Embed Size (px)
Citation preview

ORIGINAL ARTICLE
The effect of renin–angiotensin system blockade on the incidenceof end-stage renal disease in IgA nephropathy
Shigeru Tanaka1• Toshiharu Ninomiya1,5
• Ritsuko Katafuchi2 • Kosuke Masutani1 •
Masaharu Nagata1• Akihiro Tsuchimoto1
• Hideki Hirakata3• Takanari Kitazono1,5
•
Kazuhiko Tsuruya1,4
Received: 8 September 2015 / Accepted: 29 October 2015
� Japanese Society of Nephrology 2015
Abstract
Background The impact of renin–angiotensin system
blockade (RASB) on the incidence of end-stage renal dis-
ease (ESRD) remains unclear in IgA nephropathy (IgAN).
Methods This study assessed associations between RASB
treatment and the incidence of ESRD in IgAN using
propensity score approaches. We retrospectively analyzed
1273 patients with IgAN biopsied between 1979 and 2010.
Propensity scores were calculated using logistic regression.
Associations between RASB and ESRD were examined
using a Cox regression model adjusted by inverse proba-
bility of treatment weighted, regression, stratification and
matching.
Results During follow-up (median 5.1 years), 130
patients developed ESRD. With Cox regression adjusted by
inverse probability of treatment weighted, RASB use was
significantly associated with a lower risk of ESRD (hazard
ratio 0.58; 95 % confidence interval 0.42–0.80). Significant
associations were observed for other propensity score-
based approaches. In stratified analysis, a beneficial asso-
ciation between RASB and ESRD was observed in patients
C35 years, with hypertension, reduced estimated
glomerular filtration rate (\60 mL/min/1.73 m2), mesan-
gial proliferation and segmental glomerulosclerosis (P for
interaction\0.05), and tended to be greater in patients with
proteinuria (C1.0 g/24 h), extracapillary proliferation and
receiving methylprednisolone pulse therapy (P for inter-
action\0.10).
Conclusion Treatment with RASB was associated with a
lower incidence of ESRD in the real-world practice of
IgAN.
Keywords Pathology � Interaction � Causal effect
Introduction
Immunoglobulin A nephropathy (IgAN) is reported to be
the most common primary glomerulonephritis globally [1,
2]. The renin–angiotensin system plays a central role in the
progression of chronic kidney diseases [3]. In IgA
nephropathy, several randomized control trials and sys-
tematic reviews have demonstrated the beneficial effects of
renin–angiotensin system blockade (RASB) on the reduc-
tion in proteinuria and improvement in kidney function,
which is assessed by the slope of estimated glomerular
filtration rate (eGFR) decline [4–7]. Most previous trials
recruited subjects with proteinuria C1 g/day, and therefore
the renoprotective effect of RASB in IgAN has been
mainly confirmed in this population [4, 5]. Hence, the
Electronic supplementary material The online version of thisarticle (doi:10.1007/s10157-015-1195-y) contains supplementarymaterial, which is available to authorized users.
& Kazuhiko Tsuruya
1 Department of Medicine and Clinical Science, Graduate
School of Medical Sciences, Kyushu University, Fukuoka,
Japan
2 Kidney Unit, National Fukuoka-Higashi Medical Center,
Koga, Japan
3 Division of Nephrology and Dialysis Center, Japanese Red
Cross Fukuoka Hospital, Fukuoka, Japan
4 Department of Integrated Therapy for Chronic Kidney
Disease, Graduate School of Medical Sciences, Kyushu
University, 3-1-1 Maidashi, Higashi-ku, Fukuoka 812-8582,
Japan
5 Division of Research Management, Center for Cohort
Studies, Graduate School of Medical Sciences, Kyushu
University, Fukuoka, Japan
123
Clin Exp Nephrol
DOI 10.1007/s10157-015-1195-y

kidney disease improving global outcome (KDIGO) clini-
cal practice guideline for management of glomeru-
lonephritis recommends that RASB should be considered
as a first-line supportive therapy in IgAN when proteinuria
is[1 g/day [8].
In contrast, there are, as yet, few data to suggest a
favorable clinical effect of RASB in preventing the inci-
dence of end-stage renal disease (ESRD) in IgAN [8].
Additionally, there is no clinical evidence identifying the
optimal therapeutic target population for RASB therapy
according to stratification for patient background (i.e.,
proteinuria, eGFR, and pathological severity grade). In
particular, it remains uncertain whether the long-term
renoprotective effect of RASB differs among patients with
urine protein excretion levels \0.5, 0.5–1, and [1 g/day
[8].
Since most evidence for the efficacy of RASB in IgAN
is derived from randomized control trials in which the
population had a relatively short-term observation period
and an extremely low incidence of ESRD [4, 5], it is
difficult to address the relationship between RASB and
the incidence of ESRD. We speculated that the effec-
tiveness of RASB at preventing ESRD in real-world
practice could be better confirmed with observational
datasets with sufficient long-term follow-up periods rather
than in short-term randomized control trials. To this end,
we investigated whether RASB showed a long-term
benefit in reducing the incidence of ESRD using
propensity score-based approaches in a large cohort of
1273 patients with IgAN. Additionally, we examined
whether the effect of RASB use on the risk of ESRD
differed in each subgroup stratified based on clinico-
pathological parameters at presentation.
Methods
Study population
A total of 1602 patients with biopsy proven IgAN, who had
received kidney biopsy at seven participating institutions
(Kyushu University Hospital, Japanese Red Cross Fukuoka
Hospital, Hamanomachi Hospital, Munakata Medical
Association Hospital, Japan Seamen’s Relief Association
Moji Hospital, Karatsu Red Cross Hospital, and Hakujyuji
Hospital) between October 1979 and December 2010 were
eligible to participate in the study. Patients whose biopsy
specimen contained\10 glomeruli (n = 172), and patients
for whom data on one or more clinical parameters were
unavailable (n = 157) were excluded. Finally, 1273
patients with primary IgAN were enrolled in the present
study. Patients were followed until December 31, 2012.
The study was performed with the approval of the Clinical
Research Ethics Committee of the Institutional Review
Board at the Kyushu University and all participating
institutions (approval number 469-05).
Clinical parameters
Kidney biopsy records were reviewed to define potential
confounders, including age, sex, blood pressure, and levels
of cholesterol, triglycerides, serum creatinine, and 24-h
urinary protein excretion or urinary protein–creatinine
ratio. Hypertension was defined as blood pressure C140/
90 mmHg. Total cholesterol concentrations and triglyc-
erides were determined enzymatically. Serum creatinine
was measured by Jaffe’s method until April 1988, and by
the enzymatic method from May 1988 at Kyushu Univer-
sity. At the other participating institutions, serum creatinine
was measured by Jaffe’s method until December 2000, and
by the enzymatic method from January 2001. Serum cre-
atinine values measured by Jaffe’s method were converted
to values for the enzymatic method by subtracting
0.207 mg/dL [9]. eGFR was calculated using the Schwartz
formula in patients under the age of 18, and the following
formula in patients over the age of 18: eGFR (mL/min per
1.73 m2) = 194 9 Cr-1.094 9 age-0.287 (if female,
90.739) [10–12]. Proteinuria was defined as a protein
excretion C1.0 g/24 h at the time of biopsy [13]. The use
of RASB (ACE-I, ARB) or corticosteroid for at least
6 months at any time in the follow-up period was defined
as treatment. The number of patients in each group
receiving ACE-I and ARB could not obtain due to the lack
of medical record information. We adopted the definition
of drug use in accordance with previous investigations of
IgAN patients [14, 15]. The patients taking immunosup-
pressive drugs except for corticosteroid were not included
in the present cohort.
Pathologic parameters
Pathologic lesions were evaluated according to the Oxford
classification [16]. Mesangial hypercellularity score
(M) was defined as M0 if the score was B0.5 and M1 if the
score was [0.5. Endocapillary hypercellularity (E) and
segmental glomerulosclerosis (S) were defined as E0, S0 if
absent and E1, S1 if present. In addition to the Oxford
pathologic lesions, extracapillary proliferation (Ex) was
defined as Ex0 if absent and Ex1 if present. Tuft adhesions
were classified as S1 lesions. Tubular atrophy/interstitial
fibrosis (T) was semiquantitatively classified according to
the ratio of the cortical area involved with the tubular
atrophy or interstitial fibrosis: T0, if 0–25 %; T1, if
26–50 %; and T2, if[50 %.
Clin Exp Nephrol
123

Renal outcome
The primary outcome was incidence of ESRD. ESRD was
defined as the initiation of renal replacement therapy,
including hemodialysis, peritoneal dialysis and kidney
transplantation. The secondary outcome was composite
kidney outcome defined as doubling serum creatinine or
ESRD. The date of incidence of doubling serum creatinine
was defined as the date that the serum creatinine value
doubled by two or more times in succession. Kidney out-
comes of patients were surveyed by reviewing the medical
records or telephone consultation with the clinics and
hospitals where the patients visited or with the patients
themselves. Patients were censored at the date of their
death, or at the end of follow-up for those still alive.
Statistical analysis
Differences in baseline characteristics between populations
who received and did not receive administration of RASB
were compared using standardized mean difference in both
pre-matching and post-matching cohorts [17]. A standard-
ized difference was obtained from dividing absolute differ-
ence between mean of the treatment group and mean of the
control group by an estimate of the sample standard devia-
tion for each covariate. Differences of \10 % generally
suggest little or no imbalance between groups. Achieving
balance between treated and untreated patients implies the
development of a good propensity score [18]. The unadjusted
and multivariable-adjusted hazard ratios (HR) with 95 %
confidence interval (CI) of administration of RASB for the
development of ESRD were calculated using a Cox pro-
portional hazard model. To reduce the impact of selection
bias on treatment assignment and potential confounding in
observational data, we performed a rigorous adjustment for
significant imbalance between the treated and untreated
RASB groups in a weighted Cox proportional hazard model
using the inverse probability of treatment weighting (IPTW)
[19]. The IPTW can thus generate a pseudo-population in
which each covariate combination is perfectly balanced
between treatment and non-treatment groups [20]. The
propensity score for each individual was calculated using a
logistic regression model with administration of RASB (yes/
no) as the dependent variable, and age, sex, mean arterial
pressure, serum albumin, serum total cholesterol, serum
triglycerides, uric acid, urine protein excretion, eGFR, the
incidence of Oxford pathological lesions with M, E, S, T1,
T2 and Ex, and therapeutic interventions (intravenous
methylprednisolone pulse, oral corticosteroid and tonsillec-
tomy) as covariates. Model performance was assessed using
the c statistic (i.e., area under the curve by logistic regression
with binary outcomes) and Hosmer–Lemeshow goodness-
of-fit tests.
To confirm the robustness of our findings, we conducted
a further Cox regression analysis in three alternative
methods, such as a regression adjustment as a linear
covariate, a stratification analysis stratified into quintiles of
their estimated propensity score [17] and a matching
method using greedy matching algorithm, with a caliper
width of 0.2 standard deviations of the logit of the
propensity score, at a ratio of 1:1 without replacement [21].
The multivariable HRs were estimated using a Cox
regression models with robust standard errors to account
for the clustering in matched pairs [22].
The Kaplan–Meier survival curve between two groups
was compared using log-rank tests and Cox regression
analysis adjusted with inverse probability weights based on
the propensity score [23]. The starting survival time of the
cohort in the Cox regression analysis is the date of biopsy-
confirmed IgAN. Heterogeneity in the relationship between
subgroups was tested by adding a multiplicative interaction
term to the relevant Cox model weighted with propensity
score. Statistical analyses were conducted using the SAS
software package version 9.2 (SAS Institute, Cary, NC,
USA) and R version 3.0.2 (http://www.r-project.org). A
two-tailed P value \0.05 was considered statistically
significant.
Results
Study participants and baseline characteristics
During the follow-up period, 558 of 1273 patients (43.8 %)
received RASB therapy at participating study centers.
Baseline characteristics of all 1273 patients with or without
RASB in the entire cohort are shown in Table 1. Values for
mean arterial pressure, serum total cholesterol, serum
triglycerides, uric acid, urinary protein excretion, and the
incidence of Oxford pathological lesions with M1, E1, S1
and Ex1 were significantly higher in the RASB therapy
group. Imbalances in baseline characteristics in the pre-
matching cohort were well balanced after propensity score
matching (Table 1). The propensity model had good dis-
criminatory ability and was well calibrated (c-statis-
tics = 0.74, Hosmer–Lemeshow goodness-of-fit test;
P = 0.26).
Effects of RASB on the risk of ESRD and composite
kidney outcome
During the median 5.1-year follow-up period, 130 patients
(10.2 %) developed ESRD and 156 patients (12.3 %) had
composite kidney outcome. Kaplan–Meier curves for
ESRD are shown in Supplementary Fig. 2. In unadjusted
analysis of all patients, there were no significant
Clin Exp Nephrol
123

differences in kidney survival between patients with RASB
and those without RASB (P = 0.83; Supplementary
Fig. 2a). On the contrary, in weighting analysis, use of
RASB was significantly associated with better renal prog-
nosis (P\ 0.001; Supplementary Fig. 2b).
Unadjusted and multivariable Cox models
Unadjusted Cox analysis did not show any significant
association between RASB therapy and either ESRD (HR
0.96; 95 % CI 0.68–1.36; P = 0.83) or composite kidney
Table 1 Baseline characteristics of subjects with or without RASB in an entire cohort and 404 pairs with or without RASB in a propensity score-
matched cohort
Characteristics Entire cohort (n = 1273) Propensity score-matched cohort (n = 808)
Use of RASB Standardized
differences
Use of RASB Standardized
differencesNo (n = 715) Yes (n = 558) No (n = 404) Yes (n = 404)
Age, years 31.4 (14.0) 39.8 (15.0) 0.582 36.6 (14.9) 36.2 (13.8) 0.030
Gender (male), % 43.5 48.6 0.102 47.5 47.3 0.005
Follow-up, years 5.8 (2.1–8.4) 7.1 (2.9–9.7) 0.261 5.7 (2.0–8.3) 7.5 (3.0–10.1) 0.359
Mean arterial pressure, mmHg 88.7 (13.1) 96.2 (14.5) 0.541 93.2 (13.5) 93.5 (14.1) 0.018
Serum albumin, g/dL 4.2 (0.5) 4.0 (0.6) 0.274 4.1 (0.57) 4.0 (0.54) 0.085
Serum total cholesterol, mg/dL 194.9 (48.6) 209.3 (46.4) 0.303 205.5 (53.2) 204.2 (45.3) 0.027
Serum triglycerides, mg/dL 113.8 (79.7) 143.2 (99.4) 0.326 129.5 (91.8) 132.6 (90.5) 0.035
Uric acid, mg/dL 5.6 (1.5) 6.0 (1.5) 0.28 5.8 (1.6) 5.8 (1.5) 0.018
Urinary protein excretion, g/24 h 1.1 (1.5) 1.6 (1.9) 0.33 1.4 (1.7) 1.5 (1.7) 0.062
Estimated glomerular filtration rate, mL/min/
1.73 m285.1 (31.6) 70.7 (27.0) 0.49 75.9 (28.7) 75.0 (28.0) 0.034
Pathologic parameters (Oxford classification), %
Mesangial hypercellularity score
M0 (B0.5 of glomeruli) 89.9 84.2 0.171 85.4 83.9 0.041
M1 ([0.5 of glomeruli) 10.1 15.8 14.6 16.1
Endocapillary hypercellularity
E0 (absence) 64.6 54.1 0.215 56.7 58.2 0.030
E1 (presence) 35.4 45.9 43.3 41.8
Segmental glomerulosclerosis
S0 (absence) 30.4 15.6 0.356 19.1 19.1 0.000
S1 (presence) 69.7 84.4 80.9 80.9
Tubular atrophy/interstitial fibrosis
T0 (B25 %) 75.3 72.1 0.082 73.8 74 0.005
T1 (26–50 %) 15.1 17.6 14.9 14.6
T2 ([50 %) 9.7 10.4 11.4 11.4
Extracapillary proliferation
Ex0 (absence) 47.7 28.7 0.399 35.4 34.2 0.026
Ex1 (presence) 52.3 71.3 64.6 65.8
Use of oral corticosteroid
No 74.3 55.7 0.396 63.4 63.4 0.000
Yes 25.7 44.3 36.6 36.6
Use of methylprednisolone pulse
No 91.9 79.2 0.367 87.1 85.9 0.036
Yes 8.1 20.8 12.9 14.1
Tonsillectomy
No 92.7 88.9 0.133 91.1 91.1 0.000
Yes 7.3 11.1 8.9 8.9
Values are given as mean (standard deviation) or as percentages. Duration of follow-up is shown as the median (interquartile range)
RASB renin-angiotensin system blockade
Clin Exp Nephrol
123

outcome (HR 1.08; 95 % CI 0.79–1.49; P = 0.62)
(Table 2). With the subsequent multivariable Cox propor-
tional hazard model, the use of RASB was independently
associated with reduced risk of developing ESRD (HR
0.53; 95 % CI 0.36–0.79; P = 0.002) and composite kid-
ney outcome (HR 0.60; 95 % CI 0.42–0.85; P = 0.005)
(Table 2).
Propensity score-adjusted models
Significant associations were verified between RASB and
better renal prognosis using Cox proportional hazard
models adjusted using the IPTW method (HR 0.58; 95 %
CI 0.42–0.80; P\ 0.001 for primary outcome, and HR
0.66; 95 % CI 0.49–0.89; P = 0.006 for secondary out-
come) (Table 2). Multivariable Cox proportional hazard
models adjusted for propensity score-based regression and
stratification on quintiles of propensity score showed a
significant association between RASB and lower risk for
both ESRD (HR 0.56; 95 % CI 0.39–0.81; P = 0.002 for
propensity score-adjusted regression, and HR 0.58; 95 %
CI 0.40–0.84; P = 0.004 for propensity score-based strat-
ification) and composite kidney outcome (HR 0.65; 95 %
CI 0.46–0.91; P = 0.013 for propensity score-adjusted
regression, and HR 0.68; 95 % CI 0.48–0.96; P = 0.026
for propensity score-based stratification) (Table 2). Simi-
larly, propensity score matching also showed a significant
association between RASB therapy and better renal
outcome (HR 0.50; 95 % CI 0.27–0.91; P = 0.024 for
primary outcome, and HR 0.51; 95 % CI 0.29–0.91;
P = 0.022 for secondary outcome) (Table 2). Therefore,
after adjustment using these four different propensity
score-adjusted methods (IPTW, regression, stratification,
matching method), significant findings in favor of RASB
therapy for lower incidence of ESRD and composite kid-
ney outcome were confirmed (Table 2).
Sensitivity analysis
To evaluate the potential impact of pediatric patients
included in our cohort, we conducted a sensitivity analysis
of the population of 1142 adults, excluding children less
than 18 years of age. As shown in Table 2, neither sensi-
tivity analysis changed the essential findings in the present
study.
Subgroup analysis stratified by baseline
characteristics
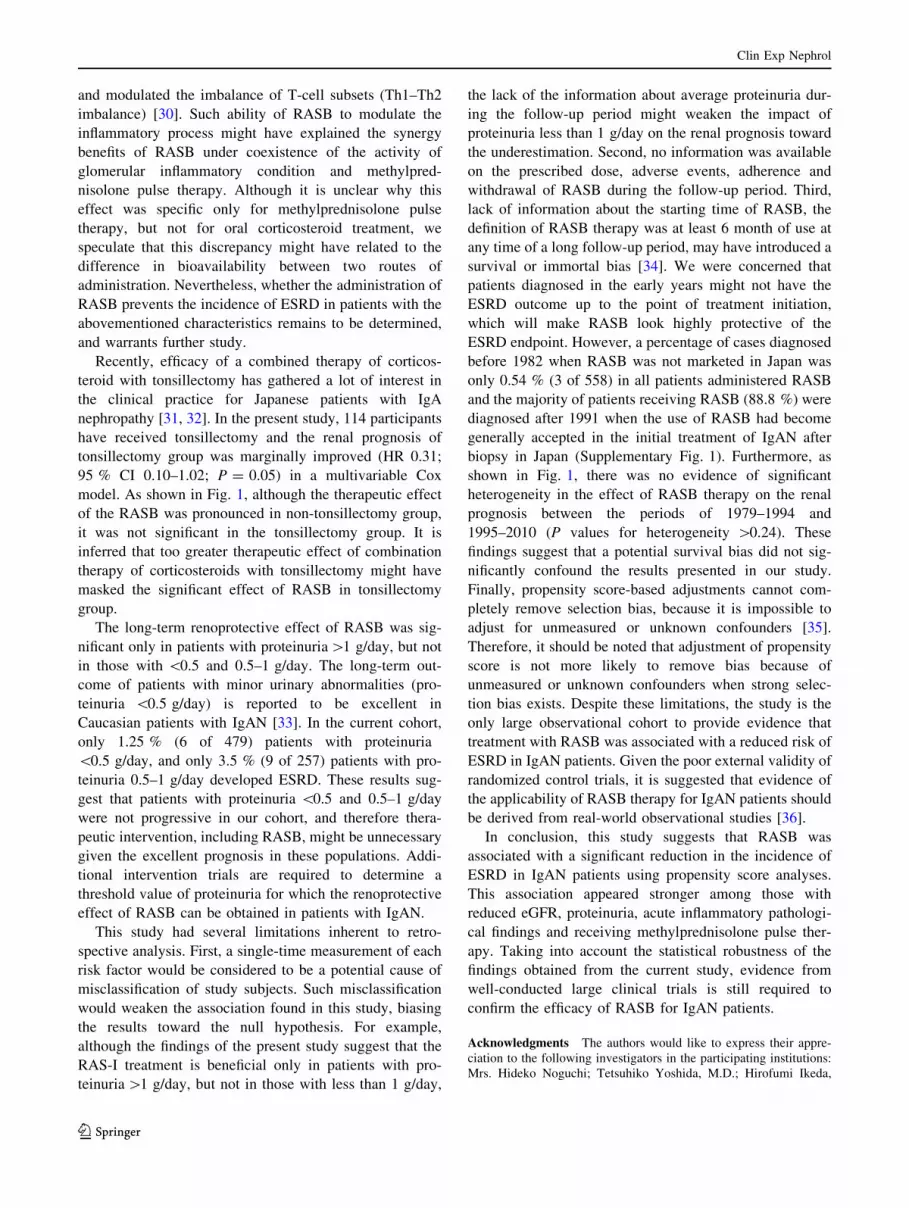
To assess the interaction between the renoprotective effect
of RASB and patient characteristics, the effect of modifi-
cation in subgroups stratified by potential confounders and
treatment assignment were examined (Fig. 1). Significant
interactions were observed in patients C35 years, with
hypertension, and with reduced eGFR (\60 mL/min/
1.73 m2) and the pathological parameters of the Oxford
Table 2 Association between treatment with RASB and the development of ESRD and composite kidney outcome
Model ESRD Composite kidney
outcome
HR (95 % CI) P value HR (95 % CI) P value
Unadjusted model (n = 1273) 0.96 (0.68–1.36) 0.83 1.08 (0.79–1.49) 0.62
Multivariable Cox model (n = 1273)a 0.54 (0.36–0.79) 0.002 0.60 (0.43–0.86) 0.005
Propensity score-adjusted models
PS-adjusted regression model (n = 1273)a 0.56 (0.39–0.81) 0.002 0.65 (0.46–0.91) 0.013
PS-stratification (n = 1273)a 0.58 (0.40–0.84) 0.004 0.68 (0.48–0.96) 0.026
PS-matched model (1:1, n = 808)a 0.50 (0.27–0.91) 0.024 0.51 (0.29–0.91) 0.022
IPTW model (n = 1273)a 0.58 (0.42–0.80) \0.001 0.66 (0.49–0.89) 0.006
Sensitivity analysis
Patients C 18 years (n = 1142)a 0.52 (0.35–0.77) 0.001 0.59 (0.41–0.84) 0.004
Population excluding subjects with an observation period of less than 12 months
(n = 1179)a0.59 (0.42–0.81) 0.001 0.67 (0.50–0.90) 0.008
Population excluding patients diagnosed in the early time period before 1982
(n = 1250)a0.65 (0.46–0.91) 0.012 0.74 (0.54–1.00) 0.052
a Adjusted for baseline characteristics (age, sex, mean arterial pressure, serum albumin, serum total cholesterol, serum triglycerides, uric acid,
urinary protein excretion, estimated glomerular filtration rate, mesangial hypercellularity score, endocapillary hypercellularity, segmental
glomerulosclerosis, tubular atrophy/interstitial fibrosis and extracapillary proliferation) and therapeutic interventions (intravenous methylpred-
nisolone pulse therapy, oral corticosteroid and tonsillectomy)
CI confidence interval, ESRD end-stage renal disease, HR hazard ratio, PS propensity score, IPTW inverse probability of treatment weighting,
RASB renin–angiotensin system blockade
Clin Exp Nephrol
123

classification (M, S) (P for interaction \0.05; Fig. 1). In
addition, the association between RASB and ESRD tended
to be greater in those with proteinuria (C1.0 g/24 h), Ex
and receiving methylprednisolone pulse therapy than in
those without these factors (P for interaction \0.10;
Fig. 1).
Subgroup analysis stratified by urinary protein
excretion levels
The renoprotective effect of RASB in patients with urine
protein excretion levels \0.5, 0.5–1 and [1 g/day at
presentation were compared in a propensity score-
weighting cohort. After adjustment using IPTW, the long-
term renoprotective effect of RASB was only found to be
significant in patients with proteinuria [1 g/day
(P\ 0.001). There was no significant evidence of the
renoprotective effect of RASB in both subgroups with
proteinuria \0.5 and 0.5–1 g/day (P = 0.52 and 0.64,
respectively) (Fig. 2).
Discussion
The results of this propensity score-based analysis showed
that treatment of IgAN patients with RASB was associated
with a significant reduction in the risk of ESRD compared
with patients who did not receive RASB. Importantly, the
findings suggest that RASB had a favorable clinical effect
on ‘‘hard’’ endpoint, such as ESRD, in the real-world
practice of IgAN. Additionally, in subgroup analysis, the
beneficial effect of RASB was stronger in patients aged
C35, with hypertension, reduced eGFR (\60 mL/min/
1.73 m2), proteinuria (C1.0 g/24 h), with pathological
parameters of the Oxford classification (M, S), Ex and
receiving methylprednisolone pulse therapy compared with
those patients without such clinical backgrounds. It is
proposed that these results suggest the effectiveness of
RASB against the development of ESRD, and go some way
to provide supporting evidence identifying the optimal
therapeutic target population for RASB treatment in IgAN
patients.
Age54 689 0.64776 584 <0.001
Sex60 691 0.02670 582 0.002
Time period88 489 0.001 42 784 0.220
Hypertension72 943 0.05658 330 <0.001
Proteinuria15 736 0.908
115 636 <0.001Reduced eGFR
44 934 0.87186 339 <0.001
Mesangial hypercellularity score88 1113 0.05742 160 <0.001
Endocapillary hypercellularity84 764 <0.00146 509 0.039
Segmental glomerulosclerosis11 304 0.124
119 969 <0.001Tubular atrophy/interstitial fibrosis
54 940 0.01338 206 0.04838 127 0.015
Extracapillary proliferation34 501 0.44096 772 <0.001
Use of oral corticosteroid93 842 0.00137 431 0.074
Methylpredonisolone puls therapy117 1099 0.00113 174 0.006
P value
effect interaction
ESRDNo. ofEventsVariable HR (95% CI)No. of
Patients
<0.001Older (≥35 years) 0.30 (0.19-0.47)
Women 0.58 (0.36-0.94) 0.63Men
Younger (<35 years) 1.13 (0.68-1.87)
0.49 (0.32-0.77)
Early period (1979-1994) 0.50 (0.33-0.76)
0.32 (0.21-0.49)
0.51 (0.34-0.76)
Late period (1995-2010) 0.71 (0.41-1.23)
Absence 0.65 (0.42-1.01)Presence 0.37 (0.23-0.61)
E0 (Absence)
0.03
<0.001
0.02
0.24
S1 (Presence)
M1 (>0.5 of glomeruli)
0.39 (0.27-0.55)
T2 (>50%) 0.46 (0.24-0.86)T1 (26-50%) 0.52 (0.28-0.99)T0 (<25%) 0.55 (0.34-0.88)
0.47 (0.33-0.66)
0.56 (0.32-0.97)E1 (Presence)
S0 (Absence) 2.84 (0.75-10.8)
Ex0 (Absence) 0.79 (0.44-1.44)
Yes 0.58 (0.32-1.06)
No
Absence (<1.0 g/24 hr) 0.91 (0.37-2.43)Presence (≥1.0 g/24 hr)
0.67 (0.45-1.01)0.32 (0.18-0.56)
M0 (≤0.5 of glomeruli)
Absence (≥60 mL/min/1.73 m2) 1.05 (0.59-1.85)Presence (<60 mL/min/1.73 m2)
Yes 0.24 (0.09-0.66)
Ex1 (Presence) 0.46 (0.32-1.06)
No 0.52 (0.35-0.77)
0.57 (0.41-0.81)
0.02
0.61
0.08
0.89
0.07
0.77
0.01
HR (95% CI)
decreasein risk
increasein risk
126 1156 <0.0014 111 0.498
NoYes 2.58 (0.17-39.9)
0.52 (0.37-0.72) 0.24
Tonsillectomy
0.10 1.00 10.00 100.0
Fig. 1 Propensity-weighted
hazard ratios and 95 %
confidence intervals for the
effect of RASB therapy on the
incidence of ESRD according to
subgroups of baseline
characteristics and treatment
assignment. Hypertension was
defined as systolic blood
pressure C140 mmHg and
diastolic blood pressure
C90 mmHg. A propensity-
weighted Cox proportional
hazards model was adjusted for
baseline characteristics (age,
sex, mean arterial pressure,
serum albumin, serum total
cholesterol, serum triglycerides,
uric acid, urinary protein
excretion, estimated glomerular
filtration rate, mesangial
hypercellularity score,
endocapillary hypercellularity,
segmental glomerulosclerosis,
tubular atrophy/interstitial
fibrosis and extracapillary
proliferation) and therapeutic
interventions (intravenous
methylprednisolone pulse
therapy, oral corticosteroid and
tonsillectomy). CI confidence
interval, eGFR estimated
glomerular filtration rate, ESRD
end-stage renal disease, HR
hazard ratio, RASB renin–
angiotensin system blockade
Clin Exp Nephrol
123

There are several reports about the impact of RASB on
short-term benefits in patients with IgAN [4–7]. Two pub-
lished systematic reviews evaluated the kidney protective
effects of RASB in patients with IgAN [6, 7]. However, the
definition of renal function decline was different in each
study, and the studies did not include patient characteristics,
so the optimal therapeutic target population of RASB
remained unclear. To the best of the authors’ knowledge, the
present study is the first investigation to adopt a clear and
uniform definition of ‘‘hard’’ renal outcome (i.e., ESRD), and
to assess the renoprotective effect of RASB in subgroups
stratified according to the patients’ backgrounds.
The strengths of this study are its large number of par-
ticipants and the use of rigorous statistical methodologies
for evaluating the association between RASB use and renal
outcome, such as the propensity score-based approach. The
IPTW method is a better statistical technique for adjusting
differences in characteristics and reducing selection bias
than is normal multivariable regression [24]. The advan-
tages of this rigorous method are that it allows a direct non-
randomized comparison of treatment effect between two
populations, and theoretically allows all data from two
groups to be used. Consistency in results between IPTW
adjustment and several other propensity-adjusted methods
was confirmed.
The synergic effect of RASB was not evident in patients
with less than 35 years, without hypertension or preserved
eGFR ([60 mL/min/1.73 m2). These results may reflect
that patients with younger, well-controlled blood pressure
or preserved eGFR did not progress to ESRD, which might
result in poor statistical power due to insufficient number
of event onset. The benefit of RASB therapy was signifi-
cantly evident not only in patients with chronic lesion,
including segmental sclerosis, but also in those with acute
inflammatory pathological findings, such as mesangial
proliferation or extracapillary proliferation.
These results indicate that the effect of RASB might be
more prominent in the active glomerular inflammatory
state rather than in advanced chronic renal fibrosis. One
possible cause of these interactions may be the anti-in-
flammatory properties of RASB [25]. Growing evidences
in many in vitro and in vivo inflammation models indicate
that angiotensin (AT) II is a potential pro-inflammatory
mediator associated with the growth and tissue remodeling
action [25, 26]. Activation of AT1 receptor results in
nuclear factor (NF)-j B activation, which plays a central
role in the production of various inflammatory cytokines,
such as TNF-a, IL-6, IL-8 and TGF-b [27]. Several human
studies reported that interruption of AT II activity by
RASB reduced the IL-1 and IL-6 concentration [28, 29],
Proteinuria <0.5 g/day, n = 479
No Use of RASBUse of RASB
Proteinuria 0.5-1.0 g/day, n = 257
No Use of RASBUse of RASB
Follow-up duration (months)50 100 150 200 250
Cum
ulat
ive
kidn
ey s
urvi
val,
% 1.0
0.2
0.4
0.6
0.8
0 Cum
ulat
ive
kidn
ey s
urvi
val,
%
1.0
0.2
0.4
0.6
0.8
0
Cum
ulat
ive
kidn
ey s
urvi
val,
%
1.0
0.2
0.4
0.6
0.8
0
Follow-up duration (months)50 100 150 200 250
Proteinuria >1.0 g/day, n = 537
Follow-up duration (months)50 100 150 200 250
No Use of RASBUse of RASB
P = 0.36
P <0.001
P = 0.64
a b
c
330 174 79 33 15 5149 85 52 25 10 5
RASB (-)RASB (+)
142 87 48 23 10 3115 69 45 26 16 9
RASB (-)RASB (+)
243 119 60 23 6 3294 218 100 36 17 9
RASB (-)RASB (+)
Fig. 2 Adjusted Kaplan–Meier
plots for ESRD with inverse
probability weights among the
subgroups stratified by different
severities of proteinuria.
Adjusted Kaplan–Meier plots in
patients with proteinuria
\0.5 g/day (a), 0.5–1.0 g/day
(b) and[1.0 g/day (c) are
shown. ESRD end-stage renal
disease, RASB renin–
angiotensin system blockade
Clin Exp Nephrol
123
and modulated the imbalance of T-cell subsets (Th1–Th2
imbalance) [30]. Such ability of RASB to modulate the
inflammatory process might have explained the synergy
benefits of RASB under coexistence of the activity of
glomerular inflammatory condition and methylpred-
nisolone pulse therapy. Although it is unclear why this
effect was specific only for methylprednisolone pulse
therapy, but not for oral corticosteroid treatment, we
speculate that this discrepancy might have related to the
difference in bioavailability between two routes of
administration. Nevertheless, whether the administration of
RASB prevents the incidence of ESRD in patients with the
abovementioned characteristics remains to be determined,
and warrants further study.
Recently, efficacy of a combined therapy of corticos-
teroid with tonsillectomy has gathered a lot of interest in
the clinical practice for Japanese patients with IgA
nephropathy [31, 32]. In the present study, 114 participants
have received tonsillectomy and the renal prognosis of
tonsillectomy group was marginally improved (HR 0.31;
95 % CI 0.10–1.02; P = 0.05) in a multivariable Cox
model. As shown in Fig. 1, although the therapeutic effect
of the RASB was pronounced in non-tonsillectomy group,
it was not significant in the tonsillectomy group. It is
inferred that too greater therapeutic effect of combination
therapy of corticosteroids with tonsillectomy might have
masked the significant effect of RASB in tonsillectomy
group.
The long-term renoprotective effect of RASB was sig-
nificant only in patients with proteinuria[1 g/day, but not
in those with \0.5 and 0.5–1 g/day. The long-term out-
come of patients with minor urinary abnormalities (pro-
teinuria \0.5 g/day) is reported to be excellent in
Caucasian patients with IgAN [33]. In the current cohort,
only 1.25 % (6 of 479) patients with proteinuria
\0.5 g/day, and only 3.5 % (9 of 257) patients with pro-
teinuria 0.5–1 g/day developed ESRD. These results sug-
gest that patients with proteinuria \0.5 and 0.5–1 g/day
were not progressive in our cohort, and therefore thera-
peutic intervention, including RASB, might be unnecessary
given the excellent prognosis in these populations. Addi-
tional intervention trials are required to determine a
threshold value of proteinuria for which the renoprotective
effect of RASB can be obtained in patients with IgAN.
This study had several limitations inherent to retro-
spective analysis. First, a single-time measurement of each
risk factor would be considered to be a potential cause of
misclassification of study subjects. Such misclassification
would weaken the association found in this study, biasing
the results toward the null hypothesis. For example,
although the findings of the present study suggest that the
RAS-I treatment is beneficial only in patients with pro-
teinuria[1 g/day, but not in those with less than 1 g/day,
the lack of the information about average proteinuria dur-
ing the follow-up period might weaken the impact of
proteinuria less than 1 g/day on the renal prognosis toward
the underestimation. Second, no information was available
on the prescribed dose, adverse events, adherence and
withdrawal of RASB during the follow-up period. Third,
lack of information about the starting time of RASB, the
definition of RASB therapy was at least 6 month of use at
any time of a long follow-up period, may have introduced a
survival or immortal bias [34]. We were concerned that
patients diagnosed in the early years might not have the
ESRD outcome up to the point of treatment initiation,
which will make RASB look highly protective of the
ESRD endpoint. However, a percentage of cases diagnosed
before 1982 when RASB was not marketed in Japan was
only 0.54 % (3 of 558) in all patients administered RASB
and the majority of patients receiving RASB (88.8 %) were
diagnosed after 1991 when the use of RASB had become
generally accepted in the initial treatment of IgAN after
biopsy in Japan (Supplementary Fig. 1). Furthermore, as
shown in Fig. 1, there was no evidence of significant
heterogeneity in the effect of RASB therapy on the renal
prognosis between the periods of 1979–1994 and
1995–2010 (P values for heterogeneity [0.24). These
findings suggest that a potential survival bias did not sig-
nificantly confound the results presented in our study.
Finally, propensity score-based adjustments cannot com-
pletely remove selection bias, because it is impossible to
adjust for unmeasured or unknown confounders [35].
Therefore, it should be noted that adjustment of propensity
score is not more likely to remove bias because of
unmeasured or unknown confounders when strong selec-
tion bias exists. Despite these limitations, the study is the
only large observational cohort to provide evidence that
treatment with RASB was associated with a reduced risk of
ESRD in IgAN patients. Given the poor external validity of
randomized control trials, it is suggested that evidence of
the applicability of RASB therapy for IgAN patients should
be derived from real-world observational studies [36].
In conclusion, this study suggests that RASB was
associated with a significant reduction in the incidence of
ESRD in IgAN patients using propensity score analyses.
This association appeared stronger among those with
reduced eGFR, proteinuria, acute inflammatory pathologi-
cal findings and receiving methylprednisolone pulse ther-
apy. Taking into account the statistical robustness of the
findings obtained from the current study, evidence from
well-conducted large clinical trials is still required to
confirm the efficacy of RASB for IgAN patients.
Acknowledgments The authors would like to express their appre-
ciation to the following investigators in the participating institutions:
Mrs. Hideko Noguchi; Tetsuhiko Yoshida, M.D.; Hirofumi Ikeda,
Clin Exp Nephrol
123

M.D., Ph.D.; Takashi Inenaga, M.D.; Akinori Nagashima, M.D.,
Ph.D.; Tadashi Hirano, M.D.; and Koji Mitsuiki, M.D., Ph.D.
Compliance with ethical standards
Conflict of interest Honoraria: Takanari Kitazono (Bayer Phar-
maceutical Co., Bristol-Myers Squibb Co., Daiichi-Sankyo Co.),
Kazuhiko Tsuruya (Chugai Pharmaceutical Co., Kyowa Hakko Kirin
Co.).
Research funding: Takanari Kitazono (Astellas Pharma Inc., Daiichi-
Sankyo Co., Eisai Co., Kyowa Hakko Kirin Co., Mitsubishi Tanabe
Pharma Co., MSD K.K., Ono Pharmaceutical Co., Otsuka Pharma-
ceutical Co., Sanofi-Aventis Pharmaceutical Co., Takeda Pharma-
ceutical Co.), Kazuhiko Tsuruya (Chugai Pharmaceutical Co., Kyowa
Hakko Kirin Co., Otsuka Pharmaceutical Co., Takeda Pharmaceutical
Co.)
Endowed department: Kazuhiko Tsuruya (Baxter)
Disclosure The authors declare that they have no relevant financial
interests.
References
1. Lv J, Zhang H, Zhou Y, Li G, Zou W, Wang H. Natural history of
immunoglobulin A nephropathy and predictive factors of prog-
nosis: a long-term follow up of 204 cases in China. Nephrol
Carlton. 2008;13:242–6.
2. D’Amico G. The commonest glomerulonephritis in the world:
IgA nephropathy. Q J Med. 1987;64:709–27.
3. Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis
JB, et al. Renoprotective effect of the angiotensin-receptor
antagonist irbesartan in patients with nephropathy due to type 2
diabetes. N Engl J Med. 2001;345:851–60.
4. Praga M, Gutierrez E, Gonzalez E, Morales E, Hernandez E.
Treatment of IgA nephropathy with ACE inhibitors: a random-
ized and controlled trial. J Am Soc Nephrol. 2003;14:1578–83.
5. Woo KT, Lau YK, Zhao Y, Liu FE, Tan HB, Tan EK, et al.
Disease progression, response to ACEI/ATRA therapy and
influence of ACE gene in IgA nephritis. Cell Mol Immunol.
2007;4:227–32.
6. Cheng J, Zhang W, Zhang XH, He Q, Tao XJ, Chen JH. ACEI/
ARB therapy for IgA nephropathy: a meta analysis of randomised
controlled trials. Int J Clin Pract. 2009;63:880–8.
7. Reid S, Cawthon PM, Craig JC, Samuels JA, Molony DA,
Strippoli GF. Non-immunosuppressive treatment for IgA
nephropathy. Cochrane Database Syst Rev 2011:CD003962.
8. KDIGO Working Group. KDIGO clinical practice guideline for
glomerulonephritis. Kidney Int. 2012;Suppl 2:139–274.
9. Imai E, Horio M, Nitta K, Yamagata K, Iseki K, Hara S, et al.
Estimation of glomerular filtration rate by the MDRD study
equation modified for Japanese patients with chronic kidney
disease. Clin Exp Nephrol. 2007;11:41–50.
10. Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al.
Revised equations for estimated GFR from serum creatinine in
Japan. Am J Kidney Dis. 2009;53:982–92.
11. Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A. A simple
estimate of glomerular filtration rate in children derived from body
length and plasma creatinine. Pediatrics. 1976;58:259–63.
12. Schwartz GJ, Brion LP, Spitzer A. The use of plasma creatinine
concentration for estimating glomerular filtration rate in infants,
children, and adolescents. Pediatr Clin North Am.
1987;34:571–90.
13. Jafar TH, Stark PC, Schmid CH, Landa M, Maschio G, Mar-
cantoni C, et al. Proteinuria as a modifiable risk factor for the
progression of non-diabetic renal disease. Kidney Int.
2001;60:1131–40.
14. Yamamoto Y, Hiki Y, Nakai S, Yamamoto K, Takahashi K,
Koide S, et al. Comparison of effective impact among tonsil-
lectomy alone, tonsillectomy combined with oral steroid and with
steroid pulse therapy on long-term outcome of immunoglobulin A
nephropathy. Clin Exp Nephrol. 2013;17:218–24.
15. Katafuchi R, Ninomiya T, Mizumasa T, Ikeda K, Kumagai H,
Nagata M, et al. The improvement of renal survival with steroid
pulse therapy in IgA nephropathy. Nephrol Dial Transplant.
2008;23:3915–20.
16. Cattran DC, Coppo R, Cook HT, Feehally J, Roberts IS, Troy-
anov S, et al. The Oxford classification of IgA nephropathy:
rationale, clinicopathological correlations, and classification.
Kidney Int. 2009;76:534–45.
17. D’Agostino RB Jr. Propensity score methods for bias reduction in
the comparison of a treatment to a non-randomized control group.
Stat Med. 1998;17:2265–81.
18. Barnieh L, James MT, Zhang J, Hemmelgarn BR. Propensity
score methods and their application in nephrology research.
J Nephrol. 2011;24:256–62.
19. Robins JM, Hernan MA, Brumback B. Marginal structural
models and causal inference in epidemiology. Epidemiology.
2000;11:550–60.
20. Linden A, Adams JL. Evaluating health management pro-
grammes over time: application of propensity score-based
weighting to longitudinal data. J Eval Clin Pract. 2010;16:180–5.
21. Austin PC. An introduction to propensity score methods for
reducing the effects of confounding in observational studies.
Multivar Behav Res. 2011;46:399–424.
22. Lin DY, Wei LJ. The robust inference for the Cox proportional
hazards model. J Am Stat Assoc. 1989;84:1074–8.
23. Cole SR, Hernan MA. Adjusted survival curves with inverse
probability weights. Comput Methods Progr Biomed.
2004;75:45–9.
24. Austin PC. The performance of different propensity score
methods for estimating marginal hazard ratios. Stat Med.
2013;32:2837–49.
25. Dagenais NJ, Jamali F. Protective effects of angiotensin II
interruption: evidence for antiinflammatory actions. Pharma-
cotherapy. 2005;25:1213–29.
26. Wolf G. Renal injury due to renin-angiotensin-aldosterone sys-
tem activation of the transforming growth factor-beta pathway.
Kidney Int. 2006;70:1914–9.
27. Niimi R, Nakamura A, Yanagawa Y. Suppression of endotoxin-
induced renal tumor necrosis factor-alpha and interleukin-6
mRNA by renin–angiotensin system inhibitors. Jpn J Pharmacol.
2002;88:139–45.
28. Trevelyan J, Brull DJ, Needham EW, Montgomery HE, Morris A,
Mattu RK. Effect of enalapril and losartan on cytokines in
patients with stable angina pectoris awaiting coronary artery
bypass grafting and their interaction with polymorphisms in the
interleukin-6 gene. Am J Cardiol. 2004;94:564–9.
29. Sironi L, Gelosa P, Guerrini U, Banfi C, Crippa V, Brioschi M,
et al. Anti-inflammatory effects of AT1 receptor blockade pro-
vide end-organ protection in stroke-prone rats independently
from blood pressure fall. J Pharmacol Exp Ther.
2004;311:989–95.
30. Shao J, Nangaku M, Miyata T, Inagi R, Yamada K, Kurokawa K,
et al. Imbalance of T-cell subsets in angiotensin II-infused hyper-
tensive rats with kidney injury. Hypertension. 2003;42:31–8.
31. Kawamura T, Yoshimura M, Miyazaki Y, Okamoto H, Kimura
K, Hirano K, et al. A multicenter randomized controlled trial of
tonsillectomy combined with steroid pulse therapy in patients
with immunoglobulin A nephropathy. Nephrol Dial Transplant.
2014;29:1546–53.
Clin Exp Nephrol
123

32. Miura N, Imai H, Kikuchi S, Hayashi S, Endoh M, Kawamura T,
et al. Tonsillectomy and steroid pulse (TSP) therapy for patients
with IgA nephropathy: a nationwide survey of TSP therapy in
Japan and an analysis of the predictive factors for resistance to
TSP therapy. Clin Exp Nephrol. 2009;13:460–6.
33. Gutierrez E, Zamora I, Ballarin JA, Arce Y, Jimenez S, Quereda
C, et al. Long-term outcomes of IgA nephropathy presenting with
minimal or no proteinuria. J Am Soc Nephrol. 2012;23:1753–60.
34. Shariff SZ, Cuerden MS, Jain AK, Garg AX. The secret of
immortal time bias in epidemiologic studies. J Am Soc Nephrol.
2008;19:841–3.
35. Sturmer T, Joshi M, Glynn RJ, Avorn J, Rothman KJ, Sch-
neeweiss S. A review of the application of propensity score
methods yielded increasing use, advantages in specific settings,
but not substantially different estimates compared with conven-
tional multivariable methods. J Clin Epidemiol. 2006;59:437–47.
36. Steg PG, Lopez-Sendon J, Lopez de Sa E, Goodman SG, Gore
JM, Anderson FA Jr, et al. External validity of clinical trials in
acute myocardial infarction. Arch Intern Med. 2007;167:68–73.
Clin Exp Nephrol
123





























