Embed Size (px)
Citation preview

Ultrasonographic colonic polyps
diagnosis of juvenile
Akira Nag i ta , MD, Kanji A m e m o t o , MD, Atsushi Yoden, MD, Takeshi Yamazaki , MD, M a k o t o Mino, MD, and Hirofumi Miyoshi, MD
From the Department of Pediatrics and the Second Department of Internal Medicine, Osaka Medical College, Osaka, Japan
To reduce the risks of air-contrast barium enemas and colonoscopy, we studied the use of saline enemas for ultrasonographic examination of children with rec- tal bleeding. Thirty-nine children, from 2 years 8 months to 8 years 3 months of age, were examined. Juvenile colonic polyps were ultrasonographically dem- onstrated and histologically confirmed in 25 children; all the polyps were sol- itary and pedunculated, and were located in the splenic flexure in 3 children, the descending colon in 6, the sigmoid colon in 12, and the rectum in 4. Ultra- sonographic findings by hydrocolonic ultrasonography were identical to those obtained by immersion ultrasonography of removed specimens. Hypoechoic areas within more hyperechoic polyps were shown histologically to be dilated glandular canals, The 14 children in whom no abnormal ultrasonographic find- ings were shown had no further rectal bleeding after resuming regular defeca- tion, and 5 of these 14 had negative colonoscopic findings. No adverse reac- tions were noted in any child during or after the saline enema examination. We conclude that ultrasonographic examination with a saline enema is a safe and accurate method of assessing children with rectal bleeding, especially for the diagnosis of juvenile colonic polyps. (J PEDIATR 1994;124:535-40)
Standard diagnostic methods for identifying juvenile co- lonic polyps, such as air-contrast barium enema or colonos- copy, are technically demanding and invasive. Transab- dominal ultrasonographic examination with infusion of tepid water has been used to evaluate the colon and the rec- tum. 1-3 We prospectively studied the diagnostic value of this method in children who had rectal bleeding.
M E T H O D S
Thirty-nine consecutive childrens (23 boys) who had blood-tinged feces were studied. Their ages ranged from 2 years 8 months to 8 years 3 months. None had a family his- tory of juvenile polyps. The duration of the bleeding before
Submitted for publication July 21, 1993; accepted Oct. 14, 1993. Reprint requests: Akira Nagita, MD, Department of Pediatrics, Osaka Medical College, 2-7, Daigaku-cho, Takatsuki, Osaka 569, Japan. Copyright �9 1994 by Mosby-Year Book, Inc. 0022-3476/94/$3.00 + 0 9/20/52164
medical care was sought varied from 1 week to 6 months. The children fasted on the day of the examination. Before
the ultrasonographic examination, they were given glycer- ine enemas to completely empty the Colon. They then received a single oral dose (60 mg/kg) of monosodium trichloroethyl phosphate syrup (chloral hydrate; Nippon Glaxo Ltd., Tokyo, Japan) as a sedative 30 minutes before the examination. After a digital examination, a balloon catheter was inserted into the rectum. Initially the balloon was filled with water, and then warmed (30 ~ C) physiologic sodium chloride solution was slowly infused into the colon through the catheter. Transabdominal ultrasonographic examination was performed with a real-time scanning de- vice with 3.5 or 7.5 MHz transducers (Sonolayer-V SSA- 90A; Toshiba Medical Co. Ltd., Japan). The saline solution was infused until the cecum was visualized (hydrocolonic ultrasonography)) For examination of the colonic flexures, a lateral intercostal view was obtained. The ultrasono- graphic diagnosis of colonic polyps was made if intralumi- nal masses, fixed to the wall, were demonstrated. The max-
535
5 3 6 1Vagita et al. The Journal of Pediatrics April 1994
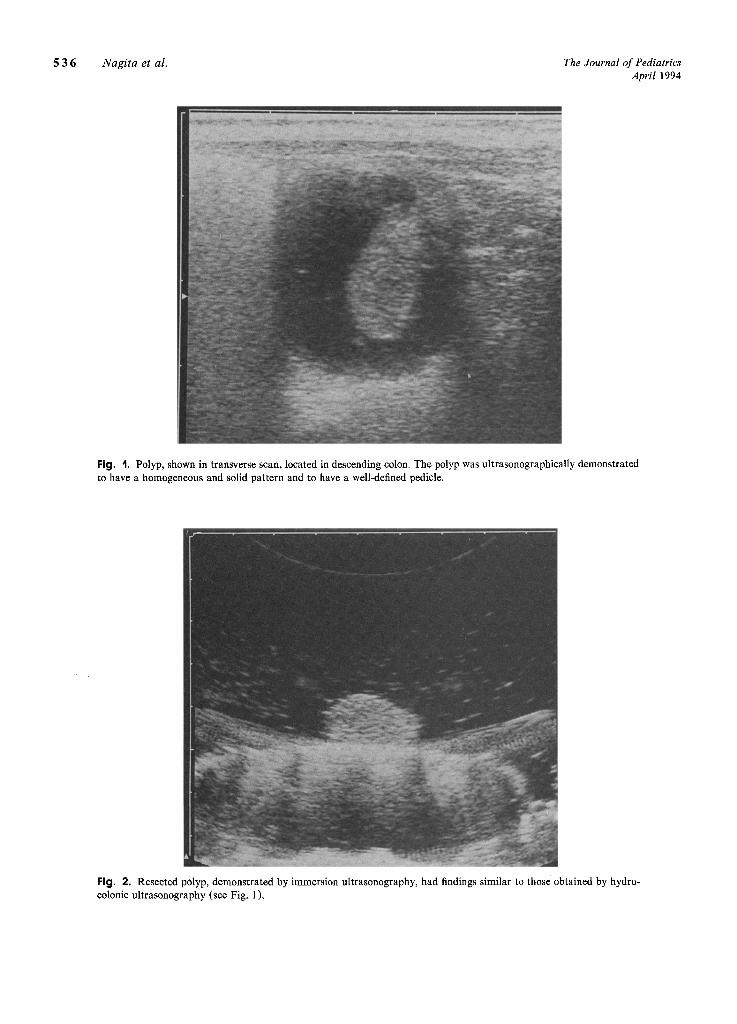
Fig. I. Polyp, shown in transverse scan, located in descending colon. The polyp was ultrasonographically demonstrated to have a homogeneous and solid pattern and to have a well-defined pedicle.
Fig. 2. Resected polyp, demonstrated by immersion ultrasonography, had findings similar to those obtained by hydro- colonic ultrasonography (see Fig. 1).
The Journal of Pediatrics Nagita et al. 5 3 7 Volume 124, Number 4
imal length of the polyps was measured by the cursor attached to the ultrasonographic device. Fecal masses were distinguishable from polyps because they were not fixed to the wall and had typical acoustic shadows. Serum electro- lytes were measured in all children 30 minutes after the ex- amination.
Children with an ultrasonographic diagnosis of colonic polyps (n = 25) underwent colonoscopy with polypectomy. The removed polyps were immersed in water and underwent a second, in vitro, ultrasonographic examination (immer- sion ultrasonography). After the size was measured with a ruler, histologic examination was performed and the find- ings were compared with those obtained by ultrasound ex- amination (Figs. 1 to 6).
Children with no demonstrable findings on ultrasound study (n = 14) were given saline purgatives or dietary and behavioral training designed to produce regular defecation habits. Children who continued to have bleeding or whose parents requested further study (n = 5) received colonos- copy. Informed consent for the study was obtained from parents or guardians as approved by the ethics committee of Osaka Medical College, Osaka, Japan.
R E S U L T S
The entire large intestine could be visualized in all chil- dren. The intratuminal space of the colon was shown either to be echo free or, especially in the ascending colon, to have a "snowstorm" appearance. Air-free visualization of the entire colon was made possible by changing the child's po- Sition. The maximal volume of saline solution infused was 800 ml. The older four children complained of an urge to defecate. The maximal time required for the examination after infusion of the solution into the colon was 30 minutes. Chloral hydrate sedation alone was adequate to allow com- pletion of the procedure in all children. No child had an ad- verse reaction. Serum electrolytes were normal 30 minutes after the examination in all children.
In 25 of 39 children, colonic polyps were demonstrated ultrasonographically as echogenic structures in the intesti- nal lumen. All polyps were solitary and pedunculated. Three were located in the splenic flexure, 6 in the descending co- lon, 12 in the sigmoid colon, and 4 in the rectum. The max- imal length of the polyps measured by the ultrasound cur- sor and ruler ranged from 14 to 25 mm and from 14 to 27 mm, respectively. The images displayed by the polyps on hydrocolonic ultrasonography were the same as those by immersion ultrasonography (Figs. 1 and 2, 4 and 5). All the resected polyps were identified histologically as juvenile co- lonic polyps. In eight polyps, small circular and more hypo- echoic areas were present within echogenic structures (Figs.
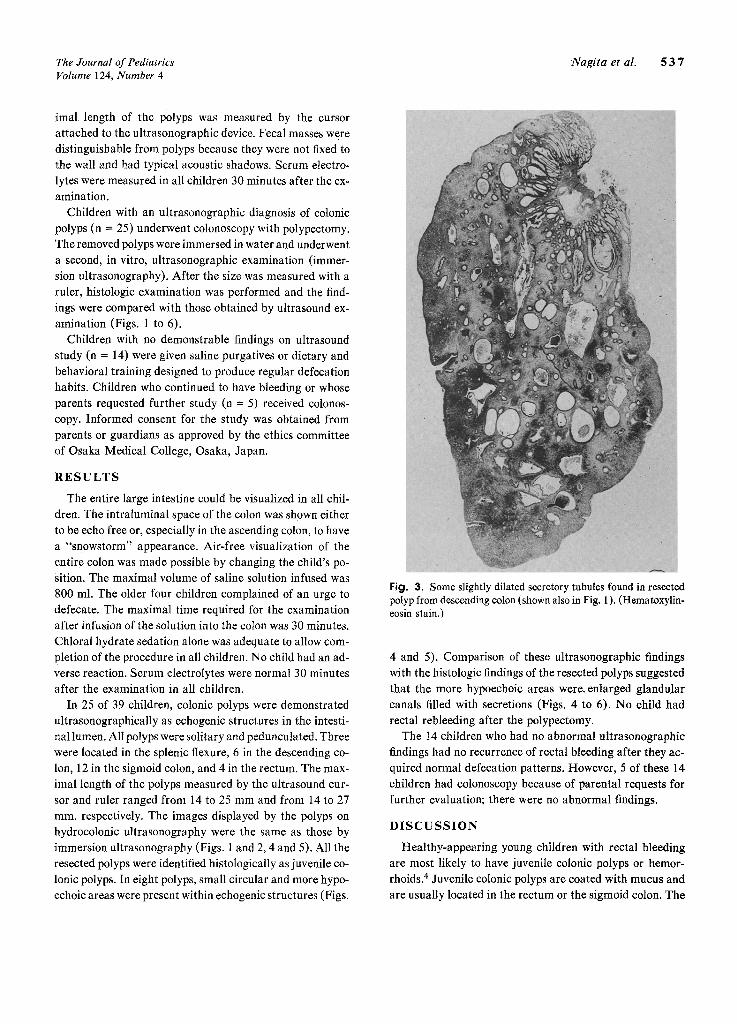
Fig. 3. Some slightly dilated secretory tubules found in resected polyp from descending colon (shown also in Fig. 1 ). (Hematoxylin- eosin stain.)
4 and 5). Comparison of these ultrasonographic findings with the histologic findings of the resected polyps suggested that the more hypoechoic areas were~ enlarged glandular canals filled with secretions (Figs. 4 to 6). No child had rectal rebleeding after the polypectomy.
The 14 children who had no abnormal ultrasonographic findings had no recurrence of rectal bleeding after they ac- quired normal defecation patterns. However, 5 of these 14 children had colonoscopy because of parental requests for further evaluation; there were no abnormal findings.
D I S C U S S I O N
Healthy-appearing young children with rectal bleeding are most likely to have juvenile colonic polyps or hemor- rhoids. 4 Juvenile colonic polyps are coated with mucus and are usually located in the rectum or the sigmoid colon. The
5 3 8 Nagita et al. The Journal of Pediatrics April 1994
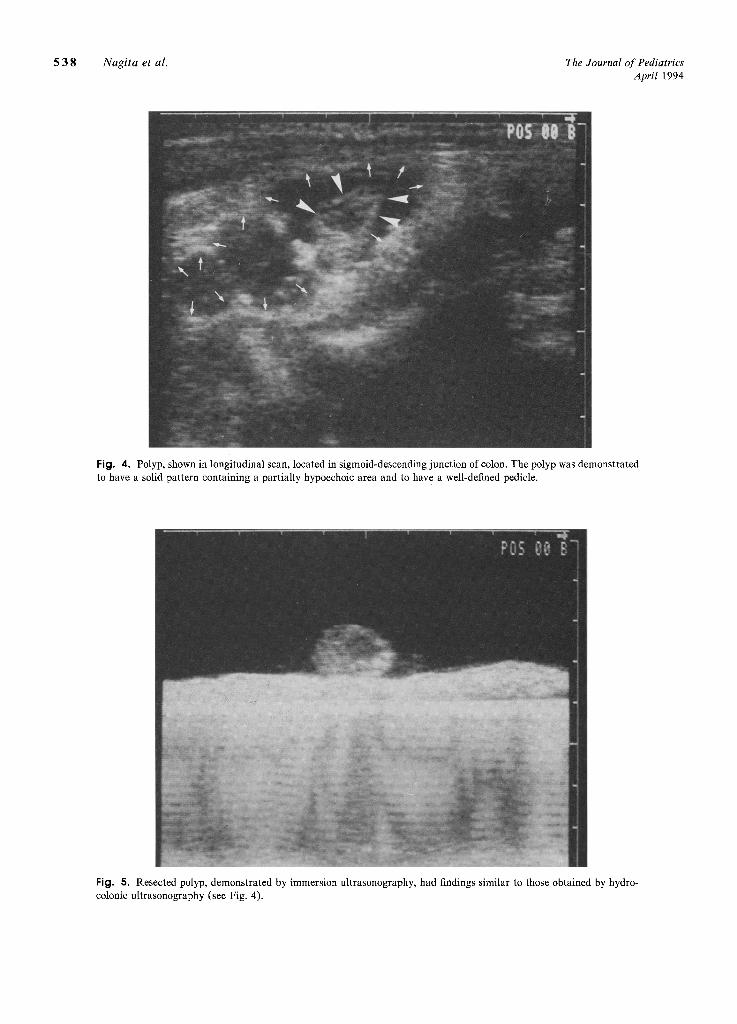
Fig. 4, Polyp, shown in longitudinal scan, located in sigmoid-descending junction of colon. The polyp was demonstrated to have a solid pattern containing a partially hypoechoic area and to have a well-defined pedicle.
Fig. 5. Resected polyp, demonstrated by immersion ultrasonography, had findings similar to those obtained by hydro- colonic ultrasonography (see Fig. 4).
The Journal o f Pediatrics Nagi ta et al. 5 3 9 Volume 124, Number 4
surface of growing polyps is presumably injured by fecal passage. Therefore the characteristic clinical symptom is passage of bright red blood-tinged mucus on the surface of feces. 5 If the polyps are located more proximally, as in the descending colon, the blood may be found not only on the surface but also in the core of the feces. A simple method of differentiating juvenile colonic polyps from hemorrhoids is to soften the stool by the use of saline purgatives; children with juvenile colonic polyps continue to bleed. Pedunculated juvenile colonic polyps may induce intussusception) ,6 Moreover, juvenile colonic polyps have a small but definite neoplastic potential] Accordingly, early resection of juve- nile colonic polyps is recommended. 6, 7
It has been thought that the definitive diagnosis of juve- nile colonic polyps requires air-contrast barium enema or colonoscopy.5, 8 In children, however, both procedures pose challenges, such as difficulty in bowel preparation and lack of patient cooperation, and both can be technically de- manding because of the multiple colonic flexures and elon- gation of the colon. Risks include radiation exposure and possible traumatic rupture of the bowel. In contrast, hydro- colonic ultrasonographyis not associated with large amounts of irrigation, radiation exposure, or traumatic complica- tions.3, 9, 10 These results confirm the diagnostic value of hydrocolonic ultrasonography in children with peduncu- lated juvenile colonic polyps. 11, 12 Additionally, when the location of the polyps was demonstrated with hydrocolonic ultrasonography, endoscopic polypectomy was technically less demanding.
The procedure reported is virtually pain free; mild chlo- ral hydrate sedation was adequate in all children. The use of physiologic saline solution is an advantage because there is virtually no effect on the serum electrolytes. When a larger amount of cold saline solution was infused into the colon, children tended to complain of an urge to defecate; warming of the solution reduced this complaint. Bowel preparation with ordinary glycerine enemas was sufficient to allow us to distinguish the polyps from fecal masses; ir- rigation of the colon was not required. As reported previ- ously, 3 infusion of sufficient solution into the colon and changing the child's position prevented interference from air accumulated in the colon. It is important to use a cath- eter with a balloon volume exceeding 20 ml to prevent leak- age of the solution from the anus.
Juvenile colonic polyps are classified as hamartomatous polyps. 13 Proliferation of glandular canals is one of their histologic features. 13 Markedly dilated canals, which may often be visible macroscopically, were demonstrated as hy- poechoic areas by hydrocolonic ultrasonography and were also demonstrated by immersion ultrasonography. Ultra-
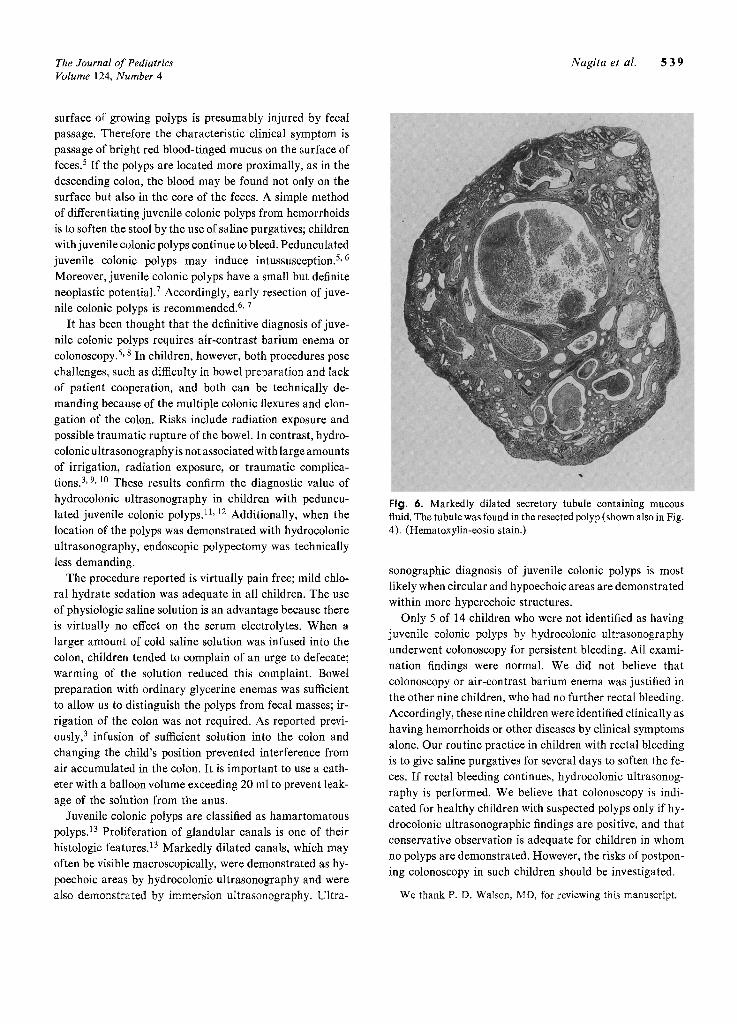
Fig. 6. Markedly dilated secretory tubule containing mucous fluid. The tubule was found in the resected polyp (shown also in Fig. 4). (Hematoxylin-eosin stain.)
sonographic diagnosis of juvenile colonic polyps is most likely when circular and hypoechoic areas are demonstrated within more hyperechoic structures.
Only 5 of 14 children who were not identified as having juvenile colonic polyps by hydrocolonic ultrasonography underwent colonoscopy for persistent bleeding. All exami- nation findings were normal. We did not believe that colonoscopy or air-contrast barium enema was justified in the other nine children, who had no further rectal bleeding. Accordingly, these nine children were identified clinically as having hemorrhoids or other diseases by clinical symptoms alone. Our routine practice in children with rectal bleeding is to give saline purgatives for several days to soften the fe- ces. If rectal bleeding continues, hydrocolonic ultrasonog- raphy is performed. We believe that colonoscopy is indi- cated for healthy children with suspected polyps only if hy- drocolonic ultrasonographic findings are positive, and that conservative observation is adequate for children in whom no polyps are demonstrated. However, the risks of postpon- ing colonoscopy in such children should be investigated.
We thank P. D. Waison, MD, for reviewing this manuscript.

5 4 0 Nagita et al. The Journal of Pediatrics April 1994
REFERENCES
1. Rubin C, Kurtz AB, Goldberg BB. Water enema: a new ultra- sound technique in defining pelvic anatomy. J Clin Ultrasound 1978;6:28-33.
2. Jasinski R, Rubin JM, Beezhold C, Aisen A. Ultrasound ex- amination of the colon. J Clin Ultrasound 1981;9:206-8.
3. Limberg B. Diagnosis and staging of colonic tumors by conventional abdominal sonography as compared with hydro- colonic sonography. N Engl J Med 1992;327:65-9.
4. Silber G. Lower gastrointestinal bleeding. Pediatr Rev 1990; 12:85-93.
5. Hamilton JR. Tumors of the digestive tract in children. In: Behrman RE, ed. Nelson textbook of pediatrics. 14th ed. Phil- adelphia: WB Saunders, 1992;992-4.
6. Arthur AL, Garvey R, Vaness DG. Colocolic intussusception in a three-year-old child caused by a colonic polyp. Conn Med 1990;54:492-4.
7. Giardiello FM, Hamilton SR, Kern SE, et al. Colorectal nee-
plasia in juvenile polyposis or juvenile polyps. Arch Dis Child 1991;66:971-5.
8. Cynamon HA, Milov DE, Andres JM. Diagnosis and man- agement of colonic polyps in children. J PED~ATR 1989; 114:593-6.
9. Wang G, Liu S. Enema reduction of intussusception by hydrostatic pressure under ultrasound guidance: a report of 377 cases. J Pediatr Surg 1988;23:814-8.
10. Woo SK, Kim JS, Suh SJ, Paik TW, Choi SO. Childhood in- tussusception: US-guided hydrostatic reduction. Radiology 1992;182:77-80.
11. Skaane P. Ultrasonic demonstration of a pedunculated colonic polyp. J Clin Ultrasound 1987;15:204-6.
12. Waiter DF, Govil S, Korula A, William RR, Chandy G. Pe- dunculated colonic polyp diagnosed by colonic sonography. Pediatr Radiol 1992;22:148-9.
13. Shermeta DW, Morgan WW, Eggleston J, White J J, Haller A Jr. Juvenile retention polyps. J Pediatr Surg 1969;4:211-5.
BOUND VOLUMES AVAILABLE TO SUBSCRIBERS
Bound volumes of the 1994 issues of THE JOURNAL OF PEDIATRICS are available to subscribers (only) from the Publisher, at a cost of $70.00 for domestic, $90.90 for Canadian, and $86.00 for international subscribers, for Vol. 124 (January-June) and Vol. 125 (July-December), shipping charges included. Each bound volume contains subject and author indexes, and a|l advertising is removed. Copies are shipped within 60 days after publication of the last issue in the volume. The binding is durable buckram, with the Journal name, volume number, and year stamped in gold on the spine. Payment must accompany all orders. Contact Mosby-Year Book, Inc., Subscrip- tion Services, 11830 Westline Industrial Dr., St. Louis, M e 63146-3318, USA/800-453-4351, or 314-453-4351.
Subscriptions must be in force to qualify. Bound volumes are not available in place of a regular Journal subscription.





























