Embed Size (px)
Citation preview
Kidney International, Vol. 50 (1996), PP. 1990—2001
Urinary IL-6/EGF ratio: A useful prognostic marker for theprogression of renal damage in IgA nephropathy
ELENA RANIERI, LORETO GESUALDO, FRANCESCO PETRARULO, and FRANCESCO P. SCHENA
institute of Nephrology, University of Bad, Polyclinic, Bad, and Nephrology Unit, Altamura Hospital, Altamura, Italy
Urinary LL-6/EGF ratio: A useful prognostic marker for the progressionof renal damage in IgA nephropathy. Interleukin 6 (IL-6) is produced byhuman mesangial and tubular cells, and its urinary levels has beenproposed as a marker of mesangial proliferation and tubulointerstitialdamage. Epidermal growth factor (EGF) is expressed within the Henle'sloop and the distal tubule and has been shown to accelerate recovery fromrenal injury. In the present study we have defined renal gene and proteinexpression of IL-6 and EGF in 10 normal, 10 nonproliferative glomeru-lonephritis (NPGN) and 30 IgA nephropathy (IgAN) human kidneys byRT-PCR, in situ hybridization and immunohistochemical techniques.Moreover, urinary IL-6 and EGF levels were measured in 41 patients withIgAN and in 20 normal subjects (N). In normal kidneys, EGF waslocalized in Henle's loop and distal convoluted tubule whereas IL-6 wasmainly located in the proximal tubule and, less, within the glomerulus. InIgAN patients, EGF was decreased whereas IL-6 expression was up-regulated. These modifications paralleled the degree of tubulointerstitialdamage. Moreover, IgAN patients as a whole exhibited a reduction ofEGF and an increase of IL-fl urinary concentration (EGF values: N,12.96 1.15; IgAN Grades 1—2, 20.05 2.64; Grades 3—4, 7.60 1.70;Grade 5, 3.14 0.71, ng/mg urinary creatinine. IL-6 values: N, 2.040.51; IgAN Grades 1—2, 3.26 0.38; Grades 3—4, 5.67 0.92; Grade 5,27.20 9.70 pg/mg urinary creatinine), that correlated with the degree ofhistological lesions, the presence of hypertension and serum creatininelevel. Interestingly, patients with the highest urinary IL-6/EGF ratioshowed a worse evolution in a three year follow-up. In conclusion, ourdata show that: (1) renal IL-6 and EGF expression are strictly correlatedto the degree of tubulointerstitial damage; and (2) urinary IL-6/EGF ratiomight be a valuable prognostic marker for the progression of the renaldamage in IgAN.
IgA nephropathy (IgAN) is a chronic mesangioproliferativeglomerulonephritis (GN) characterized by the predominance ofgranular and electron dense deposits of IgA, and frequently, C3 inthe glomerulus [1]. It has a variable course and leads to end-stagerenal disease (ESRD) in a substantial number of cases [1]. Lee,Rao and Franklin [21 observed that histologic grading at the initialrenal biopsy may be a useful prognostic indicator of the clinicaloutcome of IgAN. Indeed, it has been demonstrated that onlypatients with moderate to severe histologic lesions develop ESRD[1,21.
In the recent years several lines of evidence have pointed outthat histopathological changes within the tubulointerstitial com-partment promote the progression of renal damage, regardless ofits original disease process [reviewed in 3—6]. The extent of the
interstitial infiltrate, which consists largely of T cells and macro-phages, correlates with the degree of functional impairment and isa good predictor of long-term prognosis [3].
Several investigations showed that cultured tubular cells syn-thetize and secrete, both constitutively and inducibly, an array ofpeptides which stimulate cell trophism and proliferation (growthfactors), chemoattraction (chemokines), and modulate vessel tone(vasoactive peptides) [reviewed in 4—9]. Fine, Ong and Torman[5] hypothesized that protein overload in the glomerular ultrafil-trate or hypertension-induced microvascular ischemia may causetubular injury, which in turn induces an up- or a down-regulationof the above peptides. Therefore, we decided to focus ourattention on two cytokines, namely interleukin-6 (IL-6) andepidermal growth factor (EGF), that have been implicated in theprogression of renal damage and in the repair process [10—18].
At the renal level, glomerular mesangial and tubular epithelialcells express and secrete IL-6 [10, 19, 20]. Mesangial hyperpro-duction of IL-6, induced by phlogistic stimuli, seems to beresponsible, at least in part, for the proliferative histologic lesionsobserved in mesangioproliferative GN [10]. Moreover, an in-crease in renal IL-6 expression and urine concentration correlatewith mesangial proliferation, tubular atrophy and the intensity ofinterstitial cellular infiltrates, thus supporting a role for thiscytokine in the progression of renal damage [10—15].
On the other hand, EGF produced by the ascending portion ofHenle's loop and the distal convoluted tubule is a peptide thatseems to modulate tissue repair [16—18]. A reduction of the renalEGF expression and its urinary concentration has been reportedduring acute tubular injury [21—26]. Finally, a glomerular up-regulation of EGF-receptor (EGF-R) occurs in human mesangio-proliferative glomerulonephritis (MPGN), which indirectly sug-gests a pathogenetic involvement of the EGF/EGF-R loop inrenal damage [27].
In the present study we evaluated the renal gene expression andprotein synthesis of IL-6 and EGF, and measured urinary IL-6and EGF concentration in a chronic form of GN, namely IgAN.Furthermore, we correlated renal cytokine expression and urinaryIL-6/EGF ratio with serological (serum creatinine), urinary (pro-teinuria), and histopathological (glomerular and tubular intersti-tial damage) findings of this disease.
MethodsReceived for publication December 8, 1995and in revised form July 8, 1996Accepted for publication July 10, 1996
© 1996 by the International Society of Nephrology
Patients
Forty-one patients with biopsy-proven primary IgAN (27 malesand 14 females) gave their informed consent and were enrolled
1990

Ranieri et al: Urinary IL-6/EGF ratio in IgA nephropathy 1991
into the study. Twenty healthy volunteers and 10 patients affectedby nonproliferative GN (NPGN; 5 minimal change disease, 5membranous nephropathy) strictly matched for sex and age werealso recruited as controls.
Diagnosis was made by renal biopsy and standard examinationof the cortical tissue by light microscopy and immunofluores-cence. As routinely performed in our institution, histologic diag-nosis of IgAN was also supplemented with a grading of diseaseseverity according to the classification in five classes described byLee et a! [2]. Briefly, Grade I showed mild glomerular changeswith occasional slight mesangial thickening (segmental) withouthypercellularity and no tubulointerstitial changes (mild GN). InGrade II, glomerular changes showing localized mesangial prolif-eration and sclerosis were found in less than half of the glomeruli.Small crescents were rarely observed and no tubulointerstitialchanges were present (minor GN). Grade III was characterized bydiffuse mesangial proliferation and thickening of the basal mem-brane with a focal and segmental distribution. Occasionally, smallcrescents and adhesions, as well as tubulointerstitial changes(focal interstitial edema and infiltrate) were observed. Tubularatrophy was rare (focal segmental GN). In Grade IV there was amarked diffuse mesangial proliferation and sclerosis. Crescentswere present in up to 45% of glomeruli. Partial or total glomer-ulosclerosis was frequent. Tubular atrophy, interstitial inflamma-tion and occasional interstitial foam cells were frequent findings(diffuse proliferative GN). Finally, Grade V was similar to GradeIV but the histologic lesions were more severe. Crescents werepresent in more than 45% of glomeruli (diffuse proliferative andscierosing GN). Conventionally, we defined the Grade 1-Grade 2(G1-G2) classes as mild and nonprogressive disease, G3-G4 asmoderate and potentially progressive disease, and G5 as severeand progressive disease.
Urine collection
At the time of biopsy, fresh urine samples were collected in themorning, centrifuged at 600 x g for five minutes and dialyzedthrice against sterile PBS for two hours at 4°C. Samples wereharvested from dialysis tubes (MWCO 5,000, Spectrum, LosAngeles, CA, USA) and frozen at —20°C until tested, Urinarystudies were performed in IgAN patients and normal controls.None of them had urinary tract infection at the time of the study.
Renal studies
Thirty out of 41 renal biopsies from IgAN patients (13 patientswere in classes G1-G2, 10 patients were grouped in classes G3-G4;7 patients were in G5 class), 10 renal biopsies from patientsaffected by nonproliferative GN, and 10 normal-appearing por-tions of kidneys removed for renal carcinoma, were adequate forimmunohistochemistry and in situ hybridization. Duplicate mea-surements of total renal cortex IL-6 mRNA were performed in 20patients affected by IgAN (7 patients in classes G1-G2; 7 patientsin classes G3-G4; 6 patients in the G5 class), as well as in 10patients affected by NPGN and 10 normal appearing portion ofkidneys removed for renal carcinoma.
Total RNA extraction
Kidney specimens from percutaneous biopsy or surgical ne-phrectomy were immediately frozen in liquid nitrogen until used.After taking cryostat sections for immunohistology and in situhybridization studies, frozen renal cortex was lysed in 500 jLl of
guanidine buffer and subsequently homogenized with an Ultra-Turrax T25 (Janke & Kunkel, Staufen, Germany). Total RNA wasextracted by the single-step method, using phenol and chloroform!isoamylalcohol as previously described [28], and then analyzed indenaturing gel of 1% agarose and 2.2 M formaldehyde in lxMOPS running buffer. All gels were stained with ethidium bro-mide to visualize 28S and 18S ribosomal RNA bands and toexclude degradation of RNA. Usually, 3 to 10 .rg of total RNAwere obtained from each biopsy.
RT-PCR assayOne microgram of total RNA was reverse-transcribed into
cDNA and then amplified by using the following set of primersspecific for IL-6, EGF or GAPDH:
IL-6sense 5'-ATG AAC TCC TFC TCC ACA AGC GC-3'antisense 5'-GAA GAG CCC TCA GGC TGG ACT G-3'EGFsense 5' GAT GGG TAC TGC CTC CAT GAT GG-3'antisense 5' GCG CAG 'ITC CCA CCA €TF CAG GTC TCG-3'GAPDHsense 5'-TGG TAT CGT GGA AGG ACT CAT GAC-3'antisense 5'-ATF CGT TGT CAT ACC AGG A-3'Twenty microliters of reverse transcription —reaction mixture
containing I g of total RNA, PCR buffer (10 m Tris-HC1, pH8.3, 50 mi KC1, 2.5 m'vi MgCI2), 1 mrvi dNTPS, 20 U RNasin, 2.5/LM oligo (dT) and 100 U Moloney murine leukemia virus(M-MLV) reverse transcriptase were incubated at 42°C for 30minutes, heated to 95°C for five minutes, and then quickly chilledon ice.
PCR was performed at a final concentration of 1 X PCR buffer,200 ILM dNTPS, 0.15 fLM ofeach primer, 1.25 U of AmpliTaq DNApolymerase (Perkin Elmer, Roche Molecular System, NJ, USA),in a total volume of 50 d. The amplification profile involveddenaturation at 95°C for 30 seconds, primer annealing andextension at 60°C for one minute. For semiquantitative analysis,aliquots (10 1itl) were taken after different numbers of cycles(20-30-40) to establish the amplification plateau. Thirty cycles wasfound to be the best amplification profile able to recognizedifferences between samples. Therefore, all samples were ampli-fied for 30 cycles and then were electrophoresed in 1.5% agarosegels in Tris borate!EDTA buffer. Gels were stained with ethidiumbromide and photographed. All signals obtained were normalizedto the mRNA levels of GAPDH, a housekeeping gene, andexpressed as a ratio.
Southern blot analysis
To confirm the specificity of PCR products, 1 d of theamplified cDNA was electrophoresed on 1.5% agarose gel, blot-ted onto a nylon membrane (Schleicher & Schuell, Dassel,Germany) and crosslinked by exposure to UV light. After prehy-bridization, the filter was hybridized with fluorescein labeledeDNA probes (ECL Random Prime Labeling System; Amersham,UK) specific for human IL-6, EGF or GAPDH. Hybridization wasperformed at 60°C in 5 X SSC, 0.1% SDS, 5% dextran sulphateand denatured salmon sperm DNA (100 pg/ml). Thereafter, thefilter was washed once in 1 x SSC, 0.1% SDS and once in 0.5 XSSC, 0.1% SDS at 60°C for 15 minutes each. Following thestringency washes, the filter was blocked and incubated withhorseradish peroxidase conjugate anti-fluorescein antibody. The

1992 Ranieri et at: Urinaiy IL-6/EGF ratio in IgA nephropathy
blot was then covered with the detection buffer, containingluminol, and exposed for three minutes to Kodak X-omat X-rayfilm. The bands obtained were quantified by densitometric anal-ysis.
Urinaiy IL-6 and EGF assay
Quantitative determination of the IL-6 and EGF levels in urinewas performed using a human interleukin-6 and a human EGFELISA Kit (Biotrak; Amersham), a multiple-sandwich solid-phase enzyme immunoassay that uses monoclonal and polyclonalantibodies raised against human IL-6 and EGF proteins. Theenzymatic reaction was detected in an automatic microplatephotometer (Titertek, Flow Labs, USA). The IL-6 and EGFconcentration of the unknown samples were determined byinterpolation into a standard curve developed with knownamounts of purified human IL-6 and EGF proteins, and expressedin pg/mI. The lower detection limit was 0.7 pglml for IL-6 and 8pg/ml for EGF. The intra- and interassay coefficients of variationwere 4.2% and 7.0% for IL-6, and 2.9% and 4.1% for EGF,respectively.
In situ hybridization
Renal tissue was immediately included in OCT compound,snap-frozen in liquid nitrogen and stored in the same liquid untilused. Frozen sections (6 j.tm thick) were collected onto polylysine-coated slides, dried briefly on a hot plate at +80°Cand fixed in 4%paraformaldehyde for 20 minutes. After two washes in PBS,dehydration in graded ethanols and brief air drying, sections wereimmediately used for in situ hybridization. Sections from normaland diseased kidneys were processed in parallel, using the samebatches of probes and reagents.
For the preparation of RNA probes, the cDNA fragments weresubcloned into the plasmid pGEM1 (Promega Biotech, Florence,Italy) at the appropriate restriction sites. After linearization of theplasmids with either HindIII or EcoRI restriction endonuclease,T7 or SP6 RNA-polymerase (Boehringer Mannheim, Germany),respectively, were employed to obtain run off transcripts of eitherthe anti-sense (complementary to mRNA) or sense (anticomple-mentary to mRNA, negative control) strands. Transcription andlabeling of RNA probes were performed as described [29]. Briefly,80 Ci of [35S]uridine-5'-(a-thio)-triphosphate (S.A. 1,250 Ci!mmol; Amersham) was added to a 10 d reaction mixture (0.5 mMeach of adenosine-, cytidine- and guanosine-5'-triphosphate/l msdithiothreitol/10 units human placental RNase inhibitor/6 mviMgCl2/10 mr'i Tris-HCI, pH 7.5/2 mrvi spermidine/lO mivi NaCI)including 1 j.tg of linearized plasmid and 16 units of either SP6 orT7 RNA polymerase. The reaction was allowed to proceed for 60minutes at 38°C. The DNA plasmid was removed by digestionwith 25 j.g/ml RNase-free DNase I in a mixture containing 12.5mg/ml of yeast tRNA and 10 units of RNase inhibitor for 10minutes at 37°C. Free ribonucleotides were removed by phenol-chloroform extraction followed by ethanol precipitation. To in-crease the penetration into tissue, the size of the 35S-labeled RNAprobes was adjusted to 50 to 200 bases length by a controlledalkaline hydrolysis in 80 mi NaHCO3/120 mM Na2CO3, pH10.2/10 mi dithiothreitol at 60°C. After neutralization in 0.2 Msodium acetate, pH 6.0/1% acetic acid/lO mrvi dithiothreitol andethanol precipitation, RNA probes were stored at —80°C andused within four weeks. The specific activity usually obtained was1.2 to 1.4 X i0 cpm/j.tg of 35S-labeled RNA probe.
Prehybridization, hybridization, removal of a nonspecificallybound probe by RNase A digestion, and further washing proce-dures were performed for both positive and negative strand RNAprobes as described previously [30, 3fl. Autoradiography wasperformed by dipping the dehydrated slides into Ilford G5 nuclearemulsion (Ilford, Mobberley Cheshire, UK). The exposed slideswere developed using Kodak D19 developer (Kodak, HemelHampstead, UK), counterstained in hematoxylin-eosin and finallymounted.
ImmunohistochemistiyThe immunohistochemical detection of IL-6 and EGF was
performed on frozen kidney sections using chromatographicallypurified mouse antibody, specific for human IL-6 (Genzyme,Cambridge, MA, USA) and human EGF (IgGi, clone 144-8;Oncogene Science, Inc., Manhasset, NY, USA). Immobilizedmouse antibodies were detected by the immunoalkaline phos-phatase (APAAP) method with an affinity-purified rabbit anti-mouse immunoglobulin serum (1:20 dilution; Dako, Milan, Italy)and APAAP complex (1:50 dilution, Dako), as previously de-scribed [30, 31]. Alkaline phosphatase was developed with amixture of naphtol AS-BI phosphate and new fuchsin (Sigma,Milan, Italy). Levamisole (Sigma, Munich, Germany) was addedto the development solution in order to block endogenous alka-line phosphatase activity. Negative controls were performed byomitting the primary or secondary antibodies, and employingnon-immune mouse serum as first layer. The identification oftubular segments were performed as follows: (1) for the proximaltubule, the presence of endogenous alkaline phosphatase wasdetected by using a mixture of naphtol AS-BI phosphate and newfuchsin lacking levamisole, while the CHIP28 antigen, a waterchannel protein [321 by an indirect immunofluorescence tech-nique employing a rabbit polyclonal anti-human CHIP28 antibody(donated by Dr. G. Valenti) followed by a fluorescein-conjugatedanti-rabbit antibody; (2) for the ascending portion of Henle's loopand the distal tubule, a direct immunofluorescence technique wasemployed using a fluoresceine-conjugate anti-human Tamm-Horsfall protein (provided by Dr. G.B. Fogazzi) [33].
Microscopy studies
The histologic lesions and the optical density of the signalsgenerated by the new fuchsin (immunohistochemistry) and silvergrains (in situ hybridization) were quantitated by a computer-based morphometric analysis system. The video image was gen-erated with a video camera (Hamamatsu, Milan, Italy) connectedthrough a frame grabber (Hamamatsu) to a Power PC computer(Macintosh, Cupertino, CA, USA). Single images were digitizedfor image analysis at 256 grey levels. Imported data were analyzedquantitatively by an Optilab Pro 2.6.1 Software (Graftek, Villan-terio, PV, Italy) that operated a color-based pitch densitometry.An optical threshold and filter combination was set to select onlythe nuclei, the mesangial matrix, the interstitial infiltrate andfibrosis, the new fuchsin deposits and silver grains. Two observersindependently assessed morphological changes as well as in situhybridization and immunohistochemical signals in a double-blindprotocol, as previously described [31].
Total area, glomerular matrix area, glomerular cellularity,number of interstitial cell infiltrates, areas of interstitial fibrosisand number of pixels generated by silver grains (in situ hybrid iza-tion) and new fuchsin (immunohistochemistry) were quantified in
4'I'...
five to eight randomly selected glomeruli or interstitial areas fromeach biopsy. The structures of interest were interactively discrim-inated by the operators using the cursor and then automaticallymeasured for total area. The resulting counts divided by the totalarea gave the measures desired. Using the Statview II Software(Brain Power Inc., Calabasas, CA) the single data for eachvariable were tabulated and Pearson's correlation coefficient werecomputed by linear-least squares regression.
Statistical analysis
Quantitative data were compared among the groups byANOVA, and multiple interferences were drawn by Fisher'sprotected t-test. The correlation coefficients are Pearson's rvalues.
Results
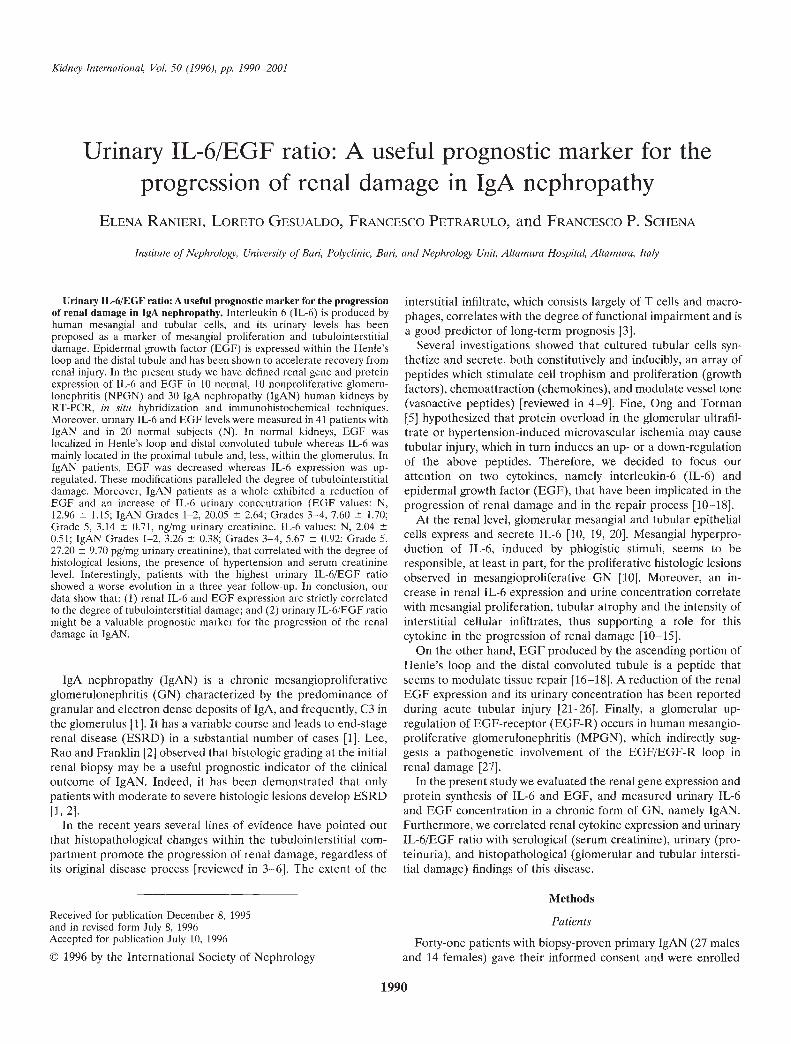
IgAN patients, as a whole, showed an increased expression ofIL-6 niRNA by PCR in total renal cortex compared to normalsand to patients affected by NPGN (Fig. 1). Specifically, theincrease was remarkable only in those biopsies showing relevantsigns of tubulointerstitial damage (tubular atrophy, cellular infil-trates). Indeed, patients with moderate-severe tubulointerstitial
lesions (G3-G4 and G5 classes) had a 1.76- and 4.24-fold increaseof IL-6 mRNA levels, respectively, compared to normals, whereasthe IL-6/GAPDH ratio of G1-G2 patients did not differ fromnormals or from patients affected by NPGN (1.0, 1.3 and 0.90,respectively; Figs. 1 and 2). It was interesting to observe that the
• only NPGN patient (a case with membranous nephropathy)• displaying high mRNA levels of IL-6 (Fig. 1) also had severe
tubulointerstitial lesions and showed an unfavorable outcome atthe follow-up.
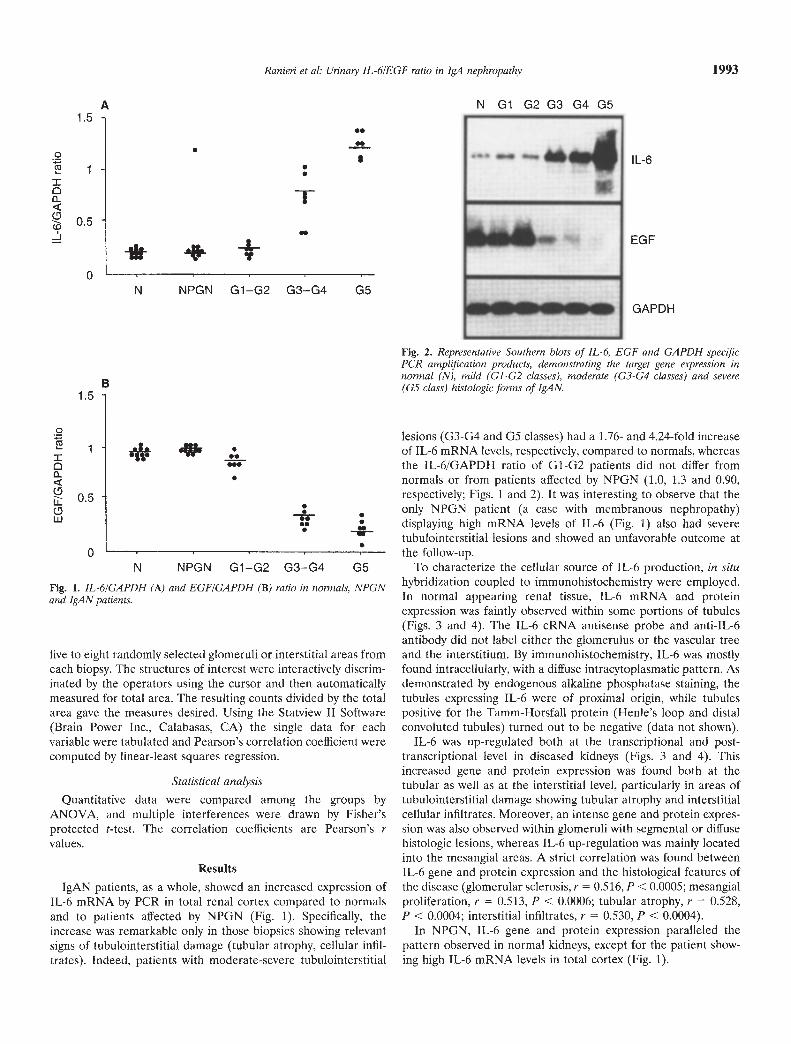
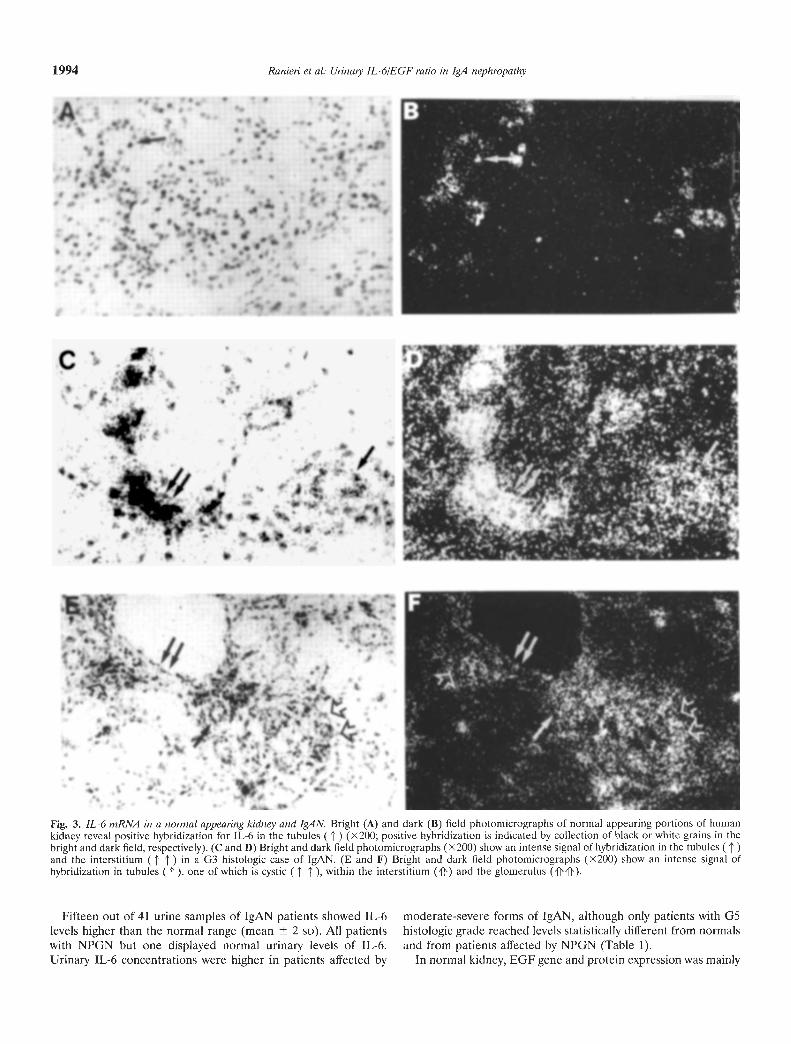
To characterize the cellular source of IL-6 production, in situhybridization coupled to immunohistochemistry were employed.In normal appearing renal tissue, IL-6 niRNA and proteinexpression was faintly observed within some portions of tubules(Figs. 3 and 4). The IL-6 cRNA antisense probe and anti-IL-6antibody did not label either the glomerulus or the vascular treeand the interstitium. By immunohistochemistry, IL-6 was mostlyfound intracellularly, with a diffuse intracytoplasmatic pattern. Asdemonstrated by endogenous alkaline phosphatase staining, thetubules expressing IL-6 were of proximal origin, while tubulespositive for the Tamm-Horsfall protein (1-lenle's loop and distalconvoluted tubules) turned out to be negative (data not shown).
IL-6 was up-regulated both at the transcriptional and post-transcriptional level in diseased kidneys (Figs. 3 and 4). Thisincreased gene and protein expression was found both at thetubular as well as at the interstitial level, particularly in areas oftubulointerstitial damage showing tubular atrophy and interstitialcellular infiltrates. Moreover, an intense gene and protein expres-sion was also observed within glomeruli with segmental or diffusehistologic lesions, whereas IL-6 up-regulation was mainly locatedinto the mesangial areas. A strict correlation was found betweenIL-6 gene and protein expression and the histological features ofthe disease (glomerular sclerosis, r = 0.516, P < 0.0005; mesangialproliferation, r = 0.513, P < 0.0006; tubular atrophy, r = 0.528,P < 0.0004; interstitial infiltrates, r = 0.530, P < 0.0004).
In NPGN, IL-6 gene and protein expression paralleled thepattern observed in normal kidneys, except for the patient show-ing high IL-6 mRNA levels in total cortex (Fig. 1).
N NPGN G1-G2 G3-G4 G5
Ranieri et al: Urinay IL-6/EGF ratio in IgA nephropathy 1993
N G1 G2 G3 G4 G5
.•S.• IL-6.
S
1EGF
GAPDH
Fig. 2. Representative Southern blots of IL-6, EGF and GAPDH specificPCR amplification products, demonstrating the target gene expression innoimal (N), mild (G1-G2 classes), moderate (G3-G4 classes) and severe(G5 class) histologic forms of IgAN.
A1.5
01-I0
a-
0-J
0-
1.5
0
•1I ___0a-
0IL0w
0-N NPGN G1-G2 G3-G4 G5
Fig. 1. IL-6/GAPDH (A) and EGF/GAPDH (B) ratio in normals, NPGNand Ig.4 N patients.
B
*
• .5
t_
:_.
S
•
S
•tf
I
p j5
'S
• I a
-
'C
• o •)
' •
*
•.c)
a t•
—
S.
, p.
S
S
.'
S.
.1
a S
S
S
'
• e
.5 •
'I-'
—
1•
.S
• S
•r
%
• p
S.
t •
• S
S
V
•
' S
• •t
p.
• —
0—
'—
• •.
.0
• •
••H
t S
—
—
• •
•54.
'4
'.•
_p•
.0
• I.
• S.,
'4
• S
c a.
5
.5—
5 S
S.
• S
—a
S.
• I • •
S
., F
•
St
? 5.
4 IS
. p
I, -—
5(
45
• .'.
•
a —
I
5,4
•'•J
—
b.
•'jf
5%
S •5
S
• I.
• p.
S •
55
•%
S.
a •
I. .9
III.
S
•••
1994 Ranieri et al: Urinaty IL-6/EGF ratio in IgA nephropathy
Fig. 3. IL-6 mRNA in a normal appearing kidney and IgAN. Bright (A) and dark (B) field photomicrographs of normal appearing portions of humankidney reveal positive hybridization for IL-6 in the tubules ('i) (X200; positive hybridization is indicated by collection of black or white grains in thebright and dark field, respectively). (C and D) Bright and dark field photomicrographs (x200) show an intense signal of hybridization in the tubules ( t)and the interstitium ( j' ) in a G3 histologic case of IgAN. (E and F) Bright and dark field photomicrographs (x200) show an intense signal ofhybridization in tubules ( ' ), one of which is cystic ( ' 1' ), within the interstitium ('()') and the glomerulus ('ff'fl').
Fifteen out of 41 urine samples of IgAN patients showed IL-6 moderate-severe forms of IgAN, although only patients with G5levels higher than the normal range (mean 2 SD). All patients histologic grade reached levels statistically different from normalswith NPGN but one displayed normal urinary levels of IL-6. and from patients affected by NPGN (Table 1).Urinary IL-6 concentrations were higher in patients affected by In normal kidney, EGF gene and protein expression was mainly
- V- 4'; -
- 41 t;.1j- -. ::'
C— ..1_I.e.3 -'t'.
.. .
j1.•
-
-. U
F
- .' I
B ft- r
t
4-a.
a-p-fS
-itV
jai
1Pt
Wk 4
I
Ranieri et ci: Urinaty IL-6/EGF ratio in IgA nephropathy 1995
Fig. 4. Immunohistochemistry for IL-6 protein in a normal appeathig kidney and IgAN. (A) Immunostaining of IL-6 protein in normal kidney is seen asthe dark red alkaline phosphatase product within the proximal tubules (t). Immunostaining of IL-6 protein in IgAN with G2 class (B), G4 class (C)and G5 class (D). In B the pattern of IL-6 immunostaining resembled that observed in A, while a striking increase of IL-6 protein was observed bothin the glomerulus ('if) and in the tubulointerstitial areas (proximal tubules, , and interstitial infiltrate, ' ' ) in C and D. (E) Note the increase of IL-6protein within tubules with atrophy and necrosis (1' ) as well as in cellular casts ('if). (F) Immunostaining with a nonimmune serum.
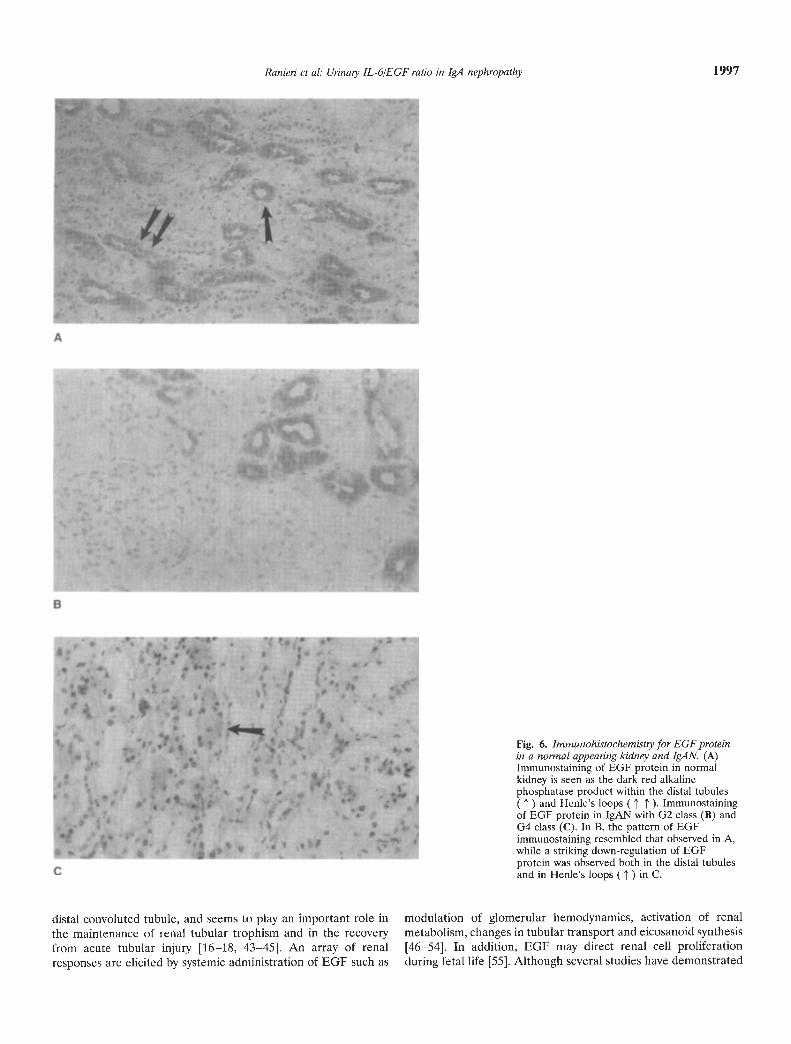
distributed in 1-lenle's loop and distal convoluted tubules, andcolocalized with Tamm-Horsfall staining (data not shown), whilethe glomerulus, the remaining tubular segments, the interstitumand the vascular tree were negative (Figs. 5 and 6).
Compared to normals and to patients affected by NPGN butone, EGF gene and protein expression, as demonstrated byRT-PCR and in situ hybridization techniques, was down-regulatedin 1gAN patients (Figs. 1, 2, 5 and 6). These modifications
• ;. . S.
S.a-. - I 55'C_s ••• .—. : C'
•lu$- I 5 5 C'?1%•: 'I '•- 'F I
•II S SS
S • •C • • e•'1S' -..;-:
!fl!.S
4 C'S
%e. • •%I •'I • •. I- 5•_ -. ••
S'Sit' S• I •• I
C— —
Sj••5_
S 1I -
SI .• .t;...: .,•-iX-.sj :----:-- - • ' .. .5t.
• •..4. - S.-.- -e ' • , -:
I..:s•' :;— ••q — •' . •#t
1996 Ranieri et al: Urinaiy IL-6/EGF ratio in IgA nephropathy
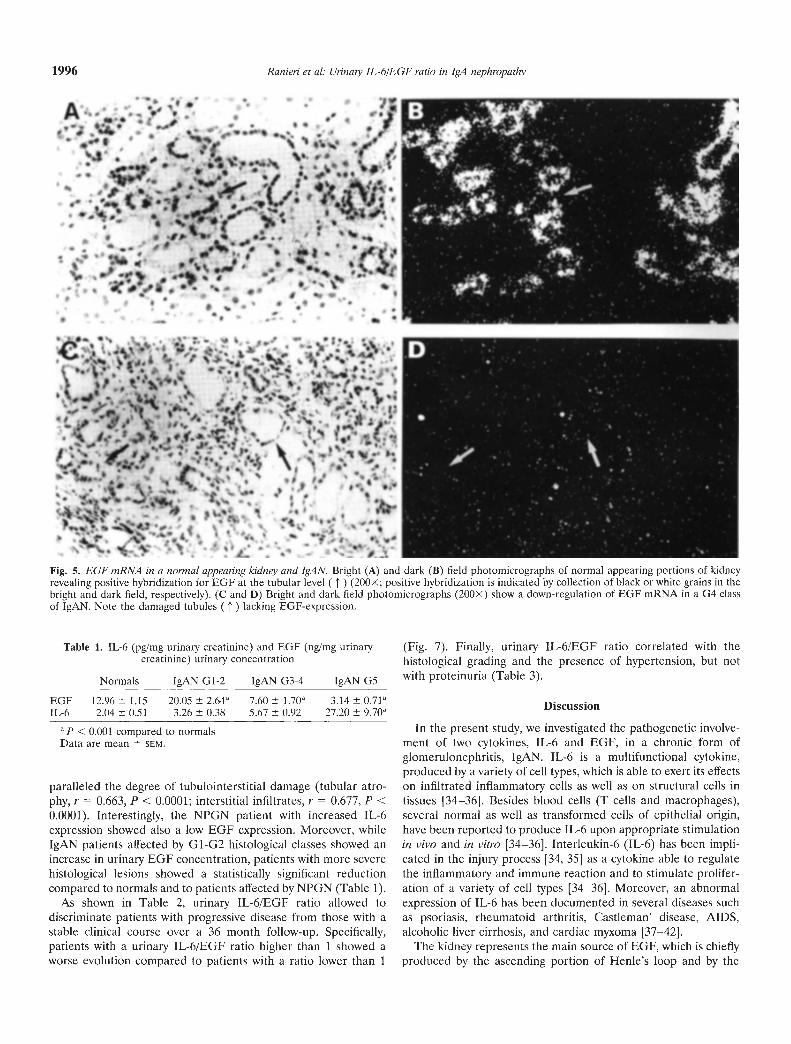
Fig. 5. EGF mRNA in a normal appearing kidney and IgAN. Bright (A) and dark (B) field photomicrographs of normal appearing portions of kidneyrevealing positive hybridization for EGF at the tubular level ( j' ) (200X; positive hybridization is indicated by collection of black or white grains in thebright and dark field, respectively). (C and D) Bright and dark field photomicrographs (200x) show a down-regulation of EGF mRNA in a G4 classof IgAN. Note the damaged tubules (1) lacking EGF-exprcssion.
Table 1. IL-6 (pg/mg urinary creatinine) and EGF (nglmg urinarycreatinine) urinary concentration
Normals IgAN G1-2 IgAN G3-4 TgAN G5
EGF 12.96 1.15 20.05 2.64a 7.60 1.70 3.14 0.71IL-6 2.04 0.51 3.26 0.38 5.67 0.92 27.20 9.70k'
P < 0.00 1 compared to normalsData are mean SEM.
paralleled the degree of tuhulointerstitial damage (tubular atro-phy, r = 0.663, P < 0.0001; interstitial infiltrates, r = 0.677, P <0.0001). Interestingly, the NPGN patient with increased IL-6expression showed also a low EGF expression. Moreover, whileIgAN patients affected by G1-G2 histological classes showed anincrease in urinary EGF concentration, patients with more severehistological lesions showed a statistically significant reductioncompared to normals and to patients affected by NPGN (Table 1).
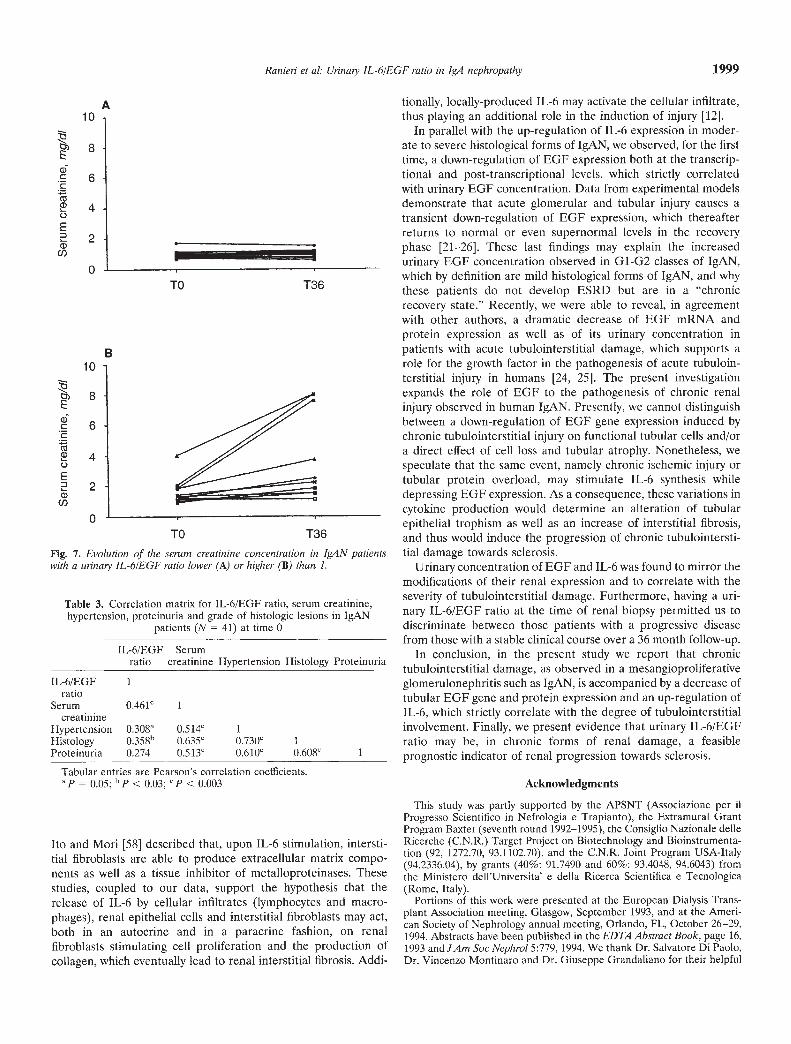
As shown in Table 2, urinary IL-6/EGF ratio allowed todiscriminate patients with progressive disease from those with astable clinical course over a 36 month follow-up. Specifically,patients with a urinary IL-6/EGF ratio higher than I showed aworse evolution compared to patients with a ratio lower than I
(Fig. 7). Finally, urinary IL-6IEGF ratio correlated with thehistological grading and the presence of hypertension, but notwith proteinuria (Table 3).
Discussion
In the present study, we investigated the pathogenetic involve-ment of two cytokines, IL-6 and EGF, in a chronic form ofglomerulonephritis, IgAN. IL-6 is a multifunctional cytokine,produced by a variety of cell types, which is able to exert its effectson infiltrated inflammatory cells as well as on structural cells intissues [34—36]. Besides blood cells (T cells and macrophages),several normal as well as transformed cells of epithelial origin,have been reported to produce IL-6 upon appropriate stimulationin vivo and in vitro [34—36]. Interleukin-6 (IL-6) has been impli-cated in the injury process [34, 35] as a cytokine able to regulatethe inflammatory and immune reaction and to stimulate prolifer-ation of a variety of cell types [34—36]. Moreover, an abnormalexpression of IL-6 has been documented in several diseases suchas psoriasis, rheumatoid arthritis, Castleman' disease, AIDS,alcoholic liver cirrhosis, and cardiac myxoma [37—42].
The kidney represents the main source of EGF, which is chieflyproduced by the ascending portion of Henle's loop and by the
Ranieri Ct al: Urinaty IL-6/EGF ratio in IgA nephropathy 1997
Fig. 6. Immunohistochemistiy for EGF proteinin a normal appearing kidney and IgAN. (A)Immunostaining of EUF protein in normalkidney is seen as the dark red alkalinephosphatase product within the distal tubules(t) and Henle's loops (1' 1). Immunostainingof EGF protein in IgAN with G2 class (B) andG4 class (C). In B, the pattern of EGFimmunostaining resembled that observed in A,while a striking down-regulation of EGFprotein was observed both in the distal tubulesand in Henle's loops () in C.
distal convoluted tubule, and seems to play an important role in modulation of glomerular hemodynamics, activation of renalthe maintenance of renal tubular trophism and in the recovery metabolism, changes in tubular transport and eicosanoid synthesisfrom acute tubular injury [16—18, 43—45]. An array of renal [46—54]. In addition, EGF may direct renal cell proliferationresponses are elicited by systemic administration of EGF such as during fetal life [55]. Although several studies have demonstrated
1998 Ranieri et al: Urinary IL-6/EGF ratio in IgA nephropathy
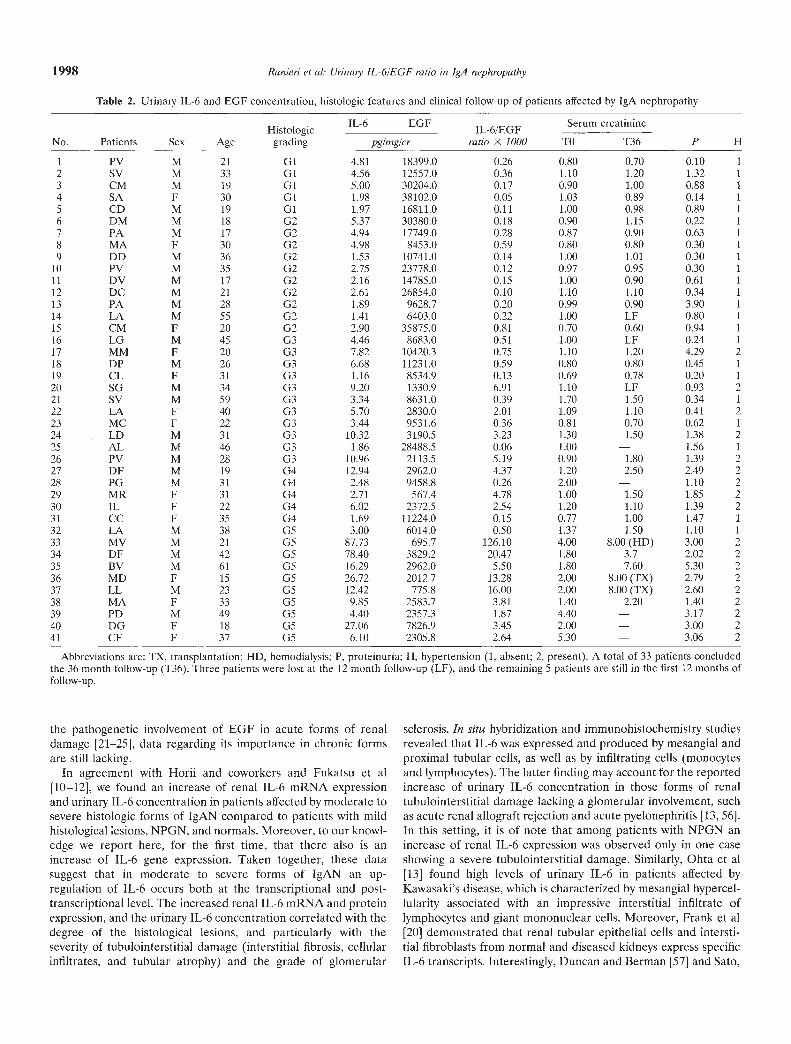
Table 2. Urinary IL-6 and EGF concentration, histologic features and clinical follow-up of patients affected by IgA nephropathy
Abbreviations are: TX, transplantation; HD, hemodialysis; P, proteinuria; H, hypertension (1, absent; 2, present). A total of 33 patients concludedthe 36 month follow-up (T36). Three patients were lost at the 12 month follow-up (LF), and the remaining 5 patients are still in the first 12 months offollow-up.
the pathogenetic involvement of EGF in acute forms of renaldamage [21—25], data regarding its importance in chronic formsare still lacking.
In agreement with Horii and coworkers and Fukatsu et al[10—12], we found an increase of renal IL-6 mRNA expressionand urinary IL-6 concentration in patients affected by moderate tosevere histologic forms of IgAN compared to patients with mildhistological lesions, NPGN, and normals. Moreover, to our knowl-edge we report here, for the first time, that there also is anincrease of IL-6 gene expression. Taken together, these datasuggest that in moderate to severe forms of IgAN an up-regulation of IL-6 occurs bt)th at the transcriptional and post-transcriptional level. The increased renal IL-6 mRNA and proteinexpression, and the urinary IL-6 concentration correlated with thedegree of the histological lesions, and particularly with theseverity of tubulointerstitial damage (interstitial fibrosis, cellularinfiltrates, and tubular atrophy) and the grade of glomerular
sclerosis. In situ hybridization and immunohistochemistry studiesrevealed that IL-6 was expressed and produced by mesangial andproximal tubular cells, as well as by infiltrating cells (monocytesand lymphocytes). The latter finding may account for the reportedincrease of urinary IL-6 concentration in those forms of renaltubulointerstitial damage lacking a glomerular involvement, suchas acute renal allograft rejection and acute pyelonephritis [13, 561.In this setting, it is of note that among patients with NPGN anincrease of rcnal IL-6 expression was observed only in one caseshowing a severe tubulointerstitial damage. Similarly, Ohta et al[13] found high levels of urinary IL-6 in patients affected byKawasaki's disease, which is characterized by mesangial hypercel-lularity associated with an impressive interstitial infiltrate oflymphocytes and giant mononuclear cells. Moreover, Frank et a![20] demonstrated that renal tubular epithelial cells and intersti-tial fibroblasts from normal and diseased kidneys express specificIL-6 transcripts. Interestingly, Duncan and Berman [57] and Sato,
IL-6 EGF Serum creatinine
pg/mg/cr TO T36 P HNo. Patients Sex AgeHistologicgrading
IL-6/EGFratio ><1000
1 PV M 21 01 4.81 18399.0 0.26 0.80 0.70 0.10 1
2 SV M 33 GI 4.56 12557.0 0.36 1.10 1.20 1.32 1
3 CM M 19 GI 5.00 30204.0 0.17 0.90 1.00 0.88 1
4 SA F 30 Cl 1.98 38102.0 0.05 1.03 0.89 0.14 1
5 CD M 19 01 1.97 16811.0 0.11 1.00 0.98 0.89 1
6 DM M 18 G2 5.37 30380.0 0.18 0.90 1.15 0.22 1
7 PA M 17 02 4.94 17749.0 0.28 0.87 0.90 0.63 1
8 MA F 30 G2 4.98 8453.0 0.59 0.80 0.80 0.30 1
9 DD M 36 02 1.53 10741.0 0.14 1.00 1.01 0.30 1
10 PV M 35 G2 2.75 23778.0 0.12 0.97 0.95 0.30 1
11 DV M 17 G2 2.16 14785.0 0.15 1.00 0.90 0.61 1
12 DC M 21 G2 2.61 26854.0 0.10 1.10 1.10 0.34 1
13 PA M 28 G2 1.89 9628.7 0.20 0.99 0.90 3.90 1
14 LA M 55 G2 1.41 6403.0 0.22 1.00 LF 0.80 1
15 CM F 20 02 2.90 35875.0 0.81 0.70 0.60 0.94 1
16 LG M 45 03 4.46 8683.0 0.51 1.00 LF 0.24 1
17 MM F 20 03 7.82 10420.3 0.75 1.10 1.20 4.29 218 DP M 26 03 6.68 11231.0 0.59 0.80 0.80 0.45 119 CL F 31 03 1.16 8534.9 0.13 0.69 0.78 0.20 120 SO M 34 03 9.20 1330.9 6.91 1.10 LF 0.93 221 SV M 59 03 3.34 8631.0 0.39 1.70 1.50 0.34 122 LA F 40 G3 5.70 2830.0 2.01 1.09 1.10 0.41 223 MC F 22 03 3.44 9531.6 0.36 0.81 0.70 0.62 124 LD M 31 G3 10.32 3190.5 3.23 1.30 1.50 1.38 225 AL M 46 G3 1.86 28488.5 0.06 1.00 — 1.56 1
26 PV M 28 03 10.96 2113.5 5.19 0.90 1.80 1.39 227 DF M 19 04 12.94 2962.0 4.37 1.20 2.50 2.49 228 PG M 31 G4 2.48 9458.8 0.26 2.00 — 1.10 229 MR F 31 G4 2.71 567.4 4.78 1.00 1.50 1.85 230 IL F 22 G4 6.02 2372.5 2.54 1.20 1.10 1.39 231 CC F 35 04 1.69 11224.0 0.15 0.77 1.00 1.47 1
32 LA M 38 05 3.00 6014.0 0.50 1.37 1.50 1.10 1
33 MV M 21 05 87.73 695.7 126.10 4.00 8.00 (HD) 3.00 234 DF M 42 G5 78.40 3829.2 20.47 1.80 3.7 2.02 235 BV M 61 05 16.29 2962.0 5.50 1.80 7.60 5.30 236 MD F 15 05 26.72 2012.7 13.28 2.00 8.00 (TX) 2.79 237 LL M 23 05 12.42 775.8 16.00 2.00 8.00 (TX) 2.60 238 MA F 33 05 9.85 2583.7 3.81 1.40 2.20 1.40 239 PD M 49 G5 4.40 2357.3 1.87 4.40 — 3.17 240 DO F 18 05 27.06 7826.9 3.45 2.00 — 3.00 241 CF F 37 05 6.10 2305.8 2.64 5.30 — 3.06 2
Ranieri et al: Urinaty IL-6/EGF ratio in IgA nephropathy 1999
IL-6/EGF 1ratio
Serum 0.461c Icreatinine
HypertensionHistology
0.308"0358b
0.514'0.635c
1
0730" 1Proteinuria 0.274 0.513c 0.610" 0.608"
Ito and Mon [58] described that, upon IL-6 stimulation, intersti-tial fibroblasts are able to produce extracellular matrix compo-nents as well as a tissue inhibitor of metalloproteinases. Thesestudies, coupled to our data, support the hypothesis that therelease of IL-6 by cellular infiltrates (lymphocytes and macro-phages), renal epithelial cells and interstitial fibroblasts may act,both in an autocrine and in a paracrine fashion, on renalfibroblasts stimulating cell proliferation and the production ofcollagen, which eventually lead to renal interstitial fibrosis. Addi-
tionally, locally-produced IL-6 may activate the cellular infiltrate,thus playing an additional role in the induction of injury [121.
In parallel with the up-regulation of IL-6 expression in moder-ate to severe histological forms of lgAN, we observed, for the firsttime, a down-regulation of EGF expression both at the transcrip-tional and post-transcriptional levels, which strictly correlatedwith urinary EGF concentration. Data from experimental modelsdemonstrate that acute glomerular and tubular injury causes atransient down-regulation of EGF expression, which thereafterreturns to normal or even supernormal levels in the recoveryphase [21—26]. These last findings may explain the increasedurinary EGF concentration observed in G1-G2 classes of IgAN,which by definition are mild histological forms of IgAN, and whythese patients do not develop ESRD but are in a "chronicrecovery state." Recently, we were able to reveal, in agreementwith other authors, a dramatic decrease of EGF mRNA andprotein expression as well as of its urinary concentration inpatients with acute tubulointerstitial damage, which supports arole for the growth factor in the pathogenesis of acute tubuloin-terstitial injury in humans [24, 25]. The present investigationexpands the role of EGF to the pathogenesis of chronic renalinjury observed in human IgAN. Presently, we cannot distinguishbetween a down-regulation of EGF gene expression induced bychronic tubulointerstitial injury on functional tubular cells and/ora direct effect of cell loss and tubular atrophy. Nonetheless, wespeculate that the same event, namely chronic ischemic injury ortubular protein overload, may stimulate IL-6 synthesis whiledepressing EGF expression. As a consequence, these variations incytokine production would determine an alteration of tubularepithelial trophism as well as an increase of interstitial fibrosis,and thus would induce the progression of chronic tubulointersti-tial damage towards sclerosis.
Urinary concentration of EGF and IL-6 was found to mirror themodifications of their renal expression and to correlate with theseverity of tubulointerstitial damage. Furthermore, having a uri-nary IL-6/EGF ratio at the time of renal biopsy permitted us todiscriminate between those patients with a progressive diseasefrom those with a stable clinical course over a 36 month follow-up.
In conclusion, in the present study we report that chronictubulointerstitial damage, as observed in a mesangioproliferativeglomerulonephritis such as IgAN, is accompanied by a decrease oftubular EGF gene and protein expression and an up-regulation ofIL-6, which strictly correlate with the degree of tubulointerstitialinvolvement. Finally, we present evidence that urinary IL-6/EGFratio may be, in chronic forms of renal damage, a feasibleprognostic indicator of renal progression towards sclerosis.
Acknowledgments
This study was partly supported by the APSNT (Associazione per iiProgresso Scientifico in Nefrologia e Trapianto), the Extramural GrantProgram Baxter (seventh round 1992—1995), the Consiglio Nazionale delleRicerche (C.N.R.) Target Project on Biotechnology and Bioinstrumenta-tion (92, 1272.70, 93.1102.70), and the C.N.R. Joint Program USA-Italy(94.2336.04), by grants (40%: 91.7490 and 60%: 93.4048, 94.6043) fromthe Ministcro dell'Universita' e della Ricerca Scientifica e Tecnologica(Rome, Italy).
Portions of this work were presented at the European Dialysis Trans-plant Association meeting, Glasgow, September 1993, and at the Ameri-can Society of Nephrology annual meeting, Orlando, FL, October 26—29,1994. Abstracts have been published in the EDTA Abstract Book, page 16,1993 and JAm Soc Nephrol 5:779, 1994. We thank Dr. Salvatore Di Paolo,Dr. Vincenzo Montinaro and Dr. Giuseppe Grandaliano for their helpful
TO T36
B
A10
8
6
4
2
0-
10
tY) BE1). 6
40E= 2a)Cl)
0TO T36
Fig. 7. Evolution of the serum creatinine concentration in IgAN patientswith a urinary IL-6/EGF ratio lower (A) or higher (B) than 1.
Table 3. Correlation matrix for IL-6/EGF ratio, serum creatinine,hypertension, proteinuria and grade of histologic lesions in IgAN
patients (N = 41) at time 0
IL-6/EGF Serumratio creatinine Hypertension Histology Proteinuria
Tabular entries are Pearson's correlation coefficients.ap = 0.05; bp < 0.03; "P < 0.003
2000 Ranieri et al: Unnaty IL-6/EGF ratio in IgA nephropathy
comments and criticism of this article. Finally, we acknowledge thetechnical support of Dr. Giosafatte Pallotta, Dr. Raffaella Monno, MissCarmela Marseglia, Mrs. Carmela Martino, Mrs. Rosa Colagiacomo andMr. Nicola Bonavoglia.
Reprint requests to Prof F.P. Schena, Institute of Nephrology, University ofBan, Polyclinic, Piazza Giulio Cesare, 11, 70124 Ban, Italy.E-mail: kidney @ teseo.it
References
1. SCHENA FP: A retrospective analysis of the natural history of primaryIgA nephropathy worldwide. Am J Med 89:209—215, 1990
2. LEE SMK, RAO MV, FRANKLIN WA: IgA nephropathy: Morphologicpredictors of progressive renal disease. Human Pathol 13:314—322,1982
3. D'Aaico 0: Role of infiltration of leukocytes in glomerular diseases.Nephrol Dial Transplant 3:596—600, 1988
4. ONo ACM, FINE LG: Tubular derived growth factors and cytokines inthe pathogenesis of tubulointerstitial fibrosis: Implications for humanrenal disease progression. Am J Nephrol 23:205—209, 1994
5. FINE LG, ONG ACM, TORMAN JT: Mechanism of tubulo-interstitialinjury in progressive renal diseases. EurJ Clin Invest 23:259—265, 1993
6. ONG ACM, FINE LG: Tubular-derived cytokines and human renaldisease progression. Nephrol Dial Transplant 9:471—472, 1994
7. EMANCIPATOR SN, SED0R JR: Cytokines in renal disease, in Cytokinesin Health and Disease: Physiology and Pathophysiology (vol 25), editedby REMICK DG, KUNKEL SL, New York, Marcel Dekker, 1992, pp467—488
8. ABBOUD HE: Growth factors in glomerulonephritis. Kidney mt 43:252—267, 1993
9. GESUALDO L, DI PAOLO S, RANIERI E, SCHENA FP: Growth factorsand their receptors in the progression of renal damage. ContribNephrol 111:38—44, 1995
10. Hom Y, MURAGUCHI A, IWANO M, MATSUDA T, HIRAYAMA T,YAMADA H, FUJII Y, DoI-n K, ISHIKAWA H, OHMOTO Y, YOSHIZAKI K,HIRANO T, KISHIMOTO T: Involvement of IL-6 in mesangial prolifer-ative glomerulonephritis. J Immunol 143:3949—3956, 1989
11. FUKATSU A, MATSUO S, TAMAI H, SAKAMOTO N, MATSUDA T, HIRANOT: Distribution of interleukin-6 in normal and diseased human kidney.Lab Invest 65:61—66, 1991
12. FUKATSU A, MATSUO S, YUZAWA Y, M!YAI H, FUTENMA A, KATO K:Expression of interleukin 6 and major histocompatibility complexmolecules in tubular epithelial cells of diseased human kidneys. LabInvest 69:5867—5874, 1993
13. OHTA K, TAKANO N, SENO A, YACHIE A, MIYAWAKI T, YOKOYAMA H,T0MOSUGI N, KATO E, TANIGUCHI N: Detection and clinical useful-ness of urinary interleukin-6 in the diseases of kidney and urinarytract. Clin Nephrol 38:185—189, 1992
14. IwAN0 M, D0HI K, HIRATA E, KURUMANTANI N, H0RII Y, SI-IIIKI H,FUKATSU A, MATSUDA T, HIRANO T, ISHIKAWA H: Urinary levels ofIL-6 in patients with active lupus nephritis. C/in Nephrol 40:16—21,1993
15. T0MIN0 Y, FUNABIKI K, OHMURO H, SHIMIZU M, YOKOYAMA K,SHIRATO I, SHIRAI T, TAKAI-IASHI M, KOIDE H: Urinary levels ofinterleukin-6 and disease activity in patients with IgA nephropathy.AmJNephrol 11:459—464, 1991
16. HUMES HD, CIESLINSKI DA, COIMBRA TM, MESSANA JM, GALVAO C:Epidermal growth factor enhances renal tubule regeneration andrepair and accelerates recovery of renal function in post-ischemicrenal failure. J Clin Invest 84:1757—1761, 1989
17. COIMBRA TM, CIESLINSKI DA, HUMES HD: Epidermal growth factoraccelerates renal repair in mercuric chloride nephrototoxicity. Am JPhysiol 259:F438—F443, 1990
18. NORMAN J, TSAU YK, BACAY A, FINE LG: Epidermal growth factor(EGF) accelerates recovery from ischemic acute tubular necrosis:Role of the EGF-receptor. C/in Sci 78:445—449, 1990
19. COLEMAN D, RUEF C: Interleukin 6: An autocrine regulator ofmesangial cell growth. Kidney Int 41:604—611, 1992
20. FRANK J, ENGLER-BLUM G, RODEMANN HP, MULLER GA: Humantubular cells as a cytokine source: PDGF-B, GM-CSF and IL-6mRNA expression in vitro. Exp Nephrol 1:26—35, 1993
21. SAFIRSTEIN R, PRICE PM, SAGGI S, HARRIS RC: Changes in geneexpression after temporary renal ischemia. Kidney mt 37:1515—152, 1990
22. STORCH 5, Sooi S, MEGYESI J, PRICE PM, SAFIRSTEIN R: Uretralobstruction decreases renal prepro-epidermal growth factor andTamm-Horsfall expression. Kidney lot 42:89—94, 1992
23. WALTON G, BUTTYAN R, GARCIA-MONTES E, OLSSON CA, HENSLETW, SAWCZUK IS: Renal growth factor expression during the earlyphase of experimental hydronephrosis. J Urol 148:510—514, 1992
24. GESUALDO L, DI PAOLO S, CALABRO A, MILANI S, MAIORANO E,RANIERI E, PANNARALE G, SCHENA FP: Expression of epidermalgrowth factor and its receptor in normal and diseased human kidney.An immunohistochemical and in situ hybridization study. Kidney Int49:656—665, 1996
25. TAIRA T, YOSHIMURA A, IIzUICA. K, IWASAKI 5, IDEURA T, KOSHIKAWAS: Urinary epidermal growth factor levels in patients with acute renalfailure. Am J Kidney Dis 22:656—661, 1993
26. NIKOLIC-PATERSON DJ, TESCH GH, LAN HY, NUKn K, F0TI R,ATKINS RC: EGF and EGF-receptor expression in rat anti-Thy-imesangial proliferative nephritis. Nephrology 1:83—93, 1995
27. NAKOPOULOU L, STEFANAKI K, BOLETIS J, PAPADAKIS J, KOSTAKIS A,VOSNIDES GR, ZEIS PM: Immunohistochemical study of epidermalgrowth factor receptor (EGFR) in various types of renal injury.Nephrol Dial Transplant 9:764—769, 1994
28. CHOMCZYNSKI P, SACCHI N: Single step method of RNA isolation byacid guanidinium thiocyanate-phenol chloroform extraction. AnalBiochem 162:156—159, 1987
29. SAMBROOK J, FRITSCH EF, MANIATIS T: Molecular Cloning: A Labo-ratory Manual. Cold Spring Harbor, Cold Spring Harbor LaboratoryPress, 1989
30. MILANI S, HERBST H, SCI-IUPPAN D, HAHN EG, STEIN H: In situhybridization for pro-collagen types I, III and IV mRNA in normaland fibrotic rat liver: Evidence for predominant expression in nonparenchymal liver cells. Hepatology 10:84—92, 1989
31. GESUALDO L, DI PAOLO 5, MILANI 5, PINZANI M, GRAPPONE C,RANIERI E, PANNARALE G, SCHENA FP: Expression of platelet-derivedgrowth factor receptors in normal and diseased human kidney. J C/inInvest 94:50—58, 1994
32. SABOLIC I, VALENTI 0, VERBAVATZ JM, VAN HOEK AN, VERKMANAS, AUSIELLO DA, BROWN D: Localization of CHIP28 water channelin rat kidney. Am J Physiol 263:C1225—C1233, 1992
33. FOGAZZI GB, BANFI G, PONTICELLI C: Retrodiffusion of Tamm-Horsfall protein (THP) into the glomerular Bowman's space (GBS):A study by immunofluorescence (IF) on renal biopsies. (abstract)Nephrol Dial Transplant 9:891A, 1994
34. HIRANO T, AKIRA 5, TAGA T, KIsHIM0T0 T: Biological and clinicalaspects of interleukin 6. Immunol Today 11:443—449, 1990
35. LE J, VILCEK J: Biology of disease. Interleukin 6: A multifunctionalcytokine regulating immune reaction and the acute phase proteineresponse. Lab Invest 61:588—598, 1989
36. MURAGUCHI A, HIRANO T, TANG B, MATSUDA T, HoRn Y, NAKAJIMAK, KISHIMOTO T: The essential role of B cell stimulatory factor 2(BSF-2/IL-6) for the terminal differentiation of B cells. J Exp Med167:332—344, 1988
37. BAUER J, HERRMANN F: Interleukin-6 in clinical medicine. AnnHematol 62:203—210, 1991
38. BHARDWAJ N, SANTI-IANAM U, LAU LL, TATrER SB, GHRAYEB J,RIVELS M, STEINMANN RM, SEHGAL PB, MAY LT: IL-6/IFN/32 insynovial effusions of patients with rheumatoid arthritis and otherarthritides. Blood 73:1279—1284, 1989
39. BRANDT SJ, BODINE DM, DUNBAR CE, NIENHUIS AW: Dysregulatedinterleukin-6 expression produces a syndrome resembling Castelman'sdisease in mice. J C/in Invest 86:592—599, 1990
40. BREEN EC, REZAI AR, NAKAJIMA K, BEALL GM, MITSUYASU T,HIRANO RT, KISI-JIMOTO T, MARTINEZ-MAZA 0: Infection with HIV isassociated with elevated IL-6 levels and production. J Immunol144:480—484, 1990
41. MOSHAGE HJ, ROELOFS HNJ, VAN PELT JF, HAZENBERG BPC, VANLEEWEN MA, LIMBURG PC, AARDEN LA, YAP SH: The effect ofinterleukin-1, interleukin-6 and its interrelationship on the synthesisof serum amyloid A and C-reactive protein in primary cultures ofadult human hepatocytes. Biochem Biophys Res Comm 155:112—117,1988
42. JOURDAN M, BATAILLE R, SEGUIN J, ZHANG XG, CHAPTAL PA, KLEIN

Ranieri ci a!: Urinaiy IL-6/EGF ratio in IgA nephropathy 2001
B: Constitutive production of interleukin-6 and immunologic featuresin cardiac myxoma. Arthritis Rheum 33:398—403, 1990
43. RALL LB,Scovr J, BELLGI, CRAWFORD RJ, PENSHOW JD, COGHLANDJP: Mouse prepro-epidermal growth factor syntesis by the kidney andother tissue. Nature 313:228—231, 1985
44. SALIDO EC, YEN P1-I, ShAPIRo Li, FISHER DA, BARAJAS L: In situhybridization of pre-pro epidermal growth factor mRNA in the mousekidney. Am J Physiol 256:F632—F638, 1989
45. SALIDO EC, LAKSHMANAN J, FISHER DA, SHAPIRO Li, BARAJAS L:Expression of epidermal growth factor in the rat kidneys. An immu-nocytochemieal and in situ hybridization study. Histochemisty 96:65—72, 1991
46. CARPENTER G, COHEN S: Epidermal growth factor. Annu Rev Biochem48:193—216, 1979
47. FISHER DA, SALIDO EC, BARAJAS L: Epidermal growth factor and thekidney. Annu Rev Physiol 5 1:67—80, 1989
48. HARRIS RC: Potential Physiologic roles for epidermal growth factor inthe kidney. Am J Kidney Dis 17:627—630, 1991
49. HARRIS RC, HoovER RL, JACOBSON HR: Evidence for glomerularactions of epidermal growth factor in the rat. J Clin Invest 82:1028—1032, 1988
50. HARRIS RC, DANIEL TO: Epidermal growth factor binding stimulationof phosphoiylation and inhibition of gluconeogenesis in rat proximaltubule. J Cell Physiol 139:383—387, 1989
51. HARRIS RC: Response of rat inner medullary collecting duct toepiderma! growth factor. Am J Physiol 256:Fl117—F1123, 1989
52. FISHER DA, LAKSHMANAN J: Metabolism and effects of epidermalgrowth factor and related growth factors in mammals. Endrocrinol Rev11:418—422, 1990
53. VEHASKARI VM, HERING-SMITH KS, MOSKOWITZ DW, WEINER 1D,HAMM LL: Effect of epidermal growth factor on sodium transport inthe cortical collecting tubule. Am J Physiol 256:F803—F809, 1989
54. ENGEL J: EGF-like domains in extracellular matrix proteins: Local-ized signal for growth and differentation? FEBS Lett 251:1—7, 1989
55. GOODYER PR, MULLIGAN L, 000DYER CG: Expression of growth-related genes in human fetal kidney. Am J Kidney Dis 17:608-610,1991
56. RAASVELD MuM, WEENING Ji, KERST JM, SURACHNO 5, TEN BERGERiM: Local production of interleukin-6 during rejection in humanrenal allografts. Nephrol Dial Transplant 8:75—78, 1993
57. DUNCAN MR, BERMAN B: Stimulation of collagen and glucosamin-oglycan production in cultured human adult dermal fibroblast byrecombinant human interleukin 6.JlnvestDer,natol97:686—692, 1991
58. SA'Io T, ITO A, M0RI Y: Interleukin 6 enhances the production oftissue inhibitor of metalloproteinases (TIMP) but not that of matrixmetalloproteinases by human fibroblasts. Biochem Biophys Res Corn-mun 170:824—829, 1992





























