall, Apple HQ. Easy access to Hwy 280.
Ground floor space in a 2-story building available. Located in close proximity to the Loyola Corners District of Los Altos.
1,175-9,546 SF AVAILABLE 3,318 SF AVAILABLE BUILT TO SUIT OPPORTUNITY 2,600-8,452 SF AVAILABLE
14830 Los Gatos Blvd, Los Gatos 825 Pollard Rd, Los Gatos 14910 Los Gatos Blvd, Los Gatos 2930 Aborn Square Rd, San Jose
Brand new medical office building. Built with the highest quality materials and finishes. TI’s available. Adjacent to Good Samaritan Hospital.
Great medical building, steps away from El Camino Hospital. Ground floor unit, TI dollars available.
Parcel: 21,400 SF. This is BTS opportunity. Call for more info. Please do not disturb tenant.
Neighborhood shopping center with wide array of retail tenants with Ross Dress For Less anchor.
1,050 SF AVAILABLE 4,336 SF AVAILABLE 600 SF AVAILABLE 2,090 SF AVAILABLE
743 S. Winchester, San Jose 521 Parrott Street, San Jose 10601 S. De Anza Blvd, San Jose 189 N. Bascom Ave, San Jose
Medical office available in newer medical/retail center near Santana Row & freeways. New building, must see! TI’s available.
Excellent for medical/dental or pro-fessional offices. On-site parking. Great steet frontage. Ample power. Turn-key TI’s available.
Medical space facing S. De Anza Blvd. Close to Apple HQ and down-town Cupertino. Great access to Hwys 85 & 280.
Fully plumbed dental suite available for lease. Easy access to Hwys 280 & 880. Space is divisible.
710-1,557 SF AVAILABLE 645-2,511 SF AVAILABLE 980-1,305 SF AVAILABLE 725-2,680 SF AVAILABLE
5150 Graves Ave, San Jose 393 Blossom Hill Rd, San Jose 4155 Moorpark Ave, San Jose 2242 Camden Ave, San Jose
Located in the West Valley Professional Center. Small suite availble NOW. Single-story building.
Modern Class A medical building. Easy access to 85 and 101, and great promotional rate!
Great medical/dental location at Saratoga & Moorpark Ave. Con-venient freeway access, excellent price!
BRAND NEW exteriors, lobby & full ADA upgrades! Located close to Willow Glen, Cambrian & Los Gatos. Easy access to Hwys 880 & 17.
2,136 SF FOR LEASE OR SALE 5,060 SF FOR SALE 5,872 SF FOR SALE 3,128 SF FOR LEASE OR SALE
15055 Los Gatos Blvd, Los Gatos 3229 S. Bascom, San Jose 200 N. Bascom Ave, San Jose 20465 Saratoga Los Gatos Rd, Saratoga
Medical, dental, or retail uses allowed. Great Los Gatos Blvd location. Easy freeway access to Hwys 85 & 17.
Price: $1,589,000. Great corner location near Good Samaritan Hospital. Zoned Pedestrian Commercial. Financing available.
Freestanding medical/retail building in shell condition. Great visibility and freeway access.
Unique owner-user opportunity in the heart of downtown Saratoga. Multi-tenant professional building.
5,000 SF AVAILABLE 1,806-1,927 SF AVAILABLE 1,080 SF AVAILABLE 1,557-4,332 SF AVAILABLE
123 Di Salvo Ave, San Jose 2081 Forest Ave, San Jose 2011 Forest Ave, San Jose 877 W. Fremont Ave, Sunnyvale
California Mission style building. Space is divisible. Waking distance from O’Connor Hospital. Great access to Hwys 280 & 880.
Medical office building with established tenants located directly adjacent to O’Connor Hospital. Flexible terms.
Medical dental suite available. Close to O’Connor Hospital. Great freeway access. Available NOW. TI’s available.
Foothill Medical-Dental Center is a 6 plus acre medical project in the heart of Sunnyvale. Various medical & plumbed (dental) suites available.
HealthMed Realty is a Full-Service Commercial Real Estate Firm specializing in Medical & Dental Real Estate. Put our experience on your side and we will save you time and money.
Call us today! (408) 217-6000
scan me to see our latest availabilities
Do you have an office EMERGENCY?
(408) 217-6000

1 Award Honoree and Past President Martin Fishman, MD, celebrates
his honor with his wife, Barbara, and family/friends.
2 James Crotty, MD, accepts the gavel as SCCMA’s 2014-2015
President.
3 SCCMA’s 2013-2014 President Sameer Awsare, MD, poses with
family.
1
32
26 | THE BULLETIN | JULY/AUGUST 2014

Congratulations to all Award Honorees this year!
Awardees included (left to right) Lisa Krieger (Special Recognition Award); Gary Hartman, MD (Outstanding Achievement in Medicine); David Campen, MD (Outstanding Contribu-tion to the Medical Association); Keith Fabisiak, MD (Outstanding Contribution in Commu-nity Service); Martin Fishman, MD (Benjamin J. Cory, MD Award); Gay Crawford (Citizen’s Award); Jonathan Blum, MD (Outstanding Contribution in Medical Education); and Sameer Awsare, MD (2013-2014 President).
JULY/AUGUST 2014 | THE BULLETIN | 27

1 L to R: Jason Bowman, William Lewis, MD (Past President), Helen
Wang, RN, Sandhya Yadav, MD, Keith Fabisiak, MD (Award Honoree), Eleanor Martinez, MD (President-Elect), and Robert Burnett, MD (Past President).
2 (Head table) L to R: Sameer Awsare, MD (President 2013-2014),
Prayoon Hwanglaa, William Parrish (CEO), James Crotty, MD (President 2014-2015) and his wife, Jenny. Bottom: Saleel Awsare, Dr. Swati Awsare, and Lisa Krieger (Award Honoree).
3A special thank you to Kaiser Permanente for their Platinum
level sponsorship of the Awards Banquet.
4 Award Honoree and Past President Martin Fishman, MD, celebrates
his honor with his wife, Barbara, and family/friends.
5 SCCMA’s incoming President James Crotty, MD, celebrates his
installation and special evening with his family.
6Peter Nosé, MD, poses with Award Honoree Gay Crawford and her
husband, Roy Crawford.
7 Keith Fabisiak, MD (Award Honoree), and his partner, Jason
Bowman.
8 SCCMA-BME staff (& spouses): Maureen Yrigoyen, Shannon
Landers, Mark Christiansen, Pam Jensen and husband Marty, Gary and Jean Cassetta, and Molly Meyers.
9 L to R: Stephen Henry, MD (Past President), James Hinsdale,
MD (Past President), and his wife, Bonnie, and Award Honoree Gary Hartman, MD, and his wife, Susan.
10 Cindy Russell, MD (VP-Community Health), Sandhya
Yadav, MD, and William Lewis, MD (Past President).
1
4
8
28 | THE BULLETIN | JULY/AUGUST 2014

2 3
765
9 10
JULY/AUGUST 2014 | THE BULLETIN | 29

1Award Honoree David Campen, MD poses with his family, Christine
Chang, MD, and Nicholas Campen.
2Award Honoree Jonathan Blum, MD, and his wife, Sheryl Sun, MD.
3L to R: Scott Benninghoven, MD (SCCMA Treasurer), Paul
Beaupre, MD (CEO, Good Samaritan Hospital), Ellen Blumenfeld, Kenneth Blumenfeld, MD (VP-External Affairs), Bruce Wilbur, MD, David Feldman, MD (SCCMA Councilor), and Richard O’Regan (Mercer). Thank you to our sponsors!
4L to R: Gay Crawford (Award Honoree), Roy Crawford, Rob
Tufel, Peter Nosé, MD, Robert Mastman, MD, Nancy Mastman, Gina Grossman, and Joel Wilhelm.
5Award Honorees Jonathan Blum, MD, and David Campen, MD,
celebrate their special evening with family and friends.
6A special thank you to Kaiser Permanente for their Platinum
level sponsorship of the Awards Banquet.
7Thank you to our guests from Santa Clara Valley Medical Center
for their Silver level sponsorship!
8L to R: David Adamson, MD, Leslie Kramer, Philip Stillman,
MD, Steve Jackson, MD (Past President). Bottom: Dr. Lynne Bui, Donna Spagna, Siggie Stillman, and Suzanne Jackson (SCCMA Alliance Foundation President).
9Pam Lindeman, Dawn Bussey, Rob Tufel, Gay Crawford (Award
Honoree), and Keith Fabisiak, MD (Award Honoree).
10Special guests of SCCMA: Donald Waters (ACCMA CEO) and his
wife, Linda, and Ron Wyatt, MD (ACCMA President), and his wife, Janelle.
1 2
5
8
30 | THE BULLETIN | JULY/AUGUST 2014

3 4
7
10
6
9
JULY/AUGUST 2014 | THE BULLETIN | 31

SCCMA Equals Extraordinary LeadershipSCCMA Past Presidents, President, and CEO pose for a memorable photo at the 2014 Awards Banquet.
Left to Right: CEO William Parrish; SCCMA Past Presidents John Longwell, MD, Stephen Henry, MD, Steve Jackson, MD, James Hinsdale, MD (also CMA Past President); Sameer Awsare, MD (outgoing president); Past Presidents Robert Burnett, MD (also CMA Past President), Martin Fishman, MD (also an award honoree), Thomas Dailey, MD; James Crotty, MD (incoming president); and Past President William Lewis, MD.32 | THE BULLETIN | JULY/AUGUST 2014

SCCMA Equals Extraordinary LeadershipSCCMA Past Presidents, President, and CEO pose for a memorable photo at the 2014 Awards Banquet.
Left to Right: CEO William Parrish; SCCMA Past Presidents John Longwell, MD, Stephen Henry, MD, Steve Jackson, MD, James Hinsdale, MD (also CMA Past President); Sameer Awsare, MD (outgoing president); Past Presidents Robert Burnett, MD (also CMA Past President), Martin Fishman, MD (also an award honoree), Thomas Dailey, MD; James Crotty, MD (incoming president); and Past President William Lewis, MD.
JULY/AUGUST 2014 | THE BULLETIN | 33

34 | THE BULLETIN | JULY/AUGUST 2014
MEMBER BENEFITS
You Create a Brighter Future. We Work to Protect It.
Let us help find the right Long-Term Care insurance plan for you, so you can spend time on things that matter the most.
People are living longer these days, but as life expectancies increase, so does the risk of serious health problems that could require long-term care. In fact, at retirement age, 70% of Americans will need long-term care and 35% will enter a nursing home.1 And with the average cost for nursing home care in a private room equating to more than $87,600 per year, that could literally cost most or all of your life’s savings.2
Long-Term Care insurance may not be for everyone. But with soaring health care costs, insurance restrictions, and the need to stretch retire-ment savings through more years... it’s a good idea to seriously consider this valuable coverage while receiving a member premium discount.
Santa Clara County Medical Association/Monterey County Medical Society, Mercer, and Long-Term Care Resources work together to pro-
vide members with a comprehensive long-term care program that gives physicians the stability and flexibility they need to protect their future. Members also have access to an interactive and educational Long-Term Care evaluation tool to help them make the best decisions for their specific situation.
To learn more about how members can help protect their assets from the rising cost of long-term care, call 800/616-8759, or visit www.myltc-plan.com/scmcma.
1. Department of Health and Human Services, www.longtermcare.gov/the-basics/how-much-care-will-you-need/, viewed April 1, 2014.
2. Genworth 2013 Cost of Care Survey, March 2013, https://www.genworth.com/corporate/about- genworth/industry-expertise/cost-of-care.html
Employment Practices Liability Insurance (EPLI)Many members think they have coverage for wrongful termination,
harassment, and discrimination claims by employees or patients (third party). However, most policies exclude coverage for these types of actions or only provide limited coverage (a contribution to defense costs).
The SCCMA/MCMS-sponsored Employment Practices Liability pro-gram includes a unique blend of risk management services and insurance specifically designed to assist physician groups in addressing these impor-tant employment issues. Among the features of the program are:
• Special First-Time Buyers program.• A Helpline staffed by experienced employment defense attorneys.
Any manager, officer, or principal of your practice has access to the Helpline for obtaining advice on handling workplace issues, including internal sexual harassment complaints, discipline, and employee terminations.
• If a member seeks Helpline advice on an employee termination, which later results in a claim, there is a 50% reduction of the
member’s EPLI deductible for that claim.• Free, comprehensive criminal background checks for newly
hired and promoted managers/supervisors.• EEO compliance training for managers/supervisors. An internet-
based training program, compliant with California law, provides supervisors with sexual harassment training.
• Wage and Hour Defense Coverage. (Subject to additional premium.)
This valuable member program is available to members through Mer-cer Health & Benefits Insurance Services LLC, our sponsored insurance program administrator, and in conjunction with the Employment Prac-tices Risk Management Association (EPRMA).
For more information on these important benefits, please contact Mercer at 800/842-3761 or email [email protected].
You Work to Protect Your Patients…We Work to Protect You.
As a physician, you probably know better than anyone else how quickly a disability can strike and not only delay your dreams, but also leave you unable to provide for your family. Whether it is a heart attack, stroke, car accident, or fall off a ladder, any of these things can affect your ability to perform your medical specialty.
That’s why the Association/Society sponsors a Group Long-Term Dis-ability program underwritten by New York Life Insurance Company:
• Benefits not tied to a practice, giving you more flexibility with potential career changes
• Benefit payments that are 100% TAX-FREE — when you pay premiums yourself
• High monthly benefits up to $10,000• Protection in your medical specialty for the first 10 years of
disabilityWith this critical protection, you’ll have one less thing to worry about
until your return.Learn more about this valuable plan today! Call Mercer for free infor-
mation, including features, costs, eligibility, renewability, limitations, and exclusions at 800/842-3761.

JULY/AUGUST 2014 | THE BULLETIN | 35
The SCCMA ALLIANCE Foundation Is Off and Running
By Suzanne Jackson, RN, MAPresident, SCCMA Alliance Foundation
The county Alliance has been busy this year providing assistance to local health care entities, as well as awarding two SCCMA Alliance Foun-dation grants to local health care charities. Importantly, your Alliance has received the final determination letter from the Internal Revenue Service (IRS), which means that we now are a functioning 501(c)(3) charitable foundation. As a result, all of your county dues are now fully tax deduct-ible. This will allow the Alliance to aggressively solicit funding in order to provide grants to our county health care related partners, as well as to provide scholarships to students pursuing a career in the medical and health care fields.
Our first official grant was awarded in December 2013 to Preven-tion Partnership International (PPI). The grant of $1,500 helped provide the cost of supplies needed in the development of the Birth-3 Component for Celebrating Families. This program addresses one of the most signifi-cant problems of our time: the deleterious effects of drug and alcohol ad-diction, and their related child abuse, family violence, and mental health problems. The program has proven to increase recovery rates from addic-tion and shortened the time to reunite families affected by addiction, while also reducing child abuse and family violence.
The population of parents with 0-3-year-old infants is increasing in the court system; consequently, the courts have requested expansion of this successful program. Primary beneficiaries will be young children (ages 0-3 years) living in situations at high risk for abuse/neglect and alco-hol/drug use leading to aversive childhood experience and toxic stress. It is anticipated that the lives of up to 35 children in Santa Clara County will be touched by this curriculum in 2013-2014. As the curriculum contin-ues to be implemented, and the number of implementation sites increases, more children will be impacted each year. Please check out their website
for more information: http://www.celebratingfamilies.net/CFmodel.htm.In March 2014, a second grant of $500 was provided to Cancer
CAREpoint for set-up costs of a new Wig Bank Program. The supplies were used to purchase Styrofoam heads, wig caps, headgear, mirrors, and other items nec-essary for the o r g a n i z a t i o n and storage of wigs, meeting the needs of women in treatment for cancer in the South Bay Community. This program will be continuing the invaluable support begun by the Alliance almost four years ago in this service to our community. Alliance members have been instrumental in the initial washing of gently-used donated wigs over three years ago. In 2013, the Alliance funded a large wall-to-wall mirror installation at the newly re-modeled Wig Bank in Campbell. Alliance members Donna Spagna and Sally Normington continue to volunteer to provide hands-on assistance, monthly, at the Stanford Cancer Center Wig Bank.
Some other Alliance members volunteer here in Santa Clara County with RotaCare, while others accompany their physician spouses in foreign countries by providing nursing and other administrative duties on these medical missions.
We are advertising for a Development Director to aid in identifying local philanthropic groups with which the Alliance can partner. We wel-come physician alliance members to actively participate in fundraising as well as helping identify those private-public partnerships that require funding.

36 | THE BULLETIN | JULY/AUGUST 2014
HOW THE LIST ON THE NEXT PAGE WAS CREATED
The American Academy of Allergy, Asthma & Immunology (AAAAI) Executive Committee created a task force to lead work on Choosing Wisely consisting of board members, the AAAAI President and Secretary/Treasurer and AAAAI participants in the Joint Task Force on Practice Pa-rameters. Through multiple soci-ety publications and notifications, AAAAI members were invited to offer feedback and recommend el-ements to be included in the list. A targeted email was also sent to an extended group of AAAAI leader-ship inviting them to participate.
The work group reviewed the submissions to ensure the best sci-ence in the specialty was included. Based on this additional members were recruited for their expertise. Suggested elements were consid-ered for appropriateness, relevance to the core of the specialty, po-tential overuse of resources and opportunities to improve patient care. They were further refined to maximize impact and eliminate overlap, and then ranked in order of potential importance both for the specialty and for the public. Fi-nally, the work group chose its top five recommendations which were then approved by the Executive Committee. AAAAI’s disclosure and conflict of interest policy can be found at www.aaaai.org.
For more information or to see other lists of Five Things Physi-cians and Patients should question, visit www.choosingwisely.org.
Originally conceived and piloted by the National Physicians Alliance through a Putting the Charter into Practice grant, leading medi-cal specialty societies along with Consumer Reports, have identified tests or pro-cedures commonly used in their fields whose necessity should be questioned and discussed. The resulting lists of "Things Physicians and Patients Should Question" will spark discussion and the need - or lack thereof - for many frequently ordered tests or treatments.
SCCMA-MCMS is publishing various Choosing Wisely® lists of "Things Physicians and Patients Should Question." Choosing Wisely - see next page - is an initiative of the ABIM Foundation to help physicians and patients engage in conversations to reduce overuse of tests and procedures, and support physician efforts to help patients make smart and effective care choices.
An initiative of the AmericanBoard of Internal Medicine (ABIM) Foundation
Choosing Wisely
PUBLIC HEALTH

JULY/AUGUST 2014 | THE BULLETIN | 37
Don’t perform unproven diagnostic tests, such as immunoglobulin G (IgG) testing or an indiscriminate battery of immunoglobulin E (IgE) tests, in the evaluation of allergy.Appropriate diagnosis and treatment of allergies requires specific IgE testing (either skin or blood tests) based on the patient’s clinical history. The use of other tests or methods to diagnose allergies is unproven and can lead to inappropriate diagnosis and treatment. Appropriate diagnosis and treatment is both cost effective and essential for optimal patient care.
Don’t order sinus computed tomography (CT) or indiscriminately prescribe antibiotics for uncomplicated acute rhinosinusitis.Viral infections cause the majority of acute rhinosinusitis and only 0.5 percent to 2 percent progress to bacterial infections. Most acute rhinosinusitis resolves without treatment in two weeks. Uncomplicated acute rhinosinusitis is generally diagnosed clinically and does not require a sinus CT scan or other imaging. Antibiotics are not recommended for patients with uncomplicated acute rhinosinusitis who have mild illness and assurance of follow-up. If a decision is made to treat, amoxicillin should be first-line antibiotic treatment for most acute rhinosinsutis.
Don’t routinely do diagnostic testing in patients with chronic urticaria.In the overwhelming majority of patients with chronic urticaria, a definite etiology is not identified. Limited laboratory testing may be warranted to exclude underlying causes. Targeted laboratory testing based on clinical suspicion is appropriate. Routine extensive testing is neither cost effective nor associated with improved clinical outcomes. Skin or serum-specific IgE testing for inhalants or foods is not indicated, unless there is a clear history implicating an allergen as a provoking or perpetuating factor for urticaria.
Don’t recommend replacement immunoglobulin therapy for recurrent infections unless impaired antibody responses to vaccines are demonstrated. Immunoglobulin (gammaglobulin) replacement is expensive and does not improve outcomes unless there is impairment of antigen-specific IgG antibody responses to vaccine immunizations or natural infections. Low levels of immunoglobulins (isotypes or subclasses), without impaired antigen-specific IgG antibody responses, do not indicate a need for immunoglobulin replacement therapy. Exceptions include IgG levels <150mg/dl and genetically defined/suspected disorders. Measurement of IgG subclasses is not routinely useful in determining the need for immunoglobulin therapy. Selective IgA deficiency is not an indication for administration of immunoglobulin.
Don’t diagnose or manage asthma without spirometry. Clinicians often rely solely upon symptoms when diagnosing and managing asthma, but these symptoms may be misleading and be from alternate causes. Therefore spirometry is essential to confirm the diagnosis in those patients who can perform this procedure. Recent guidelines highlight spirometry’s value in stratifying disease severity and monitoring control. History and physical exam alone may over- or under-estimate asthma control. Beyond the increased costs of care, repercussions of misdiagnosing asthma include delaying a correct diagnosis and treatment.
3
1
2
5
4
These items are provided solely for informational purposes and are not intended as a substitute for consultation with a medical professional. Patients with any specific questions about the items on this list or their individual situation should consult their physician.
American Academy of Allergy, Asthma & Immunology
Five Things Physicians and Patients Should Question

38 | THE BULLETIN | JULY/AUGUST 2014
Article provided by Food Addicts in Recovery AnonymousYoung or old, many food addicts think it’s too late for them to get
help. However, 40% of Food Addicts in Recovery Anonymous members have been abstinent for four years or longer, regardless of what age they entered the program.
According to Food Addicts in Recovery Anonymous (FA) member Ethel, entering the FA program at an older age, in a wheelchair and with severe health consequences, was not easy. Today, she leads a fulfilling life without abusing food, free of diabetes and other food-related medical problems.
“I am a 75-year-old Afro-American female who joined FA at a later age. Before FA, I was morbidly obese, which caused many health prob-lems such as diabetes, high blood pressure, congestive heart failure, and limited mobility requiring me to use a wheelchair. When I came into FA in 2006, I weighed 321 pounds at the time. Since being in FA, I have lost 180-plus pounds with no need for the wheelchair or meds for diabetes or blood pressure. I walk to my meetings and stand as a healthy and grateful septuagenarian.”
Founded in 1998, FA is an effective, long-term solution to food addic-tion for many people who use food as a drug. As is the case with other ad-dictions, food addiction involves physical craving and an ever-increasing dependence upon and struggle with a substance (food). The manifesta-tions of food addiction vary. Overeating, under-eating or self-starvation, bulimia (including exercise bulimia), and extreme obsession with weight or food are among the symptoms of this addiction.
Men in the program share recovery from these symptoms: “Before learning about FA, my weight was 314 pounds and climbing (yet again). As a Spanish-American male in my early thirties, six years before joining FA, my top weight was 341 (I know I was heavier than that, but I would not get on a scale). I had a laundry list of health problems. Besides being morbidly obese, I had plantar fasciitis in both feet, a bad right knee and lower back, heart palpitations, acid reflux, undiagnosed sleep apnea, high blood pres-sure, high cholesterol, I suffered from anxiety and panic attacks, bouts of vertigo, depression, fear, doubt, and insecurity. Since coming to FA, get-ting a sponsor, and utilizing the tools of the program, the weight came off my body. I now weigh 165 and have maintained this weight for more than five years. I do not suffer from any of those physical (or mental) ailments
Food Addiction Program for Food Addicts of All Ages – It’s Never Too Late

JULY/AUGUST 2014 | THE BULLETIN | 39
any longer. FA has given me a sense of peace, and I know fundamentally all is well as long as I am not eating addictively.”
Before joining the FA program, many adult and teen members were overweight, some by as much as 250 pounds. Others were dangerously underweight or controlled their eating to the point of obsession through under-eating, bulimia, laxatives, or over-exercising. For example, now in recovery, Katie is able to live her life free from the destructive cycle of bu-limia.
“l’m a 40-year-old recovering bulimic, under-eater and compulsive liar. I started bingeing and purging when I was 14 years old. I thought this was the answer to all my prayers, as I quickly took off the extra 20 pounds I couldn’t seem to release by ‘normal’ eating. I’m 5’7”, and, at one point through my use of purging and using laxatives, I weighed only 108. I mixed all of this with almost daily drinking, smoking, and intermittent drug use. I would use anything I could get my hands on that would take me out of reality and help me feel more secure about myself. Through all of this, I stopped menstruating, nearly ruined my teeth, and nearly destroyed some of my relationships because of my incessant lying. After being in recovery for just over 11 years, I’ve maintained a healthy weight and I no longer use anything to ‘control’ my weight. Thankfully, my body has fully recovered, and I was able to conceive and have two beautiful sons. I can’t believe how my life has changed. One year before FA, I recall having fun at a party I went to. Then, something happened, and I found myself at the buffet table eating all the goodies. That night, I felt so disgusting that I hitched a cab and had the driver take me to my office building so I could go throw up where no one was around. I am forever grateful to FA for giving me my health and life back!”
Derrick, 33, experienced the first symptoms of his food addiction in high school, which then carried over into college in the form of compulsive exercising. Derrick remembers, “I was thin, but I was miserably obsessed with food. I found that being thin did not mean being well. I exercised constantly and had no peace until I found FA. At first, I was one of the few guys, but there are more and more men coming into FA.”
Younger members have also experienced success in FA. Cassie, who started the program at age 14 recalls, “At first, it was tough balancing school and FA meetings, but I had to put my recovery first. I watched my grades go way up and can now concentrate on what I’m studying, instead of obsessing about what I’m going to eat.” As a result, Cassie, now in her twenties, is in a graduate program in an area where she participates in the FA program long-distance.
The FA membership of 4,000 members spans 40 states in the U.S. and countries including Canada, France, Germany, Israel, Japan, Austra-lia, New Zealand, Kenya, Turkey, and the United Kingdom. In the United States alone, there are more than 418 weekly FA meetings available for those looking for freedom from food addiction. Many members follow the program with the help of a long-distance sponsor, as there are not yet meetings in their towns and cities.
For more information about FA, visit www.foodaddicts.org, or call the FA World Service Office at 781/932-6300.
About FA:Based on the Twelve Steps and Twelve Traditions of Alcoholics Anonymous (AA), FA is an international fellowship of individuals who, through shared experience and mutual support, are recovering from food addiction. FA is not affiliated with any public or private organization, political movement, ideology, or religious doctrine. Membership in FA is free and is open to anyone who wants to recover from food addiction. The group is comprised of women and men diverse in age, ethnicity, and socio-economic background who experienced difficulty controlling the way they ate.
The 20 Questions
Are You a Food Addict? Ask yourself the following questions and answer them as honestly as you can.
1. Have you ever wanted to stop eating and found you just couldn’t?
2. Do you think about food or your weight constantly? 3. Do you find yourself attempting one diet or food plan after
another, with no lasting success? 4. Do you binge and then “get rid of the binge” through
vomiting, exercise, laxatives, or other forms of purging? 5. Do you eat differently in private than you do in front of
other people? 6. Has a doctor or family member ever approached you with
concern about your eating habits or weight? 7. Do you eat large quantities of food at one time (binge)? 8. Is your weight problem due to your “nibbling” all day long? 9. Do you eat to escape from your feelings? 10. Do you eat when you’re not hungry? 11. Have you ever discarded food, only to retrieve and eat it
later? 12. Do you eat in secret? 13. Do you fast or severely restrict your food intake? 14. Have you ever stolen other people’s food? 15. Have you ever hidden food to make sure you have
“enough?” 16. Do you feel driven to exercise excessively to control your
weight? 17. Do you obsessively calculate the calories you’ve burned
against the calories you’ve eaten? 18. Do you frequently feel guilty or ashamed about what
you’ve eaten? 19. Are you waiting for your life to begin “when you lose the
weight?” 20. Do you feel hopeless about your relationship with food? If you answered “yes” to any of the above questions, then you
may be a food addict. You are not alone. FA offers hope through a real solution to food addiction.

40 | THE BULLETIN | JULY/AUGUST 2014
Although effective with adults, token economies can be especially useful with children who have been diagnosed with chronic conditions. For example, despite advances in pharmacological treatments, hospitalization and mortality rates among children with asthma are on the rise. One explanation is medication non-adherence, which ranges from 17-90% for children with Asthma.3 A recent behavioral psychology study combined the use of education and token economy systems to improve children’s levels of medication adherence and pulmonary functioning. Education included one, one-hour session with educational videos & written handouts about pulmonary functioning, asthma pathophysiology, medications, triggers, and management. For each token economy, children earned and lost tokens for taking or missing their asthma medications. Once a specified amount of tokens were earned, they were exchanged for a list of desired privileges. Following the intervention, children demonstrated increased medication adherence and, as a result, enhanced overall pulmonary functioning.
One way to enhance a token economic system is to incorporate the intervention technique known as shaping. Shaping is a method of reinforcing successive approximations—or smaller progressive steps—toward the development of a targeted behavior (response). As an example, consider the individual working to meet a set fitness goal (e.g., walking on a treadmill for an hour without a break). While working towards the goal, a care provider (or friend) may administer tokens for successive approximations along the way (e.g., the first day walking for 20 minutes without a break, the next day 30 minutes, etc.). By providing tokens for successive approximations over an extended period of time, the individual is more likely to continue with their exercise regimen and, ideally, experience the health benefits associated with the continuation of this routine.
SJP_Summer_2014_Sharing.indd 53 7/14/14 2:59 PM
Human behavior is a major contributor to the current rise in costs of health care. Research has shown that 25 cents of every health care dollar is spent on the treatment of disabilities that result from changeable behaviors (e.g., dieting, exercise, and smoking).
PATIENT BEHAVIOR:
THE KEY TO IMPROVING PATIENT OUTCOMESAUTHORS: AMBER CANDIDO, M.A. AND DANIEL REIMER, M.A.
Understanding the reasons patients engage in unhealthy behavior, or do not engage in health behaviors is important for addressing these issues. The reasons can be examined in terms of the consequences that typically follow a given response. Recall, for example, the last time you shared a funny story with a group of friends or colleagues. What type of response immediately followed the punch line? If the response provided was laughter, it is probable that the tendency to repeat the story in the future was “reinforced.” Meaning, following the laughter, you became more likely to repeat the story in a future, similar situation.
In the behavioral literature, the term “reinforcer” describes a consequence that 1) follows a given response and 2) increases the probability that the response will recur in the future. By incorporating this principle and application techniques into a medical practice, physicians around the world may be able to improve the outcomes of various diseases affected by health behaviors. This increase in improved health outcomes will then lead to decreased health care costs and increased patient satisfaction. There are many different strategies to use, but a few of the most common and convenient to implement are discussed below.
TOKEN ECONOMIESToken economies—where patients are rewarded with points or “tokens” for reaching pre-set goals—have been used to improve human behavior in a variety of populations, including those that monitor: psychiatric patients, medical patients, alcoholics, drug addicts, nursing-home residents and persons with a variety of developmental disabilities. 2 In a token economy, patients first determine daily or weekly goals (e.g., exercising for 45 minutes a day). Then, patients receive a token, check a box, or log this information into their phone, each time the goal is met. Once the patient reaches a pre-set number of tokens, they can exchange those tokens for a reward they enjoy, like dessert or a massage.
SJP_Summer_2014_Sharing.indd 52 7/14/14 2:59 PM

Although effective with adults, token economies can be especially useful with children who have been diagnosed with chronic conditions. For example, despite advances in pharmacological treatments, hospitalization and mortality rates among children with asthma are on the rise. One explanation is medication non-adherence, which ranges from 17-90% for children with Asthma.3 A recent behavioral psychology study combined the use of education and token economy systems to improve children’s levels of medication adherence and pulmonary functioning. Education included one, one-hour session with educational videos & written handouts about pulmonary functioning, asthma pathophysiology, medications, triggers, and management. For each token economy, children earned and lost tokens for taking or missing their asthma medications. Once a specified amount of tokens were earned, they were exchanged for a list of desired privileges. Following the intervention, children demonstrated increased medication adherence and, as a result, enhanced overall pulmonary functioning.
One way to enhance a token economic system is to incorporate the intervention technique known as shaping. Shaping is a method of reinforcing successive approximations—or smaller progressive steps—toward the development of a targeted behavior (response). As an example, consider the individual working to meet a set fitness goal (e.g., walking on a treadmill for an hour without a break). While working towards the goal, a care provider (or friend) may administer tokens for successive approximations along the way (e.g., the first day walking for 20 minutes without a break, the next day 30 minutes, etc.). By providing tokens for successive approximations over an extended period of time, the individual is more likely to continue with their exercise regimen and, ideally, experience the health benefits associated with the continuation of this routine.
SJP_Summer_2014_Sharing.indd 53 7/14/14 2:59 PM
JULY/AUGUST 2014 | THE BULLETIN | 41
Human behavior is a major contributor to the current rise in costs of health care. Research has shown that 25 cents of every health care dollar is spent on the treatment of disabilities that result from changeable behaviors (e.g., dieting, exercise, and smoking).
PATIENT BEHAVIOR:
THE KEY TO IMPROVING PATIENT OUTCOMESAUTHORS: AMBER CANDIDO, M.A. AND DANIEL REIMER, M.A.
Understanding the reasons patients engage in unhealthy behavior, or do not engage in health behaviors is important for addressing these issues. The reasons can be examined in terms of the consequences that typically follow a given response. Recall, for example, the last time you shared a funny story with a group of friends or colleagues. What type of response immediately followed the punch line? If the response provided was laughter, it is probable that the tendency to repeat the story in the future was “reinforced.” Meaning, following the laughter, you became more likely to repeat the story in a future, similar situation.
In the behavioral literature, the term “reinforcer” describes a consequence that 1) follows a given response and 2) increases the probability that the response will recur in the future. By incorporating this principle and application techniques into a medical practice, physicians around the world may be able to improve the outcomes of various diseases affected by health behaviors. This increase in improved health outcomes will then lead to decreased health care costs and increased patient satisfaction. There are many different strategies to use, but a few of the most common and convenient to implement are discussed below.
TOKEN ECONOMIESToken economies—where patients are rewarded with points or “tokens” for reaching pre-set goals—have been used to improve human behavior in a variety of populations, including those that monitor: psychiatric patients, medical patients, alcoholics, drug addicts, nursing-home residents and persons with a variety of developmental disabilities. 2 In a token economy, patients first determine daily or weekly goals (e.g., exercising for 45 minutes a day). Then, patients receive a token, check a box, or log this information into their phone, each time the goal is met. Once the patient reaches a pre-set number of tokens, they can exchange those tokens for a reward they enjoy, like dessert or a massage.
SJP_Summer_2014_Sharing.indd 52 7/14/14 2:59 PM

42 | THE BULLETIN | JULY/AUGUST 2014
In a few recent behavioral psychology studies, the combined use of shaping and token economic procedures have been shown to effectively reduce smoking among adolescences.4,5 In one study, shaping procedures were created and monitored through a web-based contingency management program where individuals were expected to provide video recordings of breath CO samples three times per day. Tokens were earned and could be exchanged for monetary rewards (gift cards) for incremental reductions in breath CO. Through this program, cigarette smoking was reduced, and, because the program was completed at home, it was believed to be more effective than one which requires travel: there is less response effort on both the part of the individual and the care provider who is monitoring the progress.
VISUAL REPRESENTATIONS OF DATAVisually tracking individual performance has been utilized in a variety of work and educational settings, particularly with respect to goal setting.6 The act of visually representing data involves tracking important medical measures over time with the individual’s data graphically represented as an effective form of visual feedback. Such visual representations allow patients to 1) easily review their medical measures and 2) be held accountable for their actions (or inactions) via an additional person monitoring their progress (e.g., a physician, care provider, or friend). This type of intervention can be useful in targeting several areas of behavioral health, including: diet regulation, exercise performance, blood pressure and/or heart rate monitoring, smoking cessation, etc. Physicians interested in monitoring the performance (or omission of) target behavior(s) can use visual representations of data to set and track collaborative patient goals. Goal progression can then be monitored in a variety of ways ranging from the old “pen-and-paper” method to the use of Smart Phone applications available to us at our fingertips. Using either method, patients can track, monitor, and upload their progress to track their results in real time. Early studies of electronic weight loss aids suggest that allowing individuals to construct their own regimen on their phone or computer could be key to reversing a variety of behavioral health-related epidemics (e.g., obesity). Such affordable, accessible tools may radically change the way we conceive of and administer health care, potentially saving the system billions of dollars in the process. For example, David H. Freedman, a consulting editor for John Hopkins Medicine International, describes an iPhone application called “Lose it” that allows users to track their eating and physical activity simply by holding their phones up to a food package’s bar
code, or by tapping the screen a few times at the start and end of a walk. This data is used to provide clear, graphic feedback on a user’s daily progress—“you might see at a glance that having a dessert will send your numbers into the red, but after you walk for 20 minutes, you’ll go back into the green.”7 Additionally, Behavioral Psychologist Matt Normand (University of the Pacific) is currently working to identify precise methods to track patient caloric intake and expenditure by, for example, collecting receipts for food purchases, providing checklists to record what is eaten, and measuring physical activity using tools such as pedometers. He then provides patients with visual representations of their behavior over time.
CONCLUSION:The science of behavior change has much to offer to health care professionals. Through the use of behavioral principles and technologies, small adjustments in behavior and lifestyle can be changed and maintained for the purpose of preventative care. Weight loss regimens can be designed to aid with the obesity epidemic; medication adherence interventions can be targeted in patients of all ages; cigarette smoking can be reduced for the prevention of associated cancers; the list of possibilities is truly endless. Targeting incremental behavior change in at-risk populations can help with the prevention or reduction to the severity of the disease before they become dangerous to the patient, time-consuming for the physician, and costly for the overall health care system. Physicians and other health care professionals do not have to create and customize behavioral health care interventions on their own; there are multiple strategies to integrate these concepts into medical practice. Health care technology has developed substantially in the last decade, making tracking health behaviors easy and affordable. Many providers are also beginning to develop collaborative relationships with behavioral health institutions or professionals who are experts in developing and implementing the strategies previously discussed. These collaborations are mutually beneficial, with physicians receiving expertise, support and cost-savings and behavioral health professionals receiving access to new populations of patients. Rapid changes to healthcare policy are requiring shifts in traditional healthcare practices. The changes will require creative solutions to some of medicine’s most systemic problems. The abovementioned techniques are examples of a few small changes physicians can make to address these issues.
SJP_Summer_2014_Sharing.indd 55 7/14/14 2:59 PM

JULY/AUGUST 2014 | THE BULLETIN | 43
Samaritan Internal Medicine is
partnered with University HealthCare
Alliance, Stanford Hospital & Clinic’s
medical foundation. The structure allows
for the preservation of a private practice
environment while providing access to one
of the world’s leading medical institutions.
JOIN OUR TEAM AND ENJOY• Professional and personal life balance
• Income guarantee and comprehensive
benefits package
• Infrastructure that supports practice growth
• Providing the most advanced care possible
with enhanced quality and service
• Contributing to SHC’s research, health
education and community service mission
CONTACT
Angela Van Ginkel, MBAManager, Provider Recruitment and Relations
tel: 650.725.1501 email: [email protected]
An exceptional practice opportunity awaits you at
Samaritan Internal Medicine. Our group has been meeting
patients’ needs for more than 30 years in the Silicon Valley.
We believe that excellent communication leads to excellent
care and we are dedicated to the health and well-being of
our patients and their families.
OPPORTUNITY - POSITION DETAILS
We are seeking a full-time Internal Medicine physician to
begin work fall of 2014. Our office is located in San Jose,
CA and we currently utilize Epic EHR. We are a 5 person
medical group with 4 MDs and 1 NP/PA providing
internal medicine services to our community.
Join Samaritan Internal Medicine
Premier community healthcare providers located in Northern California
In a few recent behavioral psychology studies, the combined use of shaping and token economic procedures have been shown to effectively reduce smoking among adolescences.4,5 In one study, shaping procedures were created and monitored through a web-based contingency management program where individuals were expected to provide video recordings of breath CO samples three times per day. Tokens were earned and could be exchanged for monetary rewards (gift cards) for incremental reductions in breath CO. Through this program, cigarette smoking was reduced, and, because the program was completed at home, it was believed to be more effective than one which requires travel: there is less response effort on both the part of the individual and the care provider who is monitoring the progress.
VISUAL REPRESENTATIONS OF DATAVisually tracking individual performance has been utilized in a variety of work and educational settings, particularly with respect to goal setting.6 The act of visually representing data involves tracking important medical measures over time with the individual’s data graphically represented as an effective form of visual feedback. Such visual representations allow patients to 1) easily review their medical measures and 2) be held accountable for their actions (or inactions) via an additional person monitoring their progress (e.g., a physician, care provider, or friend). This type of intervention can be useful in targeting several areas of behavioral health, including: diet regulation, exercise performance, blood pressure and/or heart rate monitoring, smoking cessation, etc. Physicians interested in monitoring the performance (or omission of) target behavior(s) can use visual representations of data to set and track collaborative patient goals. Goal progression can then be monitored in a variety of ways ranging from the old “pen-and-paper” method to the use of Smart Phone applications available to us at our fingertips. Using either method, patients can track, monitor, and upload their progress to track their results in real time. Early studies of electronic weight loss aids suggest that allowing individuals to construct their own regimen on their phone or computer could be key to reversing a variety of behavioral health-related epidemics (e.g., obesity). Such affordable, accessible tools may radically change the way we conceive of and administer health care, potentially saving the system billions of dollars in the process. For example, David H. Freedman, a consulting editor for John Hopkins Medicine International, describes an iPhone application called “Lose it” that allows users to track their eating and physical activity simply by holding their phones up to a food package’s bar
code, or by tapping the screen a few times at the start and end of a walk. This data is used to provide clear, graphic feedback on a user’s daily progress—“you might see at a glance that having a dessert will send your numbers into the red, but after you walk for 20 minutes, you’ll go back into the green.”7 Additionally, Behavioral Psychologist Matt Normand (University of the Pacific) is currently working to identify precise methods to track patient caloric intake and expenditure by, for example, collecting receipts for food purchases, providing checklists to record what is eaten, and measuring physical activity using tools such as pedometers. He then provides patients with visual representations of their behavior over time.
CONCLUSION:The science of behavior change has much to offer to health care professionals. Through the use of behavioral principles and technologies, small adjustments in behavior and lifestyle can be changed and maintained for the purpose of preventative care. Weight loss regimens can be designed to aid with the obesity epidemic; medication adherence interventions can be targeted in patients of all ages; cigarette smoking can be reduced for the prevention of associated cancers; the list of possibilities is truly endless. Targeting incremental behavior change in at-risk populations can help with the prevention or reduction to the severity of the disease before they become dangerous to the patient, time-consuming for the physician, and costly for the overall health care system. Physicians and other health care professionals do not have to create and customize behavioral health care interventions on their own; there are multiple strategies to integrate these concepts into medical practice. Health care technology has developed substantially in the last decade, making tracking health behaviors easy and affordable. Many providers are also beginning to develop collaborative relationships with behavioral health institutions or professionals who are experts in developing and implementing the strategies previously discussed. These collaborations are mutually beneficial, with physicians receiving expertise, support and cost-savings and behavioral health professionals receiving access to new populations of patients. Rapid changes to healthcare policy are requiring shifts in traditional healthcare practices. The changes will require creative solutions to some of medicine’s most systemic problems. The abovementioned techniques are examples of a few small changes physicians can make to address these issues.
SJP_Summer_2014_Sharing.indd 55 7/14/14 2:59 PM

44 | THE BULLETIN | JULY/AUGUST 2014
Physicians need to be especially careful when managing chronic pain with opioid medications. Medical practices often seek risk management advice when they suspect a patient is misusing prescription medications, is not complying with treatment, or when the patient is making unreasonable demands for more opioids. If a patient suffers harm as a result of opioid medication use, a physician may find himself the target of a lawsuit alleging negligent treatment of chronic pain. The following tips may help
physicians and office staff
members increase patient safety
and lower liability exposure
related to these factors. >>
Risk Management, PMSLIC Insurance Company and the NORCAL Group
Jane Mock, Risk Management Specialist
Managing the Risks of Treating
Chronic Pain
with Opioids
MANAGING PROFESSIONAL RISK
PRACTICE MANAGEMENT
TREATING CHRONIC PAIN WITH OPIOIDS
Managing Professional Risk is a quarterly feature of NORCAL Mutual Insurance Company and the NORCAL Group. More information on this topic, with continuing medical education (CME) credit, is available to NORCAL Mutual insureds. To learn more, visit www.norcalmutual.com/cme.
NORCAL
N

JULY/AUGUST 2014 | THE BULLETIN | 45
HOW DOES THE MANAGEMENT OF OPIOIDS CREATE POTENTIAL LIABILITY? Claims against physicians for negligent treatment and/or management of opioid medications frequently arise from the following: · Prescribing opioids without performing any diagnostic examinations · Prescribing an excessive quantity of opioids · Prescribing additional narcotics when not indicated · Failing to consider, screen for, or suspect narcotic addiction, and failing to refer the patient for treatment of drug addiction · Negligent monitoring · Failing to consult or refer to a pain specialist
IS THE STORY CLEAR? The physician might think that he or she has managed a patient’s pain appropriately, but if the medical record documentation does not ref lect that, defense of care is difficult. Examples of poor documentation include: · No indication that the treating physician reviewed the patients prior medical records or studies · No physical exam results · No quantitative assessments of the patients pain · No indication that the treating physician discussed the risk of opioid addiction · No pain medication agreement · No evidence of assessment of effectiveness of the pain medications · No rationale for the physicians medication choices · No copies of narcotic prescriptions
RISK MANAGEMENT TIPS Clinicians can avoid reaching a point of crisis by applying a risk management approach to treating chronic pain.
Perform and document a comprehensive history and physical examination of the patient. · Complete all indicated diagnostic exams and tests. · Use an objective, comprehensive pain assessment tool. · Evaluate the patient for his or her risks of abusing medication. · Request copies of prior medical records.
Base the treatment plan on the patient’s individual needs. · Document differential diagnoses. · Consider and try both pharmacologic and non-pharmacologic pain treatments. · Manage patient expectations and educate patients about physical dependence, tolerance, and addiction.
Document this discussion, as well as a plan of action to address physical dependence. · Document clinical decision making and rationale for one treatment choice over another. · Have patient sign a pain management agreement, if indicated.
Re-evaluate and document the patient’s level of pain and response to treatment at each visit. · Consider having the patient keep a pain diary. · Note the effectiveness and patient compliance with various treatment modalities · Document the patients response, changes to the treatment plan, and your clinical rationale. · Document the name of the drug, dose, frequency with which the patient has been taking the medication; reported effectiveness; and the impact on the patient’s daily activities. · Communicate with other providers who are treating the patient. · Strongly consider utilizing your states prescription drug monitoring program · Utilize and refer to specialists when appropriate. · Be familiar with local resources that can provide assistance (e.g., pain clinics, teaching hospitals). · Obtain second opinions when indicated. · When choosing not to pursue clarification of a symptom or complaint, document the rationale.
Be aware of signs of drug abuse or misuse. · Set limits with patients; consider using a therapeutic pain medication agreement. · Do not provide narcotic refills unless the patient comes in for re-assessment. · Evaluate the appropriateness of the requests in light of the prescription provided. · If you suspect substance abuse, carefully document details of the situation and discussions with the patient in the patient’s medical record.
Monitor the patient’s non-compliance. · Enforce the pain management agreement, when indicated. · Document the patients action or inaction that led to termination or discontinuation of pain medications and rationale for the decision. · Contact your medical professional liability insurers risk management department for guidance relating to terminating a patient from the practice.

46 | THE BULLETIN | JULY/AUGUST 2014
At the close of this year’s open enrollment period, nearly 1.4 million consumers had completed the Covered California enrollment process, which significantly surpassed initial expectations. This makes it critical that physicians and their staff understand these new insurance products to minimize the inevitable frustration and confusion that has resulted from such a large-scale change to the health insurance industry.
KNOW YOUR PARTICIPATION STATUSIn late April 2014, the California Medical Association (CMA) sur-
veyed physicians about their contracting experience with Covered Cali-fornia plans. Eighty percent of respondents reported that they had been confused about their participation status in a Covered California plan and that they believed such confusion had negatively impacted patient care.
Unfortunately, checking your practice’s participation status is not as straightforward as it might seem. Plagued with inaccuracies, Covered Cal-ifornia took down its cross-plan provider directory earlier this year. Add to that the fact that some exchange plans have used vague contract terms and amendments that rope physicians into participating in their exchange networks, often without their express consent or knowledge, and you’ll see that “do you take my insurance” is not always an easy question to answer.
Physicians are encouraged to verify their participation status on the individual exchange plans’ online provider directories. When searching,
Three Things Every Physician Should Know About Covered California

JULY/AUGUST 2014 | THE BULLETIN | 47
it’s important to select the correct exchange product type, as Anthem Blue Cross and Blue Shield of Califor-nia are utilizing significantly narrowed networks for their exchange products.
It is also important that front office staff have a clear understanding of their physicians’ participation status. With all of the new exchange plans added to the mix, it is no longer satisfactory to simply accept “I have Blue Shield” as an indication of whether the patient can be seen in-network. It is important, when scheduling, to determine in advance if the physician is indeed in the patient’s network. When scheduling an appointment, practices should request that the patient provide the of-fice with a copy of the front and back of their insurance ID card. Having a copy of the ID card in advance will allow the practice to clearly identify whether they are in the patient’s network and also to verify patient eligibility before the visit. Taking these steps could help patients avoid out-of-network costs and eliminate frustration when they are faced with larger than expected bills.
Exchange Plans and ProductsFor a detailed list of the exchange plans and prod-
ucts, see “Qualified Health Plan Networks for Covered California” available in the CMA exchange resource cen-ter at www.cmanet.org/exchange.
BE AWARE OF MIRROR PRODUCTS
Every plan offered in the exchange must also be of-fered outside of the exchange, using the same provider network. This has resulted in a number of practices un-knowingly seeing patients out-of-network for products that use an exchange network, as these ID cards will not have the Covered California logo on them. The issue is specific to just Anthem Blue Cross and Blue Shield of California, because they are the only two plans offering narrowed networks. Practices must review patient ID
cards and eligibility information closely to identify whether the practice is in or out of network for that particular plan.
UNDERSTAND THE GRACE PERIODFederal law allows Covered California enrollees who receive financial
subsidies to keep their health insurance for three months after they have stopped paying their premiums. This is known as the “federal grace pe-riod.” In the first 30 days of the grace period, federal law requires plans to pay for services incurred, but in months two and three of the grace period, plans can pend and deny claims. So it will be extremely important that practices verify eligibility on all exchange patients, ideally on the date of service, or as near the time of service as possible. If the patient is in months two or three of the grace period, the health plan should indicate that cov-erage is inactive or otherwise suspended.
Insurance cards for exchange enrollees do not indicate whether the enrollee is subsidized. Current enrollment trends predict that nearly 90% of those with exchange coverage will be subsidized and receive the three-month grace period. In other words, if you see a Covered California logo on the ID card, you should assume they will have the three-month grace period.
Unsubsidized exchange patients and those with a mirror product are not entitled to the 90-day federal grace period; rather, they only receive the
30-day grace period called for under state law.CMA queried Anthem Blue Cross, Blue Shield of California, and
Health Net, which account for approximately 75% of the total Covered California enrollees, on exactly what to look for in eligibility verification to identify patients who are in months two and three of the grace period. They report the following:
Practices should have policies in place regarding how they will han-dle patients who are in months two or three of the grace period. Patients should ideally be made aware of this policy in advance. If a patient’s eligi-bility verification comes back indicating his or her coverage is not active, the practice should treat the situation as they would any other patient who has had a lapse in coverage. For non-emergent services, patients may be given the option to either pay cash at the time of service or reschedule to a later date when their coverage is effective. The office policy should include how patients will be triaged to determine whether their condition is emer-gent or urgent and the policy should be approved by the physician.
Having Trouble Finding an In-Network Provider or Facility?Patients who are having trouble finding an in-network physician or fa-
cility are encouraged to contact the Department of Managed Health Care’s Help Center at 888/466-2219 for assistance.
We also ask that physicians notify CMA if they are experiencing dif-ficulties finding in-network providers to whom they can refer patients so that we may raise the issue with Covered California and the appropriate regulator. Contact CMA’s physician helpline at 888/401-5911 or [email protected].
AVAILABLE RESOURCESThe following resources (and many more) are available free to mem-
bers in CMA’s exchange resource center at www.cmanet.org/exchange.• Covered California: Know Your Participation Status: This
document provides detailed instruction on how to check your participation status with the various exchange plans.
• Surviving Covered California Tip Sheets: These documents contain tips on what to expect from and how to survive the first year of Covered California.
• Qualified Health Plan Networks for Covered California: This document will help both physicians and patients decipher the new exchange product networks.
• Covered California—Understanding the Grace Period for Subsidized Exchange Enrollees: This document contains answers to frequently asked questions about the Covered California grace period.
• CMA’s Got You Covered: CMA’s comprehensive exchange toolkit for physicians.
• Frequently Asked Patient Questions About Covered California: Available in both English and Spanish, this document provides answers to the most common patient questions.
STILL HAVE QUESTIONS?Members and their staff have FREE access to CMA’s reimbursement
helpline at 888/401-5911 or [email protected].
Plan Name Grace Period Eligibility Status Indicator (Days 31-90 of grace period)
Anthem Blue Cross “Inactive pending investigation”
Blue Shield of California “Pended”
Health Net “Eligibility suspended”

48 | THE BULLETIN | JULY/AUGUST 2014
Here Come the Lady Physicians
By Michael A. Shea, MDLeon P. Fox Medical History Committee
The first woman to graduate from medical school in the United States was Elizabeth Blackwell. She graduated from Geneva Medical College, in Upstate New York, in 1849. Shortly thereafter, the Women’s Medical College of Pennsylvania, in Philadelphia, opened in 1850. This model for women’s medical schools was copied in Boston, New York, Detroit, and Chicago. Later, medical schools of all three systems (allopaths, homeo-paths, and eclectics) became coed.
In California, the University of California Medical School opened its doors to women applicants in 1873. The Medical School of the Pacific did, likewise, in 1877. Official recognition of women as medical practitioners did not take place until 1876, when Governor Irwin signed the Medical Practice Law. There were, however, female physicians who arrived in Cali-fornia well before this date.
The first was Dr. Eliza Pfeifer Stone. German born and educated, she arrived in Nevada City in 1857, and relocated to San Francisco in 1863. The second was Dr. Rebecca A. Howard, arriving in San Francisco in 1864, directly after receiving her degree at Philadelphia. Her husband was killed at the battle of Bull Run, and her daughter, Dr. Kate I. Howard, was to be-come a University of California medical graduate in 1885. Dr. Euthanasia S. Meade (l836-1895) (yes, that is her actual first name) was the third.
Her attention was first drawn to the profession during the last years
of the Civil War. At St. Joseph’s Hospi-tal in Philadelphia, she gained her first exposure to medicine by taking care of wounded soldiers. Four years after the war, she graduated from the Women’s College of Pennsylvania. She practiced under her preceptor, Dr. Wilson in Philadelphia, visiting the hospitals and gaining practical experience.
In 1869, she arrived in San Fran-cisco, but found San Jose a more favor-able climate for her asthma, and thus, became San Jose’s first female certified physician.
She, along with five other women physicians, were admitted to the State Medical Society, which convened in San Francisco in 1786. The vote was even, but it took-the president of the society, Dr. A. B. Nixon, to cast the deciding affirmative vote.
Dr. Meade was instrumental in forming the Women’s Medical Club of the Pacific, a statewide medical society. She was elected the first presi-dent and delivered the inaugural address at the opening convention.
Her junior partner for three years was Dr. Elizabeth Gallimore (see picture). She was born locally and received her diploma from Cooper Med-ical College, in San Francisco, in 1887. For 15 months, she was a resident physician at the Children’s Hospital in San Francisco. She also attended a post graduate course at the New England Hospital in Boston. She returned to San Jose and joined Dr. Meade in her medical practice. Dr. Gallimore served as recording secretary for the County Medical Society for many years. She enjoyed the respect and admiration of all her colleagues in San Jose.
Enrollment in the United States medical schools for 2013 was 83,473. 44,525 (53%) were men and 38,948 (47%) were women. The ladies have come a long way from 1849.
Dr. Elizabeth Gallimore

JULY/AUGUST 2014 | THE BULLETIN | 49
31 Chapters covering 110 pages of the local medical history from the Ohlone Period to the American Period • Origin of major Bay Area hospitals (SCVMC, O’Connor Hospital,
San Jose Hospital, Agnews State Hospital, and more)• History of UCSF and Stanford medical schools and founders • Biographies of pioneer physicians (e.g., Benjamin Cory, John
Townsend, John Marsh, Euthanasia Meade, Henry Warburton, and more)
• Topics of interest (e.g., Trephination, Bloodletting, Gold Rush Med-icine, Orifi cial Surgery, Cholera Epidemic of 1850, Famous Grizzly Bear Attack of 1854)
NOWAVAILABLE From Medicine Man to Medical Doctor Th e Medical History of Early Santa Clara Valley
$19.95 incl. S&H FOR INQUIRIES/ORDERS – SEND CHECK TO:Michael A. Shea, MD 6807 Leyland Park Drive San Jose, California 95120 Email: [email protected] Phone: 408/268-5820
All profi ts will be donated to the con-struction of the new medical museum at Santa Clara Valley Medical Center.
Authors:Michael A. Shea, MD;
Gerald E. Trobough, MD;Elizabeth Ahrens-Kley

50 | THE BULLETIN | JULY/AUGUST 2014
OFFICE SPACE FOR RENT/LEASE
WHY ENRICH YOUR LANDLORD? • MEDICAL OFFICE SPACE – MTN VIEWRent/Buy/or Option to purchase 2,000 sq. ft. office with minor surgical suite in first class building within walking distance of El Camino Hospital. Full service lease, with or without fur-nishings. Call 650/961-2652.
MEDICAL OFFICE SPACE FOR LEASE • SANTA CLARAMedical space available in medical building. Most rooms have water and waste. Reception, exam rooms, office, and lab. X-ray available in building. Billing available. 2,500–4,000 sq. ft. Call Rick at 408/228-0454.
MEDICAL SUITES • GILROYFirst class medical suites available next to Saint Louise Hospital in Gilroy, CA. Sizes available from 1,000 to 2,500+ sq. ft. Time-share also available. Call Betty at 408/848-2525.
DOWNTOWN MONTEREY OFFICE FOR SUBLEASESpacious, recently remodeled, excellent park-ing, flexible terms. Call Molly at 831/644-9800.
MEDICAL SPACE AVAILABLE • CAMPBELLState-of-the-art medical space available to share on Bascom and White Oaks. Up to three exam rooms with shared common areas. Ideal for primary care or specialist. For more infor-mation, please contact Davina at Age Defying Dermatology at 408/369-4210.
OFFICE FOR RENT • SAN JOSE2395 Montpelier Dr #5, San Jose 95116. Rent $2,000 per month. Lease required. Owner pays
triple net and monthly H/O dues. Two doctors set up. Three examination rooms. Approxi-mately 1,100 sq. ft., furnished or unfurnished, adequate parking, walk to Regional Med Ctr. Close to X-Ray and lab. Previous tenant doctor retired. Call Marie at 408/268-2040.
MEDICAL OFFICE SPACE TO SHARE • SUNNYVALEConvenient location. One large private office plus one exam room, shared waiting room and front office. Newly built, total 1,280 sq. ft. Avail-able now. Please call 408/438-1593.
MEDICAL OFFICE SPACE TO SUBLET • MTN VIEWMountain View medical office space to sub-let. 1,100 sq. ft. Available three days a week. In large medical complex, behind El Camino Hospital. Basement storage, utilities included. Large treatment rooms, small lab space, BR, private office, etc. Call Dr. Klein at cell 650/269-1030.
PERFECT SATELLITE OFFICE • MTN VIEW Beautiful medical office across from Palo Alto Medical Foundation. Professional office with vaulted ceilings, new interior, digital x-ray, natural light, and Wi-Fi. Trained receptionist to schedule patients, make reminder calls, collect paperwork and insurance info. Rent exam room one to five days per week, excellent office – low overhead. Call 650/814-8506.
MEDICAL/DENTAL/PROFESSIONAL OFFICE SUITE • SALINASSecond story of professional building across from SVMH. Private balcony. Freshly painted and carpeted, ready for occupancy. 1,235 sq. ft. at $1.25/sq. ft. Rent is $1,544/month. Contact Steven Gordon at 831/757-5246.
Classifieds
METRO MEDICAL BILLING, INC.
• Full Service Billing• 25 years in business• Book Keeping• ClinixMIS web based software• Training and Consulting• Client References
Contact Lynn (408) [email protected]
Visit our Website www.metromedicalbilling.com
S.C.C.M.A.8-12-08
Physicians Nurse Practitioners ~ Physician Assistants
Locum Tenens ~ Permanent Placement
Tracy Zweig AssociatesA R E G I S T R Y & P L A C E M E N T F I R M
Voice: 800-919-9141 or 805-641-9141FAX : 805-641-9143

JULY/AUGUST 2014 | THE BULLETIN | 51
PRIME MEDICAL OFFICE FOR LEASE • SANTA CLARAIdeal for medical, dental, physical therapy, optometry, office use. Approxi-mately 1,700 sq. ft., near Santana Row. Excellent parking. Call owner at 408/858-9687.
OFFICE SPACE FOR RENT • REDWOOD CITYDoctor’s space for rent. Prime Redwood City location, one support staff member, new carpet and cabinetry, cleaning included. Call 650/365-1110.
EMPLOYMENT OPPORTUNITY
OCCUPATIONAL MEDICINE PHYSICIANS • PRIMARY CARE, ORTHOPEDICS, & PHYSIATRYOur occupational medical facilities offer a challenging environment with minimal stress, without weekend, evening, or “on call” coverage. We are currently looking for several knowledgeable and progressive primary care and specialty physicians (orthopedist and physiatrist) interested in joining our team of professionals in providing high quality occupational medi-cal services to Silicon Valley firms and their injured employees. We can provide either an employment relationship including full benefits or an independent contractor relationship. Please contact Rick Flovin, CEO at 408/228-0454 or e-mail [email protected] for additional infor-mation.
INTERNAL MEDICINE PHYSICIAN NEEDEDWe are looking for an internal medicine physician for our multi-specialty group. Please email your CV to [email protected].
PART-TIME GENERAL DERMATOLOGIST NEEDEDSunnyvale Dermatology (Dr. Bernard Recht) is looking for a part-time Dermatologist. We are a well established, busy office and we are looking for someone to work one to two days per week. Please email your CV to [email protected].
FOR SALE
MIDMARK POWER 100Very good condition; little used. Tan/dark brown. Includes stirrups, 30 cloth exam gowns and drapes. $150. Pick up in Palo Alto. Contact Alan Brauer, MD at 650/329-8001 or email at [email protected].
ORDER YOURCOPIES TODAY!
There are a lot of updates andchanges in the new 2014 edition.
Make sure to order enough copies for you and your staff!
Contact Maureen Yrigoyen at 408/998-8850 today!
2014Physician
MembershipResourceDirectory
NOWAVAILABLE!
JOIN SAMARITAN INTERNAL MEDICINE
PREMIER COMMUNITY HEALTHCARE PROVIDERS LOCATED IN NORTHERN CALIFORNIA
An exceptional practice opportunity awaits you at Samaritan In-ternal Medicine. Our group has been meeting patients’ needs for more than 30 years in the Silicon Valley. We believe that excellent communication leads to excellent care and we are dedicated to the health and well-being of our patients and their families.
Opportunity - Position DetailsWe are seeking a full time Internal Medicine physician to begin work fall of 2014. Our office is located in San Jose, CA and we currently utilize Epic EHR. We are a 5 person medical group with 4 MDs and 1 NP/PA providing internal medicine services to our community.
Join our team and enjoy:• Professional and personal life balance• Income guarantee and comprehensive benefits package• Infrastructure that supports practice growth• Providing the most advanced care possible with enhanced qual-
ity and service• Contributing to SHC’s research, health education, and commu-
nity service mission
CONTACTAngela Van Ginkel, MBA Manager, Provider Recruitment & Relations 650-725-1501 [email protected]
WANTED: MEDICAL MEMORABILIA PROJECT: NEW MEDICAL MUSEUM
AT SCVMCA new, innovative, state-of-the-art medical museum is being
planned at SCVMC. It is a joint project with SCVMC and SCCMA. We are looking for any medical artifacts or antiques that would be con-nected with any medical or surgical field. Equipment, books, displays, instruments, etc., would be welcomed. If you wish to donate any of the aforementioned items, please contact Michael Shea, MD, at 408/268-5820 or [email protected].
Samaritan Internal Medicine is partnered with University HealthCare Alliance, Stanford Hospital & Clinic’s medical foun-dation. The structure allows for the preservation of a private practice environment while providing access to one of the world’s leading medical institutions.

52 | THE BULLETIN | JULY/AUGUST 2014
MEMBER SPOTLIGHT
A Different Kind of CME:Kiteboarding Epiphany
By Joseph Andresen, MDPhysician Editor, The Bulletin
Inspired by my father, I’ve always had a love of the wind and water. From that first sail, in a light summer breeze on an El Toro at our local res-ervoir, to a bald-headed jibe in 30 knots of breeze and ebb tide, racing on the San Francisco Bay, a wealth of memories come to mind. Now reaching my seventh decade, I’m beginning to see life’s horizon in the distance. This certainly causes one to reflect on what you want to do when you grow up and what remains undone.
Said so eloquently, the essence of happiness is simplicity.And kiteboarding may be one of the simplest and most intimate ways
to connect with the wind and the waves. The City Front spectacle of kite-boarders skipping over the ebb chop sparked my imagination. This would require a skilled and knowledgeable guide before venturing into this un-
known water wilderness. Nat Lincoln, Edge Kiteboarding instructor, be-came my trailblazer on this new journey, keeping me off the lee shore and always offering encouragement. After hearing that his AC skipper client was up and riding independently on his very first day, I was determined to put my best foot forward! However on day four, I was mostly in the water rather than riding on top of it.
Anxiety increased with the wind speed and the kite size, and I set an eject record of sorts, clumsily hitting the safety release with my board within the first few minutes of body dragging out to the launch site, re-quiring a shore-side untangle of lines and equipment. But day five was a different story. The wind was stronger, the kite bigger, and suddenly I was in charge, skimming across the water, not bothering to watch the kite, but taking in the texture of waves and water as my board carved through the ever changing seascape. An epiphany of sorts, my journey has just begun.
https://www.youtube.com/watch?v=IxT8Z78lZVY

JULY/AUGUST 2014 | THE BULLETIN | 53
GLOBAL MEDICAL BRIGADE
SCU STUDENTS GIVE THEIR TALENTS
This year, again, the Global Medi-cal Brigade students of Santa Clara University have had a successful mis-sion in Ghana. The 32 students under supervision by three physicians pro-vided medical and dental care and hy-giene instructions to the people of the village of Ebiram (1,300 inhabitants). Refer to January/February issue of The Bulletin, page 14.
The students extend a hearty sentiment of gratitude to those physi-cians and para-medical who so gener-ously donated to this project. For any questions or comments, please contact Mike Wallace at SCU ([email protected]) or Mel Russi, MD ([email protected]).

54 | THE BULLETIN | JULY/AUGUST 2014
We Celebrate Excellence
– Corey S. Maas, MD, FACS CAP member and founder of “Books for Botox®” community outreach program, benefitting the libraries of underfunded public schools
S a n D i e g o
o r a n g e
L o S a n g e L e S
P a L o a L T o
S a c r a m e n T o
800-252-7706 www.CAPphysicians.com
Superior Physicians. Superior Protection.
For over 30 years, the Cooperative of American Physicians, Inc. (CAP) has provided California’s finest physicians, like San Francisco facial plastic surgeon Corey Maas, MD, with superior medical professional liability protection through its Mutual Protection Trust (MPT). Physician owned and physician governed, CAP rewards excellence with remarkably low rates on medical professional liability coverage – up to 40 percent less than our competitors. CAP members also enjoy a number of other valuable benefits, including comprehensive risk management programs, best-in-class legal defense, and a 24-hour CAP Cares physician hotline. And MPT is the nation’s only physician-owned medical professional liability provider rated A+ (Superior) by A.M. Best. We invite you to join the more than 11,000 preferred California physicians already enjoying the benefits of CAP membership.
CAP_1341_SCCMA.indd 1 8/4/11 9:59 AM

JULY/AUGUST 2014 | THE BULLETIN | 55
We Celebrate Excellence
– Corey S. Maas, MD, FACS CAP member and founder of “Books for Botox®” community outreach program, benefitting the libraries of underfunded public schools
S a n D i e g o
o r a n g e
L o S a n g e L e S
P a L o a L T o
S a c r a m e n T o
800-252-7706 www.CAPphysicians.com
Superior Physicians. Superior Protection.
For over 30 years, the Cooperative of American Physicians, Inc. (CAP) has provided California’s finest physicians, like San Francisco facial plastic surgeon Corey Maas, MD, with superior medical professional liability protection through its Mutual Protection Trust (MPT). Physician owned and physician governed, CAP rewards excellence with remarkably low rates on medical professional liability coverage – up to 40 percent less than our competitors. CAP members also enjoy a number of other valuable benefits, including comprehensive risk management programs, best-in-class legal defense, and a 24-hour CAP Cares physician hotline. And MPT is the nation’s only physician-owned medical professional liability provider rated A+ (Superior) by A.M. Best. We invite you to join the more than 11,000 preferred California physicians already enjoying the benefits of CAP membership.
CAP_1341_SCCMA.indd 1 8/4/11 9:59 AM

Address service requested
700 Empey Way, San Jose, CA 95128-4705
PRSRT STDU.S. PostagePAID
San Jose, CAPermit No. 503
BULLETINTHE
Official magazine of the Santa Clara County Medical Association and the Monterey County Medical Society
Our mission begins and ends with you, the policyholder. That means connecting our members to the highest quality products and services at the lowest responsible cost. Join us as we enter a new phase of our journey and advance with our vibrant new look and expanding offerings.
hello.norcalmutual.com
Proud to be endorsed by the Monterey County Medical Society and the Santa Clara County Medical Association.
N O R C A L M u t u A L I N s u R A N C e C O M p A N y