Embed Size (px)
Citation preview
CCU Collect.
LB 1778 .C6 D5 2004 Text
COASTAL CAROLINA UNIVERSITY
DISTINGUISHED
TEACHER-SCHOLAR
LECTURER SERIES presents
Sharon H. Thompson
"Nine Nutrition Tips for a Healthier South Carolina''
Coastal Carolina University Kimbel LibraryOctober 21, 200
DISTINGUISHED
TEACHER-SCHOLAR
LECTURER SERIES
The intent of the Distinguished Teacher-Scholar Lecturer Series is to recognize annually a Coasta l Caro lina University faculty member who has distinguishe d himself or herself as a teacher, scholar, and communicator. The awardee is an individual who embodies the University's teacher-scholar ideal of searching for and transmitting knowledge through critical inquiry and teaching in his or her discipline and who supports and appreciates critical inquiry and teaching in the other disciplines of the University. The Committee that recommends selection of the awardee is unique in that it comprises faculty members and representa tives from the student body, staff, administration, and community.
The Distinguished Teacher-Scholar Lecturer Series is made possible through the generous support of
Horry Telephone Cooperative, Inc.
Coasta l Carolina University Distinguished Teacher-Scholar Lecturer Series
Colleen A. Lohr, editor This Series is copyrighted by
Coastal Carolina University ©2004
Dedication
This manuscript is dedicated to the glory of God. I am most grateful for the blessings I am sent daily from
my family, friends, colleagues, and students.
------
Introduction Nutrition confusion abounds in our country. What kind of diet
should one choose-low-fat, low-carb, high-protein , vegetarian, high-fiber, or functional foods? In the age of Internet and global communication-along with an increasing interest in nutrition and health-it is not surprising that Americans remain confused about nutrition. In addition, much of the nutrition information reported by the media is sensational, insufficient, or taken out of context. According to the ADAs Nutrition and You: Trends 2000 survey, 48% of consumers named television as their main source of nutrition information, followed by magazines at 47%, and newspapers at 18%. Doctors (1 %) and dietitians (1 %) were rarely cited. 1
Accompanying this increased interest in nutrition information is
an explosion of books and food products promoting weight loss. The pursuit of dieting has become an American way of life as weight loss books have taken permanent residence on our bestseller lists. Net carbs and fat grams are the current staple of conversations at work as well as at dinner parties. It seems ironic that while Americans contin
ue to diet and buy weight loss products, we are also eating away from home more often, choosing larger portion sizes, and increasing our daily caloric consumption. The "American way" seems to be to overeat, diet, overeat, diet-in a vicious cycle. In the midst of all of this chaos, many people have lost their sense of perspective regarding such basic concepts as hunger, satiety, taste, and peace of mind.
Unfortunately, our culture is one that thrives on quick fixes for busy lives. We want to lose weight in 24 hours after taking a magical pill that makes the entire process easy. Frustration from trying one fad diet after another often promotes binge eating and night eating syndrome. Also, when our sole goal is to lose weight, we are willing to try anything, regardless of whether it is a healthy choice or not.
It is important to remember that even very small steps toward better nutritional habits will equal big health benefits and weight loss over time.
This study will counter some of the food and nutrition misinfor
mation by summarizing research findings from a wide array of scientific, credible sources. The information presented here is not a quick fix, but a lifestyle nutrition plan. Nine nutrition tips will be outlined here along with information on causes of death that are related to poor nutritional choices-with a special emphasis on statistics from
2
South Carolina. These nutrition suggestions provide a plan to avoid obesity and also help provide protection from some of the chronic diseases that are the major causes of death in our state and nation. Think of these suggestions as one lifestyle plan to prevent many chronic health problems.
The major premise offered in this lifestyle nutritional plan is simple. Enjoy food and do not ban foods from your diet. One does not have to ban foods, try hundreds of fad diets, or live a "food-deprived" life to eat properly and well. Think in terms of foods you should select more often rather than ones to remove from your daily diet.
Learning about nutrition can encourage positive change in attitudes, beliefs, and behaviors, but it does not necessarily translate into healthier eating. Changing nutrition habits can be quite difficult. Positive self-talk, realistic beliefs and goals, and problem-solving efforts are important for success in healthier eating.
Please note that food is not a "cure" and eating properly will not prevent all diseases. Genetics and environmental factors both play significant roles in the development of certain diseases. I do, however, ask that you keep an open mind and consider adopting these nutrition suggestions in your everyday food selection. If you feel better as a result of eating right each day, that may be more important than how long you live.
Many sources claim to provide "education" when they are really
promoting products or books. Often those who publish books also sell products to "assist" in weight loss. The good news here is that this
book is free as a part of the HTC Distinguished Teacher-Scholar series. So, enjoy the fruits of my labor as a teacher and researcher in the area of public health nutrition at Coastal Carolina Universityand thank HTC for sponsoring this award.
How "healthy'' is South Carolina? South Carolina is a beautiful state and a nice place to live.
Unfortunately, we usually have dismal rankings for health status compared to the other 49 states. For example, for the past two years South Carolina has ranked 48th of the 50 United States in a national study on healch. 2 It is, therefore, not surprising chat our state also ranks 1 Och in the nation for death rates (age-adjusted rates per 100,000 population: SC= 979.9; US = 868.3). 3
South Carolina's health problems are due to many factors. For example, socioeconomic status plays a role in the state's low health rankings and high death rates as we are 25th in the nation for uninsured population. 3 Other reasons for our poor rankings include high incidences of poor diet, smoking, lack of exercise, poor health care attitudes, high cost of prescription drugs, infrequent visits to the doctor, and the disparity among racial and income groups concerning health care accessibility.4
What are the top 10 leading causes of death in our state and nation and which might be related to nutritional choices?
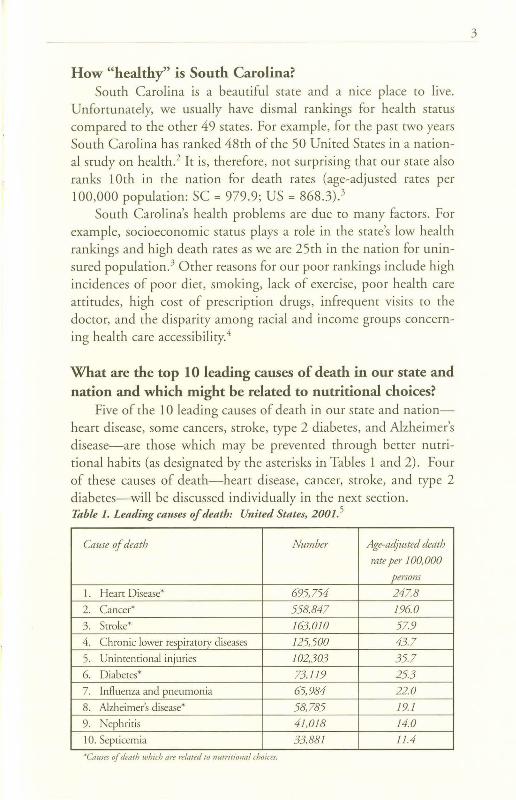
Five of the 10 leading causes of death in our state and nationheart disease, some cancers, stroke, type 2 diabetes , and Alzheimer 's disease-are those which may be prevented through better nutritional habits (as designated by the asterisks in Tables 1 and 2). Four of these causes of death-heart disease, cancer, stroke, and type 2 diabetes-will be discussed individually in the next section. Table I. Leading causes of death: United States, 2001. 5
Cause of death Number Age-adjusted death
rate per I 00, 000
persom
1. Heart Disease* 695,754 247.8
2. Cance r* 558,847 196.0
3. Stroke* 163,010 57.9
4. C hronic lower respiratrny diseases 125,500 43.7
5. Unintentional injuries 102,303 35.7
6. Diab etes* 73,119 25.3
7. Influenza and pneumonia 65,984 22.0
8. Alzheimer's disease* 58,785 19. I
9. Nephritis 41,0 18 14.0
I 0. Septicemia 33,881 11.4
·Causes of death which are re/med to nutr itional choices.
3
4
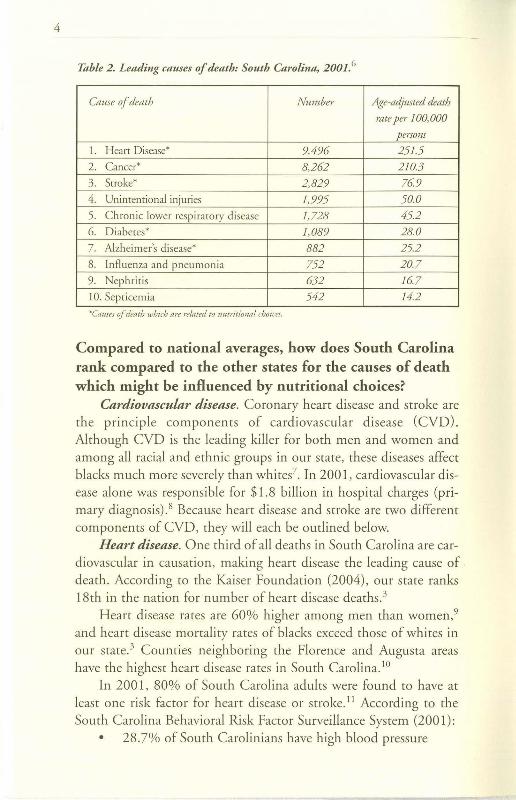
Table 2 . Leading causes of death: South Carolina, 200 I. 6
Cause of death Num ber Age-adjusted death
rate per 100,000
persons
I. Heart Disease* 9,496 25 1.5
2. Ca ncer* 8,262 2 10.3
3. Stroke* 2,829 76 9
4. Unintentional injuries 1,995 50.0
5. Chroni c lower respir ator y disease 1,728 45.2
6. Di abetes* 1,089 28.0
7. Alzheimer's disease* 882 25.2
8. Influ enza and pn eum onia 752 20.7
9. Ne phriti s 632 167
I 0. Septicemia 542 14.2
'"'Causes of death which are related to nutritional choices.
Compared to national averages, how does South Carolina rank compared to the other states for the causes of death which might be influenced by nutritional choices?
Cardiovascular disease. Coron ary heart disease and stroke are the principle components of cardiovascular disease ( CVD). Although CVD is the leading killer for both men and women and among all racial and ethnic groups in our state, these diseases affect blacks much more severely than whites 7. In 2001, cardiovascular disease alone was responsibl e for $ 1.8 billion in hospital charges (primary diagnosis) .8 Because heart disease and stroke are two different components of CVD, they will each be outlined below.
Heart disease . One third of all death s in South Carolin a are cardiovascular in causation, making heart disease the leading cause of death. According to the Kaiser Foundation (2004), our state ranks 18th in the nation for numb er of heart disease deaths. 3
Heart disease rates are 60% higher among men than women ,9 and heart disease mortality rates of blacks exceed those of whites in our state. 3 Counties neighboring the Florence and Augusta areas have the highest heart disease rates in South Carolin a.10
In 2001 , 80% of South Carolina adults were found to have at least one risk factor for heart disease or stroke. 11 According to the South Carolina Behavioral Risk Factor Surveillance System (2001):
• 28 .7% of South Carolinians have high blood pressure
• 27.6% have high blood cholesterol • 8.1 % have diabetes • 26% are current smokers • 61.3% are overweight or obese (BMI of25 or higher). 11
Stroke. Stroke, the number three cause of death in South Carolina, is responsible for approximately 8% of mortality. 11 South Carolina ranks first in the nation for number of stroke deachs.3
Portions of our state , along with Georgia and North Carolina, have become known as the "Stroke Belt" because of the high stroke mortality rates. Furthermore, the Pee Dee region and our coastal area of South Carolina are known as the "Stroke Buckle" of the "Stroke Belt" because of the exceptionally high rates of stroke deaths. 12
There are racial and gender differences in rates of stroke morbidity and mortality. In our state, rate of stroke deaths is 59% higher among blacks than whices,9 and men carry a 25% greater chance of stroke as compared co women. 13
Cancer. Cancer is the second leading cause of death in our state, causing 23% of all mortality. 9 According to the Kaiser Family Foundation, our state ranks 11 ch in the nation for number of cancer deaths per 100,000 persons. 3
There are racial and gender disparities in South Carolina death rates as blacks are 1.4 times more likely to die from cancer-related causes than whites, and cancer death races for males are 75% higher for men than women. 9
The top four cancer types diagnosed in our state (accounting for 59% of new cancer diagnoses) are prostate, lung, female breast , and colon/rectum cancers . 14 Although breast cancer is the most commonly diagnosed cancer in women and is the second leading cause of death among South Caro lina women, lung cancer is the leading cause of cancer deaths for men and women in our state. People are ofren surprised to discover chat deaths from lun g cancer are equal to deaths from colon/rectum, breast, and prostate cancers combined. 14
It was estimated chat in 2003 there would be 2,800 cases of lung cancer diagnosed and 2,500 deaths from chis disease in our state. 15
Cancer of the colon and rectum is the second leading cause of cancer-related death in the United States and South Carolina. It is estimated chat 2,300 new cases of coloreccal cancer will be diagnosed and 900 men and women will die of coloreccal cancer in our state this year.15
Diabetes. Diabetes is the sixth leading cause of death in our
5
6
state and nation. 16 In 2002, almost a quarter of a million South Carolinians had diagnosed diabetes, 9 and it is believed that there are at least 120,000 who do not know they have the disease. Diabetes is related to deaths from cardiovascular disease in that 65% of those with this disease eventually die from stroke and heart disease. 17 In 1997 the direct costs of emergency room visits and hospitalizations related to diabetes in South Carolina were more than $73 million. 16
South Carolina ranks 5th in the nation for the number of diabetes deaths and for prevalence of diagnosed diabetes cases.3 Almost one of every 10 South Carolinians (9.4%) reports having this disease-compared to a national percentage of 7. 9%. 18
The death rate from diabetes is 160% higher among blacks than whites in our state. 9 Self-reports of diabetes reveal that women have slightly higher rates of the disease than men. 16
Although genetics can play a role in diabetes, there are several behavioral risk factors for rype 2 diabetes, including:
• Overweight. Overweight is strongly related to rype 2 diabetes as 70-80% of persons with type 2 diabetes are overweight. Most South Carolinians (over 60%) are currently overweight and are, therefore, at risk for type 2 diabetes. 16
• Inactivity. Sixty-five percent of South Carolinians are physically inactive (get less than 30 minutes of exercise a day most days of the week) .16
• Poor nutrition. A standard nutrition recommendation is to eat at least five servings of fruits and vegetables a day. Although eating fewer fruits and vegetables than this recommendation will not cause diabetes, it might be considered a standard for "healthier nutritional behavior." In 1998, 78% of the adult South Carolina population consumed less than five servings of fruits and vegetables a day.16
Overweight and obesity. Although obesity is not listed as one of the top 10 causes of death in our country, it is now classified as a complex and chronic disease. According to the South Carolina Department of Health and Environmental Control's Report on the Impact of Obesity on the Health of South Carolinians, being overweight greatly increases one's chance of developing many diseasesbreast, prostate, and endometrial cancers, heart disease, stroke, diabetes, hypertension, respiratory problems, joint and gallbladder dis-
eases, high blood pressure, sleep apnea , osteoarthritis, gout , and psychosocial problems. 19 In 1997 , obesity and these obesity-related conditions cost our state more than $177 million. 19
What are the rates of obesity and overweight in our state and nation?
The dramatic increases in obesity between 1976 and 2000 have reached nearly epidemic proportions, with 95 million adults in our country at the obesity level.20 Since 1990, the obesity rate among South Carolina adults has risen by 90%. 21 According to the Centers for Disease Control (CDC), over 60% of adults in our state and nation are overweight. 21 While the number of overweight persons has slowly been climbing for the past two decades, the number of obese people has doubled since then. Moreover, the percentage of young people who are overweight has doubled in the past 20 years. Around 9 million young people, aged 6 to 19 years, are considered overweight.20
South Carolina rankings for obesity and overweight among the 50 states are quite dismal. We are 9th in the nation for obesity prevalence among adults and 13th for overweight and obesity rates combined. 3 In our state, blacks are 1.3 times more likely to be overweight than whites. 12 Among our young people , 15% of South Carolina adolescents (12 to 19 years) and children (6 to 11 years) were found to be overweight in the year 2000. 22
How are overweight and obesity defined? Overweight and obesity may be assessed in many different ways;
however, the two ways used most often for overall risk status are Body Mass Index (BMI) and waist circumference. 23 (NIH, 1998)
Body Mass Index. BMI describes the ratio of weight-to-height and is strongly correlated with total body fat content in most adults. It is determined by dividing a person's weight in kilograms by height in meters squared. To get your approximate BMI using pounds and inches, multiply your weight in pounds by 704, then divide the result by your height in inches, and divide that result by your height in inches a second time. An interactive BMI calculator is also available at this web address: www.mhlbisupport.com/bmi/bmicalc.htm. 23
Overweight. Overweight is generally defined as a BMI greater than 25 but less than 30 or body weight that is 10 to 20% above desirable weight (see Table 3). The term "overweight" refers to an excess of
7
8
body weight, but not necessarily body fat. For example, a professional athlete may be lean and muscular with little body fat and weigh more than others his/her height. Although this person may appear to have an overweight BMI, he or she is not necessarily "over fat." The greater BMI number is likely due to an increase in lean muscle.24
Obesity. Obesity is generally defined as a BMI greater than or equal to 30 or a body weight that is 20% above recommended weight range in the height-weight table. Those with a BMI above this value generally have a high amount of body fat in relation to lean body mass. 24 Again, someone who has low body fat, a large bone structure, and a muscular body may have a BMI of 30 and actually be very lean. Body fatness can be estimated by skinfold calipers, waist-to-hip circumference ratios, or several other techniques such as computed tomography, bioelectrical impedance analysis, hydrostatic weighing, or magnetic resonance imaging.
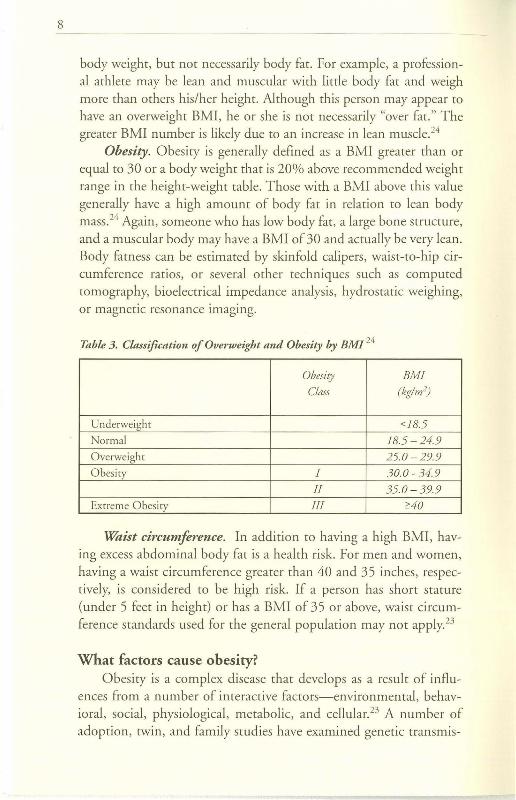
Table 3. Classification of Overweight and Obesity by BM/ 24
Obesity BM!
Class (kglm2)
Underweight <18.5
Normal 18.5-2 4.9
Overw eight 25.0-29.9 Obesity I 30.0-34.9
II 350-39.9 Extreme Obes ity III ~40
Waist circumference. In addition to having a high BMI, having excess abdominal body fat is a health risk. For men and women, having a waist circumference greater than 40 and 35 inches, respectively, is considered to be high risk. If a person has shore stature (under 5 feet in height) or has a BMI of 35 or above, waist circumference standards used for the general population may not apply. 23
What factors cause obesity? Obesity is a complex disease chat develops as a result of influ
ences from a number of interactive factors-environmenta l, behavioral, social, physiological, metabolic, and cellular.23 A number of adoption, twin, and family studies have examined genetic transmis-
sion of obesity. Studies of individuals suggest that genetic contribution to BMI may range from 25 to 70 percent. It is important to realize that weight gain is not always a result of poor adherence to nutrition and physical activity recommendations. Available research suggests that several genes have the capacity to increase the likelihood of obesity. 23
Another major influence on overweight and obesity is environment. In our country we have an abundance of delicious, high-calorie foods, and many of our social traditions promote overeating. Also, many people have sedentary daily routines, spend a good bit of time in traffic, watch hours of television or sit in front of a computer most of their waking hours. 23
What role does physical activity play in preventing chronic disease and/or major causes of death?
Although the purpose of this study is to highlight nutritional choices and how they relate to better health, physical activity must at least be mentioned because of the critical role it plays in weight control and disease prevention. Many studies have shown the benefits of regular physical activity for enhancing physical functioning, controlling weight, preventing cardiovascular disease, and preventing mortality. 25 Regular participation in physical activity also reduces the risk of diabetes, heart disease, colon cancer, high blood pressure, osteoporosis, obesity, arthritis, as well as risks of mental conditions such as depression and anxiety. Although cardiovascular health is best enhanced by vigorous physical activity, even modest increases in physical activity will decrease the risk of mortality. 25
Despite the many benefits of physical activity, more than 50% of American adults do not engage in the recommended amounts of activity and 26% are not active at all. Furthermore, more than a third of our children and teens do not get adequate physical activity either. Daily participation in high school physical education classes has continued to decrease over the past decade. 20
The combination of reducing caloric intake and increasing physical activity produces greater weight loss than diet or physical activity alone. 23 Reducing caloric intake and increasing physical activity produces weight loss, decreases abdominal fat, increases cardiorespiratory fitness, and may increase the long-term success of weight loss efforts. 23
9
10
To improve nutritional habits, should you count carbohydrates, fat, or calories?
Good nutrition can lower the risk of many of our major causes of death such as heart disease, stroke, some types of cancer, and diabetes;20 however, there is currently much confusion about the definition of good nutrition. Should you "count " carbohydrates, fats, and/or calories? The American "health trend" has led many manufacturers to remove carbohydrates or fats from foods, reduce portion sizes, and increase the prices of products-all with no change in calories over original food products. Bottom line: any food eaten in excess can lead to weight gain. Eating low-carb or low-fat foods isn't always the answer to weight loss. For example, if you eat twice as many low-fat or low-carbohydrate cookies, you may not have reduced your overall caloric intake. Calories do count. Successful weight loss occurs when daily dietary intake is reduced by 500 calories per day (1 pound weight loss per week). A minimum of 1,200 calories for women and 1,500 for men should be provided per day. 26
Nine nutrition recommendations to reduce the risk of major chronic diseases and prevent obesity
1 Eat a minimum of five fruits and vegetables each day.
If you were to close your eyes and imagine a dinner plate filled with fruits and vegetables, it is likely that this vision would be a colorful one. Meals with many different bright colors, such as red, green, orange, blue, yellow, and purple, usually are healthy. Why? If a meal consists of different fruits and vegetables, it likely has a wide array of color due to phytochemicals . Phytochemicals, or the "plant chemicals" found in fruits and vegetables, are big news in nutrition with more than 4,000 currently identified. The name "phytochemical" refers to a variety of compounds produced by plants that have potential antioxidant, anti-cancer, cardio-protective effects. Antioxidants protect cells in the body from harmful molecules, known as free radicals, that damage our DNA. Free radicals may be a cause of cancer, heart disease, and other chronic diseases. It is recommended that all Americans eat five to nine servings per day. 27
Prevention of cardiovascular disease through fruits and vegetables. Fruits and vegetables are believed to lower the risk of heart disease by
reducing inflammation, preventing the oxidation of LDL (bad) cholesterol, or preventing blood clots. Examples of some foods and phytochemical rypes include: lignans (flax, bernes, whole grains), ally[ sulfides (garlic, onions, leeks), anthocyanins (cherries, blueberries), carocenoids (tomatoes, carrots), indoles (cruciferous vegetables), phytosterols (soybeans, other beans), monoterpenes (oranges, lemons), and capsaicin (chili peppers).28
Resveracrol has been identified as one of the most promising food-related compounds with anti-cancer and anti-heart disease effects. It works as an antioxidant and as an anticoagulant or "bloodchinner," similar to aspirin. Research thus far is limited to cell and animal studies; however, initial results are encouraging. It is found in at lease 72 different planes; good sources are peanuts, grapes, wine, as well as grape jams and raisins. 28
Two recent U.S. government-sponsored dietary trials, called Dietary Approaches to Stop Hypertension (DASH), demonstrated chat a diet rich in fruits, vegetables, and low-fat dairy products can lower blood pressure and also heart disease. The first DASH trial in 1997 placed 450 people on one of three diets. Group 1 followed a diet plan chat included 10 servings of fruits and vegetables a day, plus low-fat dairy foods. Fats comprised 26% of total calories. Group 2 ace eight servings of fruits and vegetables a day and 36% of calories from fat. Group 3 followed a rypical American diet with fewer than four servings of fruits and vegetables and 36% of calories from fat. After eight weeks, chose who ate the higher-fat, fruic-andvegecable-rich diet did have reductions in blood pressure; however, chose on the low-fat, high-produce plan had readings chat had fallen most. Systolic and diastolic pressures dropped 5.5 and 3 millimeters more, respectively. This created a buzz among medical experts because all three groups took in 17% more sodium than is recommended by the National Academy of Sciences.29 This was a landmark finding because for most people who have high blood pressure, increased sodium intake tends to increase blood pressure. A followup study, called the DASH-Sodium trial, combined lower sodium with the high intake of fruits and vegetables and calcium-rich foods. Those on the DASH diet with reduced sodium lowered their systolic and diastolic blood pressure even further than in the first study.30
Because the DASH diet is consistent with dietary recommendations to prevent and treat not only heart disease, but also osteoporosis and
11
12
colon cancer, it has been acknowledged by a number of health professional and advisory groups. 30
Prevention of cancer through fruit and vegetables. Consumption of fruits and vegetables reduces cancer risk, but researchers are currently searching for the specific components that cause these beneficial effects. Clinical studies have found a reduction in cancer risk from eating whole foods such as fruits and vegetables, but not from taking antioxidant supplements. Currently, the best advice to reduce cancer risk is to eat foods high in antioxidants, like fruits and vegetables, rather than relying on antioxidant supplements. 31
Researchers at Cornell University devised a "bioactivity index" to rate antioxidant activity and suppression of cancer cells by fruits and vegetables. Those with the highest bioactivity ratings are thought to be most protective. Top-rating fruits in order of bioactivity were found to be cranberries, followed by apples, lemons, strawberries, red grapes, peaches, bananas, grapefruits, pears, and oranges. Among the vegetables, spinach was the top vegetable, followed by red peppers, broccoli, cabbage, carrots, and onions. Among grains, corn, wheat, oats, and rice comprised the list. 27
Beta-carotene is an antioxidant chemical related to vitamin A and is found in certain fruits and vegetables. Because beta-carotene consumption is associated with a lower risk of cancer, several major studies were conducted which examined synthetic beta-carotene supplements in the prevention of lung cancer and other cancers. 31
Researchers conducting studies of beta-carotene found the supplements to be associated with a higher risk of lung cancer in cigarette smokers in one study while another study found neither a benefit nor harm from the supplements. For this reason, it is recommended to eat foods high in beta-carotene rather than taking beta-carotene supplements. 31 Foods which are good sources of beta-carotene include leafy greens and orange/yellow fruits and vegetables such as apricots, peaches, summer squash, cantaloupe, and carrots.
Lycopene is a carotenoid (antioxidant) found in high amounts in tomatoes and tomato-based foods. It is a vitamin-like substance that makes tomatoes red. Although numerous studies have found that cancer risk is reduced when tomato foods are eaten, it is uncertain if lycopene is the responsible nutrient. In one study, scientists asked a group of men scheduled for prostate cancer surgery to eat tomato-based dishes (such as spaghetti) once a day for three weeks
prior co surgery. The amount of lycopene in their diets was measured along with Prostate Specific Antigen (PSA), a protein chat usually rises when prostate cancer is present. Although the study was small, results were interesting. Lycopene levels in the blood and prostate increased and PSA levels declined. Furthermore, they also found that injury to genetic material in the cancer cells was less prevalent than at the time of biopsy. Although tomato-based foods are not considered a cure for cancer, they may slow cancer progress. 32 Should one try lycopene supplements? There is no evidence that lycopene supplements prevent cancer,31 so choose lycopene rich foods such as processed tomatoes (canned tomatoes and tomato-based sauces), which actually contain more lycopene (and a more absorbable form) than fresh tomatoes. 32
Choosing.fruits and vegetables. If no fresh fruits and vegetables are available, should you choose other foods? The good news is that fruits and vegetables need not only be "fresh" to be healthy. Frozen foods are often more nutritious than fresh foods because they are usually picked ripe and quickly frozen. Canning is more likely to reduce nutrients because of the high heat used in processing. It is recommended to choose fruits and vegetables in a variety of different forms. 31 Serving sizes for fruits and vegetables are: raw leafy greens (1 cup), cooked vegetables (1/2 cup), apple, orange, banana (1 medium), grapes (12), canned fruit (1/2 cup), and fruit juice (3/4 cup).
What about the juicing trend? Juicing adds variety to the diet, increases absorption of some nutrients, and can be a great way co consume fruits and vegetables. Keep in mind chat juices may not be as filling, and usually contain much less fiber. If you choose to juice, eat adequate fibrous foods and cake care not to consume too many calories.31
2 Eat often and always eat breakfast.
Among U.S. adults, the incidence of skipping breakfast increased from 14 to 25% between the years of 1965 to 1991. 33
Many people skip breakfast because they believe it will decrease total calorie intake and help with weight loss-the opposite is actually true. Two healthy habits that can help to curb excessive hunger and feelings of deprivation are (1) to eat frequent small meals and (2)
13
14
always eat breakfast. The good news is that a healthy breakfast need not be complicated. Cereal, fruit, and low-fat milk are an easy, healthy combination.
Meal frequency and obesity prevention. The average person takes in around 1 million calories a year and expends more than 99% of them, maintaining a stable weight for years and years. However, some people eat too many calories and get fat, while some eat too little and lose weight. If you gain weight, should you skip meals to lose weight? No, because what your body perceives as starvation generally leads to a reduction in basal metabolic rate. Basal metabolic rate is the energy a person spends in a day to support the body's metabolic activities such as breathing, maintaining body temperature, heartbeat, kidney function, production of red blood cells, and nerve action. Ac least two-thirds of the calories needed per day are used for these functions. Very simply, fasting and skipping meals lower basal metabolic rate-which means your body will burn less calories than usual for basic metabolic functions. For long-term success in weight management, do not lower calories too much.
Frequent eating also helps prevent snacking or bingeing on high-calorie, high-fat, or sugary foods later in the day when you are tired. It is important to remember chat although you are encouraged to eat ofren, meals should be moderate in calories and snack sizes should be small. Three small or moderate meals and two or three small snacks-with portion sizes dependent on your age and activity level-should keep hunger away.
Many people get confused about losing weight and losing fat . Fasting is popular for "quick weight loss." Bottom line: it takes a 3,500-calorie deficit to lose a pound of fat. You can lose five pounds in one day on a total fast, but it is likely that not even one pound may be body fat (if your body has an energy need for 3,500 calories per day-which is much higher than most people need). Since very fast weight loss is mostly fluid, as soon as you drink a beverage or eat regular portions, the weight comes back. Quick weight loss usually equals quick weight return.
Meal frequency and cardiovascular disease prevention. Another benefit of increasing frequency of meals or snacks to more than three times a day is that reductions are found in blood triglycerides , LDL-cholesterol, and blood glucose swings. These are all metabolic changes which reduce risk for heart disease. 34
Breakfast and obesity prevention. Despite the fact that most Americans are familiar with the saying "breakfast is the most important meal of the day," almost one in four Americans currently skip breakfast. Often when people begin a "diet" they believe skipping breakfast is an easy way to reduce calories and promote weight loss. However, eating breakfast has been found to contribute to success in weight-loss maintenance. Probably the best support to date for eating breakfast as a means of maintaining weight loss comes from the National Weight Control Registry.33 This is a group of 3,000 persons who have maintained a weight loss of at least 30 pounds for one year. On average, individuals in this group had lost more than 60 pounds and kept the weight off for six years. This is a feat that many yo-yo dieters have found to be nearly impossible. What behaviors do these successful weight loss maintainers practice? First, almost 90% reported eating breakfast most days of the week and 78% ate breakfast seven days a week. Second, they reported eating a diet high in carbohydrate and low in fat. Third, they regularly monitored weight and food intake. Finally, they all reported high levels of physical activi ry. 33
The question is-what is it about breakfast that helps in longterm weight loss? Researchers have found that individuals who eat breakfast are more likely to consume adequate vitamins and minerals and eat less calories from fat. 33 In contrast, researchers have found that breakfast skippers are more likely to eat higher calorie foods later in the day. 33 Eating breakfast increases the calorie-burning rate-leaving you with more energy later in the day when weight control efforts are harder. Although some people complain that they feel hungrier at midday if they eat breakfast, this should be perceived in a positive way. Your metabolic rate is increasing from your morning meal and it is likely that the food choices you make at mid-day will be smarter than those late in the evening.
Also, keep in mind that WHAT type of food you start your morning with is very important. Research by the National Weight Control Registry supports the fact that those who eat breakfast cereal in the morning were most likely to be successful in weight control efforts.33
The reason for this is that a morning meal of healthful, whole grains controls the appetite until midday, so you are less likely to overeat. Sugary cereals or pastries may cause a brief energy high, but it will likely drop to lower levels. Skip the sweets and enjoy whole-grain cereals
15
16
and breads, and fresh or frozen fruit. 35 Look for high-fiber cereals with at least three grams of fiber per 100 calories. Avoid cereals high in fat, particularly saturated and trans fats like many granolas.
It is fine to eat vitamin-fortified cereals; however, there is no need to spend extra for cereals with 100% of most vitamins and minerals. 36 Other healthy choices include: whole-wheat toast with peanut butter and banana slices; breakfast parfait layered with low or nonfat yogurt, fresh fruit, whole-grain cereal with nuts and/or raisins; and instant oatmeal with raisins and/or fresh fruit. 35
Breakfast and cardiovascular disease prevention. A final reason to add whole-grain breakfast cereal to your diet is that total mortality and cardiovascular disease mortality have been found to be inversely associated with whole grain, but not refined-grain breakfast cereal intake. 37 So, bottom line, to help prevent chronic disease and keep your weight in check, emphasize whole grains for breakfast and eat balanced regular meals or snacks during the day. More about whole grains will be outlined in the next section.
3 Choose foods high in fiber.
When you choose breads and cereals, the operative word is "whole." Look for the words "whole grain" or "whole wheat" as the first or second ingredient listed. Don't be fooled by terms like "cracked wheat, " "wheat bread," "multigrain," or "stone-ground." Since whole grains are virtually unprocessed, they are therefore excellent sources of vitamins, minerals, and fiber. Only recently have studies shown that whole grains help prevent cardiovascular disease, diabetes, some cancers, and obesity. Furthermore, many people do not realize that whole grains have as many (or more) phytochemicals as fruits and vegetables. 38 The bran and germ of whole grain have significant amounts of vitamins, minerals, phytochemicals, antioxidants, lignins, insoluble fiber, vitamin E, and unsaturated fatty acids. When bread is stripped of the bran and germ (white bread), 75% of the nutrients are lost. 38 For this reason and for maximum health benefits, try to replace unrefined (white) bread with whole grains.
In addition to whole-grain bread, fruits and vegetables are also good sources of fiber. Citrus fruits, strawberries, broccoli, leafy greens, and apples are just a few fiber-rich choices. It is recommended that you get fiber from whole foods rather than fiber supple-
ments. Whole grains, fruits, and vegetables are valuable sources of antioxidants, which protect against cellular damage.
Although it is recommended for Americans to eat at least three servings of whole grains per day, the average intake is less than one serving per day;38 thus fiber intake in our country is far lower than recommended. American adults consume only 12 to 15 grams of fiber per day. New recommendations from the Institute of Medicine for daily fiber consumption are 38 grams per day for men and 25 grams per day for women (ages 31-50). 38 Serving sizes for these fiber-rich foods are: whole wheat bread (1 slice), whole-grain bagel (1/2 small bagel), whole-grain cereal (1 ounce), oatmeal (1/2 cup), or whole-wheat cooked pasta (1/2 cup).
Fiber and cardiovascular disease prevention . When J.M. Jones and colleagues examined several large epidemiological studies, they found heart disease to be reduced by 25-35% with whole grain consumption. 38 A recent study from the University of Minnesota found that for every 10-gram increase in fiber consumed each day, there was a 14% decrease in risk of heart attack and a 27% decreased risk of dying from coronary heart disease. 39 Furthermore, the Harvard Nurses' Health Study of 75,000 women showed a 36% drop in risk of stroke when women ate three servings of whole-grain foods per day. Reasons believed to cause the drop in CVD risk include lower LDL (bad) cholesterol, the bioactive compounds found in fiber, and changes in insulin sensitivity from fiber.38
Fiber and cancer prevention. A meta-analysis of 40 studies on gastrointestinal cancers found a 21-43% lower cancer risk with higher intakes of whole grains. 38 Most studies have found a relationship between high-fiber intake and a lower risk of colon cancer. Possible reasons for this include increased transit time, antioxidant activity, and fecal bulk. Grains are a good source of folic acid (and since 1998 all grain products in our country are now fortified with folic acid)and too little folic acid may increase risk of cancers of the breast, rectum, and colon. 31 Although the associations between cancer risk and fiber are not conclusive, this provides yet another reason why eating foods high in fiber is recommended-they often contain other substances that prevent cancer.3 1
Fiber and diabetes prevention. One study of more than 30,000 Iowa women showed those with the highest whole-grain intake had a 21 % lower rate of type 2 diabetes. It is believed that sol-
17
18
uble fiber may help to regulate blood sugar and reduce long-term diabetes risk.38 Soluble fiber-rich foods generally cause a lower glucose response, therefore reducing spikes in blood sugar. Foods rich in soluble fiber include fruits, (apple, citrus), oats, beans, and peas.
Fiber and obesiry prevention. How would you like to lose five pounds in four months-without dieting? In an analysis of more than 100 studies on fiber and weight control, researchers found that those who increase their fiber intake from the current American average of 15 grams a day to 25 to 30 grams a day lost five to six pounds in four months-without malcing any other dietary changes.40 Researchers found that when fiber is increased by 14 grams for only two days, there is a resulting 10% decrease in calories consumed. 41
How exactly does fiber consumption help with calorie control and weight loss? One hypothesis is that people tend to eat the same weight of food each day, and high-fiber, low-calorie foods tend to weigh more than high-calorie foods like cakes and crackers. Another finding is that fibrous foods require more chewing time , which gives the body a better chance to register "fullness" before over consuming. Furthermore, fiber slows stomach emptying and promotes satiety. By keeping the food out of the bloodstream longer, fiber moderates blood sugar levels. Fiber-rich foods tend to have a low glycemic index (or GI, a measure of how quickly the carbohydrate in food converts to simple sugar). Finally, fiber may promote stomach distension, which signals stomach nerves to tell the brain the body has enough food. The 25+ grams of fiber that are recommended for us to eat each day can be achieved with five servings of fruits and vegetables and at least three servings of whole grains.40
Choose at least 2-3 foods daily which are low-fat 4 sources of calcium.
Although calcium is essential for many body functions, it is probably best known for maintaining a healthy skeleton. Even after the body reaches full skeletal growth, adequate calcium intake is important because the body naturally loses calcium each day, leading to a disease known as osteoporosis. Osteoporosis is characterized by low bone mass and deterioration of bone tissue, leading to increased fracture susceptibility. Osteoporosis is a major public health threat because it affects 55% of the American population ages 50 and older.42
The National Osteoporosis Foundation recommends five steps for bone health and osteoporosis prevention: (1) Get recommended calcium and vitamin D; (2) regularly participate in weight-bearing exercise; (3) avoid excessive alcohol and smoking; (4) talk to your physician about bone health; (5) have a bone density test and take medication, if appropriate. 43
Calcium and cardiovascul.ar disease prevention. Epidemiological studies show an inverse relationship between calcium and blood pressure levels.44 Ochers have reported a lower risk of coronary heart disease for chose who consume adequate calcium.45 Although the mechanism for calcium's action is not folly defined, because calcium plays a role in vascular contraction many believe it causes metabolic changes related to vascular smooth muscle contraction. 46
Calcium and cancer prevention. Recent studies show calcium may play a role in decreasing the risk of developing colon and other cancers. A recent clinical trial published in the New England journal of Medicine tested more than 900 people for four years. The results showed that calcium supplementation reduced the occurrence of colorectal polyps. An animal study at Texas Tech showed that calcium from food or supplements might help prevent colorectal cancer. Calcium appears to detoxify irritants and cancer-promoting compounds found in a high-fat diet. Further research is needed on the role of calcium in the prevention of cancer.47
Calcium and obesity prevention. Dairy products-which are increasingly replaced by soft drinks in the American diet-are quickly emerging as dietary "goods" in the weight-loss arena. Researchers from the University of Tennessee placed 32 obese adults into one of three groups: (1) low in calcium and dairy; (2) high in calcium supplements but low in dairy; and (3) high in dairy. All participants consumed 500 less calories a day than normal. Ac the end of a 24-week trial, those on a low-calcium/low-dairy diet lost 15 pounds (6% of total body weight), those on a high calcium supplemented/low -dairy diet lost 19 pounds (9% of total body weight), and those on a highdairy diet (3-4 servings dairy/day) lose 24 pounds (11 % of total body weight). Interestingly, M.B. Zemel and colleagues also calculated that having a low calcium intake over several decades can more than double the risk for increased body weight. 48
The American Dietetic Association now features a Milk Your Diet plan to fuel weight loss efforts. This meal plan provides 1,600
19
20
calories per day, less than 50 grams of fat, and more than 1,000 milligrams of calcium per day- a formula that is believed to promote gradual weight loss when combined with physical activity and to reduce fat in the abdominal region. 50 How might calcium play a role in weight loss? It not only influences metabolism, but low levels of calcium may also shut down the mechanisms that break down fat.51
What would be the long-term consequences of increased calcium consumption among Americans? Researchers reviewing 90+ studies reported that if Americans increased their daily intake of calcium-rich foods to three servings per day there would be a fiveyear cumulative savings in excess of $200 million in health care costs due to the decreases in obesity, hypertension, type 2 diabetes, and osteoporosis. 49
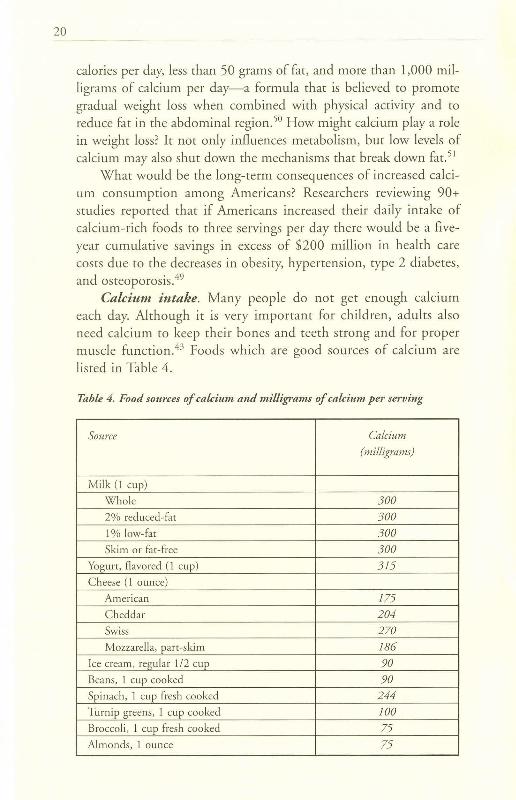
Calcium intake. Many people do not get enough calcium each day. Although it is very important for children, adu lts also need calcium to keep their bones and teeth strong and for proper muscle function. 43 Foods which are good sources of calcium are listed in Table 4.
Table 4. Food sources of calcium and milligrams of calcium per serving
Source Calcium
(milligrams)
Mi lk (1 cup)
Who le 300 2% reduced-fat 300 I% low-fat 300 Skim or fat-free 300
Yogurt, flavored (1 cup) 315 Cheese (1 ounce)
American 175 Cheddar 204 Swiss 270 Mozzare lla, part-sk im 186
Ice cream, regular 1/2 cup 90 Beans, I cup cooked 90 Spinach, 1 cup fresh cooked 244 Turnip greens, l cup cooked JOO
Broccoli, 1 cup fresh cooked 75 Almonds, 1 ounce 75
Calcium supplementation. Experts agree that increasing the intake of calcium-rich foods is the best way to tackle calcium deficiencies. If weight loss is your goal, it is important to know that some researchers have reported that calcium found in food results in greater weight loss than calcium from supplements; however, some people do find it difficult to meet calcium recommendations from food alone. If that is the case, calcium carbonate and calcium citrate are two types of supplements that are recommended. Calcium carbonate is the most common form of calcium found in supplements. For persons over the age of 60, calcium carbonate taken on an empty stomach will not break down enough for absorption because of a stomach acid deficiency. To solve this problem, rake calcium carbonate right afrer eating. Calcium citrate is the most easily absorbed and it does not matter if you take it on an empty or full stomach. Unfortunately, it is hard to pack into a pill and you might have to rake two or three tablets. For this reason, calcium carbonate might be the better choice. 52
What about coral calcium? Ir is quite expensive relative to the price of calcium carbonate and citrate. Although manufacturers say that it is the best calcium supplement and a treatment for 200 diseases, there has been little or no definitive research on coral calcium as an effective treatment for disease. 53
Manufacturers promoting this product claim that Okinawans are healthy and live longer because of the presence of coral calcium in the water. To refute this claim, the Okinawa Centenarian Study issued a report which states that it does not endorse coral calcium supplements because they are not proven to be more effective than less costly calcium supplements and that the claim that you can enhance health by making the body more alkaline has no basis in science. 54 After a few well-conducted scientific studies with coral calcium, this advice could change. At present, it is probably best to adopt a "wait and see" philosophy.
If you choose to supplement with calcium, do not take more than 500 milligrams at a time because your body cannot absorb higher doses. It is also a good idea to choose a calcium supplement that also contains Vitamin D, which assists the body 10
absorption and utilization of calcium. 32
21
22
5 Read labels to determine fat/ oil types and select monounsaturated oils more often.
Is there any illness that has not been blamed on too much fat? While all fats are equally high in calories, some types of fat are more healthful than others.
Fat, cholesterol, and cardiovascular disease risk. First, let's clear some of the confusion about cholesterol. Dietary cholesterol and blood cholesterol are two different types of cholesterol. Dietary cholesterol is found in animal foods such as pork, chicken, eggs, and beef. Blood cholesterol is a waxy substance that is necessary for sex hormones and bile and is produced naturally by our body. If blood cholesterol in the body is too high, it can stick to artery walls and cause blockage. If you have high blood cholesterol you should limit consumption of dietary cholesterol (animal products); moreover, most persons should consider limiting saturated and trans fats because these substances can raise blood cholesterol levels.55 In fact, the American Heart Association (AHA) recommends that no more than 30% of your calories should come from fat, emphasizing that saturated and trans fat intake not exceed 10% of total calories for healthy persons and be lower than 7% for those with heart disease, diabetes, or high LDL cholesterol. 56
Unsaturated fatty acids and cardiovascular disease prevention. Monounsaturated and polyunsaturated are two types of unsaturated fatty acids. They help your body get rid of newly formed cholesterol. When saturated fat in the diet is replaced with these fats, blood cholesterol levels will be lower.56
Monounsaturated fatty acids are liquid at room temperature and are found mainly in vegetable oils like olive, canola, and peanut. These oils may help lower LDL (bad) cholesterol and reduce heart disease risk. For this reason, it is recommended that you use canola as your main oil, substituting others such as olive, sesame, peanut, and safflower for different flavors.57
Polyunsaturated fatty acids are mainly found in vegetable oils like safflower, sunflower, corn, flaxseed, and soybean. They contain two essential fatty acids that our body cannot make- omega-6 and omega-3. Just like the monounsaturated fatty acids, consuming polyunsaturated fats in place of saturated fats decreases LDL (bad) cholesterol and reduces total cholesterol. Because so many restau-
rants use polyunsaturated oils for food preparation, it is suggested that if you eat away from home often you should balance polyunsaturated fatty acids with monounsaturated oils at home. 57
Saturated fatty acids. Saturated fatty acids are found mainly in animal products such as beef, poultry, whole milk, and butter. Some vegetable oils like coconut and palm are also sources of saturated fats. Usually, saturated fats are solid at room temperature. Consuming too many saturated fats can increase LDL (bad) cholesterol and total cholesterol-both risk factors for heart disease.55
Trans fats. Trans fatty acids are formed when vegetable oils are processed and changed from a liquid to a solid fat. They are often found in crackers, snack foods, and baked goods. Look for "partially hydrogenated," "hydrogenated oils," or "vegetable shortening" on product ingredient lists to determine if foods contain trans fats. Trans fats act like saturated fats in that they raise total and LDL (bad) cholesterol, yet they go a step further and also lower HDL (good) cholesterol.55
Recent findings on trans fats have been alarming. For example, a 1993 study of nearly 90,000 women found that those consuming the most trans fats (particularly from margarine) had a 50% higher risk of heart disease.58 It has been estimated that replacement of partially hydrogenated fat in our diet with natural unhydrogenated oils would prevent 30,000 premature coronary deaths per year, while epidemiologic evidence suggests this actually may be closer to 100,000 premature deaths annually. 59
Some nutrition experts believe that trans fats make up a small percentage of our fat intake and we should not be concerned with them, yet unfortunately over the past decade we have started consuming more and more foods with these fats.58 Currently, calories from trans fats are not required to be provided on the Nutrition Facts section of the food label, but food manufacturers will be required to include this informa tion beginning January 1, 2006. 60 To keep trans fat intake lower, when choosing margarine select the tub, diet, or liquid "squeeze" types. The more solid the margarine (as in stick margarine), the more hydrogenated it may be.58 Even better, look for foods labeled "no trans fat."
Fat and obesity prevention. An easy way to consume fewer calories is to eat less fat. There are nine calories in each gram of fat, whereas protein and carbohydrates have only four. Eating less fat allows you to consume fewer calories without eating less food; therefore, should fats be restricted when dieting? It might be beneficial
23
24
not to limit fats too much because people tend to have more success with diets that contain some fat. A study of 101 overweight men and women who were assigned to one of two groups-20% fat (very low-fat diet) or 30-35% fat (mostly monounsaturated [good] fats from peanut butter, nuts, olive and canola oils)-found that only one in five could stick to the very low-fat diet, whereas more than 50% stuck to the higher fat diet. Both groups lost 11 pounds the first year, but the moderate fat group (followed for over two years) kept a significant amount of weight off, while most of those on the very low-fat diet gained back their weight within a year.61 It appears that moderate fat consumption, particularly mono- and polyunsaturated fat, can be included in a healthful eating plan to lose weight.
Fat and cancer prevention. Diets high in fat are usually high in calories , which contribute to obesity. Since obesity is linked to an increased risk of certain types of cancer, fat intake should be moderate. Certain types of fats, particularly saturated fats, seem to have a greater effect on increasing risk of cancer. 31
6 To get adequate omega-3s, eat fish twice a week and/or consume flaxseed meal.
Recent studies have shown that omega-3 fats have a stellar reputation in preventing disease-and should be chosen more often. There are three forms of omega-3 fatty acids: plant-derived (alpha linolenic acid) and marine-derived (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]).
Oils from cold-water fish like salmon, halibut, striped bass, tuna, sardines, shark, and cod are all good sources of omega-3s . Because of concerns about toxins in fish from pollution, experts have issued guidelines for fish consumption. 62 To minimize risk , consumers are advised to eat up to two fish meals per week; to avoid shark, swordfish, king mackerel or tilefish; 63 to eat a variety of fish;
and to remove the skin before eating fish.64 Despite concerns about toxins, because heart disease is the number one cause of death in our country the American Heart Association also recommends that healthy adults should eat fish twice a week for heart hea!th. 65
For those who don't like fish, flaxseed is the best plant source of alpha-linolenic acid, one of the three omega-3 fatty acids. Flaxseed is recommended because it contains fiber and lignans, unlike flax
oil.66 Flaxseed is available in flour, meal, oil, and seed forms. If you purchase the seed form, it will need to be ground into flaxseed meal in order for your digestive system to absorb the active ingredients. Flaxseed meal is like cornmeal in consistency and has a slighcly nutty flavor. You can mix one or more tablespoons into cereal, salads, yogurt, soups, casseroles, or bread. Other plant sources of omega-3s are soybeans, great northern beans, kidney beans, and navy beans. 62
Omega-3 fatty acids and cardiovascular disease prevention. Evidence from clinical trials and epidemio logical studies tends to support claims chat plant and fish oils high in omega-3s may benefit heart health. 67 Omega-3s may reduce risk for cardiovascular disease in several ways: reducing risk of sudden death and arrhythmias, reducing clotting, slowing plaque growth, reducing triglycerides, reducing inflammation, and reducing blood pressure. 68 The largest controlled trial of EPA and DHA on coronary heart disease to date showed a 45% reduction in cardiac death and a 20% reduction in overall mortality from marine-based omega-3s. 67 Furthermore, women with type 2 diabetes who ace fish more often reduced their risk of developing heart disease by 40 to 64% depending on how much fish they ate each week. High fish consumption was associated with a significancly lower death rate as well.
Eating plant-based foods high in omega-3 fatty acids may also help arteries. A recent study found that vascular function and cholesterol levels were improved by a diet with increased levels of plantbased omega-3s. 69
Omega-3 fatty acids and cancer prevention. Epidemiological studies of societies that consume fish high in omega-3s have found lower rates of breast cancer. When researchers study omega-3 consumption in animals they have found suppression of cancer formation. 31 Other scientists have found that omega-3s may inhibit tumor growth and also reduce prostate cancer risk.70 No certain benefit has yet been documented in research on fish oil or omega-3 supplements. 31
Flax is a source of lignans, compounds that act as weak estrogens and may play a role in preventing estrogen-dependent cancers like breast cancers . Lignans are also antioxidants. The lignans in flaxseed are converted by intestinal bacteria into active forms chat can be used by the body.71 Most research on flaxseed and reduction of cancer risk has been done with animals. Researchers found chat mice chat were fed flaxseed had smaller and fewer tumor growths when
25
J
26
injected with skin cancer or colon cancer cells. Another study found that rats exposed to carcinogens had a lower risk of colon and breast cancer if they had flaxseed in their diets. Further study is needed to determine if the results apply to humans. 7 1
Researchers have also focused on the role of the omega-3 to omega-6 fatty acid ratio in our diets. Some researchers believe we suffer high cancer rates because of an imbalance in the omega-3 to
omega-6 ratio of fatty acids. The typical American diet is high in omega-6s and low in omega-3s. Studies of women with breast cancer show two to five times more omega-6 fatty acids than omega-3s in their diets. Although animal studies show the omega-3/omega-6 ratio plays a role in the formation of breast cancer and colon cancer, further study is needed to determine if these results are applicable to humans. 62
7 For snacks, choose nuts.
During the low-fat craze, nuts were shunned as a high-fat, highcalorie snack. New research shows that nuts are ,packed with disease fighting phytochemicals, protein, and fiber. The healthiest choices in the tree nut family are believed to be walnuts, almonds, pecans, and brazil nuts. Although peanuts are legumes, they also offer many beneficial health benefits. 72
Nuts are rich in: • monounsaturated and polyunsaturated fats, which can
lower blood cholesterol, especially when consumed in place of foods high in trans or saturated fats;
• copper, potassium, and magnesium-three minerals linked to heart health;
• vitamin £-possibly protective of cardiovascular disease; • fiber and its many health benefits; • phytochemicals that act as antioxidants; • folate and other B vitamins which reduce the risk of
heart disease.73
Nuts and cardiovascular disease prevention. An impressive number of studies indicate that people who regularly eat nuts reduce their risk of heart disease by as much as half when compared to those who rarely or never eat nuts. 74 One well-conducted study was a sixmonth controlled investigation at Pennsylvania State University.
Researchers found that , compared to the average American diet, daily consumption of peanuts and/or peanut butter reduced the risk of heart disease by 21 %. Those regularly consuming peanuts lowered total cholesterol by 11 % and LD L (bad) cholesterol by 14%. Triglycerides were also lowered , while HDL (good) cholesterol was maintained . 75
Nuts and prevention of obesity. Snacking on nuts when consuming a moderate fat diet has been found to promote longer-term weight loss than diets without nuts that are lower in fat.76 If you substitute nuts for other snacks you will find that they tend to be satisfying and reduce hunger better than other foods. Just keep your serving size to an ounce or two a day, about a handful. 73
Nuts and diabetes prevention. Nuts may also help prevent the onset of type 2 diabetes. Researchers from the Harvard School of Public Health found that women who consume nuts or peanut butter five times a week or more reduced their risk of type 2 diabetes by 30% compared to those who rarely or never ate nuts. 77 Another study found that those who ate an ounce of nuts at least five times per week had a 27% lower risk of type 2 diabetes, and those who ate peanut butter that often had a 21 % lower risk.73
8 Consider adding soy foods to your diet.
Many people are automatically turned off when they think of soy food products. If you haven't tried soy foods lately, try them again . There are some very good products on the market now. For example, the vanilla and chocolate soy milk found in the refrigerated section of the grocery store tastes great.
Soy foods include soybeans, tofu, tempeh, and isolated soy protein that is added to other foods. Good sources of soy protein include soy nuts, tofu, soy flour, soy milk, tempeh, and energy bars. 78 Soy is the only plant protein that is a complete protein. In other words, it is equivalent to an animal protein. Also, soy foods come without cholesterol and saturated fat that are present in many animal products. 79 Soy foods have a protein content which ranges from 1-2 to 18-20 grams per serving. 80 Average serving sizes of common soy foods and grams of protein in each are: 1 soy "burger" ( 10-12 grams), 8 oz. plain soy milk (10 grams), 1/4 cup of soy nuts (19.5 grams), and 4 oz. firm tofu (13 grams). 81
27
28
Soy and cardiovascular disease prevention. The FDAapproved health claim for soy protein reads, "25 grams of soy protein a day as part of a diet low in saturated fat and cholesterol may reduce the risk of heart disease."78 The phytosterols and fiber in soy foods are believed to reduce cholesterol absorption from the intestines, lowering both total and LDL (bad) cholesterol. 82
Isoflavones and isoflavonoids are two ocher active ingredients found in soy foods. Isoflavones are classified as phytoescrogens because they act as weak estrogens in the body. This is a positive effect because estrogens protect against heart disease by increasing HDL (good) and by decreasing LDL (bad) cholescerol. 83
lsoflavonoids are phytochemicals chat reduce the risk of heart disease, cancer, and osceoporosis. 84
Although researchers have identified the soy active ingredients described previously, it is important to note chat they don't know exaccly what soy components are most beneficial because findings have been conflicting. Some studies have suggested chat isoflavones alone will not decrease blood cholestero l levels or promote cardiovascular health. For example, P.J. Nestel and colleagues found chat blood lipid profiles were not improved when poscmenopausal women consuming 80 mg . of soy isoflavone supplements were compared to other women caking a placebo. 85 On the ocher hand, C.R. Sircori and colleagues found chat soy flour produces used in Italian studies did not contain isoflavones, yet were related to overall vascular health. 85 Therefore, don 't expect to get the benefits of soy by caking an isoflavone pill. Consuming whole soy food products to improve cardiovascular healch is probably the best choice until further research is conducted. 83
Soy and cancer prevention. Geniscein, one rype of isoflavonoid found in soy, has been found to reduce the growth of breast and prostate cancer cells in laboratory studies. Ocher cancer benefits from soy may be from the presence of phycic acid, which is believed co bind to carcinogens in the intestinal cract.84
Although consumption of soy has been correlated with lower rates of breast cancer among Asians, soy foods in Asia are quite different from chose consumed in the United States. Many of the soy produces manufactured in our country are partially purified isoflavone-containing products which may not have the same health benefits as who le soy foods. Seveney-five percent of breast cancer
cases are diagnosed in women over 50, and most are estrogendependent cancers. For this population, consuming too many highly processed isoflavone foods may be risky. In one animal study, mice were fed equal concentrations of the soy isoflavone genistein to determine the influences other bioactive soy compounds had on genistein's ability to stimulate estrogen-dependent breast tumor growth. As bioactive compounds were removed from soy food, there was an increase in estrogen-dependent tumor growth. Therefore, dietary soy products with purified isoflavones may be associated with greater tumor growth for those who have estrogen-dependent breast cancer. 86
Also unknown are the effects of phytoestrogens on women who are at risk for a recurrence of breast cancer or those at risk of developing it due to genetic factors. If one has any risk for breast cancer, isoflavone supplements should be avoided. 87 Specialists do still agree there are health benefits from a diet rich in naturally occurring soy products. 87
9 Take a multivitamin supplement each day.
There is little risk involved in taking a multivitamin that has 100% of the Recommended Dietary Allowance (RDA) for vitamins and minerals. In fact, there is emerging evidence that it may actually be helpful to prevent disease. It has been estimated that daily use of a multivitamin by older adults could lead to $1.6 billion in Medicare savings over the next five years. In a systemic literature review of multivitamin use by adults over the age of 65, researchers were able to identify cost savings based on improved immune functioning, reduction in relative risk of coronary heart disease, reduced hospitalizations, and less cell damage. It was concluded chat multivitamins are safe and effective for health and the prevention of many chronic diseases. 88
Multivitamins and cardiovascular disease prevention. Heart Disease Weekly recently reported that those persons who cook a daily multivitamin had C-reactive protein levels (CRP), a risk factor for heart disease, that were reduced by 32% over baseline levels before starting the multivitamin. Greatest reductions in CRP were for chose with elevated baseline levels.89 Other researchers found CRP levels to drop 14% after parcici pants took a commercial supplement for six
29
30
months-chose taking a placebo had increased CRP levels by the scudy's end. 90 Researchers have also found chat homocysceine, another independent risk factor for coronary heart desease, can be lowered by folic acid, found in multivitamin supplements. Patients with cardiovascular risk factors are recommended to cake a multivitamin once daily co reduce development and progression of heart disease.91
Multivitamins and cancer prevention. For chose with ulcerative colitis, daily multivitamin supplementation may protect against colon cancer-folate is believed to be the responsible vitamin in this case.92 Other researchers have also reported daily intake of multivitamins to be associated with a reduced risk of colon cancer.93 Overall, however, the clinical trials testing reducing cancer risk in humans through the use of supplements have yielded disappointing results.31
Multivitamins and diabetes. For those with type 2 diabetes, consuming a regular multivitamin was found to be associated with a reduced incidence of infection and absenteeism from work .94
Guidelines for supplementation. If 100% of the RDA of vitamins and minerals might improve your health, is more better? No, upper limits are sec for several vitamins and minerals because too much can cause harmful effects if they build up to toxic levels in your body. Stick with one multivitamin tablet a day. They are called supplements because they are designed to supplement an otherwise healthy diet. They are not magic pills.
When choosing supplements, look for labels chat have the United States Pharmacopeia (USP) symbol. 43 Although some good products may not display this symbol, it is a good indicator of quality. It verifies that the product meets the USP's standards for product purity, accuracy of ingredient labeling and proper manufacturing procedures. The USP is a voluntary, not-for-profit organization chat secs quality standards for many medicines and supplements. 95
Summary of nutrition recommendations. 1. Strive for a variety of color at each meal and for colorful
snacks. Eat at least five fruits and vegetables per day. 2. Always eat breakfast, preferably whole-grain cereal with
fruit, and eat frequent small meals or snacks during the day. 3. Choose two co three foods daily which are good sources
of calcium. 4. Choose whole-grain breads and cereals at least three
times a day. Look for the word "whole grain" or "whole wheat" on the label or as one of the first ingredients.
5. When selecting oils for household use, choose canola or olive oil.
6. To increase omega-3s, eat fish twice a week and/or give f1axmeal a cry.
7. Give soy foods a second chance. 8. Add nuts as a snack-just watch serving sizes. 9. Take a mulcivitamin each day-not as an excuse for a
poor diet, but to supplement a healchy one. Conclusion. Eating properly will not prevent all chronic dis
eases, but there is some pretty strong evidence for the dietary advice provided here. Diets high in fruits, vegetables, whole grains and ocher whole foods can prevent heart disease, some cancers, type 2 diabetes, stroke, high blood pressure and help to keep our weight in a healthy range.
The nutrition recommendations provided here are applicable for all ages, including young people. As we strive in our state to improve the health of all citizens, it is hoped chat those with decision-making responsibilities will provide support for better nutritional choices and increased physical activity for all ages. Changes chat promote healchier lifestyles will surely improve the quality of life for all South Carolinians.
31
32
References 1 Ame rican D ietetic Associat ion ( I 999) . Nutrition and You-Trends 2000 Final Report. 2 Uni ted Healcl1 Foundat ion (2003) . Americas health: State health rankings-2003 edition.
Retrieved on May 4, 2004 from: http://www.unitedhealthfoundacion.org/shr.2003/ Findin gs.hcml Kaiser Family Foundat ion (20 04) . State health facts online. Retr ieved on May 12, 2004 from: http: / /scacehealchfaccs.org. C ited by: Q uick, D. (2003, January 13) . South Caro lina health status on critical list. Charleston Regional Business journal Retrieved on May I 0, 2004 from: Imp:/ /www.charlestonbusiness.com/issues/6_ l / news/2457-1 .html. Ce nters for D isease Con tro l and Prevent ion (2004, February 11). National Vital Statistics Reports, 52( 13), 4 .
6 South Carolina De partm ent of Health and Environm ent al Co nt rol (2004) . SCAN Death Certificate Data. Retrieved on Jun e 2 1, 2004 from: http ://scang is.dh ec.sc.gov/ sea n net/ tab I es/ deat h 2 cab I e.aspx.
7 Sou th Caro lin a Depart ment of Heal ch and Environm ent al Co nt rol (2004). Annual Report, 2004.
8 South Ca rolin a Depa rtm ent of Health and Env ironm ental Co nt rol (2003) . Division of cardiovascular health. Presentat ion at SC DH EC conference.
9 Ce nters for D isease Co ntrol and Prevent ion (2004, Febru ary). The burden of chronic diseases and their risk factors: National and state perspectives.
IO Ce nters for Disease Co ntrol and Prevention (2003, November, 18) . Facts about heart disease: South Carolina. Ret rieved on May 10, 2004 from: http://a pps.nccd.c dc.gov/ giscvh/fact_s heet.asp.
11 C ited by: Centers for Disease Co nt rol and Prevention (2004, April). South Carolina basic imp lementation. Retrieved on May 11, 2004 from: http:/ /www.cdc .gov.cvh/ sta te_progra m /sc.htm .
12 South Caro lina Depart ment of Health and Envi ronm ent al Co ntr o l (2003, Ju ne). Welcome to the division of cardiovascular health. Retrieved on May 4, 2004 from: http: //www .scdh ec.gov I cvh/.
13 Gard ner, A. (2001) . M ap red raws stroke belt. The Mi lwaukee Channel. Retr ieved on May 28, 2004 from: htt p://w isn-rvhea1th.ip2 m.com .
14 South Caro lina Cent ral Cance r Registry {2002, November). Cancer in South Carolina: 1999 Cancer Incidence, South Ca rolina Department of Health and Environmental Co ntrol.
15 Ce nt ers for Disease Control and Preventi on {2003, Jun e 13) . 2003 Cancer Burden Data Fact Sheets - South Carolina. Retrieved on May 11, 2004 from: htt p:/ /www.cdc.gov/ cancer/ Can cerBurd en/sc .h tm.
16 South Ca rolina Departm ent of Hea lth and Environm ental Co ntrol & Diabetes Initi ative of South Ca rolin a (2000 ). Burden of Dia betes in South Carolina, 1999.
17 South Ca rolin a De partm ent of Hea lth and Envi ronm ental Co nt rol (200 3, Decem ber 15) . Division of Diabetes Prevention and Control. Retrieved on May 4, 2004 from : http: //www.scd hec.gov/ hs/co mhlch /diabetes/ index .asp.
18 Ce nters for Di sease Co nt rol and Preventi on (200 3) . Obesity trends. Retr ieved on May I 0, 2004 from: http:/ /www.cdc.gov/nccdph p/d npa/obesicy/trend/obesicy _d iabetes_scaces.hcm.
19 Cited by: Sou th Ca rolina Departm ent of Health and Environm ental Con tro l (1999, December). Report on the impact of obesity on health in South Carolina.
2° Ce nters for Disease Control and Prevention (2004 ) . Physical activity and good nutrition: Essential elements to prevent chronic diseases and obesity.
21 Centers for Disease Co nt rol and Preventi on (2004, Jan uary 23) . Overweight and obesity state programs. Retrieved on May 12, 2004 from: http: //www .cdc.g ov/ nccdh php /dnpa/ obesicy/state_progra ms/south _caro nlina.htm.
22 Ce nters for Disease Co ntrol and Prevention (2004) . Fast stats. Retrieved on May 4, 2004 from: h ttp://www.cdc.gov/ nchs.faststats/deachs.hcm.
23 C ited by: Na tiona l l nscicuces of Health (1998). Clinical guidelines on the identification, evaluation, and tream,ent of overweight and obesity in adults .
Bethesda, Maryland: Department of Health and Human Services, National Instit utes of Healrl1, National Heart, Lung, and Blood Institute.
24 National Research Counci l (1989). Diet and health: implications for reducing chronic disease risk. Washington, D.C.: National Academy Press.
25 Ci red by: United Stares Department of Health and Human Services (2003). Health United States, 2003, 230.
26 Sr. Jeor, S.T., Howard, B.V, Prewitt , TE., Bovee, V, Bazzarre, T., & Eckel, R.H. (2001). Dietary protein and weight reduction. Circulation, 104(15) , 1869-1978 .
27 Phytochemical watch: Resverarrol helps to prevent cancer, heart disease (2000). American Institute for Cancer Research, 69, 8.
28 Phyro-protect your health (2003, October). University of California, Berkeley Wellness Letter, 1-2.
29 Beyond the salt shaker: A new look at diet and blood pressure (June, 1997). Tufts University Health and Nutrition Letter, 8.
30 A new look at dietary patterns and hypertension (2001, May/June). Dairy Council Digest, 72(3), 13-18.
31 American Cancer Society (2002). Common questions about diet and cancer. Retrieved on May 19, 2004 from hrrp://www.cancer.org/docroor/PED/ content?ped_3_2X_Common_Quesrions_Abour_Diet_and_Cancer.asp
32 The beauty of tomatoes: Crushed, diced, or stewed (2002, April). University of California, Berkeley Wellness Letter, 5.
33 Cited by: Wyatt, H.R., Grunwald, G .K., Mosca, C.L., Klem, M.L. , Wing, R.R. & Hill,
J.O. (2002). Long- term weight loss and breakfast in subjects in the National Weight Control Registry. Obesity Research, I 0, 78-82.
34 Wardlaw, G.M., Hampl, J.S., & DiSilvesrro, R.A . (Eds .) (2004). Cardiovascular disease.
Perspectives in Nutrition, (p. 219) . New York: McGraw Hill. 35 The right start (2003, Fall). American Institute of Cancer Research Newsletter, 81, 12. 36 Cerea l: The whole rrum (2002, April). University California, Berkeley Wellness Letter, 3. 37 Liu, S., Sesso, H.D., Manson, J .E., Willert, W.C., & Buring, J.E. (2003). ls intake of
breakfast cereals rel a red to total and cause-specific mortality in men? American Journal of Clinical Nutrition, 77, 594-599.
38 Jones, J.M., Reicks, M., Adams, J., Fulcher, G., & Marquart, L. (2004). Becom ing proactive with the whole-grains message. Nutrition Today, 39(1 ), 10- I 8.
39 Fiber lowers heart disease risk, but by how much? (2004, June). Tufts University Health and Nutrition Letter, 6.
40 Tufts nutrition: Translating the research for use at your table (2004, February). Tufts University Health and Nutrition Letter, 3-4.
41 Howath, N .C., Saltzman, E., & Roberts, S.B. (2001). Dietary fiber and weight regulation. Nutrition Reviews, 59(5), 129-139.
42 National Osteoporosis Foundation (2004). Disease statistics. Retrieved on May 14, 2004 from http://www.nof.org/osteoporosis/srats.htm.
43 National Osteoporosis Foundation (2004). Prevention. Retrieved on May 14, 2004 from http://www.nof.org/prevention/index.htm.
44 Dwyer, J.H., Li, L., Dwyer, K.M., Currin, L.R., & Feinleib (1996). Dietary cakium, alcohol, and incidence of treated hypertension in the NHANES l ep idemiolog ic follow-up study. American journal of Epidemiology, 144(9), 828-838.
45 Jacqmain, M., Doucet, E., Despres, J., Bouchard, C., & Tremblay, A. (2003) .
Calcium intake, body composition, and lipoprotein-lipid concentrations in adults. American journal of Clinical Nutrition, 77(6), 1448-1452.
46 National Dairy Council (2004). Diet and hypertension progress towards a better
understanding. Retrieved on May I 4, 2004 from: http:/ /www.nationaldai1ycouncil.org/healch/ digest/dcd/68-4.asp?page=4.
47 Cited by: American Cancer Society (2000). Calcium appears to be beneficial for colorectal cancer. Retrieved on June 2 1, 2004 from: http:/ /www.cancer.org/.
33
34
48 Ze mel, M .B., T hompson, W., M ilstead , A., Mo rris, K., & Ca mpb ell, P. (2004) . Calc ium and dairy acceleratio n of weight and far loss dur ing ene rgy restrict ion in obese adul ts. Obesity Research, 12, 582-590 .
49 McCa rron, K.A., & Heaney, R.P. (2004) . Estim ated healthcare savings associated with adequate dairy food intake. American journal of Hypertension, 17(1), 88-97 .
50 American D ietetic Association (2004) . Milk your diet : A new approach to fuel your weight loss efforts. Retrieved on May 13 , 2004 from http ://www.ea trighr.org/ Public/ N ur ririonl nformarion/92_ 18458 .cfm.
51 New stud y shows 3-4 servings of dair y each day help burn fat (2004 , April 16) . Natio11al Dairy Council. Retrieved on May 13, 2004 from: http://www. narionaldai rycoun cil.org/ press/alerr/ newsAlert_84 636.asp.
52 Yes, but which calcium suppl ement ? (1997, Febru ary). 7iifts University Health and Nutrition letter, 4-5.
53 University of Ca lifornia, Berkeley (200 3, February). Coral calcium. Retrieved on May 14, 2004 from ht tp:// berkeleywellness.com/ htm l/ds/dsCora lCa lcium.php.
54 Okin awa Ce nt enarian Stud y (2003, January 7) . Okinawa Centenarian Study position statement on coral calcium. Retrieved on May 14, 2004 from http ://okin awaprogram.com/ coral_calcium/co ral-calcium.h tml.
55 American D ietetic Associat ion (200 1) . A primer on fats and oils. Retrieved on May 13, 2004 from: h ttp://www .eatrighr.org/ Pub lic/N utri tionln formation/92_9292 .cfm.
56 American Heart Association (2004) . Fat. Retrieved on May l 7, 200 4 from http :/ /www.americanhearr.or g/ presen rer. j h tm i 'ide n t i fier=4 582.
57 Liebm an, B. (2002 July/August). Face the fats. Nutrition Action Newsletter, 3-6 . 58 Stealth fats: How food makers hide them from you (200 2, April) . University of
California, Berkeley Wellness Letter, 7(18), 1. 59 Ascherio, A., Srampfer, M.]. , & Willett , W.C. (1999) . Trans fatty acids and coronary heart
disease. Departm ents of Nutriti on and Epidemiology, Harvard School of Public Health . 60 United Scares Depart ment of H ealth and Hum an Services (200 3, July 9). HHS to
require food labels to include trans fat contents. Retr ieved on May 17, 2004 from h ttp ://www .hh s.gov/ news/press/2 00 3pres/2 0030709 . h rm!.
61 Hut chinso n, R., Co llins, J ., & Powell, P. (2001 ). Mediterranean dietfimnd to be more
effective than strict low fat option. Brigham Wo men's Ho spi tal. 62 American Ca ncer Society (2000 ). Omega-3 fatty acids. Retr ieved May 19, 200 4
from http :/ /www.cancer.org/do croo r/ ETO /co n renr/ETO _5_3 X_ Om ega-3_ Farry _ acids.asp?sitearea + ET O .
63 Schm id, R.E. (2004) . FDA pushes limit ed fish int ake. The Sun News, 3A. 64 Tu fts University (2004, Sprin g) . A fish srory. 7iifts Nutrition, 5(2), 1. 65 American Heart Association Journ al Report (2003, April I ). Dia betic women gain
significant health benefits from eating fish . Retrieved May 19, 2004 from http :/ /www.americanheart.org/p resenrer.jhrm1?idenrifier=3010 5 18.
66 Five hot topics that might trul y spell bette r health (n .d.) . Special Supplement to the Tufts University Health and Nutrition letter.
67 Am erican Pharmacists Association (2003). New recommendations far omega-3 fatty acids. 68 American Heart Association Journ al Report (200 3, August, 12). Eatingfish may Lower
heart rate, reduce risk of sudden death. Retr ieved May 19, 2004 from h ttp: //www.a mericanh eart.org/ presen tcr. j h rm! ' idenrifier=30 l 44 2 5.
69 American Heart Associat ion (2004, May). Plan t based omega-3 fat s may help artery function . Retr ieved on May 19, 2004 from: htt p://www .americanhearr.org/ presen rer.jhrml ?ide nt ifier=302 l 876 .
70 Wardlaw, G .M ., Hamp !, J.S., & DiSilvestro, R.A. (Eds.) (2004) . Omega-3 . Perspectives in Nutrition, (p. 36 9). New York: McG raw Hi ll.
71 American Ca ncer Society (2000 ) . Flaxseed Retrieved M ay l 9, 2004 from: http://www.c.a1icer.org/docroor/ETO/co ntenr/ET0_5_3X_ Flaxseed.asp's itearea=ETO&vie .
72 FDA affirms health claim th at a hand ful of peanut s daily may help keep th e
heart doctor away (2003, July 15). The Peanut Institute. 73 Nuts are on a roll (2003, May). University of California, Berkeley Wellness letter, 19(8), I. 74 Amer ican Dietetic Association (2004). A nutty addition to a healthy diet. Retrieved on
May 13, 2004 from: http://www.earright.org/Public/Nurritionlnformarion/index_2956.cfm. 75 Cited by: Kris-Et herton, P.M., Pearson, TA., Wan, Y., Hargrove, R.L., Moriarty, K.
Fishell, V., & Etherton, TO. (1999) . High-monounsaturated fatty acid diets lower both plasma cho lestero l and rriacylglycerol concentrations . American Journal of Clinical Nutrition, 10( 6), I 009- 15.
76 La Bell, F. (200 I ). Food product development: Nuts about nutrition. Retrieved on May 13, 2004 from: www.preparedfoods.com.
77 Wome n who ear nuts or peanut butter regularly sign ificantly reduce their risk for type 2 diabetes (2002, November 26). Harvard School of Public Health.
78 Ame rican Dietetic Association (2004, May 13) . The best sources of soy. Retrieved on May 13, 2004 from: http://www.eatright.org/Print/index_l9465.cfm.
79 Messina, M. (1999). A close look at soybeans. In Ward law, G .M . (Ed.), Perspectives in Nutrition, (pp. 176- 177), New York: McGraw Hill.
80 Soyfoods Association of Nort h America (l 999). Soy and health. Retrieved on March 2, 2004 from: http://www .soyfoods.o rg/p ress/FAQ_healrh.hrm.
81 Henkel, J . (2000, May/June). Soy: Health claims for soy prote in , quest ions about other compo nents. FDA Consumer, 13-17.
82 lnsel, P., Turner, R.E., & Ross, D. (Eds.) (2004). Diet and health. Nutrition (p. 655) Sudbury, Massachusetts: Jones & Bartlett.
83 Genisoy ( 1999) . Soy facts-Answering your questions about soy. Retrieved on October 29, 1999 from: http: //www.genisoy.com/QA. htm.
84 lnsel, P., Turner, R.E., & Ross, D. (Eds.) (2004). Prote ins in rhe diet. Nutrition (p. 229). Sudbury, Massachusetts: Jon es & Bartlett.
85 Potter, S.M. (I 998) . Soy protein and cardiovascu lar disease: T he imp act of bioactive compone nts in soy. Nutrition Reviews, 56(8), 23 I -235.
86 Un iversity of lllino is, Urbana-Champaign (2004, May 7). Soy processing inAuences estrogen-depende nt breast cancer growth in mice. Science Daily. Retrieved on May 19, 2004 from: http:/ /www .sciencedai ly.com/ releases/2004/0 5/040 507083422. h tm.
87 Ame rican Cance r Society (1999). Soy and breast cancer. Retrieved on May 19, 2004 from http:/ /www.cance r.org/docroot/NWS/content/NWS_1 _ I x_Soy _and_Breast_ Ca ncer.asp.
88 Study: Increased multivitamin use by elderly could save Medicare $1.6B (2003 , November 2). Heart Disease Weekly, 42.
89 Study shows mu ltivitamin offers cardiovascular risk facto r protection (2004, June 25). Heart Disease Weekly, 29.
90 Heart beat: Dai ly mult ivitamin may chill inAammarion (2004, April). Harvard Heart letter. 91 Abby, S.L., Harris, I.M., & Harris, K.M. (1998). Homocysteine and cardiovascular
disease. journal of American Board of Family Practitioners, 11(5), 391-398. 92 Lashner, B.A., Provencher, K.S., Seidn er, D.L., Knesebeck, A., & Brzezinski,
A. (I 997) . T he effect of folic acid suppl ementation on the risk for cancer of dysp lasia in ulcerative colitis. Gastroenterology, 12( 1 ), 29-32.
93 W hite , E., Shannon , J .S., & Patterson, R.E. (1997). Relationship between vitamin and calciu m supple ment use and colon cancer. Cancer Epidemiology Biomarkers Prevention, 6(1 O), 769-774.
94 Barringer, T.A ., Kirk, J.K., Santaniello, A.C ., Foley, K.L., & Michielurre, R. (2003). Effect of a multivitamin and mineral sup plement on infection and quality of life. A randomized, double-blind, placebo-contro lled trial. Annals of Internal Medicine, 138(5), 365-37 1.
95 lnsel, P., Turner, R.E., & Ross, D. (Eds.) (2004). Choosi ng dietary suppl ements. Nutrition (p. 89). Sudbury, Massachusetts: Jones & Bartlett.
35
36
Biography: Sharon Howell Thompson was born in Greenwood and moved to Florence when she was two. She is the daughter of Dr. and Mrs. Alfred Wayne Howell Jr. of Florence and she has two younger siblings who live in Columbia, Allison Howell DeLoache and Al Howell.
Thompson graduated from West Florence High School in 1976 and completed a bachelor's degree in plant sciences at Clemson University in 1980. Two years later, she earned a master's degree in community and occupational education from the University of Sou th Caro lina .
In 1993, Thompson joined the Coastal Carolina University faculty as assistant professor, having earned an educational specialist degree in 1992 in the area of educational administration and an educational doctorate in 1993 in the area of health education administration-both from the University of South Carolina.
During her tenure at CCU, Sharon has overseen the development, implementation, and growth of the health promotion major. Starting with only seven students when the major began in 1997, the program has grown to 250 student majors and mmors.
A national authority on nutrmon and weight disorders, Thompson began more than a decade of inquiry with her dissertation research, "Adolescent Males' Body Image Perceptions of Themselves and Females." Sharon has authored or coauthored numerous peer-reviewed articles in international, national, and state journals on disordered eating; produced a 20-minute video for middle level teachers on body image; edited a cookbook entitled Tasteful Treasures: Healthy Favorites ftom Coastal Carolina University Students; and has made presentations at numerous national and local conferences on these topics. Additionally, Thompson has written articles in other ropic areas such as cooperative education partnerships and creating positive learning environments, and has co-authored a book chapter titled "Service learning: Meeting student and community needs."
Thompson has embraced the teacher-scholar model by integrating her research and service experiences into classroom lessons and by involving students in scholarly pursuits. Most recently, she sponsored several students at the National Conference for Undergraduate Research, co-authored manuscripts with students, and mentored student presentations. Thompson has continued her professional training with official recognitions as a certified health education specialist and a certified personal trainer. She has also earned South Carolina. teaching certifications for superintendent, high school supervisor, high school principal, biology, general science, and agriculture.
While teaching four classes each semester and advising approximately 100 students keeps her busy within the college, Thompson still finds time to serve her university, her profession, and her community, often in the role of chairperson, board member, coordinator, or other elected office. Thompson's commitment and involvement with the Waccamaw Youth Center, a
37
38
home for abused and neglected teenage males in Horry County, earned her The Sun News Volunteer of the Year Award for 2002-2003. She was also the recipient of the Excellence in Community Nutrition Award given by the Dannon Institute in 2003. In 1997 she was named the South Carolina Health Education Professional of the Year. The following year she was presented the Coastal Carolina University Student Affairs Award, and in 1999 she was named the Distinguished Teacher
and Scholar for the Spadoni College of Education. Additionally, she has written numerous grants and has been awarded almost $1 million in funding for various health promotion and technol
ogy-related projects.
Sharon is married to Frank Austin Thompson II, and they have two daughters, Leslie (18) and Austin (11). When Sharon, Frank, Leslie, and Austin are not supporting CCU sporting events , involved in church and community affairs, or enjoying their friends, family, and home in Conway, they are relaxing with their dog Snickers at the beach in Garden City.
Acknowledgements Special thanks to those who offered assistance in the editing and
content of this manuscript. Sherer Royce, assistant professor of Health Promotion, provided thoughtful insights which expanded the public health perspectives. Sohailla Digsby, registered dietitian for Waccamaw Public Health District, gave recommendations to increase the "user friendliness" of the nutrition information. Colleen Lohr, associate provost at Coastal Carolina University, gra
ciously assisted with the editing and content of this paper. Finally, special thanks to my husband, Frank, who read (yet) another one of
my manuscripts and provided me honest feedback. When he told me that this paper "was a very good compilation of all of the lectures our family has heard for the past decade," I knew all of my favorite
nutrition soapboxes were included.
Notes
Notes
111 r,rr,111,~rr,11nm111r[1111 1 300 00049955
IITC On the Ii ne for you every day
COASTAL CAROLINA U~ITY





























