Embed Size (px)
Citation preview

Patient Safety
When Do Supervising Physicians Decide toEntrust Residents With Unsupervised Tasks?Anneke Sterkenburg, MD, Paul Barach, MD, MPH, Cor Kalkman, MD, PhD,Mathieu Gielen, MD, PhD, and Olle ten Cate, PhD
AbstractPurposePatient-care responsibilities stimulatetrainee learning but training maycompromise patient safety. The authorsinvestigated factors guiding clinicalsupervisors’ decisions to trust residentswith critical patient-care tasks.
MethodIn a mixed quantitative and qualitativedescriptive study carried out at UniversityMedical Center Utrecht, Utrecht, theNetherlands, from March to September2008, the authors surveyed attendinganesthetists and resident anesthetistsregarding when attendings shouldentrust each of six selected critical tasksto residents. The authors conductedstructured interviews with both groups,
using trigger case vignettes to solicitopinions on factors that affectentrustment decisions.
ResultsThirty-two attending anesthetists and 31residents answered the questionnaire(response rate 58%), and 10 participantsfrom each group were interviewed.Attendings varied in their opinionsregarding how much independence togive residents, particularly postgraduateyear (PGY) 2, 3, and 4 residents. PGY1residents reported working above theirexpected level of competence butestimate their own ability as sufficient,whereas PGY5 residents reportedworking below their expected level ofcompetence. The authors classified
factors that determine entrustment intofour groups: characteristics of theresident, the attending, the clinicalcontext, and the critical task.
ConclusionsResidents’ and attendings’ opinions andimpressions differ regarding what isexpected from residents, what residentsactually do, and what residents thinkthey can do safely. The authors listfactors affecting why and whensupervisors trust residents to proceedwithout supervision. Future studiesshould address drivers behindentrustment decisions, correlations withpatient outcomes, and tools that enablefaculty to justify their entrustmentdecisions.
Editor’s Note: A commentary on this article appearson pages 1399 –1400.
Deciding when a trainee is ready forunsupervised patient care is not easy.Early unsupervised care can impact thepatient’s safety, add to the cost of care,and increase liability for the supervisorand/or the organization. In contrast, notenough self-guided and independentdecision making may negatively affect thetrainee’s learning curve and timelyachievement of competence. Incompetency-driven postgraduate medicaltraining, residents must combine learningnew and critical materials with takingincreasing responsibility for safe patientcare.1,2 Learning cannot occur without afirst time to independently performprocedures and make decisions. One way
to approach this dilemma is to instate anumber of critical procedure attemptsresidents must successfully completebefore particular competency levels canbe assumed.3–5 Another approachincorporates qualitative performancefeedback, and given residents’ differentlearning curves, this one is perhaps moredefensible because supervisors decide toentrust a clinical or proceduralresponsibility to a resident deliberatelyand only after careful consideration—rather than automatically after a setamount of time. This crucial decisionshould be based on the trainee’s phase oftraining, on a valid assessment of his orher competence for the specific task, andon patient acuity.6 However, a myriad ofother factors also affect such decisions,and these are not well understood. Toour knowledge, no valid instrument isavailable to robustly assess, given thesevarying factors, the level of independencethat a trainee deserves.
Carrying out activities that are just at theedge of one’s competence can stimulatemaximum comprehension and a steeplearning curve,7,8 but a paucity of studiessupport this phenomenon in clinicalpractice.9 An educational psychology
term for doing something that is justbeyond the learner’s competence, or thegap between what the learner already cando and what he or she is about to learn todo, is “constructive friction.” Whensupervisors entrust learners, includingmedical trainees, with only routineactivities, learning is likely to be too slowor absent. Conversely, too muchresponsibility required at too early a stagemay result in adverse effects for—in thecase of medicine— both the patient andthe trainee. Educational psychologistshave labeled both of these situations“destructive friction.”9 –11
Ten Cate12 introduced the concept of“entrustable professional activity” (EPA)to signify the professional tasks thatmedical trainees need to master duringpostgraduate training that requireentrustment decisions by clinicalsupervisors. EPAs are useful units ofanalysis for establishing a competency-based curriculum. Ten Cate and Scheele13
used EPAs to define five levels ofresponsibility and proficiency (i.e.,having limited knowledge, acting underclose supervision, acting undersupervision on call, acting independently,and supervising others). They postulated
Please see the end of this article for informationabout the authors.
Correspondence should be addressed to Dr. tenCate, Center for Research and Development ofEducation, University Medical Center Utrecht, PO Box85500, 3508 GA Utrecht, the Netherlands;telephone: (!31) 88-755-7010; fax: (!31) 88-755-3409; e-mail: [email protected].
Acad Med. 2010;85:1408–1417.doi: 10.1097/ACM.0b013e3181eab0ec
Academic Medicine, Vol. 85, No. 9 / September 20101408
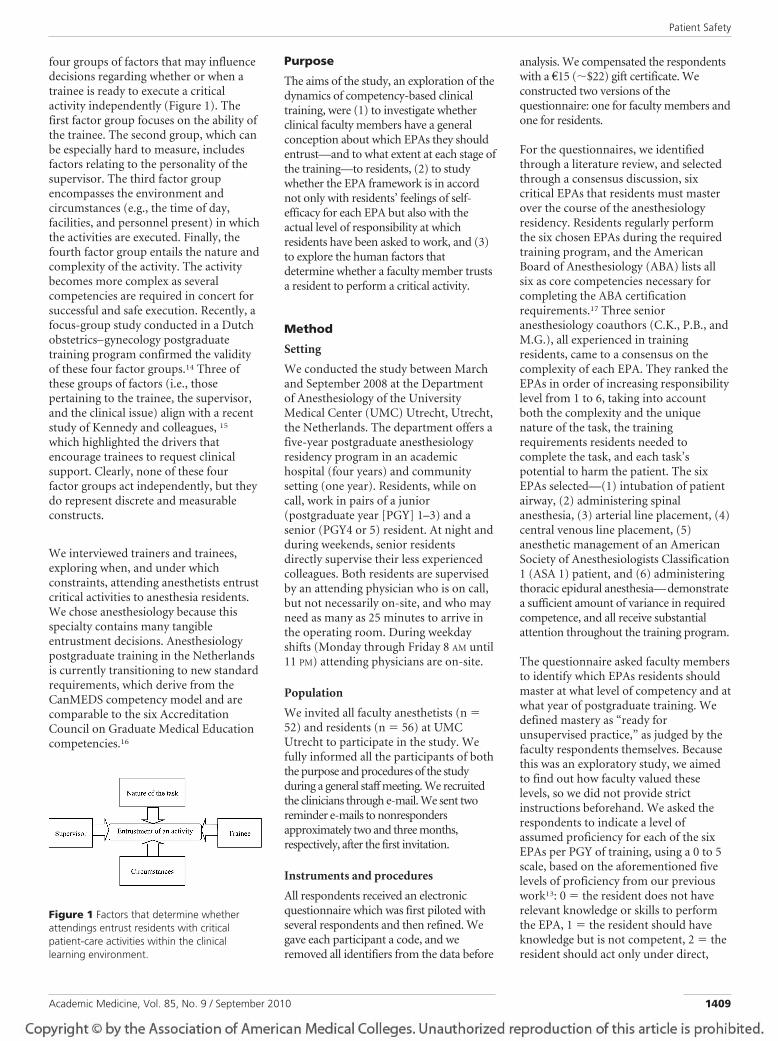
four groups of factors that may influencedecisions regarding whether or when atrainee is ready to execute a criticalactivity independently (Figure 1). Thefirst factor group focuses on the ability ofthe trainee. The second group, which canbe especially hard to measure, includesfactors relating to the personality of thesupervisor. The third factor groupencompasses the environment andcircumstances (e.g., the time of day,facilities, and personnel present) in whichthe activities are executed. Finally, thefourth factor group entails the nature andcomplexity of the activity. The activitybecomes more complex as severalcompetencies are required in concert forsuccessful and safe execution. Recently, afocus-group study conducted in a Dutchobstetrics–gynecology postgraduatetraining program confirmed the validityof these four factor groups.14 Three ofthese groups of factors (i.e., thosepertaining to the trainee, the supervisor,and the clinical issue) align with a recentstudy of Kennedy and colleagues, 15
which highlighted the drivers thatencourage trainees to request clinicalsupport. Clearly, none of these fourfactor groups act independently, but theydo represent discrete and measurableconstructs.
We interviewed trainers and trainees,exploring when, and under whichconstraints, attending anesthetists entrustcritical activities to anesthesia residents.We chose anesthesiology because thisspecialty contains many tangibleentrustment decisions. Anesthesiologypostgraduate training in the Netherlandsis currently transitioning to new standardrequirements, which derive from theCanMEDS competency model and arecomparable to the six AccreditationCouncil on Graduate Medical Educationcompetencies.16
Purpose
The aims of the study, an exploration of thedynamics of competency-based clinicaltraining, were (1) to investigate whetherclinical faculty members have a generalconception about which EPAs they shouldentrust—and to what extent at each stage ofthe training—to residents, (2) to studywhether the EPA framework is in accordnot only with residents’ feelings of self-efficacy for each EPA but also with theactual level of responsibility at whichresidents have been asked to work, and (3)to explore the human factors thatdetermine whether a faculty member trustsa resident to perform a critical activity.
Method
Setting
We conducted the study between Marchand September 2008 at the Departmentof Anesthesiology of the UniversityMedical Center (UMC) Utrecht, Utrecht,the Netherlands. The department offers afive-year postgraduate anesthesiologyresidency program in an academichospital (four years) and communitysetting (one year). Residents, while oncall, work in pairs of a junior(postgraduate year [PGY] 1–3) and asenior (PGY4 or 5) resident. At night andduring weekends, senior residentsdirectly supervise their less experiencedcolleagues. Both residents are supervisedby an attending physician who is on call,but not necessarily on-site, and who mayneed as many as 25 minutes to arrive inthe operating room. During weekdayshifts (Monday through Friday 8 AM until11 PM) attending physicians are on-site.
Population
We invited all faculty anesthetists (n "52) and residents (n " 56) at UMCUtrecht to participate in the study. Wefully informed all the participants of boththe purpose and procedures of the studyduring a general staff meeting. We recruitedthe clinicians through e-mail. We sent tworeminder e-mails to nonrespondersapproximately two and three months,respectively, after the first invitation.
Instruments and procedures
All respondents received an electronicquestionnaire which was first piloted withseveral respondents and then refined. Wegave each participant a code, and weremoved all identifiers from the data before
analysis. We compensated the respondentswith a !15 (#$22) gift certificate. Weconstructed two versions of thequestionnaire: one for faculty members andone for residents.
For the questionnaires, we identifiedthrough a literature review, and selectedthrough a consensus discussion, sixcritical EPAs that residents must masterover the course of the anesthesiologyresidency. Residents regularly performthe six chosen EPAs during the requiredtraining program, and the AmericanBoard of Anesthesiology (ABA) lists allsix as core competencies necessary forcompleting the ABA certificationrequirements.17 Three senioranesthesiology coauthors (C.K., P.B., andM.G.), all experienced in trainingresidents, came to a consensus on thecomplexity of each EPA. They ranked theEPAs in order of increasing responsibilitylevel from 1 to 6, taking into accountboth the complexity and the uniquenature of the task, the trainingrequirements residents needed tocomplete the task, and each task’spotential to harm the patient. The sixEPAs selected—(1) intubation of patientairway, (2) administering spinalanesthesia, (3) arterial line placement, (4)central venous line placement, (5)anesthetic management of an AmericanSociety of Anesthesiologists Classification1 (ASA 1) patient, and (6) administeringthoracic epidural anesthesia—demonstratea sufficient amount of variance in requiredcompetence, and all receive substantialattention throughout the training program.
The questionnaire asked faculty membersto identify which EPAs residents shouldmaster at what level of competency and atwhat year of postgraduate training. Wedefined mastery as “ready forunsupervised practice,” as judged by thefaculty respondents themselves. Becausethis was an exploratory study, we aimedto find out how faculty valued theselevels, so we did not provide strictinstructions beforehand. We asked therespondents to indicate a level ofassumed proficiency for each of the sixEPAs per PGY of training, using a 0 to 5scale, based on the aforementioned fivelevels of proficiency from our previouswork13: 0 " the resident does not haverelevant knowledge or skills to performthe EPA, 1 " the resident should haveknowledge but is not competent, 2 " theresident should act only under direct,
Figure 1 Factors that determine whetherattendings entrust residents with criticalpatient-care activities within the clinicallearning environment.
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 2010 1409

close supervision, 3 " the resident shouldact only under supervision on call, 4 "the resident should be able to actindependently, or 5 " the residentshould be able to supervise others.
The residents’ questionnaire requiredthem to rate their self-efficacy for eachEPA from 0 to 5, using a scale similar tothat of the attendings. We also asked theresidents, again using a similar 1 to 5scale, to indicate the highest level atwhich they had performed the givenactivities in the last three months.
We invited a random sample of 10supervising faculty members and 10residents to participate in follow-upinterviews. A secretary picked names inrandom order from an existing list. Wepersonally informed all participantsabout the interview process and assuredtheir confidentiality. We offeredinterviewees a !50 ($75) gift certificatefor completing the interview. A senioranesthetist from a different academicmedical center who was not involved inthe UMC Utrecht residency training orsupervision (M.G.) conducted in-personinterviews with faculty members. Ayoung physician trainee, not involved inthe anesthesiology training program(A.S.), conducted in-person interviewswith the residents. The interviews weresemistructured and lasted about 30 to 45minutes. We gave the same guidance toboth interviewers, and they both askedthe same questions in the same order. Weused two emergency night case vignettesas triggers to explore factors thatinfluence entrustment decisions. Inaddition to the case vignettes, wepresented to faculty members a list of allpossible resident pairs, in each programyear, and asked them to indicate, first,which of the two residents they wouldchoose to perform a specific task and,second, what factors would make themtrust one resident over the other. Theinterviewers (A.S. or M.G.) audio-recordedthe 20 interviews, and A.S. transcribedthem verbatim, removing all identifiersfrom the transcripts. The interviewers(M.G. and A.S.) also took extensive fieldnotes during the interview process.
Data analysis
The questionnaire data were analyzedwith statistical software (SPSS Inc.,Chicago, Illinois; version 15.0). Wecalculated frequencies, mean scores, andthe discrepancy scores between faculty
members’ and residents’ answers. Weused qualitative data analysis software(MAXQDA, Berlin, Germany; version2007) to analyze the interview transcripts.The analysis began by open coding, thatis, sorting and labeling the data bycontent. We attempted to place the datainto one of the four predefined categoriesdescribed above (Figure 1). For example,after the interviewer presented a casevignette, one attending might say, “Thispatient is obese, has a beard … there are alot of risks involved. I would definitelycome if a resident is young or notexperienced enough in my eyes.” Wewould assign this comment the maincategory code “Nature of the task” andthe subcode “The risk of (severe)complication,” plus the main code“Factor in the resident” and subcodes“resident’s stage of training” and “resident’sestimated experience.” A.S. did all initialcoding. Then, all of us further refined thecategories (e.g., what to include in“circumstances”) through discussions.After all the quotes were coded, we countedthem. We used the frequency of commentsand the fact that some interviewees clearlynoted some reasons for trust as mostimportant to create a rank order ofimportance within each of the fourcategories.
Ethical considerations
We minimized the potential harm toresidents and faculty by having a juniorphysician (A.S.), not employed in thehospital and not acquainted with therespondents, carry out the residentinterviews. We employed a senioranesthesiologist (M.G.) not employed bythe hospital, to carry out the facultyinterviews. We ensured the confidentialityof the interviewees and stressed thevoluntary nature of the interviews. Theinterviews started with an explanation ofthe purpose of the study, and nointerviewees indicated that their risk ofparticipating exceeded the benefits of thisstudy. Because we invited all eligibleresidents and faculty to participate,equitability was not an issue. All transcribedinterviews were coded before analysis andseen only by A.S., M.G., O.t.C., and asecretarial assistant. We coded allquestionnaires before processing them. Wesought informed consent at threemoments: during a staff meeting, in apersonal e-mail to each potentialparticipant, and during an introductoryexplanation preceding the interview. Wedid not have participants sign an informed
consent form because we allowedparticipants to opt out at any time.
Results
Characteristics of the respondents
Of the 52 attending anesthetists involvedin postgraduate training, 32 (62%)completed the questionnaire. Nineteenrespondents (59%) were male, and 13(41%) were female. The mean age of theattendings was 46 (range: 32–61; SD:8.8). Half of the attending anesthetistspracticed general anesthesiology, whereasthe others worked in subspecialties: 4(13%) worked in pediatricanesthesiology, 3 (9%) in pediatriccardiothoracic anesthesiology, 4 (13%) inadult cardiothoracic anesthesiology, and1 (3%) in intensive care. Three attendings(9%) were fellows. We categorized facultyrespondents into three groups based onyears of practice and experience inpostgraduate training with cutoff pointsat 5 and 15 years. Thirteen facultymembers (41%) were junior attendings($5 years of experience), 12 (37%) wereintermediate (5–15 years of experience),and 7 (22%) were senior (%15 years).
Of the 56 residents, 31 (55%) completedthe questionnaire. Of these, 12 (39%)were male, and 19 (61%) were female.The mean age of the residents was 31years (range: 24 –39; SD: 3.7). The studypopulation consisted of 7 PGY1 residents(23%), 5 PGY2 residents (16%), 4 PGY3residents (13%), 9 PGY4 residents (29%),and 6 PGY5 residents (19%).
All of the participants whom we initiallyapproached for interviews agreed toparticipate. Of the faculty members whoparticipated in an interview, 3 (30%)were junior, 5 (50%) intermediate, and 2(20%) senior. Six out of 10 (60%)provided anesthesia for general surgery, 2(20%) for adult cardiothoracic surgery, 1(10%) for general pediatric surgery, and 1(10%) for pediatric cardiothoracicsurgery. Three (30%) of the residentsinterviewed were PGY1, 5 (50%) werePGY4, and 2 (20%) were PGY5. Half ofthe residents who were interviewed werejunior, and the other half were seniorresidents. (The pediatric rotation in thefourth year concludes the junior stage oftraining, which explains why some PGY4residents are still junior.)
We found no significant differences on anyparameters between the participating
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 20101410
attendings and residents and the totalpool of attendings and residents, butthere were slightly (nonsignificant)more female resident respondents andslightly (nonsignificant) fewer seniorattending respondents.
Expected levels of proficiency atsubsequent stages of training
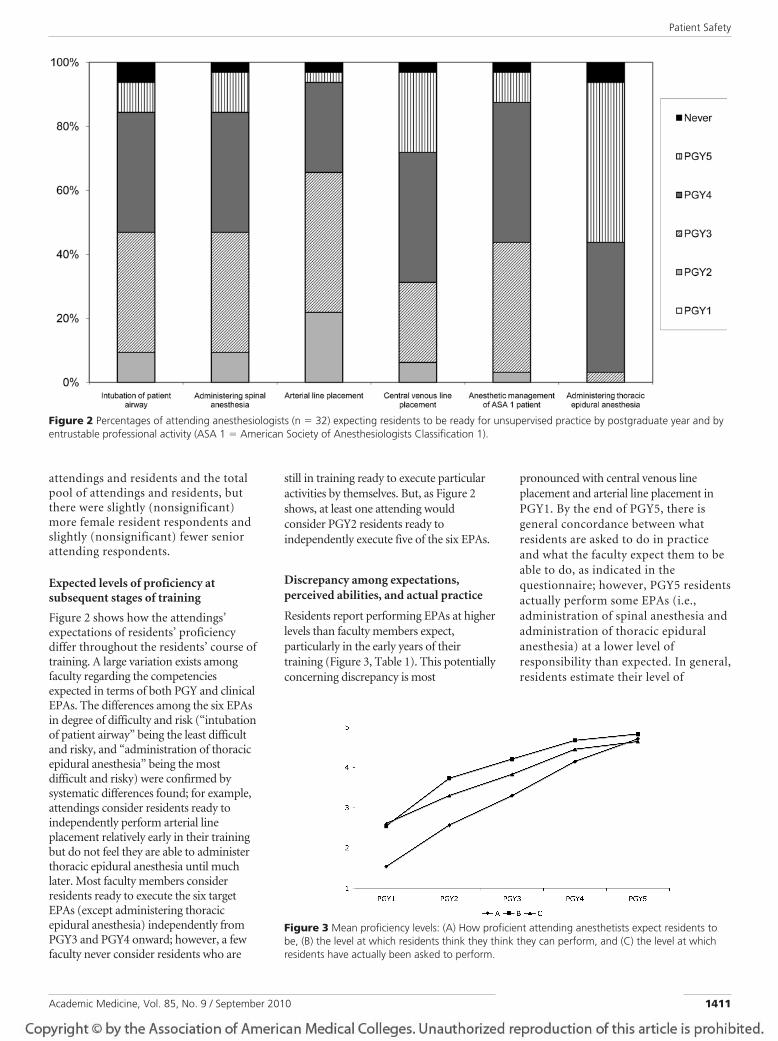
Figure 2 shows how the attendings’expectations of residents’ proficiencydiffer throughout the residents’ course oftraining. A large variation exists amongfaculty regarding the competenciesexpected in terms of both PGY and clinicalEPAs. The differences among the six EPAsin degree of difficulty and risk (“intubationof patient airway” being the least difficultand risky, and “administration of thoracicepidural anesthesia” being the mostdifficult and risky) were confirmed bysystematic differences found; for example,attendings consider residents ready toindependently perform arterial lineplacement relatively early in their trainingbut do not feel they are able to administerthoracic epidural anesthesia until muchlater. Most faculty members considerresidents ready to execute the six targetEPAs (except administering thoracicepidural anesthesia) independently fromPGY3 and PGY4 onward; however, a fewfaculty never consider residents who are
still in training ready to execute particularactivities by themselves. But, as Figure 2shows, at least one attending wouldconsider PGY2 residents ready toindependently execute five of the six EPAs.
Discrepancy among expectations,perceived abilities, and actual practice
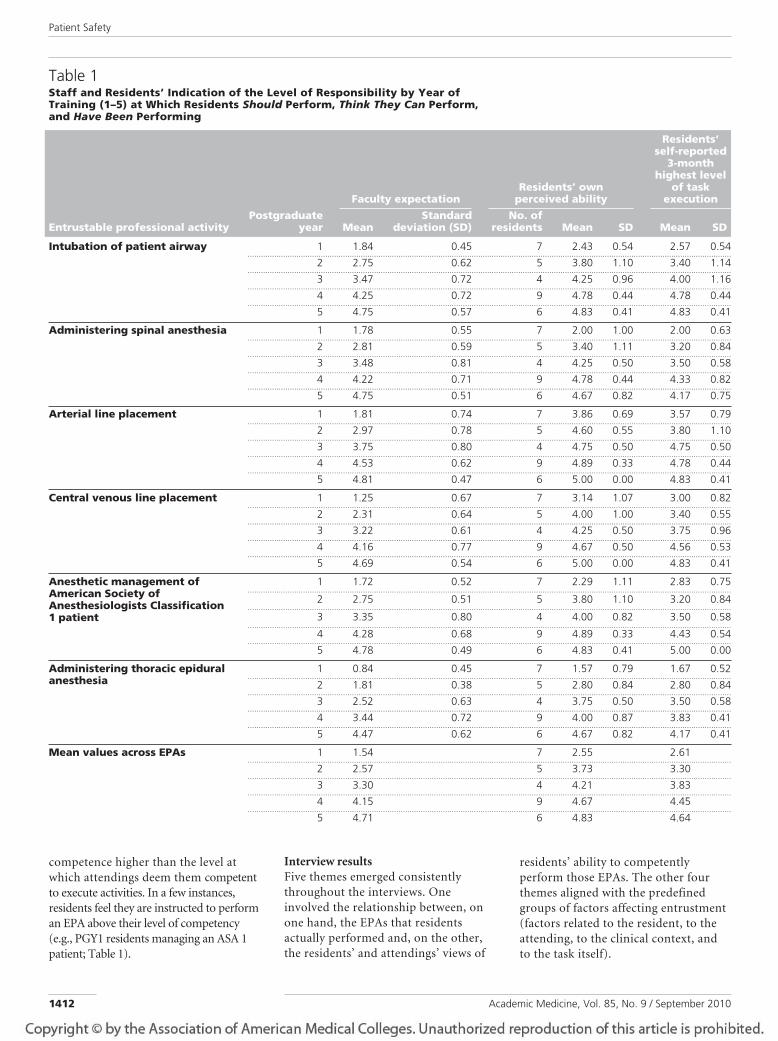
Residents report performing EPAs at higherlevels than faculty members expect,particularly in the early years of theirtraining (Figure 3, Table 1). This potentiallyconcerning discrepancy is most
pronounced with central venous lineplacement and arterial line placement inPGY1. By the end of PGY5, there isgeneral concordance between whatresidents are asked to do in practiceand what the faculty expect them to beable to do, as indicated in thequestionnaire; however, PGY5 residentsactually perform some EPAs (i.e.,administration of spinal anesthesia andadministration of thoracic epiduralanesthesia) at a lower level ofresponsibility than expected. In general,residents estimate their level of
Figure 2 Percentages of attending anesthesiologists (n " 32) expecting residents to be ready for unsupervised practice by postgraduate year and byentrustable professional activity (ASA 1 " American Society of Anesthesiologists Classification 1).
Figure 3 Mean proficiency levels: (A) How proficient attending anesthetists expect residents tobe, (B) the level at which residents think they think they can perform, and (C) the level at whichresidents have actually been asked to perform.
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 2010 1411
competence higher than the level atwhich attendings deem them competentto execute activities. In a few instances,residents feel they are instructed to performan EPA above their level of competency(e.g., PGY1 residents managing an ASA 1patient; Table 1).
Interview resultsFive themes emerged consistentlythroughout the interviews. Oneinvolved the relationship between, onone hand, the EPAs that residentsactually performed and, on the other,the residents’ and attendings’ views of
residents’ ability to competentlyperform those EPAs. The other fourthemes aligned with the predefinedgroups of factors affecting entrustment(factors related to the resident, to theattending, to the clinical context, andto the task itself).
Table 1Staff and Residents’ Indication of the Level of Responsibility by Year ofTraining (1–5) at Which Residents Should Perform, Think They Can Perform,and Have Been Performing
Entrustable professional activityPostgraduate
year
Faculty expectationResidents’ own
perceived ability
Residents’self-reported
3-monthhighest level
of taskexecution
MeanStandard
deviation (SD)No. of
residents Mean SD Mean SD
Intubation of patient airway 1 1.84 0.45 7 2.43 0.54 2.57 0.54..........................................................................................................................................................................................................................
2 2.75 0.62 5 3.80 1.10 3.40 1.14..........................................................................................................................................................................................................................
3 3.47 0.72 4 4.25 0.96 4.00 1.16..........................................................................................................................................................................................................................
4 4.25 0.72 9 4.78 0.44 4.78 0.44..........................................................................................................................................................................................................................
5 4.75 0.57 6 4.83 0.41 4.83 0.41
Administering spinal anesthesia 1 1.78 0.55 7 2.00 1.00 2.00 0.63..........................................................................................................................................................................................................................
2 2.81 0.59 5 3.40 1.11 3.20 0.84..........................................................................................................................................................................................................................
3 3.48 0.81 4 4.25 0.50 3.50 0.58..........................................................................................................................................................................................................................
4 4.22 0.71 9 4.78 0.44 4.33 0.82..........................................................................................................................................................................................................................
5 4.75 0.51 6 4.67 0.82 4.17 0.75
Arterial line placement 1 1.81 0.74 7 3.86 0.69 3.57 0.79..........................................................................................................................................................................................................................
2 2.97 0.78 5 4.60 0.55 3.80 1.10..........................................................................................................................................................................................................................
3 3.75 0.80 4 4.75 0.50 4.75 0.50..........................................................................................................................................................................................................................
4 4.53 0.62 9 4.89 0.33 4.78 0.44..........................................................................................................................................................................................................................
5 4.81 0.47 6 5.00 0.00 4.83 0.41
Central venous line placement 1 1.25 0.67 7 3.14 1.07 3.00 0.82..........................................................................................................................................................................................................................
2 2.31 0.64 5 4.00 1.00 3.40 0.55..........................................................................................................................................................................................................................
3 3.22 0.61 4 4.25 0.50 3.75 0.96..........................................................................................................................................................................................................................
4 4.16 0.77 9 4.67 0.50 4.56 0.53..........................................................................................................................................................................................................................
5 4.69 0.54 6 5.00 0.00 4.83 0.41
Anesthetic management ofAmerican Society ofAnesthesiologists Classification1 patient
1 1.72 0.52 7 2.29 1.11 2.83 0.75..........................................................................................................................................................................................................................
2 2.75 0.51 5 3.80 1.10 3.20 0.84..........................................................................................................................................................................................................................
3 3.35 0.80 4 4.00 0.82 3.50 0.58..........................................................................................................................................................................................................................
4 4.28 0.68 9 4.89 0.33 4.43 0.54..........................................................................................................................................................................................................................
5 4.78 0.49 6 4.83 0.41 5.00 0.00
Administering thoracic epiduralanesthesia
1 0.84 0.45 7 1.57 0.79 1.67 0.52..........................................................................................................................................................................................................................
2 1.81 0.38 5 2.80 0.84 2.80 0.84..........................................................................................................................................................................................................................
3 2.52 0.63 4 3.75 0.50 3.50 0.58..........................................................................................................................................................................................................................
4 3.44 0.72 9 4.00 0.87 3.83 0.41..........................................................................................................................................................................................................................
5 4.47 0.62 6 4.67 0.82 4.17 0.41
Mean values across EPAs 1 1.54 7 2.55 2.61..........................................................................................................................................................................................................................
2 2.57 5 3.73 3.30..........................................................................................................................................................................................................................
3 3.30 4 4.21 3.83..........................................................................................................................................................................................................................
4 4.15 9 4.67 4.45..........................................................................................................................................................................................................................
5 4.71 6 4.83 4.64
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 20101412
Working, related to supposed level ofability. Residents were comfortable withthe training program’s expectations.They did not think that executingactivities with more supervision thanthey thought they needed hamperedtheir learning, but they usually did not
perceive performing above theirexpected level of competence asuncomfortable or unsafe either.
Yes, it happens sometimes that I receivesupervision on activities I have done bymyself many times before. Yoursupervisor is your trainer and assessor, so
I understand. Also, they can give youpointers on how to improve your skills.(Resident, PGY1)
I think it is a good thing that supervisorswatch you perform occasionally. Youmight think you are doing fine, and thatyou do not need any supervision anymore, but that might just be the pointwhere you start making mistakes.(Resident, PGY4)
Yes, sometimes I do perform activities ona higher level, but since there is alwayssupervision around, these areopportunities for me to grow. (Resident,PGY4)
You learn to work independently,especially in the second year of training[done in community hospital]. When Ido not feel competent, when I do nottrust myself, I just tell my boss I needhelp. When you ask for supervision, youalways receive it. (Resident PGY4)
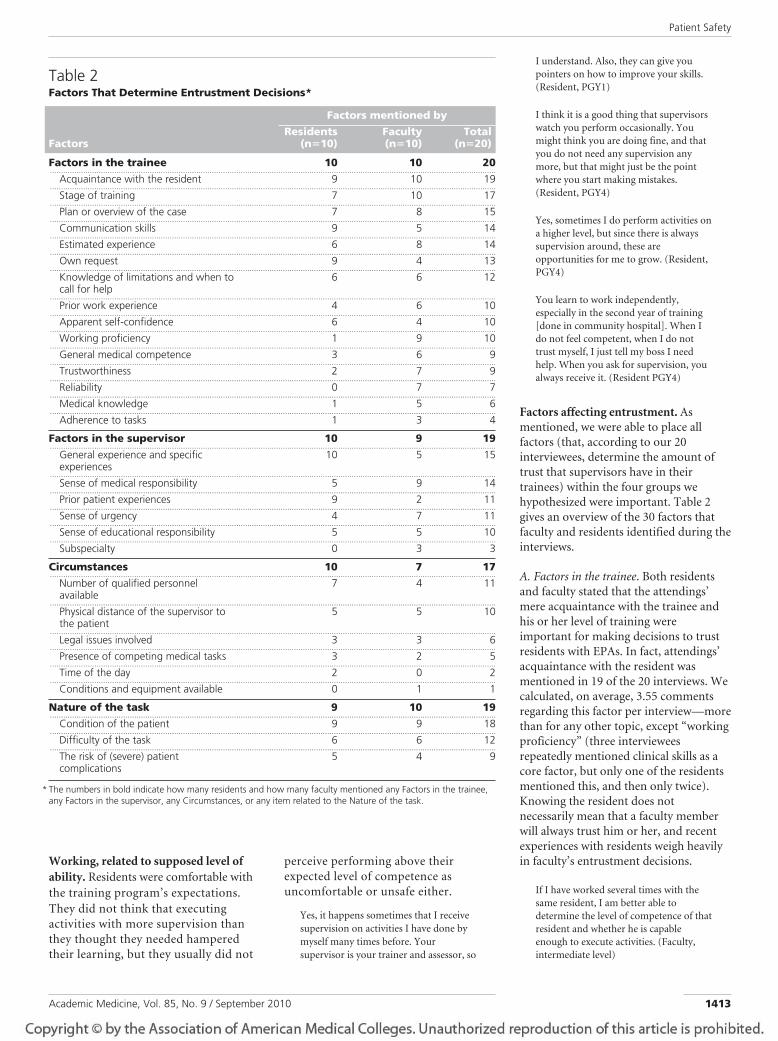
Factors affecting entrustment. Asmentioned, we were able to place allfactors (that, according to our 20interviewees, determine the amount oftrust that supervisors have in theirtrainees) within the four groups wehypothesized were important. Table 2gives an overview of the 30 factors thatfaculty and residents identified during theinterviews.
A. Factors in the trainee. Both residentsand faculty stated that the attendings’mere acquaintance with the trainee andhis or her level of training wereimportant for making decisions to trustresidents with EPAs. In fact, attendings’acquaintance with the resident wasmentioned in 19 of the 20 interviews. Wecalculated, on average, 3.55 commentsregarding this factor per interview—morethan for any other topic, except “workingproficiency” (three intervieweesrepeatedly mentioned clinical skills as acore factor, but only one of the residentsmentioned this, and then only twice).Knowing the resident does notnecessarily mean that a faculty memberwill always trust him or her, and recentexperiences with residents weigh heavilyin faculty’s entrustment decisions.
If I have worked several times with thesame resident, I am better able todetermine the level of competence of thatresident and whether he is capableenough to execute activities. (Faculty,intermediate level)
Table 2Factors That Determine Entrustment Decisions*
Factors
Factors mentioned byResidents
(n!10)Faculty(n!10)
Total(n!20)
Factors in the trainee 10 10 20.........................................................................................................................................................................................................
Acquaintance with the resident 9 10 19.........................................................................................................................................................................................................
Stage of training 7 10 17.........................................................................................................................................................................................................
Plan or overview of the case 7 8 15.........................................................................................................................................................................................................
Communication skills 9 5 14.........................................................................................................................................................................................................
Estimated experience 6 8 14.........................................................................................................................................................................................................
Own request 9 4 13.........................................................................................................................................................................................................
Knowledge of limitations and when tocall for help
6 6 12
.........................................................................................................................................................................................................Prior work experience 4 6 10
.........................................................................................................................................................................................................Apparent self-confidence 6 4 10
.........................................................................................................................................................................................................Working proficiency 1 9 10
.........................................................................................................................................................................................................General medical competence 3 6 9
.........................................................................................................................................................................................................Trustworthiness 2 7 9
.........................................................................................................................................................................................................Reliability 0 7 7
.........................................................................................................................................................................................................Medical knowledge 1 5 6
.........................................................................................................................................................................................................Adherence to tasks 1 3 4
Factors in the supervisor 10 9 19.........................................................................................................................................................................................................
General experience and specificexperiences
10 5 15
.........................................................................................................................................................................................................Sense of medical responsibility 5 9 14
.........................................................................................................................................................................................................Prior patient experiences 9 2 11
.........................................................................................................................................................................................................Sense of urgency 4 7 11
.........................................................................................................................................................................................................Sense of educational responsibility 5 5 10
.........................................................................................................................................................................................................Subspecialty 0 3 3
Circumstances 10 7 17.........................................................................................................................................................................................................
Number of qualified personnelavailable
7 4 11
.........................................................................................................................................................................................................Physical distance of the supervisor tothe patient
5 5 10
.........................................................................................................................................................................................................Legal issues involved 3 3 6
.........................................................................................................................................................................................................Presence of competing medical tasks 3 2 5
.........................................................................................................................................................................................................Time of the day 2 0 2
.........................................................................................................................................................................................................Conditions and equipment available 0 1 1
Nature of the task 9 10 19.........................................................................................................................................................................................................
Condition of the patient 9 9 18.........................................................................................................................................................................................................
Difficulty of the task 6 6 12.........................................................................................................................................................................................................
The risk of (severe) patientcomplications
5 4 9
* The numbers in bold indicate how many residents and how many faculty mentioned any Factors in the trainee,any Factors in the supervisor, any Circumstances, or any item related to the Nature of the task.
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 2010 1413
I call my supervisor and tell him I think Ican handle the case, but if he has neverseen me work … I think that makes ithard for him to determine whether or nothe can trust me. (Resident, PGY1)
Faculty also consider the quality andcomprehensiveness of the trainee’s planto be important. This considerationincludes an estimation of the trainee’spreparation and insight into potentialpatient complications that may occur inchoosing one clinical plan over anotherplan.
When a resident consults me, I value thequality of his plan highly when making adecision in the amount of trust I give.Having little to add to his plan gives meconfidence that he can handle the case.(Faculty, intermediate level)
I think it is important for my supervisorsto hear me present the case in an orderlyand complete way, which shows them Iknow what I am doing. (Resident, PGY4)
For faculty, competence is not entirelydependent on the year of training.Interviewees acknowledged learningcurve differences among residents.
Residents’ competencies can differ withintheir year of training, especially in the firstyear of training. When a resident hasworked at an intensive care unit prior tostarting residency training I tend to putmore trust in him than if he would havestarted residency training straight aftermedical school. Also, some residentsevolve faster while others need more timeto master skills. (Faculty, intermediatelevel)
In general, faculty assume moreindependence in senior residents, as theseresidents are supposed to be ready tograduate soon and become certifiedspecialists. For junior residents,attendings state that the clinicalexperience, such as managing acute carepatients prior to residency, is important.
If a first-year resident has already workedat an ICU for two years, I will probably lethim execute activities, such as arterial lineaccess, more independently than a first-year resident who entered the programstraight after medical school. (Faculty,intermediate level)
If residents state that they do not feelconfident, they generally receivesupervision, whether or not a facultymember trusts a resident to execute anactivity.
When a resident asks me to assist him, Iwill, even if I do not think it is reallynecessary. (Faculty, senior level)
Sometimes, your supervisor will ask you ifyou want him to come; when you admityou do, there is never any discussion, hewill come, no questions asked. (Resident,PGY4)
Attendings consider whether a resident isaware of his or her limitations to be veryimportant.
This resident performs well, but Isometimes have trouble assessing what Ican trust him to do. He does not seem toknow when he needs to call for help.(Faculty, intermediate level)
I think it is important that my supervisorcan trust that I will call before I get intotrouble. (Resident, PGY4)
The supervisor’s knowledge of thetrainee’s clinical skills and workingmanners is also important.
This resident is very skilled and knowswhat he is doing. (Faculty, senior level)
Clearly, supervisors’ knowledge of theresident’s competencies and attitudesweighs on their judgment. We have theimpression that the mere lack ofacquaintance leads to fewer independentresponsibilities and more scrutiny andthat, conversely, the mere fact that thesupervisor knows the resident generallyleads to more readily grantedresponsibilities.
B. Factors in the supervisor. All residentsmentioned that characteristics of thesupervisor, such as their generalexperience and specific expertise, canaffect entrustment decisions.
There are differences among supervisors;I think it has to do with their experience.For example, a more senior boss has moreexperience in assessing residents and willhave fewer problems letting a residentperform certain tasks independently thanwould a junior supervisor. (Resident,PGY1)
I think a supervisor who has recently losta patient in a similar case will just come, ifonly for his own confidence. (Resident,PGY4)
I made a deal with him: “You can watchor try once, and you have to tell me whatyou see.” He failed to do both. I had poorjudgment; it was misplaced trust on myside. That situation had its effect later on.A week later, he again was my juniorresident, and thinking back, I believe I didnot let him do as much as I wouldnormally have allowed him to do.(Resident, PGY5)
Attendings stated that whether or notthey actually oversee a procedure is notalways balanced against trustingthe resident, but it also depends on theresponsibility they feel for both thepatient and the residents they train.
You just have to be there for yourresident, even though you know he canprobably handle the case just fine.(Faculty, intermediate level)
As a supervisor, you are responsible forwhat goes on in your practice. (Faculty,intermediate level)
The amount of trust can be influenced bythe attitude of the supervisors towardclinical training.
It is necessary for a resident’s confidenceto perform on his own sometimes. Iusually peek through the OR window tomake sure he is doing well, so I’m therewithout the resident realizing I am.(Faculty, senior level)
C. Circumstances. Attendings state thatentrustment decisions also depend on theclinical environment, including thequality and availability of the teamsurrounding the resident.
It is also important whether or not myresident gets enough support from otherteam members. (Faculty, senior level)
It makes a difference whether the juniorwho is with me on call is in his first or inhis third year; faculty members knowthat. (Resident, PGY5)
After 11 PM, an attending can take calleither at home or in the hospital.Decisions on whether or not to entrustresidents with clinical tasks are affectedby the attendings’ whereabouts.
It depends on where I am. In thisparticular situation, if I am at home I willcome to the hospital. If I am already here,I would tell my resident to call me whenhe needs me. (Faculty, junior level)
I live too far away to go home when I amon call. And since I am already here … it’seasy to just be there and see how myresident is doing. (Faculty, junior level)
It makes a difference where my supervisoris. If he is at home, he will have to decideif he can trust me to perform on my own,whether or not it is necessary to postponeexecution of activities for 15 minutes orso. If he is here already … it’s easier, hewill be here whether it is really necessaryor not. (Resident, PGY4)
Residents also stated that the time of dayand mere convenience can each be a
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 20101414

factor in the amount of trust that anattending places in them.
This may sound strange, but also the timeof day…. It can make a difference whenyou call your supervisor at 11 PM, whenhe is still awake and alert, or in the middleof the night. When you wake him, I thinksometimes he might be less eager tocome. (Resident, PGY4)
It’s contradictory sometimes. Forexample, during the day, you receive fullsupervision on a spinal needle placementon an ASA 2 patient who comes in for anACL reconstruction, and in the middle ofthe night I find myself managing an ASA3 patient without supervision. (Resident,PGY4)
D. Type of activity. Both faculty andresidents stated that the condition of thepatient, the team, and discrete steps ofthe EPA are important in entrustingdecisions.
For such a complicated case I will justcome, the risks are too high. (Faculty,intermediate level)
I think the most important [thing] for myboss is the case, how the patient is doing.(Resident, PGY4)
Discussion
We explored when and why attendinganesthesia specialists decide to trustresidents to execute critical patient-caretasks. Residents’ and attendings’expectations differ with regard to what isexpected from residents, what residentsactually do, and what residents think theycan do safely.
Attendings generally agree more on thelevels of responsibility residents shouldhave at the beginning and end of trainingthan in their views about how muchresponsibility residents should have inthe intervening years (PGY2–4). Onesurveyed faculty member would not fullyentrust any resident with any EPA at anystage. It is tempting to speculate on thereasons for these differences amongfaculty, but any suggestions would needfurther analysis. Our impression is thatoverbearing attendings may lead residents tobe more hesitant, resulting in attendingstrusting residents less, whereas open andengaging attendings likely give the residentspace to grow and think, resulting in greatertrust. More in-depth studies are needed tosubstantiate this speculation.
Residents, especially trainees in PGY1, 2,and 3, estimate their own abilities higher
than attendings consider justified.Interestingly, PGY1 residents reportedthat, in the last three months, they hadbeen assigned responsibilities beyond thelevel that attendings on average indicateas justified for this stage. The residentsthemselves see few problems with thissituation, as they also perceive theirabilities to usually meet or exceed thosenecessary to perform these assignments.To determine whether residentsoverestimate their abilities or not isdifficult. Successfully and independentlyexecuting a critical activity that exceedsone’s expected ability, if nocomplications occur, may boostresidents’ self-efficacy.18 Self-confidenceis needed to stimulate furtherdevelopment, and it may be natural, eveneducationally necessary, for trainees tooverestimate their ability somewhat.However, the supervisor’s judgment tolimit independent execution of EPAs iscritical if a trainee’s overconfidence maycompromise patient safety (e.g., whenairway intubations take longer than theyshould, thoracic epidurals overshoot theepidural space, or central lines requireseveral needle punctures).
We found substantial differences amongsurveyed attendings’ views of whichactivities residents should be able tohandle across varying stages of training.Factors related to individual residents,the clinical circumstances, or the natureof the EPA affect differences across EPAs,but factors related to the supervisor seemespecially important for individual EPAs(Figure 2). This greater importance couldreflect the supervisor’s estimation of thedifficulty or complexity of the EPAs and hisor her estimation of the risk to patients.
Through the interviews, we identified 30factors that influence entrustmentdecisions. All of these factors fit withinthe four categories we defined in anearlier study13: factors related to theresident, supervisor, clinicalcircumstances, and patient-care task.Given the expected levels of proficiencyat different stages of training, themultitude of factors involved helpsexplain the differences among theattendings’ entrustment decisions.
The appropriate amount of trustattendings should place in a resident in aparticular year of training cannot bedetermined in a generalized sense butmust be individually customized to the
trainee. In fact, supervisors must judgethe interplay of factors related to the (1)resident, (2) the EPA, and (3) the clinicalcircumstances, including the facilities andthe available clinical support of themicrosystem.19,20 Table 2 may thereforeserve as a first step in developing anentrustment decision support model andchecklist. Sufficient acquaintance withthe resident, the resident’s stage oftraining, the availability of otherpersonnel, the difficulty of the task, therisk of complications, and the conditionof the patient all seem important. Thesefactors may appear self-evident; however,they presently create much ambivalenceand anxiety among faculty, and notunderstanding these factors and theirinterplay could potentially lead to muchambiguity and patient harm. Forexample, the finding that the quality ofpatient care is inadvertentlycompromised during the time of the yearwhen more inexperienced residents areemployed in hospitals allows hospitalleaders to act on that information.21
We suggest that these factors may beoperationalized in a robust manner andgive faculty the tools to make betterdecisions when faced with decidingwhether to entrust residents withclinical activities.
We recognize several limitations to thestudy. We confined our study to a singleDutch anesthesia training program, andthus our findings need to be replicated inother clinical settings to determineexternal generalizability. Further,qualitative studies involving interviewsbear an inherent risk of subjectivitybecause the interviewer can influence thenature of the interview, and otherresearchers may find different themes. Tominimize these risks, we structured ourinterviews with a carefully scriptedinterview guide, and we identifiedrelevant factors using factor analysis andtheme saturation. We assessed only sixEPAs, and assessing other clinicaldomains might yield additional factors,but these would most likely overlap withthe factors we identified above.
To our knowledge, this is the first timea study has assessed the opinions ofindividual faculty and trainees onentrustment decisions. Dijksterhuis andcolleagues14 conducted a related, focus-group study among obstetrics–gynecologyfaculty and trainees, but our study yields
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 2010 1415

factors on a more detailed, generalizable,and actionable level. Dijksterhuis andcolleagues make a conceptual distinctionbetween levels of competence and degreesof independence, whereas we consider thelevel of competence a measure of thetrainee. In another study of internists andemergency medicine physicians, Kennedyand colleagues15 used a similarmethodology but from a different angle.Their questions was not, “When dosupervisors entrust responsibility?” but,rather, “When do trainees ask for help?”They found that factors in the resident,factors in the supervisor, and the nature ofthe clinical question (i.e., those related tothe EPA) determine the requests.Requesting help from an attending anddeciding to trust a resident are intimatelyrelated, and we feel the Kennedy andcolleagues’ study supports our findings. Inanother recent qualitative study, Ginsburgand colleagues22 interviewed 19experienced internal medicine attendingson qualities of outstanding, average, andproblematic residents. They came up witheight clusters of factors, based on agrounded theory approach, that are similarto our findings (Table 2, “Factors in thetrainee”), but they also uncoveredadditional resident qualities, such as workethic, leadership skills, and impact on staff.These factors do not overlap with ours but,rather, seem to supplement them. Thisindicates that further studies will be helpfulto complete the picture of factors that affectdecisions to entrust critical care to trainees.
Finally, we hope this study will help toimprove postgraduate training. Thestudy’s findings fit into the competency-based postgraduate training models thathave emerged in recent years.2,13,20,23–25
Construct assessments that address bothtrainee competence and patient safety arenecessary. Current methods of assessingclinical competence, which use durationof training as a major criterion, may notbe sufficient. Assessments should includeboth measuring the amount of trustattendings place in residents andunderstanding why they do so.Understanding entrustment decisionsand including them in assessing andpromoting trainees will lead to physicianswho are competent, safe, andtrustworthy.6,24
Future studies might include a more in-depth analysis of the mechanisms that
determine supervisors’ decisions toentrust residents with patient-care tasks.These studies might aim to validlymeasure these decisions or to understandwhether and how entrustment decisionscan play an important part in assessingtrainees. If entrustment decisions can bebetter validated, they may lead to moreformalized statements of awardedresponsibility that could be included asmilestones in a trainee’s competencyportfolio.13,26 Such an advance couldaccelerate the development of acompetency-based training program.These programs support patient andprovider educational outcomes, and theyare more influenced by the quality of careand the providers’ actions than the mereeducational content or duration of thetraining program.
Dr. Sterkenburg was, at the time of this study,research associate, Center for Research andDevelopment of Education, University MedicalCenter Utrecht, Utrecht, the Netherlands.
Dr. Barach was, at the time of this study,anesthetist, Department of Anesthesiology; hecurrently is visiting researcher, Patient Safety Center,University Medical Center Utrecht, Utrecht, theNetherlands.
Dr. Kalkman is professor of anesthesiology,Department of Anesthesiology, and director, PatientSafety Center, University Medical Center Utrecht,Utrecht, the Netherlands.
Dr. Gielen is senior anesthetist, University MedicalCenter St. Radboud, Nijmegen, the Netherlands.
Dr. ten Cate is professor of medical education anddirector, Center for Research and Development ofEducation, University Medical Center Utrecht,Utrecht, the Netherlands.
Funding/Support: None.
Ethical approval: This study was exempt fromethical approval by the ethical review board ofthe University Medical Center Utrecht, Utrecht,the Netherlands (See also “Method / Ethicalconsiderations,” above).
Conflicts of interest: None.
Previous presentations: Some of the results of thisstudy were orally presented at the 2009 meetingof the Association for Medical Education inEurope (Malaga, Spain) and the 2009 AnnualMeeting of the American Society ofAnesthesiologists (New Orleans, Louisiana).
References1 AAMC policy guidance on graduate medical
education: Assuring quality patient care andquality education. Acad Med. 2003;78:112–116.
2 Leung WC. Competency based medicaltraining: Review. BMJ. 2002;325:693–696.
3 Konrad C, Schupfer G, Wietlisbach M,Gerber H. Learning manual skills inanesthesiology: Is there a recommendednumber of cases for anesthetic procedures?Anesth Analg. 1998;86:635–639.
4 de Oliveira Filho GR. The construction oflearning curves for basic skills in anestheticprocedures: An application for thecumulative sum method. Anesth Analg. 2002;95:411–416.
5 Sites BD, Gallagher JD, Cravero J, LundbergJ, Blike G. The learning curve associated witha simulated ultrasound-guided interventionaltask by inexperienced anesthesia residents.Reg Anesth Pain Med. 2004;29:544 –548.
6 Ten Cate O. Trust, competence and thesupervisor’s role in postgraduate training.BMJ. 2006;333:748 –751.
7 Vygotsky LS. Chapter 6: Interaction betweenlearning and development. In: Cole M, John-Steiner V, Scribner S, Souberman E, eds.Mind in Society: The Development of HigherPsychological Processes. Cambridge, Mass:Harvard University Press; 1978:79 –91.
8 Cantillon P, Macdermott M. Doesresponsibility drive learning? Lessons fromintern rotations in general practice. MedTeach. 2008;30:254 –259.
9 Kennedy TJ, Regehr G, Baker GR, LingardLA. Progressive independence in clinicaltraining: A tradition worth defending? AcadMed. 2005;80(10 suppl):S106 –S111.
10 Vermunt JD, Verloop N. Congruence andfriction between learning and teaching. LearnInstr. 1999;9:257–280.
11 Ten Cate O, Snell L, Mann K, Vermunt J.Orienting teaching toward the learningprocess. Acad Med. 2004;79:219 –228.
12 Ten Cate O. Entrustability of professionalactivities and competency-based training.Med Educ. 2005;39:1176 –1177.
13 Ten Cate O, Scheele F. Competency-basedpostgraduate training: Can we bridge the gapbetween theory and clinical practice? AcadMed. 2007;82:542–547.
14 Dijksterhuis MG, Voorhuis M, TeunissenPW, et al. The assessment of competence andprogressive independence in postgraduateclinical training. Med Educ. 2009;43:1156 –1165.
15 Kennedy T, Regehr G, Baker GR, Lingard L.Preserving professional credibility: Groundedtheory study of medical trainees’ requests forclinical support. BMJ. 2009;338:b128.
16 Scheele F, Teunissen P, Van Luijk S, et al.Introducing competency-based postgraduatemedical education in the Netherlands. MedTeach. 2008;30:248 –253.
17 The American Board of Anesthesiology.Examinations and certifications. Available at:http://www.theaba.org/Home/examinations_certifications. Accessed June 1, 2010.
18 Bandura A. Social Foundations of Thoughtand Action: A Social Cognitive Theory.Englewood Cliffs, NJ: Prentice-Hall; 1986.
19 Mohr J, Batalden P, Barach P. Integratingpatient safety into the clinical microsystem.Qual Saf Health Care. 2004;13(suppl 2):ii34 –ii38.
20 Long DM. Competency-based residencytraining: The next advance in graduatemedical education. Acad Med. 2000;75:1178 –1183.
21 Haller G, Myles PS, Taffe P, Perneger TV, WuCL. Rate of undesirable events at beginning of
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 20101416
academic year: Retrospective cohort study.BMJ. 2009;339:b3974.
22 Ginsburg S, McIlroy J, Oulanova O,Eva K, Regehr G. Toward authenticclinical evaluation: Pitfalls in thepursuit of competency. Acad Med. 2010;85:788 –786.
23 Ten Cate O, Snell L, Carraccio C. Medicalcompetence: The interplay between
individual ability and the health careenvironment. Med Teach. In press.
24 Carraccio C, Wolfsthal SD, Englander R,Ferentz K, Martin C. Shifting paradigms:From Flexner to competencies. Acad Med.2002;77:361–367.
25 Carraccio CL, Benson BJ, Nixon LJ, DerstinePL. From the educational bench to theclinical bedside: Translating the Dreyfus
developmental model to the learning ofclinical skills. Acad Med. 2008;83:761–767.
26 Brigham TP, Nasca TJ. ACGME, milestones,and CBET: Grieving the old world andaccepting the new. Acad Intern Med Insight.2009;7(3):17–19. Available at: http://www.im.org/Publications/Insight/Archives/V7I3/Documents/brigham73.pdf. Accessed May 17,2010.
Patient Safety
Academic Medicine, Vol. 85, No. 9 / September 2010 1417





























