Embed Size (px)
Citation preview

International Journal of Cardiology. 4 (1983) 285-295
Elsevier
285
Thallium-201 scanning to decide CCU admission in patients with non-diagnostic electrocardiograms
L.R. van der Wieken ‘, G. Kan, A.J. Belfer, C.A. Visser, W. Jaarsma,
K.I. Lie, E. Busemann-Sokole, J. van der Schoot and D. Durrer
Department of Cardiology and Clinical Physiology and the Department of Nuclear Medicine, Wilhelmina
Gasthuis, Uniuersiiy of Amsterdam, and the Interuniversity Cardrological Institute. Eerste Helmersstraat 104, 1054 EG Amsterdam, The Netherlands
(Received 14 May 1982; second revision received 28 March 1983; accepted 26 May 1983)
Van der Wieken LR, Kan G, Beifer AJ, Visser CA, Jaarsma W, Lie KI, Busemann- Sokole E, Van der Schoot J, Durrer D. Thallium-201 scanning to decide CCU admission in patients with non-diagnostic electrocardiograms. Int J Cardiol 1983: 4:
285-295.
To determine the value of thallium-201 scintigraphy as a decisive factor in admission policy for patients with acute chest pain and nondiagnostic electrocardio- grams, we undertook a prospective study in 149 such patients. The interval between pain and scan never exceeded 12 hr. Of 57 patients in whom a defect was seen, 34 had an acute infarction, 7 developed infarction within 2 months, and in 11 coronary heart disease was proven by angiography or strongly suggested by stress tests (ECG and thallium-201 scan). In 13 patients with an equivocal scan, coronary heart disease was proven or strongly suggested in 5. Of 79 patients with a normal scan, only 1 had acute infarction, and stress tests were positive in 6 and negative in 72. In these 72 no cardiac event occurred during a l-year follow-up.
Thallium-201 scintigraphy can help to select those patients with acute chest pain and nondiagnostic electrocardiograms who need observation in a CCU.
Introduction
A growing number of patients are referred to our department each year because of acute chest pain. The limited number of coronary care beds and nursing staff, as
’ Present address: Ziekenhuis Ziekenzorg, De Ruyterlaan 5, 5711 JH Enschede, The Netherlands.
Reprint requests to: G. Kan. M.D., Department of Cardiology, Wilhelmina Gasthuis, Eerste Helmers- straat 104, 1054 EC Amsterdam, The Netherlands.
0167-5273/83/$03.00 0 i983 Elsevier Science Publishers B.V.
286
well as the rising costs of hospitalization and the potential risk of causing psycho-
logical harm by admitting a patient for coronary care, make a clear-cut and fairly
rigid admission policy mandatory. Admission to a coronary care unit (CCU) should
ideally be restricted to those patients with cardiovascular disease in whom close
monitoring is essential to immediate survival.
Many patients referred to an emergency ward because of acute chest pain are
immediately admitted to the CCU because they have both a suggestive or typical clinical history and an ECG diagnostic of acute myocardial infarction or ischemia. Another larger group can be discharged in the absence of either indication, or may
be admitted to an ordinary ward, usually internal medicine, if they need hospitaliza- tion.
Particular diagnostic problems are posed by those patients presenting with a
typical or suggestive clinical history but without diagnostic ECG changes when first seen. Until recently most of these patients were admitted to the CCU for observa- tion, where many were shown not to have acute myocardial infarction or ischemia or coronary heart disease at all. The potential value of acute thallium-201 scintigraphy as a means of recognizing acute myocardial infarction or ischemia in the early phase
after the onset of symptoms was studied prospectively in this particular group of patients.
Patients and Methods
In May 1978 a pre-coronary care unit was opened in our hospital. The purpose of this outpatient facility is to receive patients with acute chest pain with minima1
delay, and to come as quickly as possible to a diagnosis on which admission policy
and therapeutic strategy can be based. Patients entering this unit may be referred by a physician or may present on their own initiative. Median hospital arrival time
during the study period was 175 min. During the 10 months from May 1978 to March 1979 in which the prospective
study was performed, 2319 patients were seen on the pre-coronary care unit. Briefly the 2319 patients consisted of the following subgroups: myocardial infarction 484
(20.9%) unstable angina pectoris 336 (14.5%) stable angina 334 (14.4%) other manifestations of coronary heart disease 118 (5.1%), arrhythmias 239 (10.3%), other cardiac disorders 232 (lO.O%), aspecific chest pain 109 (4.7%) primary hyperventila- tion 146 (6.3%), and non-cardiac disease 321 (13.8%). Details have been published elsewhere [ 11.
Those patients who posed a clinical problem by presenting with a history
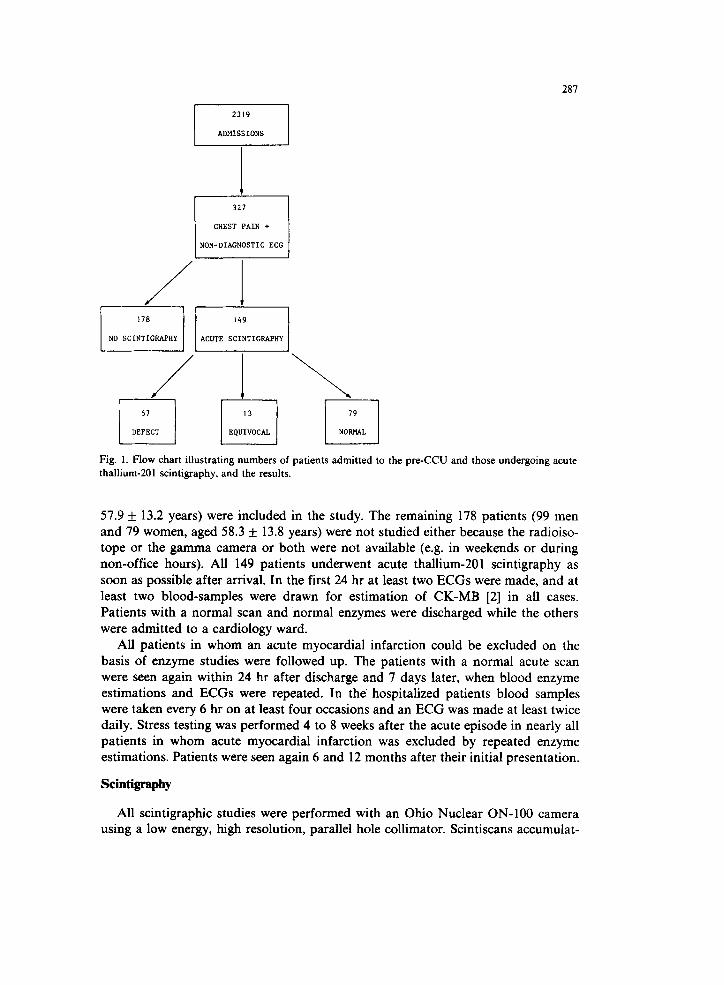
suggestive of or typical for an acute myocardial infarction or ischemia, but without diagnostic ECG changes, form the basis of this report (Fig. 1).
The interval between subsidence of pain and the time of scintigraphy never exceeded 12 hr. Patients whose clinical history and/or ECG demonstrated a previous myocardial infarction or in whom coronary artery disease had otherwise been proven before referral to our unit were excluded. No other selection criteria were applied, except that the radiopharmaceutical and the gamma-camera had to be available. A total of 149 patients (88 men and 61 women with a mean age f SD of
281
1 NON-DIAGNOSTIC ECG j
/
CHEST PAIN +
Fig. 1. Flow chart illustrating numbers of patients admitted to the pre-CCU and those undergoing acute
thallium-201 scintigraphy, and the results.
57.9 &- 13.2 years) were included in the study. The remaining 178 patients (99 men and 79 women, aged 58.3 + 13.8 years) were not studied either because the radioiso- tope or the gamma camera or both were not available (e.g. in weekends or during non-office hours). All 149 patients underwent acute thallium-201 scintigraphy as soon as possible after arrival. In the first 24 hr at least two ECGs were made, and at least two blood-samples were drawn for estimation of CK-MB [2] in all cases. Patients with a normal scan and ‘normal enzymes were discharged while the others were admitted to a cardiology ward.
All patients in whom an acute myocardial infarction could be excluded on the basis of enzyme studies were followed up. The patients with a normal acute scan were seen again within 24 hr after discharge and 7 days later, when blood enzyme estimations and ECGs were repeated. In the’ hospitalized patients blood samples were taken every 6 hr on at least four occasions and an ECG was made at least twice daily. Stress testing was performed 4 to 8 weeks after the acute episode in nearly all patients in whom acute myocardial infarction was excluded by repeated enzyme estimations. Patients were seen again 6 and 12 months after their initial presentation.
Scintigraphy
All scintigraphic studies were performed with an Ohio Nuclear ON-100 camera using a low energy, high resolution, parallel hole collimator. Scintiscans accumulat-

288
ing 300 Kcounts were obtained in three views, i.e. 45” left anterior oblique, anterior
and lateral. All scans were interpreted by two independent observers. Acute scans were obtained as soon as possible after arrival and 10 min after intravenous injection
of 1.7-2.5 mCi of thallium-201 chloride (Byk-Mallinkrodt). Acute scintigraphic
studies showing a consistent area of definitely diminished uptake in the left
ventricular myocardium on visual inspection in at least two views were read as
positive. Slight irregularities that are commonly seen in thallium-201 rest scans, were ignored, as was the so-called apical slit. Scans showing a defect in only one view, showing a consistent area of diminished activity higher than lung activity, or scans which the two observers did not agree upon, were classified as equivocal.
In patients who did not have myocardial infarction exercise scanning was performed at a later stage. A 20-gauge cannula was inserted in a forearm vein and a
12-lead ECG was recorded. The patients were exercised at zero load on an electri- cally braked bicycle ergometer for 1 min. after which work load was increased by 50 Watts every 2 min until one of the exercise end points was reached (v.i.). Thallium-201
was injected and the patient was exercised for 2 more min at the same or reduced
work load. Imaging was started within 6 min of the injection. Two hours after the exercise scan redistribution images were obtained. Scans were called positive when a
defect present on the immediate post-exercise scan disappeared or markedly di-
minished after redistribution. When no defect was seen on either the scan was considered normal. Normal scans and scans showing defects without redistribution
were considered negative for ischemia. Scans not classified as negative or positive were judged equivocal.
Electrocardiography
A standard 12-lead electrocardiogram was obtained in all patients on arrival before thallium-201 scintigraphy.’ Patients with ECGs showing at least one of the
following abnorma!ities in the absence of left bundle branch block were excluded from the study: (1) pathological Q waves of > 0.04 set duration (isolated Q waves in lead III were not considered evidence of infarction); (2) ST elevation of > 1 mm in standard leads, which could not be attributed to early repolarization; (3) horizontal or downsloping ST depression of > 1 mm; and/or (4) deeply negative precordial T
waves. Patients with complete or incomplete left bundle branch block were included in the absence of the signs of Cabrera [3] or Chapman [4]. Patients admitted to the CCU had ECGs taken at least daily. Those discharged after scintigraphy were
scheduled for a second ECG within 24 hr of the first, and further tracings were made
at follow-up visits at 1 week and at 6 and 12 months. During exercise testing a 12-lead ECG was recorded using a six-channel machine.
Exercise ECGs were considered positive if with the PR segment as the baseline, horizontal ST depression of at least 1 mm persisted for 0.08 set or more in any lead, in the absence of left bundle branch block or other severe conduction abnormalities such as preexcitation. In those cases the electrocardiogram on exercise was consid- ered uninterpretable. There were no patients with ST elevation on exercise. All patients (in sinus rhythm and off beta-blockers for at least 48 hr prior to exercise
289
testing) were exercised to a sinus tachycardia of at least 85% of the predicted
maximal value [5] unless they experience pain, arrhythmia, blood pressure drop or ST segment abnormalities prior to this.
Enzyme determination
In all patients blood samples were drawn approximately 6 hr after the beginning
of the attack of chest pain for determination of levels of CK-MB [2]. Those who
stayed in hospital had at least four other samples taken at 6-hourly intervals to
determine CK-MB peak value. Those who were discharged were scheduled for at
least one more sample within 24 hr of the onset of chest pain.
Diagnosis
Acute myocardial infarction was diagnosed in the presence of a typical rise and fall in CK-MB levels. The electrocardiographic development of diagnostic Q waves, loss of R waves, or T wave inversion was not essential to the diagnosis of acute myocardial infarction, but such changes were present in sequential ECGs in all but one of the patients diagnosed as having acute infarction.
A diagnosis of coronary artery disease was considered definite if there was: (1) myocardial infarction soon after admission or during follow-up; or (2) significant stenosis of > 70% in one or more major coronary arteries.
A diagnosis of coronary artery disease was considered probable on the basis of: (1) positive exercise ECG; or (2) positive exercise thallium-201 scan.
In patients with none of these findings the acute attack was thought to be of
non-cardiac origin.
Results
Acute scintigraphy
Of the 149 patients, 57 had positive, 13 had equivocal, and 79 had normal scans.
The average interval between subsidence of pain and the time of acute scintigraphy was 5, 6 and 5 hr respectively.
Electrocardiogram
The ECG was normal in 66 patients and showed non-specific ST segment changes in 68. These non-specific ECG-changes were flattening of T waves or slight ST-seg- ment depression (< 1 mm) in all but 5. These 5 patients had tall symmetric T waves,
progressing to ST-segment elevation after a few hours. Abnormal initial ventricular activation was present in 15. Abnormal ventricular activation was caused by the presence of the Wolff-Parkinson-White syndrome in 3, complete left bundle branch
block in 4, incomplete left bundle branch block in 2, and mere absence of normal Q waves in leads I, AVL and V6 in 6. The relation between acute scintigraphic and

290
TABLE 1
Relation between results of thallium-201 scintigraphy, ECG findings and history.
Acute scintigraphy Normal Non-specific
ECG ST changes
Abnormal
activation
History
typical
History
suggestive
Defect 51 24 23 a 10 45 12
Equivocal 13 6 6 I 10 3
Normal 19 36 39 4 36 43
Total 149 66 68 15 91 58
a Including 5 with hyperacute T-waves.
electrocardiographic findings is shown in Table 1. Of the 23 patients with defects on scanning and non-specific ECG-changes 21 progressed to infarction (transmural in 19 and sub-endocardial in 2). The 5 patients with hyperacute T-waves progressed to anteroseptal transmural infarctions.
Follow-up
Patients with a defect on acute scintigraphy (n = 57). Acute myocardial infarc- tion developed in 35 patients within 24 hr; in 26 the infarct was electrocardiographi- cally transmural. Four patients developed infarction between 1 and 7 days after admission and 3 more did so between 7 and 55 days. The total number of infarctions in this subgroup was 42 (Table 2). Moreover coronary angiography was performed in one patient on the 4th day and showed severe coronary artery disease; this case subsequently underwent bypass surgery.
Patients with equivocal scans (n = 13). Of these patients, who were all admitted to the CCU, 3 developed acute myocardial infarction within the first 24 hr. No infarctions occurred thereafter in the remaining 10 patients. The 3 infarctions in this subgroup were confined to the subset of patients with non-specific ECG abnormali- ties. There were no patients with hyperacute T waves in this subgroup.
TABLE 2
Results of acute scintigraphy vs. prevalence of acute myocardial infarction.
Acute scintigraphy AMI within
24 hr
AM1 between 1
and I days
AMI between I
and 55 days
Defect 51 35 4 3
Equivocal 13 3 0 0
Normal 19 1 0 0
Peak CK-MB
(U/l)
6-80 (mean 22.5)
16, 29, 25
12
Total 149 39 4 3
AMI-acute myocardial infarction.

291
Patients with normal scans (n = 79). Only 1 patient in this subgroup developed acute infarction within 24 hr, whilst the other 78 did not. This patient’s ECG was normal at presentation and during follow-up,
Fate of non-study patients. Of the 178 patients not included in the study 51 developed infarctions (transmural in 39 and subendocardial in 12). There was only one death, a patient with free wall rupture on the 3rd day of a transmural anteroseptal infarct. Thus there seems to have been no bias in the patients who were and who were not studied. We did not perform stress tests in these patients and follow-up was at the discretion of the patients’ own physicians.
Stress testing
In the three groups there remained a total of 102 patients (14, 10 and 78 respectively) who did not develop infarction. Stress testing was performed in all but
one 4 to 8 weeks after presentation (stress testing was not done in the patient who underwent early bypass surgery). The relation between acute scintigraphic results and the results of the stress tests is shown in Table 3. Coronary angiography was performed in 5 patients (2 with abnormal, 2 with equivocal and 1 with normal acute scans). Coronary artery disease was demonstrated in all 5 and all underwent bypass surgery. One male patient with severe hypertension, who had a normal a&ute scan, a positive exercise ECG and a normal exercise scan, died of an acute cerebrovascular accident 4 months after presentation. Autopsy was not performed.
None of the remaining 96 patients showed significant ECG changes during follow-up. Chest pain persisted in 9 patients. Four were considered having angina pectoris on the basis of a positive exercise ECG (1 patient) or positive exercise ECG
TABLE 3
Relation between acute scintigraphy and stress. testing after 4-8 weeks.
Acute scintigraphy Normal or
uninterpretable
ex. ECG and
normal or
equivocal
ex. scan
Normal or
uninterpretable
ex. ECG and
positive
ex. scan
Pos. ex. ECG
and normal
or equiv.
ex. scan
Pos. ex. ECG
and
pos. ex. scan
Defect 14 5 3b I 5
Equivocal 10 8’ 0 2 0
Normal 78 72 I 3’ 2d
Total 102 85 4 6 7
il Coronary artery disease proven by coronary angiography in 2 patients.
h Coronary artery disease proven by coronary angiography in 2 patients.
’ One severely hypertensive male.
d Coronary artery disease proven by coronary angiography in 1 patient.

292
TABLE 4
Relation between acute scintigraphy and final diagnosis.
Acute scintigraphy AM1 AMI at Proven or Probably
follow-up probable CAD non-cardiac
Defect 5-I 35 7 IO 5
Equivocal 13 3 0 4 6
Normal 79 I 0 6 72
Total 149 39 7 20 83
AM1 = acute myocardial infarction: CAD = coronary artery disease
and exercise scan (3 patients). One patient was shown to have mitral valve prolapse and 3 were thought to have non-cardiac pain (both exercise ECG and exercise scan
were normal). The 9th patient, a woman with positive exercise ECG and a normal exercise scan, experienced relief of symptoms after cholecystectomy for cholethiasis.
During the 12 months of follow-up the remaining 87 patients experienced no chest
pain or any other major complaint. Eighty of these patients had normal stress tests, rendering coronary artery disease highly unlikely. In 4, one test was positive (ECG in 3, scan i;n l), while in the remaining 3 both were positive. These patients probably had coronary artery disease.
At the end of follow-up one of the following diagnoses was made: acute myocardial infarction, acute infarction during follow-up, proven or probable coronary artery disease, and chest pain of non-cardiac origin. The relationship
between final diagnosis and the acute scintigraphic results is given in Table 4.
Sensitivity, specificity and predictive accuracy
Acute thallium-201 scans showing a defect have a 90% sensitivity and an 80%
specificity for detecting acute myocardial infarction developing within 24 hr if
equivocal scans are considered normal. The predictive accuracy of a positive test is
61% and the predictive accuracy of a negative test 96%. If equivocal scans are considered abnormal the figures are 97% for sensitivity, 71% for specificity, and 54% and 99% for positive and negative predictive accuracy, respectively.
In detecting significant coronary artery disease (including acute myocardial
infarction both within 24 hr and occurring during follow-up, as well as angiographi- tally demonstrated coronary artery disease) acute scanning with thallium-201 is 86% sensitive and 88% specific, if equivocal scans are counted as negative. The positive and negative accuracy then is 79% and 92%, respectively. If equivocal scans are counted as positive, sensitivity becomes 96% and specificity 79%; the predictive accuracy of a positive test now is 71% and that of a negative test 97%.

293
Discussion
Correlation of myocardiai infarction with results of acute scanning
Although 39 patients in this study sustained an acute infarction no definite diagnosis could be reached on the basis of history and ECG alone when they were
first seen in the unit. The result of thallium-201 scintigraphy was positive in 35 of
these patients and equivocal in 3. In the remaining patient the scan was negative after an interval of only 3 hr, a puzzling fact in the light of an earlier publication
showing a 100% correlation between the presence of acute myocardial infarction and scintigraphic abnormalities when scintigraphy was performed within 6 hr [6]. How- ever, the infarction was very small in this patient (peak CK-MB 12 U/l; normal up
to 4 U/l).
Significance in different groups of patients
Patients with normal scans. In the remaining 78 patients with a normal acute
scan no late infarctions occurred, and the one death in this group was not related to coronary artery disease. All the other patients had a favorable course and stress
testing suggested the presence of coronary artery disease in only 6. Thus the early discharge of all patients with a normal acute thallium-201 scan, made with a
maximal delay of 12 hr. seems to be a fairly safe policy in this particular group of
patients.
Patients with positive scans. In the 57 patients with a positive acute scan 35 had acute myocardial infarction, and 7 sustained infarction within 55 days. It seems most
likely that the defects seen on admission in patients with scintigraphic defects who developed their infarction only days to months later, reflected resting ischemia which
was still reversible at that time [7]. There was evidence of coronary artery disease in another 10 patients: in only 5 of
these patients signs and symptoms of coronary artery disease were absent on follow-up. In 2 of these 5 the original scintigraphic defect was still evident on exercise scintigraphy. Although prior infarction might account for these findings this
was not suggested by findings in the patients’ history or ECG. In the remaining 3 patients the defect seen on the acute scan had disappeared on the exercise scan.
Although spasm of the coronary arteries might explain this finding, this too was not suggested by the ECG. As these patients were symptom-free at follow-up we saw no
reason to explore this possibility by invasive procedures.
Patients with equivocal thallium scans. Of the 13 patients with equivocal scans 3
had acute infarction (sub-endocardial in all 3) and in 4 others there was either suggestive or definite evidence of coronary heart disease. In 6 patients no signs and symptoms of coronary disease were found at follow-up. Though the number of patients in this subgroup was too small to draw firm conclusions, the severity of trivascular coronary artery disease was striking in the 2 patients who underwent

294
coronary angiography. It appears prudent therefore, to consider an equivocal thallium-210 scan an indication for CCU admission in this particular group of patients. These conclusions are in accordance with those of Wackers et al. [8].
Limitations of the present study
In this study the diagnostic criteria of significant coronary artery disease in patients who were not submitted to angiography could be criticized as false-positive thallium stress tests have been shown to occur 191. False-positive exercise ECGs are much more common, and 6 of our patients probably had a false-positive stress ECG as these were accompanied by a normal or equivocal thallium stress scan. It is conceivable that some patients in this subgroup did not have significant coronary heart disease even though 5 of them were included under this heading. One of these 5 patients had severe hypertension and left ventricular hypertrophy. In this case pain was termed non-cardiac and the patient died 4 months later from a cerebrovascular accident.
Coronary angiography was performed in only a small number of patients. Although coronary angiography in all would have been the best method to rule out or in coronary artery disease, this was deemed unjustified because most patients experienced chest pain only once and were symptom-free afterwards. Even if coronary disease would have been detected in a few of these patients this would not have led to changes in treatment, as our policy is to operate only upon symptomatic patients who cannot be managed medically.
One could object against the different kinds of follow-up in those patients with normal scans and those with abnormal or equivocal scans, as this might lessen the chance of detecting subsequent pathology in the former. Our aim, however, was not to detect with the highest degree of certainty the presence of coronary artery disease or exclude it, but to decide which patients should be admitted to our limited number of very expensive CCU beds, and which patient could be safely dismissed. This goal was reasonably well met because in only one of the patients who were dismissed an infarct developed.
Although thallium-201 scanning is expensive the amount of money that can be saved by avoiding CCU admission in a large number of patients, is likely to outweigh this objection.
Conclusion
We conclude that a positive acute thallium-201 scan in the group of patients described in this study is a strong indicator of significant coronary artery disease and fully warrants admission to the CCU. An equivocal scan would also seem to be a fairly strong indicator for admission, although the number of patients in this group was small and precludes meaningful statistical analysis. It is of note that this latter group included 2 patients who were subsequently shown to have severe trivascular disease. On the basis of the data presented the early discharge of patients with negative scans seems justified, provided that the interval between the subsidence of

295
pain and acute scanning does not exceed 12 hr. In this group only 1 out of 79 patients suffered acute infarction, and it is in these patients that acute thallium-201 scintigraphy has its greatest value. It justifies early discharge thereby saving the patient admission to the CCU, which is likely to be of psychological, social and financial benefit.
Acknowledgements
We thank Pia Botman and Anita Nan-y for secretarial assistance.
References
1 Durrer D, Lie KI, Van der Wieken LR. Results of 24 hour a day outpatient facility for acute cardiac disease (Eerste Hart Hulp) in Amsterdam. Proc K Ned Akad Wet 1979;82:507-526.
2 Fiolet JWT, Willebrands AF, Lie KI, Ter Welle HF. Determination of creatine kinase enzyme MB (CK-MB): comparison of methods and clinical evaluation. Clin Chim Acta 1977;80:23-35.
3 Cabrera E, Friedland C. La onda de activation ventricular en el bloqueo de rama izquierda con infarto: un nuevo signo electrocardiografico. Arch Inst Cardiol Mexico 1953;23:441-450.
4 Chapman MG, Pierce ML. Electrocardiographical diagnosis of myocardial infarction in the presence of left bundle branch block. Circulation 1957; 16:558-571.
5 Sheffield LT, Holt JH, Reeves TL. Exercise graded by heart rate in electrocardiographic testing for angina pectoris. Circulation 1965;32:622-629.
6 Wackers FJTh, Bosemann-Sokole E, Samson G, Van der Schoot J, Durrer D. Value and limitations of thallium-201 scintigraphy in the acute phase of myocardial infarction. N Engl J Med 1976;295: l-5.
7 Wackers FJTh, Lie KI, Liem KL, Busemann-Sokole E, Samson G, Van der Schoot J, Durrer D. Thallium-201 scintigraphy in unstable angina pectoris. Circulation 1978;57:738-742.
8 Wackers FJTh, Lie KI, Liem KL, Busemann-Sokole E, Samson G, Van der School J, Durrer D. Potential value of thallium-201 scintigraphy as a means of selecting patients for the coronary care unit. Br Heart J 1979;41:111-117.
9 Bodenheimer MM, Banka VS, Helfant RH. Nuclear cardiology. II. The role of myocardial perfusion imaging using thallium-201 in diagnosis of coronary heart disease. Am J Cardiol 1980;45:674-684.





























